Back to Journals » Journal of Pain Research » Volume 15
Evaluating Adherence of Evidence-Based Post-Operative Discharge Opioid Prescribing Guidelines and Patient Outcomes Two Weeks Post-Discharge
Authors Arwi GA, Tuffin PHR ![]() , Schug SA
, Schug SA ![]()
Received 20 October 2021
Accepted for publication 14 August 2022
Published 10 October 2022 Volume 2022:15 Pages 3115—3125
DOI https://doi.org/10.2147/JPR.S345241
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Erica Wegrzyn
Gerardo A Arwi,1,2 Penelope HR Tuffin,1 Stephan A Schug2
1Royal Perth Hospital, Perth, Western Australia, Australia; 2Anaesthesiology and Pain Medicine, University of Western Australia, Perth, Western Australia, Australia
Correspondence: Gerardo A Arwi, Email [email protected]
Introduction: There is a growing public health concern regarding inappropriate prescribing practices of discharge analgesia. A tertiary Australian hospital first developed its Postoperative Inpatients Discharge Analgesia Guidelines after an initial audit in 2015. Adherence to the guidelines were evaluated in 2016 and 2017 which show reduced compliance from 93.5% in 2016 to 83.4% in 2017.
Aim: To assess ongoing compliance with the guidelines five years following its implementation and to evaluate patient outcome in terms of its clinical impact and minimization of harmful events.
Methods: Prescribing data were obtained for discharge analgesic medication for 200 surgical patients from August 2019 to April 2020. Records were assessed against the hospital’s Postoperative Inpatients Discharge Analgesia Guidelines and compared with equivalent data from the previous 2015, 2016, and 2017 audits. Patients were interviewed by telephone two weeks after hospital discharge.
Results: Prescribing of analgesia was most compliant with overall guidelines for paracetamol (100% unchanged from 2017), followed by celecoxib (98%, up from 96% in 2017), tramadol IR (89% up from 74% in 2017), and pregabalin (89% up from 50% in 2017). Two weeks after discharge, 112 (56%) patients were surveyed and reported a mean pain-score of 2 (95% CI 1.5– 2.5) out of 10 at that time. Thirty-two (29%) patients interviewed were still taking pain medication, with 17 (53%) taking medication supplied from the hospital. Seventy-eight (88%) patients stored their pain medication in an unlocked location. Among those no longer taking analgesia, 28 (43%) had unused pain medications, and only two (6%) had returned these to a community pharmacist.
Conclusion: This study found that compliance with hospital discharge analgesia prescribing guidelines has increased, although there is room for improvement. Follow-up of the participants reveals high rates of unused opioids, improper storage and disposal of their pain medication.
Keywords: discharge, analgesia, opioid, guidelines, pain, surgery, postoperative, pharmacotherapy
Introduction
There is a growing public health concern regarding the current prescribing practices of post-discharge analgesia.1 The number of patients discharged from the hospital with opioids for ongoing management of acute pain is rising.2,3 One of the reasons for this trend is the increasing number of ambulatory or short-stay surgery leading to requirements of more aggressive discharge analgesia planning.4 Prescribing appropriate discharge opioids remains a challenge. The increasing rate of opioid prescriptions can lead to the development of opioid diversion, misuse, and unintentional long-term use.5 Drug poisoning deaths in USA involving opioid drugs quadrupled from 1999 to 2010.6 In Australia, there is 1.7-fold increase in deaths due to opioids between 2002 and 2011.7
The importance of high-quality hospital guidelines for prescribing discharge opioids cannot be understated. Research has shown that introduction of state-wide guidelines improves opioid stewardship in hospitals.8 Adhering to evidence-based hospital guidelines is an important component in the provision of safe and effective acute pain management.9 However, ongoing compliance with the guidelines can be a challenge.
The Royal Perth Hospital (RPH) is a 450-bed tertiary teaching hospital in Western Australia. RPH provides a wide range of specialist surgical services including plastics, general surgery, orthopaedic, urology and vascular. The RPH Postoperative Inpatients Discharge Analgesia Guidelines (Guidelines) were created in 2015 via professional consensus from a group of pain specialists, anaesthetists, pain nurses and pharmacists at RPH. Audits assessing adherence to the Guidelines were performed in 2015, 2016, and 2017.9 Overall there have been improvements in appropriate discharge analgesia prescribing since 2015, however results from 2017 show reduced compliance to the Guidelines in comparison to 2016. This demonstrates that maintaining adherence to the Guidelines over an extended period of time remains an ongoing challenge.
Aim
The aim of this audit is two-fold. First, to assess whether the improvements in post-operative discharge analgesia prescribing have been sustained five years following the implementation of the Guidelines. Second, to evaluate patient outcome from the Guidelines in terms of its clinical impact in relation to post-discharge pain level, and minimisation of potential harmful events associated with discharge analgesia such as excessive ongoing use, as well as improper storage and disposal of opioids.
Materials and Methods
This audit was approved by RPH as a quality improvement activity and for publication (WA Health GEKO approval 31394).
The first stage of this audit involved assessing adherence to the RPH Postoperative Inpatients Discharge Analgesia Guidelines (Box 1). The methodology to assess this outcome was based on previous audits at RPH on adherence to the Guidelines performed in 2015, 2016, and 2017.9 This study obtained analgesic medication dispensing data for all patients discharged from surgical wards of RPH from August 18, 2019 to April 1, 2020; excluded were patients prescribed paracetamol only or discharged from emergency department or medical wards.
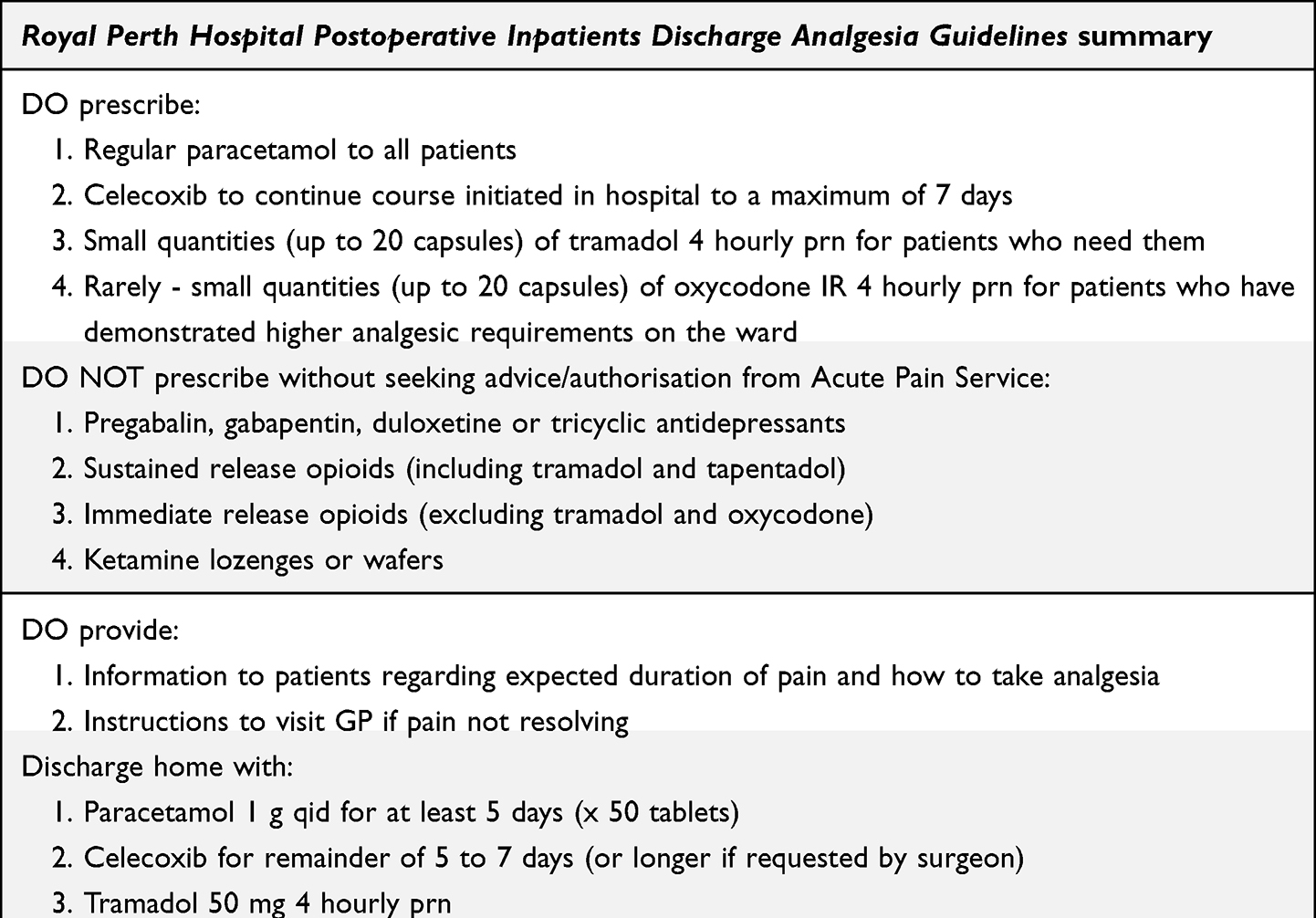 |
Box 1 Summary of the Royal Perth Hospital Postoperative Inpatients Discharge Analgesia Guidelines |
Data were collected retrospectively from patients’ medical records. The prescribing of analgesia at discharge was evaluated against the hospital Guidelines, which included assessing the type of analgesia, quantities and dosing of medications prescribed, involvement of the Acute Pain Service (APS), and whether instructions were given to the patient to see their general practitioner (GP) if pain is not resolving.
Prescriptions were classified as complying with the Guidelines if they fully adhered to the “DO prescribe” and “DO NOT prescribe” rules of the Guidelines. The quantity of medication prescribed was also assessed as complying with the guidelines if they fully adhered to the recommendations. Prescriptions for analgesic medication that patients were taking prior to hospital admission were considered repeat prescriptions and excluded from analysis. Data collected were then compared to equivalent data from the previous 2015, 2016, and 2017 audits.
The second stage of this audit involved random selection of a subset of the surgical patients via telephone survey to determine patient outcome from the Guidelines. A 17-question survey was developed to assess their post-discharge pain (Question 1 to 2), information given about their pain medication (Question 3 to 5), pain medication use after discharge (Question 6 to 9), any unused pain medication (Question 10 to 12), storage of pain medication (Question 13 to 14), and patient perception of number of prescribed tablets/capsules they were given on discharge (Question 15 to 16) (Supplemental Figure 1).
The calls were made two weeks following discharges on a weekend. In the event of a nonresponse, another attempt was made the following day. Consent was obtained verbally at the start of the survey.
Results
Data were collected for 200 patients discharged from ENT surgery, general surgery, neurosurgery, oral surgery, orthopaedic surgery, plastic reconstructive surgery, spinal surgery, and urology wards at the Royal Perth Hospital from August 18, 2019 to April 1, 2020. Of the 200 patients, 112 (56%) completed the telephone interview, 74 (37%) did not answer the call and 14 (7%) declined to participate. Table 1 shows the gender, age, and length of stay of responder and non-responder to the telephone interview.
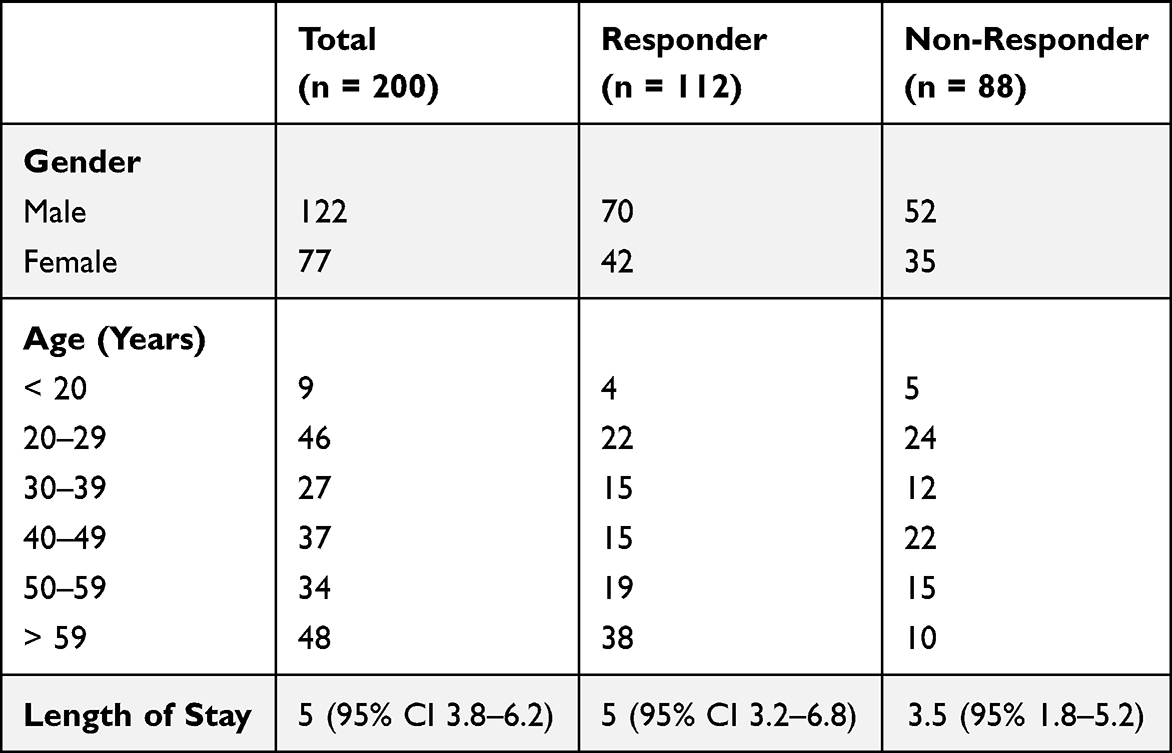 |
Table 1 Characteristics of Responder and Non-Responder to Telephone Interview |
Assessing Adherence to the Post-Operative Inpatients Discharge Analgesia Guidelines
The most commonly prescribed analgesia was paracetamol with 176 (89%) patients receiving it on discharge (Figure 1). This was followed by celecoxib 102 (51%), tramadol immediate-release (IR) 98 (49%), oxycodone IR 40 (20%), tapentadol modified-release (MR) 36 (18%), pregabalin 20 (10%), buprenorphine sublingual tablets 9 (4.5%), and ketamine lozenges 2 (1%) patients. No patient had a new prescription on discharge for a slow-release opioid or opioid transdermal patch.
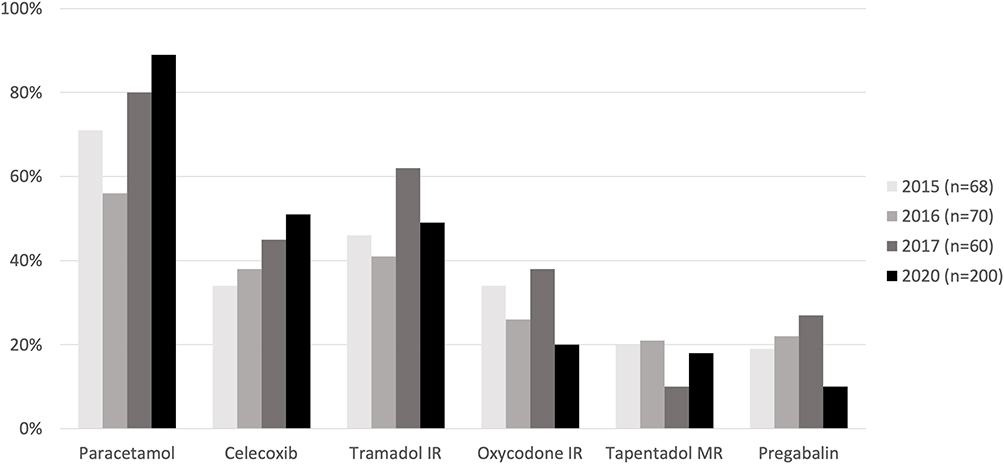 |
Figure 1 Analgesia on discharge. |
The overall compliance with the Discharge Analgesia Guidelines was 94.0%. The overall compliance has improved from 83.4% in 2017, and it was similar to the 93.5% rate in 2016. Table 2 compares the gender, age, and length of stay between the compliant and non-compliant participants.
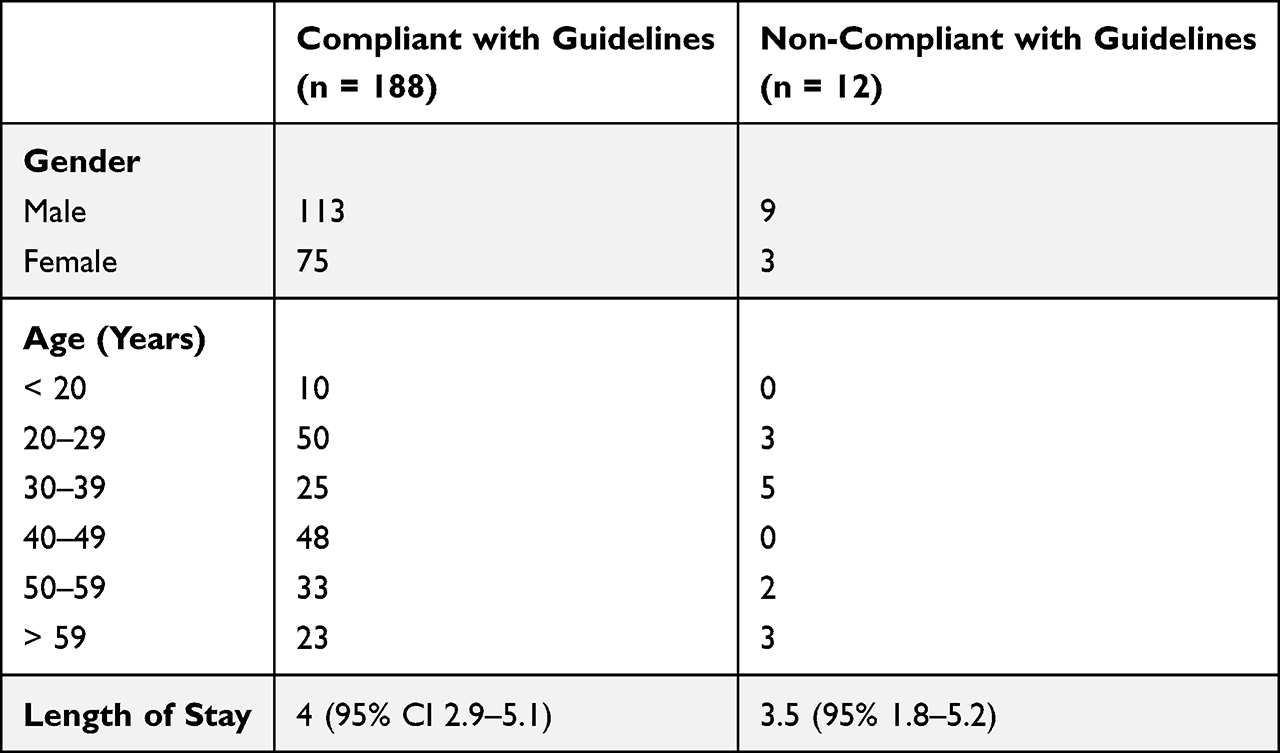 |
Table 2 Characteristics of Participants Who Were Compliant and Non-Compliant with the Guidelines |
The highest compliance rate involved paracetamol (100% unchanged from 2017) (Figure 2). This was followed by celecoxib (98%, up from 96% in 2017), tramadol IR (89% up from 74% in 2017), pregabalin (89% up from 50% in 2017), oxycodone IR (83% up from 74% in 2017), and tapentadol MR (61% up from 60% in 2017).
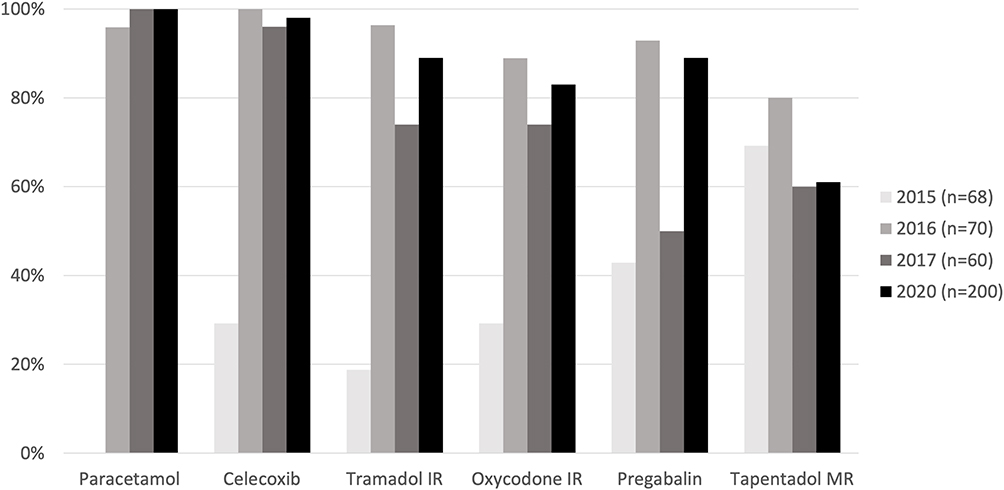 |
Figure 2 Compliance with guidelines: medication. |
Medications most compliant with quantity guidelines for prescription on discharge were paracetamol (100%, up from 96% in 2017), followed by celecoxib (98% up from 86% in 2017), tramadol IR (80%, up from 66% in 2017) and oxycodone IR (76%, up from 56% in 2017) (Figure 3).
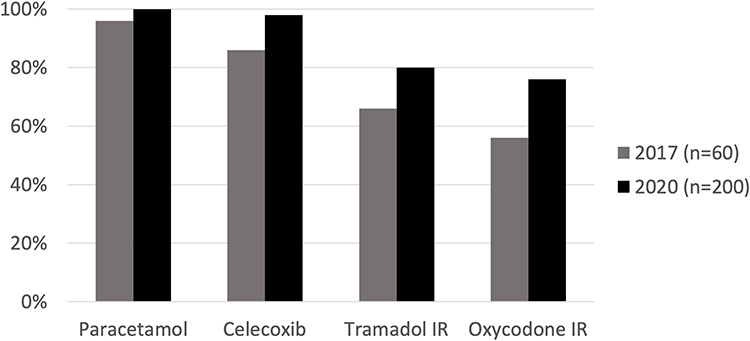 |
Figure 3 Compliance with guidelines: quantity. |
APS was involved in the pain management on the wards of 30% of the patients in this 2020 audit (up from 18% in 2017, 9% in 2016, and 26% in 2015). When APS involvement was indicated for prescribing discharge analgesia, APS input was identified in 73% of cases.
Overall, 32 (16%) patients were discharged with instructions written in their discharge letter to see their GP if their pain is not resolving (up from 14% in 2017).
Evaluating Patient Outcomes from the Post-Operative Discharge Analgesia Prescribing Guidelines
Patients reported a median pain-score two weeks after hospital discharge of 2 on a numerical pain scale of 0 to 10 (95% CI 1.5–2.5). When asked about their level of satisfaction with their pain control post-discharge from the hospital, 57% of participants reported being very satisfied, 15% reported being mostly satisfied, 15% reported being neither satisfied or unsatisfied, 7% reported feeling mostly unsatisfied, and 5% reported not being satisfied at all.
Eighty-three (74%) participants reported receiving written information about their pain medication, and 100 (90%) verbal information. The levels of patient satisfaction with the information provided about their pain medication are illustrated in (Figure 4).
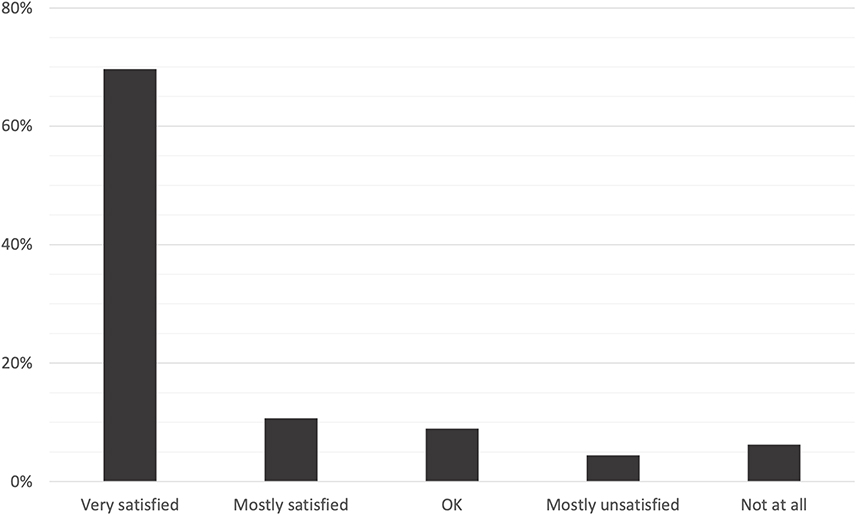 |
Figure 4 Patient perception on information regarding pain medication. |
Storage locations for their pain medication were the kitchen cupboard (45%), bedroom drawer (17%), medicine cabinet (11%), dining room (10%), fridge (12%), and bathroom (5%). Ninety-eight (88%) participants stored their pain medication in an unlocked storage.
Thirty-two (29%) participants were still taking pain medication at the time of the survey. Of those, 17 (53%) were taking pain medication received at discharge from the hospital, 13 (41%) medication prescribed by their GP, and 2 (6%) medication prescribed at a follow-up clinic. Table 3 compares the gender, age, and length of stay between participants who required secondary scripts with participants who did not require secondary scripts.
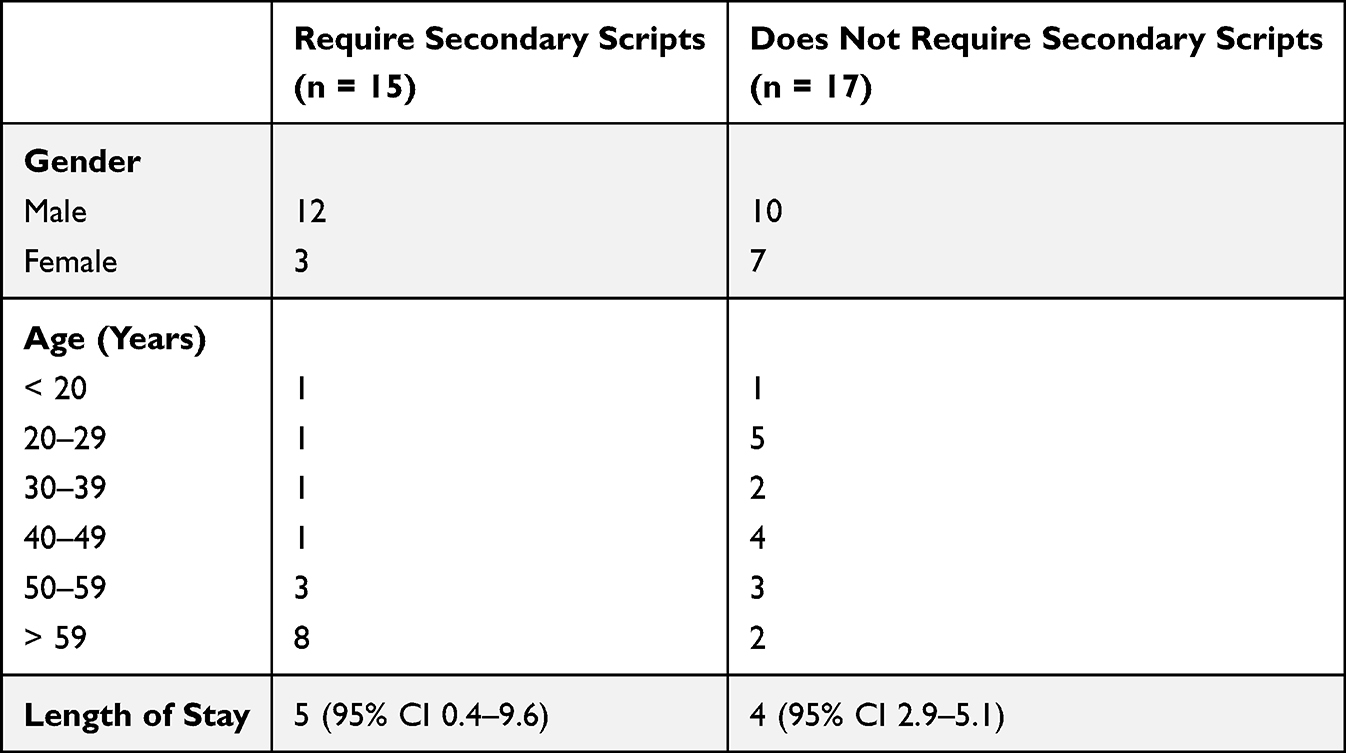 |
Table 3 Characteristics of Participants with Secondary Scripts and Participants without Secondary Scripts |
The pain medication still being consumed at 2-weeks post-discharge, the frequency of use, and the source are summarised in Table 4. Note that some participants were taking more than 1 pain medications at a time. The survey question did not distinguish between immediate-release and slow-release.
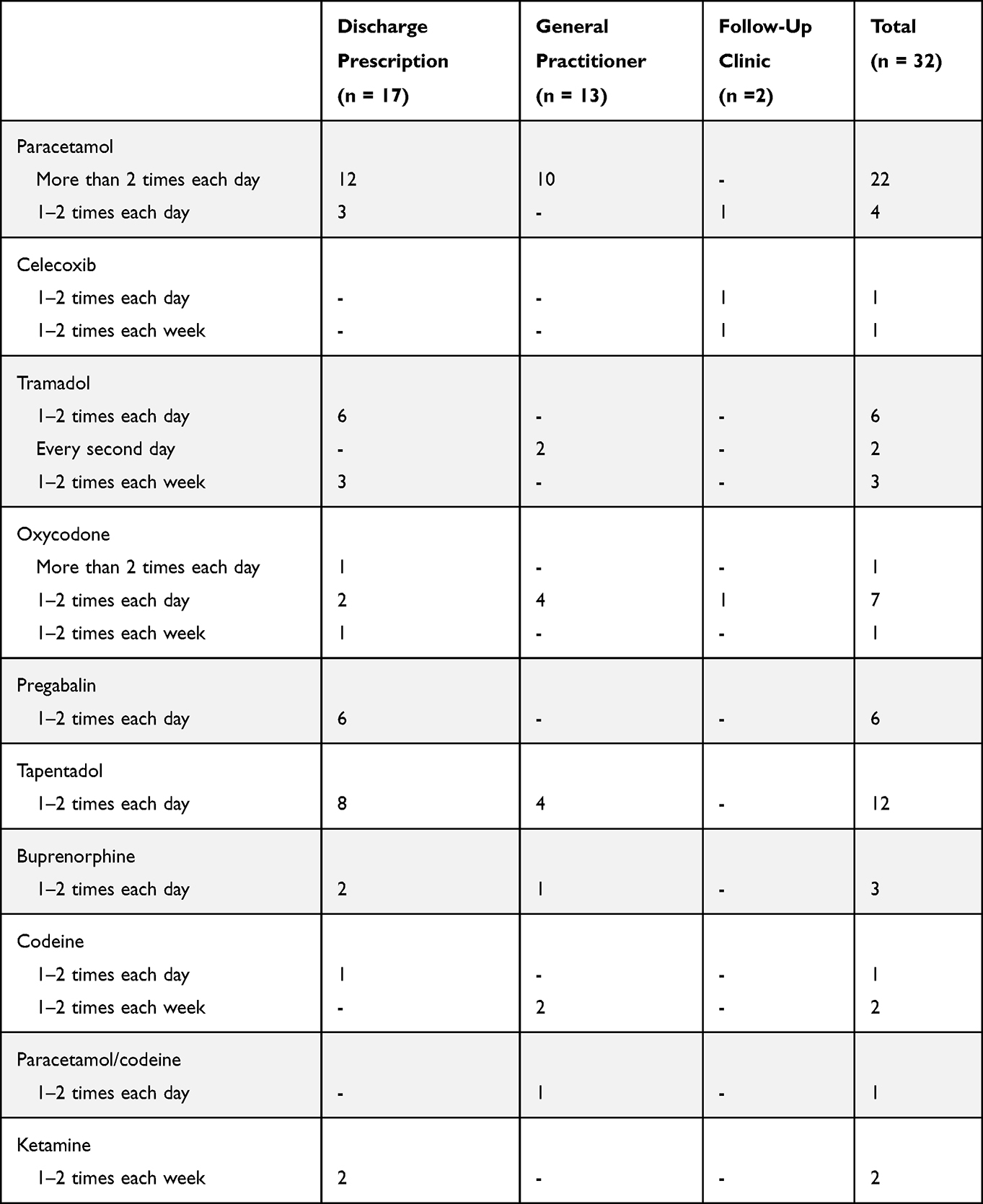 |
Table 4 Summary of Pain Medication Still Being Consumed 2 Weeks Post-Discharge |
Conversely, 80 (71%) participants were no longer taking any pain medication. From those, 28 (43%) had leftover pain medication from their discharge supply. Amongst participants with leftover pain medication, 7 (12%) had disposed of it in the rubbish bin, while 2 (6%) returned their unused pain medication to a pharmacist. The most common unused pain medication, without taking into account the number of individual pills, were paracetamol (43%), followed by tramadol IR (25%), oxycodone IR (22%), tapentadol MR (4%), buprenorphine (4%), and celecoxib (2%) (Figure 5). In total, still remaining in the home at the time of interview were 457 unused paracetamol tablets, 143 tramadol IR capsules, 45 oxycodone IR tablets, 18 tapentadol MR tablets, 10 celecoxib capsules, and 10 buprenorphine tablets.
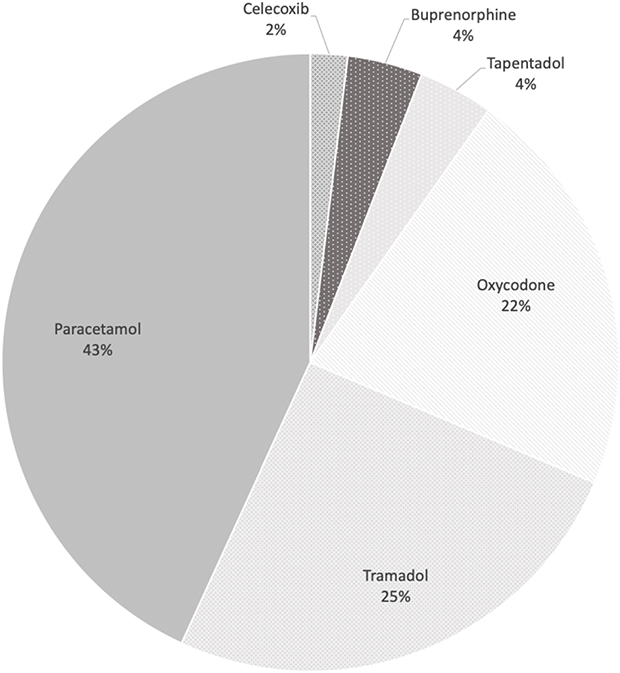 |
Figure 5 People with unused medication at 2 weeks post-discharge. |
When asked about their satisfaction with the amount of pain medication prescribed upon discharge, 27 (24%) participants reported being prescribed too few tablets, 77 (69%) reported being prescribed the right amount, and 8 (7%) reported being prescribed too many pain tablets.
Discussion
This study found that analgesia prescribing on discharge has changed over time in the hospital. Paracetamol is still the most prescribed discharge pain medication, but celecoxib has overtaken tramadol as the second most commonly prescribed medication. Looking at the overall trend of discharge analgesia prescription from 2015 until now, the rates of paracetamol and celecoxib prescribing have increased, while the rates of tramadol IR, oxycodone IR, tapentadol MR, and pregabalin prescribing have decreased. The increased prescribing of non-opioids, coupled with the decreased prescribing of opioids and pregabalin, are important findings as they illustrate that safer analgesic prescribing following evidence-based recommendations is being observed over time.
Overall compliance with the Guidelines has improved for most pain medications compared to 2017. Notably, the significant increase in compliance rate for pregabalin may be explained by increased APS input, a requirement specified in the Guidelines.
Gabapentinoids such as pregabalin and gabapentin were historically considered to be non-addictive with low potential for abuse, however there is now growing evidence that pregabalin misuse is increasing worldwide.10 Increasing literature regarding the addictive nature of gabapentinoids may lead to a change in the discharge prescription guidelines away from these medications. Conversely, poor compliance with tapentadol MR was noted due to the lack of APS input prior to discharge. The relatively small size of participant in this study who were non-compliant with the guidelines compared to those who are compliant means a meaningful analysis between the group cannot be performed.
A recent systematic review identified high rates of unused discharge opioids in the community and emphasized the importance of adherence to evidence-based hospital guidelines.2 Appropriate discharge analgesic prescribing is crucial in reducing the rates of opioids and pregabalin abuse and misuse in the community. The compliance to quantity recommendations has improved for all discharge analgesia compared to 2017 in our hospital. The compliance with quantity guidelines for celecoxib, tramadol IR and oxycodone IR has improved significantly from 2017, although there is still room for improvement. The quantity guidelines are based on inpatient pain medication usage before discharge, which has been shown to be the best predictor of post-discharge opioid requirements.11 Giving patients more pain medication than they need can lead to unused pain medication. Clinical pharmacists are experienced in recommending the appropriate quantity of discharge pain medication, and their expertise should be regularly consulted to ensure best-practice prescribing.12
This study showed that the majority of patients had low levels of pain 2 weeks after hospital discharge, therefore indicating that their analgesia plan was appropriate. However, nearly a third of patients were still taking analgesia, with the majority of these patients still using the tablets they received upon leaving the hospital. The most common analgesia still taken was paracetamol, a safe and appropriate analgesia for longer term use. Tapentadol MR, tramadol IR, and oxycodone IR were the next most common medications that these patients were still taking after discharge. We note one patient who described receiving codeine from the hospital; however, this is inconsistent with their medical record. It is difficult to determine if these continued therapies were appropriate without clinical assessment, which reinforces the difficulty in weaning pain medication outside the infrastructure of a hospital. The need for step-down analgesia after discharge is becoming increasingly common due to the rise in ambulatory surgeries.13 One possible solution to this is the implementation of a transitional pain services adept at managing post-operative pain using multimodal analgesic regimen.4
The study showed that 13% of responders were taking medications prescribed from a second source, either from their general practitioner or outpatient clinic. This emphasizes the importance of follow-up with a general practitioner as stipulated in the guidelines, to ensure that patients continue to have a proper analgesia regimen in the community. Furthermore, this figure may suggest a gap in Guidelines efficacy, as these participants received inadequate post-discharge analgesia. One possible explanation for this is inadequate tailoring of the guidelines to individuals in this group. The guidelines do not consider patient’s pre-admission characteristics that may predispose to them to either decrease or increase analgesic needs post-discharge may be responsible for the excess quantities of medications of patients in this study. Further refinement to the guidelines may implement patient’s pre-admission characteristics to personalize the guidelines to suit their analgesic needs.
Within the group of patients that have ceased taking pain medication, 43% had leftover medication, this is lower rate than the more than two-thirds of patients previous studies have reported.14 In addition, the most common medication remaining in the patients’ homes was paracetamol accounting for 67% of all tablets/capsules. There were, however, also a large number of unused opioids. This underlines the value of following quantities recommended by evidence-based guidelines. Physicians are often inclined to give excess analgesics under the assumption that more discharge pain medications are equal to better pain control. Unused discharge opioids have been shown to lead to prolonged opioid use, as well as abuse, misuse, and diversion.2 Very few patients in this study reported taking unused medication to a pharmacy for disposal. These findings highlight a gap in patient knowledge and/or education regarding proper storage and disposal of pain medication, consistent with another recent study.15
Hospitals need to continuously review their evidence-based discharge analgesia prescribing Guidelines to improve analgesic stewardship. The evaluation of adherence to the RPH Guidelines is planned to continue on a regular basis, and results from this study will form the benchmark for compliance with future post-operative discharge analgesia prescribing. The expanded scope of this study, which included the follow-up of patients 2 weeks post-discharge, also needs continuous assessment. Results from this study will also improve on the growing literature surrounding post-operative discharge analgesia prescribing and can be used as reference for future national and international guideline.
To our knowledge, this is the first study to measure both the adherence to prescribing guidelines and patient outcome in the same group of participants. This allows a more meaningful analysis of the Guidelines and introduces more directed improvements. The large sample size of this study increases its validity. The large data collection period reduces the chance that the data are affected by any seasonal variations or situations that affect prescribing practices temporarily.
This study has several limitations. This is a single-institution, observational study, and hence causality and efficacy of guidelines cannot be inferred from the result. Analysis regarding how post-operative discharge analgesia prescribing varies between surgical subspecialities is outside the scope of this study. The guideline is consensus-based, and while it was formed in accordance with the latest research surrounding post-operative discharge analgesia, its accuracy remains uncertain. The previous audits, used for comparison, were conducted by different clinical staff and, hence, there may be some inconsistencies in interpretation of the Guidelines in ambiguous situations. The prescribing data presented are dependent on accurate documentation by the hospital staff. Information pertaining to consumption, leftover medication, storage and disposal are self-reported by the patients, and hence they might be unintentionally affected by recall bias or deliberately inaccurate due to social desirability bias.16 The single follow-up at 2 weeks after hospital discharge might not be sufficient to accurately deduce the patient’s long-term behaviour regarding their pain medication, and the 2-week follow-up might miss patients with poor pain control within days of discharge. The survey was not validated. Furthermore, the time frame of this study (August to April) does not align with the 2017 audit (April to July). The study did not evaluate the characteristics of non-responder to the telephone survey, which may lead to possible non-response bias. Another limitation is the small sample size of non-compliant participant in this study, preventing analysis between the two groups.
Conclusion
This study found that compliance with hospital discharge analgesia prescribing Guidelines has improved. There are some aspects that need more focus such as consulting with medication and pain management experts when appropriate and ensuring patients have instructions to see their general practitioner for further pain management. Follow-up of the participants reveals high rates of unused opioids as well as improper storage and disposal of their pain medication. High rates of unused opioids were identified which can contribute to the unused opioid reservoir in the community. This study highlights the importance of adhering to hospital guidelines, discussing with clinical pharmacists and Acute Pain Services when appropriate, and educating patients about how to take their analgesia safely and appropriately, and how to store and dispose of their pain medication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors report no funding was received for this study.
Disclosure
Gerardo A Arwi and Penelope HR Tuffin have no conflicts of interest to declare. Unrelated to this study, the Anaesthesiology Unit of the University of Western Australia, but not Professor Schug personally, has received research and travel funding and speaking and consulting honoraria from Aspen, Biogen, Foundry, Grünenthal, Indivior, iXBiopharma, Komipharm, Luye Pharma, Mundipharma, Pfizer, Phosphagenics, Pierre Fabre, Seqirus and Xgene within the past three years. Since October 2019, again unrelated to this study, Professor Schug personally has received travel funding, speaking and consulting honoraria from Aspen, ESA, Grünenthal, HealthEd, Seqirus, Therapeutic Guidelines and WAPHA. The authors report no other conflicts of interest in this work.
References
1. Makary MA, Overton HN, Wang P. Overprescribing is major contributor to opioid crisis. BMJ. 2017;359:j4792. doi:10.1136/bmj.j4792
2. Arwi GA, Schug SA. Potential for harm associated with discharge opioids after hospital stay: a systematic review. Drugs. 2020;80(6):573–585. doi:10.1007/s40265-020-01294-z
3. Macintyre PE, Huxtable CA, Flint SL, Dobbin MD. Costs and consequences: a review of discharge opioid prescribing for ongoing management of acute pain. Anaesth Intensive Care. 2014;42(5):558–574. doi:10.1177/0310057X1404200504
4. Roth B, Boateng A, Berken A, Carlyle D, Vadivelu N. Post-operative weaning of opioids after ambulatory surgery: the importance of physician stewardship. Curr Pain Headache Rep. 2018;22(6):40. doi:10.1007/s11916-018-0694-4
5. Schug SA, Palmer GM, Scott DA, Halliwell R, Trinca J. Acute pain management: scientific evidence, fourth edition, 2015. Med J Aust. 2016;204(8):315–317. doi:10.5694/mja16.00133
6. CDC. QuickStats: number of deaths from poisoning, drug poisoning, and drug poisoning involving opioid analgesics—USA, 1999–2010. Atlanta: Morbidity and Mortality Weekly Report (MMWR); 2013. Available from: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6212a7.htm.
7. Blanch B, Pearson SA, Haber PS. An overview of the patterns of prescription opioid use, costs and related harms in Australia. Br J Clin Pharmacol. 2014;78(5):1159–1166. doi:10.1111/bcp.12446
8. Weiner SG, Baker O, Poon SJ, et al. The effect of opioid prescribing guidelines on prescriptions by emergency physicians in Ohio. Ann Emerg Med. 2017;70(6):799–808.e1. doi:10.1016/j.annemergmed.2017.03.057
9. Stewart JE, Tuffin PH, Kay J, et al. The effect of guideline implementation on discharge analgesia prescribing (two years on). Anaesth Intensive Care. 2019;47(1):40–44. doi:10.1177/0310057X18811746
10. Evoy KE, Morrison MD, Saklad SR. Abuse and misuse of pregabalin and gabapentin. Drugs. 2017;77(4):403–426. doi:10.1007/s40265-017-0700-x
11. Hill MV, Stucke RS, Billmeier SE, Kelly JL, Barth RJ
12. Genord C, Frost T, Eid D. Opioid exit plan: a pharmacist’s role in managing acute postoperative pain. J Am Pharm Assoc. 2017;57(2s):S92–s98. doi:10.1016/j.japh.2017.01.016
13. Kharasch ED, Brunt LM. Perioperative opioids and public health. Anesthesiology. 2016;124(4):960–965. doi:10.1097/ALN.0000000000001012
14. Bicket MC, Long JJ, Pronovost PJ, Alexander GC, Wu CL. Prescription opioid analgesics commonly unused after surgery: a systematic review. JAMA Surg. 2017;152(11):1066–1071. doi:10.1001/jamasurg.2017.0831
15. Allen ML, Kim CC, Braat S, et al. Post-discharge opioid use and handling in surgical patients: a multicentre prospective cohort study. Anaesth Intensive Care. 2020;48(1):36–42. doi:10.1177/0310057X19895019
16. Brenner PS, DeLamater J. Lies, damned lies, and survey self-reports? Identity as a cause of measurement bias. Soc Psychol Q. 2016;79(4):333–354. doi:10.1177/0190272516628298
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.