Back to Journals » Journal of Pain Research » Volume 19
Evaluate the Analgesic Effect and Functional Recovery of Designed Novel 3D CT-Guided Intelligent-Assisted Radiofrequency Nonpharmacological Ablation for Suprascapular Nerve Entrapment: A Retrospective Study
Authors Fan J ![]() , Guang Z, Yang W, Li Y, Yang Q
, Guang Z, Yang W, Li Y, Yang Q ![]() , Feng W
, Feng W
Received 4 December 2025
Accepted for publication 5 March 2026
Published 10 March 2026 Volume 2026:19 580963
DOI https://doi.org/10.2147/JPR.S580963
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Andrea Tinnirello
Junzi Fan,1 Ze Guang,2 Wenzhe Yang,3 Yanyun Li,3 Qian Yang,1 Weike Feng1
1School of Medicine, Shandong University of Traditional Chinese Medicine, Ji’nan, Shandong, People’s Republic of China; 2School of Ophthalmology and Optometry, Shandong University of Traditional Chinese Medicine, Ji’nan, Shandong, People’s Republic of China; 3School of Acupuncture and Tuina, Shandong University of Traditional Chinese Medicine, Ji’nan, Shandong, People’s Republic of China
Correspondence: Weike Feng, School of Medicine, Shandong University of Traditional Chinese Medicine, Ji’nan, Shandong, 250355, People’s Republic of China, Email [email protected]
Background: Suprascapular nerve entrapment is a medical condition characterized by clinical symptoms such as neck and shoulder pain, discomfort, upper limb weakness, and heaviness. These symptoms are caused by the compression of the suprascapular nerve at the suprascapular notch. The treatment of this nerve entrapment has been a long-standing challenge. Intelligent-assisted radiofrequency neurolysis is a novel and promising non-pharmacological treatment. Herein, we presented the therapeutic efficacy of this technique in 40 patients.
Objective: This study was designed to evaluate the feasibility of three-dimensional (3D) CT imaging integrated with intraoperative intelligence-assisted calibration for radiofrequency ablation of the suprascapular nerve.
Methods: A total of 40 patients were enrolled. The control group received the conventional surgery, while the treatment group was given 3D CT imaging plus the intraoperative intelligence-assisted calibration. Intelligence-assisted refers to the use of a smartphone app based on gravity calibration to realize the precise measurement and correction of the puncture needle angle during the operation, combined with 3D CT imaging to achieve the accurate positioning of the suprascapular nerve entrapment site. Data was analyzed on the two groups, including the time taken from starting positioning to successful puncture, Visual Analogue Scale (VAS) scores and ROWE scores before and after treatment, the therapeutic effect, complications, and number of cases with abnormal electromyography (EMG) items before and after treatment.
Results: Time of puncture completion in the treatment group was significantly shorter than that in the control group (8.06 vs 15.98 min, p < 0.05). Postoperative therapeutic effect in the treatment group was also superior to that in the control group. The treatment group had significant differences between pre- and post-treatment VAS scores and had superior ROWE scores compared to the control group.
Conclusion: The application of 3D CT imaging combined with intraoperative intelligence-assisted calibration for suprascapular nerve radiofrequency ablation can effectively shorten the operation time, improve the procedural efficiency and therapeutic effect and significantly reduce patients’ clinical symptoms.
Plain Language Summary: To the best of our knowledge, our study is the first to test how well intelligent-assisted radiofrequency ablation works to treat suprascapular nerve entrapment (a condition that causes pain or weakness in the shoulder due to pressure on a specific nerve).
Our team found that this technique can accurately position the treatment area and shorten the time needed for surgery. It also produced promising clinical results and is suitable for minimally invasive procedures (surgeries that use small incisions, causing less harm to the body).
This means the surgery reduces stress for patients during the procedure, lowers the chance of related complications (problems after surgery), and creates a positive cycle that improves the overall treatment process.
Keywords: three-dimensional CT imaging, intraoperative intelligence-assisted calibration, suprascapular nerve, radiofrequency ablation, analgesic effect
Introduction
Suprascapular nerve entrapment is closely related to the unique anatomical position of the suprascapular nerve. The suprascapular nerve primarily arises from the C5-C6 nerve roots via the upper trunk of the brachial plexus. It mainly traverses the osteofibrous foramen, a spatially narrow and relatively fixed structure that is formed by the transverse scapular ligament and the spinoglenoid notch. When the upper limb is lifted or moved to the side, the nerve is extremely susceptible to traction and friction at this narrowed area, leading to inflammatory edema, adhesion, and nerve injury, and therefore entrapment symptoms. Therefore, entrapment of the nerve leads to an array of discomforts like cervicogenic dorsalgia, notalgia paresthetica, and SICK scapula.1 There may be two mechanisms to the pain associated with entrapment:2 First, the stretching or compression of the nerve trunk stimulates the inner layer of the nerve, which comprises the intrinsic innervation of the nerve sheath. Perineurial membranes function as nociceptors in a way that direct stimulation elicits pain impulses, resulting in neurogenic pain with movement. Stretched perineurial membranes may discharge inflammatory neuropeptides that bring about mast cell degranulation, vasospasm, local tissue ischemia, and clumping of leukocytes, leading to local pain. Second, the presence of tight bundles of tendons within the fibers of relevant skeletal muscles, such as the supraspinatus and infraspinatus muscles, results in muscle shortening, thus inducing contraction of secondary nerves and the production of myalgia.
It is estimated that shoulder pain secondary to rotator cuff injury with suprascapular nerve (SSN) involvement accounts for 1% to 4% of all shoulder pain cases.3–5 Cervical plexus nerve lesions are more prevalent in athletes and workers performing repetitive overhead movements. Rotator cuff injuries have also been investigated in specific athletic populations, including volleyball, baseball, tennis, and badminton players.6,7 According to clinical data from the Departments of Orthopedics and Pain Medicine in tertiary hospitals in Shandong Province, the overall incidence of suprascapular nerve entrapment in the adult population is approximately 0.8%, with a higher incidence (approximately 2.5%) documented in manual laborers and athletes; this condition exerts a significant adverse impact on patients’ work and daily life.
Suprascapular nerve entrapment can be treated either conservatively or surgically.8 Initially, conservative treatment is the most recommended option and the option more preferable in patients who are at early stage or exhibiting less severe symptoms. Recovery can be achieved within 6 to 8 months with non-steroidal anti-inflammatory drugs (NSAIDs) and physiotherapy (PT). Surgery is a necessary option when conservative treatment fails or a severe median nerve injury is present.9 The surgery is primarily intended to alleviate nerve compression and reestablish the normal functionality of nerve.10 Conservative treatment has certain limitations due to its therapeutic effect notably affected by the severity of the patient’s condition, the disease history, and individual differences.
Recent advances have been made in pain management approaches within non-traditional surgical procedures, including neuromodulation via peripheral nerve stimulation (PNS),11 transcutaneous electrical nerve stimulation (TENS),12 and radiofrequency ablation.13 As a non-invasive superficial intervention, TENS has key limitations including insufficient penetration depth and poor targeting accuracy. TENS can only provide temporary pain relief, and fails to address the underlying structural etiology of suprascapular nerve entrapment. For implantable PNS, as an invasive implantable modality, its core limitations include elevated risks of surgical trauma, infection, electrode displacement, electrode fracture, and other procedure-related complications. This treatment is associated with high costs and low medical insurance coverage. Furthermore, PNS is only indicated for refractory pain relief, and cannot resolve the underlying cause of nerve entrapment.
Radiofrequency ablation is a minimally invasive technique for treating suprascapular nerve entrapment with positive clinical results.14 Compared with oral non-steroidal anti-inflammatory drugs and opioid analgesics, it avoids systemic side effects such as gastrointestinal injury, drug dependence and liver and kidney function damage.15 However, this technique requires multiple CT scans, exposing patients to a considerable radiation dose, and its precision still needs to be improved.16 More critically, the success of the puncture largely depends on the operator’s spatial imagination and empirical experience, leading to variability among physicians of different seniority and limiting the technique’s adoption in primary care settings. The intelligent-assisted calibration in this study is based on the “Multifunctional Measurement” mobile app developed by Wuhan Zhenji Technology Co., Ltd., which utilizes the smartphone’s gravity calibration function to accurately measure and correct the angle error of the puncture needle in the coronal and sagittal planes during the operation, and cooperates with 3D CT imaging to realize the precise positioning of the suprascapular notch.
Most patients experiencing suprascapular nerve entrapment frequently present with tenderness in the suprascapular notch. In this study, the suprascapular notch was used as the target for performing radiofrequency neurolysis of the suprascapular nerve. Intelligence-assisted neurolysis combined technologies like 3D CT imaging and smartphone angle measurement to allow accurate intraoperative measurements of angles and distances and converted abstract angular deviations into quantifiable visual data. Compared to conventional radiofrequency neurolysis of the suprascapular nerve, this technique exhibited shorter operation time, less trauma, and greater therapeutic effect. Previous clinical studies have confirmed that intelligent-assisted navigation technology based on mobile terminal sensors can achieve millimeter-level puncture accuracy in minimally invasive interventions of peripheral nerves, with measurement error less than 1° for spatial angle, which is consistent with the accuracy of professional medical navigation equipment, and has been widely used in orthopedic and pain medicine procedures.17 The clinical significance lies in the following aspects: Firstly, by reducing the number of puncture attempts, it is expected to directly lower the incidence of complications (eg, hematoma, nerve injury). Secondly, the standardized angle measurement process reduces reliance on the operator’s “tactile sensation”, enhancing the reproducibility and homogeneity of the procedure. Lastly, improving the first-attempt success rate can significantly reduce the number of CT scans, thereby lowering medical radiation and shortening anesthesia waiting time, offering potential health economic benefits. Therefore, this study aims to evaluate the feasibility and clinical efficacy of this method in the treatment of suprascapular nerve entrapment.
Data Collection
Detailed Baseline Characteristics of Patients
Case analysis was performed on 40 patients with suprascapular nerve entrapment who were hospitalized between 2023 and 2024. The 40 enrolled patients were randomly divided into the treatment group and the control group by the random number table method (random sequence generation by SPSS 21.0 software, allocation concealment by sealed envelope), 20 cases in each group. The outcome assessors (who measured VAS, ROWE scores and counted complications) and the people who analyzed the data were blinded to the group assignment of patients to reduce selection bias and performance bias. The 2-month follow-up timeframe was selected based on the clinical characteristics of suprascapular nerve entrapment. The short-term therapeutic effect of radiofrequency ablation for peripheral nerve entrapment can be observed within 2 months after operation, and the pain relief and shoulder joint function recovery of patients tend to be stable, which is a commonly used follow-up timeframe in the preliminary clinical research of this field. Due to the preliminary nature of this single-center clinical study, the sample size was determined based on the previous relevant clinical research and the actual clinical conditions of our center. There were 12 males and 8 females in the control group aged between 51 and 77 years with a mean age of 63.8 ± 6.42 years. The treatment group consisted of 8 males and 12 females aged between 58 and 78 years with a mean age of 67.5 ± 4.91 years. No significant differences were noted in gender, age, and other variables between groups (P > 0.05). Disease duration (reatment group: 1.5–8.0 years, mean 4.2 ± 1.8 years; control group: 1.2–7.8 years, mean 4.0 ± 1.6 years), symptom severity (VAS score before treatment: treatment group 7.8 ± 1.2, control group 7.6±1.3), and previous treatments (all patients received conservative treatments such as physical therapy and nerve block, with no significant effect. All patients reported pain in the region innervated by the suprascapular nerve, accompanied by limited joint mobility. Local tenderness in the surface projection area of the suprascapular notch was observed, and local block therapy produced an effective relief from pain. Abnormal findings in EMG examination included visible spontaneous potentials, increased polyphasic potentials, and decreased motor unit potentials. Before treatment, there were 37 abnormal EMG items in the treatment group, including 6 patients with 3 abnormalities, 5 patients with 2 abnormalities, and 9 patients with 1 abnormality. The control group consisted of 36 abnormal EMG items with 5 patients having 3 abnormal items, 6 patients having 2 abnormal items, and 9 patients having 1 abnormal item.
Patients were enrolled with following exclusion criteria: (1) patients with severe primary diseases of the internal medicine system, infections, or severe mental health disorders; (2) patients with a prior history of shoulder joint surgery.
Therapeutic effect criteria:18 The ROWE score is a specific scale for evaluating the function of the shoulder joint, with a total score of 100 points, including pain (30 points), daily activity ability (40 points) and range of motion (30 points). The higher the score, the better the shoulder joint function; a score >90 points indicates complete recovery of shoulder joint function, 75–89 points indicates partial recovery, and <75 points indicates poor recovery. Criteria for radiofrequency neurolysis for suprascapular nerve entrapment: Cure: Complete disappearance of symptoms such as shoulder and back pain and discomfort, involved limb pain and discomfort, impairment of movement of the homologous limb, numbness with radiating pain in the affected limb; ROWE score >90 points. Effective: Partial relief of pain and discomfort over the back and shoulder, pain and discomfort over the affected limb, limitation in movement of the affected limb, numbness with pain that radiates in the affected limb; ROWE score of 75–89 points. Improved: Improvement in symptoms such as pain and discomfort in the shoulder and back, pain and discomfort in the affected limb, movement impairment of the corresponding limb, and numbness with radiating pain in the affected limb; Rowe score higher than the preoperative score. Ineffective: No appreciable relief of symptoms from that of the patient on admission to hospital.
Methods
Control Group Surgical Procedure
The suprascapular notch, through which the suprascapular nerve traverses, was approximately marked before the procedure. The angular bisector of the inferior angle of the scapula was then extended to intersect the line along the superior border of the scapula spine. Further, the lateral superior angle formed by these two intersecting lines was bisected to obtain an angular bisector. A mark 1.5 cm away from the vertex of this lateral superior angle along the bisector was placed and this marked point corresponded to the location of the suprascapular notch.
When all preparations has been completed, the patient was placed in the lateral decubitus position. A neutral electrode was placed on the exposed skin over the involved upper limb. After the suprascapular notch identified by CT was cleaned, a fenestrated drape was applied, local infiltrative anesthesia was administered, and the needle was inserted at the preoperative marked position. CT scans were acquired and reconstructed into 3D images for optimal needle trajectory adjustment. The images were utilized by the surgeon to verify and optimize the needle trajectory for insertion. This procedure required several CT scans for the surgeon to adjust the needle direction according to clinical experience until the needle tip was accurately aligned with the suprascapular notch.
The radiofrequency generator was connected, and the positive electrode was inserted in the cannula. The impedance of the puncture site was 350 Ω. Both sensory and motor nerve testing were performed separately, and there was minimal pain on the patient during the procedure. The procedure continued to the therapeutic phase using 42°C of therapeutic temperature and delivering pulsed radiofrequency ablation for 6 min. After treatment, the electrode was removed. The post-treatment examination did not show any significant discomfort or other visible pathology in the patient.
Lidocaine hydrochloride, triamcinolone acetonide, vitamin B12, and normal saline were injected as a combination solution into the puncture site. The needle was then withdrawn, and an adhesive bandage applied to close the puncture site. Symptomatic treatment, including analgesia to relieve pain, was administered postoperatively. The patient was instructed to do functional exercises in the affected limb and to keep the puncture site dressing as clean and dry as possible throughout the post-treatment period.
Treatment Group Surgical Procedure
The suprascapular notch, through which the suprascapular nerve traverses, was approximately marked before the procedure. The scapular spine was identified, and a line along the superior border of the scapular spine was drawn from the superior border of the scapular spine from vertebral border of the scapular spine to the apex of the acromion. The angular bisector of the inferior angle of the scapula was then extended to intersect the line along the superior border of the scapula spine. Further, the lateral superior angle formed by these two intersecting lines was bisected to obtain an angular bisector. A mark was placed 1.5 cm along this secondary bisector using an electronic acupuncture pen for precise localization. This marked point corresponded to the location of the suprascapular notch.
After all preparations had been completed, the patient was placed in lateral decubitus and a neutral electrode was put on the exposed skin overlying the involved upper limb. The needle was inserted at the site marked preoperatively. CT scans were subsequently obtained and reconstructed to 3D images. Subsequent to this, 3D mapping was done in order to quantify two major parameters: 1) the distance errors between the target site and the needle path along the coronal, sagittal, and axial planes; and 2) the angle between the target site and the site of needle insertion. Distance errors were corrected by the surgeon, and angle errors were measured and corrected in real time with the “Multifunctional Measurement” mobile app developed by Wuhan Zhenji Technology Co., Ltd. The measurement error range of the app for the puncture needle angle was ±0.5°, and the comparative test with the professional medical navigation device (Medtronic StealthStation S8) showed that the correlation coefficient of the angle measurement results was 0.98 (P < 0.001), which indicated that the app had high clinical reliability. The “Multifunctional Measurement” mobile app was installed on a common smart phone (Android system, version ≥10.0), and the gravity sensor of the phone was used to collect the spatial angle data of the puncture needle, and the real-time angle error was displayed on the app interface for the surgeon to adjust the puncture needle direction until the angle error was less than 1°. The gravity calibration function on the smartphone facilitated the measurement of accurate angle errors of the puncture needle in coronal and sagittal planes if the patient stood upright. With the position of needle insertion confirmed, stable positioning of the puncture needle was achieved once the errors in the coronal and sagittal planes were overcome. In principle, any smartphone with similar sensors could be used, but we used the same device for all patients to ensure consistency.
Once it reached the vicinity of the target site, the positive electrode was placed into the cannula, and the radiofrequency generator was connected. Other measures remain the same as before.
As shown in Figures 1 and 2: the angle in the coronal plane was 135° with a distance error of 29.1 mm; the angle in the sagittal plane was 52° with a distance error of 31.8 mm; and the angle in the horizontal plane was 11° with a distance error of 45.9 mm.
 |
Figure 1 The angle and the distance error in the three-dimensional horizontal, sagittal and coronal plane. |
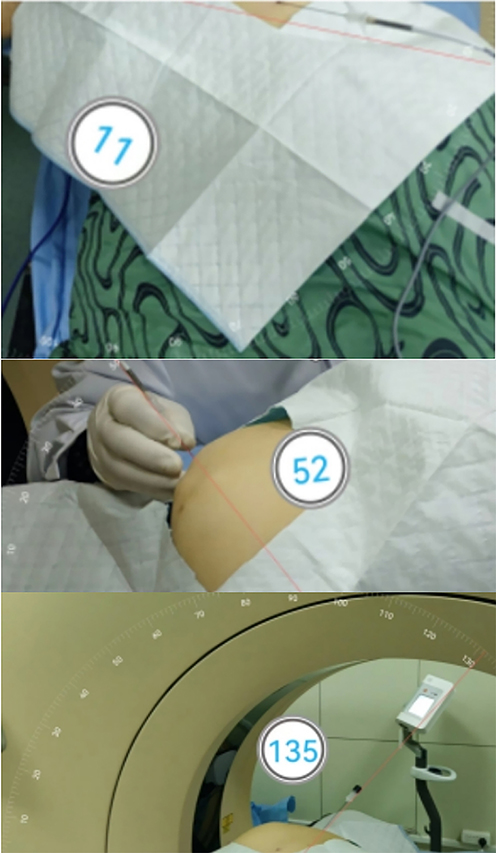 |
Figure 2 The angle of needle entry after horizontal, sagittal and coronal plane correction. |
Statistical Analysis
Statistical analysis was conducted using SPSS 21.0 to analyze the time taken from starting positioning to successful puncture, VAS scores, ROWE scores before and after treatment, therapeutic effect, complications, and the incidence of abnormal EMG findings before and after treatment in both groups. Primary end points: procedural time of puncture, postoperative 2-month VAS score and ROWE score; Secondary end points: overall effective rate, complication rate, number of abnormal EMG items. The measurement data were presented as  . The independent t-test was utilized for intergroup comparisons and paired t-test was employed for intragroup comparisons before and after treatment. The chi-square test was employed to analyze differences in the total effective rate and complication rate. A value of P < 0.05 was considered statistically significant. When comparing multiple outcomes (VAS, ROWE) at multiple time points, the Bonferroni correction was used for multiple comparisons to reduce the risk of Type I error, and the corrected P-value <0.0083 was considered statistically significant.
. The independent t-test was utilized for intergroup comparisons and paired t-test was employed for intragroup comparisons before and after treatment. The chi-square test was employed to analyze differences in the total effective rate and complication rate. A value of P < 0.05 was considered statistically significant. When comparing multiple outcomes (VAS, ROWE) at multiple time points, the Bonferroni correction was used for multiple comparisons to reduce the risk of Type I error, and the corrected P-value <0.0083 was considered statistically significant.
Results
Comparison of Successful Puncture Time Between the Control Group and the Treatment Group
In the treatment group, a method was implemented that integrated intraoperative data measurement through 3D CT images reconstruction and intraoperative angle measurement using smartphone to obtain a mean puncture completion time of 8.06 min. The control group underwent conventional surgery with a mean puncture duration of 15.98 min. It was found that the puncture time in the treatment group was significantly shorter than that in the control group (Table 1).
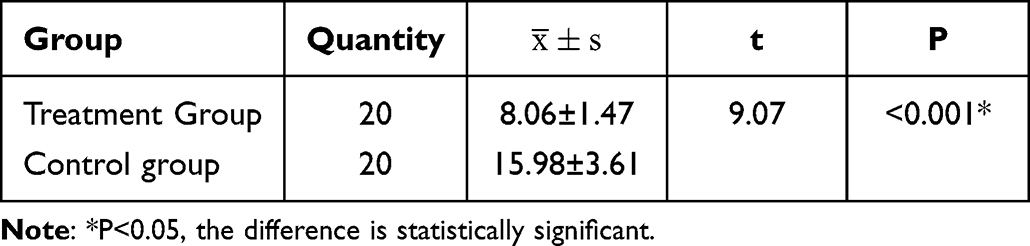 |
Table 1 Independent t-test for Puncture Success Time Between the Control Group and the Treatment Group (Minutes) |
Comparison of VAS Pain Score Trends Before and After Treatment Between the Two Groups
Repeated-measures ANOVA was applied to compare the VAS pain scores between the two groups at three time points: before treatment, 2 weeks after treatment, and 2 months after treatment. The results showed that the main effects of treatment time F = 1327.6, P < 0.001, group F = 9.124, P = 0.004, and the interaction effect between time and group F = 131.8,P < 0.001 were all statistically significant. This indicated that VAS pain scores of both groups decreased significantly with postoperative recovery, and the treatment group had a significantly faster pain relief rate and greater reduction amplitude at each postoperative time point compared with the control group (Table 2).
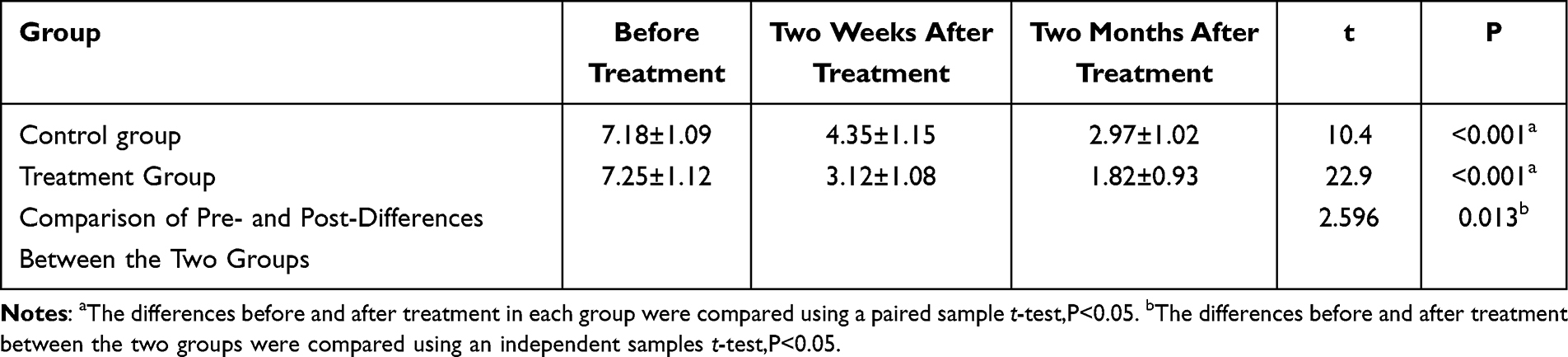 |
Table 2 Comparison of VAS Pain Score Trends Before and After Treatment Between the Two Groups (n = 20, |

Intra-group paired t-test showed that the differences in VAS scores before and 2 months after treatment were statistically significant in both the treatment group t = 22.9,P < 0.001 and the control group t = 10.4,P < 0.001. The inter-group comparison of pre- and post-treatment VAS score differences by independent samples t-test showed a statistically significant difference between the two groups t = 2.596,P = 0.013, which confirmed that 3D CT-guided intelligent-assisted radiofrequency ablation had a better and more durable analgesic effect for patients with suprascapular nerve entrapment (Table 2).
Comparison of ROWE Scores Before and After Treatment Between the Two Groups
Repeated-measures ANOVA was applied to compare the ROWE scores between the two groups at three time points: before treatment, 2 weeks after treatment, and 2 months after treatment. The results showed that the main effects of treatment time, group, and the interaction effect between time and group were all statistically significantly different (P < 0.01). This indicated that there were statistically significant differences in ROWE scores between the treatment group and the control group at the time points of before treatment, 2 weeks after treatment, and 2 months after treatment (Table 3).
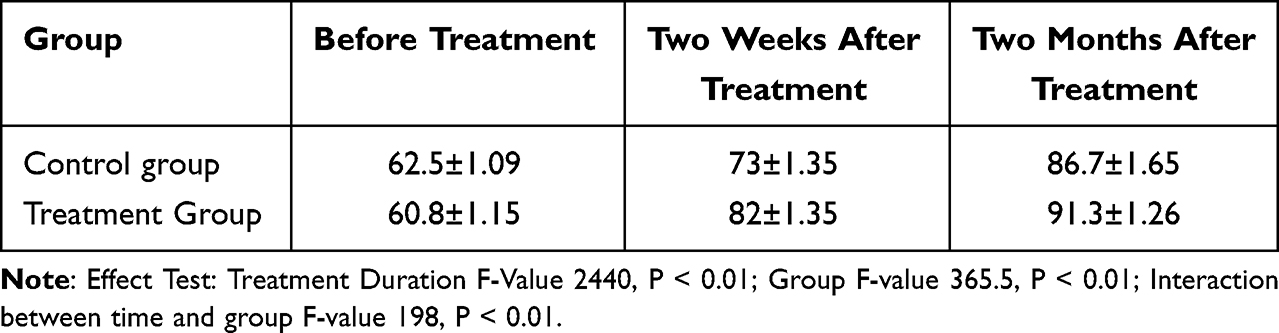 |
Table 3 ROWE Scores in the Two Groups Before and After Treatment (n = 20, |

Analysis of Therapeutic Effect and Complications Between the Two Groups
The therapeutic effect was evaluated two weeks after treatment. Fourteen cured cases, 2 effective cases, and 2 improved cases were in the treatment group, with an overall effective rate of 90%. The control group showed 10 cured cases, 2 effective cases, and 2 improved cases, with an overall effective rate of 70% (P > 0.05), which had no statistically significant difference in therapeutic effect between the two groups. The control group of 20 patients all received conventional radiofrequency ablation treatment, which had a longer operation time and higher number of puncture attempts. Within this group, 8 cases of complications were reported: 2 cases of hematoma at the puncture site, treated by compression hemostasis; 4 cases of postoperative hypertension, which normalized after administration of antihypertensive treatment and mood stabilization; and 2 cases of increased body temperature within 3 days after surgery, treated with ibuprofen and antibiotics. In the treatment group that included 20 patients, there was only one case of postoperative hypertension, which resolved to normal levels following the administration of oral antihypertensive medication and symptomatic management. The incidence of complications between the two groups was analyzed using the chi-square test, revealing a statistically significant difference (P < 0.05), (Table 4).
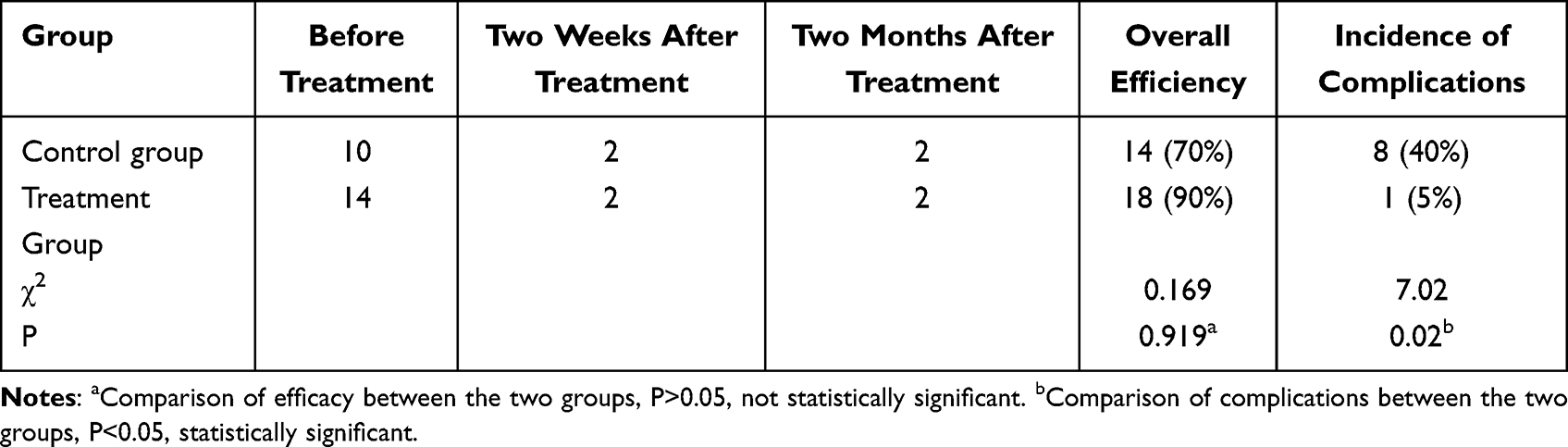 |
Table 4 Therapeutic Effect and Complications (n = 20) |
Statistical Analysis of the Number of Abnormal EMG Cases
There were 10 abnormal postoperative EMG cases in the treatment group and 12 in the control group. Statistical comparison was performed with the rank sum test, which revealed no significant difference between the number of abnormal EMG cases in both groups before and after treatment (P > 0.05) (Table 5).
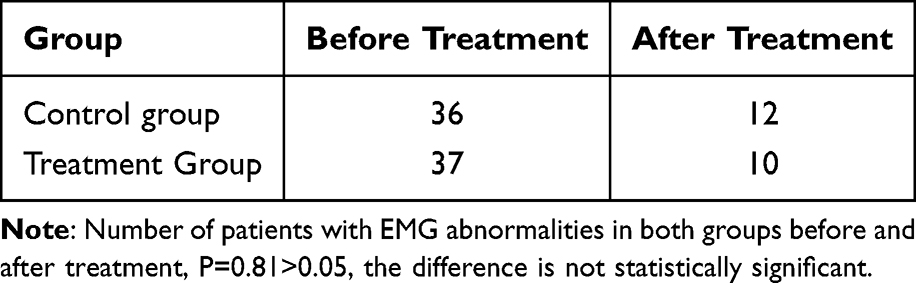 |
Table 5 Statistical Analysis of Abnormal Case Data in EMG Examinations (n = 60) |
Discussion
The suprascapular nerve innervates the shoulder joint for both a motor and sensory nerve. The nerve originates from the C5 and C6 nerve roots traverses the supraspinatus fossa via the suprascapular notch beneath the transverse scapular ligament and gives off branches to innervate the supraspinatus muscle within the supraspinatus fossa. It then passes through the spinoglenoid notch, a fibro-osseous canal bordered by the scapular spine and the spinoglenoid ligament, to enter the infraspinatus fossa, terminating in the subscapular fossa, where it innervates the infraspinatus muscle and the shoulder joint capsule.19 Suprascapular nerve lesions have become increasingly recognized as one of the causes of shoulder pain. Its unique anatomical structure of the nerve makes it susceptible to dynamic and static compression and direct trauma.20 The suprascapular nerve is most commonly entrapped at the suprascapular notch and the spinoglenoid notch. Patients with entrapment typically exhibit extensive dull pain around the shoulder joint, mainly in the posterolateral part of the shoulder joint. This discomfort may occasionally radiate to the neck and arms. Some patients may experience nighttime pain.21
Conventional surgery of the control group also applies 3D CT imaging guidance but without distance and angle measurements or intraoperative intelligent software assistance. The surgeon has to perform several corrections and carry out repeated scans during surgery, depending on personal experience, which increases the operation time and risks intraoperative radiation exposure and bleeding.22 Our new surgical procedure overcame the issues accompanying blind puncture. By integrating 3D CT image reconstruction, it made intraoperative error distance and needle insertion angle measurement accurate, thereby offering substantial support to surgeons. The core difference between the two groups is whether the smartphone-assisted angle measurement is used, which is a more rigorous clinical comparison design for the preliminary research of the intelligent-assisted technology. This design can exclude the interference of CT imaging on the research results and more accurately evaluate the clinical value of the smartphone-assisted angle measurement technology. Wuhan Zhenji Technology Co., Ltd., developed the “Multifunctional Mobile Measurement App”. It is a free mobile angle measurer, and it relies on the phone’s recognition system to provide quite accurate measurements of variations in angles under various circumstances. The advancement of smartphones has led to a significant enhancement in the capabilities of mobile applications. More specifically, smartphone intrinsic balance assessment can accurately assess coronal, sagittal, and horizontal plane balancing capacity with relatively high accuracy.23
Suprascapular nerve radiofrequency ablation, as a mature technology, has been extensively used to treat suprascapular nerve entrapment.24 Its main principle is to insert a radiofrequency puncture needle into the suprascapular notch and perform low-temperature pulsed radiofrequency treatment. This allows for the stimulation of the suprascapular nerve by constant, low-temperature pulses, which helps in the restoration of the nerve function, the enhancement of the internal and external environment of the nerve, the elimination of adhesions, and the relief of pain. CT-assisted radiofrequency ablation makes it possible to visualize the very layer that is penetrated by the puncture needle and also allows one to recognize important structures like blood vessels and nerves. This makes it possible to steer clear of these structures while inserting the needle, thus giving it the aspect of high safety and strong recognizability.9 Besides this, the procedure is performed by trained radiology technicians, thus guaranteeing expertise and accurate tissue recognition. But CT scans do come with radiation, inherently. Multiple and extended scans might have some impacts on the area scanned in the patient.25 Thus, it is required that we address the very crucial issue of finding measures to enhance the effectiveness of surgery, the minimization of CT scans, and reduction of CT scanning time. In this study, we integrated the positional images obtained through 3D CT scans with the angle measurement aided by a smartphone. Meanwhile, we utilized the integrated gravity balance calibration function of the smartphone to offer accurate support for intraoperative procedures from a 3D stereoscopic aspect. Compared to other minimally invasive interventions such as ultrasound-guided nerve block and shockwave therapy, radiofrequency ablation offers sustained analgesic efficacy while preserving minimal invasiveness, attributable to its targeted application of radiofrequency energy on neural tissue. Under image guidance, this modality demonstrates notably superior and durable symptomatic improvement in refractory suprascapular nerve compression—particularly in cases with evident structural compromise or prior failure of conservative management—thereby representing a critical therapeutic alternative for clinically challenging patients.
All surgeons who performed the operation in this study had more than 5 years of clinical experience in radiofrequency ablation for peripheral nerve entrapment, and the operator experience was homogeneous. Before the formal study, all surgeons received 2 weeks of standardized training on the intelligent-assisted system, and the learning curve test showed that the operation time of the surgeon was stable after 3 cases of operation, indicating that the intelligent-assisted technology had a short learning curve and was easy to master.
Through comparison between the treatment group and the control group, this study was able to quantify the benefit of the new approach in clinical efficacy, safety, and efficiency in surgery. Firstly, there were notable improvements in surgical efficiency and accuracy in the treatment group. According to Table 1, completion of puncture in the treatment group (8.06 min) was significantly shorter than in the control group (15.98 min). This confirmed that the method greatly improved accuracy and efficiency of puncture procedures and saved operation time. Second, main clinical therapeutic effect indexes had a very noticeable improvement in the treatment group. From the view of pain reduction, Table 2 shows that the VAS values before and after treatment in the treatment group were statistically higher than those in the control group, suggesting that our new approach reduced patients’ pain more efficiently. According to repeated-measures ANOVA in Table 3, the treatment group exhibited more improvement in the ROWE score at different time points than the control group did in the recovery of the shoulder joint function. This finding reflects that our innovative method permitted more rapid and total restoration of shoulder joint function. Finally, the treatment group performed more favorably regarding treatment safety and occurrence of complications. Although Table 4 shows no statistically significant difference in the total effective rate between the two groups at 2 weeks after treatment, the control group’s complication rate (8 cases) was statistically significantly higher than that of the treatment group (1 case). This indicates that the intelligent-assisted radiofrequency ablation improves the puncture precision and reduces the number of puncture attempts and intraoperative trauma, which not only improves the procedural efficiency and therapeutic effect of the operation but also significantly reduces the incidence of complications (such as puncture site hematoma, postoperative hypertension). There is a positive correlation between the improvement of operation efficiency and the reduction of complication rate, which is the core advantage of the new method compared with the traditional method.
There was no significant difference in the number of abnormal EMG cases between the two groups after treatment in Table 5(P > 0.05), which may be because the EMG mainly reflects the morphological and functional changes of the peripheral nerve, and the radiofrequency ablation in this study is a minimally invasive intervention for the nerve entrapment site, which can relieve the clinical symptoms of patients by reducing nerve compression and inflammatory response, but the repair of nerve morphological damage needs a longer time. The short follow-up time (2 months) of the study may not be enough to observe the significant improvement of EMG indicators. Although it is impossible to assert that there existed statistically significant differences in clinical effectiveness and EMG between the two compared forms of surgery, the reduction of operation time and the enhancement of surgical precision had indeed reduced intraoperative trauma for patients, which had a secondary impact on surgical outcomes. Although the two methods were equal in some markers of effectiveness, our new method still had many advantages. The significant difference in effectiveness was primarily due to precise intraoperative navigation, which rendered nerve ablation more intuitive and effective. Precise manipulation reduced puncture number (mean 2 vs 4 in control), surgical time, and intraoperative trauma. Fewer punctures and reduced puncture time reduced patients’ intraoperative anxiety and decreased the rate of complications.26 All the above variables created a promising circle in the treatment group, which also influenced the patients’ postoperative rehabilitation process. All the findings indicated that the strategy adopted in the treatment group showed high efficiency, had a promising therapeutic effect, and ensured security.
The management of suprascapular nerve entrapment is increasingly evolving toward precision-based, minimally invasive strategies. Recent progress is marked by the application of high-resolution magnetic resonance neurography, which significantly improves diagnostic precision. Ultrasound- or CT-guided nerve blocks and pulsed radiofrequency ablation have become widely adopted minimally invasive procedures, with the latter demonstrating considerable efficacy in refractory cases. The incorporation of smart navigation and 3D anatomic mapping now allows for millimeter-level accuracy in intervention. Furthermore, etiology-driven and patient-tailored treatment algorithms have been established to enhance clinical outcomes and procedural safety. This study is a single-center preliminary clinical study. Based on the previous relevant clinical research on radiofrequency ablation for suprascapular nerve entrapment, the sample size of 20 cases in each group was initially set, with a follow-up time of two months. Due to the preliminary nature of the study, power analysis was not performed in the early stage. The small sample size may lead to limited statistical power. Due to limitations of objective conditions, this study still requires intraoperative scanning for enhanced precision in positioning and operation. There is a possibility of inaccurate needle insertion points, and preoperative identification of the surface projection of the suprascapular nerve is hindered by anatomical variations among patients.
This study is the first to apply the smartphone gravity calibration-assisted angle measurement technology to the radiofrequency ablation of suprascapular nerve entrapment, and the results show that this technology can significantly improve the procedural efficiency and safety of the operation. The innovative point is to combine the conventional 3D CT imaging with the low-cost and easy-to-promote smartphone intelligent assistance, which makes up for the deficiency of the traditional radiofrequency ablation with low puncture precision and high radiation dose. In the future research, we will carry out multi-center, large-sample, randomized controlled trials with longer follow-up time (6 months to 1 year); integrate the intelligent-assisted system with robotic navigation systems to further improve the puncture precision; and conduct in-depth research on the long-term therapeutic effect and cost-effectiveness of the technology to enhance patient outcomes.
Conclusion
This study investigated 3D CT-guided intelligent-assisted radiofrequency ablation for suprascapular nerve entrapment. The results show that this technique significantly shortens puncture success time (8.06 ± 1.47 min vs 15.98 ± 3.61 min, P < 0.05), improves postoperative VAS pain and ROWE shoulder function scores (all P < 0.05), and reduces perioperative complication rate (5% vs 40%, P < 0.05), with no significant between-group differences in 2-month overall effective rate and EMG improvement (both P > 0.05). This method has good clinical applicability, as it is based on conventional 3D CT imaging and common smart phones, with low equipment cost and no need for complex professional training; it has good scalability, and can be popularized and applied in primary hospitals with basic CT imaging conditions and minimally invasive surgery capabilities.
In summary, 3D CT-guided intelligent-assisted radiofrequency ablation is a safe, effective and easy-to-promote minimally invasive strategy for suprascapular nerve entrapment, which can optimize procedural efficiency, relieve patients’ pain, improve shoulder joint function, and reduce perioperative risks.
Data Sharing Statement
The data that support the findings of this study are available on request from the first author. The data are not publicly available due to privacy or ethical restrictions.
Ethical Approval
The Medical Ethics approval Committee of Zibo First Hospital, Shandong, China, approved the study on June 7, 2023 (ID:YXLL2023060205).
Patient Consent
All patients provided informed consent to participate in this research, in accordance with the Declaration of Helsinki.
Acknowledgments
Data were provided by Fukang Han, ZiBo First Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Reform Research Project of Undergraduate Education in Shandong Province (M2022050), Shandong Provincial Traditional Chinese Medicine Science and Technology Project(Q-2023163).
Disclosure
The authors declare that they have no conflicts of interests in this work.
References
1. Shanahan EM, Gill TK, Briggs E, Hill CL, Bain G, Morris T. Suprascapular nerve block for the treatment of adhesive capsulitis: a randomised double-blind placebo-controlled trial. RMD Open. 2022;8(2):e002648. doi:10.1136/rmdopen-2022-002648
2. Muir B. Dorsal scapular nerve neuropathy: a narrative review of the literature. J Can Chiropr Assoc. 2017;61(2):128–13.
3. Reece CL, Varacallo MA, Dulebohn SC, Susmarski AJ. Suprascapular nerve injury. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
4. Memon AB, Dymm B, Ahmad BK, Sripathi N, Schultz L, Chandok A. Suprascapular neuropathy: a review of 87 cases. Muscle Nerve. 2019;60(3):250–253. doi:10.1002/mus.26630
5. Clavert P, Thomazeau H. Peri-articular suprascapular neuropathy. Orthop Traumatol Surg Res. 2014;100(8):S409–S411. doi:10.1016/j.otsr.2014.10.002
6. Young SW, Dakic J, Stroia K, Nguyen ML, Harris AHS, Safran MR. High incidence of infraspinatus muscle atrophy in elite professional female tennis players. Am J Sports Med. 2015;43(8):1989–1993. doi:10.1177/0363546515588177
7. Witvrouw E, Cools A, Lysens R, et al. Suprascapular neuropathy in volleyball players. Br J Sports Med. 2000;34(3):174–180. doi:10.1136/bjsm.34.3.174
8. Hu Q, Zhang ZY, Fan S. Summarization of Professor Zhang Zhenyu’s experience in the treatment of suprascapular nerve entrapment syndrome based on the theory of “keeping tendons in tendons” and dynamic and static combination by manipulations of precise tendon relaxation(Chinese). China Medical Herald. 2023;20(7):152–156.
9. Chen L, Wang J, Wu GP, Shi CG, Ni XJ. Ultrasound-guided suprascapular nerve pulsed radiofrequency combined with physical therapy for the treatment of shoulder joint pain after a stroke: analysis of its curative effect(Chinese). J Interv Radiol. 2022;31(05):495–498.
10. Cao SC, Wang JC, Yan LQ. Efficacy of direct arthroscopy-guided suprascapular nerve block under shoulder arthroscopy in postoperative analgesia of rotator cuff repair(Chinese). China J Endosc. 2019;25(11):55–60.
11. Huntoon MA, Burgher AH. Ultrasound-guided permanent implantation of peripheral nerve stimulation (PNS) system for neuropathic pain of the extremities: original cases and outcomes. Pain Med. 2009;10(8):1369–1377. doi:10.1111/j.1526-4637.2009.00745.x
12. Lan F, Ma YH, Xue JX, Wang TL, Ma DQ. Transcutaneous electrical nerve stimulation on acupoints reduces fentanyl requirement for postoperative pain relief after total hip arthroplasty in elderly patients. Minerva Anestesiol. 2012;78(8):887–895.
13. Albayrak I, Apiliogullari S, Dal C, Levendoglu F, Ozerbil O. Efficacy of pulsed radiofrequency therapy to dorsal root ganglion adding to TENS and exercise for persistent pain after total knee arthroplasty. J Knee Surg. 2016;30(02):134–142. doi:10.1055/s-0036-1583268
14. Xie DB, Gu XK, Chen YH, Zhang YK, Zhang PY, Mo YF. Analysis on morphological classification characteristics of spinoglenoid notch based on three-dimensional CT reconstruction images(Chinese). J Tradit Chin Orthop Traumatol. 2021;33(12):
15. Pan W, Peng J, Elmofty D. Occipital Neuralgia. Curr Pain Headache Rep. 2021;25(9):61. doi:10.1007/s11916-021-00972-1
16. Wang LH, Jiang Y, Sun CH, Chen PT, Ding YN. Advancements in the application of ablative therapy and its combination with immunotherapy in anti-cancer therapy. Biochim Biophys Acta Rev Cancer. 2025;1880(2):189285. doi:10.1016/j.bbcan.2025.189285
17. Youssef HA, Abdel-Ghaffar HS, Mostafa MF, Abbas YH, Mahmoud AO, Herdan RA. Sphenopalatine ganglion versus greater occipital nerve blocks in treating post-dural puncture headache after spinal anesthesia for cesarean section: a randomized clinical trial. Pain Physician. 2021;24(4):E443–E451.
18. Shi DL, Fu YF. Analysis of the therapeutic effect of suprascapular nerve pulsed radiofrequency combined with hydraulic dilation therapy on periarthritis of shoulder(Chinese). Chin J Pain Med. 2013;19(07):447–448.
19. Bozzi F, Alabau-Rodriguez S, Barrera-Ochoa S, et al. Suprascapular neuropathy around the shoulder: a current concept review. J Clin Med. 2020;9(8):2331. doi:10.3390/jcm9082331
20. Moen TC, Babatunde OM, Hsu SH, et al. Suprascapular neuropathy: what does the literature show? J Shoulder Elbow Surg. 2012;21(6):835–846. doi:10.1016/j.jse.2011.11.033
21. Boykin RE, Friedman DJ, Higgins LD, Warner JJ. Suprascapular neuropathy. J Bone Joint Surg Am. 2010;92(13):2348–2364. doi:10.2106/JBJS.I.01743
22. Sultan HE, Younis El-Tantawi GA. Role of dorsal scapular nerve entrapment in unilateral interscapular pain. Arch Phys Med Rehabil. 2013;94(6):1118–1125. doi:10.1016/j.apmr.2012.11.040
23. Yao K, Kasai S, Shiomi A, et al. Development of a predictive score for prolonged pelvic operation time in robot-assisted low anterior resection: a single-center, retrospective study in Japan. Surg Endosc. 2025;39(11):7525–7535. doi:10.1007/s00464-025-12122-4
24. Rosenberg A, Untersteiner H, Guazzarini AG, et al. A digitally supported multimodal lifestyle program to promote brain health among older adults (the LETHE randomized controlled feasibility trial): study design, progress, and first results. Alzheimers Res Ther. 2024;16(1):252. doi:10.1186/s13195-024-01615-4
25. Pereira P, Severo M, Monteiro P, et al. Results of lumbar endoscopic adhesiolysis using a radiofrequency catheter in patients with postoperative fibrosis and persistent or recurrent symptoms after discectomy. Pain Pract. 2016;16(1):67–79. doi:10.1111/papr.12266
26. Vij N, Kiernan H, Miller-Gutierrez S, et al. Etiology diagnosis and management of radial nerve entrapment. Anesth Pain Med. 2021;11(1):e112823. doi:10.5812/aapm.112823
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.