")
Back to Journals » International Journal of General Medicine » Volume 14
Etiological Factors of the Midline Diastema in Children: A Systematic Review
Authors Nuvvula S, Ega S, Mallineni SK , Almulhim B, Alassaf A, Alghamdi SA, Chen Y, Aldhuwayhi S
Received 6 February 2021
Accepted for publication 12 April 2021
Published 8 June 2021 Volume 2021:14 Pages 2397—2405
DOI https://doi.org/10.2147/IJGM.S297462
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sivakumar Nuvvula,1 Sravani Ega,1 Sreekanth Kumar Mallineni,1,2 Basim Almulhim,2 Abdullah Alassaf,2 Sara Ayid Alghamdi,2 Yong Chen,3 Sami Aldhuwayhi4
1Department of Pedodontics and Preventive Dentistry, Narayana Dental College, Nellore, Andhra Pradesh, India; 2Department of Preventive Dental Science, College of Dentistry, Majmaah University, Al-Majmaah, Saudi Arabia; 3Department of Stomatology, School of Medicine, Xiamen University, Xiamen, People’s Republic of China; 4Department of Prosthodontics, College of Dentistry, Majmaah University, Al-Majmaah, Saudi Arabia
Correspondence: Sreekanth Kumar Mallineni
Department of Preventive Dental Science, College of Dentistry, Majmaah University, Majmaah, 11952, Saudi Arabia
Tel +966-507780161
Email [email protected]
Background: Midline diastema in children is a prevalent developmental entity, and this pathological condition may remain in many children due to various factors. Nonetheless, the evidence on etiological factors of the midline diastema in children is minimal.
Purpose: To evaluate the etiological factors of midline diastema causes in children below 12 years of age from the published data.
Methods: A literature search was confined to the English language using MeSH terms conferring to PICO format in PubMed, Cochrane Library, and Ovidsp covering the period from January 1960 to December 2019. Search in Google Scholar, grey literature, and hand search on references were performed to find additional data. Suitable studies were selected based on the predefined inclusion and exclusion criteria. Quality analysis of the chosen studies conducted using the Newcastle-Ottawa Scale (NOS) adapted for cross-sectional studies.
Results: Only eight studies were available for final analysis among those four studies from India, two studies from Korea, one study from Brazil, and another study from Canada. The most common etiology for midline diastema was supernumerary teeth followed by morphology labial frenum and nasal airflow condensation. The quality analysis of these studies based on NOS showed one study with unsatisfactory, four studies with satisfactory, and three with good quality.
Conclusion: Morphology of frenum, pre-maxillary supernumerary teeth, and nasal airflow condensation seem to be the most common causes of midline diastema in children below 12 years.
Keywords: aetiological, midline diastema, children
Introduction
Diastema means “interval” in Greek, and it is a space or gap between two or more adjacent teeth. This entity frequently occurs in the midline of the maxillary arch between the two central incisors, and hence it is called median or midline or central diastema.1,2 The diastema is observed in many children as part of healthy development in the mixed dentition, and it disappears naturally in most cases as dental development proceeds.3 Maxillary midline diastema is an aesthetic concern for the pediatric population and their parents. It may, however, persist either because of its width or other associated factors.4 Subsequently, there was a more extensive range of findings from 1.6% to 25.4% in adults and an even greater variety in the young population groups.5–8 Differences in epidemiological study findings are attributable to many factors contributing to midline diastema, to the definitions used to explain its presence and gender and race differences in the hereditary feature’s distribution in question.8
A dental midline diastema is characterized by a space between two central incisors commonly seen in the maxillary arch while rarely in the mandibular arch9 Andrews opined that diastemas are not witnessed in dentition with tight contacts.10 In a growing child, a midline diastema is also observed in the “ugly duckling” stage, which is part of the development of the dentition. This stage is the transitional phase indicating the space available for the erupting permanent dentition.11 Sanin et al. 12 amplified a method to predict the spontaneous closure of the available space in the permanent dentition stage. This method was claimed to be 88% accurate in the early mixed dentition phase. The size of the diastema and the possibility of space closure without treatment are inversely proportional. Nonetheless, the measurements could be made after the lateral incisors’ eruption, and if the space of the midline diastema is more than 1.85 mm, early intervention has been suggested.12 Numerous etiological factors have contributed to the development of midline diastema in children.5,7,8,13 The predominant view seems to consider its development as a multi-factorial phenomenon.1–4,12 Nevertheless, corrective and preventive intervention is obligatory in children with the persistence of the midline diastema, even subsequent eruption of the canines in permanent dentition.13 An understanding of the etiology is essential if the diastema is to be closed satisfactorily by orthodontics.1–4 The current search aims to illuminate all aspects and identify evidence-based information provided by contemporary scientific literature to answer the question of the aetiological factors associated with midline diastema in children below 12 years.
Materials and Methods
Research Protocol
The protocol was registered in the Prospective International Registration of Systematic Reviews (PROSPERO) database under the reference number CRD42019128021. The recommendations from the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) (Appendix A) statement to report this systematic review also followed.14
Search Strategy
A detailed database search had conducted using MeSH terms conferring to PICO format in “PubMed” via “Medline,” “Cochrane Central Database,” and “OvidSP” (Appendices B–D), covering the period from January 1960 to December 2019 and search was limited to the English language. The MeSH terms used were “children,” “dentition,” “midline diastema,” and “etiology” in various combinations, and the details of the search strategy were summarised in Table 1. An additional search was performed in Google scholar, grey literature, and hand search on cross-references of the included and relevant studies to find out additional data. Two researchers (SE and NSK) verified the studies that met the inclusion criteria for the review and evaluated the titles and abstracts of the retrieved articles independently. The Boolean operators (“AND” and “OR”) were applied to combine keywords. Articles published only in the English language from January 1960 to March 2019, human studies, observational studies, children =<12 years, and children without any systemic illness were included in the study. The articles published in a language other than English, studies performed in children >12 years, review articles, animal studies, conference abstracts, letters to the editor, comments, personal opinions, book chapters, and studies with insufficient information about how the data were collected and systematic reviews excluded from the final analysis.
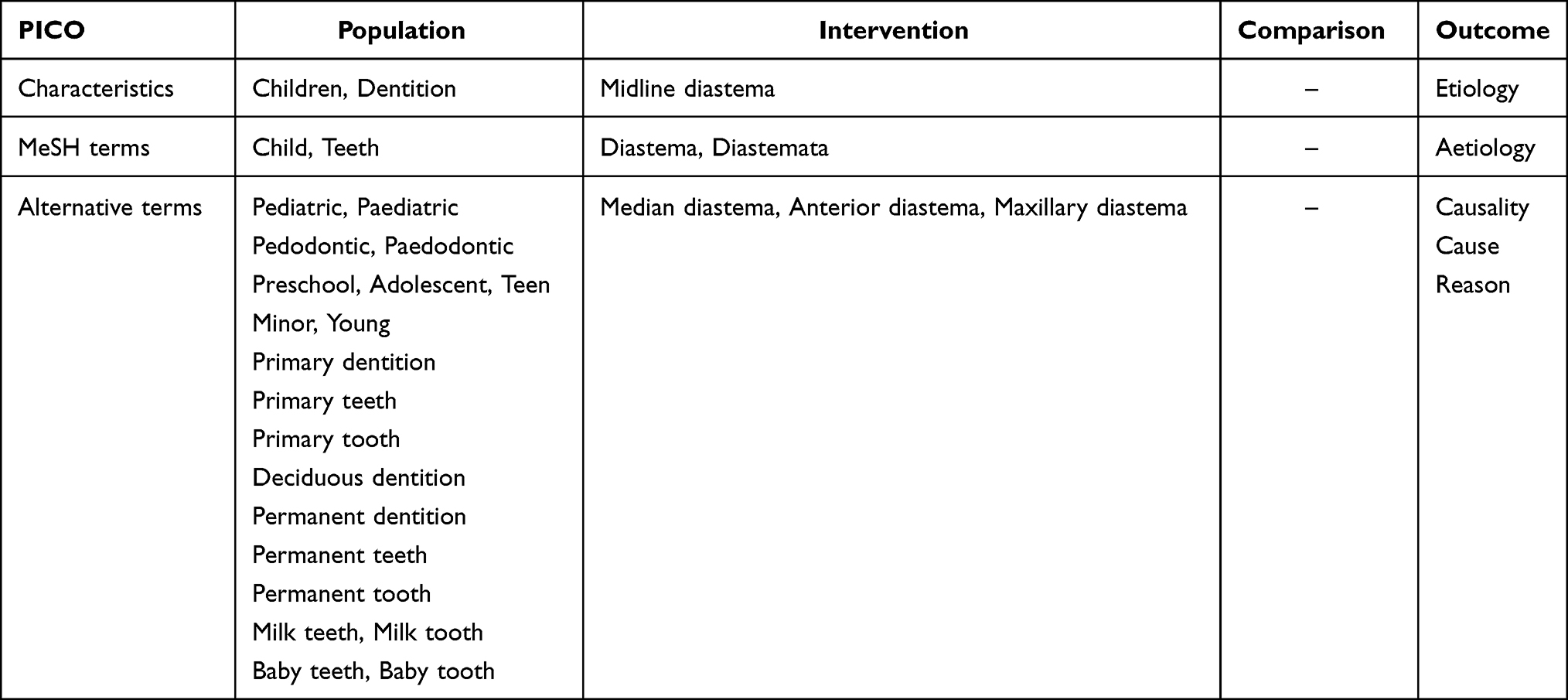 |
Table 1 MeSH Terms and Alternate Terms Used in PICO Format for the Search |
Data Extraction
Studies that met the inclusion criteria were critically appraised by two researchers independently. All the identified records were scanned by title and abstract. The titles and abstracts of the available studies identified from the search engines and hand search were checked at the first phase. The full-text was reviewed when the title and abstract of the retrieved articles have not provided adequate information. Then, data extraction was carried out using the variables suitable for the study. The discussion was made among the authors (MSK, NSK, and SE) until agreement was achieved in case of inconsistency. The articles appearing in more than one database were considered only once. The details of the authors, sample size, type of study, methods used for diagnosis, aetiological factors, and observations were used for evaluation of finally available studies.
Quality Appraisal
The assessment of the quality of the finally available studies performed independently using the “Newcastle-Ottawa Scale” (NOS) adapted for cross-sectional studies. The quality ranked as unsatisfactory (0 to 4 points), satisfactory (5–6 points), and good (7–8 points), or very good (9–10 points).15
Results
This systematic review was performed to collect and analyze studies to determine the aetiological factors of midline diastema in children. The search has retrieved a total of 1280 articles from all three databases [(PubMed, Cochrane library, and Ovidsp-1275) and hand search (5)]. At the first level, 63 duplicates were excluded, and 1217 titles were screened. After screening the titles of retrieved articles, 1158 records were excluded due to various reasons, such as animal studies, adult studies, without abstracts, independent studies, and narrative reviews, systematic reviews, syndromes, and letters to the editor. After screening the abstracts (59), eight were available for full-text assessment (Figure 1). All eight articles were included for the quality assessment (NOS). The substantial inter-examiner agreement corresponding to kappa statistics for the methodological quality assessments was 0.89 for all the categories. The details of the studies are summarised based on the authors, sample size, type of study, methods used for diagnosis, aetiological factors, and observations in Table 2.16–23
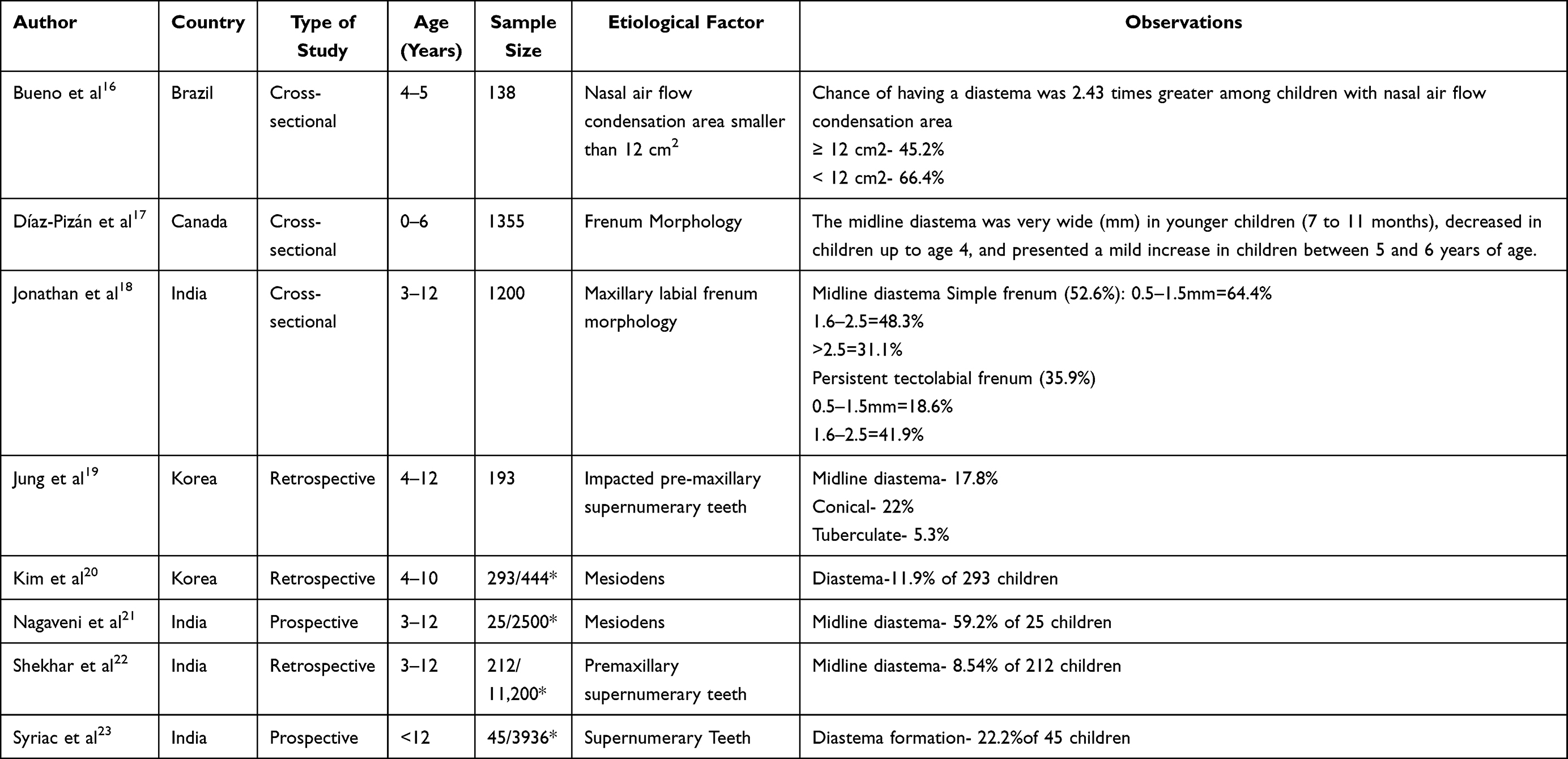 |
Table 2 Details of the Included Studies |
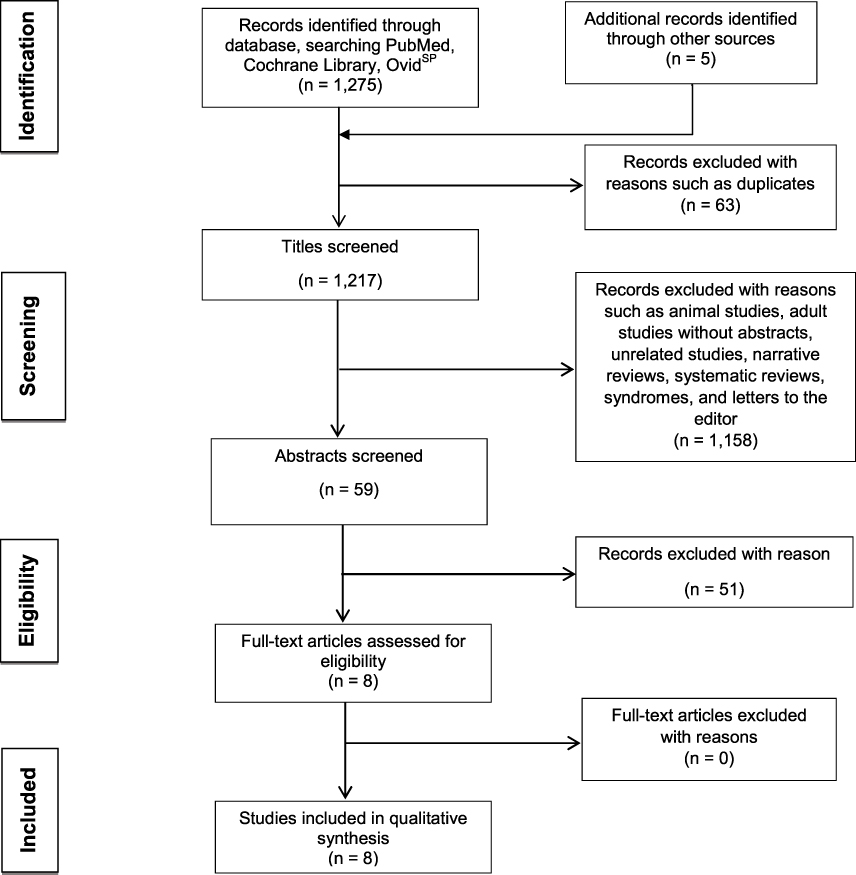 |
Figure 1 PRISMA flow chart of records reviewing process.Notes: Adapted from Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;15(4):264–269.14 Creative Commons Attribution License. |
Among the available eight studies, three were cross-sectional studies,16–18 three were retrospective studies19–21 and the other two were prospective studies21,23 The age ranges from birth to 12 years in all the studies that were finally included for analysis. The commonly reported etiological factors were supernumerary teeth,19–23 maxillary frenum morphology17,18, and nasal airflow condensation area.17 Three studies used clinical and radiographic records19,21–23 for the diagnosis of this pathology, whereas a Korean study20 used CBCT (cone beam computerized tomography) images and panoramic radiographs, and another Korean study19 used both clinical records and CBCT images and panoramic radiographs. Brazilian study16 used the dental aesthetic index (DAI) to diagnose midline diastema, while Canadian study17 used a direct visual method (Table 3).16–23
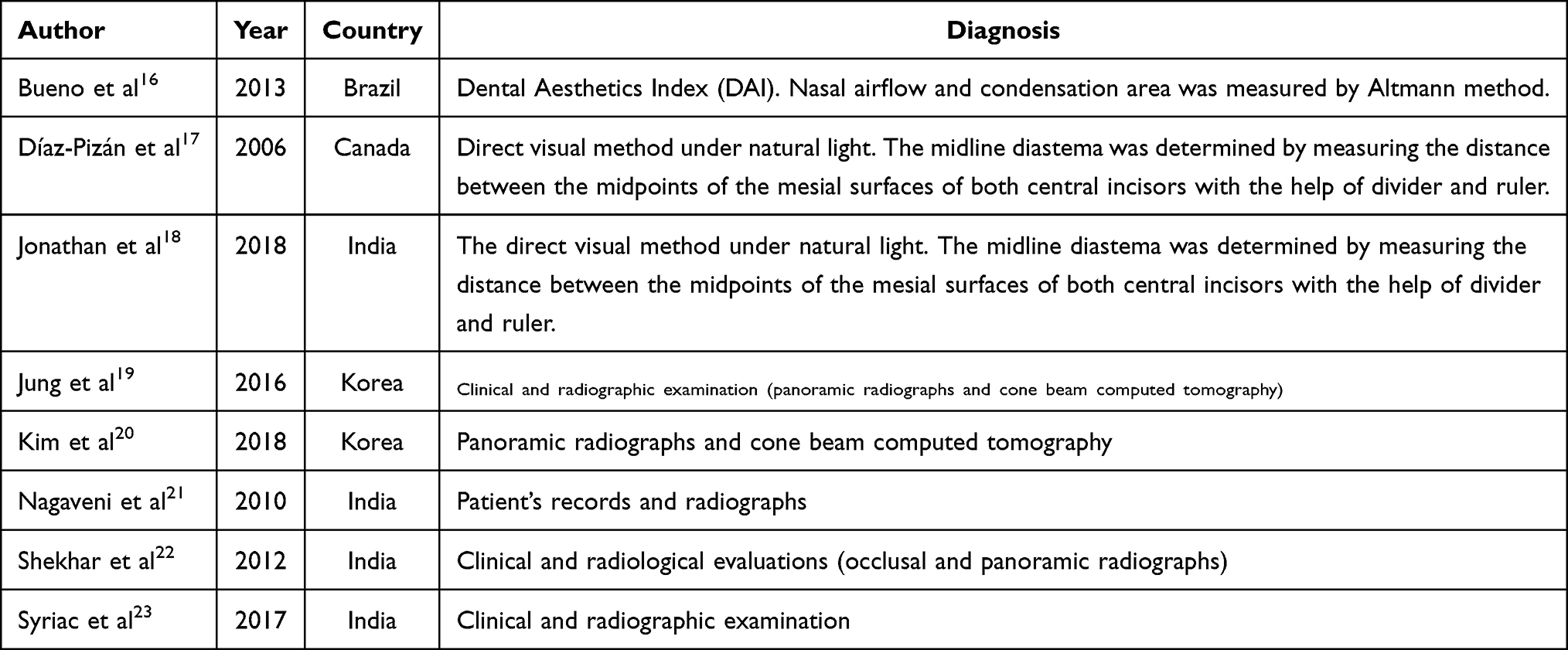 |
Table 3 Details of the Diagnostic Methods Used for the Diagnosis of Midline Diastema |
A version of the Newcastle-Ottawa Scale adapted for cross-sectional studies was used for quality assessment. All studies submitted were appropriate for the aim of the study: eight cross-sectional studies. The categories such as “comparability” and “non-respondents” were not applicable for studies included in this review and were not considered for scoring. The scale assessed in studies under mainly three domains: selection, comparability, and outcome. The highest number of stars that could be awarded for each area was 5, 2, and 3, respectively. The methodological quality of a study was measured by the number of points the study received. If study 9–10 stars scored, the study was considered to be very good, if study 7–8 stars scored, the study was good if study 5–6 stars achieved, the study was considered as satisfactory and 0–4 stars score, the study was considered unsatisfactory. The calculated quality assessment showed that one study got an unsatisfactory rating,21 whereas four studies got satisfactory,16–18,23 and three studies,19,20,22 got a good quality of evidence, as mentioned in Table 4.
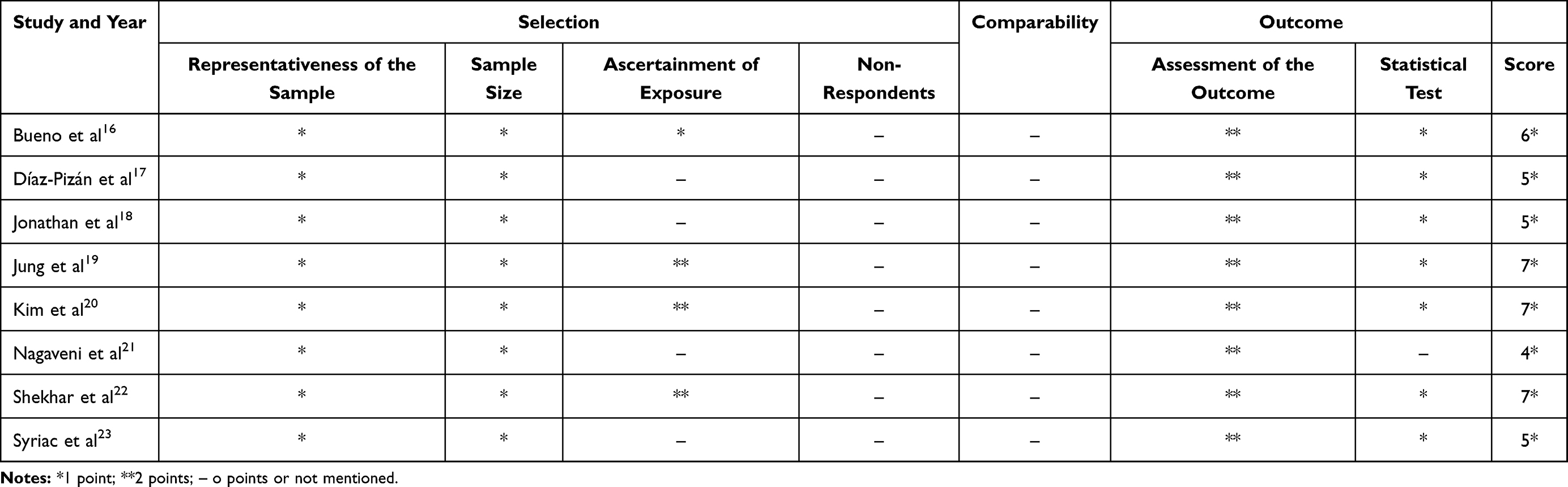 |
Table 4 Newcastle-Ottawa Scale Adapted for Cross-Sectional Studies |
Discussion
Various methods had have been used for the diagnosis of midline diastema by different authors. All the authors have given priority to clinical records; some of them included radiographs to diagnose midline diastema. Two studies17,18 used the direct visual method under natural light for the diagnosis, while the Brazilian study used the dental aesthetics index. Jung et al19 used clinical records and radiographic records, including panoramic and CBCT images; on the other hand, Kim et al20 used only CBCT images and panoramic radiographs for the diagnosis. Clinical records and radiographic records (anterior occlusal radiographs and panoramic radiographs) were used for the diagnosis of midline diastema in the rest of the studies.21–23
A cross-sectional study reported in Canada17 included 1355 subjects ranging from newborns to children (0–6years) with primary dentition. The authors studied the labial frenum morphology and the presence of midline diastema. The authors used direct visual examination under natural light and consisted of lifting the upper lip with both hands’ index finger and thumb. The observation and classification of the labial frenum were made based on Sewerin’s typology, and also, the midline diastema was determined by measuring the distance between the midpoints of the mesial surfaces of both central incisors. The authors observed that the most significant average size of the midline diastema was found in children aged 7 to 11 months and decreased in children from 2 to 4 years old, and mildly increased in children 5 to 6 years old as a consequence of the eruption of the other primary teeth. The study’s limitation was that radiographic examinations and model casts were not taken because of the sample size (economic barrier) and very young children’s management.17
Another cross-sectional study18 by Indian authors assessed the relationships between morphologic types of maxillary labial frenum and midline diastema. A clinical examination performed similarly to a study done by a Canadian study. Out of 1200 children (3 to 12 years), 501 children (41.75%) presented a midline diastema greater than 0.5 mm. The children were divided into three groups, ie, mild (0.5–1.5 mm), moderate (1.6–2.5 mm), and severe (>2.5 mm), to further evaluate midline diastema. On assessing the types of maxillary labial frenum among different age groups, simple frenum showed the highest prevalence in 10 to 12 years of age group, and persistent tectolabial type was more common in 3–5 years group. The relationship was found that among children with midline diastema, 52.6% had simple frenum with mild diastema 64%, moderate 48.4%, and severe 31.1%, and 35.9% had persistent tectolabial frenum with mild diastema 18.6%, moderate 41.9% and severe 66.6%. The authors found that a statistically significant relationship between midline diastema and persistent tectolabial frenum.18
A retrospective study19 reported from Korea involved 193 children of age between 4 to 12 years. The authors performed clinically, and radiographs examination (CBCT images and panoramic radiography) was performed to identify impacted pre-maxillary supernumerary teeth. The authors reported that supernumerary teeth (17.8%) are common complications associated with diastema (conical –22% and tuberculate– 5.3%). In addition, the authors observed midline or transversely positioned supernumerary teeth in the majority of the children with midline diastema. Another Korean retrospective study20 analyzed data for supernumerary teeth using CBCT images and all patients’ panoramic radiographs. A total of 66% of Korean children aged 4–10 years were diagnosed with mesiodens were included among them; only 44% of children observed complications. The authors observed that the midline diastema was 11.9% due to mesiodens on adjacent permanent teeth.20
A prospective Indian study21 looked at the patients’ records, and radiographic examinations were performed to evaluate the mesiodens of 2500 Indian children aged between 3 to 12 years. The mesiodens were diagnosed in 25 children in this study. The authors reported that midline diastema was associated with mesiodens. A retrospective study of 11,200 Indian children aged between 3 to 12 years was observed with clinical and radiographic (anterior occlusal and panoramic radiographs) examinations to investigate the characteristics and distribution of pre-maxillary supernumerary teeth. A total of 212 children exhibited pre-maxillary supernumerary teeth, and 8.54% of supernumerary teeth were associated with midline diastema. In another Indian study,18 authors screened clinical and radiographical records of 3936 children below 12 years of age, and supernumerary teeth were detected in 45 subjects. The authors stated that the midline diastema was 22.2% associated with patients with supernumerary teeth.
A cross-sectional study reported from Brazil16 examined 138 children, children of age 4–5 years. The clinical data were obtained according to the dental aesthetic index (DAI) recommended by the World Health Organization (WHO), and an Altmann graded mirror was used to measure the condensation area produced by nasal airflow. The authors reported that the chance of having a diastema was 2.43 times greater among children with a nasal airflow condensation area smaller than 12 cm2.17
A Canadian study17 conducted a study with 1355 newborn children to 6 years of age with complete primary dentition involved in observing labial frenum characteristics and the presence of midline diastema. Bueno et al16 performed a cross-sectional study using a sample of 138 Brazilian school children of 4 to 5 years of age. Two retrospective studies, Korean studies by Jung et al19 and Kim et al20 included 1200 and 193, respectively, in their studies. A cross-sectional study18 from India involved 1200 children age 3 to 12 years, while two prospective studies21,23 from India performed with 2500 and 3939 children of age below 12 years. Shekar et al22 conducted a retrospective study with 11,200 school children of age 3 to 12 years.
A Brazilian study16 reported that the chance of having a diastema was 2.43 times greater among children with nasal airflow condensation area more than 12 cm2 and the authors found 66.4% of their subjects with nasal condensation airflow is more than 12 cm2 had midline diastema. A Canadian study17 and an Indian study reported that the maxillary labial frenum morphology is the reason for midline diastema in children. Two Korean studies19,20 and three Indian studies21–23 stated that the presence of pre-maxillary supernumerary teeth causes midline diastema in children below 12 years. Kim et al20 reviewed 444 CBCT images and panoramic radiographs and found 293 patients with mesiodens among those subjects; 11.9% of children showed midline diastema, and the overall prevalence of midline diastema was 7.8%. Nagaveni et al21 studied 2500 clinical and radiographic records of school children and found 25 (1%) of mesiodens among the sample; 59.2% exhibited midline diastema. The overall prevalence of midline diastema in this study was 0.5%. Another Indian study22 reported that 212 children were diagnosed with mesiodens of 11,200 children among those children, 8.54% found to have midline diastema, whereas the prevalence of the midline diastema in the sample was 0.1%. A recent Indian prospective study23 found 45 children with supernumerary teeth in 3936 school children of 12 years of age. Among these children, 22.2% of the children showed midline diastema, and the total prevalence of midline diastema was 0.25%.
The etiology of midline diastema is multi-factorial, and an appropriate diagnosis and timely management are very crucial. Management of midline diastema includes observation and follow-up, orthodontic treatment, frenectomy, space closure, restorative treatment, and removal of the supernumerary tooth.24,25 Clinical assessment of effective maxillary expansion may also result in midline diastema,25 and this diastema is not considered true diastema. Hence, it is essential to have a history of the maxillary expansion in the child prior to diagnosis. Removal of the etiologic and the development of the central incisors may help in closing the midline diastema.26,27 Huang and Creath28 opined that midline diastema’s accurate diagnosis involves dental and medical histories, clinical and radiographic examinations, and tooth-size evaluations. The authors also opined that the timing of treatment is too important to achieve acceptable outcomes. The midline diastema is unlikely to close spontaneously following the eruption of lateral incisors and canines if diastema is more than 2 mm.29 Furthermore, the eruption of adjacent teeth to diastema (lateral incisors and canines) has also been critical in the management of space in the maxillary arch.26 A recent study30 from Italy has suggested that the opaque resin’s aesthetical appearance is not possible to show in such cases with space issues. The authors opined the final aesthetic restorations’ realistic preview and recommended the virtual smile planning with 3D mock-ups.
The search was limited to full-text articles in the English language, time, and children. The calculated quality assessment was an unsatisfactory for a south Indian study,21 satisfactory scores were evident for the Brazilian study,16 Canadian study,17 and two Indian studies;18,23 on the other hand, two Korean studies19,20 were scored as good along with an Indian retrospective study.22 However, further studies are necessary. Primarily, these could elucidate more clearly the association of aetiological factors of midline diastema in children.
Conclusions
There is evidence in the literature showing the aetiological factors of midline diastema in children. From the present systematic review, frenum morphology, pre-maxillary supernumerary teeth, and nasal airflow condensation seem to be the most common causes of midline diastema in children.
Acknowledgments
The authors would like to thank the Principal, Narayana Dental College, and Hospital, Nellore, Andhra Pradesh, India.
The author would like to thank the Deanship of Scientific Research at Majmaah University for supporting this work under Project Number No. R-2021-89.
Funding
There is no funding to report.
Disclosure
The authors reported no conflicts of interest for this work.
References
1. Azzaldeen A, Muhamad AH. Diastema closure with direct composite: architectural gingival contouring. J Adv Med Dent Sci Res. 2015;3:134–139.
2. Abu-Hussein M, Watted N, Abdulgani A. An interdisciplinary approach for improved esthetic results in the anterior maxilla diastema. J Dent Med Sci. 2015;14:96–101.
3. Abu-Hussein M, Abdulgani A, Watted N, Zahalka M. Congenitally missing lateral incisor with orthodontics, bone grafting and single-tooth implant: a case report. J Dent Med Sci. 2015;14:124–130.
4. Gandini P, Schiavi A, Manuelli M, Camassa D. Epidemiological survey of caries occurrence in school age children. Mondo Ortod. 1989;14(1):63–72.
5. Abate A, Cavagnetto D, Fama A, Matarese M, Lucarelli D, Assandri F. Short term effects of rapid maxillary expansion on breathing function assessed with spirometry: a Case-Control Study. Saudi Dent J. 2020;In Press. doi:10.1016/j.sdentj.2020.09.001
6. Nainar SM, Gnanasundaram N. Incidence and etiology of midline diastema in a population in south India (Madras). Angle Orthod. 1989;59(4):277–282. doi:10.1043/0003-3219(1989)059<0277:IAEOMD>2.0.CO;2
7. Steigman S, Weissberg Y. Spaced dentition. An Epidemiologic Study. Angle Orthod. 1985;55(2):167–176. doi:10.1043/0003-3219(1985)055<0167:SD>2.0.CO;2
8. Sullivan TC, Turpin DL, Artun J. A postretention study of patients presenting with a maxillary median diastema. Angle Orthod. 1996;66(2):131–138. doi:10.1043/0003-3219(1996)066<0131:APSOPP>2.3.CO;2
9. Shilpa G, Gokhale N, Mallineni SK, Nuvvula S. Prevalence of dental anomalies in deciduous dentition and its association with succedaneous dentition: a cross-sectional study of 4180 South Indian children. J Indian Soc Pedod Prev Dent. 2017;35(1):56–62. doi:10.4103/0970-4388.199228
10. Andrews LF. The six keys to normal occlusion. Am J Orthod. 1972;62(3):296–309. doi:10.1016/S0002-9416(72)90268-0
11. Farronato G, Giannini L, Galbiati G, Pisani L, Mortellaro C, Maspero CJ. Verification of the reliability of the three-dimensional virtual presurgical orthodontic diagnostic protocol. Craniofac Surg. 2014;25(6):2013–2016. doi:10.1097/SCS.0000000000001046
12. Sanin C, Sekiguchi T, Savara BS. A clinical method for the prediction of closure of the central diastema. ASDC J Dent Child. 1969;36(6):415-8.
13. Lombardo G, Vena F, Negri P, et al. Worldwide prevalence of malocclusion in the different stages of dentition: a systematic review and meta-analysis. Eur J Paediatr Dent. 2020;21(2):115–122. doi:10.23804/ejpd.2020.21.02.05
14. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;15(4):264–269. doi:10.7326/0003-4819-151-4-200908180-00135
15. Newcastle- Ottawa: quality assessment scale adapted for cross-sectional studies. Available from: https://wellcomeopenresearch.s3.amazonaws.com/supplementary/13880/ea30a2fb-a15a-44a9-b35e-5f0914db80b3.docx.
16. Bueno SB, Bittar TO, Vazquez FD, Meneghim MC, Pereira AC. Association of breastfeeding, pacifier use, breathing pattern and malocclusions in preschoolers. Dent Press J Orthod. 2013;18(1):30e1–6. doi:10.1590/S2176-94512013000100006
17. Díaz-Pizán ME, Lagravère MO, Villena R. Midline diastema and frenum morphology in the primary dentition. J Dent Child. 2006;73:11–14.
18. Jonathan PT, Thakur H, Galhotra A, Galhotra V, Gupta N. Maxillary labial frenum morphology and midline diastema among 3 to 12-year-old schoolgoing children in Sri Ganganagar city: A cross-sectional study. J Indian Soc Pedod Prev Dent. 2018;36(3):234–239. doi:10.4103/JISPPD.JISPPD_51_18
19. Jung YH, Kim JY, Cho BH. The effects of impacted premaxillary supernumerary teeth on permanent incisors. Imaging Sci Dent. 2016;46(4):251-258. doi:10.5624/isd.2016.46.4.251
20. Kim Y, Jeong T, Kim J, Shin J, Kim S. Effects of mesiodens on adjacent permanent teeth: a retrospective study in Korean children based on cone-beam computed tomography. Int J Paediatr Dent. 2018;28(2):161-169. doi:10.1111/ipd.12317
21. Nagaveni NB, Sreedevi B, Praveen BS, Praveen BR, Vidyullatha BG, Umashankara KV. Survey of mesiodens and its characteristics in 2500 children of Davangere city, India. Eur J Paediatr Dent. 2010;11(4):185–188.
22. Shekhar MG. Characteristics of pre-maxillary supernumerary teeth in primary and mixed dentitions: a retrospective analysis of 212 cases. J Investig Clin Dent. 2012;3(3):221–224. doi:10.1111/j.2041-1626.2012.00118.x
23. Syriac G, Joseph E, Rupesh S, Philip J, Cherian SA, Mathew J. Prevalence, characteristics, and complications of supernumerary teeth in nonsyndromic pediatric population of South India: a Clinical and Radiographic Study. J Pharm Bioallied Sci. 2017;1(5):S231. doi:10.4103/jpbs.JPBS_154_17
24. Mallineni SK, Anthonappa RP, King NM. Reliability of horizontal and vertical tube shift techniques in the localisation of supernumerary teeth. Eur Arch Paediatr Dent. 2016;17(6):455–460. doi:10.1007/s40368-016-0253-9
25. Lo Giudice A, Rustico L, Ronsivalle V, Nicotra C, Lagravère M, Grippaudo C. Evaluation of the changes of orbital cavity volume and shape after tooth-borne and bone-borne rapid maxillary expansion (RME). Head Face Med. 2020;16(1):21. doi:10.1186/s13005-020-00235-1
26. Portelli M, Matarese G, Militi A, Cordasco G, Lucchese A. A proportional correlation index for space analysis in mixed dentition derived from an Italian population sample. Eur J Paediatr Dent. 2012;13(2):113–117.
27. Mallineni SK, Jayaraman J, Wong HM, King NM. Dental development in children with supernumerary teeth in the anterior region of maxilla. Clin Oral Investig. 2019;23(7):2987–2994. doi:10.1007/s00784-018-2709-2
28. Huang WJ, Creath CJ. The midline diastema: a review of its etiology and treatment. Pediatr Dent. 1995;17(3):171–179.
29. Gkantidis N, Kolokitha OE, Topouzelis N. Management of maxillary midline diastema with emphasis on etiology. J Clin Pediatr Dent. 2008;32(4):265–272. doi:10.17796/jcpd.32.4.j087t33221771387
30. Lo Giudice A, Ortensi L, Farronato M, Lucchese A, Lo Castro E, Isola G. The step further smile virtual planning: milled versus prototyped mock-ups for the evaluation of the designed smile characteristics. BMC Oral Health. 2020;20(1):165. doi:10.1186/s12903-020-01145-z
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.