")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Ethnobotanical Survey of Medicinal Plants Used in Breast Cancer Treatment by Traditional Health Practitioners in Central Uganda
Authors Lutoti S , Kaggwa B , Kamba PF, Mukonzo J, Sesaazi CD, Katuura E
Received 23 August 2022
Accepted for publication 22 February 2023
Published 8 March 2023 Volume 2023:16 Pages 635—651
DOI https://doi.org/10.2147/JMDH.S387256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Stephen Lutoti,1,2 Bruhan Kaggwa,1,2 Pakoyo Fadhiru Kamba,1 Jackson Mukonzo,3 Crispin Duncan Sesaazi,2,4 Esther Katuura5
1Department of Pharmacy, Makerere University, Kampala, Uganda; 2Pharmbiotechnology and Traditional Medicine Centre, Mbarara University of Science and Technology, Mbarara, Uganda; 3Department of Pharmacology and Therapeutics, Makerere University, Kampala, Uganda; 4Department of Pharmacy and Pharmaceutical Sciences, Mbarara University of Science and Technology, Mbarara, Uganda; 5Department of Plant Sciences, Biotechnology and Microbiology, Makerere University, Kampala, Uganda
Correspondence: Stephen Lutoti, Department of Pharmacy, College of Health sciences, Makerere University, P.O Box 7062, Kampala, Uganda, Tel +256782764180, Email [email protected]
Purpose: The study aimed to document the existing knowledge and practices related to breast cancer recognition and treatment using medicinal plants by traditional health practitioners in Central Uganda.
Methods: This cross-sectional exploratory survey, conducted between February and August 2020, applied a mixed methods research approach. A semi-structured questionnaire was administered to 119 traditional health practitioners (THPs) in Kampala, Wakiso and Mukono. Content analysis of qualitative data was done. Quantitative ethnobotanical survey indices, namely user reports (Nur), percentage of respondents with knowledge (PRK), informant consensus factor (Fic), fidelity level (FL), preference ranks (PR) and direct matrix ranking (DMR) were determined.
Results: Most THPs recognized breast cancer by breast swelling (n=74, 62.2%) and breast pain (n=29, 24.4%). They cited 30 plants from 30 genera in 23 families (Fic 0.75 on breast cancer). Asteraceae, Apocynaceae, Euphorbiaceae, Fabaceae, Lamiaceae and Rutaceae were the predominant families. The ten most cited plants were Annona muricata L. (Nur=24), Rhoicissus tridentata (L.f.) Wild & R.B.Drumm (Nur =19), Erythrococca bongensis Pax (Nur=11), Ficus sp. (Nur=10), Cannabis sativa L. (Nur=8), Ipomoea wightii (Wall.) Choisy (Nur=7), Erythrina abyssinica DC. (Nur=5), Leucas martinicensis (Jacq.) R.Br. (Nur=4), Abelmoschus esculentus (L.) Moench (Nur=4) and Zanthoxylum chalybeum Engl. (Nur=3). Annona muricata L. was highly preferred by THPs (PR 1), Ficus sp. had highest fidelity level (FL=77%) and Zanthoxylum chalybeum Engl. ranked as the highest multipurpose plant (DMR 1). Herbs (n=14, 47%) were the most commonly used life forms besides trees (n=11, 37%) and shrubs (n=5, 16%). THPs mostly used leaves (46%), prepared decoctions (82%) and applied residues on the breast.
Conclusion: THPs in Central Uganda recognized breast cancer by symptoms. Medicinal plants applied in its folk treatment have been documented and the claims of cure by THPs merit further investigation.
Keywords: breast tumors, ethnomedicine, herbal medicine, indigenous knowledge
Introduction
Breast cancer is the most frequently diagnosed cancer and the leading cause of cancer-related deaths among women; it accounts for 23% of total cancer cases and 14% of annual cancer deaths globally.1 Breast cancer incidence of 22:100,000 with 5-year survival rate at 56% in Uganda has been reported, and the burden is expected to double in 2030 due to changes in risk factors and population growth.2,3
Chemotherapy, radiotherapy and surgery are the main breast cancer treatment modalities. However, only 25% of Ugandan breast cancer patients can access such care due to the limitations of poor nursing care and surgery, inadequate access to radiotherapy, poor availability of basic and modern systemic therapies translating into lower survival rates.3 In Uganda, a mean delay to seek treatment by breast cancer patients of 13 months and majority of patients presenting with clinical stages IV (88.5%) and III (9.4%) have been reported.4 The delay could be due to the fact that many breast cancer patients, particularly in rural Ugandan settings, are unable to access the only public health facility for specialized cancer treatment.5 Furthermore, while 92.7% of the cost of medicines used at the Uganda Cancer Institute is covered by the government of Republic of Uganda,6 the drugs are out of stock most of the time and patients have to buy them. Those who cannot afford these medicines discontinue treatment because of the economic burden. Like other cancer patients (up to 60%), breast cancer patients often resort to herbal concoctions prepared at home or by traditional health practitioners.5
Additionally, the anti-breast cancer drugs in clinical use exert toxicities and require long-term use, posing adherence challenges and the gradual resistance of cancer cells against these drugs.7 This justifies the need to improve current therapeutic responses by additional novel approaches.7,8 Whereas plants are important sources of modern anti-cancer drugs like Paclitaxel, Vincristine, Vinblastine and plant remedies used by breast cancer patients, with even claims of cure, the traditional treatment practices and plants used by the communities in Uganda and many other developing countries to treat breast cancer and the theories that explain their continued use are not well documented.9–12 The responsible active compounds in these plants and their anti-breast cancer activity profiles are not known, and hence patients are at risk of using non-validated remedies.11–13 This has hindered development of potential useful medicinal plants into modern pharmaceutical dosage forms for possible use in the battle against cancers.13 The study aimed to document the existing knowledge and practices related to breast cancer recognition and treatment using medicinal plants by traditional health practitioners in Central Uganda.
Materials and Methods
Research Design
A cross-sectional exploratory survey was conducted between February and August 2020. A mixed methods research approach was adopted to enable the research team to assess knowledge of traditional health practitioners (THPs) on breast cancer (BC) to address the questions of community knowledge and practices in treating breast cancer by traditional health practitioners, what medicinal plants were used to treat breast cancer from the perspective of traditional health practitioners and how the plants were prepared and administered to patients over the past 5 years (January 2015–August 2020).
Study Area
The study was conducted in the districts of Kampala (0.347° N, 32.5825°E), Wakiso (0.3987° N, 32.4793°E) and Mukono (0.3549° N, 32.752°E). These districts are among the top ten most populated districts in Uganda. They are located in the central region, popularly known as Buganda region and neighbourhood of Uganda Cancer Institute.14 They are accessible by road and well known in Uganda for their use of traditional medicine in the treatment of diseases and the local language spoken is Luganda.15
Study Population
There are no recent estimates of THPs in Uganda. The Ugandan government has enacted a law that seeks to regulate the practice of THPs and hopes to have THPs registered (not yet done as time of this study). However, as per the World Bank IK series, there is at least one traditional health practitioner for nearly 290 people in Uganda.16 The population of THPs in the study area was therefore obtained by dividing the sum of the population aged 18 years and above as reported in the national population and housing census on area specific data for the districts by 290.14–16 Accordingly, the study targeted 7457 THPs who were aged 18 years and above. In this study, THPs were defined as individuals who hold indigenous knowledge in traditional methods of treatment; they prepare, prescribe and/or administer herbal medicines to others within the community.
Sample Size Estimation and Selection
Sample size was estimated using Equation 1:

Where n=approximate sample size; N=population size under study; p=proportion of population considered; d=limit to error estimate; α=level of significance considered; Zα/2=value obtained from the table of standard normal distribution.17,18 The study considered a population size of 7457 (N=7457), as earlier explained, confidence coefficient of 95% (Zα/2= 1.96), sampling error of 0.05 (d=0.05) and a proportion of 0.5 (p=0.5) was assigned due to nonexistence of previous information for this value to arrive at total estimated sample size of 366. The study population was divided into 20 strata-termed communities (Table 1), as guided by a method of determining sample size for ethnobotanical studies by Espinosa, Bieski and Martin.18,19
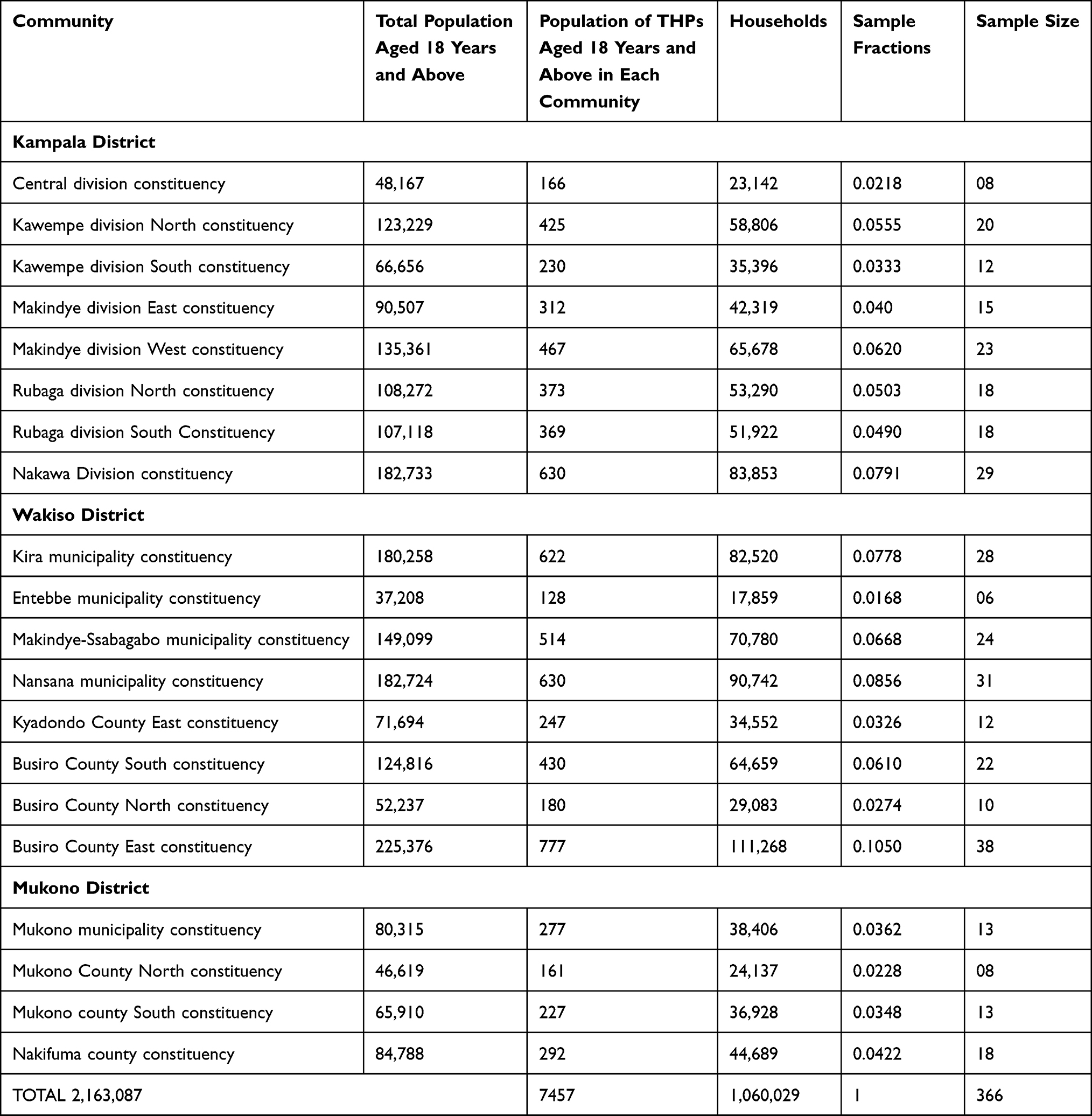 |
Table 1 Distribution of 20 Communities in the Study Districts Including Sample Fractions |
Each constituency was a stratum, “a community” for study, and it represented the number of households sampled per community, considering an informant (THP) per household. To estimate sample size for each community as shown in Table 1, we multiplied the sample fraction by the total sample size (366). For calculation of sample fraction, we divided the number of households in that community by the total number of households for the entire study area, which was 1,060,029 households.14,17–20 An absolute minimum sample of four individuals within each category is indispensable for any statistical analysis.20
Sampling Techniques and Procedure
Each community, as indicated in Table 1, formed a stratum. We randomly sampled one THP per household from each stratum. The contacts for THPs were obtained from leaders of traditional healer associations in Buganda. THPs in each community were mapped, consented and interview schedule planned. A list of THPs in each stratum was generated, randomized by Microsoft Excel and the required number of THPs was obtained by simple random sampling. All THPs who did not treat breast cancer and those who did not use herbs in treatment of patients were excluded.
In order to maximize community co-operation, the study team was introduced to one chairperson of each area’s local council. A researcher administered questionnaire was administered to the respondents by the principal investigator and four trained research assistants who were conversant with the language and cultures of the local people in the study area. This made it easy to extract information from respondents as desired. The leaders of traditional healer associations in Buganda region, respondents and local council authorities assisted the researchers to identify study respondents in the study districts.
The plants mentioned in the study were identified in the field using their local names, based on their taxonomic characters and the voucher specimens collected for confirmation at Makerere University Herbarium. Herbarium specimens were prepared, assigned voucher numbers and deposited at Makerere University herbarium and the Pharmacognosy Laboratory in the Department of Pharmacy Makerere University. Plant names have been checked with scientific plant databases at https://wfoplantlist.org/plant-list and https://plants.jstor.org/.
Data Collection Instruments
Primary data was collected using a semi-structured questionnaire constructed by the principal investigator and two senior researchers. This helped to improve the number and accuracy of responses to the survey.21,22 A Luganda version of the questionnaire was used on participants who had low English literacy, but were fluent in Luganda. The questionnaire used can be accessed at Supplementary Information to this publication.
Data Quality Control
Validity of the questionnaire was established by determining its content validity index (CVI); three experts scored the relevance of the questions in the questionnaire in relation to the study variables. A content validity index of 0.7 or more was acceptable and a Likert scale analysis of each question by the experts was done as very relevant (4), quite relevant (3), somewhat relevant (2), and not relevant (1).
Reliability was established by a pilot testing of the questionnaire to ensure consistency, dependability and its ability to tap data that would answer the objective of the study. The pilot testing of the questionnaire was done in Nakasongola District (1.3490° N, 32.4467° E), one of the districts in Central Uganda. The results were subjected to reliability analysis (data available on request).22
Data Organization and Analysis
Data Organization
Filled questionnaires were cross-checked by each data collector for completeness immediately after filling in the last response so that any missing information was collected before ending the interview. Data was organized using Microsoft Excel 2003 then analysed using SPSS V.18.0. The responses obtained from open-ended questions were grouped into categories according to similarities in the responses. Both theoretical and practical individual ethnobotanical knowledge of informants was analysed. Theoretical or passive knowledge refers to intellectual ability, such as the ability to name plants. Practical ethnobotanical knowledge refers to the practical dimension, for example ability to put knowledge into practice.23
Percentage of Respondents Having Knowledge
The percentage of respondents having knowledge (PRK) regarding the use of a plant species in the treatment of breast cancer was estimated using Equation 2:
where Np is the total number of informants who are claiming to use a plant species to treat breast cancer and Nt is the total number of individuals interviewed.24
Informant Consensus Factor
Informant consensus factor was calculated to analyse individual ethnobotanical knowledge and indicate quality of information using Equation 3:

where Nur is the number of use reports and Ntaxa is the number of species in each use category [17].
Fic values range between 0 and 1, where “1” indicates the highest level of informant consent. Within a community, Fic points to the extensively used plants and helps in the selection of important medicinal plants for further pharmacological and phytochemical studies.25
Fidelity Level (FL)
Fidelity level indicates the importance of a certain plant species for a particular purpose. All reported ailments are grouped into major classes for calculation of FL values. In this study, FL values were estimated using Equation 4:

where Ip is the total number of informants who claimed to use a plant species to treat breast cancer and Iu is the total number of respondents who mentioned the same plant for any ailment. The assumption is that plant species that are used frequently by most respondents for the same disease category are more likely to be biologically active plants.26
Preference Ranking (PR)
Rank values were assigned by 12 key informants to ten medicinal plants used for treating breast cancer in the study. The 12 key informants were randomly selected from among THPs who had treated at least five breast cancer patients and claimed cure of at least two of them in their settings over the past five years.
Direct Matrix Ranking
Direct matrix ranking (DMR) is used to gather data on use diversity of multipurpose medicinal plants. Target selection method was employed to identify 12 informants among interviewed THPs selected to rank the purposes of the cited plants beside their medicinal value in the community. DMR was determined for the top 10 plants.
Results
Demographic, Social and Economic Characteristics of Respondents
We interviewed 119 out of the 366 targeted traditional health practitioners (THPs) in Central Uganda, who came from Kampala 57(47.9%), Wakiso 41(34.5%) and Mukono 21(17.6%). The rest of the targeted participants were excluded as they did not treat breast cancer (n=150) and others did not use herbs in treatment of patients (n=97). Majority of the interviewed THPs (n=81, 72.3%) were male. The age of the respondents ranged between 30–73 years, with a mean of 54.61 years (SD=12.56) and had household members ranging between 1–11 (mean=4.97 members/household, SD=1.76); 81 (68.1%) THPs were married, 66 (55.5%) had attained primary education, 22 (18.5%) had no formal education, 24 (20.2%) had secondary education and only 7 (5.9%) had attained tertiary education.
The respondents were Baganda (62%), Banyankore (16%) and Bakiga (12%). Other ethnic groups in the study area were Basoga (5%), Langi (3.5%) and Lugbara (1.5%). THPs held religious beliefs. Participants disclosed their religions as Christians (56%), Muslims (24%), traditionists (7%), atheists (3%) and others (10%) did not disclose their religion.
Business and farming were the major economic activities of 65% and 30% of respondents, respectively. Only 5% were civil servants; 55% of THPs practised both farming and business as their source of livelihood.
Traditional Knowledge About Breast Cancer
Breast cancer in the study area is locally referred to as Kokoolo wa mabere. THPs commonly recognized breast cancer as a disease by looking for symptoms that included breast swelling (n=74, 62.2%), breast pain (n=29, 24.4%), colour changes in the nipple (n=7, 5.9%), pus from breast (n=6, 5%), and wounds on breast (1, 0.8%) or by asking for hospital documents (n=1, 0.8%).
Treatment Practices and Plant Species Used by THPs for Breast Cancer Patients in Central Uganda
Breast cancer was classified as a rare disease by THPs. Over the past 5 years (January 2015-–August 2020), the 119 THPs had treated a total of 4760 breast cancer patients. The number of patients treated by each THP per year ranged between 1–6 patients, with a mean of 3.76 (SD=1.59). Majority (n=108, 90.8%) of the THPs interviewed claimed that their herbal medicine had cured the patients they treated. However, only 3 (2.5%) of the interviewed THPs provided the first names and contacts of the patients treated for confirmation purposes. The rest of THPs (n=116, 97.5%) reported ignorance of the names and addresses of their patients, claiming it was the patients who sought their services and hence no need to keep their particulars, eg, “I don’t keep their phone numbers; they always call me. I don’t call them” (PID 050).
Some THPs (n=10, 8.4%) freely reported death of their patients: “I don’t have those details but the last patient to treat passed away after a few months because medication was strong for her since the cancer was in its last stages” (PID-071). Another respondent stated: “I have treated one patient and he died after one year for breast cancer otherwise I treat all cancers similarly” (PID-070).
Whereas majority of THPs (n=117, 98.3%) treated BC patients based on symptoms, a few THPs (n=2, 1.7%) reported to have sent patients to the laboratory to confirm diagnosis. Some THPs (n=3, 2.5%) claimed to have a laboratory to diagnose breast cancer, but when the research team asked to confirm existence of such a laboratory, they were not shown any. Patient monitoring was done based on symptoms to assess progress of those on treatment.
In case of treatment failure, 61 (51.3%) THPs reported change to another herbal medicine for the patient, 28 (23.5%) referred to the government health facility and only 6 (5%) THPs reported having abandoned the patients. Alternative ways of handling treatment failure included buying western medicine for the patient (n=6, 5%), discharging the patient (n=5, 4.2%), giving same medicine but adding another plant (n=4, 3.4%), consulting qualified medical doctor (n=3, 2.5%), referring to another THP (n=3, 2.5%) or changing dose (n=1, 0.8%). Only 2 (1.7%) THPs reported never having had any of their herbal medicines failing to cure a breast cancer patient.
A respondent who believes in both traditional medicine and allopathic medicine stated, in the case of patients not responding to their herbal medicine: “I encourage the patient to persist on my medication as they also seek treatment from the hospital” (PID 071).
Over 99.2% (n=118) of referrals of breast cancer patients to other care facilities (other THPs, government health facility or clinic) were verbal. Only 1 THP claimed to make written referrals, although no such copy was available for verification. There were no written notes about breast cancer patients and herbal medicines given to them by all the THPs interviewed. A THP remarked: “We stopped treating so we discarded the records” (PID 057).
None of the THPs admitted to adding western medicine to herbal products for treatment of breast cancer in order to make them stronger. However, 117 (98.2%) THPs admitted to supplying herbal medicines to breast cancer patients in government hospitals and clinics.
Follow up of patients was also reported. In the study, 51 (42.8%) THPs interviewed reported following up their patients after they return to their homes or go to government health facilities and clinics.
THPs held a number of opinions about western medicines used to treat breast cancer. Majority of them stated they have side effects (n=67, 56.3%). Some believed they do not work (n=31, 26.1%), they just relieve symptoms (n=16, 14%). Other opinions reported by THPs included they work (n=1; 0.84%), they work but for a few (n=1, 0.84%), they work but have a lot of side effects (n=1, 0.84%), they work but require herbs to supplement (n=2,1.68%).
One respondent stated: “There is no cure for breast cancer. Western medicine just relieves the symptoms for some time” (PID 057). Another THP stated: “They come with side effects” (PID 085). Another cast doubt on efficacy of modern anti-breast cancer medicines and stated as follows: “I think those drugs don’t work because those patients keep using herbal medicine” (PID 050).
THPs reported advertising on radio (n=32, 26.9%), vending in buses (n=27, 22.7%) and advertising on television (n=21, 17.6%) as means through which breast cancer patients came to know about their services. Others means of access to THP services are indicated in Table 2.
 |
Table 2 How Breast Cancer Patients Come to Know About Services of THPs in Uganda |
Medicinal Plants for Treatment of Breast Cancer by THPs
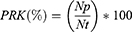
We documented 30 plants used to treat breast cancer by traditional health practitioners in Kampala, Wakiso and Mukono. The plants were distributed over 30 genera and 23 families; predominant families were Asteraceae, Apocynaceae, Euphorbiaceae, Fabaceae, Lamiaceae and Rutaceae. The families Annonaceae (n=24, 20.2%), Vitaceae (n=19, 16%) and Euphorbiaceae (n=11, 9.2%) contributed majority of the species. The most known plants in folk use against breast cancer were Annona muricata L. (Annonaceae), Rhoicissus tridentata (L.f.) Wild and R.B.Drumm (Vitaceae), Erythrococca bongensis Pax (Euphorbiaceae), Ficus sp (Moraceae) and Cannabis sativa L (Cannabaceae) with PRK values of 20.7%, 15.97%, 9.24%, 8.41% and 6.72% respectfully. Other top mentioned plants were Ipomoea wightii (Wall.) Choisy, Erythrina abyssinica DC, Leucas martinicensis (Jacq.) R.Br., Abelmoschus esculentus (L.) Moench and Zanthoxylum chalybeum Engl.
We found an informant consensus factor of 0.75 based on the 119 user reports on breast cancer for the 30 plants documented in the study area. Annona muricata L. had the highest number of user reports on breast cancer. The plants were also used to treat diseases other than breast cancer, as indicated in Table 3.
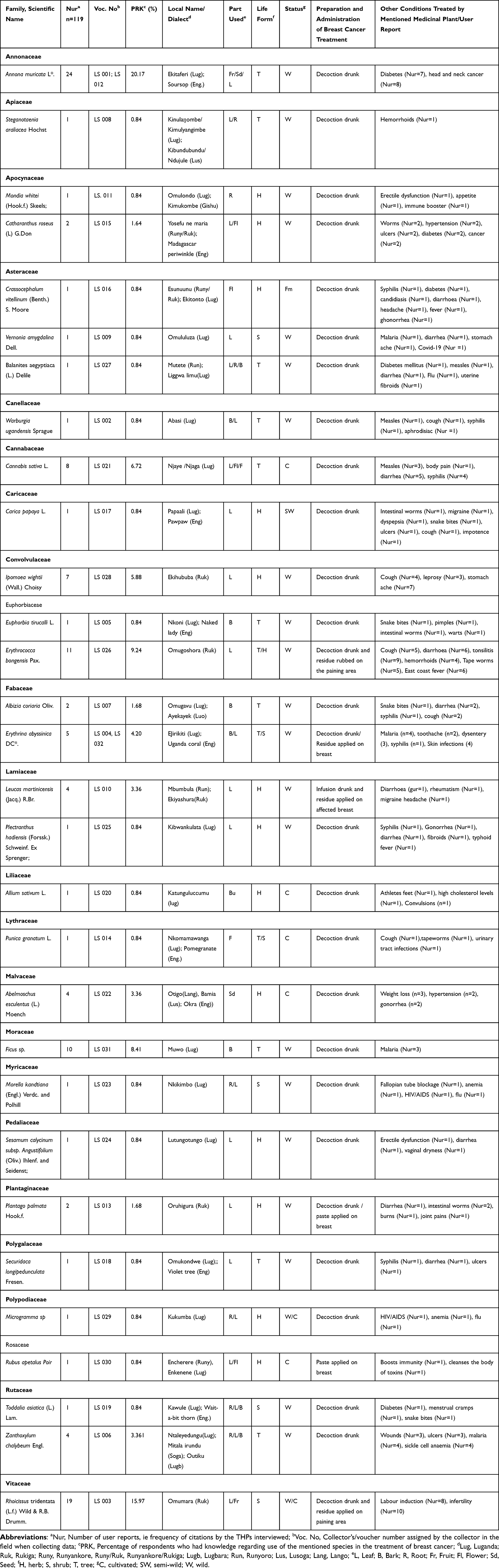 |
Table 3 Medicinal Plants Used to Treat Breast Cancer by Traditional Health Practitioners in Central Uganda |
Fidelity Levels of Medicinal Plants Cited for Treatment of Breast Cancer by THPs
For the 30 cited plant species, a fidelity level was calculated to quantify their importance in treating breast cancer. Ficus sp had the highest fidelity level, 77%, followed by Annona muricata L. (62%) and Leucas martinicensis (Jacq.) R.Br. (57%). Rhoicissus tridentata (L.f) Wild & R.B.Drumm and Steganotaenia araliacea Hochst had similar fidelity levels, of 51% and 50%, respectively. High fidelity levels for these species point to their outstanding preference for treating breast cancer by THPs (Table 4).
 |
Table 4 Fidelity Levels of Medicinal Plants Used in Breast Cancer Treatment by THPs in Central Uganda |
Preferred Medicinal Plant for Breast Cancer Treatment
Annona muricata was highly ranked and regarded the most important in the treatment of breast cancer by the THPs. Table 5 shows rankings of ten most important plant species according to the key informants, together with scores assigned by each informant.
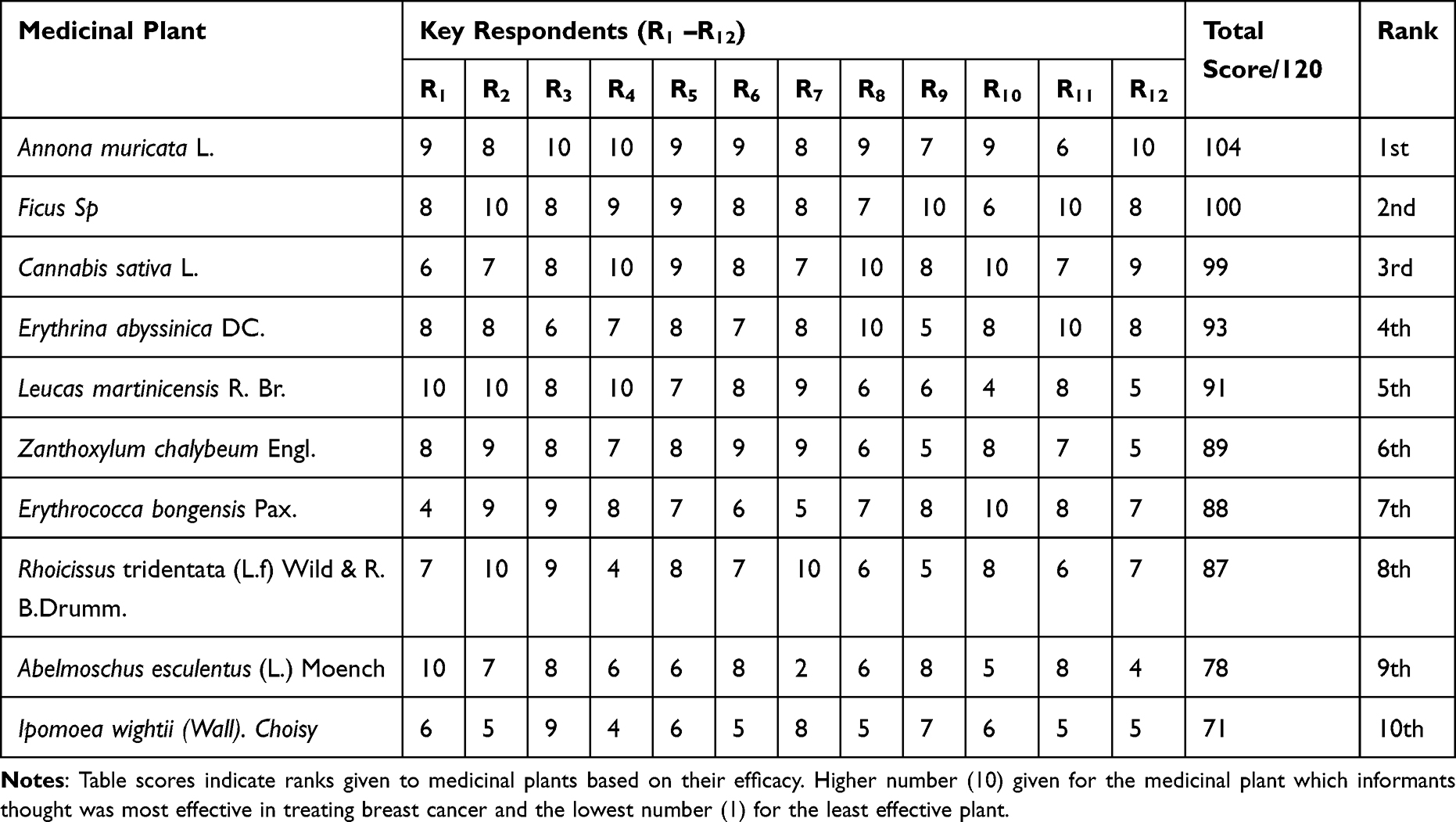 |
Table 5 Preference Ranking of Ten Medicinal Plants Used to Treat Breast Cancer |
Direct Matrix Ranking
DMR results showed that all ten preferred plant species for treatment of breast cancer by THPs have a variety of other non-medicinal uses. Zanthoxylum chalybeum Engl was ranked the highest multipurpose species among the preferred plants for breast cancer treatment by THPs in Central Uganda. Other species utilized for food, construction, fodder, fuel/fire wood beside their medicinal value were Erythrina abyssinica Lam Ex Dc, Erythrococca bongensis, Annona muricata and Ipomoea wightii (Table 6).
 |
Table 6 Direct Matrix Ranking of Preferred Medicinal Plants for Breast Cancer Treatment in Uganda |
Life Forms, Management Status and Plant Parts
The most commonly used life forms were herbs (n=14, 47%) followed by trees (n=11, 37%) and shrubs (n=5, 16%). Majority of these plants occur in the wild (n=23, 72%). Only 25% of plants were cultivated and 3% were semi-wild in their management status. The THPs mentioned the leaves (46%) as the most commonly used plant part in breast cancer treatment, followed by roots (13%), fruits (10%) and flowers (8%), while the rest were used occasionally.
Preparation and Administration of Herbal Remedies
THPs prepared herbal remedies mainly as decoctions (82%) and infusions (3%) that are administered orally. The residues of these preparations were applied on the affected breasts (9%). Some THPs (6%) prepared a paste.
Availability Status and Source of Plants
Most (94.1%) THPs reported that plants used to treat breast cancer were scarce, 5% indicated that the plants were rare and 2% did not know. Despite this, only 6% of THPs reported owning a medicinal garden and only 3.3% had plans to establish such a garden. More than half (52.1%) of THPs collected the plants from the wild source. Other sources of plants were markets (47.1%) and gardens (0.8%).
Discussion
Ethnobotanical surveys have been reported to help scientists identify plants whose medicinal properties may be useful in the development of new drugs for further research.17 In this study, we conducted an ethnobotanical survey to document the existing knowledge and practices related to breast cancer recognition and treatment using medicinal plants by traditional health practitioners (THPs), commonly referred to as herbalists, in the management of breast cancer in the Central Ugandan districts of Kampala, Wakiso and Mukono.
THPs in Central Uganda recognized breast cancer by mainly symptoms of breast swelling and pain. Whereas these are some of the symptoms of breast cancer, they are not conclusive as other diseases such as mastitis can also cause these symptoms. In a Ghanaian study, traditional practitioners are reported to have identified cancers by symptoms of advanced disease such as masses that are visible, fungating lesions, ulceration and bleeding.13 Diagnosis of breast cancer based on symptoms by THPs is not adequate. This can lead to misdiagnosis and wrong treatments given by THPs. There is a need to build capacity of THPs to be able to recognize all the common signs and symptoms of breast cancer in its early stage, as indicated in the established national cancer treatment guidelines, and refer the patients for proper diagnosis by oncologists. This will minimize the number of cases that present to hospitals in advanced stages of the disease and deaths that occur as a result of such advanced disease and wrong treatments given to patients.27,28
Majority of THPs in Central Uganda did not refer patients to biomedical laboratories to confirm diagnosis. In contrast and without specifying the type of cancer, cancer patient referral by THPs to biomedical facilities has been reported in Northern Uganda.29 Non-referral by THPs in Central Uganda implies that they treated unconfirmed breast cancer, and this could account for reported high mortality attributed to breast cancer in Uganda. Studies indicate that THPs cannot properly define cancer.30,31 Elsewhere, some THPs have wrongly defined cancer as having high cholesterol or abscess accumulation.32 Furthermore, there are breast cancer molecular profiles like triple negative breast cancer and HER2 positive breast cancer that have been reported to be significant determinants of advanced stage diagnosis.33 These cannot be diagnosed by simply looking at symptoms, as observed in this study. Therefore, THPs should be sensitized to refer patients to biomedical laboratories for proper diagnosis.
About half of the study participants reported changing to another herbal medicine for patients in case of treatment failure. Only a quarter of the THPs in the study referred the patients to a government health facility in case of treatment failure. This implies that THPs in Central Uganda are hesitant to refer patients to modern health workers. Accordingly, this results in patient delays and late diagnosis as herbalists keep on attempting to cure the breast cancer with different herbal medicines. In contrast, Australian herbalists are reported to be aware of the value of medical diagnosis and inter-referrals, are well informed about patient medications and initiate closer working relationships with the medical community.34 The claims by some THPs that their herbal medicines had cured patients, though there was lack of documentation in place to back up these claims, and fear of losing the patients to modern health care facilities could account for the hesitancy in referring patients.
THPs denied ever adding western medicine to their herbal products for breast cancer in order to make them stronger. This means that THPs treating breast cancer are aware of dangers of adulteration or feared disclosing the practice of adulteration. However, the possibility of adulteration should not be ignored because some THPs reported buying western drugs for patients in case of treatment failure. Accordingly, it can be deduced that THPs can access some of the anti-breast cancer medicines on the market. Studies have shown that some THPs tend to adulterate their herbal products to sustain the claims at expense of patient safety occasioned by compromise in quality and efficacy of products.35–40 Adulteration of herbal products can occur during production or at point of sale, and is in violation of acceptable standards and is a serious standardization problem which affects the quality and reliability of these products.41 There is a need to employ analytical chemistry methods and DNA meta barcoding to rule out adulteration of herbal products supplied by THPs.42,43
When asked about how breast cancer patients came to know about their services, THPs reported vending in buses and advertising on radio and television as the main means. This implies that educational programs like breast cancer screening campaigns targeting breast cancer patients and the general population can be passed on through these channels. Furthermore, the regulatory framework in regard to herbal medicine promotion through advertising by THPs needs to be strengthened. This will ensure delivery of complete, true and unbiased information to the public in regard to herbal medicines for breast cancer treatment and national prevention and treatment guidelines for not only breast cancer but also other health conditions.
THPs in the study area reported using 30 plants belonging to 23 families to treat breast cancer in Central Uganda. Predominant families were Asteraceae, Apocynaceae, Euphorbiaceae, Fabaceae, Lamiaceae and Rutaceae. The ten most commonly mentioned plants were Annona muricata L., Rhoicissus tridentata (L.f.) Wild & R.B.Drumm, Erythrococca bongensis Pax, Ficus sp, Cannabis sativa L., Ipomoea wightii (Wall.) Choisy, Erythrina abyssinica DC., Leucas martinicensis (Jacq.) R.Br., Abelmoschus esculentus (L.) Moench and Zanthoxylum chalybeum Engl. In contrast, 25 plant species belonging to 17 families have been identified for management of breast cancer by traditional medical practitioners in North East Nigeria.44 This finding confirms folk use of medicinal plants in traditional treatment of breast cancer in different countries, including Uganda.
Furthermore, whereas family Asteraceae had highest number of plant species reported to treat breast cancer, the mentioned plants in the study had low user reports on breast cancer by the THPs. This means one was more likely to find a plant species in the family Asteraceae; however, THPs did not frequently use plants in this family against breast cancer as compared to plant species from the other plant families. Asteraceae is one of the most abundant plant families, with more than 23,600 species of plants spread across 1620 genera and 13 subfamilies that occupy all continents except Antarctica.45,46 Accordingly, occurrence of plant species from Asteraceae in the study area was more likely. Low use reports of plants from the family Asteraceae against breast cancer could relate to the effectiveness of plants or scanty documentation of plants within the study area as regards use of these plants for breast cancer. There is a need to explore further the reasons for the observed low use reports of plant species from Asteraceae family for folk treatment of breast cancer. Previous works indicate plant extracts of some species like Senecio graveolens Wedd., Ageratum conyzoides L., and others belonging to family Asteraceae exhibit significant anti-breast cancer activity.47,48 Therefore Asteraceae should be investigated further to document plants with potential anti-breast cancer activities.
An informant consensus factor (IFC) is one of the quantitative indices used to express the benefits, importance and coverage of ethnomedicine.26 In this study, an IFC on breast cancer of 0.75 was observed. This took into account the total number of use reports for breast cancer and total number of species of plants used to treat breast cancer. In contrast, an IFC of 0.96 has been reported in West Bank Palestine.49 A high IFC close to 1, the maximum IFC value, means the mentioned plants in the study are being used extensively within the community and are thus important medicinal plants that can be considered for future pharmacological investigation.
Additionally, the high fidelity levels obtained and preference ranks assigned by THPs indicated that Annona muricata L., Ficus sp, Cannabis sativa L, Erythrina abyssinica Dc and Leucas martinicensis R. Br are considered the most important plants by THPs in Central Uganda in treating breast cancer. Ficus dawei Hutch has previously been reported to be in folk use against breast cancer in Uganda, but quantitative ethnobotanical indices were not reported.50 The other plants are being reported for the first time for breast cancer treatment in the study area. This calls for focusing research efforts on documenting medicinal plants used to treat specific cancers, as there exist more than 277 different types of cancer, with different aetiologies, risk factors, clinical courses and management approaches.51–53
Whereas Annona muricata L has been reported to contain annonaceous acetogenins (Annopentocin A-C, Annomuricin D and Annomuricin E) which account for its anti-breast cancer activity, Ficus sp, though having highest fidelity level and ranked second in terms of preference by the THPs in this study, like many plants mentioned in folk treatment of breast cancer remains uninvestigated, hence the need to generate scientific evidence to justify their continued folk use.54–57 Further research on the plants may lead to isolation of important lead compounds that can be developed into useful drugs for breast cancer treatment. Reports indicate that the anti-breast cancer activity of plants is attributed to presence of important phytochemical compounds, namely, alkaloids, flavonoids, coumarins, phenolic compounds and terpenoids, among some of which their chemical structures have been elucidated.48,58,59 Additionally, there is a likelihood of phytochemical variation that could arise from changes in environmental factors, biophysical limits, part of plant used, extraction methods, age of the plant and other factors, and hence the need to standardize the herbal products made from these plants such that patients are not exposed to unsafe, poor quality and non-efficacious remedies which can worsen their quality of life.
Medicinal plants reported in the study have non-medicinal uses as well. These were used in determining the direct matrix rank (DMR) of each of the preferred plants. Zanthoxylum chalybeum Engl had the highest DMR, calculated based on use category scores assigned by the THPs. This was followed by Erythrina abyssinica DC, Erythrococca bongensis Pax, Annona muricata L. and Ipomea wightii (Wall.) Choisy. The high DMRs of these plants point to the stress placed on them arising from their multipurpose nature in relation to their use and management practices within the community.23 This was the first time DMRs were determined in Uganda for the mentioned plants. Given the high DMR values, these plants are likely to be harvested more by THPs and other community members. There is a need to protect such plants, their natural habitats and promote sustainable use and conservation, in order to not threaten their existence. Such plants may help to offer alternative and complementary treatments for breast cancer patients, based on the fact that conventional anti-cancer medicines are not affordable, the Covid-19 pandemic interrupted the healthcare system and presence of other perceived barriers to health seeking in Uganda.60–62
Limitations of the Study
Besides being time consuming to fill the questionnaires and analyse the data, respondents could have had a recall bias. Many of them had no records of patients treated and hence difficult to recall and verification of the responses difficult. In addition, the length of practice of each THP was not captured during data collection; the findings of this study are limited to Central Uganda and cannot be generalized. The study was cross sectional and data collected during covid-19 pandemic that interrupted in health services delivery due to lock downs.60–62
Conclusions
THPs in Central Uganda recognized breast cancer by symptoms. Medicinal plants applied in its folk treatment have been documented and the claims of cure by THPs merit further investigation. We underscored the need for documentation of such medicinal plant folk knowledge in the context of traditional diagnosis and management of breast cancer by the herbalists. Future works should focus on providing scientific validation of the documented plants in terms of chemical profiling, preclinical pharmacological testing against specific breast cancer cell lines and clinical evaluation. Promotion of good agricultural practices for sustainable utilization of the mentioned plants is warranted.
Ethics Approval and Informed Consent
The study was approved by Mbarara University Faculty of Medicine Research Committee (Ref DMS6), Gulu University Research and Ethics Committee (GUREC-016-19) and registered with the Uganda National Council of Science and Technology (HS405ES). Participants’ informed consent included publication of anonymized responses.
Acknowledgments
We would like to thank Ms. Wanyana Olivia of Makerere University Herbarium for identifying the plants in the study; Mr Majeme Deo for technical assistance in data analysis; research participants and field work team in data collection; financial assistance from Pharm-Biotechnology and Traditional Medicine Centre at Mbarara University of Science and Technology.
Disclosure
Dr Stephen Lutoti reports grants from Pharmbiotechnolgy and Traditional medicine centre Mbarara university of Science and Technology, Uganda, during the conduct of the study. All authors declare no other conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics. CA Cancer J Clin. 2019;69:7–34.
2. Asasira J, Lee S, Tran TXM, et al. Infection-related and lifestyle-related cancer burden in Kampala, Uganda: projection of the future cancer incidence up to 2030. BMJ Open. 2022;16:e056722. doi:10.1136/bmjopen-2021-056722
3. Uganda Cancer Institute. Cancer treatment guidelines; 2017:22–41.
4. Odongo J, Makumbi T, Kalungi S, Galukande M. Patient delay factors in women presenting with breast cancer in a low income country. BMC Res Notes. 2015;8:467. doi:10.1186/s13104-015-1438-8
5. Mwaka AD, Abbo C, Kinengyere AA. Traditional and complementary medicine use among adult cancer patients undergoing conventional treatment in Sub-Saharan Africa: a scoping review on the use, safety and risks. Cancer Manag Res. 2020;12:3699–3712. doi:10.2147/CMAR.S251975
6. Mwesige B. Economic evaluation of cancer medicines usage at Uganda Cancer Institute. Value Health. 2016;19:A886. doi:10.1016/j.jval.2016.08.257
7. Liu J, Ming B, Gong GH, et al. Current research on anti-breast cancer synthetic compounds. RSC Adv. 2018;8:4386–4416. doi:10.1039/C7RA12912B
8. Nakaganda A, Solt K, Kwagonza L, et al. Challenges faced by cancer patients in Uganda: implications for health systems strengthening in resource limited settings. J Cancer Policy. 2021;27:100263. doi:10.1016/j.jcpo.2020.100263
9. Benarba B. Use of medicinal plants by breast cancer patients in Algeria. EXCLI J. 2015;14:1164–1166. doi:10.17179/excli2015-571
10. Benarba B, Belabid L, Righi K, et al. Ethnobotanical study of medicinal plants used by traditional healers in Mascara (North West of Algeria). J Ethnopharmacol. 2015;175:626–637. doi:10.1016/j.jep.2015.09.030
11. Jaikumar B, Jasmine R. A review on a few medicinal plants possessing anticancer activity against human breast cancer. IJPRIF. 2016;9:333–365.
12. James PB, Wardle J, Steel A, Adams J. Traditional, complementary and alternative medicine use in Sub-Saharan Africa: a systematic review. BMJ Glob Health. 2018;3:e000895. doi:10.1136/bmjgh-2018-000895
13. O’Brien KS, Soliman AS, Annan K, et al. Traditional Herbalists and Cancer Management in Kumasi, Ghana. J Cancer Educ. 2012;27:573–579. doi:10.1007/s13187-012-0370-z
14. Uganda Bureau of Statistics. The National population and Housing census 2014-Area Specific Profile series. Pigm Resin Technol. 2017;1:19–91.
15. Tabuti JR, Kukunda CB, Kaweesi D, Kasilo OM. Herbal medicine use in the districts of Nakapiripirit, Pallisa, Kanungu, and Mukono in Uganda. J Ethnobiol Ethnomed. 2012;8:35. doi:10.1186/1746-4269-8-35
16. Weisheit A; For World Bank. Traditional medicine practice in Contemporary Uganda. Indian Knowl. 2003;54:1–4.
17. Tugume P, Kakudidi KE, Buyinza M, et al. Ethnobotanical survey of medicinal plant species used by communities around Mabira Central Forest Reserve, Uganda. J Ethnobiol Ethnomed. 2016;12:5. doi:10.1186/s13002-015-0077-4
18. Bieski IGC, Rios Santos F, de Oliveira RM, et al. Ethnopharmacology of medicinal plants of the Pantanal region (Mato Grosso, Brazil). Evid Based Complement Alternat Med. 2012;2012:272749. doi:10.1155/2012/272749
19. Espinosa MM, Bieski IGC, Martins DT. Probability sampling design in ethnobotanical surveys of medicinal plants. Rev Bras Farmacogn. 2012;22:1362–1367. doi:10.1590/S0102-695X2012005000091
20. Höft M, Barik SK, Lykke A. Quantitative Ethnobotany Applications of multivariate and statistical analyses in ethnobotany; 1999:1–46.
21. Alshenqeeti H. Interviewing as a data collection method: a critical review. Engl Linguist Res. 2014;3:39. doi:10.5430/elr.v3n1p39
22. Creswell JW, Creswell JD. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches.
23. Yassin S, Abera B, Kelbessa E. Ethnobotanical study of indigenous knowledge of plant-material culture in Masha and Yeki Districts, Southwest Ethiopia. AJPS. 2015;9:25–49.
24. Opio DR, Andama E, Kureh GT. Ethnobotanical Survey of Antimalarial Plants in Areas of Abukamola, Angeta, Oculokori and Omarari of Alebtong District in Northern Uganda. European J Med Plants. 2017;21:1–14. doi:10.9734/EJMP/2017/38043
25. Reyes-García V, Martí N, McDade T, et al. Concepts and methods in studies measuring individual ethnobotanical knowledge. J Ethnobiol. 2007;27:182–203. doi:10.2993/0278-0771(2007)27[182:CAMISM]2.0.CO;2
26. Faruque MO, Uddin SB, Barlow JW, et al. Quantitative ethnobotany of medicinal plants used by indigenous communities in the bandarban district of Bangladesh. Front Pharmacol. 2018;9:40. doi:10.3389/fphar.2018.00040
27. Akuoko CP, Armah E, Sarpong T, et al. Barriers to early presentation and diagnosis of breast cancer among African women living in sub-Saharan Africa. PLoS One. 2017;12:e0171024. doi:10.1371/journal.pone.0171024
28. Opoku SY, Benwell M, Yarney J. Knowledge, attitudes, beliefs, behaviour and breast cancer screening practices in Ghana, West Africa. Pan Afr Med J. 2012;11:28.
29. Mwaka AD, Achan J, Adoch W, Wabinga H. From their own perspectives: a qualitative study exploring the perceptions of traditional health practitioners in northern Uganda regarding cancers, their causes and treatments. BMC Fam Pract. 2021;22:155. doi:10.1186/s12875-021-01505-w
30. Co M, Lee A, Kwong A. Delayed presentation, diagnosis, and psychosocial aspects of male breast cancer. Cancer Med. 2020;9:3305–3309. doi:10.1002/cam4.2953
31. Louise B, Jonine F, Ernest A, et al. Factors contributing to delays in diagnosis of breast cancers in Ghana, West Africa. Breast Cancer Res Treat. 2017;162:105–114. doi:10.1007/s10549-016-4088-1
32. Al-Naggar RA, Bobryshev YV, Abdulghani MA, et al. Knowledge and perceptions of cancer and cancer prevention among Malaysian traditional healers: a qualitative study. Asian Pac J Cancer Prev. 2012;13:3841–3850. doi:10.7314/APJCP.2012.13.8.3841
33. Agodirin O, Aremu I, Rahman G, et al. Determinants of delayed presentation and advanced-stage diagnosis of breast cancer in Africa: a systematic review and meta-analysis. Asian Pac J Cancer Prev. 2021;22:1007–1017. doi:10.31557/APJCP.2021.22.4.1007
34. Casey M, Adams J, Sibbritt D. An examination of the clinical practices and perceptions of professional herbalists providing patient care concurrently with conventional medical practice in Australia. Complement Ther Med. 2008;16:228–232. doi:10.1016/j.ctim.2007.06.002
35. Ariffin SH, Wahab IA, Hassan Y, Abd Wahab MS. Adulterated traditional-herbal medicinal products and its safety signals in Malaysia. DHPS. 2021;13:133–140. doi:10.2147/DHPS.S305953
36. Crighton E, Mullaney I, Trengove R, et al. The application of metabolomics for herbal medicine pharmacovigilance: a case study on ginseng. Essays Biochem. 2016;60:429–435. doi:10.1042/EBC20160030
37. Cunningham AB, Long X. Linking resource supplies and price drivers: lessons from Traditional Chinese Medicine (TCM) price volatility and change, 2002–2017. J Ethnopharmacol. 2019;229:205–214. doi:10.1016/j.jep.2018.10.010
38. Heinrich M. Quality and safety of herbal medical products: regulation and the need for quality assurance along the value chains. Br J Clin Pharmacol. 2015;80:62–66. doi:10.1111/bcp.12586
39. Ichim MC. The DNA-based authentication of commercial herbal products reveals their globally widespread adulteration. Front Pharmacol. 2019;10:1227. doi:10.3389/fphar.2019.01227
40. Sorkin BC, Kuszak AJ, Bloss G, et al. Improving natural product research translation: from source to clinical trial. FASEB J. 2020;34:41–65. doi:10.1096/fj.201902143R
41. Miray E. The Hidden Danger in Phytopharmaceuticals: adulteration. In: Durgesh NC, Kamal S, editors. Phytopharmaceuticals: Potential Therapeutic Applications. Beverly: Scrivener Publishing LLC; 2021:77–98.
42. de Boer HJ, Ichim MC, Newmaster SG, Barcoding DNA. Pharmacovigilance of Herbal medicines. Drug Saf. 2015;38:611–620. doi:10.1007/s40264-015-0306-8
43. Urumarudappa SKJ, Tungphatthong C, Prombutara P, et al. DNA metabarcoding to unravel plant species composition in selected herbal medicines on the National List of Essential Medicines (NLEM) of Thailand. Sci Rep. 2020;10:18259. doi:10.1038/s41598-020-75305-0
44. Zainab M, Hajja H, Aliyu D, et al. Ethnomedicinal survey of folkloric plants used in managing breast cancers by the traditional medical practitioners of North‐east Nigeria (LB240) - Mohammed - 2014. FACEB J. 2014;28:240.
45. Broholm SK, Teeri TH, Elomaa P. Molecular Control of Inflorescence Development in Asteraceae. The molecular genetics of floral transition and flower development. In: Fabio F, editor. Advances in Botanical Research. Oxford: Elsevier Academic Press; 2014:297–333.
46. Tamokou JDD, Mbaveng AT, Kuete V. Antimicrobial Activities of African Medicinal Spices and Vegetables. In: Medicinal Spices and Vegetables from Africa: Therapeutic Potential Against Metabolic Inflammatory Infectious and Systemic Diseases. Cambridge: Academic press; 2017:207–237.
47. Adebayo AH, Tan NH, Akindahunsi AA, Zhang YM, Adebayo AH. Anticancer and antiradical scavenging activity of Ageratum conyzoides L. (Asteraceae). Pharmacogn Mag. 2010;6:62–66. doi:10.4103/0973-1296.59968
48. Echiburú-Chau C, Alfaro-Lira S, Brown N, et al. The selective cytotoxicity elicited by phytochemical extract from Senecio graveolens (Asteraceae) on breast cancer cells is enhanced by hypoxia. Int J Oncol. 2014;44:1357–1364. doi:10.3892/ijo.2014.2302
49. Jaradat NA, Al-Ramahi R, Zaid AN, et al. Ethnopharmacological survey of herbal remedies used for treatment of various types of cancer and their methods of preparations in the West Bank-Palestine. BMC Complement Altern Med. 2016;16:93. doi:10.1186/s12906-016-1070-8
50. Omara T, Kiprop AK, Ramkat RC, et al. Medicinal plants used in traditional management of cancer in Uganda: a review of ethnobotanical surveys, phytochemistry, and anticancer studies. Evid Based Complement Alternat Med. 2020;2020:3529081. doi:10.1155/2020/3529081
51. Blackadar CB. Historical review of the causes of cancer. World J Clin Oncol. 2016;7:54–86. doi:10.5306/wjco.v7.i1.54
52. Hassanpour SH, Dehghani M. Review of cancer from perspective of molecular. J Cancer Res Pract. 2017;4:127–129. doi:10.1016/j.jcrpr.2017.07.001
53. Wang S, Liu Y, Feng Y, et al. A review on curability of cancers: more efforts for novel therapeutic options are needed. Cancers. 2019;11:1782. doi:10.3390/cancers11111782
54. CABI Compedium. Annona muricata (soursop). Virginia; 2015. Available from https://www.cabidigitallibrary.org/doi/10.1079/cabicompendium.5812.
55. Levitsky DO, Dembitsky VM. Anti-breast cancer agents derived from plants. Nat Prod Bioprospect. 2015;5:1–16. doi:10.1007/s13659-014-0048-9
56. Moghadamtousi SZ, Fadaeinasab M, Nikzad S, et al. Annona muricata (Annonaceae): a review of its traditional uses, Isolated acetogenins and biological activities. Int J Mol Sci. 2015;16:15625–15658. doi:10.3390/ijms160715625
57. Syed Najmuddin SUF, Romli MF, Hamid M, et al. Anti-cancer effect of Annona Muricata Linn Leaves Crude Extract (AMCE) on breast cancer cell line. BMC Complement Altern Med. 2016;16:311. doi:10.1186/s12906-016-1290-y
58. Rishton GM. Natural products as a robust source of new drugs and drug leads: past successes and present day issues. Am J Cardiol. 2008;101:43D–49D. doi:10.1016/j.amjcard.2008.02.007
59. Yin S-Y, Wei W-C, Jian F-Y, et al. Therapeutic applications of herbal medicines for cancer patients. Evid Based Complement Alternat Med. 2013;2013:302426. doi:10.1155/2013/302426
60. Meacham E, Orem J, Nakigudde G, et al. Exploring stigma as a barrier to cancer service engagement with breast cancer survivors in Kampala, Uganda. Psychooncology. 2016;25:1206–1211. doi:10.1002/pon.4215
61. Abila DB, Ainembabazi P, Wabinga H. COVID-19 pandemic and the widening gap to access cancer services in Uganda. Pan Afr Med J. 2020;35(Suppl 2):140. doi:10.11604/pamj.supp.2020.35.2.25029
62. Mwaka AD, Walter FM, Scott S, et al. Symptom appraisal, help-seeking and perceived barriers to healthcare seeking in Uganda: an exploratory study among women with potential symptoms of breast and cervical cancer. BMJ Open. 2021;11:e041365.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.