Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Ethical Dilemmas in Physicians’ Consultations with COPD Patients
Authors Sigurgeirsdottir J ![]() , Halldorsdottir S
, Halldorsdottir S ![]() , Arnardottir RH
, Arnardottir RH ![]() , Gudmundsson G
, Gudmundsson G ![]() , Bjornsson EH
, Bjornsson EH ![]()
Received 6 January 2022
Accepted for publication 28 March 2022
Published 2 May 2022 Volume 2022:17 Pages 977—991
DOI https://doi.org/10.2147/COPD.S356107
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Jonina Sigurgeirsdottir,1,2 Sigridur Halldorsdottir,3 Ragnheidur Harpa Arnardottir,3– 5 Gunnar Gudmundsson,1,6 Eythor Hreinn Bjornsson2
1Faculty of Medicine, University of Iceland, Reykjavik, Iceland; 2Pulmonary Department, Reykjalundur Rehabilitation Center, Mosfellsbaer, Iceland; 3Faculty of Graduate Studies, School of Health Sciences, University of Akureyri, Akureyri, Iceland; 4Department of Rehabilitation, Akureyri Hospital, Akureyri, Iceland; 5Department of Medical Sciences, Respiratory-, Allergy- and Sleep Research, Uppsala University, Uppsala, Sweden; 6Department of Respiratory Medicine and Sleep, Landspitali University Hospital, Reykjavik, Iceland
Correspondence: Jonina Sigurgeirsdottir, Pulmonary Department, Reykjalundur Rehabilitation Center, Furubyggd 28, Mosfellsbaer, 270, Iceland, Tel +354 6261740, Email [email protected]
Aim: This phenomenological study was aimed at exploring principal physicians’ (participants’) experience of attending to COPD patients and motivating their self-management, in light of the GOLD clinical guidelines of COPD therapy.
Methods: Interviews were conducted with nine physicians, who had referred patients to PR, five general practitioners (GPs) and four lung specialists (LSs). The interviews were recorded, transcribed, and analyzed through a process of deconstruction and reconstruction.
Results: The participants experienced several ethical dilemmas in being principal physicians of COPD patients and motivating their self-management; primarily in the balancing act of adhering to the Hippocratic Oath of promoting health and saving lives, while respecting their patients’ choice regarding non-adherence eg, by still smoking. It was also a challenge to deal with COPD as a nicotine addiction disease, deal with patients’ denial regarding the harm of smoking and in motivating patient mastery of the disease. The participants used various strategies to motivate their patients’ self-management such as active patient education, enhancing the patients’ inner motivation, by means of an interdisciplinary approach, involving the patients’ significant other when appropriate, and by proposing PR.
Conclusion: The findings indicate that being a principal physician of COPD patients and motivating their self-management is a balancing act, involving several dilemmas. Patients’ nicotine addiction and physicians’ ethical obligations are likely to create ethical dilemmas as the physician is obligated to respect the patients’ will, even though it contradicts what is best for the patient. The participants suggest strategies to motivate COPD patients’ self-management.
Keywords: physicians, physician-patient relations, physician’s role, COPD, self-management, motivation, patient education, qualitative research, interviews
Introduction
Enhancing best practice in motivating self-management in multimorbidity is an important aspect of general healthcare.1–3 The GOLD guidelines (2019) outline the importance of physician’s quick response to signs of chronic obstructive pulmonary disease (COPD) with early diagnosis and a medication plan to act against exacerbations, instant focus on cigarette smoking as an independent risk-factor, and proposing a referral to a smoking cessation therapy and pulmonary rehabilitation (PR) to enhance patients’ health and quality of life.4–6
Therefore, it has been questioned why General Practitioners’ (GPs’) routine checkups of COPD patients sometimes seem to fail to involve active measures towards motivating patients’ smoking cessation.7 Patient motivation has been defined as readiness for change,8 preparation for treatment, or as how committed patients are to start a change process.9,10 For us, the concept of motivation is in this respect defined as the probability that a person will enter into, continue, and adhere to a specific change strategy,8 connected with the patient’s active engagement and goal-setting.11,12
Self-management is a key concept in COPD therapy and the focus of a multi-component intervention.13 In spite of well-known guidelines, the diagnosis of COPD is too often made late enough to leave the patients’ lungs damaged, with an unnecessary delay to providing patients with the needed treatment.14 Furthermore, physicians have noted that compared with patients addicted to alcohol, there is a lack of detoxification for patients dealing with nicotine dependency.15
Both rehabilitation and chronic illness literature promote the importance of interdisciplinary team work to serve the growing number of chronically ill people, which connects concepts of self-management and interdisciplinary rehabilitation.16,17 Interventions regarding self-management support have been linked with reduced COPD patients’ hospital re-admission rate and quality of life.18,19 Therefore, the interpersonal relations between health professionals and patients may be a valuable source of power that health professionals can use to mobilize their patients.20,21
Physicians’ role in the treatment of COPD is crucial, as is the physicians’ role to provide information, education, and guidance about patients’ own critical role in the disease trajectory.22,23 Some physicians refer to nicotine addicted patients as a difficult group who may reject them if pressed to stop smoking, and a study concludes that physicians’ tendency to avoid addressing patients’ tobacco dependence, needs to be further explored,15 as well as a link has been established between nicotine addiction and depression which is underdiagnosed in COPD patients.24,25 Adding psychological services to the treatment of nicotine dependence has been suggested, as well as allowing for more flexibility for GPs to allocate depressed COPD patients with extra consultation time for educational and medical therapy.24
From 2000–2015 the rate of smoking or using some form of tobacco in Iceland declined from 33% to about 8.2% of the population. Moreover, smoking prevalence of adults in Iceland is currently the third lowest in the world.25
The physician has a key role in helping COPD patients to cope with their uncurable chronic disease and finding the way through the myriad of complicated comorbidities, but studies suggest that interdisciplinary team-work is also important for the patients.26 Our previous studies imply that identification of COPD patients’ self-reported needs and their needs-driven coping strategies can help the physician to enhance the patients’ self-management.27 Furthermore, we have found that COPD patients’ immediate families (spouse/adult children) experience frustration against an advancing burden of caring and trying to motivate the patients towards self-management.28 Self-management interventions in COPD focus on individuals’ needs, aim at improving their self-management skills, giving feedback on new skills, focusing on exacerbations rate, duration of hospitalizations and healthcare costs, enhancing patients’ active role and improved health-related quality of life (HRQoL).15,29 Healthcare professionals receive little guidance in providing self-management support, and the available resources have been outside the scope of traditional training.30 Physicians’ experiences of attending to COPD patients and motivating them towards self-management, have not yet been explored, even though their experience is crucial to provide a holistic view of COPD patients’ self-management.
The researchers, therefore, aimed at answering the following twofold research question: What is physicians’ experience of attending to COPD patients’ and what are their strategies to facilitate their patients’ self-management?
Materials and Methods
The research methodology used was the Vancouver School of Doing Phenomenology (the Vancouver-School), which traces its roots to the works of Spiegelberg31 (phenomenology) in a unique blend with Ricoeur32,33 (hermeneutic phenomenology), and Schwandt34 (constructivism). Deepening understanding and increasing knowledge about human phenomena is the focus of the Vancouver-School, and the aim is to explore participants’ experiences in a way that hopefully can eventually result in improved human services.33 In-depth interviews are characteristic for the methodology of the Vancouver-School and in this study the first author interviewed nine physicians.35 An example of the interview guide is provided (Figure 1). The research process is divided into seven main cognitive aspects (Figure 2), repeated in each of the 12 main research steps of the Vancouver-School (Table 1). Each participant was regarded as a case study because the Vancouver-School involves individual cases analysis (Steps 1–7) followed by inter-case analysis (Steps 8–12). By means of text analysis methods and abstract thought processes, researchers construct their findings.35 A temporal overlapping of the literature search, data collection and data analysis was according to the Vancouver-School.35 The participants were suggested by patients who participated in a previous study,27 five General Practitioners and four Lung Specialists (Table 2). Quantity of raw data is presented in Table 3 and data saturation was achieved when no new themes were identified in the interviews and the research team deemed that the research question had been successfully answered.
 |
Table 1 The 12 Research Steps of the Vancouver School of Doing Phenomenology and How These Steps Were Followed in the Present Study |
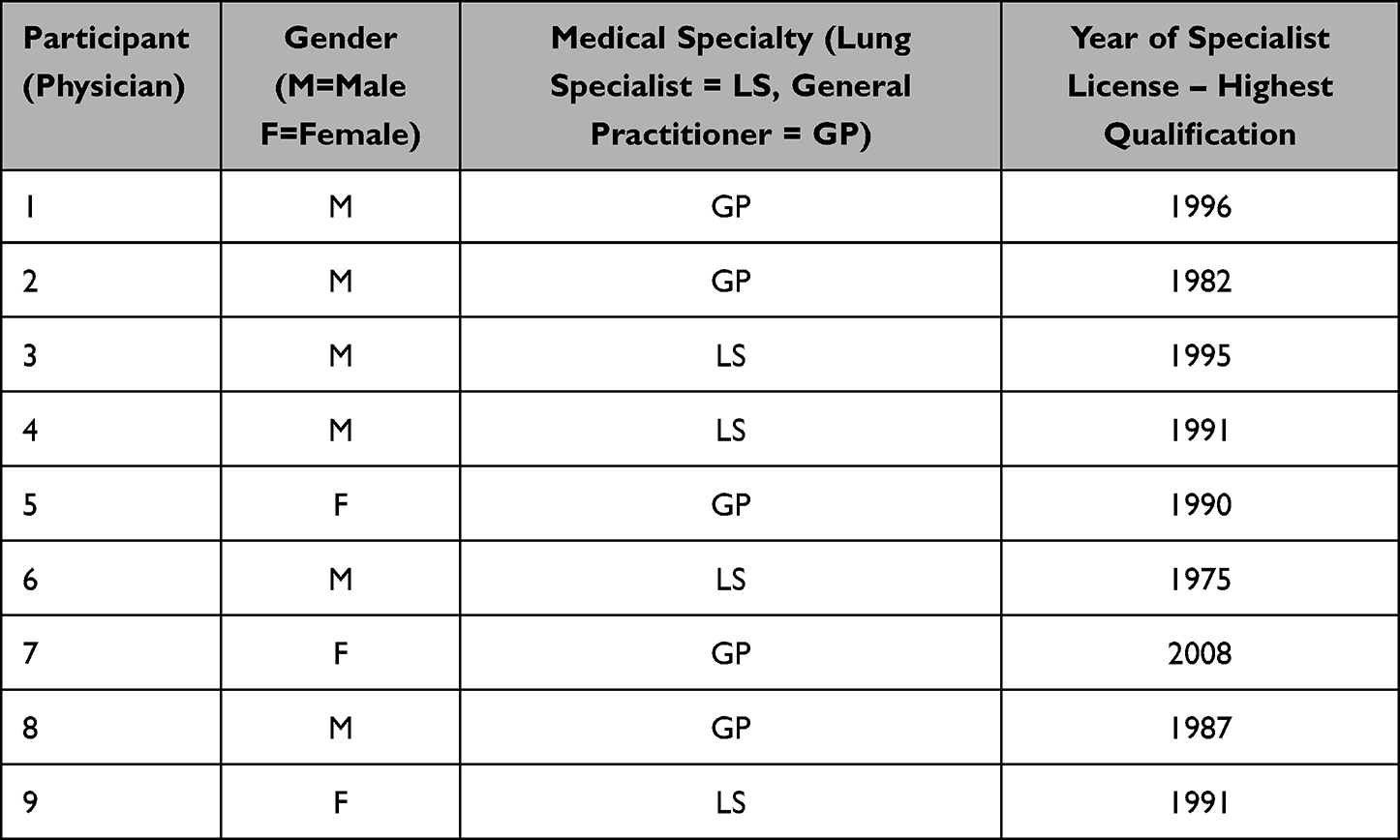 |
Table 2 Overview of the Participants |
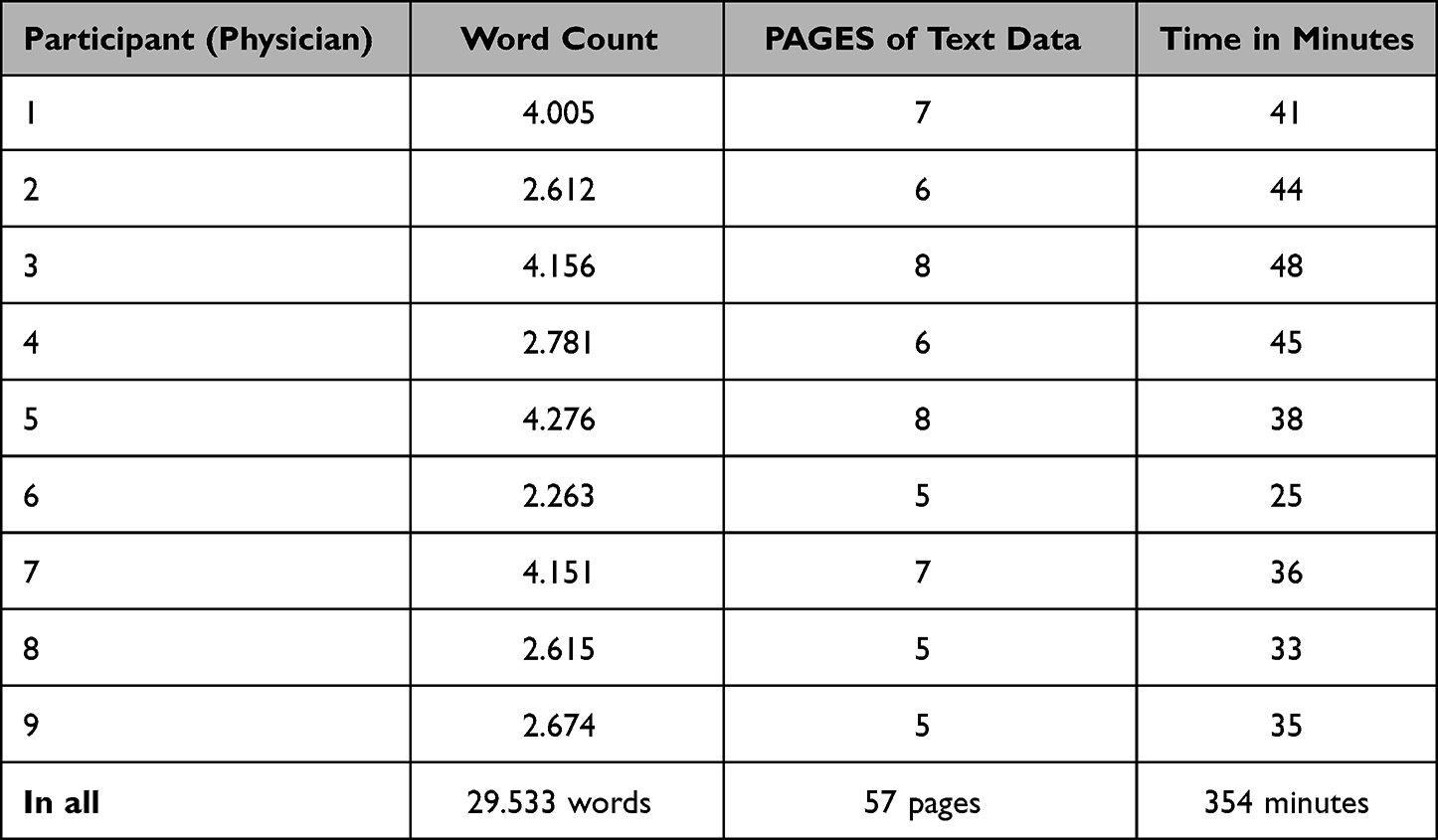 |
Table 3 Raw Data - Quantity |
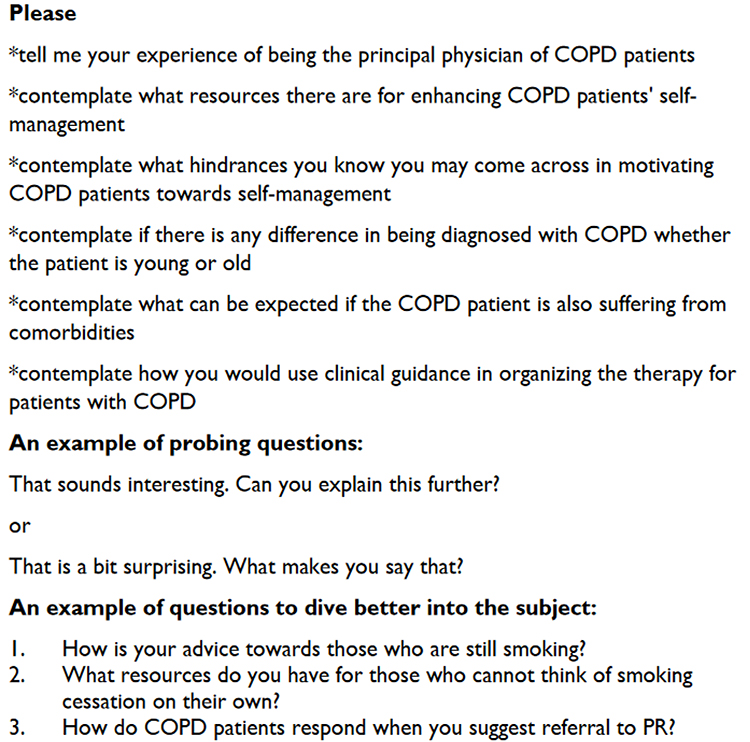 |
Figure 1 Sample of interview questions posed in Study 3. |
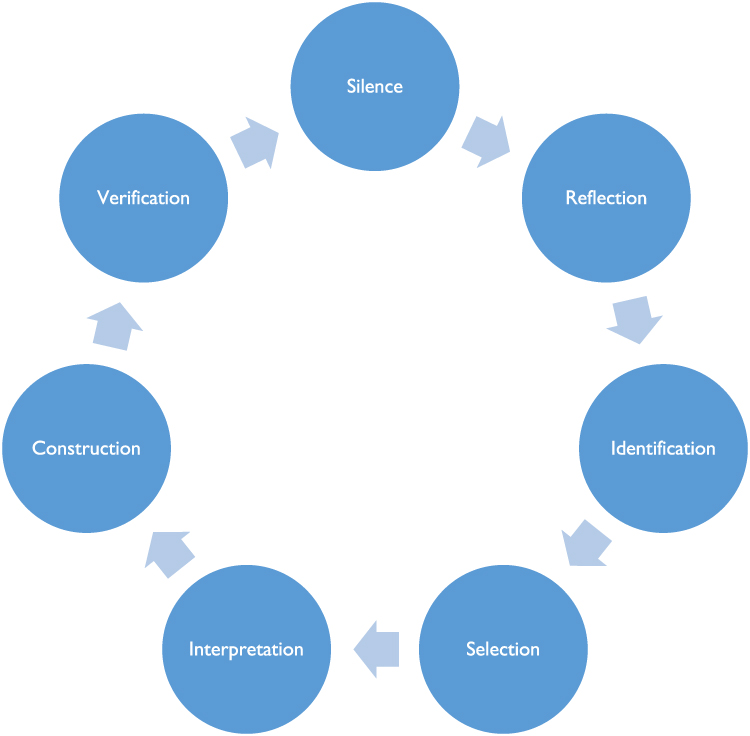 |
Figure 2 The repeated cycle of cognitive work in each of the 12 steps in the Vancouver School of Doing Phenomenology. Notes: Adapted with permission from: Halldorsdottir S. The Vancouver School of Doing Phenomenology. In: Fridlund B, Hildingh C, editors. Qualitative research Methods in the Service of Health. Lund: Studentlitteratur; 2000:47–81.35 Copyright © Studentlitteratur 2000. |
An ethical clearance for conducting the study was provided by The Icelandic National Bioethics Committee (Reference number 17–120). Possible participants were informed about the study in writing and orally. No data were collected until informed consent was signed and the participants’ informed consent included publication of anonymized responses.
Results
The participants experienced several ethical dilemmas in being physicians of COPD patients and motivating their self-management; primarily in the balancing act of adhering to the Hippocratic Oath of promoting health and saving lives and seeing tobacco discussion as an ethical duty while respecting their patients’ choice regarding non-adherence eg, by still smoking. It was also a challenge to deal with COPD as a nicotine addiction disease, deal with patient denial regarding the harm of smoking and in motivating patient mastery of the disease. The participants used various strategies to motivate the patients’ self-management such as active patient education, enhancing the patients’ inner motivation, using certain strategies to help smokers quit smoking, promoting an interdisciplinary approach, involving the patients’ significant other when appropriate and by proposing PR. Some participants reflected on the Nursing Care for individuals with lung diseases and individuals, dependent on mechanical ventilation, and their families, in an outpatient clinic at the National University Hospital Reykjavik Iceland (The Outpatient Nursing Clinic), as a vital service for COPD patients and their families. However, one participant considered if the prolonged continuity of this service might increase the patients’ dependency on healthcare staff, and eventually lead to their decreased self-management (Participant 6=P6).
Physicians’ Ethical Dilemmas Regarding Attending to COPD Patients
The experience of being the principal physician of patients with COPD was characterized for participants by several ethical dilemmas, primarily concerning patient smoking. The participants urged their patients to stop smoking while simultaneously trying to avoid scaring them away. As one of them said:
Scolding is useless and leads the patient to think. ‘this physician is no good’. and he never comes back. (P2)
One participant noted that the attitude towards smoking has drastically changed in Iceland which has made much difference:
Smoking has declined, it’s almost taboo, and people smoke outside. They hide. They don’t smoke around other people and hide it if they do smoke. It is also defined as low-class; you are marking yourself as such by being a smoker … You need to confess. not only that you are a loser by being a smoker, you’re also poor, and all that. (P5)
Dealing with COPD as a Nicotine Addiction Induced Disease
All the participants mentioned nicotine addiction as a major issue for COPD patients and concluded that their medical education had provided too little preparation for this role. The participants recommended motivating patients to stop smoking and some proposed the idea of consulting a specialist in addiction diseases or specialized smoking cessation support (P3,4). Two participants observed that older patients were more likely than younger ones to accept the advice to stop smoking; younger patients could not see any reason to deal with it now because they did not see nicotine dependence as their main problem (P2,3). The participants prescribed drugs for smoking cessation such as Nicotine supplement (P9) and Varenicline (P1,2,7,8), but only a few mentioned the Icelandic Smoke-free Helpline (P7,9). One participant speculated whether it would be wise to integrate more comprehensive drug dependence treatment into the current PR, regarding smoking addiction (P4).
These people, like all others, receive the respiratory drugs they need (P1). Dependence is the big problem of those who are addicted to some substances as they need to have their substance at whatever cost. But there are many examples where we [the participant and a pulmonary nurse] work together as a team to get people off tobacco. And we often succeed, thank goodness. [Official smoking cessation therapy is] what is lacking in my opinion, at the hospital or somewhere else. (P4)
Dealing with Patient Denial Regarding the Harm of Smoking
Some participants observed better compliance by elderly patients and that younger patients were more likely to deny the risk of tobacco smoking, and some found them resistant to acknowledging their slowly but gradually developing COPD until they identified themselves as patients because of severe breathlessness (P1,2). This denial may be caused by fear of dyspnea, but it delays tests that provide the necessary basis for diagnosis to initiate therapy (P2,8). Denial was explained by one participant as if someone wants me to do something that I do not intend to do, I will avoid or confront that person (P5). If a patient suspects that he or she will be urged to stop smoking, that suspicion may be a reason for avoidance (P2,5), although recognizing the causal relationship between smoking and illness is of vital importance (P3,9).
Clinging to independence and self-determination, rather than considering whether life will be prolonged for some years, was associated by two participants with child-like non-compliance (P5,7).
[Late medical consultation] may be caused by denial, nicotine addiction or slowly exacerbating symptoms that the patient has not observed. Some may fear consulting the GP, fear being told to stop smoking [and] finding that a bad idea. But if you have a good talk with the patient and inform him or her that the symptoms might be relieved, it is a valuable motivation, and some quit smoking immediately. (P8)
Some participants regarded younger people as more likely to deny being ill … and likely to refuse giving up smoking (P2,7).
Although patients enter [the clinic] breathless, some of them constantly minimize their symptoms. You might say. it is a kind of resistance to admitting they have disease when they say. ‘I’m not that bad’. Convincing someone below the age of 60 that smoking cessation is feasible, is difficult. They are in denial, and it is extremely difficult to deal with them. Smoking is difficult also because smokers are looked down upon these days. People feel ashamed for smoking and try to hide it. When they realize that their symptoms are irreversible, they start behaving responsibly, or 90% of them do. (P2)
On the contrary, one participant explained:
It’s my gut feeling that younger people, this is complicated, are more responsive, in a way. You often mention their age in such a conversation, especially if we are discussing smoking cessation. You talk about life span, what is ahead, you have so much to gain – you’re 42 years of age, but your time will be much harder if you can’t stop smoking. This may be unethical, but it seems such a long and difficult time they have ahead. I think about it a lot. (P4)
Dealing with Tobacco Discussion as an Ethical Duty
As two participants said, a kind of equilibrium is needed between the physician and the patient, taking care not to reiterate inappropriate propaganda in every visit (P4,5). Those two ended their comments essentially in the same way: I regard [tobacco discussion] as my ethical duty and I will continue to do that (P4,5). However, despite tobacco discussions some patients kept on smoking:
Some people continue smoking regardless of what you say, repeatedly getting pneumonia … their lungs infected, an illness caused by smoking and we both know that, but they claim they need nothing except their pulmonary drugs. We’re dealing with all kinds of people. The poorest ones are for me the most difficult to reach, some of them willful, stubborn, or bitter. This may be a social phenomenon, if someone expects me to do something and I don’t intend to do it, then I’ll stay away from him or her. I think some people are more interested in clinging to their right to self-determination than whether they are healthy or not, or whether they may live a bit longer. (P5)
Physicians’ Strategies to Motivate COPD Patients’ Self-Management
The participants’ experience of motivating the COPD patients’ self-management was characterized by six main strategies ie, educating the COPD patient and family, enhancing patients’ inner motivation, actively using certain strategies to help the smokers quit smoking, facilitating an interdisciplinary approach, consulting other professionals, involving the patients’ significant other when appropriate and proposing PR.
Actively Using Patient Education
Most of the participants emphasized being open to teachable moments for patient education as important for motivating COPD patients’ self-management, eg, when initiating therapy (P6), ordering a chest radiograph (P1), following-up in a slow tempo (P7), and enhancing patients’ insight by showing them their spirometry and other results on the screen (P1,4,9). All participants stressed that smoking abstinence is of great importance for COPD patients and their self-management.
The participants had differing views regarding patient education. Although for them all patients must be informed about their health condition, two wondered whether physicians should invest more time in interpersonal communication (P4,9), while one confessed not rushing to educate patients, as most people know the risk of smoking, but claimed to respond to patients’ questions and provide information as needed (P5). Traditional resources were mentioned, such as offering booklets, written guidelines (P9), recommending physical training and drugs to enhance smoking abstinence (P6,9).
Everyone is ashamed of being a smoker … [However] when they stop smoking, they miss it so much. There is much sorrow. [You must educate them] that there will be difficulties. You will be a bit down for six weeks or so. And inform them that it is possible to help with drugs temporarily and that they need to make major changes to their lifestyle to get over this. (P2)
Enhancing the Patient’s Inner Motivation
All the participants mentioned the importance of enhancing the COPD patients’ motivation for regular physical exercise, staying smoke free, and adhering to medical treatment. Many mentioned the need to get to know the patients to find out their preferences (P2,7) and to urge patients to eliminate as far as possible practical obstacles against exercise, such as cost, long distance, or inconvenient timing (P3,4,9). Some felt they needed to use motivational interviewing (P2), apply unusual approaches to motivate patients, like teasing them (P2), or using the metaphor that if the physician and the patient are to be in the same boat, they must both row in the same direction (P6).
If you find [COPD] in very young people, perhaps near 50 years of age, you’ll strive to guide them towards the healthy path as soon as possible. We can say that people with COPD at a certain level may expect to live 15 years if nothing is done. It involves more constraints if you are 50 than 75. Of course, I would not tell people that they only have limited years left. But I might say that as the lungs are presenting now, they cannot be expected to function for more than 10-15 years, but with good adherence to recommended therapy they might work well for 30 years or more. (P6)
Using Certain Strategies to Help the Smokers Quit Smoking
The participants felt that everything regarding smoking cessation counselling was a complicated balancing act. Although younger patients were less likely to take the risk of smoking seriously (P2), one participant hesitated to use her “strong voice”, not willing to destroy the patients’ good years, although they would perhaps have urgently needed that kind of talk (P7).
All the participants focused on advising their patients to stop smoking. Their strategies to motivate them in this regard included eg, suggesting they book consultations themselves (P1); invest a little time in this; try to deal with each person in the situation he or she is in; making it a little fun and appealing (P9); and introducing the topic of smoking (P2,4,5,7,9). The participants used many other strategies in their endeavors:
Asking them to look inside, speculate what promoted smoking initially and what other than addiction may maintain their current smoking. Ask in what situation they tend to smoke, and if smoking helps in that situation or with other problems in daily life. (P9)
Some participants felt they lacked knowledge of available resources such as smoking cessation (P5,7), or reported patients’ lack of interest in available resources, such as PR and exercise prescription (P3).
One participant mentioned the age of 60 years as a kind of “cut off” age regarding smoking cessation, when the patients start to feel their dyspnea (P2). With higher age, the patients may start feeling and fearing the dyspnea, and some see themselves as being too breathless to endure PR (P8). Some participants emphasized motivating COPD patients’ mastery of the disease:
It is my duty to discuss smoking. In the first 5-10 consults I am very firm, trying to utilize the patient’s motivation while he or she is ill. You may be cruel to talk like that. I show the patients their graphs, their CT scan, and the figures, as they are displayed on my computer. I use that a lot. Having noted that by using this method, the patients realize that they need to master the problem, not me. This promotes a kind of transparency. That’s the way you work with smokers. (P4)
Another physician used the analogy of driving a car to emphasize the COPD patients’ mastery of the disease:
As a driver you are responsible for steering the car, although a teacher is teaching you how to drive. You must drive yourself, no one else takes that from you. (P1)
Some participants emphasized respecting patients’ rights to bad choices regarding smoking:
Non-adherence doesn’t bother me. If people aren’t suffering from dementia, they have the right to decide for themselves. People who have smoked for a long time and still do are, in my opinion, a bit stubborn, and may have certain character traits that make them reluctant to accept advice from others. And that is their right, but of course, if I feel they are at risk I simply make my case clear about that. But all my patients can decide for themselves. However, in the last year or so I haven’t suggested the Smoke-free helpline as much. I don’t know why. [Hesitates] I don’t anymore see so many who are still smoking! I think most people have already stopped smoking, so you don’t rush into scare tactics. Starting to explain what might be ahead, comparing smoking cessation with the disaster that may await if you continue smoking, is more likely to happen if you meet people who are smoking and struggling with cessation. In such a situation that discussion can take place rather early. (P7)
Two participants mentioned that explaining to patients their symptoms on which they can have an impact, provides a motivation, and for some patients the diagnosis [of COPD] may lead to their complete [smoking] cessation and abstinence (P6,8).
I try to enhance the patient’s awareness about underlying anxiety, depression, or loneliness, seeking other solutions than smoking. I may start by asking the patient to look back in time, review things he or she used to like doing as a child or adolescent and might still increase joy and wellness, ask them to write down three favorite things to do before our next appointment. Then I suggest they do more of that. I ask the patient to start this mindful journey and connect with him- or herself. When that has been accomplished, I suggest they start by increasing their positive hobbies, exercise, and companionship with others, and then start cutting down [tobacco]. (P9)
Using an Interdisciplinary Approach
The participants understand that COPD patients often deal with a range of other diseases such as obesity, diabetes, heart disease, advanced age, anxiety, depression, as well as social problems (P2,5,9). Therefore, lifestyle changes are an important coping strategy for COPD patients (P3):
Listening to the patient is all [the physicians’ job], actively listening, to find what they are complaining about. It takes time, lending people your ear, that is your main work. And you try to identify whether it is the heart, the blood or what (P2)
Motivating self-management of patients with complicated disease or comorbidities was perceived by most of the participants as an interdisciplinary effort, such as smoking cessation therapy, physical exercise, and follow-up after hospitalization (P1,3,4,5,7,9). Some participants (GPs) used a referral to lung specialists as a way of conveying to patients the severity of their disease (P2,7,8). Unfortunately, the lung physicians’ specialty seems to be almost a dying profession, as new recruits is scarce (P9). Most often, however, the participants mentioned specialized nurses as important co-workers, like The Outpatient Nursing Clinic, and referred to that team as an outstanding service for those who need more support than just a single consultation (P3,4,5,9). Furthermore, nurses were mentioned as having a special role in spirometry in primary healthcare (P1,3,6,8,9) and enhancing LLT patients’ self-management (P1,4,5,8). The participants also mentioned referral to physical therapists and sports therapists:
I mention exercise to all my patients, and if there is something I have started to believe in through my own life and career, it is the value of exercise.
Participants also mentioned a need to be able to refer to psychologists (P1,3,4,5,7,8,9) but hesitated making it formal:
Perhaps I should make it more formal, like ‘may I refer you to a psychologist’, e.g., to help people to cope with denial. etc.?. (P4)
Most of the participating lung specialists had a clear focus about available inpatient PR and mentioned The Outpatient Nursing Clinic, and Home Physical Therapy (P3,4,6,9). The general practitioners were more likely to mention outpatient PR (P5,7), and most of them were more focused on small physiotherapy centers or public facilities such as swimming pools and outside walking (P1,8).
I think [for COPD patients] it is crucial to have a good, strong relationship with a healthcare professional who is familiar with the disease. It may be a physician, nurse, physical therapist, or a good team, which might be best of all, where the patient is provided with the support that is needed regarding all the factors that can prevent exacerbation of the disease; but first and foremost, increase exercise. (P9)
Involving the Patient’s Significant Other When Appropriate
The participants often referred to themselves as a team with the patient and the patient’s significant other, seeing it as mostly positive that more than one person is listening to explanations, because of memory changes caused by the chronic disease and/or the patients’ more advanced age (P1,2,3,6,7). Suggestions of involving a family member were more common for elderly patients than younger ones and might be considered as offensive and regarded as inappropriate by the younger ones (P2,3,5). Some participants mentioned planning a family meeting when symptoms are evident, rather than smoking dependence alone (P3,7,8,9) and smoking cessation therapy was considered important, promoting a smoke-free home, and finding smoke-free friends to be around (P9):
If a family member has accompanied the patient to a consultation once, it becomes a rule. And as the years go by, I purposely invest in this, talking to couples. Sometimes it is the husband or the wife that is the patient and it may become an important dynamic when you start using it. If this dynamic is positive, it can be a huge opportunity. But if it is not, then it may become a barrier, for which I’m certainly not good at finding solutions to. (P4)
You see. close family members tend to interfere with elderly people, and think they know what’s best for the elderly person, as we do! But the independent group from 20 years of age … generally, don’t invite a close family member to join them in consults. And they may not even have a close family member they feel they can trust with information about their health. A husband or a wife is not necessarily their confidant. (P5)
Usually, in the case of mild disease, I talk to the patient alone, but as the caring burden increases and things become more complicated, maybe more diseases are identified, more exacerbations, more severe illness, I generally include a family member. Whether or not someone else smokes in the home, is a big concern. I know several cases where an inpatient PR went well, and the person managed to stop smoking but resumed smoking when back home again because there were so many smokers in the home. (P9)
Proposing Pulmonary Rehabilitation
Last, but not least, the participants proposed PR to their patients to increase their self-management. It is nice seeing the patients’ advances – how much [PR] means to them and what changes it involves (P8,9). Finding the right time for the COPD patient to engage in PR may, however, be a challenge (9).
Some patients have the mental image that PR isn’t appropriate unless COPD is at end stage. As I have worked in PR myself, I know it may be of best use for those who have still some working energies. People may make the most of PR if they are middle aged, not yet severely ill but working with some effort. However, [at that point in time] they may not have the insight that this is needed. (P3)
Another participant noted that some PR centers demand smoking abstinence which for some patients is very difficult.
Smoking abstinence is terribly difficult for some people and most often those who refuse PR are not ready to stop smoking. That is the most likely explanation. A few times there are other problems, like alcohol consumption or some other substance addiction. Occasionally it is depression. (P9)
Having received interdisciplinary rehabilitation made some patients more easily motivated later for PR (P1,7). More than one felt that reluctance to accept the offer of PR might be caused by domestic responsibilities, being responsible for someone else, work that they cannot or will not take a leave from, unwillingness to give up smoking, being antisocial (P6,9), short of money or stressed (P5) and some women may find it hard to leave their family for PR (P5,9).
Some people are still active on the labor market and don’t make time for PR. But I think if they are offered PR, most of them will accept it gladly, to increase their mobility and exercise, although not all of them manage to stick to lifestyle changes. (P8)
Discussion
The findings indicate that being a principal physician of COPD patients and motivating their self-management is a balancing act that causes challenges, likely to cause strain in the patient-physician partnership (Figure 3). Good medical practice is ethically guided by the oath of Hippocrates, Code of Ethics, and based on exchanged information between the patient and a physician who listens to the patient’s worries, informs the patient, resulting in shared decision making and informed consent.36 According to the oath, the physician is obligated to act promptly regarding any signs of risk or compromise, eg to the patients safety or wellbeing.36 The physician is responsible for keeping up to date with best practice, respecting patients’ will and supporting patients’ self-management36 but a study indicates that clinical guidelines about how to manage exceptions from these obligations are lacking.37 Although many western cultures opt for GPs as a first contact in the healthcare system this simple measure does not in itself guarantee holistic primary care, rather as a state-of-the-art training is needed as well as education to enhance primary care teams’ gatekeeping role.38
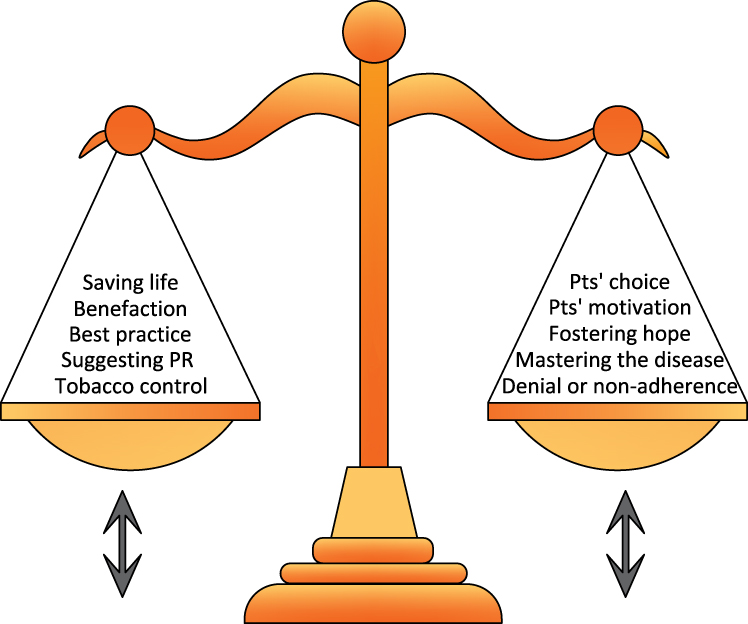 |
Figure 3 Ethical dilemmas in physicians’ consultations with COPD patients. |
Physicians try to respect the patients’ choices, whether health-promoting or not. One of their ethical dilemmas is concerned with helping the patients to deal with COPD as an addiction disease, patients’ denial concerning the harm of smoking, motivating patients’ self-management and mastery of the disease.15 It was interesting to observe a mismatch in participants’ thoughts about the effects of age on patients’ readiness to respond to motivation towards healthy lifestyle changes.
Patients’ nicotine addiction and physicians’ ethical requirements can create various dilemmas for the physician, who must base the selection of treatment on best scientific knowledge and patients’ choices. Listening to patients’ point of view regarding their own health and well-being helps the physician to identify patients’ likelihood of adherence,39 or if the patient’s choice is to reject the recommended therapy. Physicians are expected to provide the patient with necessary information about the disease and prospects, as well as truth-telling which is essential to the physician-patient relationship.40 A physician must preserve patients’ trust and be honest and open-minded.36 However, the patient has the right to know about the diagnosis and the prognosis but he or she also has the right to refuse being informed.40 Sometimes, however, there may be incongruences between the patients’ wishes (eg continued smoking) and their needs (eg smoking cessation).36
The importance of understanding patients’ reluctance to adhere to recommended practice has been stressed,41 and the results of the current study imply that some physicians go to lengths to find out ways to raise patients’ awareness about possible psychological reasons for their smoking addiction. The results indicate that discussing the harm of smoking can be interpreted negatively by some patients, and lead to more focus on symptomatic treatment only instead of smoking cessation support. A physician supports patients’ self-management in improving their health and to enhance interdisciplinary work in a way that best serves the patients’ interests. Findings of a qualitative study suggest GPs’ lack of clinical support within their institutions, to carry out these duties, like time restraints, challenging contacts with specialists, and pressure towards productivity.2 The GOLD clinical guidelines for treatment of COPD recommend providing medical therapy as needed, as well as motivating COPD patients to stop smoking.4 Although the Icelandic Smoking Helpline is a free and user-friendly resource,42 the current study indicates that more effective systemic approaches need to be developed and implemented in Icelandic General practice, PR, and Lung Specialists’ working environment.2 Iceland is ranked as the world second lowest nation regarding smoking prevalence43 which may imply a successful tobacco prevention and smoking cessation support by the Icelandic healthcare and school system.
The participants were aware of some patients’ denying the harm of smoking, clinging to independence and self-determination, and even postponing an urgent need to seek medical consultations, despite being ashamed of being a smoker. The participants’ recommendations were eg to help patients recognizing the relationship between smoking and their illness. As nonadherence to medical regime is quite common, a study reiterates physicians’ duty to identify nonadherence, manage it, and warn about the consequences.39 Physicians’ lack of understanding why patients are reluctant to face their addiction has been identified.44 Our results raise the question if physicians could be more actively motivated towards regarding themselves as responsible for enhancing patients’ smoking cessation. One perspective on physicians’ ethical dilemma regarding health promotion of COPD patients is physician’s perceived ethical duty to take the discussion with their patients about smoking. Most of them also have a clear focus on patient mastery of the disease and patients’ right to make wrong decisions. This focus is noteworthy and may be related to the concepts self-agency and self-mastery, as presented to explain who is perceived in charge of treating a disease,45 and a model on the functional mastery of health as presented in another study.46
How Do Physicians Enhance COPD Patients’ Self-Management?
The current study reflects both GPs’ vital role regarding education and other significant work with patients with early-stage COPD as well as LSs’ worries about lack of formal self-management support for COPD patients. The researchers identified five strategies to motivate COPD patients’ self-management in the principal physicians’ results: special attention on education, self-management motivation, using an interdisciplinary approach, involving significant others as appropriate, and referring patient to PR. Most of the participants emphasized being alert to teachable moments for patients, whether it is when test results are discussed, therapy is initiated or followed-up. This reflects in a way that the medical specialty is currently experiencing a focus revolution, where the art of medicine regarding patient-physician relationship is evolving into a patient-physician partnership in care, where recognizing patients’ coping patterns is of significant importance.47 It might be helpful, as previously suggested, to identify what kind of education would be most effective in each phase of the progressive and exacerbating COPD, early stage, intermediary stage, or advanced stage.28 Our results also imply that GPs express a need for education about available resources for COPD patients. All participants were aware of the importance of patients’ motivation regarding COPD treatment. It was mentioned in connection with exercise, smoking abstinence, and medical treatment adherence. Patient preferences were mentioned and eliminating practical obstacles. According to some of the participants, younger people seem to deny their symptoms, procrastinate contacting the healthcare clinic and be more likely than the elder patients to refuse the advice of smoking cessation, while others found the younger patients more receptive. One participant stressed how valuable motivation it can be to “have a good talk” with the smoking patient to inform him or her that quitting smoking can be a way of relieving the symptoms of COPD. Some patients do not need any more motivation and quit smoking on the spot. All participants mentioned that COPD tends to be complicated by other diseases, which reflects the importance of sound patient-physician relations and, therefore, the methodology of motivational interviewing has gained ground among the participants.48,49
The participants regarded both outpatient and inpatient PR effective in COPD treatment, but some mentioned that accessibility of these resources is lacking. Skillful education and communication regarding goals of care are the main characteristics of interdisciplinary teamwork and a cornerstone of PR, grounded in respect for different cultures and diversity as well as it is based on advanced knowledge of symptom assessment.50 The teamwork orientation of PR and skillful communication regarding goals of care, is useful to motivate patients’ self-management while they are guided towards coping with impairments of COPD.50 Comprehensive PR is based on empowering self-management components like: action plan regarding COPD exacerbations, interactive process providing feedback on actions, and educating about COPD, while also providing a physical activity in a safe environment.51
Some GPs participants do not seem knowledgeable about when to use patients’ rights to be referred to PR which should be one of the first resources according to the GOLD guidelines4 but rather refer COPD patients’ therapy to a poorly staffed profession of lung specialists.
The participants discussed the involvement of a family member in the patient-physician team, as appropriate, and some suggested a family meeting. Family involvement was mentioned more commonly regarding elder patients than younger, and some participants noted that suggesting family involvement might even be regarded negatively by younger patients. A difference has been found regarding the preconditions of enrolment in PR, as some facilities require patients’ smoking abstinence and other do not.52 Furthermore, how physicians would be more actively motivated to refer smoking patients to PR, was also questioned by other researchers.15 Both these questions are worth further investigation.
Conclusions
We conclude that motivating COPD patients’ self-management through the role of being their principal physician is a balancing act, that involves several dilemmas. Of importance there, is patients’ nicotine addiction. Physicians’ ethical obligations may create ethical dilemmas as the physicians’ obligations involve respecting the patients’ will, even though the patients’ will be incompatible with best medical practice. The participants suggest strategies to motivate COPD patients’ self-management.
Funding
The Oddur Olafsson Scientific Research Fund at the Reykjalundur Rehabilitation Institute, and the B-section of the Science Fund of the Icelandic Nurses’ Association funded the study.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Luijks HD, Loeffen MJ, Lagro-Janssen AL, et al. GPs’ considerations in multimorbidity management: a qualitative study. Br J Gen Pract. 2012;62(600):e503–510. doi:10.3399/bjgp12X652373
2. Loeb DF, Bayliss EA, Candrian C, et al. Primary care providers’ experiences caring for complex patients in primary care: a qualitative study. BMC Fam Pract. 2016;17:34. doi:10.1186/s12875-016-0433-z
3. Morrison D, Agur K, Mercer S, et al. Managing multimorbidity in primary care in patients with chronic respiratory conditions. NPJ Prim Care Resp M. 2016;26:16043. doi:10.1038/npjpcrm.2016.43
4. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
5. Gudmundsson G. [Acute exacerbations of chronic obstructive pulmonary disease - review]. Laeknabladid. 2015;101(7–8):357–362. Icelandic.
6. Rigotti NA. Pharmacotherapy for smoking cessation in adults: summary and recommendations. Available from: https://www.uptodate.com/contents/pharmacotherapy-for-smoking-cessation-in-adults#H13314646. 2021.
7. Baker TB, Breslau N, Covey L, et al. DSM criteria for tobacco use disorder and tobacco withdrawal: a critique and proposed revisions for DSM-5. Addiction. 2012;107:263–275. doi:10.1111/j.1360-0443.2011.03657.x
8. Miller WR, Rollnick S. Motivational Interviewing: preparing People to Change Addictive Behavior. New York: Guilford; 1993.
9. Keijsers GPJ, Schaap CPDR, CAL H. The impact of interpersonal patient and therapist behavior on outcome in cognitive-behavior therapy. A review of empirical studies. Behav Modif. 2000;24(2):264–297. doi:10.1177/0145445500242006
10. Ziedonis D, Zammarelli L, Seward G, et al. Addressing tobacco use through organizational change: a case study of an addiction treatment organization. J Psychoactive Drugs. 2007;39(4):451–459. doi:10.1080/02791072.2007.10399884
11. Drieschner K, Lammers S, Van der Staak C. Treatment motivation: an attempt for clarification of an ambiguous concept. Clin Psychol Rev. 2004;23(8):1115–1137. doi:10.1016/j.cpr.2003.09.003
12. Schunk D. Coming to terms with motivation constructs. Contemp Educ Psychol. 2000;25(1):116–119. doi:10.1006/ceps.1999.1018
13. Effing TW, Vercoulen JH, Bourbeau J, et al. Definition of a COPD self-management intervention: international expert group consensus. Eur Respir J. 2016;48:46–54. doi:10.1183/13993003.00025-2016
14. Linnell JHJ, Hurst JR. COPD exacerbations: a patient and physician‘s perspective. Adv Ther. 2020;37:10–16. doi:10.1007/s12325-019-01138-7
15. van Eerd EAM, Bech Risor M, Spigt M, et al. Why do physicians lack engagement with smoking cessation treatment in their COPD patients? A multinational qualitative study. NPJ Prim Care Respir Med. 2017;27(1):41. doi:10.1038/s41533-017-0038-6
16. Bodenheimer T, Chen E, Bennett HD. Confronting the growing burden of chronic disease: can the U.S. health care workforce do the job? Health Aff. 2009;28(1):64–74. doi:10.1377/hlthaff.28.1.64
17. Ryrso CK, Godtfredsen NS, Kofod LM, et al. Lower mortality after early supervised pulmonary rehabilitation following COPD-exacerbations: a systematic review and meta-analysis. BMC Pulm Med. 2018;18(1):154. doi:10.1186/s12890-018-0718-1
18. Jonkman NH, Westland H, Trappenburg JC, et al. Characteristics of effective self-management interventions in patients with COPD: individual patient data meta-analysis. Eur Respir J. 2016;48(1):55–68. doi:10.1183/13993003.01860-2015
19. Jordan R, Majothi S, Heneghan N, et al. Supported self-management for patients with moderate to severe chronic obstructive pulmonary disease (COPD): an evidence synthesis and economic analysis. Health Technol Assess. 2015;19:1–515.
20. Halldorsdottir S. Eflandi og niðurbrjótandi samskiptahættir og samfélög [Empowering and disempowering modes of communication and communities]. Icelandic Nurs J. 2003;79:6–12. Icelandic.
21. Lee CT, Doran DM. The role of interpersonal relations in healthcare team communication and patient safety: a proposed model of interpersonal process in teamwork. Can J Nurs Res. 2017;49(2):75–93. doi:10.1177/0844562117699349
22. Bourbeau J, Bartlett SJ. Patient adherence in COPD. Thorax. 2008;63(9):831–838. doi:10.1136/thx.2007.086041
23. Molin KR, Egerod I, Valentiner LS, et al. General practitioners’ perceptions of COPD treatment: thematic analysis of qualitative interviews. Int J Chronic Obstr Pulmon Dis. 2016;11:1929–1937.
24. Yohannes A. General practitioners views and experiences in managing depression in patients with chronic obstructive pulmonary disease. Expert Rev Respir Med. 2012;6(6):589–595. doi:10.1586/ers.12.64
25. World Health Organaization. WHO Global Report on Trends in Prevalence of Tobacco Use 2000–2025.
26. Hillas G, Perlikos F, Tsiligianni J,et al. Managing comorbidities in COPD. Int J Chronic Obstruct Pulmon Dis. 2015;10:95–109.
27. Sigurgeirsdottir J, Halldorsdottir S, Arnardottir RH, et al. COPD patients’ experiences, self-reported needs, and needs-driven strategies to cope with self-management. Int J Chronic Obstruct Pulmon Dis. 2019;14:1033–1043.
28. Sigurgeirsdottir J, Halldorsdottir S, Arnardottir RH, et al. Frustrated caring: family members’ experience of motivating COPD patients towards self-management. Int J Chronic Obstruct Pulmon Dis.2020;15:2953–2965.
29. Bourbeau J. Clinical decision processes and patient engagement in self-management. Dis Manag Health Out. 2008;16(5):327–383. doi:10.2165/0115677-200816050-00009
30. O´Brien R, Wyke S, Guthrie B, et al. An ‘endless struggle’: a qualitative study of general practitioners’ and practice nurses’ experiences of managing multimorbidity in socio-economically deprived areas of Scotland. Chronic Illn. 2011;7:45–59. doi:10.1177/1742395310382461
31. Spiegelberg H. The Phenomenological Movement: A Historical Introduction by Herbert Spiegelberg.
32. Ricoeur P. Existence and Hermeneutics. (translated by K. McLaughlin). In: McLaughlin K, Bleicher J, editors. Contemporary Hermeneutics: Hermeneutics as Method, Philosophy and Critique. London: Routledge & Kegan Paul;1980.
33. Ricoeur P. Hermeneutics and the Human Sciences. Essays on Language, Action and Interpretation. Cambridge: Cambridge University Press; 1990.
34. Schwandt T. Constructivist, interpretivist approaches to human inquiry. In: Denzin N, Lincoln Y, editors. Handbook of Qualitative Research. Thousand Oaks CA: Sage; 1994.
35. Halldorsdottir S. The Vancouver school of doing phenomenology. In: Fridlund B, Hildingh C, editors. Qualitative Research Methods in the Service of Health. Lund: Studentlitteratur; 2000:47–81.
36. General Medical Council. Good medical practice Available from: https://www.gmc-uk.org/ethical-guidance/ethical-guidance-for-doctors/good-medical-practice.
37. Wendler D. Are physicians obligated always to act in the patient’s best interests? J Med Ethics. 2010;36:66–70. doi:10.1136/jme.2009.033001
38. Hoffmann K, George A, Van Loenen T, et al. The influence of general practitioners on access points to health care in a system without gatekeeping: a cross-sectional study in the context of the QUALICOPC project in Austria. Croat Med J. 2019;60(4):316–324. doi:10.3325/cmj.2019.60.316
39. Jakobson J. The effect of patients’ noncompliance on their surgeons’ obligations. Surg Clin North Am. 2007;87:937–948. doi:10.1016/j.suc.2007.07.014
40. Varkey B. Principles of clinical ethics and their application to practice. Med Prin Pract. 2021;30(1):17–28.
41. Wai Yin L, Fresco P. Medication adherence measures: an overview. BioMed Res Int. 2015;2015. doi:10.1155/2015/217047
42. Icelandic Directorate of Health. Reyklaus.is [smokefree helpline]. Available from: http://www.reyklaus.is/opptur/dispatcher?marketplaceId=989008&languageId=2&siteNodeId=989177.
43. OECD. Daily smokers. Available from: https://data.oecd.org/healthrisk/daily-smokers.htm.
44. Caponnetto P, Polosa R. Common predictors of smoking cessation in clinical practice. Respir Med. 2008;102:1182–1192. doi:10.1016/j.rmed.2008.02.017
45. Arzy S, Schacter D. Self-agency and self-ownership in cognitive mapping. Trends Cogn Sci. 2019;23(6):476–487. doi:10.1016/j.tics.2019.04.003
46. Donnelly M. Functional mastery of health ownership: a model for optimum health. Nurs Forum. 2018;53(2):117–121. doi:10.1111/nuf.12223
47. Stoilkova-Hartmann A, Franssen FME, Augustin IML, et al. COPD patient education and support – achieving patient-centredness. Patient Educ Couns. 2018;101(11):2031–2036. doi:10.1016/j.pec.2018.05.024
48. Miller WR, Rollnick S. Meeting in the middle: motivational interviewing and self-determination theory. Int J Behav Nutr Phy. 2012;9:25. doi:10.1186/1479-5868-9-25
49. Cottrell E, Yardley S. Lived experiences of multimorbidity: an interpretative meta-synthesis of patients’, general practitioners’ and trainees’ perceptions. Chronic Illn. 2015;11(4):279–303. doi:10.1177/1742395315574764
50. Janssen DJ, Engelberg RA, Wouters EF, Curtis JR. Advance care planning for patients with COPD: past, present and future. Patient Educ Couns. 2012;86(1):19–24. doi:10.1016/j.pec.2011.01.007
51. Lenferink A, Brusse-Kaiser M, van der Valk P, et al. Self-management interventions including action plans for exacerbations versus usual care in patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;8:CD011682.
52. Jonsdottir H, Ingadottir TS. Reluctance of patients with chronic obstructive pulmonary disease in its early stages and their families to participate in a partnership-based self-management trial: a search for explanation. Chron Respir Dis. 2018;15(3):315–322. doi:10.1177/1479972317743758
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.