")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Estimating the Health and Economic Impact of Improved Management in Prevalent Chronic Obstructive Pulmonary Disease Populations in England, Germany, Canada, and Japan: A Modelling Study
Authors Adams EJ , van Doornewaard A, Ma Y , Ahmed N, Cheng MK , Watz H, Ichinose M, Wilkinson T, Bhutani M, Licskai CJ, Turner KME
Received 13 April 2023
Accepted for publication 17 September 2023
Published 27 September 2023 Volume 2023:18 Pages 2127—2146
DOI https://doi.org/10.2147/COPD.S416988
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Min Zhang
Elisabeth J Adams,1 Alexander van Doornewaard,1 Yixuan Ma,1 Nurilign Ahmed,1 Man Ki Cheng,1 Henrik Watz,2 Masakazu Ichinose,3 Tom Wilkinson,4 Mohit Bhutani,5 Christopher J Licskai,6– 8 Katy M E Turner1
1Aquarius Population Health, London, UK; 2Pulmonary Research Institute at Lungen Clinic Grosshansdorf, Airway Research Center North (ARCN), German Center for Lung Research (DZL), Grosshansdorf, Germany; 3Academic Center of Osaki Citizen Hospital, Osaki, Japan; 4Southampton University Faculty of Medicine, Southampton, UK; 5University of Alberta, Edmonton, Alberta, Canada; 6London Health Sciences Centre, Western University, London, Ontario, Canada; 7Lawson Health Research Institute, London, Ontario, Canada; 8Asthma Research Group Windsor Essex County Inc., Windsor, Ontario, Canada
Correspondence: Elisabeth J Adams, Aquarius Population Health, Unit 29 Tileyard Studios, London, N7 9AH, UK, Tel +44 207 993 2930, Email [email protected]
Introduction: COPD is a leading cause of morbidity and mortality globally. Management is complex and costly. Although international quality standards for diagnosis and management exist, opportunities remain to improve outcomes, especially in reducing avoidable hospitalisations.
Objective: To estimate the potential health and economic impact of improved adherence to guideline-recommended care for prevalent, on-treatment COPD populations in four high-income settings.
Methods: A disease simulation model was developed to evaluate the impact of theoretical improvements to COPD management, comparing outcomes for usual care and policy scenarios for interventions that reduce avoidable hospitalisations: 1) increased attendance (50% vs 31– 38%) of early follow-up review after severe exacerbation hospitalisation; 2) increased access (30% vs 5– 10%) to an integrated disease management (IDM) programme that provides guideline adherent care.
Results: For cohorts of 100,000 patients, Policy 1 yielded additional life years (England: 523; Germany: 759; Canada: 1316; Japan: 512) and lifetime cost savings (-£ 2.89 million; -€ 6.58 million; -$40.08 million; -¥ 735.58 million). For Policy 2, additional life years (2299; 3619; 3656) and higher lifetime total costs (£ 38.15 million; € 35.58 million; ¥ 1091.53 million) were estimated in England, Germany and Japan, and additional life years (4299) and cost savings (-$20.52 million) in Canada. Scenarios found that the cost impact depended on the modelled intervention effect size.
Conclusion: Interventions that reduce avoidable hospitalisations are estimated to improve survival and may generate cost savings. This study provides evidence on the theoretical impact of policies to improve COPD care and highlights priority areas for further research to support evidence-based policy decisions.
Keywords: health intervention, exacerbations, re-admission, integrated care, economic evaluation
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive respiratory disorder characterised by irreversible airflow limitation and symptoms including dyspnoea, persistent cough, and sputum production. Exacerbation of symptoms is common and occurs more frequently as the disease progresses.1,2 Severe exacerbations are the primary cause of hospitalisation, and re-admission following discharge is common.3,4
In 2019, COPD was the third leading cause of death worldwide, responsible for 3.23 million deaths.5 The global cost of illness was estimated to be US$2.1 trillion in 2010 and is expected to more than double by 2030.6 Hospitalisations and re-admissions are primary drivers of healthcare system costs, and their frequency is highly influenced by exacerbation frequency and severity.7,8
According to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) case definition (a fixed ratio value of forced expiratory volume in one second (FEV1) to forced vital capacity (FVC): FEV1/FVC<0.7).,9 the global prevalence of COPD was estimated at 10.3% (392 million cases, ages 30–79) in 2019.10 Prevalence is higher in men, urban areas and high-income countries.11
Currently, no curative treatments exist for COPD. However, effective symptom management and slower disease progression can be achieved through pharmacological and non-pharmacological interventions.12 GOLD describes international recommendations for the optimal diagnosis and management of COPD,9 and many countries publish national guidelines to support best practices.13–17 Despite this, challenges remain in delivering optimal care to patients. A recent study in high-income settings reported common barriers to include low consideration of COPD, underutilisation of effective pharmacological and non-pharmacological interventions, and sub-optimal management of exacerbations.18
Improvements in care for people with COPD are expected to reduce hospitalisations, improve patient outcomes, and increase life expectancy.17,19,20 Interventions to identify undiagnosed patients, such as active case finding, improve patient outcomes and are cost-effective.21–23 However, evidence on the health and economic benefit of interventions that provide optimal management in line with best practices is more limited.24
Early follow-up review post-discharge (within one month) is recommended in international guidelines9 and quality standards19 for patients hospitalised due to severe exacerbation and can reduce re-admission risk.25 Despite this, uptake is low;26,27 not attending early follow-up represents a missed opportunity to review and amend discharge therapy and may contribute to re-admissions and poor survival.9
Integrated disease management (IDM) programmes provide structured, multidisciplinary care and address the complex nature of managing COPD.28 Administered by teams in both primary and secondary care settings, these programmes vary in composition. They often include pharmacological and non-pharmacological interventions (eg, treatment review, smoking cessation counselling, telemonitoring, etc.). Pulmonary rehabilitation is a well-known form of IDM; the organisation of two primary care programmes from Canada29,30 and Germany31 is detailed in Table S1. A recent meta-analysis of 52 studies found improvements in disease-specific quality of life, exercise capacity and respiratory-related hospital admissions for patients with IDM.28 Despite this evidence of effectiveness, access and uptake remain limited.31
This study evaluates the potential health and economic impact of two policy scenarios to improve the management of prevalent, on-treatment COPD populations in England, Germany, Canada, and Japan, through interventions that align with recommendations in international quality standards on management.19 The interventions were 1) early follow-up review after severe exacerbation hospitalisation and 2) provision of IDM to optimise COPD care.
Methods
Model Overview
A discrete-time cohort-level Markov state-transition model was developed to simulate the natural disease history for COPD. Consistent with prior models,21,32,33 health states were based on GOLD airflow obstruction stages (GOLD I–IV).9 While the GOLD ABE (ABCD pre-2023) clinical risk classifications are central to individualised therapeutic decision-making, spirometry remains a key prognostic measure for COPD, and the airflow obstruction stages are preferred for population-level modelling. Death was included as an absorbing state.
A lifetime horizon was assumed, and the cycle length was three months; a half-cycle correction was applied. In each cycle, simulated individuals either remain in their current GOLD stage, improve and move to the previous stage, or worsen and progress to the next stage while lung function typically declines over time, some improvements to earlier stages were observed in the source data and included in the disease progression model parameters.21,34 Simulated individuals are also subject to risks of severe exacerbation hospitalisation, subsequent re-admission, and death. Deaths were determined by background COPD and in-hospital mortality. Severe exacerbation and background COPD mortality event risks were conditional upon GOLD stage.
The model predicts total life years, severe exacerbation hospitalisations (including re-admissions), in-hospital deaths, and lifetime costs for defined cohorts of patients. Modelled costs include inhaled medication, background disease management, hospitalisation, and intervention (ie, early follow-up review and IDM administration) costs.
Figure 1 presents an overview of the model structure. The model was implemented in TreeAgePro 2021 (TreeAgePro Software, Williamstown, Massachusetts, USA).35
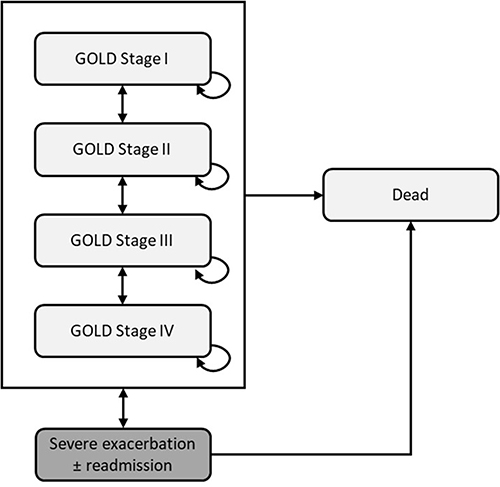 |
Figure 1 Schematic diagram of the model structure. Abbreviation: GOLD, Global Initiative for Chronic Obstructive Lung Disease. |
Inputs
The model was parameterised using published evidence on usual care (UC) for prevalent COPD populations in each country (Table 1). Data were obtained from population studies, prior modelling studies, national-level audits, and cost databases. Disease progression and severe exacerbation risk profiles were representative of single long-acting muscarinic antagonist (LAMA) therapy. All patients were assumed to be on-treatment. Intervention effects were based on the findings of retrospective population-based studies25,36 for early follow-up review and randomised controlled trials (RCTs)28,29 for IDM. A healthcare payer perspective was assumed. Costs reflect 2021/2022 prices. Future costs and benefits were discounted at country-specific rates: England, 3.5%; Germany, 3%; Canada, 1.5%; and Japan, 2%.
 |
Table 1 Input Parameters Applied in the Model |
Further detail on the input sources and employed assumptions is provided in Supplemental S1.
Primary Analyses
Considerable gaps and uncertainty exist in the evidence on UC in each country and the intervention effect sizes. To assess the potential impact of improvements in care, primary analyses employed the most robust intervention effect evidence and assumed realistic uptake targets for the policy scenarios.
Early Follow-Up Review - Policy 1
- Intervention effect: the 90-day odds of re-admission were 66% (odds ratio [OR]: 0.34)25 lower for patients attending early follow-up review within one month of severe exacerbation hospitalisation.
- Policy impact: assumed at 50%, the percentage of patients attending early follow-up review was increased for the policy. UC attendance levels ranged from 31.1–37.8% across settings.26,53
IDM - Policy 2
- Intervention effect: patients receiving IDM were at reduced odds (36% lower; OR: 0.6428) of severe exacerbation hospitalisation across the modelled time horizon.
- Policy impact: the percentage of patients receiving lifelong management with IDM was assumed to be 30% in the policy, while UC levels were 5–10% across settings (Table 2).
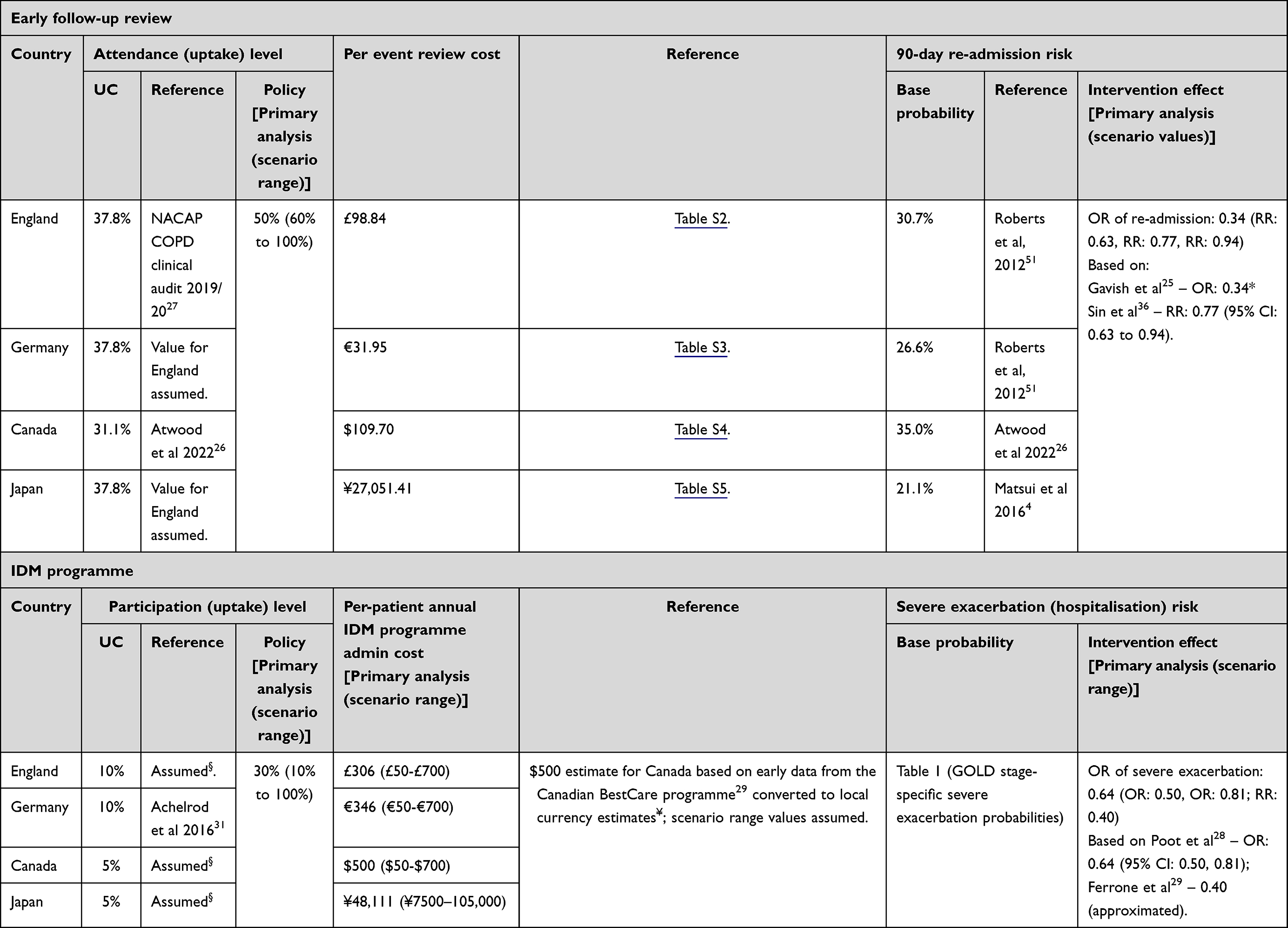 |
Table 2 Overview of Usual Care and Policy Scenario Intervention Implementations |
Early follow-up review intervention costs reflected healthcare provider interactions for local practice (Tables S2–S5), while annual IDM administration costs were assumed to be £306, €346, $500, and ¥48,111. Intervention costs do not include additional costs due to treatment regimen changes, other non-pharmacological interventions, or other resource use.
Further information on the intervention effect data sources and assumptions made is provided in Supplemental S2. The impact of the policies was defined by differences in life years, severe exacerbation hospitalisations, in-hospital deaths, and total costs from UC.
Scenario and Uncertainty Analyses
Given considerable uncertainty in several key inputs and assumptions due to limited data, extensive scenario analyses were conducted to assess the impact for a range of intervention effect sizes and uptake levels and at alternative IDM administration costs (Table 2). One-way sensitivity analysis was conducted for all other key parameters.
Ethics approval was not required as no patient-specific information was used in this study.
Results
Primary Analyses
Table 3 presents discounted, primary analysis results for cohorts of 100,000 patients.
 |
Table 3 Cohort-Level (n=100,000) Discounted Primary Analysis Results by Country and Policy |
Policy 1
Increasing attendance of early follow-up review to 50% (from 37.8% in England, Germany and Japan, and 31.1% in Canada) resulted in fewer severe exacerbation hospitalisations (England: 1894; Germany: 3354; Canada: 5528; Japan: 1911) and fewer in-hospital deaths (England: 96; Germany: 127; Canada: 210; Japan: 97). Life year gains were predicted for all countries, ranging from 512 in Japan to 1316 in Canada.
While the costs of inhaled medication, background disease management, and early follow-up review were higher for the policy, hospitalisation costs were notably lower and the policy generated lifetime cost savings of £2.89 million, €6.58 million, $40.08 million, and ¥735.58 million.
Policy 2
Increasing IDM access to 30% (from 10% in England and Germany; from 5% in Canada and Japan) yielded fewer severe exacerbation hospitalisations (England: 8516; Germany: 16,153; Canada: 18,290; Japan: 14,412) and in-hospital deaths (England: 425; Germany: 613; Canada: 695; Japan: 735).
While this reduced hospitalisation-related costs, inhaled medication, background disease management, and IDM administration costs were higher for the policy, and the overall cost impact varied by country. In England, Germany, and Japan, the policy was estimated to generate additional life years (2299; 3619; 3656) at higher total lifetime costs (£38.15 million; €35.58 million; ¥1091.53 million), while in Canada, the policy generated 4299 additional life years at cost savings of $20.52 million.
Scenario and Uncertainty Analyses
Figures 2–5 show incremental differences between UC and the policies for different intervention effect sizes and uptake levels. As expected, for both policies, the number of hospitalisations avoided and life years gained increased with greater effect sizes and higher uptake levels. Estimated benefits were larger for Policy 2 than Policy 1, in all countries. The cost impact varied with the effect size. Policy 1 was cost-saving for implementations where the intervention effect corresponded to a ≥23% reduction in the risk (odds/ probability) of re-admission in England and Japan; in Germany and Canada, the policy was cost-saving for all effect sizes. For Policy 2, cost savings were predicted for implementations where the intervention effect corresponded to a ≥36% reduction in severe exacerbation risk in Canada and a ≥50% reduction in Japan. The policy was associated with higher total costs for all effect sizes in England and Germany.
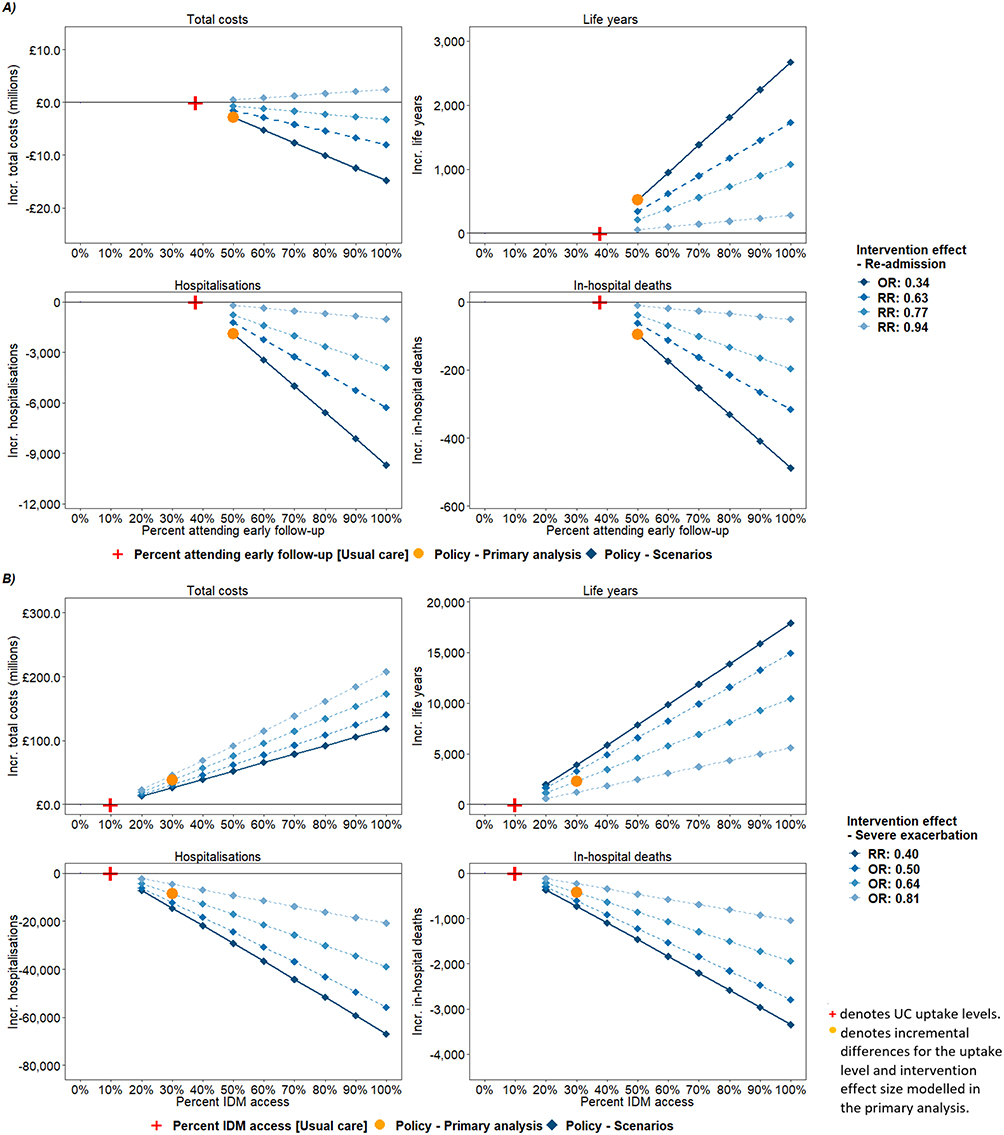 |
Figure 2 Cohort-level (n=100,000) incremental policy intervention scenario results by outcome - England. (A) Policy 1 - Early follow-up review: Values represent incremental differences between the policy intervention scenario and UC for the range of considered policy uptake levels and intervention effect sizes. (B) Policy 2 - IDM: Per A. Abbreviations: IDM, integrated disease management; Incr, incremental (Policy - UC); OR, Odds ratio; RR, relative risk. |
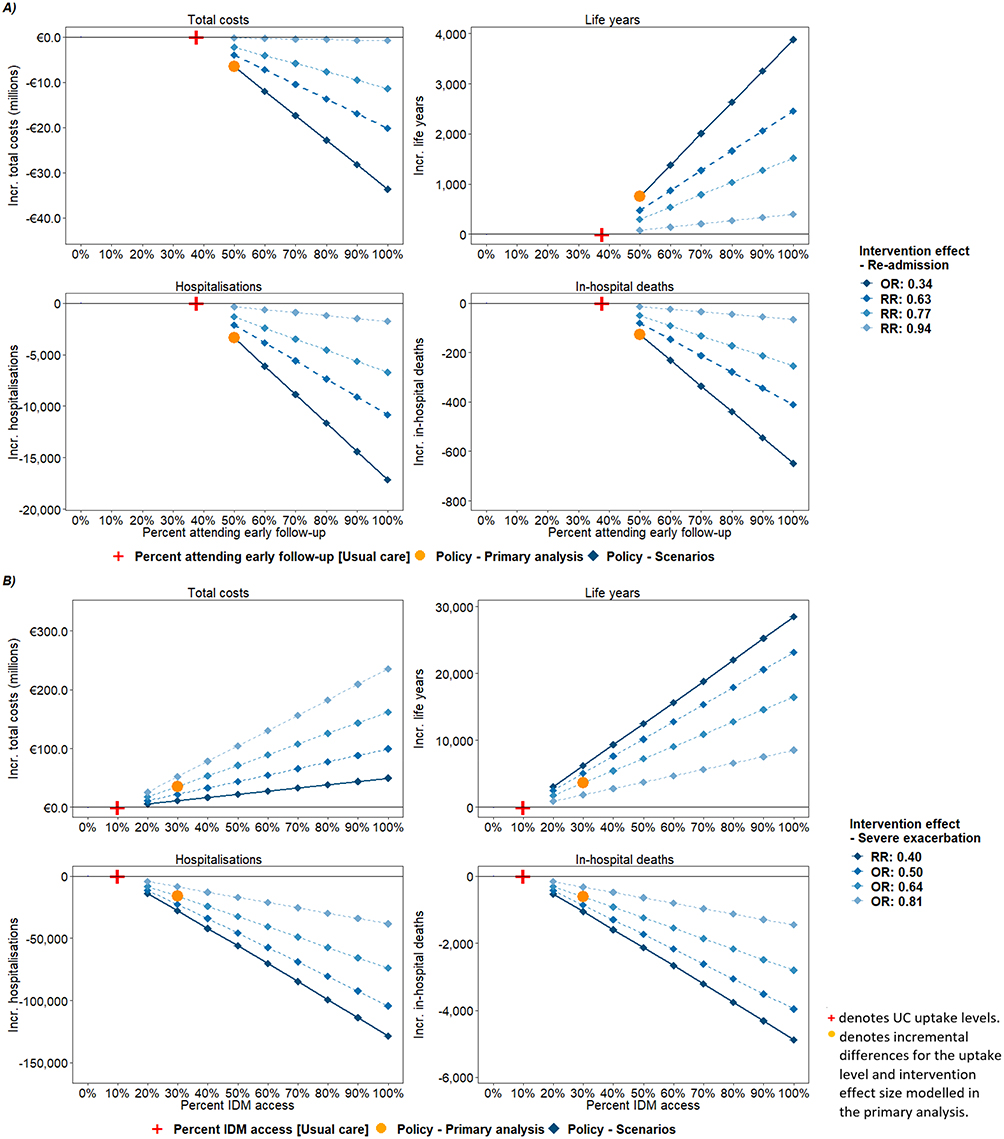 |
Figure 3 Cohort-level (n=100,000) incremental policy intervention scenario results by outcome - Germany. (A) Policy 1 - Early follow-up review: Values represent incremental differences between the policy intervention scenario and UC for the range of considered policy uptake levels and intervention effect sizes. (B) Policy 2 - IDM: Per A. Abbreviations: IDM, integrated disease management; Incr, incremental (Policy - UC); OR, Odds ratio; RR, relative risk. |
 |
Figure 4 Cohort-level (n=100,000) incremental policy intervention scenario results by outcome - Canada. (A) Policy 1 - Early follow-up review: Values represent incremental differences between the policy intervention scenario and UC for the range of considered policy uptake levels and intervention effect sizes. (B) Policy 2 - IDM: Per A. Abbreviations: IDM, integrated disease management; Incr, incremental (Policy - UC); OR, Odds ratio; RR, relative risk. |
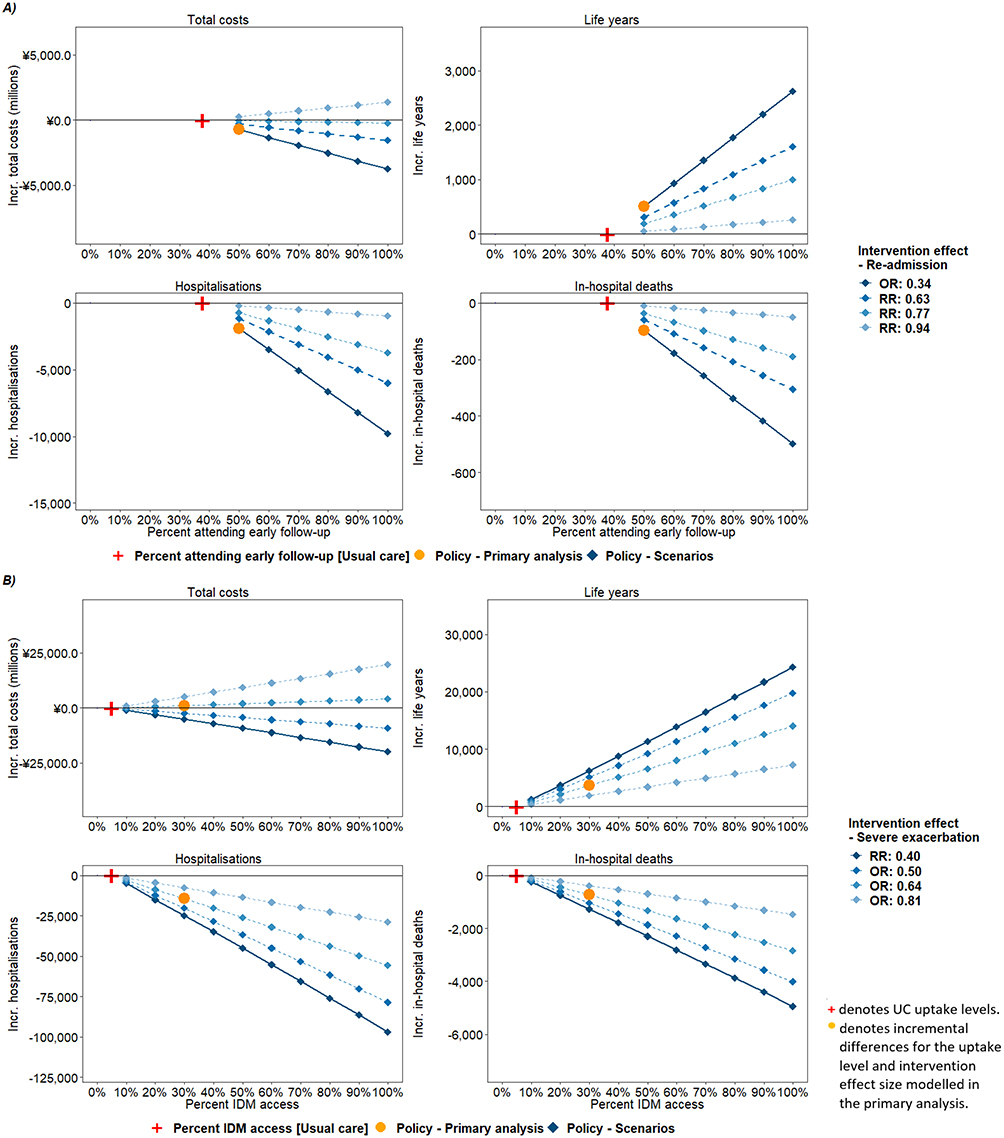 |
Figure 5 Cohort-level (n=100,000) incremental policy intervention scenario results by outcome - Japan. (A) Policy 1 - Early follow-up review: Values represent incremental differences between the policy intervention scenario and UC for the range of considered policy uptake levels and intervention effect sizes. (B) Policy 2 - IDM: Per A. Abbreviations: IDM, integrated disease management; Incr, incremental (Policy - UC); OR, Odds ratio; RR, relative risk. |
Table 4 shows the impact for alternative IDM administration cost levels. The policy was cost-neutral (ie, total policy costs equivalent to UC) at annual, per-patient administration costs of £95, €170, $584, and ¥42,681, under primary analysis intervention effect sizes and uptake levels.
 |
Table 4 Cohort-Level (n=100,000) Incremental Cost Estimates for IDM Programme Administration Cost Scenarios |
Figures S1–S8 present tornado plots of incremental outcomes for one-way sensitivity analyses. As expected, parameters related to severe exacerbations, including severe exacerbation costs and event probabilities, and in-hospital mortality probabilities, were influential; results were also sensitive to variations in baseline age and cost and benefit discount rates. Notably, in some cases (Japan and Canada, Policy 2), the cost impact of the policy depended on the severe exacerbation cost level.
Discussion
Main Findings
This modelling study suggests a significant opportunity to realise health gains and potentially generate cost savings through better management of prevalent, on-treatment COPD populations, via increased uptake of two evidence-based interventions, in England, Germany, Canada and Japan. These findings are likely generalisable to other high-income settings.
While increased attendance of early follow-up review after severe exacerbation hospitalisation (Policy 1) and increased access to IDM (Policy 2) are both predicted to reduce hospitalisations and improve survival, results suggest Policy 2 has a larger potential for impact. This highlights the importance of sustained, multidisciplinary care to prevent avoidable exacerbations and improve patient outcomes; all patients may achieve the benefits of IDM while the potential of early follow-up review is limited to patients experiencing severe exacerbation.
Policy 1, however, is likely of value to both patients and payers, with improved outcomes predicted at reduced total costs for a wide range of intervention effect sizes and across settings. This contrasts with Policy 2 where benefits come with higher total costs, except where cost savings were predicted in Canada and Japan under certain effect sizes. Sensitivity analyses found the cost impact for Policy 2 depended on the severe exacerbation cost level at primary analysis effect sizes in Canada and Japan. The cost impact at a given effect size depends on the underlying cost of COPD management, including during additional years of life, and the cost of the intervention, and the finding of directional variations across and within countries, coupled with the absence of evidence for key parameters, highlights the need for further study to verify our findings.
Findings in the Context of Existing Literature
Early follow-up review after severe exacerbation hospitalisation has been shown to reduce re-admission rates25,36 and mortality risks.55 However, no prior studies have evaluated the value of improved attendance of early follow-up review in terms of health outcomes and costs.
Literature on the cost and effectiveness of IDM is mixed. Short-term studies in Italy56 (2 years) and Poland57 (six months) found that IDM reduced hospitalisations and was cost-effective. Assessing outcomes over three years, a large study of the German IDM programme found participants had reduced mortality risk (hazard ratio: 0.89, 95% confidence interval [CI]: 0.84–0.94) and higher total costs (€553 per year).31 IDM can improve quality of life;28–30 a recent cost-effectiveness analysis of IDM in Canadian primary care by Scarffe et al, found the programme dominated UC, with cost savings and higher quality-adjusted life years (QALYs) in the short- (1-year; within-trial) and long-term (30-years; model-based analysis).58 Approximating the effect on severe exacerbation from the same RCT,29 corresponding analyses from our study (Canada, Policy 2; RR: 0.40) corroborate this finding of improved health outcomes and cost savings and provide additional evidence on the impact at alternative uptake levels.
Notably, Scarffe et al, reported IDM to generate incremental lifetime QALYs (1.732) greater than incremental life years (0.244).58 Our study did not evaluate QALYs. However, considering incremental cost-per-life year estimates from the primary analyses (England: £16,594; Germany: €9832; Japan: ¥298,560) and cost-per-QALY willingness-to-pay thresholds of £20,000,37 €20,000, and ¥5,000,000, the policy is likely also cost-effective in these settings. There are no formal willingness-to-pay threshold exists in Germany or Japan, so the currency equivalent cost-per-QALY threshold for England has been assumed.59
Differences in findings across studies are likely due to variations in the composition of IDM and UC, evaluation follow-up time,28 as well as measured outcomes and patient and provider factors.60 IDM typically yields health benefits, mainly due to reduced exacerbation frequency, but the cost impact varies across settings. This is consistent with findings across the four countries in our study.
Strengths
The policies were selected to align with the international consensus statement on COPD management and designed to be feasible to implement in the study countries, ie based on improving existing management and reducing the variability of care.19 Modelled intervention effects were based on the best available evidence, including data from a contemporary meta-analysis of 52 RCTs for IDM.28 In practice, the interventions may be implemented differently according to local health services provisions and their costs and effect sizes vary accordingly. In addition, the achievable uptake will depend on the design of the associated policies, which may vary based on local-level infrastructure and existing care processes as well as budgetary considerations. Broad applicability of the findings was ensured through scenario analyses considering an extensive range of intervention effect sizes, uptake levels, and IDM administration costs.
Limitations
The management of COPD is highly complex and the care provision varies both on an individual basis and by setting. Capturing these intricacies and differences in outcomes between countries presents challenges. Where possible, country-specific data were used for UC profiles, and the impact of evaluated interventions was informed by published evidence. However, relevant data were lacking for many parameters, and differences exist in how studies measured outcomes or interventions. Combining this evidence robustly presented challenges requiring assumptions. The model framework makes these explicit, and sensitivity analyses highlight priority areas where further data on COPD care is needed.
The achievable impact of the policies may differ in practice in several ways. 1) Exacerbation history and symptom severity are core components of the GOLD ABE clinical assessment tool and key for therapeutic decision-making.9 Based on these factors, both interventions may result in treatment changes (likely escalation), which were not modelled. Therefore, treatment costs may increase alongside slower disease progression rates and improved health outcomes. 2) Only the effect of IDM on severe exacerbations was modelled. IDM could beneficially impact disease progression, but limited data were available to inform this. Whilst our model captures the indirect effect of reductions in severe exacerbations on mortality, capturing the broader effects could yield more optimistic outcomes. 3) Studies of IDM report short-term (3–36 months) effects. Our model extrapolated these to a lifetime horizon, which may overestimate benefits in the case of waning. 4) The effects of IDM and early follow-up review were assumed to apply equally across patients, GOLD stages, and settings. In practice, not all patients may benefit equally from or be able to access these interventions; the effect may vary by disease stage and setting, and the benefits be greater for high-risk populations. Barriers such as distance from care may also limit the achievable impact.9,25 However, this is a reasonable simplifying assumption for a population-level model, and a range of uptake and effect size scenarios were evaluated.
Policy Implications and Future Research
While the socio-economic burden of COPD is well established, the impact of policies that improve its management is less so. This study provides policymakers with evidence on the potential health and economic impact of improved COPD care in different healthcare settings by quantifying the potential value of policy scenarios to prevent and better manage severe exacerbations. Additionally, in making explicit the notable evidence gaps, priority areas for further research to support evidence-based policy decisions are highlighted.
Additional country-specific data on current and guideline-recommended care should be collected to support more robust assessment of the chosen interventions and to validate the impact shown in this study. Future studies could evaluate treatment-regimen changes due to early follow-up review and IDM, the impact on mild to moderate exacerbations which may also influence patients’ disease trajectory,61 and the impact in high-risk populations (eg, smokers). With prevalence estimates ranging from 5.1% to 13.5% for 40- to 64-year-olds high-income country prevalence is based on the GOLD case definition,10 many COPD patients are of working age and the economic impact on patients and governments may be considerable.9,62,63 Future studies could also assess the impact of improved outcomes on productivity losses ie, societal costs.
Conclusion
Preventing severe exacerbations is key to improving patient outcomes in COPD, and reductions in related hospitalisations will support healthcare system resilience and sustainability. This study provides evidence that suggests improved adherence to early follow-up review post severe exacerbation hospitalisation (Policy 1) and increased access to IDM (Policy 2) can positively impact patient outcomes, reduce hospitalisations, and may generate cost savings across four high-income countries while highlighting priority areas for further research to support evidence-based policy decisions.
Abbreviations
CI, Confidence interval, COPD, Chronic Obstructive Pulmonary Disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; IDM, Integrated Disease Management; LAMA, Long-acting muscarinic antagonist; OR, Odds ratio; QALY, Quality-adjusted life year; RR, Relative risk; UC, Usual care.
Acknowledgments
Editorial support and strategic input were provided by Orjola Shahaj of Aquarius Population Health.
Funding
Aquarius Population Health was funded by AstraZeneca to carry out this research.
Disclosure
The study design, data gathering, data analysis, results and interpretation were carried out independently by the authors who declare that the source of funding has not led to any competing or conflicting interests. AstraZeneca reviewed the manuscript for medical and scientific accuracy. EA reports that Aquarius received funding for their company to do the research and their company has received funding for other projects relating to COPD and respiratory conditions from grants and commercial contracts (including AstraZeneca which funded the project in question). Outside of the submitted work, TW reports receiving consulting fees and/or fees for attending lectures, meetings and conferences and/or travel expenses and/or research grants from My mhealth, AstraZeneca, GlaxoSmithKline, Synairgen, Bergenbio, UCB, UKRI, NIHR, Valneva, OM Pharma, Boehringer Ingelheim, Roche, Chiesi, Teva and Nutricia. TW is a founder, director and shareholder of My mhealth. TW has served on monitoring boards for trials sponsored by Synairgen and Valneva, and has applied for patents with GlaxoSmithKline and My mhealth. HW reports receiving consulting fees and/or fees/honoraria for attending/presenting lectures, meetings and conferences and/or travel expenses and/or grants from AstraZeneca, Boehringer Ingelheim, Chiesi, Novartis, Bayer, GlaxoSmithKline and Veronapharma. HW has served on monitoring boards for AstraZeneca, Boehringer Ingelheim, Chiesi, Novartis, Bayer and GlaxoSmithKline. MB reports receiving consulting fees and/or fees/honoraria for attending/presenting lectures, meetings and conferences and/or travel expenses and/or grants from AstraZeneca, GlaxoSmithKline, Pfizer, Sanofi, Covis, Grifols, Boehringer Ingelheim, Valeo, The Lung Association of Saskatchewan, Alberta Lung and NWT, CIHR, Alberta Innovates, Novartis and Mereo. MB has a leadership or fiduciary role in the Canadian Thoracic Society and Alberta Health Services. CL reports grants and personal fees from AstraZeneca, Boehringer Ingelheim, Novartis, and Pfizer, grants from Ontario Ministry of Health and Canadian Institutes of Health Research and personal fees from GSK, Valeo, Teva and Covis, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Miravitlles M, Guerrero T, Mayordomo C, Sánchez-Agudo L, Nicolau F, Segú JL. Factors associated with increased risk of exacerbation and hospital admission in a cohort of ambulatory COPD patients: a multiple logistic regression analysis. The EOLO Study Group. Respiration. 2000;67(5):495–501. doi:10.1159/000067462
2. Donaldson GC, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10):847–852. doi:10.1136/thorax.57.10.847
3. Hurst J, Stone RA, McMillan V, Mortier K. National Asthma and Chronic Obstructive Pulmonary Disease Audit Programme (NACAP). Outcomes of patients included in the 2017/18 COPD clinical audit; 2020.
4. Matsui H, Jo T, Fushimi K, Yasunaga H. Outcomes after early and delayed rehabilitation for exacerbation of chronic obstructive pulmonary disease: a nationwide retrospective cohort study in Japan. Respir Res. 2017;18:68. doi:10.1186/s12931-017-0552-7
5. World Health Organization. The top 10 causes of death. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
6. Bloom DE, Cafiero E, Jané-Llopis E, et al. The global economic burden of noncommunicable diseases. PGDA Working Papers; 2012.
7. Rehman A, Hassali MAA, Muhammad SA, Harun SN, Shah S, Abbas S. The economic burden of chronic obstructive pulmonary disease (COPD) in Europe: results from a systematic review of the literature. Eur J Health Econ. 2020;21(2):181–194. doi:10.1007/s10198-019-01119-1
8. Starkie HJ, Briggs AH, Chambers MG. Pharmacoeconomics in COPD: lessons for the future. Int J Chron Obstruct Pulmon Dis. 2008;3(1):71–88.
9. GOLD. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Global Initiative for Chronic Obstructive Lung Disease - GOLD; 2023.
10. Adeloye D, Song P, Zhu Y, Campbell H, Sheikh A, Rudan I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;1(1). doi:10.1016/S2213-2600(21)00511-7
11. Safiri S, Carson-Chahhoud K, Noori M, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990–2019: results from the global burden of disease study 2019. BMJ. 2022;378:e069679. doi:10.1136/bmj-2021-069679
12. NHS. Chronic obstructive pulmonary disease (COPD) - Treatment; 2017. Available from: https://www.nhs.uk/conditions/chronic-obstructive-pulmonary-disease-copd/treatment/.
13. National Institute for Health and Care Excellence. Chronic obstructive pulmonary disease in over 16s: diagnosis and Management; 2018. Available from: https://www.nice.org.uk/guidance/ng115.
14. Vogelmeier C, Buhl R, Criée CP, et al. Leitlinie der Deutschen Atemwegsliga und der Deutschen Gesellschaft für Pneumologie und Beatmungsmedizin zur Diagnostik und Therapie von Patienten mit chronisch obstruktiver Bronchitis und Lungenemphysem (COPD)[Guidelines for the diagnosis and therapy of COPD issued by Deutsche Atemwegsliga and Deutsche Gesellschaft für Pneumologie und Beatmungsmedizin]. Pneumologie. 2007;61(5):e1–40. German. doi:10.1055/s-2007-959200
15. Bourbeau J, Bhutani M, Hernandez P, et al. Canadian Thoracic Society clinical practice guideline on pharmacotherapy in patients with COPD - 2019 update of evidence. Can J Respir Crit Care Sleep Med. 2019;3(4):210–232. doi:10.1080/24745332.2019.1668652
16. Japanese Respiratory Society. Guidelines for the diagnosis and treatment of COPD (Chronic Obstructive Pulmonary Disease) 3rd Edition: pocket guide; 2010. Available from: https://www.jrs.or.jp/modules/english/index.php?content_id=15.
17. Pullen R, Miravitlles M, Sharma A, et al. CONQUEST quality standards: for the collaboration on quality improvement initiative for achieving excellence in standards of COPD care. COPD. 2021;16:2301–2322. doi:10.2147/COPD.S313498
18. Meiwald A, Gara-Adams R, Rowlandson A, et al. Qualitative validation of COPD evidenced care pathways in Japan, Canada, England, and Germany: common barriers to optimal COPD care. Int J Chron Obstruct Pulmon Dis. 2022;17:1507–1521. doi:10.2147/COPD.S360983
19. Bhutani M, Price DB, Winders TA, et al. Quality standard position statements for health system policy changes in diagnosis and management of COPD: a global perspective. Adv Ther. 2022;39(6):2302–2322. doi:10.1007/s12325-022-02137-x
20. Simons SO, Hurst JR, Miravitlles M, et al. Caring for patients with COPD and COVID-19: a viewpoint to spark discussion. Thorax. 2020;75(12):1035–1039. doi:10.1136/thoraxjnl-2020-215095
21. Lambe T, Adab P, Jordan RE, et al. Model-based evaluation of the long-term cost-effectiveness of systematic case-finding for COPD in primary care. Thorax. 2019;74(8):730–739. doi:10.1136/thoraxjnl-2018-212148
22. Jordan RE, Adab P, Sitch A, et al. Targeted case finding for chronic obstructive pulmonary disease versus routine practice in primary care (TargetCOPD): a cluster-randomised controlled trial. Lancet Respir Med. 2016;4(9):720–730. doi:10.1016/S2213-2600(16)30149-7
23. Jordan RE, Lam K, Bong H, et al. Case finding for chronic obstructive pulmonary disease: a model for optimising a targeted approach. Thorax. 2010;65(6):492–498. doi:10.1136/thx.2009.129395
24. Koolen EH, van der Wees PJ, Westert GP, Dekhuijzen R, Heijdra YF, Hul AJ. The COPDnet integrated care model. Int J Chron Obstruct Pulmon Dis. 2018;13:2225–2235. doi:10.2147/COPD.S150820
25. Gavish R, Levy A, Dekel OK, Karp E, Maimon N. The Association between hospital readmission and pulmonologist follow-up visits in patients with COPD. CHEST. 2015;148(2):375–381. doi:10.1378/chest.14-1453
26. Atwood CE, Bhutani M, Ospina MB, et al. Optimizing COPD acute care patient outcomes using a standardized transition bundle and care coordinator. Chest. 2022;162(2):321–330. doi:10.1016/j.chest.2022.03.047
27. Hurst J, Amusan L, Andrews R, et al. National Asthma and Chronic Obstructive Pulmonary Disease Audit Programme (NACAP). COPD clinical audit 2019/20 (people with COPD exacerbations discharged from acute hospitals in England, Scotland and Wales between October 2019 and February 2020). Data analysis and methodology report; 2021. https://www.nacap.org.uk/nacap/welcome.nsf/reportsSC.html.
28. Poot CC, Meijer E, Kruis AL, Smidt N, Chavannes NH, Honkoop PJ. Integrated disease management interventions for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2021;9(9). doi:10.1002/14651858.CD009437.pub3
29. Ferrone M, Masciantonio MG, Malus N, et al. The impact of integrated disease management in high-risk COPD patients in primary care. NPJ Prim Care Respir Med. 2019;29(1):1–9. doi:10.1038/s41533-019-0119-9
30. Hussey AJ, Wing K, Ferrone M, Licskai CJ. Integrated Disease management for chronic obstructive pulmonary disease in primary care, from the controlled trial to clinical program: a cohort study. Int J Chron Obstruct Pulmon Dis. 2021;16:3449–3464. doi:10.2147/COPD.S338851
31. Achelrod D, Welte T, Schreyögg J, Stargardt T. Costs and outcomes of the German disease management programme (DMP) for chronic obstructive pulmonary disease (COPD)—A large population-based cohort study. Health Policy. 2016;120(9):1029–1039. doi:10.1016/j.healthpol.2016.08.002
32. Hoogendoorn M, Feenstra TL, Asukai Y, et al. Cost-effectiveness models for chronic obstructive pulmonary disease: cross-model comparison of hypothetical treatment scenarios. Value Health. 2014;17(5):525–536. doi:10.1016/j.jval.2014.03.1721
33. Eklund O, Afzal F, Borgström F, et al. Cost-effectiveness of tiotropium versus glycopyrronium in moderate to very severe chronic obstructive pulmonary disease in Canada, Spain, Sweden, and the UK. Clinicoecon Outcomes Res. 2016;8:243–252. doi:10.2147/CEOR.S105579
34. Hettle R, Wouters H, Ayres J, et al. Cost-utility analysis of tiotropium versus usual care in patients with COPD in the UK and Belgium. Respir Med. 2012;106(12):1722–1733. doi:10.1016/j.rmed.2012.09.006
35. TreeAge Pro, R1. TreeAge software. Williamstown, MA; 2021. Available from: http://www.treeage.com.
36. Sin DD, Bell NR, Svenson LW, Man SFP. The impact of follow-up physician visits on emergency readmissions for patients with asthma and chronic obstructive pulmonary disease: a population-based study. Am J Med. 2002;112(2):120–125. doi:10.1016/S0002-9343(01)01079-8
37. NICE. Economic evaluation NICE health technology evaluations: the manual guidance NICE; 2022. Available from: https://www.nice.org.uk/process/pmg36/chapter/economic-evaluation#presenting-expected-cost-effectiveness-results.
38. Institute for Quality and Efficiency in Health Care. Allgemeine Methoden - Entwurf für Version 6.1. IQWiG; 2021.
39. CADTH. Guidelines for the economic evaluation of health technologies: Canada — 4th edition. Available from: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition.
40. Shiroiwa T, Fukuda T, Ikeda S, Takura T, Moriwaki K. Development of an official guideline for the economic evaluation of drugs/medical devices in Japan. Value Health. 2017;20(3):372–378. doi:10.1016/j.jval.2016.08.726
41. Adab P, Fitzmaurice D, Dickens A, et al. Cohort profile: the Birmingham Chronic Obstructive Pulmonary Disease (COPD) cohort study. Int J Epidemiol. 2017;46(1):23. doi:10.1093/ije/dyv350
42. Worth H, Buhl R, Criée CP, Kardos P, Mailänder C, Vogelmeier C. The ‘real-life’ COPD patient in Germany: the DACCORD study. Respir Med. 2016;111:64–71. doi:10.1016/j.rmed.2015.12.010
43. Maleki-Yazdi MR, Kelly SM, Lam SY, Marin M, Barbeau M, Walker V. The burden of illness in patients with moderate to severe chronic obstructive pulmonary disease in Canada. Can Respir J. 2012;19(5):319–324. doi:10.1155/2012/328460
44. Kobayashi S, Hanagama M, Ishida M, et al. Clinical characteristics and outcomes in Japanese patients with COPD according to the 2017 GOLD classification: the Ishinomaki COPD Network Registry. Int J Chron Obstruct Pulmon Dis. 2018;13:3947–3955. doi:10.2147/COPD.S182905
45. Office Of National Statistics. National Life Tables: England 2018–20. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/lifeexpectancies/datasets/nationallifetablesenglandreferencetables/current.
46. Leivseth L, Brumpton BM, Nilsen TIL, Mai XM, Johnsen R, Langhammer A. GOLD classifications and mortality in chronic obstructive pulmonary disease: the HUNT Study, Norway. Thorax. 2013;68(10):914–921. doi:10.1136/thoraxjnl-2013-203270
47. Statistisches Bundesamt Deutschland. GENESIS-online 2019–21; 2022. Available from: https://www-genesis.destatis.de/genesis/online?operation=previous&levelindex=3&levelid=1643641082608&levelid=1643641067302&step=2#abreadcrumb.
48. Government of Canada, Statistics Canada. 2016 census of Canada: data tables - age (in single years) and average age (127) and sex (3) for the population of Canada, provinces and territories, census divisions, census subdivisions and dissemination areas, 2016 census - 100% data; 2017. Available from: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/dt-td/index-eng.cfm.
49. National Institute of Population and Social Security Research. All Japan: 2021 life table data series. Japanese Mortality Database; 2022. Available from: https://www.ipss.go.jp/p-toukei/JMD/00/index-en.html.
50. Karner C, Chong J, Poole P. Tiotropium versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;CD009285. doi:10.1002/14651858.CD009285.pub2
51. Roberts CM, Pozo-Rodríguez DF. An International Comparison of COPD Care in Europe: Results of the First European COPD Audit. European Respiratory Society; 2012.
52. Shirakawa C, Shiroshita A, Shiba H, et al. The prognostic factors of in-hospital death among patients with pneumonic COPD acute exacerbation. Respir Investig. 2021;60:271–276. doi:10.1016/j.resinv.2021.11.009
53. National Asthma and COPD Audit Programme (NACAP). Secondary care workstream - COPD. RCP London; 2016. Available from: https://www.rcplondon.ac.uk/projects/national-asthma-and-copd-audit-programme-nacap-secondary-care-workstream-copd.
54. Xe. Xe currency converter - live exchange rates today. Available from: https://www.xe.com/currencyconverter/.
55. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2020 report; 2020.
56. Costa F, Porcu A, Balestracci S, et al. Cost and effectiveness of 2 years integrated care intervention in COPD. Eur Respir J. 2015;46(suppl 59). doi:10.1183/13993003.congress-2015.PA679
57. Bandurska E, Damps-Konstańska I, Popowski P, et al. Cost-effectiveness analysis of integrated care in management of advanced Chronic Obstructive Pulmonary Disease (COPD). Med Sci Monit. 2019;25:2879–2885. doi:10.12659/MSM.913358
58. Scarffe AD, Licskai CJ, Ferrone M, Brand K, Thavorn K, Coyle D. Cost-effectiveness of integrated disease management for high risk, exacerbation prone, patients with chronic obstructive pulmonary disease in a primary care setting. Cost Eff Resour Alloc. 2022;20(1):39. doi:10.1186/s12962-022-00377-w
59. Hasegawa M, Komoto S, Shiroiwa T, Fukuda T. Formal implementation of cost-effectiveness evaluations in Japan: a unique health technology assessment system. Value Health. 2020;23(1):43–51. doi:10.1016/j.jval.2019.10.005
60. Bourbeau J. Integrated disease management for adults with chronic obstructive pulmonary disease. BMJ. 2014;349:g5675. doi:10.1136/bmj.g5675
61. Whittaker H, Rubino A, Müllerová H, et al. Frequency and severity of exacerbations of COPD associated with future risk of exacerbations and mortality: a UK routine health care data study. Int J Chron Obstruct Pulmon Dis. 2022;17:427–437. doi:10.2147/COPD.S346591
62. van Boven JFM, Vegter S, van der Molen T, Postma MJ. COPD in the working age population: the economic impact on both patients and government. COPD. 2013;10(6):629–639. doi:10.3109/15412555.2013.813446
63. Foo J, Landis SH, Maskell J, et al. Continuing to confront COPD international patient survey: economic impact of COPD in 12 countries. PLoS One. 2016;11(4):e0152618. doi:10.1371/journal.pone.0152618
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.