Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Estimating Proportion and Barriers of Medication Error Reporting Among Nurses in Hail City, Saudi Arabia: Implications for Improving Patient Safety
Authors Alrasheeday AM, Alkubati SA ![]() , Alrubaiee GG, Alqalah TA, Alshammari B
, Alrubaiee GG, Alqalah TA, Alshammari B ![]() , Abdullah SO, Loutfy A
, Abdullah SO, Loutfy A ![]()
Received 28 February 2024
Accepted for publication 20 May 2024
Published 23 May 2024 Volume 2024:17 Pages 2601—2612
DOI https://doi.org/10.2147/JMDH.S466339
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Awatif M Alrasheeday,1 Sameer A Alkubati,2,3 Gamil G Alrubaiee,4,5 Talal A Alqalah,2 Bushra Alshammari,2 Saleh O Abdullah,3 Ahmed Loutfy6,7
1Nursing Administration Department, University of Hail, Hail, Saudi Arabia; 2Department of Medical Surgical Nursing, University of Hail, Hail, Saudi Arabia; 3Department of Nursing, Hodeidah University, Hodeida, Yemen; 4Department of Community Health, University of Hail, Hail, Saudi Arabia; 5Department of Community Health, Al Razi University, Sanaa, Yemen; 6Maternal and Child Nursing Department, College of Nursing, University of Hail, Hail, 2440, Saudi Arabia; 7Department of Nursing, College of Health Sciences, University of Fujairah, Fujairah, 1207, United Arab Emirates
Correspondence: Sameer A Alkubati, Department of Medical Surgical Nursing, University of Hail, Hail, Saudi Arabia, Tel +966506575284, Email [email protected]
Background: Determining the proportion of nurses reporting medication errors (MEs) and identifying the barriers they perceive in ME reporting are crucial to encourage nurses to actively report MEs.
Objective: This study aimed to determine the proportion of nurses experiencing and reporting MEs, perceived barriers to reporting MEs and their association with nurses’ sociodemographic and work-related characteristics.
Methods: A cross-sectional study was conducted among 350 nurses from June to November 2023. Data about sociodemographic and work-related characteristics, and ME reporting, were collected using a validated self-administered questionnaire.
Results: The study found that 34.3% of nurses reported MEs, while 11.1% reported experiencing MEs during their practice. ME reporting was higher proportion among nurses who were older than 40 years (52.1%), males (41.4%), held a master’s degree (58.7%), Saudi nationals (37.8%), experienced for more than 10 years (43.1%), working in intensive care units (44.3%), working for 48 hours or more per week (39.7%), working in hospitals with a nurse-to-patient ratio of 1:3 (44.9%) and having a system for incident reporting (37.7%) and with no training on patient safety (44.6%) compared to their counterparts. The rate of experiencing MEs was higher proportion among nurses who were older than 40 years (16.7%), males (17.3%), married (14.8%), Saudi nationals (13.4%), experienced for more than 10 years (15.6%) and with no training on patient safety (15.3%) compared to their counterparts. Lack of knowledge of the person responsible for reporting MEs was the most frequent perceived barrier to ME reporting (66.6%), followed by fears of blame (65.4%).
Conclusion: In this study, nurses reported and experienced MEs during their practice. Most nurses perceive the lack of knowledge and fear of blame or disciplinary actions as barriers to reporting. Healthcare administrators should implement educational programs and workshops to increase nurses’ awareness of ME reporting.
Keywords: nurse, medication error, reporting, barrier, patient safety, Saudi Arabia
Introduction
The use of medications is the most frequently recommended intervention for patients with health conditions.1 However, medication errors (MEs) can occur during their prescription or dispensing. These errors can be avoided through appropriate prescription practices.2 MEs have serious consequences and significantly affect patient safety and healthcare quality. Ensuring appropriate drug prescriptions is critical for improving patient safety and lowering morbidity and mortality rates.1,3 The Joint Commission on Accreditation of Healthcare Organizations has identified MEs as the most common preventable errors in healthcare practice.4 MEs affect approximately 2–14% of inpatients, resulting in an estimated 7000 annual deaths.5 Several studies have been conducted in various regions of Saudi Arabia to assess MEs, with rates ranging from 41.6% to 70%.6–8
MEs can arise at any point during the treatment process provided by a multidisciplinary healthcare team.9,10 These errors can be caused by both individual and systemic factors. Individual factors contributing to MEs include clinical experience, neglect, forgetfulness or lack of attention, failure to adhere to basic protocols, insufficient understanding, and ineffective communication. Similarly, systemic factors, such as excessive workload, ambiguous communication or guidance and unclear guiding principles, also contribute to MEs.11 There are several barriers perceived by nurses that hinder the reporting of MEs, with personal barriers being the most significant. These include the fear of facing negative consequences or disciplinary actions upon reporting MEs, fear of victimization, fear of reaction from nursing staff or coworkers, and fear of losing one’s position.1 In addition, nurses have identified their experiences in error reporting as personal barriers to reporting such MEs.12
Medication administration is a routine and essential nursing task that is extremely challenging.1,13 Nursing staff are the frontline healthcare workers who frequently administer medications during their shifts, resulting in higher rates of MEs than other healthcare workers.1 Nurses also play a crucial role in identifying and recognizing MEs, ensuring accurate and prompt documentation of such errors.13 They are responsible for communicating and collaborating with other stakeholders involved in reporting MEs, as well as actively participating in the analysis of underlying error reasons.14 In medical institutions, nursing staff is more relied upon than other healthcare providers to recognize and report MEs. However, the decision to report MEs is ultimately influenced by a variety of factors, including their attitudes towards reporting and the barriers to ME reporting.15
Number of modifiable barriers to ME reporting have been identified for nurses in various studies that include organizational factors such as lack of ME system, inadequate information on reporting a ME, absence of positive feedback for accurately administering medication, fear of losing job, and inadequate level of managerial guidance and assistance16–18 In a study that was conducted by Alshammari et al 2201, they found that lack of knowledge and training were the main barrier of reporting ME.17 In another study was conducted by Jember et al 2018 revealed that nurses’ sex and marital status significantly associated with medication error reporting.1
Understanding nurses’ attitudes and perceived barriers to reporting MEs is crucial for building a cooperative and non-punitive culture in healthcare institutions and encouraging nurses to report MEs. Several studies have assessed the prevalence of MEs in various regions of Saudi Arabia, with considerable variations in their findings.6,8,19 However, the barriers to reporting these errors, along with their association with sociodemographic and work-related factors, have not been extensively investigated. Therefore, this study aimed to determine the proportion of nurses experiencing and reporting MEs, perceived barriers to reporting MEs and their association with nurses’ sociodemographic and work-related characteristics.
Methods
Study Design and Population
A cross-sectional design was used in this study. This study was conducted among nurses at all public hospitals in Hail city, Saudi Arabia, from June to November 2023. The study included both Saudi and non-Saudi nurses who had more than one year of nursing practice and agreed to participate voluntarily. OpenEpi, Version 3.01 (www.openepi.com), a software program used to determine the sample size for a proportional or descriptive study based on a population size of 1500, 95% confidence level, and 5% absolute precision, was used to estimate a minimum sample size of 306 nurses. The sample size was 350 nurses who satisfied the inclusion criteria in all public hospitals of the city.
Data Collection
Data were collected using a self-administered questionnaire, which was adapted from a previous study by Jember et al1 and consisted of four sections related to MEs. The first section included items related to ME incidence and nurses’ experiences with MEs. The proportion of nurses who reported experiencing MEs was calculated from the question “Have you ever experienced any medication administration error?”. The second section included items related to the self-reporting of MEs to determine the proportion of nurses reporting MEs. The proportion of nurses who reported MEs was calculated from the question “Have you ever reported a medication error?”. The third section included items related to nurses’ attitudes towards barriers to ME reporting. This part consist of eight questions related to the possible causes that the nurse think that they hinder them from reporting medication errors. Each question was rated as “Yes = 1” or “No = 0”, so the scoring of this part was rated from 0–8 with the high scores mean more barriers to ME reporting. The fourth section included items related to nurses’ perceptions of organizational culture and their actual dealing with MEs. This part contains two questions of 5-point Likert scale (strongly disagree, disagree, neither agree nor disagree, agree, strongly agree). The choice of neutral was excluded before questionnaire distribution. After that we combined the responses of “strongly agree” and “agree” responses into a single “agree” category and “strongly disagree” and “disagree” into “disagree”., which reflects the nurses’ perception of the organization’s effectiveness in handling errors. In addition, the tool included questions about the sociodemographic and work-related characteristics of nurses such as sex, age, marital status, education level, nationality, experience, department, position at work, weekly working hours, nurse-to-patient ratio, and the presence of an error incident-reporting system.
The face and content validity of the tool were previously tested in other studies.1,20 The reliability of the tool was established in previous study with a Cronbach’s alpha coefficient of 0.8.20 In this study, an English version of the tool was used, as it is the official language in the hospitals involved. To ensure the readability and feasibility of the tool, a pilot study was conducted among 35 nurses who were not included in the final analysis. The results of the pilot study revealed that the tool was easily understood and took 15–20 minutes to complete. The reliability of the tool was further confirmed with a Cronbach’s alpha coefficient of 0.88. The head nurses of hospitals encouraged nurses, and the researchers subsequently invited these nurses to participate. During the nurses’ break, a researcher gave the nurses the questionnaires and informed consent forms, explaining the purpose of the study and waiting for them to fill them out. After filling out the questionnaires, respondents were asked to send them back to the heads of their departments. 400 questionnaires were distributed, from them 350 were returned with the response rate 87.5%.
Ethical Approval
The University of Ha’il’s Research Ethics Committee approved the study (Ethical Approval No: H-2023-363). All participants provided written informed consent after being informed that their participation was voluntary and that they could withdraw at any time without giving a reason. The participants’ anonymity was maintained by sharing only aggregated data. Each participant was assigned a unique code number during data collection and analysis to ensure their privacy and maintain the confidentiality of their data.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics, version 27.0 (IBM Corp., Armonk, NY, USA). The chi-square test was used to determine the association between the independent variables and the dependent categorical outcomes (error reporting and error experience). The non-normal distribution of the data of continuous variables was determined using the Kolmogorov–Smirnov test. Accordingly, nonparametric tests (Mann–Whitney U-test or Kruskal–Wallis H-tests) were used to assess the relationship between the independent variables and the total scores of the nurses’ attitudes to barriers for reporting MEs. Statistical significance was set at p <0.05.
Results
Characteristics of Participating Nurses
Table 1 shows that most nurses were females (53.7%), aged between 30 and 40 years (56.6%) and married (59.7%). The majority of nurses held a bachelor’s degree in nursing (75.7%) and were Saudi nationals (70%). The highest proportion of nurses had less than five years of experience (38%), and the majority were affiliated with intensive care units (ICUs) (32.9%), held the position of registered nurses (74.6%) and had direct contact with patients (87.1%). More than half of nurses (51.1%) reported working 48 hours or more per week, and the nurse-to-patient ratio was most commonly 1: ≥6 (35.1%).
 |
Table 1 Characteristics of Nurses Included in the Study (N = 350) |
Proportion of Nurses Reporting and Experiencing MEs
Of nurses working in public hospitals in Hail city, the proportion of nurses who reported MEs based on their own assessment was 34.3% (120/350), with a 95% confidence interval (CI) between 29.3% and 39.5%. On the other hand, 11.1% (39/350) of nurses reported experiencing MEs during their practice.
Association of Nurses’ Characteristics with Reporting and Experiencing MEs
Table 2 shows that the rate of experiencing MEs was higher proportion among nurses older than 40 years (16.7%; p <0.001), male nurses (17.3%; p <0.001), married nurses (14.8%; p = 0.016), Saudi nationals (13.4%; p = 0.038), nurses with more than 10 years of experience (15.6%; p = 0.048) and among nurses who had not received training on patient safety (15.3%; p = 0.026) compared to their counterparts. On the other hand, ME reporting was higher proportion among nurses older than 40 years (52.1%; p = 0.018), male nurses (41.4%; p = 0.010), nurses with a master’s degree in nursing (58.7%; p <0.001), Saudi nationals (37.8%; p = 0.033), nurses with more than 10 years of experience (43.1%; p = 0.023), nurses affiliated with ICUs (44.3%; p = 0.046), those working for 48 hours or more per week (39.7%; p = 0.030), those working in hospitals with a nurse-to-patient ratio of 1:3 (44.9%; p = 0.020) and having a system for incident reporting (37.7%; p <0.001), and among nurses who had not received training on patient safety (44.6%; p <0.001) compared to their counterparts. Furthermore, concerning nurses’ attitudes towards barriers to ME reporting, significant relationships were found with the variables of age (p = 0.023), sex (p = 0.025), educational level (p <0.001), working hours per week (p <0.001) and receiving training on patient safety (p <0.001). Table 2
 |
Table 2 Association of Sociodemographic and Work-Related Characteristics with Experiencing MEs, Reporting MEs, and Attitudes Towards Barriers to ME Reporting Among Nurses |
As shown in Table 3, the majority of nurses answered that medication errors should be reported in general (94.9%) and should be reported should be reported if they were done by the person himself or herself (91.4%) or by others (79.4%). Approximately one third of nurses reported a medication error (34.3%). The majority of nurses preferred to report the medication error for team leader nurse (71.1%) followed by the nursing director (14.3%).
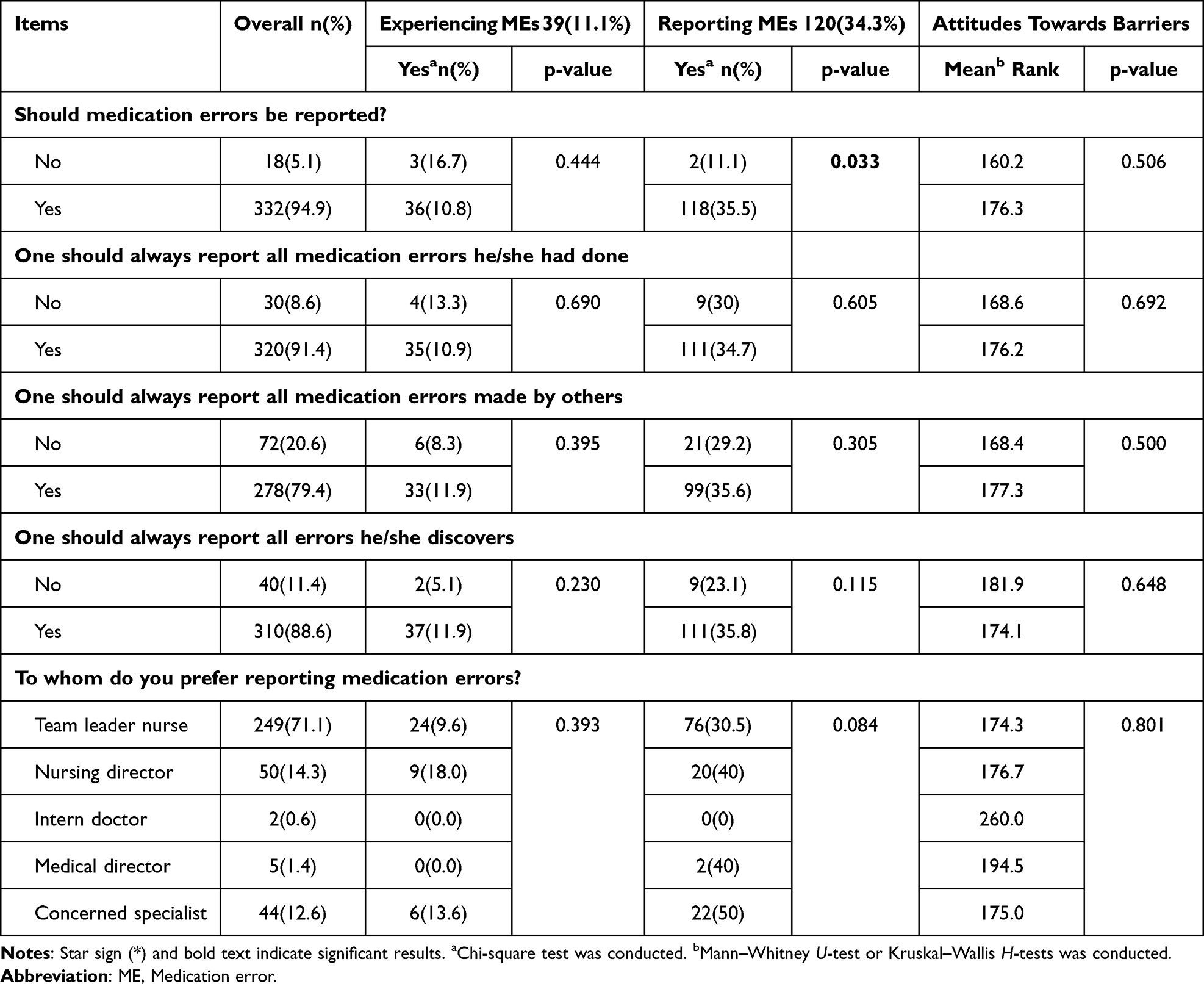 |
Table 3 Association of Experiencing Errors, Reporting MEs and Attitudes Towards Barriers to ME Reporting Among Nurses and Their Perception of Reporting MEs |
Nurses’ Perceived Barriers to Reporting MEs
Figure 1 shows that “Not knowing who is responsible for reporting MEs” was the most frequent barrier perceived by nurses to report MEs (66.6%), followed by “Fear of being blamed” (65.4%), “Fear of disciplinary actions” (64.9%) and “Lack of knowledge of the usefulness of reporting MEs” (63.7%). However, “Belief that it is unnecessary to report MEs not associated with patient harm” was the least frequent barrier perceived by nurses to report MEs (55.4%).
 |
Figure 1 Perceived barriers to ME reporting among nurses in public hospitals of Hail city, Saudi Arabia. |
Nurses’ Perceptions of Organizational Culture Regarding Reporting MEs
Table 4 shows that 87.1% of nurses perceived that medication error discovering and reporting leads to a beneficial and constructive activity within the organization. On the other hand, 78.8% of them had concerns about the negative impact of discovering MEs on the nurse’s possible development and career in the organizational hierarchy.
 |
Table 4 Perceptions of Organizational Culture Regarding Reporting MEs Among Nurses in Public Hospitals of Hail City, Saudi Arabia |
Discussion
This study revealed that approximately one-third of nurses working in public hospitals in Hail city reported MEs based on their own assessment. Accordingly, it is concerning that a substantial proportion of nurses were hesitant or unwilling to report MEs that occur in their practice, suggesting that there is a lack of appropriate ME reporting.9 Meanwhile, the present study also revealed that a smaller proportion of nurses, specifically 11%, reported personally experiencing MEs during their practice. The relatively low proportion of nurses reporting personal experiences of MEs raises concerns about the possibility that some nurses may have encountered errors but chose not to report them, possibly due to concerns about the consequences or fear of being held accountable This highlights the existence of barriers to transparent reporting within the healthcare system.
The proportion of ME reporting in our study is lower compared to previous findings from other regions within the country (41.2%).17,21 Similarly, it is also lower than the proportions reported from other countries, including Jordan (42.1%),22 Ethiopia (37,9%)20 and Australia (50%).23 In contrast, the proportion of ME reporting in the present study is slightly higher than the proportion reported for nurses in the United States (28.9%).24 These discrepancies in the rates of ME reporting can be attributed to differences in the definition, setting, and methods used to assess MEs. Furthermore, the variations in the proportions of ME reporting may be influenced by the type and severity of the MEs encountered and reported by different healthcare institutions. Several factors, such as varying levels of awareness, reporting systems and organizational policies, can contribute to these variations in the rates of ME reporting across institutions and regions. However, this emphasized the need for ME reporting systems that help in improving patient safety and serve as a key instrument for retrospective medication safety risk management because they offer data on the incidents that have occurred.25
The study revealed that specific groups of nurses and certain work-related characteristics were associated with significantly higher proportions of ME reporting among nurses. Male nurses and those with Saudi nationality showed a higher proportion of ME reporting compared to their counterparts. This finding contradicts previous studies, which consistently showed that females tended to report MEs more frequently than males.1,20,26 The observed discrepancy in ME reporting could be attributed to variations in personality traits between males and females. Additionally, the influence of the patient safety culture within healthcare institutions may contribute to these variations. Unlike Saudi nurses, non-Saudi nurses working in a punitive and unsupportive environment for patient safety may experience greater hesitancy in reporting MEs due to concerns over potential consequences.
In the present study, nurses over the age of 40 and with more than 10 years of experience were more likely to report MEs, which could be attributed to their experience and knowledge in recognizing and acknowledging mistakes, as well as their understanding of the importance of reporting for patient safety. As nurses accumulate more experience, they become more aware of the potential risks and consequences of errors, motivating them to report incident when they occur. Furthermore, nurses working in ICUs demonstrated a higher tendency to report errors. It is possible that the critical nature of the environment, where even minor errors can have severe consequences, leads to a heightened culture of reporting and accountability among ICU nurses. On the other hand, longer weekly working hours (≥48 hours/week) was associated with significantly higher rate of ME reporting among nurses. The extended working hours might increase the exposure to potential errors, prompting nurses to be more vigilant in recognizing and reporting them.
The present study revealed that the presence of an incident-reporting system in hospitals positively influenced ME reporting among nurses. Hospitals that have a structured system for ME reporting in place usually provide nurses with a clear mechanism and support to report MEs, encouraging a culture of transparency and continuous improvement within the healthcare institution. On the other hand, handling three to six patients per shift was associated with a higher proportion of reporting MEs. This finding could be attributed to the increased likelihood of errors due to the higher patient load. Handling a larger number of patients during a shift can intensify workload, stress and fatigue, leading to a greater awareness of potential errors and a higher likelihood of reporting them. According to Jang et al3 a supportive patient safety culture can lead to increased rates of reporting MEs. However, their study did not identify any significant differences in ME reporting among South Korean nurses based on their work hours or work units. On the other hand, nurses in Saudi Arabia were found to report MEs regardless of the severity of the condition being treated.9 Several factors, including sex, previous incidents of MEs, experience with MEs and the work environment, were found to be significantly associated with ME reporting by Ethiopian nurses.1 These findings emphasize the multifaceted nature of ME reporting and highlight the importance of considering various factors that impact reporting behavior.
Our study revealed a higher likelihood of ME reporting among nurses with higher qualifications compared to those with diploma certifications. This finding is consistent with those reported in several other studies, which found that nurses with a bachelor’s or master’s degree were more likely to report MEs than nurses with a diploma certification.1,20,27 One possible explanation for this observation is that people with higher educational attainment have a better understanding, attitude, and practice regarding the side effects of drugs. Furthermore, their educational experiences may have contributed to a better understanding of the code of ethics, thereby increasing the likelihood of reporting medication side effects. Therefore, further investigations are warranted to identify any potential gaps in nursing curriculum and training programs, as well as potential areas for improvement in nursing education. It is important to ensure that nurses across all levels of education receive adequate preparation and knowledge to actively report MEs, thereby contributing to the enhancement of patient safety efforts.
Concerning nurses’ attitudes toward patient safety barriers, our findings indicate that nurses with less than 30 years of experience, master’s degrees, and working less than 48 hours per week are more optimistic about patient safety barriers. This indicates that younger nurses and those with higher education are more aware of patient safety standards, have better understanding of patient safety, and possess the necessary knowledge and skills to overcome barriers effectively. On the other hand, excessive workload and fatigue negatively impact nurses’ attitudes towards patient safety. Consequently, it is recommended that nurses receive regular patient safety training and have sufficient rest and recovery time between shifts to maintain a positive attitude and prioritize patient safety. The findings are comparable with similar studies conducted in Saudi Arabia and other nations.1,20,26
Similarly, female nurses and those who had received patient safety training were found to be more optimistic about patient safety barriers than the other groups. This could be attributed to a number of factors, including differences in communication styles, empathy, and personal views that women bring to their nursing practice. This may highlight a difference in perception, but it does not mean that males are less concerned about patient safety. Many previous studies have found that female nurses and those who have received patient safety training had more positive attitudes toward patient safety barriers than other groups of nurses.20,26
Our study identified several barriers perceived by nurses when it comes to reporting MEs. The most commonly reported barrier was a lack of knowledge regarding the one responsible for reporting MEs, followed by fears of being blamed or facing disciplinary actions. These findings highlight an uncooperative and punitive culture in hospitals, which is concerning and can negatively impact patient safety. These barriers emphasize the importance of establishing a safe and supportive ME reporting program within healthcare institutions. By creating an environment that encourages open communication and learning from errors rather than placing blame, healthcare organizations can actively promote a culture of reporting and learning. These findings are consistent with previous studies conducted in Taiwan and Malaysia, which identified fear of negative consequences following reporting as the most significant barrier to ME reporting.15,28 Studies conducted in Saudi Arabia have found that nurses were reluctant to disclose MEs because of fear of being held accountable, and when MEs occurred, nurses tended to focus on individual blame rather than exploring the underlying causes.5,9,21 These findings can be attributed to the existence of a poor reporting safety culture that hinders nurses from reporting MEs and a lack of awareness about the importance of such reporting. These observations underscore the need to reevaluate and modify the supportive safety culture within hospitals in Saudi Arabia, and the importance of ME reporting in clinical practice should be emphasized across training programs and guidelines.
The perception of nurses regarding the organizational culture surrounding ME reporting can be influenced by the type of safety culture established within their healthcare organization. The present study revealed that the majority of nurses recognized the value and constructive nature of discovering and reporting MEs within their organization. However, more than two-thirds of them expressed concerns about the potential adverse consequences of such reporting on their professional growth and advancement within the organizational hierarchy. These findings emphasize the importance of changing the safety culture to one that is blameless and non-punitive, as well as implementing training programs to raise awareness of the value of reporting MEs for both organizations and individuals. Our findings are consistent with those by Evans et al23 who found that nurses, especially those with more than five years of professional experience, were more likely to believe that reporting an incident provides little benefit. Similarly, another study highlighted the benefits and constructive nature of reporting MEs, including improved patient safety, reduced hospitalizations, lower healthcare costs and enhanced organizational reputation.29 Furthermore, the failure to report MEs can impair patient satisfaction and create distrust in healthcare organizations.2 There are some limitations, though. Initially, a cross-sectional and quantitative approach was taken in this study; however, to explore more details of the phenomenon, a longitudinal and qualitative study is advised. Secondly, a convenience sample was employed, which could introduce bias and reduce the sample’s representativeness of the population under study.
Conclusion
Reporting MEs by nurses in public hospitals of Hail city is relatively low, with about one-third reporting them. However, certain groups tend to report more frequently, including older, male and Saudi nurses, and those with higher qualifications, longer years of experience and no training on patient safety. ME reporting also increases with longer working hours, as well as working in ICUs and hospitals with low workload and incident-reporting systems. Most nurses perceive that a lack of knowledge regarding the responsible person for reporting and fears of being blamed or facing disciplinary actions are the barriers to ME reporting. While most nurses recognize the benefits of reporting MEs within their hospitals, they express concerns about the potential negative impact such reporting may have on their professional development and careers. Therefore, healthcare administrators should consider implementing educational programs and workshops to increase nurses’ awareness of ME reporting and its importance. Also, they have to encourage anonymous reporting or a culture that places no blame on others promotes reporting by eliminating stigma and punishment. Future research of qualitative and longitudinal design may help to explore more barriers to reporting ME and strategies to overcome this problem.
Data Sharing Statement
The corresponding author will provide the data from this study upon request.
Informed Consent Statement
Informed written consent was obtained from all participants who were involved in the study.
Acknowledgments
We would like to thank the Scientific Research Deanship at University of Ha’il - Saudi Arabia for their support. Also, we would like to thank all CCNs who participated in this study.
Funding
This research has been funded by Scientific Research Deanship at University of Ha’il, Saudi Arabia through project number (RG-23,128).
Disclosure
The authors declare that there is no conflict of interest in this work.
References
1. Jember A, Hailu M, Messele A, Demeke T, Hassen M. Proportion of medication error reporting and associated factors among nurses: a cross sectional study. BMC Nurs. 2018;17(1):1–8. doi:10.1186/s12912-018-0280-4
2. Tariq RA, Vashisht R, Sinha A, Scherbak Y Medication dispensing errors and prevention; 2018.
3. Jang S-J, Lee H, Son Y-J. Perceptions of patient safety culture and medication error reporting among early-and mid-career female nurses in South Korea. Int J Environ Res Public Health. 2021;18(9):4853. doi:10.3390/ijerph18094853
4. Joint C Sentinel event alert 39: preventing pediatric medication errors. TJC website; 2021. Available from: https://www.jointcommission.org/resources/patient-safety.
5. Hammoudi BM, Ismaile S, Abu Yahya O. Factors associated with medication administration errors and why nurses fail to report them. Scand J Caring Sci. 2018;32(3):1038–1046. doi:10.1111/scs.12546
6. Almalki ZS, Alqahtani N, Salway NT, et al. Evaluation of medication error rates in Saudi Arabia: a protocol for systematic review and meta-analysis. Medicine. 2021;100(9):e24956. doi:10.1097/MD.0000000000024956
7. Mazhar F, Akram S, Al-Osaimi YA, Haider N. Medication reconciliation errors in a tertiary care hospital in Saudi Arabia: admission discrepancies and risk factors. Pharm Pract. 2017;15(1):864. doi:10.18549/PharmPract.2017.01.864
8. Al-Rashoud I, Al-Ammari M, Al-Jadhey H, et al. Medication discrepancies identified during medication reconciliation among medical patients at a tertiary care hospital. Saudi Pharm J. 2017;25(7):1082. doi:10.1016/j.jsps.2017.05.004
9. Alsulami SL, Sardidi HO, Almuzaini RS, et al. Knowledge, attitude and practice on medication error reporting among health practitioners in a tertiary care setting in Saudi Arabia. Saudi Med J. 2019;40(3):246. doi:10.15537/smj.2019.3.23960
10. Alomari A, Wilson V, Solman A, Bajorek B, Tinsley P. Pediatric nurses’ perceptions of medication safety and medication error: a mixed methods study. Compr Child Adolesc Nurs. 2018;41(2):94–110. doi:10.1080/24694193.2017.1323977
11. Zaree TY, Nazari J, Jafarabadi MA, Alinia T. Impact of psychosocial factors on occurrence of medication errors among Tehran public hospitals nurses by evaluating the balance between effort and reward. Saf Health Work. 2018;9(4):447–453. doi:10.1016/j.shaw.2017.12.005
12. Kagan I, Barnoy S. Factors associated with reporting of medication errors by Israeli nurses. J Nurs Care Qual. 2008;23(4):353–361. doi:10.1097/01.NCQ.0000336674.10348.09
13. Martyn J-A, Paliadelis P, Perry C. The safe administration of medication: nursing behaviours beyond the five-rights. Nurs Educ Pract. 2019;37:109–114. doi:10.1016/j.nepr.2019.05.006
14. Ravi P, Pfaff K, Ralph J, Cruz E, Bellaire M, Fontanin G. Nurse-pharmacist collaborations for promoting medication safety among community-dwelling adults: a scoping review. Int J Nurs Stud Adv. 2022;4:100079. doi:10.1016/j.ijnsa.2022.100079
15. Yung HP, Yu S, Chu C, Hou IC, Tang FI. Nurses’ attitudes and perceived barriers to the reporting of medication administration errors. J Nurs Manag. 2016;24(5):580–588. doi:10.1111/jonm.12360
16. Centre for Research on the Epidemiology of Disasters. Annual Disaster Statistical Review 2015: the Numbers and Trends. Available from: https://reliefweb.int/report/world/annual-disaster-statistical-review-2015-numbers-and-trends.
17. Alshammari FM, Alanazi EJ, Alanazi AM, Alturifi AK, Alshammari TM. Medication error concept and reporting practices in Saudi Arabia: a multiregional study among healthcare professionals. Risk Manag Healthc Policy. 2021;14:2395–2406. doi:10.2147/RMHP.S281154
18. Rutledge DN, Retrosi T, Ostrowski G. Barriers to medication error reporting among hospital nurses. J Clin Nurs. 2018;27(9–10):1941–1949. doi:10.1111/jocn.14335
19. Sadat-Ali M, Al-Shafei BA, Al-Turki RA, Ahmed SE, Al-Abbas SA, Al-Omran AS. Medication administration errors in Eastern Saudi Arabia. Saudi Med J. 2010;31(11):1257–1259.
20. Asefa K, Dagne D, Mekonnen WN. Medication administration error reporting and associated factors among nurses working in public hospitals, Ethiopia: a cross-sectional study. Nurs Res Pract. 2021;2021:1–8. doi:10.1155/2021/1384168
21. Alandajani A, Khalid B, Ng YG, Banakhar M. Knowledge and attitudes regarding medication errors among nurses: a cross-sectional study in major Jeddah hospitals. Nurs Rep. 2022;12(4):1023–1039. doi:10.3390/nursrep12040098
22. Mrayyan MT, Shishani K, Al‐Faouri I. Rate, causes and reporting of medication errors in Jordan: nurses’ perspectives. J Nurs Manag. 2007;15(6):659–670. doi:10.1111/j.1365-2834.2007.00724.x
23. Evans SM, Berry JG, Smith BJ, et al. Attitudes and barriers to incident reporting: a collaborative hospital study. BMJ Qual Saf. 2006;15(1):39–43. doi:10.1136/qshc.2004.012559
24. Ulanimo VM, O’Leary-Kelley C, Connolly PM. Nurses’ perceptions of causes of medication errors and barriers to reporting. J Nurs Care Qual. 2007;22(1):28–33. doi:10.1097/00001786-200701000-00007
25. Afaya A, Konlan KD, Kim Do H. Improving patient safety through identifying barriers to reporting medication administration errors among nurses: an integrative review. BMC Health Serv Res. 2021;21(1):1156. doi:10.1186/s12913-021-07187-5
26. Alenezi AM, Baker OG. Knowledge, attitude, and behavior toward medication error in Saudi Arabia. Saudi J Nurs Health Care. 2023;6(9):297–304. doi:10.36348/sjnhc.2023.v06i09.002
27. Bifftu BB, Dachew BA, Tiruneh BT, Beshah DT. Medication administration error reporting and associated factors among nurses working at the University of Gondar Referral Hospital, Northwest Ethiopia, 2015. BMC Nurs. 2016;15(1):1–7. doi:10.1186/s12912-016-0165-3
28. Dyab EA, Elkalmi RM, Bux SH, Jamshed SQ. Exploration of nurses’ knowledge, attitudes, and perceived barriers towards medication error reporting in a tertiary health care facility: a qualitative approach. Pharmacy. 2018;6(4):120. doi:10.3390/pharmacy6040120
29. Çetin SB, Cebeci F. Perceptions of clinical nurses about the causes of medication administration errors: a cross-sectional study. Florence Nightingale J Nurs. 2021;29(1):56. doi:10.5152/FNJN.2021.19135
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.