Back to Journals » Journal of Inflammation Research » Volume 18
Establishment and Validation of a Novel Nutritional-Immune-Inflammatory Score Model for Predicting Survival Prognosis in Hepatocellular Carcinoma Patients Treated with PD-1 Inhibitors
Authors Liu K ![]() , Lv Y, Fu S, Mao Y, Xu Y
, Lv Y, Fu S, Mao Y, Xu Y ![]() , Huang S, Wu J
, Huang S, Wu J
Received 11 June 2025
Accepted for publication 11 September 2025
Published 27 September 2025 Volume 2025:18 Pages 13397—13412
DOI https://doi.org/10.2147/JIR.S546164
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Junhao Wang
Kan Liu,1,* Yaqin Lv,2,* Shumin Fu,1,* Ye Mao,1 Yongkang Xu,1 Shenglan Huang,1 Jianbing Wu1
1Department of Oncology, The Second Affiliated Hospital, Jiangxi Medical College, Nanchang University, Nanchang, Jiangxi Province, People’s Republic of China; 2The Wuxi Branch of the 904th Hospital of the Joint Logistic Support Force, Wuxi, Jiangsu Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianbing Wu, Department of Oncology, The Second Affiliated Hospital of Nanchang University, No. 1, Minde Road, Donghu District, Nanchang City, Jiangxi Province, 330006, People’s Republic of China, Email [email protected] Shenglan Huang, Department of Oncology, The Second Affiliated Hospital of Nanchang University, No. 1, Minde Road, Donghu District, Nanchang City, Jiangxi Province, 330006, People’s Republic of China, Email [email protected]
Purpose: Immune checkpoint inhibitors, particularly PD-1 inhibitors, are widely used in hepatocellular carcinoma therapy, many received PD-1 inhibitors beyond first-line, but heterogeneous treatment responses require reliable biomarkers. The interaction of immune function, nutritional status, and inflammatory responses affects tumor progression and survival, yet their prognostic value in PD-1 inhibitor-treated HCC patients remains unclear. This study developed a novel nutritional-immune-inflammatory score (NIIS) to evaluate its prognostic value in HCC patients receiving PD-1 inhibitors.
Patients and Methods: We analyzed 355 HCC patients treated with PD-1 inhibitors (training: n=249; validation: n=106), the cohort included 18.6% Child-Pugh B patients. Fourteen nutritional, immune, and inflammatory biomarkers were evaluated. Prognostic indicators were selected via univariate and LASSO Cox regression. The NIIS was constructed and validated for OS prediction. A nomogram integrating the NIIS with clinical variables was developed and validated based on calibration curves, AUC, and DCA, and compared with the BCLC staging system. The primary outcome assessed was OS from the initiation of PD-1 inhibitor therapy in HCC patients.
Results: The NIIS (ALRI, APRI, PALBI, AAPR) showed strong prognostic stratification. High-risk patients had shorter OS (training: P =1.764× 10^− 8; verification: P=2.775× 10^− 6). Higher NIIS were significantly associated with advanced tumor stage, poor liver function grade, multiple and larger tumors, tumor thrombus, vascular invasion, and elevated AFP levels (P< 0.05). Multivariate Cox analysis confirmed the NIIS as an independent prognostic factor for OS (training: HR=1.565, 95% CI: 1.273– 1.925; verification: HR=1.341, 95% CI: 1.065– 1.687). A nomogram integrating the NIIS with clinical variables was constructed for individualized prognosis prediction, demonstrating superior predictive performance compared to the conventional BCLC staging system.
Conclusion: The NIIS and nomogram provide a clinically useful tool for risk stratification in HCC immunotherapy, this model outperforming conventional staging systems and may optimize patient selection for PD-1 inhibitor therapy. Prospective multicenter studies are warranted to validate its generalizability.
Keywords: nutritional-immuno-inflammatory indicators, PD-1 inhibitors, hepatocellular carcinoma, survival prediction, prognostic model
Introduction
Hepatocellular carcinoma (HCC) is the most common primary solid tumor of the liver, accounting for 75% of 85%. It is also the fifth most common tumor and the third deadliest tumor in the world.1,2 The incidence of HCC is hidden, most clinical patients are often diagnosed as middle and late stage, can not be cured by surgery or local treatment, the five-year survival rate is less than 15%,3 the prognosis is very poor. In the past, chemotherapy and local interventional therapy were mainly used in the treatment of HCC.4 In recent years, immunotherapy of programmed cell death protein-1 inhibitor has provided a new treatment model for patients with HCC and brought new hope.5,6 The CheckMate040 study and KEYNOTE-224 study explored the efficacy of Nivolumab and Pembrolizumab in the treatment of advanced hepatocellular carcinoma. Studies have shown that patients have achieved sustained efficacy and survival benefits.7,8 However, the efficacy of immunotherapy varies from person to person, and most patients still can not benefit from it. The effective rate of PD-1 inhibitors in patients with HCC is less than 20%.9,10 One of the main reasons is that the biological indicators for predicting the effective efficacy of PD-1 inhibitors are not clear,11–13 so it is very important to find effective predictors and to screen out the benefit groups of patients with HCC treated with PD-1 inhibitors.
The nutritional status, immune function, and inflammation of patients are closely related to tumor development and progression.14 In recent years, multiple studies have shown that nutritional, immune, and inflammatory indicators hold significant potential for predicting treatment outcomes in cancer patients.15–23 Poor nutritional status leads to decreased immunity, impairing T-cell activity and antitumor immune responses.24 Research by Chen et al demonstrated that the prognostic nutritional index (PNI) can predict overall survival (OS) and disease-free survival (DFS) in patients with locally advanced esophageal squamous cell carcinoma after minimally invasive esophagectomy.25 With advances in research on the tumor immune microenvironment, inflammatory responses have been found to closely interact with tumor immune processes, and tumor-associated inflammatory cells are critical components of the tumor immune microenvironment.26,27 Multiple studies indicate that inflammatory markers such as the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) can predict prognosis in various cancers.28–30 Nutritional, immune, and inflammatory indicators may also have prognostic value in predicting outcomes for HCC patients treated with PD-1 inhibitors. However, individual blood biomarkers have limitations in fully reflecting the integrated nutritional-immune-inflammatory status of patients, and no combined nutritional-immune-inflammatory predictive model currently exists for HCC patients.
Therefore, this study collected nutritional, immune, and inflammatory indicators from clinical HCC patients and developed a novel nutritional-immune-inflammatory score (NIIS) predictive model to evaluate the survival prognosis of HCC patients treated with PD-1 inhibitors clinically, aiming to screen beneficiary populations and guide treatment. Simultaneously, an NIIS nomogram was constructed and validated based on the NIIS and other clinical case characteristics to provide individualized predictions of survival probability and treatment guidance for HCC patients.
Materials and Methods
Study Object
In this study, we enrolled patients with hepatocellular carcinoma (HCC) who received PD-1 inhibitor therapy at the Department of Oncology and Hepatobiliary Surgery of the Second Affiliated Hospital of Nanchang University, China, between January 2018 and January 2023. Patients meeting all the following inclusion criteria were included: 1) age ≥18 years; 2) HCC diagnosis confirmed by imaging or histopathology according to the American Association for the Study of Liver Diseases (AASLD) criteria; 3) documented administration of PD-1 inhibitors with complete and traceable medical records; 4) Eastern Cooperative Oncology Group Performance Status (ECOG PS) score of 0–1; and 5) Child-Pugh (CP) classification of grade A or B. Patients were excluded if they met any of the following criteria: 1) presence of severe underlying diseases; 2) concurrent malignancies other than HCC; or 3) history of severe immune-related adverse events or autoimmune diseases. A total of 355 patients were ultimately included and randomly divided into a training group (n=249) and a verification group (n=106) at a ratio of 7:3. This study was approved by the Ethics Committee of the Second Affiliated Hospital of Nanchang University, China, and complied with the ethical principles of the World Medical Association Declaration of Helsinki. Due to the retrospective nature of the study, written informed consent was waived. Clinical trial number: not applicable. This study is a retrospective analysis and does not involve intervention-based clinical trial registration.
Treatment Procedure
Patients received intravenous infusion of PD-1 inhibitors at recommended doses: toripalimab (240 mg every 3 weeks), sintilimab, tislelizumab, camrelizumab, or pembrolizumab (200 mg every 3 weeks). Specific dosages and patient numbers are detailed in Table S1. During PD-1 inhibitor therapy, combination with local interventional therapies or molecular targeted therapies (including sorafenib, lenvatinib, regorafenib, donafenib, or apatinib) was permitted. PD-1 inhibitor treatment was discontinued under the following circumstances: 1) disease progression requiring discontinuation upon evaluation; 2) intolerable adverse reactions; 3) patient request for discontinuation; or 4) physician-determined need to discontinue PD-1 inhibitors and modify the treatment regimen.
Baseline Data Collection
Patient demographic and tumor baseline data included: age, sex, Barcelona Clinic Liver Cancer (BCLC) stage, Child-Pugh score, performance status (PS) score, hepatitis B virus (HBV) infection status, tumor number, maximum tumor diameter, vascular invasion, tumor thrombus, distant metastasis, metastatic sites, prior antitumor therapies, and type and treatment cycles of PD-1 inhibitors. Blood biochemical parameters comprised: D-dimer, total bilirubin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), albumin, alkaline phosphatase (ALP), alpha-fetoprotein (AFP), white blood cell count, platelet count, neutrophil count, lymphocyte count, monocyte count, and fibrinogen. All blood samples for biochemical analysis were collected within 3 days before the initial administration of PD-1 inhibitors.
Definition and Calculation of Nutritional-Immune-Inflammatory Indicators
The pre-treatment blood biochemical parameters assessed prior to the first PD-1 inhibitor administration included 14 nutritional, immune, and inflammatory indices: platelet-to-lymphocyte ratio (PLR), neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), systemic immune-inflammation index (SII), systemic inflammation response index (SIRI), pan-immune-inflammation value (PIV), prognostic nutritional index (PNI), fibrinogen-to-albumin ratio index (FARI), aspartate aminotransferase-to-lymphocyte ratio (ALRI), aspartate aminotransferase-to-platelet ratio (APRI), albumin-to-alkaline phosphatase ratio (AAPR), derived neutrophil-to-lymphocyte ratio (dNLR), albumin-bilirubin index (ALBI), and platelet-albumin-bilirubin index (PALBI). Calculation formulas for all indices are provided in Table S2. Classification criteria:ALBI grades were categorized as grade 1 (score≤−2.60),grade 2 (−2.60<score≤−1.39), and grade 3 (score >−1.39).PALBI grades were defined as grade 1 (score ≤−2.53), grade 2 (−2.53 < score ≤−2.09), and grade 3 (score >−2.09).Other indices were stratified into binary categories based on their median values.
Follow-up and Assessment
The follow-up period concluded on May 31, 2024. During follow-up, laboratory parameters including alpha-fetoprotein (AFP), complete blood count (CBC), and blood biochemical profiles were routinely monitored. Contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI) scans were performed every 2–3 cycles of PD-1 inhibitor therapy. Overall survival (OS) was defined as the time interval from the first administration of PD-1 inhibitors to tumor-related death.
Construction of NIIS
First, prognostic biomarkers associated with nutritional-immune-inflammatory status were identified via univariate Cox regression analysis. Variables with P < 0.05 were retained for further analysis. Subsequently, a least absolute shrinkage and selection operator (LASSO) Cox regression model was applied to evaluate the prognostic significance of these biomarkers, selecting variables with non-zero coefficients. Finally, the nutritional-immune-inflammatory prognostic score (NIIS) was calculated based on the retained variables.
Validation of Prognostic Value of NIIS
To investigate the association between the NIIS and clinicopathological characteristics, Wilcoxon rank-sum tests were performed to compare NIIS across subgroups stratified by clinicopathological features. The predictive value of the NIIS for 1-, 2-, and 3-year overall survival (OS) in hepatocellular carcinoma (HCC) patients was evaluated using receiver operating characteristic (ROC) curves in both the training and verification group. Patients were stratified into high-risk and low-risk groups based on the median NIIS as the cut-off value. Survival differences and OS between these groups were analyzed using Kaplan-Meier curves and Log rank tests. Univariate and multivariate Cox proportional hazards regression analyses were conducted to identify independent prognostic factors associated with OS in HCC.
Construction and Validation of the Nomogram
Prognostic nomogram for overall survival (OS) was constructed in the training cohort using multivariate Cox regression analysis with backward stepwise selection based on the minimal Akaike Information Criterion (AIC) value. The predictive performance of the nomogram was validated in both training and verification groups through time-dependent area under the receiver operating characteristic curve (AUC) and calibration plots. Clinical decision curve analysis (DCA) was employed to compare the clinical utility of the nomogram with the Barcelona Clinic Liver Cancer (BCLC) staging system.
Statistical Analysis
Continuous variables with non-normal distributions were described using medians and interquartile ranges (IQRs). Independent two-group comparisons of continuous variables were performed using t-tests, while categorical variables were analyzed using Chi-square tests. Survival outcomes were evaluated via the Kaplan-Meier method, with between-group differences assessed by Log rank tests. Univariate and multivariate Cox proportional hazards regression models were employed to identify prognostic factors associated with overall survival (OS), with hazard ratios (HRs) and 95% confidence intervals (CIs) calculated. All statistical analyses were conducted using SPSS 24.0 (IBM Corp)., GraphPad Prism 9.5 (GraphPad Software), and R software (version 4.3.0; R Foundation). A two-sided P < 0.05 was considered statistically significant.
Results
Baseline Characteristics of Patients
This study included a total of 355 HCC patients. The median age of the patients was 55 years (48–64), with 310 males (87.3%) and 45 females (12.7%). Most patients had hepatitis B virus (HBV) infection (82.3%), were classified as BCLC stage C (77.7%), and had Child-Pugh grade A (81.4%). The median overall survival (OS) for the entire cohort was 16.03 months (95% CI: 14.62–17.22), with 1-year, 2-year, and 3-year OS rates of 66.2%, 31.2%, and 17.3%, respectively. Detailed baseline characteristics of the overall cohort (n=355), training group (n=249), and verification group (n=106) are shown in Table 1. Baseline characteristics were well-balanced between the two groups.
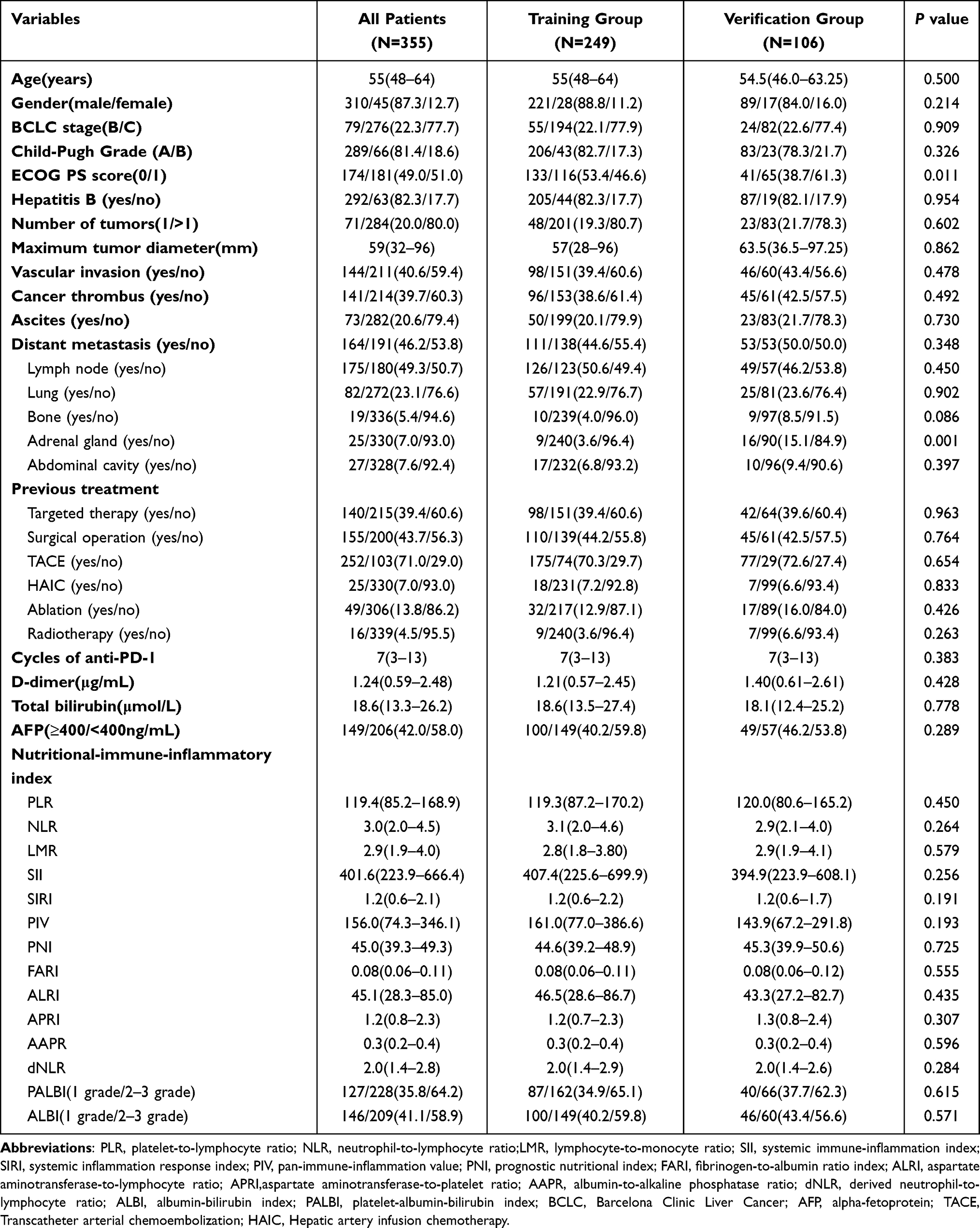 |
Table 1 Baseline Clinical Characteristics of Patients in the Training and Verification Groups |
Development of the NIIS Model
This study collected 14 nutritional-immune-inflammatory indicators. Kaplan-Meier curve analysis revealed that HCC patients with lower PLR, NLR, SII, SIRI, PIV, FARI, ALRI, APRI and dNLR, as well as higher LMR, AAPR, PNI, and ALBI/PALBI grade 1 had significantly improved OS (Figure 1).Univariate Cox regression analysis further identified PLR, NLR, SII, ALRI, APRI, PALBI, ALBI, and AAPR as independent prognostic factors for OS (P < 0.05) (Table 2). These eight variables were included in the least absolute shrinkage and selection operator (LASSO) Cox regression analysis, which revealed that only ALRI, APRI, PALBI, and AAPR had non-zero coefficients and were associated with survival outcomes in HCC patients treated with PD-1 inhibitors (Figure 2A and B).The nutritional-immune-inflammatory score (NIIS) was constructed using the following formula:Risk score = ALRI × 0.0023979 + APRI × 0.0433094 + PALBI × 0.6318392 − AAPR × 0.9802759.
 |
Table 2 Univariate Cox Regression Analysis of Fourteen Indicators |
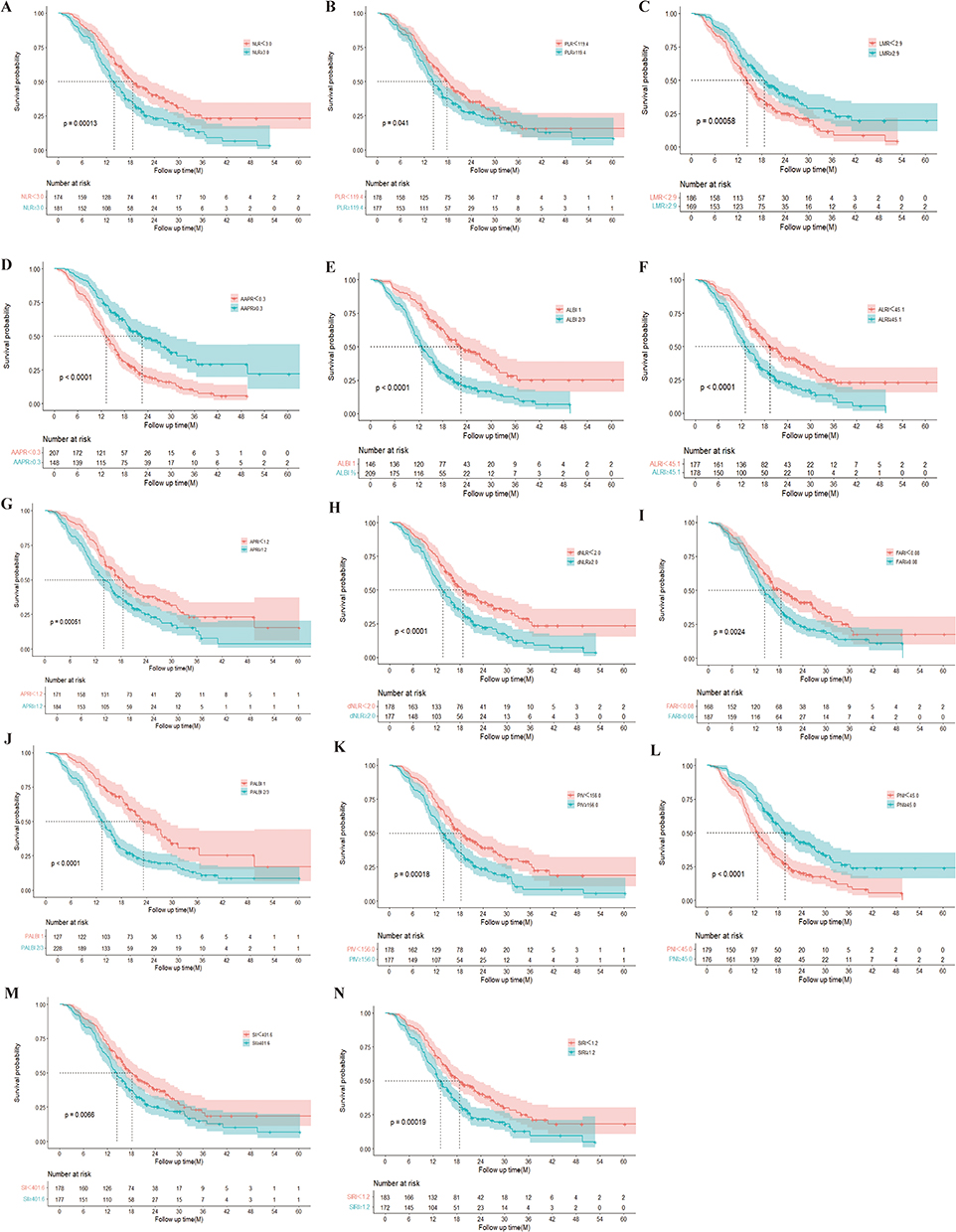 |
Figure 1 Kaplan-Meier Curves of Overall Survival (OS) Stratified by Fourteen Indicators in HCC Patients. (A) NLR (B) PLR (C) LMR (D) AAPR (E) ALBI (F) ALRI (G) APRI (H) dNLR (I) FARI (J) PALBI (K) PIV (L) PNI (M)SII (N) SIRI. Abbreviations: PLR, platelet-to-lymphocyte ratio; NLR, neutrophil-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; SII, systemic immune-inflammation index; SIRI, systemic inflammation response index; PIV, pan-immune-inflammation value; PNI, prognostic nutritional index; FARI, fibrinogen-to-albumin ratio index; ALRI, aspartate aminotransferase-to-lymphocyte ratio; APRI,aspartate aminotransferase-to-platelet ratio; AAPR, albumin-to-alkaline phosphatase ratio; dNLR, derived neutrophil-to-lymphocyte ratio; ALBI, albumin-bilirubin index; PALBI, platelet-albumin-bilirubin index; HCC, Hepatocellular Carcinoma. |
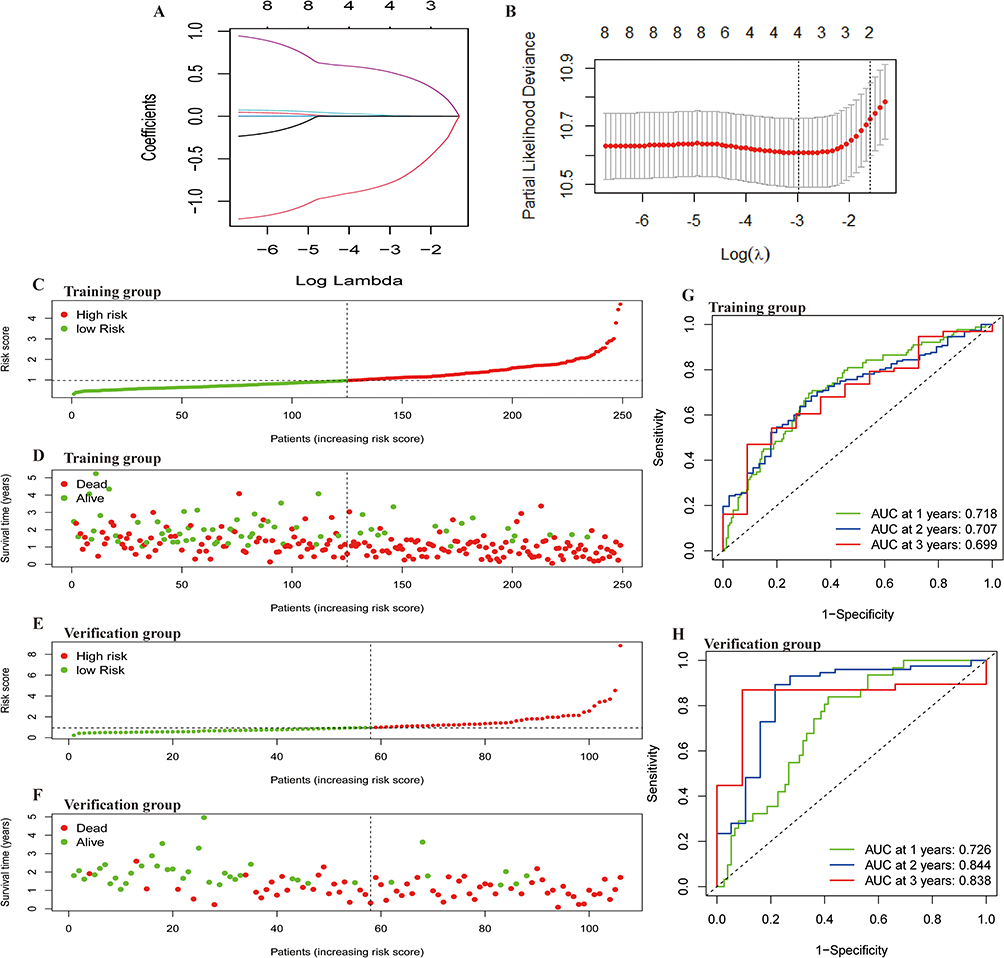 |
Figure 2 Construction of the NIIS Using LASSO Cox Regression Model. (A) Partial Likelihood Deviance Plot of LASSO Coefficients. Red dots represent partial likelihood deviance values, while gray lines indicate standard error (SE). The vertical dashed line denotes the optimal lambda value selected based on the 1-SE criterion. (B) Minimum Absolute Shrinkage and Selection Operator (LASSO) coefficient profile for 14 indicators (C and D) Risk Factor Plot for the Training group (E and F) Risk Factor Plot for the Verification group (G) Receiver Operating Characteristic (ROC) Curves for Predicting 1-, 2-, and 3-Year Overall Survival (OS) in the Training group (H) ROC Curves for Predicting 1-, 2-, and 3-Year OS in the Verification group. |
Validation of the Prognostic Value of the NIIS
This study constructed risk factor plots to evaluate the association between NIIS risk scores and patient survival. In the training group, higher risk scores were associated with poorer survival, with deceased patients exhibiting higher risk scores than surviving patients (Figure 2C and D). Similar results were observed in the verification group (Figure 2E and F). The predictive performance of the NIIS model was evaluated using ROC curves. In the training group, the AUC values for 1-year, 2-year, and 3-year OS were 0.718, 0.707, and 0.699, respectively (Figure 2G). In the verification group, the AUC values for 1-year, 2-year, and 3-year OS were 0.726, 0.844, and 0.838, respectively (Figure 2H), indicating good predictive performance of the NIIS model.The relationship between NIIS and clinicopathological characteristics was further evaluated. Patients with Child-Pugh grade B (Figure 3D), BCLC stage C (Figure 3E), multiple tumors (>1) (Figure 3G), tumor size ≥5 cm (Figure 3H), tumor thrombus (Figure 3I), vascular invasion (Figure 3K), and AFP ≥400 ng/mL (Figure 3L) exhibited significantly higher NIIS. No significant differences were observed in, sex (Figure 3A), age (Figure 3B), PS score (Figure 3C), HBV status (Figure 3F), or distant metastasis (Figure 3J), suggesting that the NIIS correlates with adverse clinical and tumor features.Using the median NIIS as the cutoff, patients were stratified into high-risk and low-risk groups. Kaplan-Meier analysis with Log rank tests revealed significantly shorter OS in the high-risk group compared to the low-risk group in both the traininggroup (P=1.764×10^-8; Figure 3M) and verification group (P=2.775×10^-6; Figure 3O). Univariate Cox regression analysis (Table 3) identified factors with P<0.1 for inclusion in multivariate Cox analysis. Multivariate Cox regression results demonstrated that a high NIIS was an independent prognostic risk factor for OS in HCC patients in the training group (HR=1.565, 95% CI: 1.273–1.925, P<0.001; Figure 3N), with similar findings in the verification group (HR=1.341, 95% CI: 1.065–1.687, P=0.012; Figure 3P). These results confirm the robust predictive value of the NIIS for survival in HCC patients treated with PD-1 inhibitors.
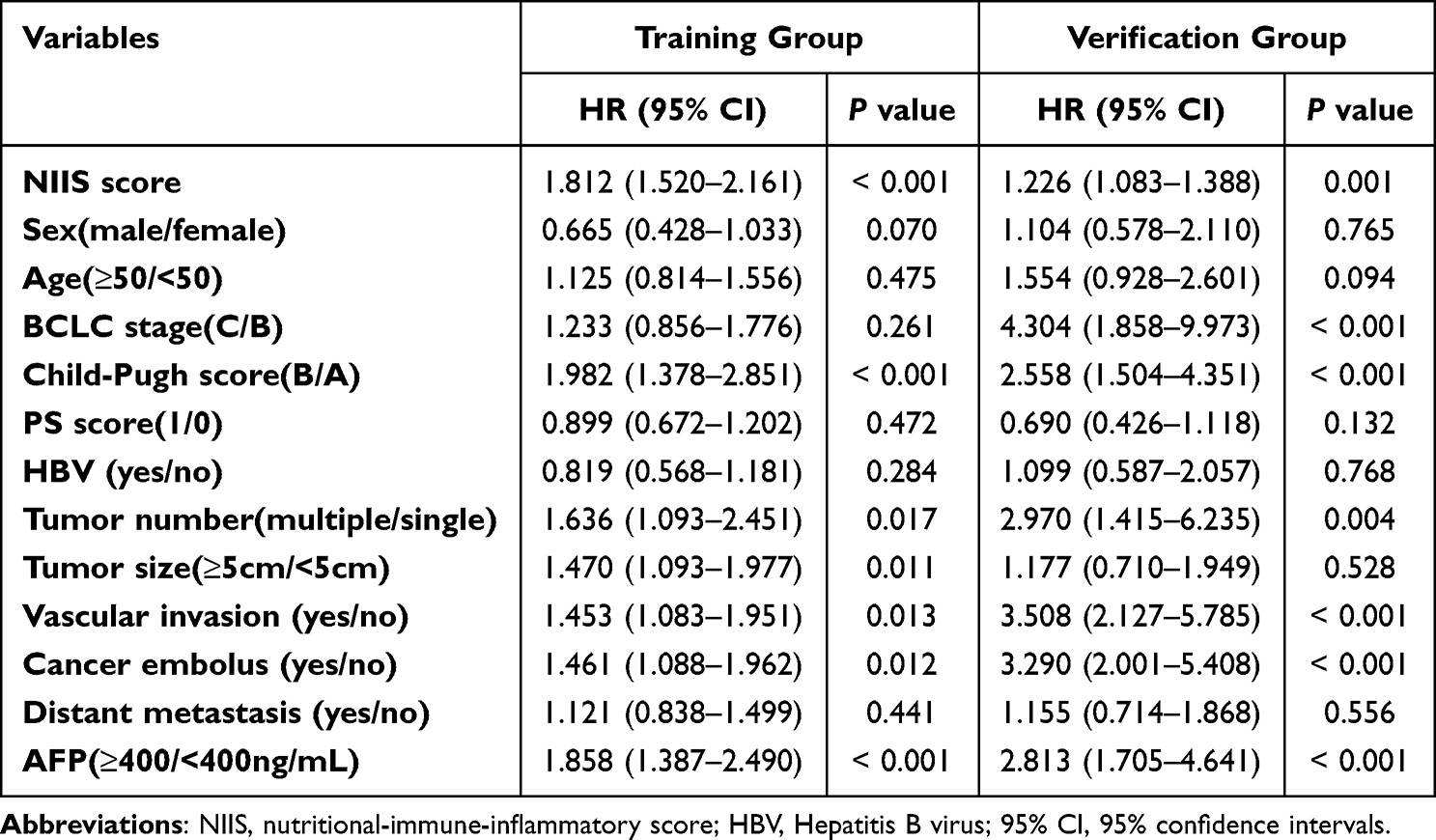 |
Table 3 Results of Univariate Survival Analysis in Training and Verification Groups |
 |
Figure 3 Analysis of NIIS Distribution Differences Across Clinicopathological Features and Prognostic Significance. (A–L) Distribution of NIIS Across Different Clinicopathological Features, comparisons between groups were performed using the Wilcoxon test: P < 0.05*, P < 0.01**, P < 0.001***, “ns” indicates no significant difference. (M and N) Kaplan-Meier Curves and Multivariate Cox Regression Forest Plot for OS by NIIS Risk Groups in the Training group. (O and P) Kaplan-Meier Curves and Multivariate Cox Regression Forest Plot for OS by NIIS Risk Groups in the Verification group. |
Construction and Validation of the NIIS Nomogram
Based on the Akaike Information Criterion (AIC) values, the NIIS score, sex, Child-Pugh score, tumor number, tumor size, vascular invasion, tumor thrombus, and AFP were included to construct a nomogram for predicting OS (Figure 4A). To compare the predictive accuracy of the NIIS model and the Barcelona Clinic Liver Cancer (BCLC) staging system, time-dependent receiver operating characteristic (ROC) area under the curve (AUC) analysis was performed. Results showed that the NIIS model exhibited significantly higher AUC values than the BCLC staging system in the training group (Figure 4B), with similar findings in the verification group (Figure 4C). Calibration curves demonstrated good consistency between predicted and observed outcomes (Figure 5A–F). Further decision curve analysis (DCA) was conducted to evaluate the clinical utility of the nomogram. In the training group, the NIIS score-based nomogram outperformed the BCLC staging system in predicting survival outcomes for HCC patients treated with PD-1 inhibitors (Figure 5G–I), with analogous results observed in the verification group (Figure 5J–L).
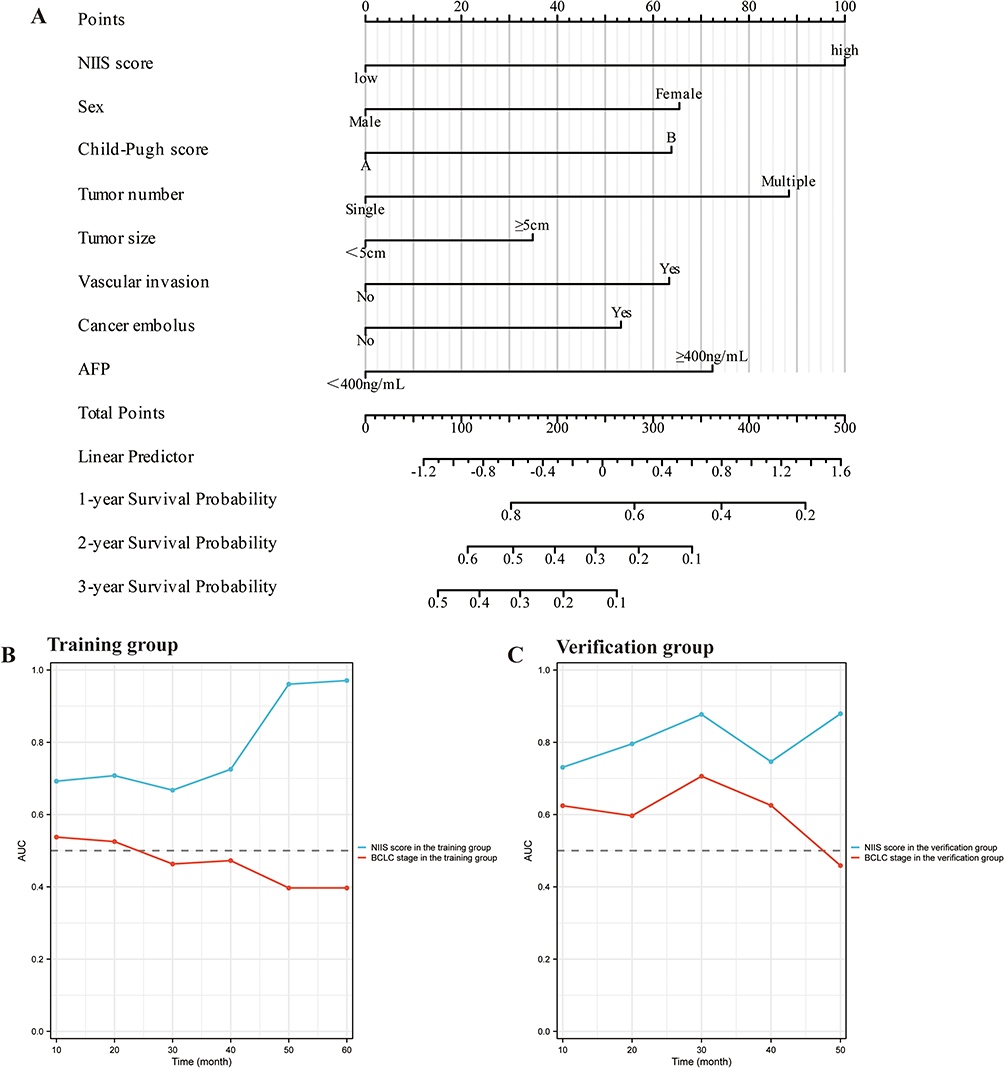 |
Figure 4 Construction and validation of the nomograms. (A) Nomogram Incorporating NIIS and Clinical Indicators for Predicting OS in the Training group.(B and C) Comparison of Time-Dependent AUC Between NIIS Nomogram and BCLC Staging System for Predicting OS in Training and Verification groups. |
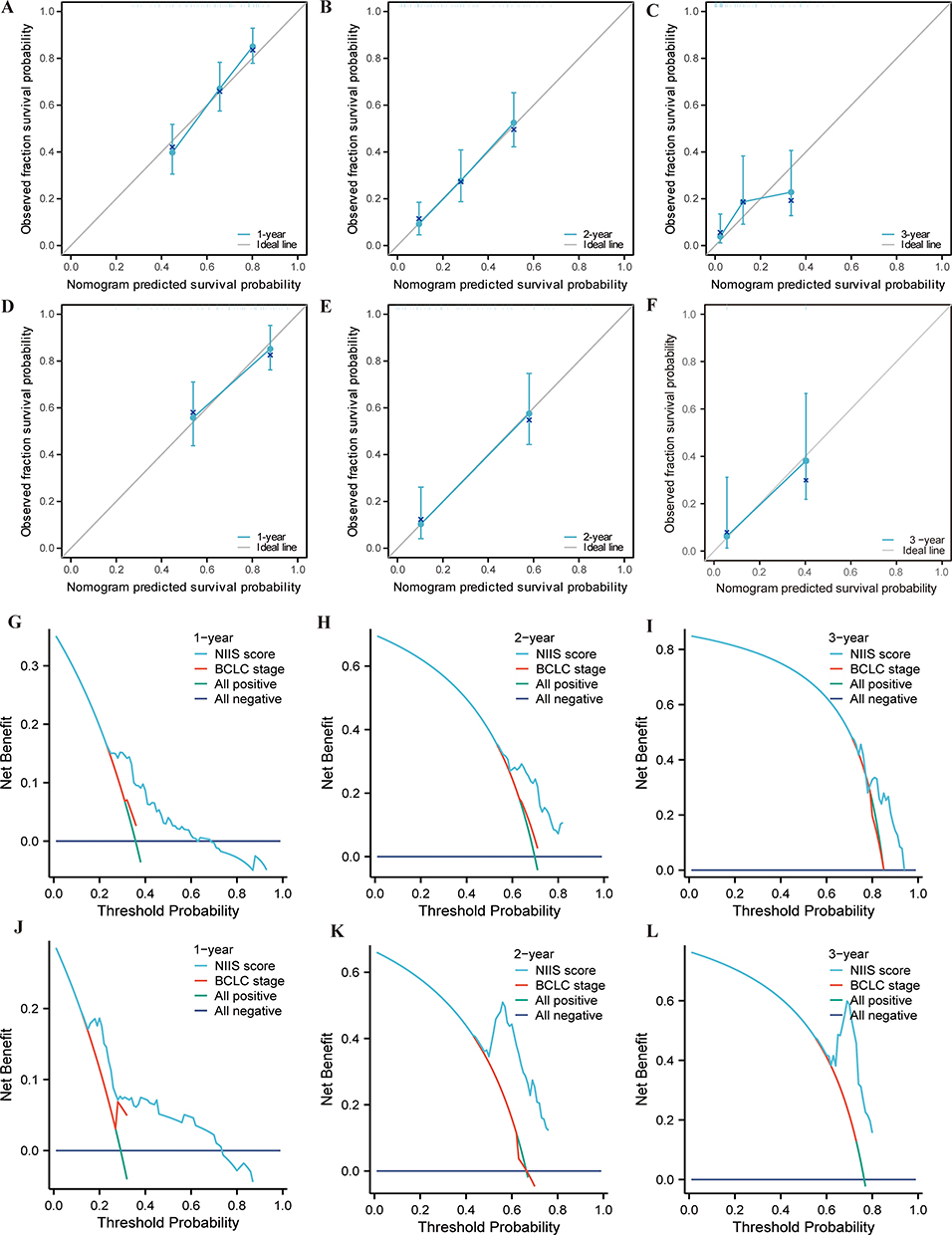 |
Figure 5 Calibration Curves and Decision Curve Analysis (DCA) of the Nomogram for Predicting OS. (A–C) Calibration Curves for Nomogram-Predicted Versus Observed 1-, 2-, and 3-Year OS in the Training group. (D–F) Calibration Curves for Nomogram-Predicted Versus Observed 1-, 2-, and 3-Year OS in the Verification group. The dashed line of 45° represents the perfect prediction of the nomogram. (G–I) DCA comparing the Nomogram and BCLC Staging System for 1-Year, 2-Year, and 3-Year OS in the Training group. (J–L) DCA comparing the Nomogram and BCLC Staging System for 1-Year, 2-Year, and 3-Year OS in the Verification group. |
Discussion
Currently, immunotherapy has been widely applied in various cancers, and programmed cell death protein 1 (PD-1) inhibitors, as primary immune checkpoint inhibitors, have become a mainstay treatment for HCC patients.31 However, due to interpatient heterogeneity, response rates in clinical practice remain suboptimal. Although PD-L1 expression may guide treatment decisions,32 its detection process is complex and has limitations. Therefore, there is an urgent need for effective predictive biomarkers to screen beneficiary populations and guide therapeutic strategies. This study developed and validated a novel nutritional-immune-inflammatory score (NIIS) based on clinical peripheral blood biochemical parameters to predict survival outcomes in HCC patients receiving PD-1 inhibitor therapy by integrating key prognostic biomarkers.
The interaction between nutrition, immunity, inflammation, and tumors exhibits specific associations. Current studies highlight the critical roles of systemic inflammation, immune dysregulation, and nutritional status in modulating immunotherapy responses.33,34 Immune-inflammatory biomarkers such as the systemic inflammation response index (SIRI), advanced lung cancer inflammation index (ALI), C-reactive protein (CRP), and neutrophil-to-lymphocyte ratio (NLR) have been reported to predict prognosis in cancer patients receiving immunotherapy.35–38 Nutritional indices, including the cholesterol-modified prognostic nutritional index (CPNI), body mass index (BMI), platelet-to-albumin ratio (PAR), geriatric nutritional risk index (GNRI), and Controlling Nutritional Status (CONUT) score, have also emerged as potential prognostic biomarkers in cancer therapy.39–42 However, individual biomarkers fail to achieve accurate prognostic risk stratification for HCC patients treated with PD-1 inhibitors, necessitating the integration of these biomarkers into a novel predictive model.This study comprehensively collected peripheral blood-derived nutritional, immune, and inflammatory indicators to construct a prognostic scoring model, evaluating its prognostic value and clinical relevance in HCC patients undergoing PD-1 inhibitor therapy. Key findings revealed that PLR, NLR, SII, SIRI, PIV, FARI, ALRI, APRI, dNLR, LMR, AAPR, PNI, ALBI, and PALBI were significantly associated with OS in HCC patients. The NIIS model demonstrated robust prognostic stratification power, validated in both training and verification groups, and exhibited predictive value for OS in PD-1 inhibitor-treated HCC patients. Furthermore, compared to the conventional Barcelona Clinic Liver Cancer (BCLC) staging system, the NIIS model demonstrated superior predictive performance. The nomogram integrating the NIIS and clinical factors enhanced the predictive capability for OS in HCC patients receiving PD-1 inhibitors.
The NIIS comprises four clinically accessible indicators—ALRI, APRI, PALBI, and AAPR—whose individual predictive potential has been validated across multiple malignancies.ALRI, reflecting nutritional and immune-inflammatory status, combines aspartate aminotransferase and lymphocyte counts. Liao et al demonstrated that postoperative ALRI accurately predicts clinical outcomes in HCC patients after hepatectomy,43 while Toshiya Miyata et al linked elevated ALRI levels to shorter OS and disease-free survival (DFS) in colorectal cancer patients undergoing curative resection.44 These findings align with our results showing poorer OS in high-ALRI subgroups.APRI, integrating aspartate aminotransferase and platelet counts, reflects nutritional and immune status. Chen et al confirmed APRI’s prognostic value for OS and progression-free survival (PFS) in colorectal cancer patients with liver metastasis, where high APRI correlated with worse outcomes and increased recurrence risk. Single-cell RNA sequencing in high-APRI subgroups revealed elevated epithelial cell malignancy, enrichment of inflammatory-like cancer-associated fibroblasts (CAFs) and SPP1+ macrophages, and suppressed T-cell functionality. Multiplex immunohistochemistry/immunofluorescence (mIHC/IF) further demonstrated increased PD1+ CD4+ T cells, FOXP3+ CD4+ T cells, PD1+ CD8+ T cells, FOXP3+ CD8+ T cells, SPP1+ macrophages, and inflammatory CAFs in both intratumoral and peritumoral regions,45 mechanistically validating APRI’s predictive role—consistent with our findings.AAPR, calculated as albumin-to-alkaline phosphatase ratio, reflects nutritional and immune status. Multiple studies associate higher AAPR with improved prognosis across cancers, corroborated by our observation of prolonged OS in high-AAPR HCC patients.46–48 PALBI, a refinement of the ALBI first proposed by Oikonomou et al,49 incorporates platelet count to enhance prognostic accuracy in cirrhosis and portal hypertension. Validated as an independent prognostic biomarker for HCC,50,51 our study confirmed worse OS in high-PALBI grades, aligning with prior evidence.These parameters, routinely assessed in HCC clinical practice, ensure the NIIS simplicity and feasibility for real-world implementation.
The NIIS model demonstrated robust predictive performance for OS in HCC patients treated with PD-1 inhibitors. In the training group, the AUC values for predicting 1-year, 2-year, and 3-year OS were approximately 0.7, while the verification group achieved AUC values of 0.726, 0.844, and 0.838, respectively, surpassing previous studies.52–54 The NIIS exhibited strong prognostic stratification, with higher scores significantly associated with adverse clinical features such as advanced tumor stage, vascular invasion, and elevated AFP levels, and was identified as an independent prognostic risk factor for OS in HCC patients. Notably, the NIIS outperformed the widely used BCLC staging system in predicting 1-, 2-, and 3-year OS, as confirmed by time-dependent AUC comparisons in both training and verification groups. A clinically practical nomogram was constructed by integrating the NIIS with established prognostic variables (Child-Pugh grade, tumor burden, AFP), demonstrating superior discrimination and calibration accuracy across diverse clinical scenarios. DCA revealed higher net benefit, further supporting its potential utility in personalized therapeutic decision-making, particularly for identifying patients likely to benefit from PD-1 inhibitor therapy.This study expands upon prior research on inflammatory biomarkers (eg NLR, PLR) by demonstrating that a composite score integrating multidimensional biological processes (nutrition-immunity-inflammation) provides more comprehensive prognostic insights. These findings align with recent advances in understanding the tumor immune microenvironment, where chronic inflammation and malnutrition synergistically impair antitumor immunity.55,56 The NIIS ability to capture these complex biological interactions likely underlies its superior predictive performance compared to single biomarkers or traditional staging systems.
This study has several limitations. First, it is a single-center retrospective study. Although internal validation via bootstrap resampling and external validation in an independent cohort enhanced reliability, prospective multicenter studies are still required to further validate its generalizability. Second, all included patients were of Chinese ethnicity, necessitating additional evaluation in diverse ethnic populations. Third, the lack of objective response rate (ORR) and disease control rate (DCR) data limits our ability to evaluate whether the NIIS possesses predictive value for treatment response in addition to its prognostic utility. Future prospective studies should incorporate standardized radiological response assessments to address this question. Furthermore, tumor molecular biomarkers such as programmed death-ligand 1 (PD-L1) expression and tumor mutational burden (TMB) were not incorporated, warranting further refinement of the predictive model. Finally, molecular mechanisms underlying immunotherapy responses remain unexplored, and future studies should investigate these pathways to elucidate prognostic heterogeneity. If validated in larger multicenter cohorts, the NIIS score could be integrated into treatment decision-making to identify highrisk patients who may benefit from TKIs instead of PD-1 monotherapy, intensified regimens (eg, PD-1 + TKI combinations), clinical trial enrollment, or early palliative care integration.
Conclusion
In conclusion, the NIIS and its associated nomogram provide a clinically practical tool for risk stratification in HCC immunotherapy. By incorporating multidimensional biological profiling to address the limitations of conventional staging systems, this approach may facilitate the development of personalized treatment strategies and optimize patient selection for PD-1 inhibitor therapy.
Data Sharing Statement
All the data generated or analysed during this study are included in this article (and its Supplementary Information Files). Available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the Second Affiliated Hospital of Nanchang University, China, The Examination and Approval No. Review [2020] No. (095). In view of the nature of the retrospective study, this study does not require the patient’s informed consent. In any case, patient data confidentiality was guaranteed.
Consent for Publication
All the authors have agreed to publish this manuscript.
Acknowledgments
We are very grateful for the tireless efforts and dedication of all the authors who participated in the conception, execution, and analysis of this study, and we are also very grateful to the editors and reviewers and staff for their guidance and input on this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding for this study was obtained from the National Natural Science Foundation of China, under Grant Number 82460609, Science and Technology Project of Jiangxi Provincial Department of Education (No.GJJ2400117), 2024 Changyi Leading Research(ZL049) and the Beijing science and technology innovation medical development foundation(KC2023-JX-0288-FZ127).
Disclosure
The authors report no potential conflicts of interest in this work.
References
1. Singal AG, Kanwal F, Llovet JM. Global trends in hepatocellular carcinoma epidemiology: implications for screening, prevention and therapy. Nat Rev Clin Oncol. 2023;20(12):864–884. doi:10.1038/s41571-023-00825-3
2. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Chidambaranathan-Reghupaty S, Fisher PB, Sarkar D. Hepatocellular carcinoma (HCC): epidemiology, etiology and molecular classification. Adv Cancer Res. 2021;149:1–61.
4. Yang C, Zhang H, Zhang L, et al. Evolving therapeutic landscape of advanced hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2023;20(4):203–222. doi:10.1038/s41575-022-00704-9
5. Singal AG, Kudo M, Bruix J. Breakthroughs in hepatocellular carcinoma therapies. Clin Gastroenterol Hepatol. 2023;21(8):2135–2149. doi:10.1016/j.cgh.2023.01.039
6. Giraud J, Chalopin D, Blanc JF, Saleh M. Hepatocellular carcinoma immune landscape and the potential of immunotherapies. Front Immunol. 2021;12:655697. doi:10.3389/fimmu.2021.655697
7. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label Phase 2 trial. Lancet Oncol. 2018;19(7):940–952. doi:10.1016/S1470-2045(18)30351-6
8. El-Khoueiry AB, Sangro B, Yau T, et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet. 2017;389(10088):2492–2502. doi:10.1016/S0140-6736(17)31046-2
9. Zhou Y, Liu Z, Yu A, Zhao G, Chen B. Immune checkpoint inhibitor combined with antiangiogenic agent synergistically improving the treatment efficacy for solid tumors. ImmunoTargets Ther. 2024;13:813–829. doi:10.2147/ITT.S494670
10. Pavelescu LA, Enache RM, Roşu OA, Profir M, Creţoiu SM, Gaspar BS. Predictive biomarkers and resistance mechanisms of checkpoint inhibitors in malignant solid tumors. Int J Mol Sci. 2024;25(17):9659. doi:10.3390/ijms25179659
11. Llovet JM, Castet F, Heikenwalder M, et al. Immunotherapies for hepatocellular carcinoma. Nat Rev Clin Oncol. 2022;19(3):151–172. doi:10.1038/s41571-021-00573-2
12. Xing R, Gao J, Cui Q, Wang Q. Strategies to improve the antitumor effect of immunotherapy for hepatocellular carcinoma. Front Immunol. 2021;12:783236. doi:10.3389/fimmu.2021.783236
13. Yu SJ. Immunotherapy for hepatocellular carcinoma: recent advances and future targets. Pharmacol Ther. 2023;244:108387. doi:10.1016/j.pharmthera.2023.108387
14. Zhao H, Wu L, Yan G, et al. Inflammation and tumor progression: signaling pathways and targeted intervention. Signal Transduct Target Ther. 2021;6(1):263. doi:10.1038/s41392-021-00658-5
15. Zhang Y, Chen Y, Guo C, Li S, Huang C. Systemic immune-inflammation index as a predictor of survival in non-small cell lung cancer patients undergoing immune checkpoint inhibition: a systematic review and meta-analysis. Crit Rev Oncol/Hematol. 2025;210:104669. doi:10.1016/j.critrevonc.2025.104669
16. Yarahmadi HB, Shahryari K, Bozorgi M, et al. Dietary inflammatory index and the risk of esophageal cancer: a systematic review and meta-analysis. BMC Cancer. 2025;25(1):826. doi:10.1186/s12885-025-14199-5
17. Xie Y, Yu Q, Zhu Y, et al. The value of peripheral blood inflammation markers in risk assessment and prediction of lung cancer. Future Science OA. 2025;11(1):2476870. doi:10.1080/20565623.2025.2476870
18. Wu Z, Zhang Z, Gu C. Prognostic and clinicopathological impact of systemic inflammation response index (SIRI) on patients with esophageal cancer: a meta-analysis. Syst Rev. 2025;14(1):104. doi:10.1186/s13643-025-02847-7
19. Wind KL, Steffensen JH, Jakobsen AV, Kronborg C, Spindler KG. Prognostic significance of pre-treatment immune-inflammation biomarkers in anal cancer: a study combining real-world data and a meta-analysis. Int J Cancer. 2025;157(1):193–200. doi:10.1002/ijc.35404
20. Ma L, Mao JH, Barcellos-Hoff MH. Systemic inflammation in response to radiation drives the genesis of an immunosuppressed tumor microenvironment. Neoplasia. 2025;64:101164. doi:10.1016/j.neo.2025.101164
21. Aslan V, Karabörk Kılıç AC, Rustamova Cennet N, et al. Splenic index score as a predictor of outcomes in metastatic non small cell lung cancer patients treated with immune checkpoint inhibitors. Sci Rep. 2025;15(1):15781. doi:10.1038/s41598-025-00708-w
22. Artusa F, Lamatsch S, Phan MD, et al. Soluble urokinase plasminogen activator receptor predicts survival and hepatic decompensation in advanced hepatocellular carcinoma. Liver Int. 2025;45(6):e70121. doi:10.1111/liv.70121
23. Zhang X, Hu X, Qian L, et al. The association between nutritional-inflammatory status and chronic kidney disease prognosis: a population-based study. Renal Failure. 2025;47(1):2471016. doi:10.1080/0886022X.2025.2471016
24. Nobs SP, Zmora N, Elinav E. Nutrition regulates innate immunity in health and disease. Ann Rev Nutr. 2020;40:189–219. doi:10.1146/annurev-nutr-120919-094440
25. Chen C, Xu SJ, Zhang ZF, et al. Severe postoperative complications after minimally invasive esophagectomy reduce the long-term prognosis of well-immunonutrition patients with locally advanced esophageal squamous cell carcinoma. Ann Med. 2025;57(1):2440622. doi:10.1080/07853890.2024.2440622
26. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature07205
27. Kennel KB, Bozlar M, De Valk AF, Greten FR. Cancer-associated fibroblasts in inflammation and antitumor immunity. Clinical Cancer Res. 2023;29(6):1009–1016. doi:10.1158/1078-0432.CCR-22-1031
28. Ouyang H, Xiao B, Huang Y, Wang Z. Baseline and early changes in the neutrophil-lymphocyte ratio (NLR) predict survival outcomes in advanced colorectal cancer patients treated with immunotherapy. Int Immunopharmacol. 2023;123:110703. doi:10.1016/j.intimp.2023.110703
29. Gupta V, Chaudhari V, Shrikhande SV, Bhandare MS. Does Preoperative Serum Neutrophil to Lymphocyte Ratio (NLR), Platelet to Lymphocyte Ratio (PLR), and Lymphocyte to Monocyte Ratio (LMR) predict prognosis following radical surgery for pancreatic adenocarcinomas? Results of a retrospective study. J Gastrointestinal Cancer. 2022;53(3):641–648. doi:10.1007/s12029-021-00683-1
30. Du J, Huang Z. NLR stability predicts response to immune checkpoint inhibitors in advanced hepatocellular carcinoma. Sci Rep. 2024;14(1):19583. doi:10.1038/s41598-024-68048-9
31. Li Q, Han J, Yang Y, Chen Y. PD-1/PD-L1 checkpoint inhibitors in advanced hepatocellular carcinoma immunotherapy. Front Immunol. 2022;13:1070961. doi:10.3389/fimmu.2022.1070961
32. Doroshow DB, Bhalla S, Beasley MB, et al. PD-L1 as a biomarker of response to immune-checkpoint inhibitors. Nat Rev Clin Oncol. 2021;18(6):345–362. doi:10.1038/s41571-021-00473-5
33. Marques P, de Vries F, Dekkers OM, Korbonits M, Biermasz NR, Pereira AM. Serum inflammation-based scores in endocrine tumors. J Clin Endocrinol Metab. 2021;106(10):e3796–e819. doi:10.1210/clinem/dgab238
34. Kuang T, Qiu Z, Wang K, Zhang L, Dong K, Wang W. Pan-immune inflammation value as a prognostic biomarker for cancer patients treated with immune checkpoint inhibitors. Front Immunol. 2024;15:1326083. doi:10.3389/fimmu.2024.1326083
35. Zhang X, Wang D, Sun T, Li W, Dang C. Advanced lung cancer inflammation index (ALI) predicts prognosis of patients with gastric cancer after surgical resection. BMC Cancer. 2022;22(1):684. doi:10.1186/s12885-022-09774-z
36. Yu X, Jiang W, Dong X, et al. Nomograms integrating the collagen signature and systemic immune-inflammation index for predicting prognosis in rectal cancer patients. BJS Open. 2024;8(2). doi:10.1093/bjsopen/zrae014
37. Kou J, Huang J, Li J, Wu Z, Ni L. Systemic immune-inflammation index predicts prognosis and responsiveness to immunotherapy in cancer patients: a systematic review and meta‑analysis. Clin Exp Med. 2023;23(7):3895–3905. doi:10.1007/s10238-023-01035-y
38. Ding Y, Liu Z, Li J, Niu W, Li C, Yu B. Predictive effect of the systemic inflammation response index (SIRI) on the efficacy and prognosis of neoadjuvant chemoradiotherapy in patients with locally advanced rectal cancer. BMC Surgery. 2024;24(1):89. doi:10.1186/s12893-024-02384-5
39. Shi J, Liu T, Ge Y, et al. Cholesterol-modified prognostic nutritional index (CPNI) as an effective tool for assessing the nutrition status and predicting survival in patients with breast cancer. BMC Med. 2023;21(1):512. doi:10.1186/s12916-023-03225-7
40. Qiu J, Yu Y, Wang Z, Hong L, Shao L, Wu J. Comprehensive analysis of the prognostic value of pre-treatment nutritional indicators in elderly rectal cancer patients. Sci Rep. 2024;14(1):22078. doi:10.1038/s41598-024-73123-2
41. Ding P, Wu J, Wu H, et al. Inflammation and nutritional status indicators as prognostic indicators for patients with locally advanced gastrointestinal stromal tumors treated with neoadjuvant imatinib. BMC Gastroenterol. 2023;23(1):23. doi:10.1186/s12876-023-02658-x
42. Chen J, Song P, Peng Z, et al. The Controlling Nutritional Status (CONUT) score and prognosis in malignant tumors: a systematic review and meta-analysis. Nutr Cancer. 2022;74(9):3146–3163. doi:10.1080/01635581.2022.2059091
43. Liao M, Sun J, Zhang Q, et al. A novel post-operative ALRI model accurately predicts clinical outcomes of resected hepatocellular carcinoma patients. Front Oncol. 2021;11:665497. doi:10.3389/fonc.2021.665497
44. Miyata T, Hayama T, Ozawa T, Nozawa K, Misawa T, Fukagawa T. Predicting prognosis in colorectal cancer patients with curative resection using albumin, lymphocyte count and RAS mutations. Sci Rep. 2024;14(1):14428. doi:10.1038/s41598-024-65457-8
45. Chen Q, Deng Y, Li Y, et al. Association of preoperative aspartate aminotransferase to platelet ratio index with outcomes and tumour microenvironment among colorectal cancer with liver metastases. Cancer Lett. 2024;588:216778. doi:10.1016/j.canlet.2024.216778
46. Zhang X, Xin Y, Chen Y, Zhou X. Prognostic effect of albumin-to-alkaline phosphatase ratio on patients with hepatocellular carcinoma: a systematic review and meta-analysis. Sci Rep. 2023;13(1):1808. doi:10.1038/s41598-023-28889-2
47. Zhang K, Dong S, Jing YH, et al. Albumin-to-alkaline phosphatase ratio serves as a prognostic indicator in unresectable pancreatic ductal adenocarcinoma: a propensity score matching analysis. BMC Cancer. 2020;20(1):541. doi:10.1186/s12885-020-07023-9
48. Zhang F, Lu SX, Hu KS, et al. Albumin-to-alkaline phosphatase ratio as a predictor of tumor recurrence and prognosis in patients with early-stage hepatocellular carcinoma undergoing radiofrequency ablation as initial therapy. Int J Hyperthermia. 2021;38(1):1–10.
49. Oikonomou T, Goulis L, Doumtsis P, Tzoumari T, Akriviadis E, Cholongitas E. ALBI and PALBI grades are associated with the outcome of patients with stable decompensated cirrhosis. Ann Hepatol. 2019;18(1):126–136. doi:10.5604/01.3001.0012.7904
50. Wang Q, Sheng S, Xiong Y, Han M, Jin R, Hu C. Machine learning-based model for predicting tumor recurrence after interventional therapy in HBV-related hepatocellular carcinoma patients with low preoperative platelet-albumin-bilirubin score. Front Immunol. 2024;15:1409443. doi:10.3389/fimmu.2024.1409443
51. Lee SK, Song MJ, Kim SH, Park M. Comparing various scoring system for predicting overall survival according to treatment modalities in hepatocellular carcinoma focused on Platelet-albumin-bilirubin (PALBI) and albumin-bilirubin (ALBI) grade: a nationwide cohort study. PLoS One. 2019;14(5):e0216173. doi:10.1371/journal.pone.0216173
52. Mei J, Sun XQ, Lin WP, et al. Comparison of the prognostic value of inflammation-based scores in patients with hepatocellular carcinoma after Anti-PD-1 therapy. J Inflamm Res. 2021;14:3879–3890. doi:10.2147/JIR.S325600
53. Zhang Y, Lu L, He Z, et al. C-reactive protein levels predict responses to PD-1 inhibitors in hepatocellular carcinoma patients. Front Immunol. 2022;13:808101. doi:10.3389/fimmu.2022.808101
54. Sun X, Mei J, Lin W, et al. Reductions in AFP and PIVKA-II can predict the efficiency of anti-PD-1 immunotherapy in HCC patients. BMC Cancer. 2021;21(1):775. doi:10.1186/s12885-021-08428-w
55. Cortellino S, D’Angelo M, Quintiliani M, Giordano A. Cancer knocks you out by fasting: cachexia as a consequence of metabolic alterations in cancer. J Cell Physiol. 2025;240(1):e31417. doi:10.1002/jcp.31417
56. Denk D, Greten FR. Inflammation: the incubator of the tumor microenvironment. Trends Cancer. 2022;8(11):901–914. doi:10.1016/j.trecan.2022.07.002
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.