Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 11
Essential Newborn Care and Associated Factors Among Obstetrical Care Providers in Awi Zone Health Facilities, Northwest Ethiopia: An Institutional-Based Cross-Sectional Study
Authors Ayenew A, Abebe M, Ewnetu M
Received 13 August 2020
Accepted for publication 16 October 2020
Published 11 November 2020 Volume 2020:11 Pages 449—458
DOI https://doi.org/10.2147/PHMT.S276698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Asteray Ayenew,1 Mahlet Abebe,2 Mesafint Ewnetu1
1Department of Midwifery, School of Health Sciences, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia; 2Department of Midwifery, School of Health Sciences, College of Medicine and Health Sciences, Mizan Tepi University, Mizan Teferi, Ethiopia
Correspondence: Asteray Ayenew Email [email protected]
Background: Each year, millions of newborns die as a result of birth asphyxia, infections, and complications of preterm birth. This burden of death is disproportionately concentrated in low-income countries including Ethiopia. As a result, the care given immediately after birth is crucial for making a successful transition from intrauterine to extrauterine function and to reduce neonatal mortality.
Methods: Facility-based cross-sectional study design was carried out on a sample size of 208 obstetrical care providers. A simple random sampling technique was used to select the study subjects. The data were collected through Interview-administered questionnaires and observational checklists. The data were entered into Epi-info version 7 and exported to SPSS 23 for analysis.
Results: A total of 201 obstetric care providers participated in the study, making a response rate of (96.6%). This study revealed that 62.7% of obstetric care providers practiced essential newborn care properly. The factors significantly associated were received in-service training (AOR = 2.7, 95% CI: 1.35, 5.51), level of education (AOR = 0.46, 95% CI: 0.22, 0.96), midwifery profession (AOR = 3.1, 95% CI: 1.35, 7.39), having good knowledge of essential newborn care (AOR = 2.1, 95% CI: 1.03, 4.49), availability of drugs for essential newborn care (AOR = 2.3, 95% CI: 1.16, 4.72), and availability of medical equipment to perform essential newborn care (AOR = 2, 95% CI: 1.01, 3.96).
Conclusion: The practice of essential newborn care was generally low. Having in-service training, midwifery profession, a good knowledge of essential newborn care, availability of drugs, level of education, and availability of medical equipment for essential newborn care were the determinant factors for essential newborn care practice. Improvement in essential newborn care practices could be attained through modifiable proven interventions like provision of in-service training, availed drugs, and medical equipment for essential newborn care.
Keywords: essential newborn care, obstetric care providers, Ethiopia
Background
Essential newborn care is the care provided to the neonate after birth within the delivery room by skilled personnel which includes drying and stimulating, assessing breathing, cord care, skin to skin contact, initiating exclusive breastfeeding, eye care, vitamin k provision, place of identification band and weighing.1
Birth is the main challenge for the newborn to settle successfully from the maternal womb to extrauterine life. The first few hours after birth are the most basic period in the life of an infant for better growth and development2 at which obstetric care providers have a significant role.3 Globally, every year 2.7 million neonates die which accounts 45%, 58%, 75% of under-5, infant, and neonatal mortality respectively.4,5 Among those global neonatal deaths, neonatal deaths in low and middle income countries accounted for most of the growing proportion of all under-five mortality.6 If the trend continues like this, the share of neonatal deaths to under-5 death is projected to increase from 45% in 2015 to 52% in 2030.7 According to the 2016 Ethiopia Demographic and Health Surveys (EDHS) report, the infant mortality rate was 48 per 1000 live births and the neonatal mortality rate is 29 per 1000 in Ethiopia.8
Another study conducted in Ethiopia on trends and determinants of neonatal mortality identified preterm birth, intrapartum events such as birth asphyxia, infections such as sepsis, and congenital malformations as a cause of early newborn neonatal mortality.9
Essential newborn care interventions to protect against newborn morbidity and mortality are, by using clean cord care, thermal care including drying and wrapping of the newborn immediately after delivery and delaying the newborn’s first bath for at least 24 h (or several days to reduce hypothermia risk), and initiation of breastfeeding within the first one hour of birth, management of immediate asphyxia, management of early sepsis.10 About 3 million lives could be saved each year with worldwide coverage of the evidence based solutions such as care during labor and around birth by skilled birth attendants. The “Every Newborn Action Plan” (ENAP) calls for an increased center of attention on the time around birth with targeted high impact interventions as a strategy for dropping not only newborn deaths but also maternal deaths and stillbirths, producing a triple return in investment.11 Even though there has been considerable progress over the last two decades on neonatal mortality, still, poor care during delivery and immediately after birth was largely responsible for the annual deaths of an estimated 2.5 million newborns in the first month of life in 2017.12 Generally, Ethiopia, like other sub-Saharan countries, has a high perinatal mortality and, specifically, the area of study Amhara regional state (Awi zone) is the first region with a high burden of perinatal mortality and stillbirth from all regional states of Ethiopia according to EDHS 2016.
Children who die within the first 28 days of birth suffer from circumstances, diseases of birth, and in the first days of life. Quality skilled care at birth would make certain that the newborn receives essential newborn care including drying and stimulating, assessment of breathing, cord care, skin to skin contact, early breast feeding, vitamin k provision, labeling, and weighing properly.13
Proper essential care of a newborn is significantly important for survival, growth, and development of a newborn.3 Little is known about practice and factors associated with the practice of essential care of the newborn in Ethiopia. As a result, this study aimed to assess the practice of essential newborn care and its associated factors among obstetrical care providers in the Awi zone, northwest Ethiopia, to develop effective strategies to promote care and baseline for further research.
Methods
Study Design and Study Participants
The facility-based cross-sectional study design was used in the governmental public health facilities of Awi Zone. The study period was from March 1 to April 15, 2019. The source population was all obstetrical care providers in the Awi zone who were working in the study area and the study population was all selected obstetrical care providers from the selected health facilities.
Study Area
The study was conducted in the Awi zone, Amhara region, northwest Ethiopia. It is located 449 km from Addis Ababa, the capital city of Ethiopia, and 114 km from Bahir Dar, the main city of the Amhara region. The zone is bordered on the west by the Benishangul–Gumuz Region, on the north by the North Gondar zone, and on the east by West Gojjam. Based on the 2007 census data, conducted by the Central Statistical Agency, the Awi zone has a total population of 1,220,316 in 2016, of whom 598,880 (49.1%) are men and 621,436 (50.9%) are women.14 In the zone there are 46 health centers and 5 hospitals that provide labor and delivery service for the community. Midwives, nurses, public health officers, and IESO are responsible for attending labor and delivery services and essential newborn care services in the zone. The zone had 496 obstetric care providers, and the annual institutional delivery of 25,606 attended by those obstetric care providers.
Sample Size and Sampling Procedure
A sample size of 208 was determined using the following formula;

Assumptions: n = required sample size,
Za/2 = critical value for normal distribution at 95% confidence interval (1.96),
P = 72.77% proportion of practice of essential new born care among health care providers taken from the study conducted in the eastern zone of the Tigray region,15
d = 0.05 (margin of error).
Additionally, the sample size for the specific objectives was determined using the double population proportion formula by considering the following assumptions, taking a significant factor from a study conducted in the Tigray region eastern zone, Ethiopia.15 Finally, by comparing the calculated sample size the largest was taken (305). Because the source population is less than 10,000, we used the correction formula;

Where, nf = final sample size,
n = initial sample size,
N = source population (obstetric care provider).
Finally, by adding 10% to the sample size for non response rate, the total of 208 individuals were included in the study.
There are nine woredas in the Awi zone, and six were selected by the lottery method. All public health facilities found in the selected woredas were included in the study. Then, the calculated sample size was proportionally allocated for each health facility based on the number of obstetric care providers. Since the number of obstetric care providers in each governmental health facility is not equal, the calculated sample size allocated for each health facility was proportionally allocated to determine the number of obstetric care providers included in the study from each facility. Finally, all randomly selected obstetrical care providers who were available during the data collection period were included in the study.
Data Collection Instruments, Procedure and Quality Assurance
The data were collected through interviewer-administered structured and pretested questionnaires, and observational checklists.
The questioner and checklist were adapted from different relevant literature like the World Health Organization, Integrated Maternal Newborn care Basic skill course Learning and Evaluation checklist, and other related sources.16–19 The structured questionnaire had three parts; socio-demographic factor with seven items, associated factors with eighteen questions, and an observational checklist containing fifteen tasks for assessment of the practice of essential newborn care. The data were collected by 5 BSc midwives by using the English version of the questioner and checklist. The data collectors and supervisors were recruited based on their academic status and previous experience in data collection.
To assure the quality of the data, three-day technical training was given for data collectors and supervisors regarding the objectives of the study, methods of data collection, and the significance of the study. A pretest was conducted on 11 obstetric care providers (5%) of the sample size from Dangla woreda. Throughout the data collection, interviewers were supervised. Every afternoon a meeting was held between data collectors, supervisors, and principal investigators to discuss and address any issues arising during data collection. The collected data were checked and reviewed for completeness before data entry.
Data Management and Analysis
The collected data was cleaned code and entered to the Epi-info version 7 and then exported to SPSS version 23. Bivariate analysis was done for all explanatory variables concerning the practice of essential newborn care and variables with p-value < 0.20 in the bivariate analysis were selected for the multivariate logistic regression model for adjustment of confounding effects between explanatory variables. Adjusted odds ratio with 95% confidence interval was computed and variables having P-value less than 0.05 in the multivariate logistic regression model were considered as statistically significant for the practice of essential newborn care. For descriptive statistics like frequency and cross-tabulations, graphical presentations such as tables, bar, and pie charts were used to present the result findings.
Operational Definition
- Essential newborn care: it is sequential care given to all newborn infants starting from delivery of the head and it includes drying and stimulating, evaluation of breathing, cord care, keeping the newborn warm, initiating breastfeeding in the first one hour, administering eye ointment, administering vitamin k intramuscularly, weighing, and putting on an identification band and recording.20
- Proper practice of essential newborn care: If the obstetrical health care providers perform above the mean score on practice-related tasks on the checklist.20
- Not practiced properly: not practiced properly: If the obstetrical health care providers perform less than the mean score on practice-related tasks on the checklist.20
- Obstetrical care provider: health care providers that provide delivery and newborn care service in the delivery ward which could be doctors, nurses, IESO, and midwives.20
Ethical Consideration
Ethical clearance for this study was obtained from the Institutional review board, College of Medicine and Health Science, of Bahir Dar University. A supporting letter was written by the College of Medicine and Health Science to the Awi zone health office then written permission was given to the selected woreda health bureaus of Awi zone. Health facility managers gave written permission to the MCH (maternal and child health) department head. Before taking the interview the purpose and possible benefit of the study was explained and written permission was obtained from each respondent.
Results
Socio-Demographic Characteristics
A total of 201 obstetric care providers were involved in this study with a response rate of 96.6%. According to this study, 110 (54.7%) of the participants were males and 91 (45.3%) were females. The mean ages of the respondents were 27.3 years (standard deviation ± 4.62 years). Most of the respondents were working at health centers 146 (72.6%) and 115 (57.2%) of the respondents were degree holders. The majority of respondents 166 (82.1) were orthodox in religion (Table 1). Regarding the knowledge of obstetrical care providers on essential newborn care, 72.1% of the obstetrical care providers had good knowledge and 27.9% of the respondents had poor knowledge (Table 2).
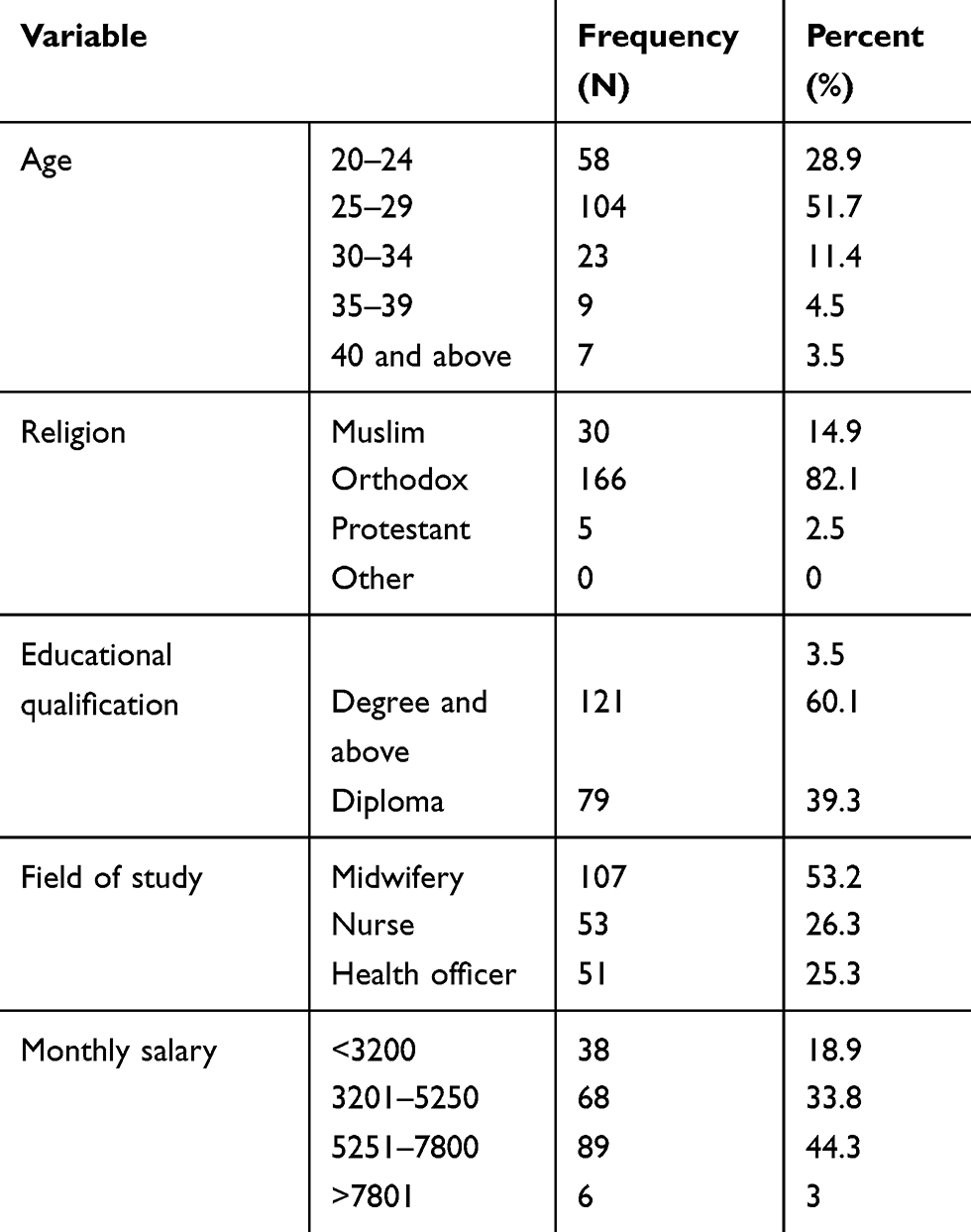 |
Table 1 Distribution of Socio-Demographic Characteristics of Study Participants in Awi Zone Public Health Care Facilities, Amhara Regional State, Ethiopia, from March to April 15, 2019 |
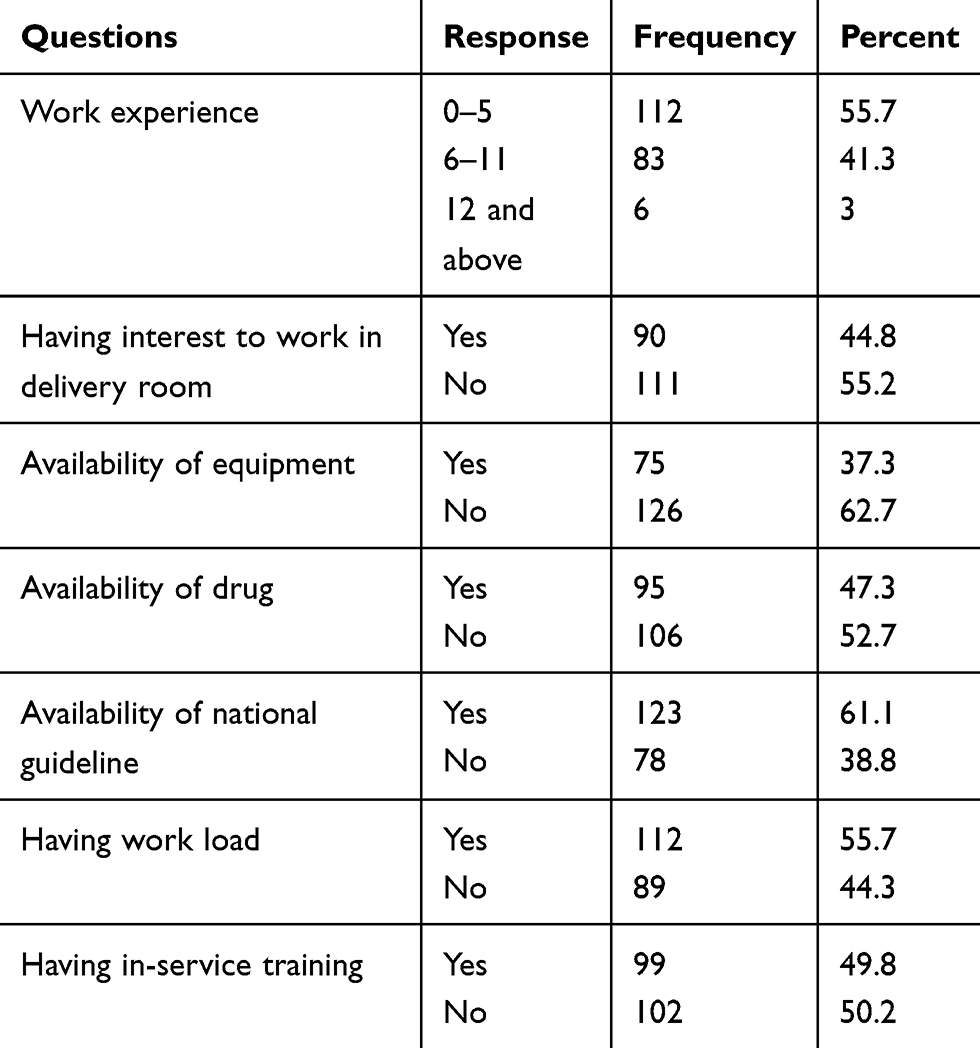 |
Table 2 Distribution of Institutional and Personal Factors of Practice of Essential Newborn Care Among Participants Working at Public Health Facilities in Awi Zone, Amhara Region, Ethiopia, from March to April 15, 2019 |
The Practice of Essential Newborn Care
The results of this study showed that 128 (62.7%) obstetric care providers practiced essential newborn care properly while 73 (37.3%) obstetrical care providers did not practice properly (Figure 1). In this study, 61.7% of obstetric care providers deliver the baby on the maternal abdomen, dry the baby and only 48.8% of them remove the wet towel. Regarding airway maintenance, only 67.7% maintained this by wiping the mouth, and nose after delivery of the head. Moreover, 52.2% of the study participants had evaluated breathing while drying and stimulating the baby. This study revealed that less than half (48.3%) of the study participants cut the cord of a crying baby after 2–3 minutes of birth or until the cord ceases to pulsate (Figure 2). This study showed that 63.7% of the participants administered eye ointment without the tip of the bottle or the tube touching the eye of the baby or the object, and less than half of the participants 48.8% were administered vitamin k intramuscularly in the anterolateral part of the thigh with an appropriate dose of vitamin k which is 1 mg for normal weight, and 0.5 mg for babies with a weight of less than 1500 grams. In this study, only 47.8% of the participants put the baby on skin-to-skin contact after removal of the wet towel. This study also revealed that 82.1% of the study participants initiate exclusive breast feeding within the first hour of delivery. About 81.6% of the participants weighed the baby by putting or placing a clean paper on the pan of the weighing scale. Regarding the identification band, only 5% of the study participants put the identification band on the newborn in this study (Table 3).
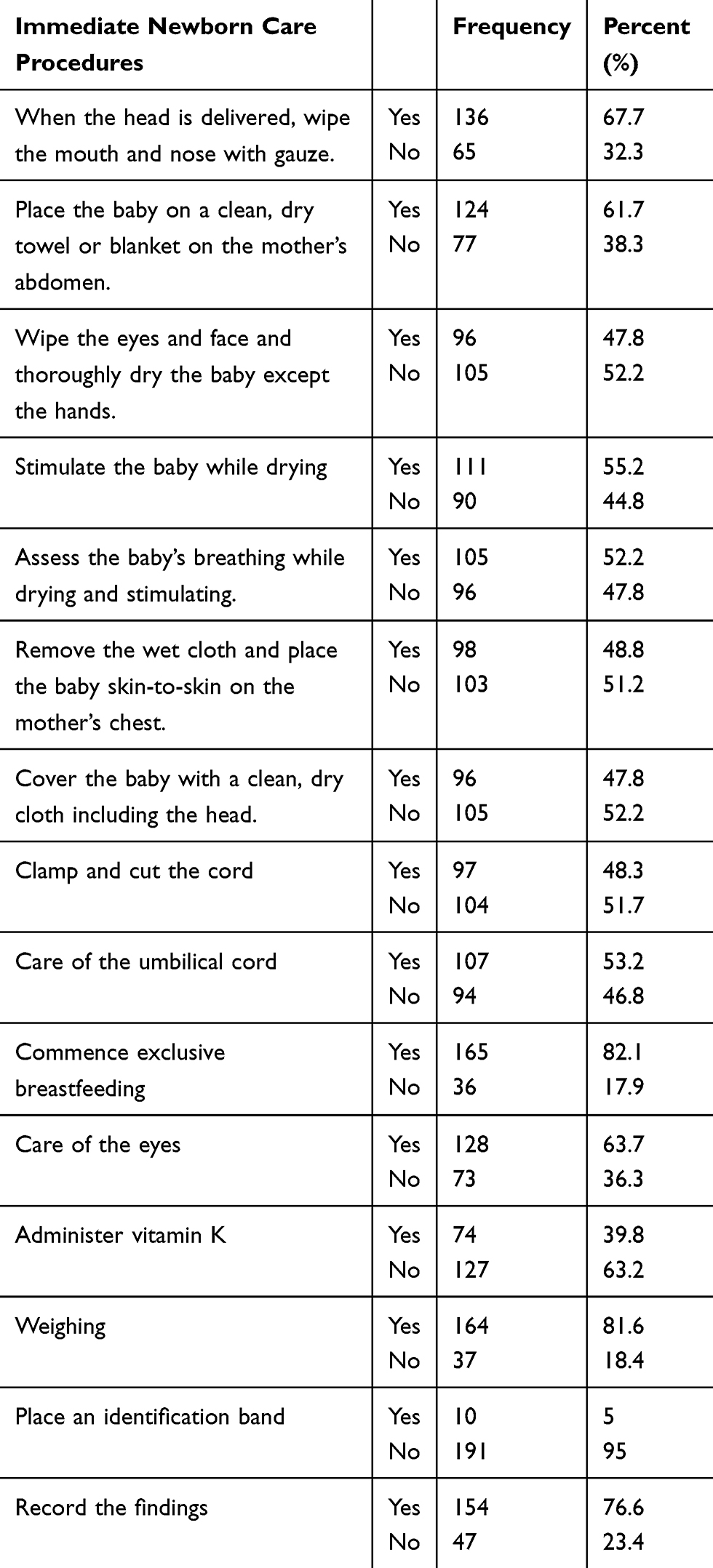 |
Table 3 Practice of Essential Newborn Care Among Obstetrical Care Providers in Public Health Facilities, Awi Zone, Amhara Regional State, Ethiopia, 2019 |
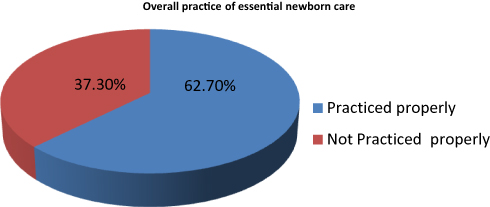 |
Figure 1 Overall practice of essential newborn care among obstetrical care providers in public health facilities, Awi zone, Amhara regional state, Ethiopia, 2019. |
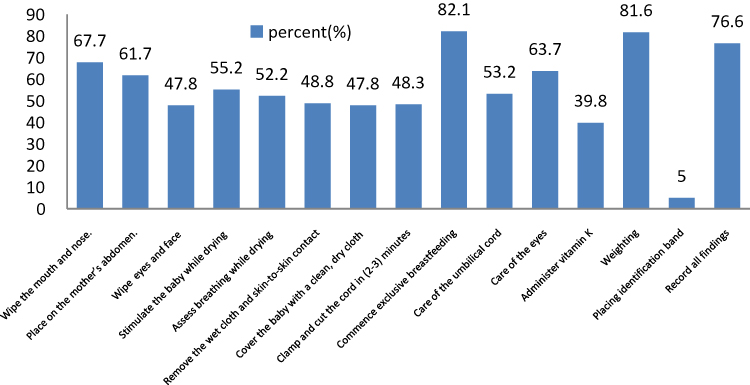 |
Figure 2 Practice of essential newborn care among obstetrical care providers in public health facilities, Awi zone, Amhara regional state, Ethiopia, 2019. |
Factors That Affect the Practice of Essential Newborn Care
This study revealed that educational level, knowledge of essential newborn care, in-service training, field of study, availability of drugs, and availability of medical equipment were significantly associated with the practice of essential newborn care.
Obstetric care providers who were midwives by profession were about 3.1 times more likely to practice essential newborn care than nurses (AOR = 3.1, 95% CI: 1.35, 7.39). Those obstetrical care providers who received in-service training on essential new born care were 2.7 times more likely to practice essential new born care than those who have not received in-service training (AOR = 2.7, 95% CI: 1.03, 4.49). Obstetric care providers who had good knowledge on essential new born care were 2.1 times more likely to practice essential new born care than obstetric care providers who had poor knowledge on essential new born care (AOR = 2.1, 95% CI: 1.03, 4.49).
Availability of medical equipment for essential newborn care was also significantly associated with the practice of essential newborn care. Obstetrical care providers who can access medical equipments for essential newborns were 2 times (AOR = 2, 95% CI: 1.01, 3.96) more likely to practice essential newborn care compared to obstetric care providers who did not access medical equipment for essential newborn care. Likewise, obstetric care providers who access drugs for essential newborn care were 2.3 times (AOR = 2.3, 95% CI: 1.16, 4.72) more likely to practice essential newborn care as compared to obstetric care providers who did not access the drugs.
However, obstetric care providers who were degree holders had 53.2% lower odds of essential newborn care practice as compared to obstetric care providers whose educational level were diplomas (AOR = 0.46, 95% CI: 0.22, 0.96) (Table 4).
 |
Table 4 Simple Binary Logistic Regression and Multiple Logistic Regression Analysis to Identify Factors Associated with the Practice of Essential Newborn Care in Public Health Facilities at Awi Zone, Amhara Regional State, Ethiopia, 2019 |
Discussion
The first few hours after birth are the most critical period in the life of an infant for further growth and development, which is mostly determined by the quality of care that the newborn receives.
In this study, the practice of immediate newborn care among obstetrical care providers was 62.7% (95% CI: 55.7, 69.7). The finding of this study is in line with a study done in Bahir Dar town which was 59.7%.21 This might be due to the similarity of region in which the studies were conducted. This finding was higher than the study done in the central Tigray region which was 52.4%.22 This difference might be due to the difference in study period in which the study was conducted, 2019 in the case of this study, and 2015 for central Tigray. This study's finding is also higher as compared to a study done in Khartoum which was 41%.20 This difference might be due to difference in study setting in which the Khartoum study was done only among hospitals, whereas our study also includes health centers. The finding of this study is lower as compared to the study done in the eastern Tigray region which was 72.7%.15 The difference might be related to the in-service training provided for obstetric care providers on essential care of the newborn which was 45.3% in our study and around 70% in the case of eastern Tigray.
Regarding airway maintenance, in our study 67.7% maintained this by wiping the mouth and nose after delivery of the head. In studies done in the central zone of the Tigray region, and the Ambala district, the practice of airway maintenance was 63.9% and 67.7% respectively.22,23 Additionally, in studies done in El-komminoufiya, Egypt; Khartum; and Bahir Dar, 30.4%, 3.1% and 90%, respectively,of the obstetric care providers maintained the airway of the baby by the wiping of the mouth and nose.2,20,21
In this study, 61.7% of obstetric care providers deliver the baby on the maternal abdomen, dry the baby, and only 48.8% of them remove the wet towel. In a study done in Bahir Dar 58.2% of the participants dry the baby and 54.9% of them remove the wet towel.21 A study done in central Tigray revealed 91.8% of the study participants put the baby on the mother's abdomen and 90.5% of them removed the wet cloth.22 Another study done in Tanzania on the prevalence of drying the baby on the mother's abdomen and removing the wet cloth was 91% and 93% respectively.24
In this study, 52.2% of the study's participants had evaluated the breathing while drying and stimulating the baby. In other studies, 92.7% in Khartum and 86.4% in the eastern zone of Tigray region evaluated the breathing of the newborn while drying and stimulating the baby.15,20 In another study done in Egypt it was 47.8%.2 Avoidance of early cutting of the cord immediately after delivery is very important for the newborn since it promotes placento-fetal transfusion and protects the newborn from developing anemia related to the blood loss that the baby loses when the cord is cut immediately.25 This study revealed that less than half, 48.8% of the study participants, were aware that cutting the cord of a newborn baby should wait for 2–3 minute after birth or until the cord ceases to pulsate. The finding in other studies done in Ethiopia (32%), Egypt (3%), and Khartoum (8.3%) showed how many participants were cutting the cord only after cessation of the pulsation of the cord.2,20,26
Thermal protection is very important and necessary for newborns, which includes skin-to-skin contact. It provides warmth for the new born and it can prevent the complications of hypothermia and it's a significant variable in a study done on hypothermia in Addis Ababa's public hospitals.27 In this study, only 47.8% of the participants put the baby on skin-to-skin contact after removal of the wet towel. In other studies done in Tanzania, eastern Tigray, central Tigray, and Jimma, 42%, 86.4%, 72.1% and 62.12%, respectively, of the health care providers kept the baby on skin-to-skin contact after removal of the wet towel.15,22,24,28
Exclusive breast feeding has an important protective effect in opposition to infection. It reduces the risk of hypothermia and hypoglycemia. Additionally, it helps to maintain thermo regulation by keeping the baby close to the mother and this concept is strengthened by a study done in Addis Ababa on hypothermia.27 This study revealed that 82.1% of the study participants initiate exclusive breast feeding within the first hour of delivery. The findings in other studies done in Jimma, a descriptive study done in Bahir Dar and a study done in Tanzania showed the practice of initiation of exclusive breast feeding within the first hour was 86.4%, 85.8%, and 50%, respectively.21,28,29
This study showed that 63.7% of the participants administered eye ointment without the tip of the bottle or the tube touching the eye of the baby or the object, and less than half of the participants, 48.8%, administered vitamin k intramuscularly in the anterolateral part of the thigh with an appropriate dose of vitamin k, which is 1 mg for normal weight, and 0.5 mg for babies with a weight of less than 1500 grams. In studies done in Egypt, 52.6% of the participants put in eye ointment and in a study done in the Jimma zone the percent of administration of eye ointment and vitamin k was 54.8% and 16.9% respectively.2,28 Another study done in the eastern zone of Tigray showed that 73.2% of the participants provided eye ointment, whereas 66.2% of the participants administered vitamin k.15
About 81.6% of the participants weighed the baby by putting or placing a clean paper on the pan of the weighing scale. A descriptive study done at Bahir Dar town 85.5%, and observational study done in Egypt showed 85.5% and 73.9%, respectively of the obstetric care providers weigh the baby.2 Regarding the identification band only 5% of the study's participants put the identification band on the newborn in this study. The finding in a study done in Bahir Dar town was 26.8%, and central Tigray region was 0.7%.21,22
The profession of obstetric care providers is one factor for the practice of essential newborn care. Practice of proper essential newborn care was higher among midwives than nurses. This result agreed with a study conducted in the same country in Jimma.28 The possible reason might be midwives have more chance to work in a labor ward; more chance to receive in-service training on essential newborn care which might, in turn, improves their knowledge and skill over others.
Obstetric care providers who received in-service training on essential newborn care were 2.7 times more likely to practice proper essential newborn care than their counterparts. This result is supported by the studies done in eastern Tigray and Jimma.15,28 This might be due to the fact that in-service training improves the obstetric care provider’s knowledge, and skill to practice essential newborn care.
Obstetric care providers who had a good knowledge were 2 times more likely to practice essential newborn care than obstetric care providers with poor knowledge. This finding is in line with the study done in Jimma.28 The possible reason might be that knowledge is the core prerequisite to practice essential newborn care.
Obstetric care providers who work in health facilities with adequate medical equipment were 2 times more likely to practice essential newborn care as compared to their counterparts. Moreover, obstetric care providers who work in health facilities with adequate drugs for essential newborn were 2.3 times more likely to practice essential newborn properly compared to obstetric care providers who did not access essential drugs for newborn care.
Regarding educational qualification, the result of this study revealed that degree holders were 0.471 times less likely to practice essential newborn care than diploma holders. This result is supported by studies done in other regions of Ethiopia.26 But in the studies done in Jimma and Egypt, degree holders were more likely to practice proper essential newborn care, more than diploma holders.2,28 This discrepancy might be due to the fact that in our study participants who were degree holders are nurses and health officers. Additionally, the degree holders might be less experienced than diploma holders which in turn decrease the proper practice of essential newborn care.
Limitation
A non-participatory method of data collection was held for assessment of practice by using a checklist, there might be Hawthorne bias.
Conclusion
The overall prevalence of essential newborn care practices was low in Ethiopia. In-service training, midwifery profession, availability of medical equipment, knowledge of essential newborn care, availability of drugs, and level of education were found to be predictors of essential newborn care practice among obstetric care providers. Improvements in essential newborn care practices could be attained through modifiable proven interventions like provision of in-service training, availability of drugs, and medical equipment for essential newborn care.
Abbreviations
AOR, adjusted odds ratio; CI, confidence interval; INC, immediate newborn care; ENC, essential newborn care; EDHS, Ethiopian demographic and health survey; OCP, obstetrical care provider; OR, odds ratio; SD, standard deviation; WHO, World Health Organization.
Data Sharing Statement
The data sets generated during the current study are available from the corresponding author ([email protected]) on reasonable request.
Ethics Approval and Consent to Participate
Ethical approval and clearance for the study were from the Institutional review board, College of Medicine and Health Science, of Bahir Dar University. A supporting letter was written by the College of Medicine and Health Science to the Awi zone health office, and then written permission was given to the selected woreda health bureaus of Awi zone. Health facility managers gave written permission to MCH (maternal and child health) department heads of the selected health facilities. After explaining the purpose and the possible benefit of the study, written permission was obtained from each respondent before taking the interview. Confidentiality was maintained in each level of the response in this study.
Acknowledgment
The authors would like to pass their gratitude to Bahir Dar University for financial support and approval of ethical clearance to carry out this research. We would like to extend our thanks to Awi zone health bureau and, respectively, the woredas and health offices for providing us with the necessary information and cooperative support for the accomplishment of our research work. Our gratitude also goes to supervisors and data collectors for their hard work in obtaining the necessary information. Our special thanks goes to study participants who generously shared their thoughts and feelings despite other tasks and commitments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Corresponding Author
Correspondence goes to Asteray Ayenew.
Funding
The source of funding to carry out this research was Bahir Dar University. The funding organization has no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript, this was the role of authors.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Lazzerini M, Valente EP, Covi B, et al. Use of WHO standards to improve quality of maternal and newborn hospital care: a study collecting both mothers’ and staff perspective in a tertiary care hospital in Italy. BMJ Open Quality. 2019;8(1):e000525–e000525. doi:10.1136/bmjoq-2018-000525
2. Fattah NeamaabdEl ZED. Assessment of quality of nursing care provided immediately after Birth At University Hospital. Life Sci J. 2012;9(4):2115–2126.
3. Paul V. Newborn Nursing for Facility Based Care.
4. Eriksson L, Nga NT, Målqvist M, et al. Evidence-based practice in neonatal health: knowledge among primary health care staff in northern viet nam. Hum Resour Health. 2009.
5. Level and trends of child mortality, U. WHO, UN and World bank report 2015. Available from: http://www.childmortality.org/files_v20/download/IGME%20report%202015%20child%20mortality%20final.pdf.
6. Kim, Kim YM, Ansari N, et al. Assessing the capacity for newborn resuscitation and factors associated with providers’ knowledge and skills: a cross-sectional study in Afghanistan. BMC Pediatr. 2013;13(1). doi:10.1186/1471-2431-13-140
7. UNICEF W, World Bank Group and UN. Levels and trends in child mortality, 2015 report. Available from: http://www.childmortality.org/files_v20/download/igme%20report%202015_9_3%20lr%20web.pdf.
8. Central Statistical Agency/CSA/Ethiopia and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, E., and Rockville, Maryland, USA: CSA and ICF; 2016.
9. Mekonnen, Mekonnen Y, Tensou B, et al. Neonatal mortality in Ethiopia: trends and determinants. BMC Public Health. 2013;13(1). doi:10.1186/1471-2458-13-483
10. WHO recommendations on ways to improve quality of newborn care in health facilities, a.a.h.w.w.i.f.q.-c.-f.e.
11. Bhutta ZA, Das JK, Bahl R, et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet. 2014;384(9940):347–370. doi:10.1016/S0140-6736(14)60792-3
12. UNICEF/WHO. Skilled Attendance at Birth Joint Database. November; 2017.
13. Amouzou A, Ziqi M, Carvajal–Aguirre L, et al. Skilled attendant at birth and newborn survival in Sub–Saharan Africa. J Glob Health. 2017;7(2):020504. doi:10.7189/jogh.07.020504
14. C.P.a.H.C.o.E.A.R.. Available from: http://unstats.un.org/unsd/censuskb20/Attachment489.aspx.
15. Berhe AK, Tinsae F, Gebreegziabher G. Knowledge and practice of immediate newborn care among health care providers in eastern zone public health facilities, Tigray, Ethiopia, 2016. BMC Pediatr. 2017;17(1):157. doi:10.1186/s12887-017-0915-8
16. Central Statistical Agency. T.E.d.a.h.s.p.r.A.A. Ethiopia; 2016.
17. directorate., F.m.o.h.p.p. Health and Health Related Reports. Addis Ababa: Federal ministry of health; 2011.
18. Mah-Mungyeh E, Chiabi A, Tchokoteu FL, et al. Neonatal mortality in a referral hospital in Cameroon over a seven year period: trends, associated factors and causes. Afr Health Sci. 2015;14(4):985–992. doi:10.4314/ahs.v14i4.30
19. Ghana Ministry of Health. U.F.s.C.H.P.A.a.h.e.w.i.n.g.s.d.f.G.U.F.s.
20. Faiza A, Nasortaha. Assessment of knowledge, Attitude and Practices of nurse midwives towards immediate care of the newbornIn Khartoum state teaching hospitals (2011). J Am Sci. 2013;9:263–270.
21. Yemane Y. Knowledge and Practice of Immediate New Born Care Among Obstetrical Care Provider in Bahirdar Town. Quality in Primary Care. 2016.
22. Tsegay T. Knowledge and Practice of Immediate New Born Care Among Midwives. University Addis Ababa; 2015.
23. Louis D, Kumar P, Gupta A. Knowledge and practices of healthcare providers about essential newborn care and resuscitation in a district of Haryana. J Indian Med Assoc. 2013;111(2):114–117.
24. USAID. Common Maternal and Newborn Complications, A Study of 12 Regions in Tanzania. Report 2. Findings on Labour, Delivery and Newborn Care; August, 2010.
25. Al Ninia K, Ashmauey A, Al Qahtani N. Effect of early and late clamping of the umbilical cord on the newborns blood analysis. J Nurs Health Stud. 2017;02(01). doi:10.21767/2574-2825.1000003
26. Ricca J. Quality of care for prevention and management of common maternal and newborn complications. A Study of Ethiopia ’ s Hospitals. 2011;34–35.
27. Demissie BW, Abera BB, Chichiabellu TY, et al. Neonatal hypothermia and associated factors among neonates admitted to neonatal intensive care unit of public hospitals in Addis Ababa, Ethiopia. BMC Pediatr. 2018;18(1):263. doi:10.1186/s12887-018-1238-0
28. Bereka B, Hailu F, DemissieMegenta A. Knowledge and practice of essential newborn care and associated factors among nurses and midwives working at health centers in Jimma Zone, Ethiopia. J Nurs Care. 2018;7(446):2167–2168
29. MAISHA, p. MAISHA Quality of Maternal and Newborn Care Study. Tanzania: Key findings: immediate essential newborn care and resuscitation; 2010–2012.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.