Back to Journals » Drug Design, Development and Therapy » Volume 17
Escitalopram Personalized Dosing: A Population Pharmacokinetics Repository Method
Authors Liu X, Ju G ![]() , Yang W, Chen L, Xu N, He Q
, Yang W, Chen L, Xu N, He Q ![]() , Zhu X, Ouyang D
, Zhu X, Ouyang D ![]()
Received 13 June 2023
Accepted for publication 20 September 2023
Published 27 September 2023 Volume 2023:17 Pages 2955—2967
DOI https://doi.org/10.2147/DDDT.S425654
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Tuo Deng
Xin Liu,1– 3 Gehang Ju,1– 3 Wenyu Yang,4 Lulu Chen,3,5,6 Nuo Xu,4 Qingfeng He,4 Xiao Zhu,4,* Dongsheng Ouyang1– 3,5,*
1Department of Clinical Pharmacology, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 2Institute of Clinical Pharmacology, Central South University, Changsha, People’s Republic of China; 3Hunan Key Laboratory for Bioanalysis of Complex Matrix Samples, Changsha Duxact Biotech Co., Ltd, Changsha, People’s Republic of China; 4Department of Clinical Pharmacy and Pharmacy Administration, School of Pharmacy, Fudan University, Shanghai, People’s Republic of China; 5Changsha Duxact Biotech Co., Ltd, Changsha, People’s Republic of China; 6Department of Pharmacy, Affiliated Hospital of Xiangnan University, Chenzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dongsheng Ouyang, Changsha Duxact Biotech Co., Ltd, Lutian Road 28, Changsha, 410221, People’s Republic of China, Tel +86 0731-84805380, Email [email protected] Xiao Zhu, Department of Clinical Pharmacy and Pharmacy Administration, School of Pharmacy, Fudan University, Zhangheng Road 826, Shanghai, 201203, People’s Republic of China, Tel +862151980024, Email [email protected]
Abstract: Escitalopram (SCIT) represents a first-line antidepressant and antianxiety medication. Pharmacokinetic studies of SCIT have demonstrated considerable interindividual variability, emphasizing the need for personalized dosing. Accordingly, we aimed to create a repository of parametric population pharmacokinetic (PPK) models of SCIT to facilitate model-informed precision dosing. In November 2022, we searched PubMed, Embase, and Web of Science for published PPK models and identified eight models. All the structural models reported in the literature were either one- or two-compartment models. In order to investigate the variances in model performance, the parameters of all PPK models were derived from the literature published. A representative virtual population, characterized by an age of 30, a body weight of 70 kg, and a BMI of 23 kg/m2, was generated for the purpose of replicating these models. To accomplish this, the rxode2 package in the R programming language was employed. Subsequently, we compared simulated concentration–time profiles and evaluated the impact of covariates on clearance. The most significant covariates were CYP2C19 phenotype, weight, and age, indicating that dosing regimens should be tailored accordingly. Additionally, among Chinese psychiatric patients, SCIT showed nearly double the exposure compared to other populations, specifically when considering the same CYP2C19 population restriction, which is a knowledge gap that needs further investigation. Furthermore, this repository of parametric PPK models for SCIT has a wide range of potential applications, like design miss or delay dose remedy strategies and external PPK model validation.
Keywords: escitalopram, population pharmacokinetics, precision medicine, CYP2C19
Introduction
Depression and anxiety disorders are prevalent mental health conditions that affect approximately 7.5% of individuals worldwide and contribute to 3% of the global disease burden.1 Antidepressant medication is an essential component of the pharmacological management of depression and anxiety.2 Escitalopram (SCIT), an antidepressant and antianxiety drug derived from racemic citalopram, has been reported to be more potent with less adverse reaction and more pharmacological effects than R-citalopram.3,4 Its antidepressant action has presumed the inhibition of the central nervous system’s neuronal reuptake of serotonin.5 Due to its relatively safe adverse effect profile, SCIT is recommended as a first-line therapy for patients with anxiety and depression.6,7
After oral administration, SCIT is absorbed by nearly 80%, with the peak blood levels occurring at approximately about 3–5 hours (h). It is mainly metabolized by CYP2C19 and CYP3A4, with a terminal half-life of about 27–32.5,8–10 However, only 50%–60% of patients respond to SCIT,11 this may be partially ascribed to inter-individual (IIV) differences in metabolic capacity, influenced by genetic variability in drug-metabolizing enzymes, specifically the hepatic cytochrome P450 (CYP) system.12–15 Consequently, using a one-size-fits-all approach for all patients could lead to treatment failure and unexpected adverse drug reactions.
The population pharmacokinetic (PPK) model has been recognized as a valuable approach in identifying covariates that influence pharmacokinetics (PK) parameters and estimating individual PK parameters through Bayesian forecasting to develop individualized therapy. To date, several PPK studies on SCIT have been conducted to identify the covariates that may significantly affect the PK characteristics.16–23 For instance, the influence of CYP2C19 polymorphism on SCIT exposure was found to be substantial. Consequently, diverse dosage regimens were simulated to enable personalized dosing recommendations for distinct populations.17,20–23 Notably, Liu’s report highlighted that older patients with poor metabolizer status may be at risk of adverse effects and potential overdosing when administered with 15 or 20 mg SCIT.21 Therefore, the authors strongly advised exercising heightened vigilance in monitoring this specific population to mitigate potential risks. However, to achieve individualized dosing and improve the clinical use of SCIT, a comprehensive description of the PK parameters and PPK models of SCIT is necessary. Therefore, the objective of this study was to provide an overview of published SCIT PPK studies, summarize significant covariates that affect SCIT PK, and identify knowledge gaps that require further exploration, thereby facilitate the clinical precision usage of SCIT.
Materials and Methods
Search Strategy
PubMed, Web of Science, and Embase were data sources for systematically searching of SCIT PPK model up to 12 November 2022, according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline to ensure that all parametric PPK models are included. The relevant PPK researches on SCIT were unified using the following search terms: “escitalopram”, “escitalopram oxalate”, “Lexapro”, “citalopram”, “Cytalopram”, “Citalopram Hydrobromide”, “Lu-10-171”, “Lu10171”, “Seropram”, “Celexa” and “population pharmacokinetic”, “pharmacokinetic”, “nonlinear mixed effect model”, “NONMEM”, “Pmetrics”, “WINNONMIX”, “ADAPT”, “P-PHARM”, “nlmixr”, “NLME”, “MONOLIX”, “WinBUGS”. On top of these, all reference lists from selected articles were studied to ensure the comprehensiveness of our review. Two independent authors (Xin Liu and Gehang Ju) conducted the literature research and study selection independently using EndNote (Version X9; Thomson Scientific, Box Hill, Victoria, Australia). A third senior investigator (Qingfeng He) was consulted to resolve any discrepancies between the two authors.
All studies identified from databases and other sources were screened to evaluate their eligibility based on the consolidated criteria: (1) the subjects of studies were human including healthy volunteers and patients; (2) SCIT was the study drug or citalopram was the study drug with SCIT modeled separately; (3) PPK or pharmacokinetic/pharmacodynamics analysis was conducted in the study; (4) the study was published in English. A publication was excluded if (1) it was not an article or only focused on the methodology, algorithm, or software studies; (2) critical PK parameters were insufficient.
Literature Quality Evaluation and Information Extraction
The quality of the PPK studies was evaluated based on 33 items from previous guidelines.24 The literature was divided into five parts including title and abstract, introduction, methods, results, conclusion and discussion. For each item, one point was assigned if the involved literature met the criteria (low risk of bias), whereas incomplete data were assigned 0.5 points (some concerns). If the item did not meet the criteria, it was assigned 0 points (high risk of bias).
A standardized data extraction method was applied to conduct the data collection from all eligible studies: (1) demographic characteristics of included PPK studies (eg age, sex and weight range); (2) the study design (eg number of subjects and observations, dosage, administration and sampling schedule); (3) model strategies and final pharmacokinetic parameters of included studies (eg software/algorithm, fixed effect parameters, inter-individual variation, residual unexplained variability (RUV), model evaluation); (4) investigated and identified covariates in the model.
Study Comparison of the PPK Model Repository
To provide a comprehensive overview and comparative analysis of the demographic characteristics, as well as the population analysis strategies, PK parameters, and screened covariates, a tabular format was utilized.
One thousand virtual patients population were created, each with a standard age of 30 years old, a typical weight of 70 kg, and a body mass index (BMI) of 23 kg/m2. Published models were utilized to simulate concentration–time profiles based on this set of virtual populations, and a dosing regimen of 10 mg/d was administered consecutively for 30 days to ensure a steady state was reached. After the final dose was administered, a sampling schedule was carried out for 24 hours to observe the concentration. All the simulations were using the rxode2 package (version 2.0.13) in R software (Version 4.2; http://www.r-project.org/).
A forest plot was constructed to illustrate the influence of identified covariates on the clearance (CL) of SCIT. The clinical significance of CL change was deemed insignificant if it fell within the range of less than 80% to 125%. In order to facilitate comparison, all continuous covariates were standardized to the same range. The categorization for weight was established as follows: 20–40 kg for low, 41–100 kg for middle, and >100 kg for high, based on the classification published by others.24–26 As per the standards set by the World Health Organization, age was classified into four stages to represent juveniles, young adults, middle-aged adults, and older adults, respectively.
As for binary covariates, such as co-administration with CYP2C19 inhibitors, the common condition would be treated as the reference (COVi = 0). The uncommon condition would be treated as the test (COVi = 1). CLi = CLcommon + CLdiff*COVi. The range of CLi would be [CLcommon, CLcommon + CLdiff] (if CLdiff > 0), or [CLcommon + CLdiff, CLcommon] (if CLdiff < 0). Then, the effect range of identified covariate on CL was calculated by equation 1:

And for triadic covariates, such as CYP2C19 phenotypes, there are always divided into CYP2C19 extensive metabolizers (EM), intermediate metabolizers (IM) and poor metabolizers (PM, or divided into rapid metabolizers (RM)/EM, IM/PM and missing individuals. In this classification, the middle was set as the reference and the range of CLi would be [CLcommon + CLdiff1, CLcommon + CLdiff2] (CLdiff1 < 0, CLdiff2 > 0). The effect range of identified covariate on CL was also calculated by equation 1.
Results
Study Identification
In total, 771 papers were identified through a comprehensive search strategy, comprising 297 articles from PubMed, 245 articles from Embase, and 229 articles extracted from Web of Science. Following a rigorous eligibility assessment, 15 full-text studies were scrutinized for their adherence to the inclusion criteria. Of these, 2 studies were deemed ineligible due to the absence of pertinent PPK parameters, while 2 studies were found to solely report on the citalopram PPK model. Additionally, 3 studies focusing on PPK in rats were excluded from further analysis. Ultimately, 8 articles were deemed eligible for inclusion in the present study. A visual representation of the workflow is provided in Figure 1.
 |
Figure 1 PRISMA Diagram of population pharmacokinetic studies screen. |
Study Characteristics
All the included studies were published from 2009 to 2022, involving populations from Australia, China, Korea, Italy, the USA, Switzerland, and France. The literatures quality evaluation results were presented in Table S1 and Figure S1. Seven of eight studies were prospective in design,16–20,22,23 with only one study from China being retrospective.21 The number of subjects investigated in the studies ranged from 29 to 172, with seven studies utilizing a sparse sampling strategy,16–19,21–23 and only one study sampling intensively,20 focusing solely on healthy individuals.20 One study conducted PPK analysis based on the data from perinatal period women, aimed at assessing the genetic and environmental factors on drug concentrations and transfer into breast milk.23 Only two of eight studies enrolled a population under 18 years old,21,22 with the youngest age being 12 years old, and one study did not report age information.20 Detailed characteristics of all included studies are presented in Table 1.
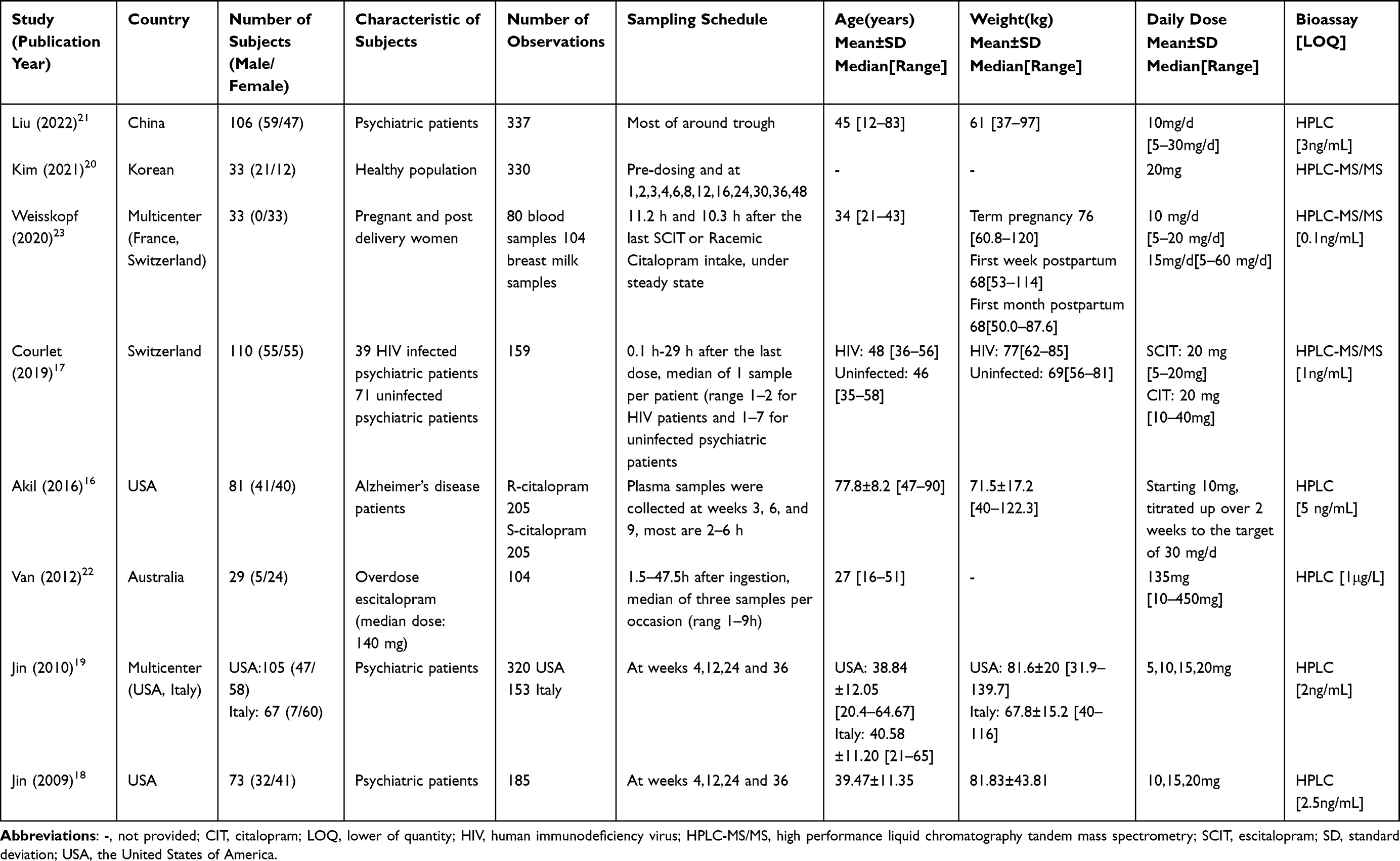 |
Table 1 Characteristics of Included Population Pharmacokinetic Studies |
The PPK modeling strategies employed and the resultant PK parameters obtained from the included studies are comprehensively summarized in Table 2. Most of the studies utilized NONMEM (ICON, Dublin, Ireland) for PPK modeling, with the exception of one study that used WinBUGS.22 The algorithms were first-order condition estimation with interaction and full Bayesian analysis, respectively. Seven studies finally built a one-compartment model to fit the SCIT data they collected,16–19,21–23 while Kim et al concluded with a two-compartment model.20 Only one study had external validation out of all the included studies,17 while all the studies were evaluated by internal validation, like goodness-of-fitness (GOF), visual predictive check (VPC), and bootstraps. However, few studies had reported their methods to deal with the missing data or data below quantitative limits. IIV was described by an exponential model in all included studies. RUV was described by a proportional model in five studies,16,19–21,23 an additive model in one study,17 and a combined proportional and additive model in two studies.18,22
 |
Table 2 Model Strategies and Final Pharmacokinetic Parameters of Included Studies |
Five studies performed simulations for model application. Most simulations were about the dosage design for different CYP2C19 phenotype populations and abnormal QTc prolongation at different SCIT concentrations.
Study Comparison
Comparison of SCIT PK Profiles
Figure 2 (Supplementary Material 1–2, Table S2-S4) presents a comprehensive comparison of all the reproduced PK parameters for SCIT. The results indicate no significant differences in SCIT exposure between psychiatric patients and healthy populations, due to the Cmax and AUC between Kim’s group and other reports were quite similar. Notably, with the exception of the Chinese population,21 there were no significant ethnic differences in PK parameters among the enrolled populations, including Korean,20 French,23 Swiss,17,23 American,16,18,19 and Italian19 exposure for their main PK parameters were quite closed. However, the Chinese population exhibited an almost 2-fold exposure compared to the other populations.
 |
Figure 2 Escitalopram main pharmacokinetic parameters (Cmax and AUC0-τ) at steady state of missing phenotype, CYP2C19 poor metabolizers and CYP2C19 extensive metabolizers population. (A) The Cmax comparison between the missing phenotype population. (B) The Cmax comparison between the CYP2C19 extensive metabolizers population. (C) The Cmax comparison between the CYP2C19 poor metabolizers population. (D) The AUC0-τ comparison between the missing phenotype population. (E) The AUC0-τ comparison between the CYP2C19 extensive metabolizers population. (F) The AUC0-τ comparison between the CYP2C19 poor metabolizers population. Notes: To generate Figure 2, the corresponding R-script can be found in Supplementary Material 1–2, while the necessary dataset is provided in Table S2-S4. |
It is important to acknowledge that the classification standards for CYP2C19 varied among the different studies we reviewed. Akil16 et al and Jin19 et al grouped CYP2C19 IM and PM together and combined RM and EM into another group. While Liu et al classified the CYP2C19 phenotype population into EM, IM, and PM populations, and Weisskopf et al divided the population into PM and normal phenotypes. Therefore, differences in PK parameters between populations may not have been significant in the former studies, but the latter revealed a nearly 2-fold exposure difference between CYP2C19 PM and EM populations.
Covariate Screening and Covariate Effect
The majority of included studies aim to achieve individualized therapy, thus, the covariates that affect PK performance and the extent of their influence on PK are extremely important. All the investigated and significant covariates are summarized in Table 3. A stepwise approach included forward inclusion and backward elimination was commonly employed for covariates assessments. The comparison of identified and investigated covariates was presented in Figure 3 (Supplementary Material 3, Table S5).
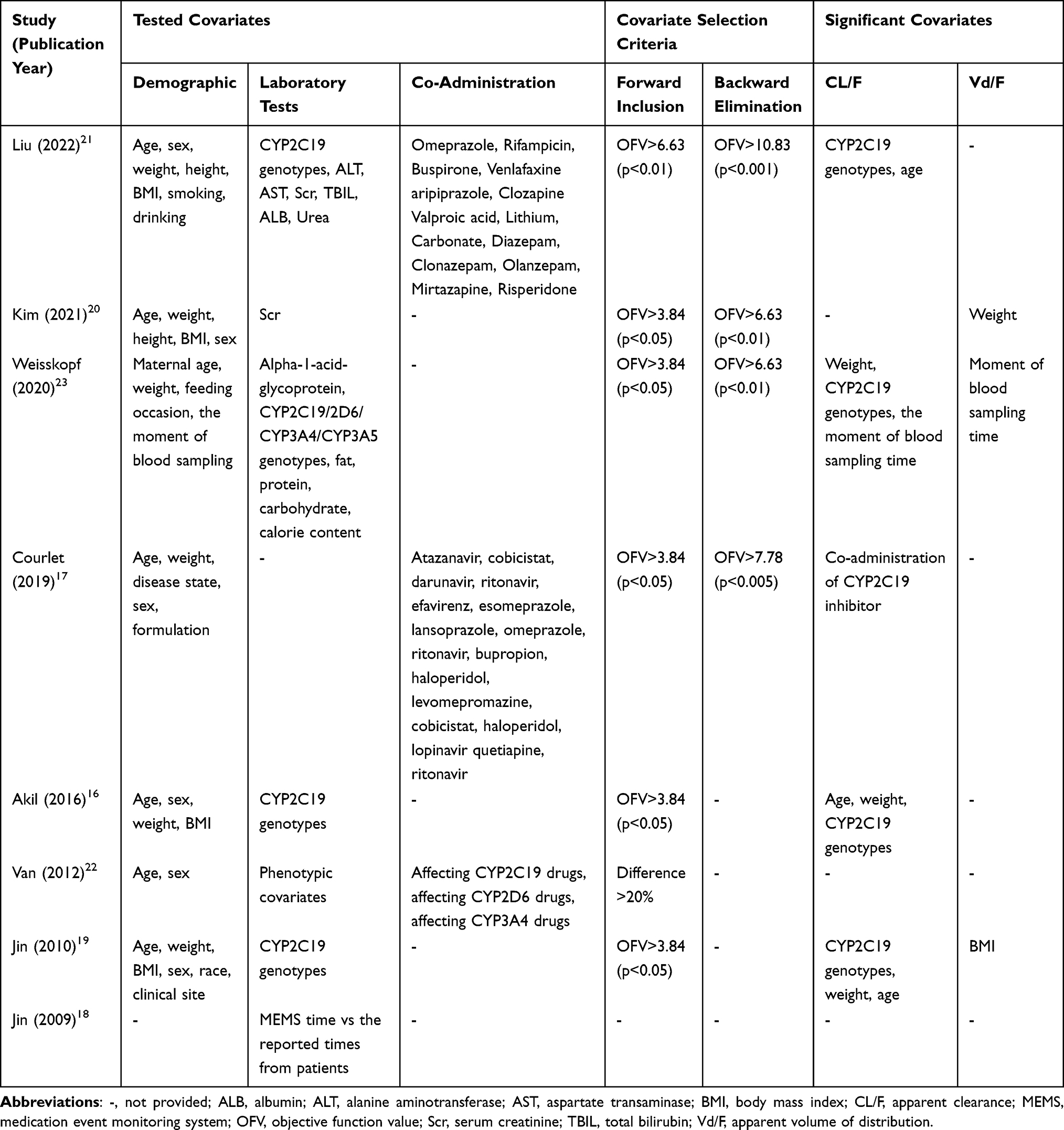 |
Table 3 List of Tested and Significant Covariates in the Model |
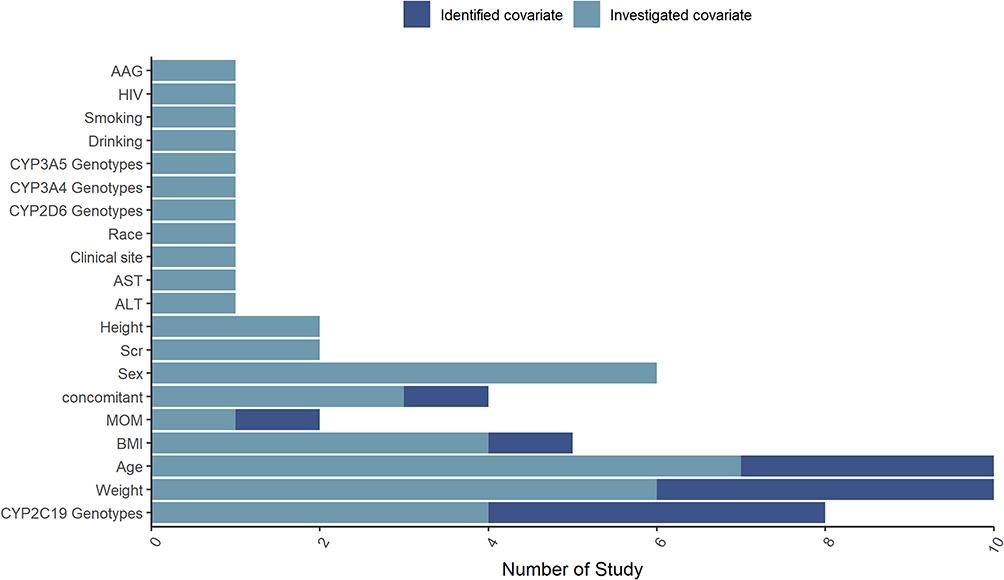 |
Figure 3 Investigated and Identified covariates of all the population pharmacokinetic models. Abbreviations: AAG, alpha-1-acid glycoprotein concentration; AST, aspartate transaminase; ALT, alanine transaminase; BMI, body mass index; HIV, human immunodeficiency virus; MOM, the moment of blood or milk sampling (four categories: during labor, after delivery, first week postpartum or 1 month after delivery); Scr, serum creatinine. Notes: To generate Figure 3, the corresponding R-script can be found in Supplementary Material 3, while the necessary dataset is provided in Table S5. |
The CYP2C19 phenotype, body weight and age were found to significantly affect SCIT CL in most of the included final models. CYP2C19 phenotype was included in 5 studies (62.5%) and was found to be a significant covariate in all 5 studies (100%).16,17,19,21,23 Of the 7 studies investigating the influence of age on CL, 3 studies (42.85%) found age to be a significant covariate.16,19,21 Two of 6 studies (33.33%) found that body weight was also a significant covariate on CL16,19 and only one study found that body weight was also a significant covariate on the distribution volume of SCIT.20
Moreover, three studies investigated the influence of concomitant drugs on SCIT PK, and only one study found that CYP2C19 inhibitors, such as proton-pump inhibitors, modestly influenced SCIT elimination (clearance decreased by 19%).17 One study based on perinatal women observed no differences during labor, right after delivery, and during the first week of postpartum; however, a 10% decrease in CL was observed at 1 month after delivery compared to the perinatal period.23
To further compare significant covariates and provide suggestions for precision dosing, a forest plot was presented in Figure 4 (Supplementary Material 4, Table S6). Pregnancy and co-administration with CYP2C19 inhibitors were reported to have a significant influence on SCIT disposition; however, the change was below 1.25-fold, which assumed no clinically significant difference. For weight, three groups were designed to detect the difference in different populations. One study showed that weight had a clinical significance of an influence on CL larger than 5% to 15%. In other weight ranges (20–40 kg and 101–200 kg), the results indicated that there was no need to adjust the dosage. For age between 18 and 65 years old, Akil et al16 showed a great discrepancy between Liu21 and Jin,19 which may be caused by the difference in the population they investigated. Akil constructed a PPK model mainly based on Alzheimer’s disease patients, whose average age was 77.8 with a range from 47 to 90 years old; however, Liu and Jin’s studies were based on populations with an average age of 45 and 39.52, respectively. For the CYP2C19 phenotype’s influence on CL of SCIT, approximately 2-fold different exposure of SCIT was observed between CYP2C19 poor metabolizers and extensive metabolizers.
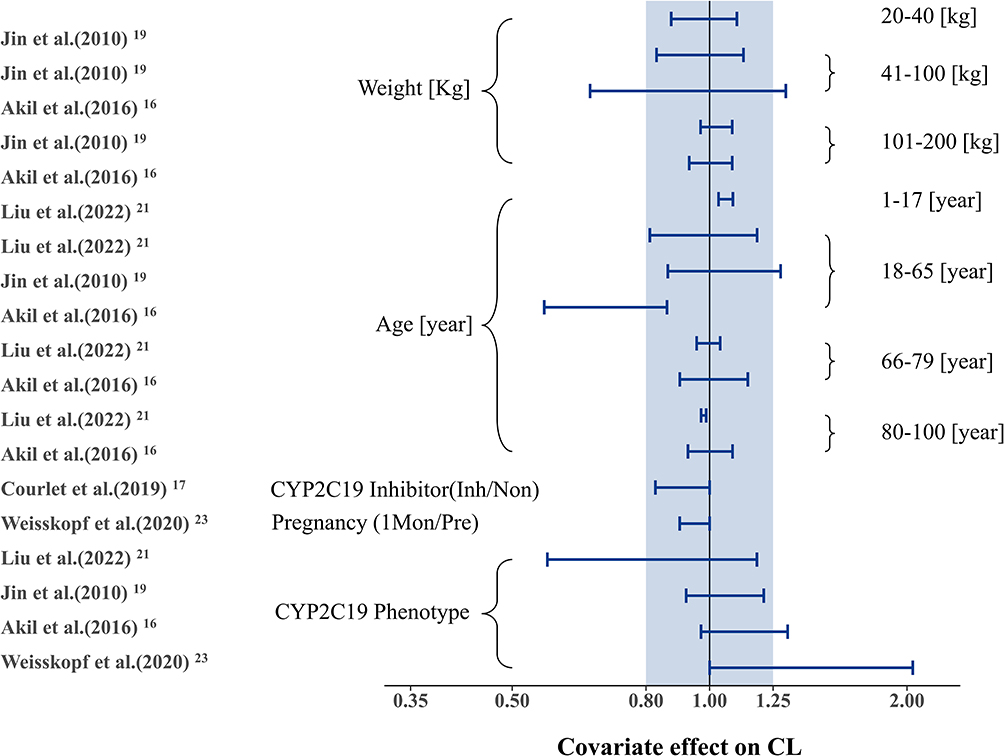 |
Figure 4 Forest plot of covariates effects on clearance of escitalopram. Notes: The horizontal bars represent the covariate effect on clearance in each study. The shadow area ranges from 0.8 to 1.25. To generate Figure 4, the corresponding R-script can be found in Supplementary Material 4, while the necessary dataset is provided in Table S6. |
Discussion
SCIT pertains to one of the most extensively utilized antidepressants. The interest in exploring the PK of SCIT has persisted over the last few years, and a number of PPK studies have been revealed the source of variability. To our best knowledge, this is the first investigation that consolidates all the published PPK studies and furnishes proof for tailored dosage predicated on the ascertained sources of variability. Since SCIT is mainly eliminated by the hepatic CYP system, particularly CYP2C19.27–30 Although SCIT is also metabolized by CYP3A4 and CYP2D6, the clinical studies indicate that the impact of CYP3A4 and CYP2D6 function on SCIT exposure is minimal. For example, Marelo et al reported no significant differences in SCIT PK when co-administered with ritonavir, a strong CYP3A4 inhibitor.31 Similar results were found by Gutierrez et al, who observed no notable changes in citalopram PK when co-administered with ketoconazole.32 Regarding CYP2D6 influence, a study investigating the influence of CYP2D6 functional enzyme status on escitalopram found no significant associations between SCIT serum concentration, metabolite-to-parent ratios, dose-corrected serum concentrations, and CYP2D6 functional enzyme status.33 Solhaug et al genotyped patients for CYP2D6 and CYP2C19 and found that only CYP2C19 genotype was linked to SCIT serum concentration levels.34 Thus, CYP2C19 polymorphism has been reported as a major contributor to the IIV of SCIT exposure.35–37 Such variability may lead to lower drug tolerance or even toxicity (such as QT prolongation). Three studies included in this research have found that the CL/F in CYP2C19 PM population was almost half of that in the CYP2C19 EM population. Additionally, two other studies have reported that the CYP2C19 EM/RM population had 1.3-fold CL/F compared to the PM/IM population. These findings are in line with those of other clinical investigations.27,30,35 Notably, the Dutch Pharmacogenetics Working Group (DPWG) guidelines recommend that the CYP2C19 PM population should not receive a dose that exceeds 50% of the normal maximum dose, while the IM population should receive 75%.38 Therefore, many countries consider pharmacogenomics-guided testing as an actionable tool for SCIT dose adjustment to increase the likelihood of treatment effectiveness and reduce adverse events.39,40
Furthermore, it has been reported that the distribution of CYP2C19 polymorphism differs significantly by region, with the incidence of PM population being 3%–5% in Caucasians and 13%–23% in Asians.41,42 However, no obvious ethnic differences were observed in this study except for the Chinese population. Moreover, the PPK study conducted by Jin et al19 directly compared the PK of SCIT among Americans and Italians, and found no significant differences between these two subpopulations. Moreover, the comparison of SCIT PK parameters (Figure 2) revealed no statistically significant differences in PK among patients with psychosis, Alzheimer’s disease, HIV infection, and healthy individuals. This finding suggests that the PK of SCIT is not influenced by the presence of these conditions. In a study conducted by Courlet et al18 a direct comparison of SCIT exposure between HIV-infected psychiatric patients and non-HIV infected psychiatric patients was performed, and no significant differences were observed. Furthermore, their analysis concluded that HIV infection did not exert any significant impact on SCIT disposition. In the case of Alzheimer’s disease and depression, characterized by cognitive and mood alterations, SCIT disposition may not exhibit significant differences compared to the healthy population. However, there is almost a 2-fold SCIT exposure difference between Chinese psychotic patients and other populations in different CYP2C19 phenotypes. Since there is only one study reported on the Chinese population, the difference remains unclear and warrants further investigation.
SCIT is not only used for depression but also for anxiety disorders, which affect up to 15% of children and adolescents.43 However, there are few PPK studies involving patients under 18 years old, and in this study, only Liu21 and Van22 et al involved adolescents, although the proportion remains unclear. Thiele et al reported that CYP2C19 PM children and adolescents had higher risks of switching and suicide attempt/self-harm than the normal genotype.44 Aldrich et al also found that children and adolescents with CYP2C19 IM phenotype had a slightly increased rate of discontinuation of using SCIT.11 Therefore, there is a need to explore the SCIT’s performance and influence covariates in children and adolescents using PPK methods. Additionally, only one PPK study reported on elderly individuals (average age 77.8), and the age effects on CL were opposite to those of other PPK models findings (Table 2). This discrepancy also deserved further investigation to determine the actual PK performance in elderly individuals and the significant covariates, especially the age effects on CL.
Several limitations need to be considered. Firstly, the study’s restricted scope to English-language literature may have led to the inadvertent exclusion of pertinent studies published in other languages, thereby limiting the opportunity for comparative analyses within the same geographic region. Secondly, only the parametric PPK models were included in this study, and the non-parametric PPK models were excluded because the parameters of the non-parametric models were hard to bridge to parametric models.
Conclusion
The utilization of a model repository containing parametric PPK models for SCIT holds great promise in advancing the field of MIPD. By implementing model repository techniques, this approach can identify gaps in current knowledge, thereby facilitating external validation and sensitivity analysis of newly developed PPK models. Furthermore, the optimization of SCIT dosing regimens must take into consideration the patients’ CYP2C19 phenotype. It is imperative that additional PPK studies be conducted in pediatric and adolescent patients, and prospective PPK investigations should be carried out to elucidate the differences in SCIT exposure within the CYP2C19 Chinese population.
Acknowledgments
The authors sincerely thank Phamark Data Technology Co, Ltd, Changsha, Hunan, China, for their assistance in model simulation.
Funding
This work was supported by the National Natural Science Foundation of China (Project No. 82073942), the Nature Science Foundation of Hunan Province (Project No.2022JJ80100) and Hunan Province's “Three Top” Innovative Talent Project (Project No.2023RC3232).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. World Mental Health Report: Transforming Mental Health for All. WHO; 2022.
2. Malhi GS, Mann JJ. Depression. Lancet. 2018;392(10161):2299–2312. doi:10.1016/S0140-6736(18)31948-2
3. Ho T, Pollock BG, Mulsant BH, et al. R- and S-citalopram concentrations have differential effects on neuropsychiatric scores in elders with dementia and agitation. Br J Clin Pharmacol. 2016;82(3):784–792. doi:10.1111/bcp.12997
4. Jacquot C, David DJ, Gardier AM, Sánchez C. Escitalopram et Citalopram: le rôle inattendu de l’énantiomère R [Escitalopram and citalopram: the unexpected role of the R-enantiomer]. Encephale. 2007;33(2):179–187. doi:10.1016/s0013-7006(07)91548-1
5. Pastoor D, Gobburu J. Clinical pharmacology review of escitalopram for the treatment of depression. Expert Opin Drug Metab Toxicol. 2014;10(1):121–128. doi:10.1517/17425255.2014.863873
6. Guideline Development Panel for the Treatment of Depressive Disorders. Summary of the clinical practice guideline for the treatment of depression across three age cohorts. Am Psychol. 2022;77(6):770–780. doi:10.1037/amp0000904
7. Tor PC, Amir N, Fam J, et al. A Southeast Asia Consensus on the Definition and Management of Treatment-Resistant Depression. Neuropsychiatr Dis Treat. 2022;18:2747–2757. doi:10.2147/NDT.S380792
8. von Moltke LL, Greenblatt DJ, Giancarlo GM, Granda BW, Harmatz JS, Shader RI. Escitalopram (S-citalopram) and its metabolites in vitro: cytochromes mediating biotransformation, inhibitory effects, and comparison to R-citalopram. Drug Metab Dispos. 2001;29(8):1102–1109.
9. Allergan USA, Inc. Lexapro® (Escitalopram) [Package Insert]. Madison, NJ: Allergan USA, Inc; 2021.
10. Ohlsson Rosenborg S, Mwinyi J, Andersson M, et al. Kinetics of omeprazole and escitalopram in relation to the CYP2C19*17 allele in healthy subjects. Eur J Clin Pharmacol. 2008;64(12):1175–1179. doi:10.1007/s00228-008-0529-z
11. Aldrich SL, Poweleit EA, Prows CA, Martin LJ, Strawn JR, Ramsey LB. Influence of CYP2C19 Metabolizer Status on Escitalopram/Citalopram Tolerability and Response in Youth With Anxiety and Depressive Disorders. Front Pharmacol. 2019;10:99. doi:10.3389/fphar.2019.00099
12. Bousman CA, Bengesser SA, Aitchison KJ, et al. Review and Consensus on Pharmacogenomic Testing in Psychiatry. Pharmacopsychiatry. 2021;54(1):5–17. doi:10.1055/a-1288-1061
13. Huang X, Li C, Li C, et al. CYP2C19 Genotyping May Provide a Better Treatment Strategy when Administering Escitalopram in Chinese Population. Front Pharmacol. 2021:12730461. doi:10.3389/fphar.2021.730461
14. Joas E, Jonsson L, Viktorin A, et al. Effect of CYP2C19 polymorphisms on antidepressant prescription patterns and treatment emergent mania in bipolar disorder. Pharmacogenomics J. 2023;23(1):28–35. doi:10.1038/s41397-022-00294-4
15. Strawn JR, Poweleit EA, Mills JA, et al. Pharmacogenetically Guided Escitalopram Treatment for Pediatric Anxiety Disorders: protocol for a Double-Blind Randomized Trial. J Pers Med. 2021;11(11):1188. doi:10.3390/jpm11111188
16. Akil A, Bies RR, Pollock BG, et al. A population pharmacokinetic model for R- and S-citalopram and desmethylcitalopram in Alzheimer’s disease patients with agitation. J Pharmacokinet Pharmacodyn. 2016;43(1):99–109. doi:10.1007/s10928-015-9457-6
17. Courlet P, Guidi M, Glatard A, et al. Escitalopram population pharmacokinetics in people living with human immunodeficiency virus and in the psychiatric population: drug-drug interactions and probability of target attainment. Br J Clin Pharmacol. 2019;85(9):2022–2032. doi:10.1111/bcp.13994
18. Jin Y, Pollock BG, Frank E, et al. The effect of reporting methods for dosing times on the estimation of pharmacokinetic parameters of escitalopram. J Clin Pharmacol. 2009;49(2):176–184. doi:10.1177/0091270008327538
19. Jin Y, Pollock BG, Frank E, et al. Effect of age, weight, and CYP2C19 genotype on escitalopram exposure. J Clin Pharmacol. 2010;50(1):62–72. doi:10.1177/0091270009337946
20. Kim Y, Kim A, Chung JY. Population pharmacokinetic/pharmacodynamic modeling of delayed effect of escitalopram-induced QT prolongation. J Affect Disord. 2021;285:120–126. doi:10.1016/j.jad.2021.02.048
21. Liu S, Xiao T, Huang S, et al. Population pharmacokinetics model for escitalopram in Chinese psychiatric patients: effect of CYP2C19 and age. Front Pharmacol. 2022:13964758. doi:10.3389/fphar.2022.964758
22. van Gorp F, Duffull S, Hackett LP, Isbister GK. Population pharmacokinetics and pharmacodynamics of escitalopram in overdose and the effect of activated charcoal. Br J Clin Pharmacol. 2012;73(3):402–410. doi:10.1111/j.1365-2125.2011.04091.x
23. Weisskopf E, Guidi M, Fischer CJ, et al. A population pharmacokinetic model for escitalopram and its major metabolite in depressive patients during the perinatal period: prediction of infant drug exposure through breast milk. Br J Clin Pharmacol. 2020;86(8):1642–1653. doi:10.1111/bcp.14278
24. Chen YT, Wang CY, Yin YW, et al. Population pharmacokinetics of oxcarbazepine: a systematic review. Expert Rev Clin Pharmacol. 2021;14(7):853–864. doi:10.1080/17512433.2021.1917377
25. Qin Y, Zhang LL, Ye YR, Chen YT, Jiao Z. Parametric population pharmacokinetics of linezolid: a systematic review. Br J Clin Pharmacol. 2022;88(9):4043–4066. doi:10.1111/bcp.15368
26. Yang W, Mak W, Gwee A, et al. Establishment and Evaluation of a Parametric Population Pharmacokinetic Model Repository for Ganciclovir and Valganciclovir. Pharmaceutics. 2023;15(7). doi:10.3390/pharmaceutics15071801
27. Milosavljevic F, Bukvic N, Pavlovic Z, et al. Association of CYP2C19 and CYP2D6 Poor and Intermediate Metabolizer Status With Antidepressant and Antipsychotic Exposure: a Systematic Review and Meta-analysis. JAMA Psychiatry. 2021;78(3):270–280. doi:10.1001/jamapsychiatry.2020.3643
28. Islam F, Marshe VS, Magarbeh L, et al. Effects of CYP2C19 and CYP2D6 gene variants on escitalopram and aripiprazole treatment outcome and serum levels: results from the CAN-BIND 1 study. Transl Psychiatry. 2022;12(1):366. doi:10.1038/s41398-022-02124-4
29. Maruf AA, Greenslade A, Arnold PD, Bousman C. Antidepressant pharmacogenetics in children and young adults: a systematic review. J Affect Disord. 2019;254:98–108. doi:10.1016/j.jad.2019.05.025
30. Jukić MM, Haslemo T, Molden E, Ingelman-Sundberg M. Impact of CYP2C19 Genotype on Escitalopram Exposure and Therapeutic Failure: a Retrospective Study Based on 2087 Patients. Am J Psychiatry. 2018;175(5):463–470. doi:10.1176/appi.ajp.2017.17050550
31. Gutierrez MM, Rosenberg J, Abramowitz W. An evaluation of the potential for pharmacokinetic interaction between escitalopram and the cytochrome P450 3A4 inhibitor ritonavir. Clin Ther. 2003;25(4):1200–1210. doi:10.1016/s0149-2918(03)80076-0
32. Gutierrez M, Abramowitz W. Lack of effect of a single dose of ketoconazole on the pharmacokinetics of citalopram. Pharmacotherapy. 2001;21(2):163–168. doi:10.1592/phco.21.2.163.34101
33. Scherf-Clavel M, Frantz A, Eckert A, et al. Effect of CYP2D6 pharmacogenetic phenotype and phenoconversion on serum concentrations of antidepressants and antipsychotics: a retrospective cohort study [published online ahead of print, 2023 May 11]. Int J Clin Pharm. 2023. doi:10.1007/s11096-023-01588-8
34. Solhaug V, Haslemo T, Kringen MK, Molden E, Dietrichs ES. Genotyping of patients treated with selective serotonin reuptake inhibitors. Genotyping av pasienter behandlet med selektive serotoninreopptakshemmere. Tidsskr nor Laegeforen. 2022;142(13):71. doi:10.4045/tidsskr.22.0017
35. Chang M, Tybring G, Dahl ML, Lindh JD. Impact of cytochrome P450 2C19 polymorphisms on citalopram/escitalopram exposure: a systematic review and meta-analysis. Clin Pharmacokinet. 2014;53(9):801–811. doi:10.1007/s40262-014-0162-1
36. Fudio S, Borobia AM, Piñana E, et al. Evaluation of the influence of sex and CYP2C19 and CYP2D6 polymorphisms in the disposition of citalopram. Eur J Pharmacol. 2010;626(2–3):200–204. doi:10.1016/j.ejphar.2009.10.007
37. Hicks JK, Bishop JR, Sangkuhl K, et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and CYP2C19 Genotypes and Dosing of Selective Serotonin Reuptake Inhibitors. Clin Pharmacol Ther. 2015;98(2):127–134. doi:10.1002/cpt.147
38. Brouwer JMJL, Nijenhuis M, Soree B, et al. Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene-drug interaction between CYP2C19 and CYP2D6 and SSRIs. Eur J Hum Genet. 2022;30(10):1114–1120. doi:10.1038/s41431-021-01004-7
39. Lunenburg CATC, Gasse C. Pharmacogenetics in psychiatric care, a call for uptake of available applications. Psychiatry Res. 2020;292:113336. doi:10.1016/j.psychres.2020.113336
40. Whirl-Carrillo M, Huddart R, Gong L, et al. An Evidence-Based Framework for Evaluating Pharmacogenomics Knowledge for Personalized Medicine. Clin Pharmacol Ther. 2021;110(3):563–572. doi:10.1002/cpt.2350
41. Oates NS, Shah RR, Idle JR, Smith RL. Influence of oxidation polymorphism on phenformin kinetics and dynamics. Clin Pharmacol Ther. 1983;34(6):827–834. doi:10.1038/clpt.1983.257
42. Xiao ZS, Goldstein JA, Xie HG, et al. Differences in the incidence of the CYP2C19 polymorphism affecting the S-mephenytoin phenotype in Chinese Han and Bai populations and identification of a new rare CYP2C19 mutant allele. J Pharmacol Exp Ther. 1997;281(1):604–609.
43. COVID-19 Mental Disorders Collaborators. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. 2021;398(10312):1700–1712. doi:10.1016/S0140-6736(21)02143-7
44. Thiele LS, Ishtiak-Ahmed K, Thirstrup JP, et al. Clinical Impact of Functional CYP2C19 and CYP2D6 Gene Variants on Treatment with Antidepressants in Young People with Depression: a Danish Cohort Study. Pharmaceuticals. 2022;15(7):870. doi:10.3390/ph15070870
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.