Back to Journals » Infection and Drug Resistance » Volume 19
Eravacycline–Cefiderocol Combination Therapy for Carbapenem-Resistant Acinetobacter baumannii Infective Endocarditis: A Case Report and Brief Review of the Literature
Authors Lou L, Li X, Zhang P, Wu H, Chen H, Ma J, Zhang K
Received 9 April 2026
Accepted for publication 18 May 2026
Published 8 June 2026 Volume 2026:19 615678
DOI https://doi.org/10.2147/IDR.S615678
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Lixin Lou,1 Xiaohua Li,1 Peng Zhang,1 Hongyu Wu,1 Haiying Chen,1 Jie Ma,2 Kaiyu Zhang1
1Department of Infectious Diseases and Center of Infectious Diseases and Pathogen Biology, The First Hospital of Jilin University, Changchun, Jilin, 130000, People’s Republic of China; 2Department of Clinical Pharmacy, The First Hospital of Jilin University, Changchun, Jilin, 130000, People’s Republic of China
Correspondence: Kaiyu Zhang, Department of Infectious Diseases and Center of Infectious Diseases and Pathogen Biology, The First Hospital of Jilin University, No. 1, Xinmin Street, Chaoyang District, Changchun, Jilin, 130000, People’s Republic of China, Tel +86-13578673635, Email [email protected]
Background: Infective endocarditis (IE) caused by carbapenem-resistant Acinetobacter baumannii (CRAB) is rare and associated with limited treatment options because of extensive antimicrobial resistance.
Case Presentation: We hereby present a case of prosthetic valve endocarditis (PVE) caused by CRAB, presenting with fever, persistent bloodstream infection, cerebellar hemorrhage, and aortic valve vegetation. The application of a novel combination therapy comprising eravacycline and cefiderocol effectively eliminated the bloodstream infection. Concomitantly, the monitoring of adverse reactions and the subsequent adjustment of medication and dosage ensured the favorable safety. Although bloodstream infection and valve vegetation were controlled, progressive perivalvular leakage indicated the need for timely surgical intervention when clinically feasible.
Conclusion: This case indicates that eravacycline combined with cefiderocol may represent a novel and effective treatment option for refractory IE caused by carbapenem-resistant Gram-negative pathogens, including PVE caused by CRAB.
Keywords: infective endocarditis, carbapenem-resistant Acinetobacter baumannii, clinical manifestations, metagenomic next-generation sequencing, novel combined anti-infective regimen
Introduction
Infective endocarditis (IE) is an infection affecting the endocardium surface of the heart, predominantly involving the heart valves, the endocardium, ventricular septal defects, or implanted cardiac devices.1 With the increasing use of invasive cardiac procedures, the incidence of IE has risen steadily in recent decades.2 IE following valve replacement occurs in 1–94% of patients and accounts for 95–15% of all IE cases, with mortality rates of up to 69%.3 Staphylococcus, streptococcus, and enterococcus are the predominant pathogens,4,5 whereas Gram-negative organisms are relatively uncommon, representing only 1–10% of IE instances.6 Among them, Acinetobacter baumannii is a rare but clinically important pathogen because of its ability to survive under adverse conditions and spread rapidly in hospital settings.7 More importantly, the increasing prevalence of carbapenem resistance has further complicated the treatment of Acinetobacter baumannii infections, especially in refractory infections like IE.6 Data from the China Antimicrobial Surveillance Network indicated that carbapenem resistance among Acinetobacter baumannii isolates remained consistently high at 75–78%.8 Carbapenem-resistant Acinetobacter baumannii (CRAB) has become endemic across Europe, South America, Asia, and Africa, causing more than 50,000 deaths annually worldwide.9 Nevertheless, effective regimens for CRAB infection remain limited, and for CRAB-related IE in particular, evidence is restricted to sporadic case reports without standardized antimicrobial recommendations.3,10–12
Eravacycline, a novel fluorocycline, has demonstrated potent in vitro activity and favorable clinical efficacy comparable to that of tigecycline against CRAB infections.13 Real world data suggests that the 30-day survival rate for patients with CRAB infections treated with eravacycline was 75%.14 Cefiderocol, a novel siderophore containing cephalosporin, also exhibits strong in vitro activity against CRAB, with meta-analyses suggesting superior clinical efficacy compared with the best available therapy.15–17 To the best of our knowledge, no cases of IE treated with eravacycline have been reported, and only three cefiderocol-treated IE cases have been published, all achieving successful pathogen eradication.18–20 The present study details a rare case of IE induced by CRAB, in which the bloodstream infection was successfully eliminated by an innovative combination regimen of eravacycline and cefiderocol. Furthermore, we reviewed the clinical characteristics and treatment strategies of CRAB-related IE to provide evidence for the management of this refractory infection.
Case Presentation
A 66-year-old man was admitted with a 10-day history of persistent fever accompanied by chills, fatigue, cough, and dysuria. He had a two-year history of hypertension and a pacemaker implanted over 20 years ago due to bradycardia, with a permanent dual-chamber replacement 1 year 8 months ago. Eight years prior, he underwent biological aortic valve replacement, and due to valve aging, he had a second biological aortic valve replacement and tricuspid valve repair 2 months earlier, after which warfarin was prescribed. In the early stage of fever, treatment with moxifloxacin (400 mg qd) at a local facility was ineffective. Although methylprednisolone (40 mg qd) administered 8 days prior transiently reduced the fever, symptoms recurred shortly thereafter. Transferred to another hospital a week prior, blood cultures (four times) and metagenomic next-generation sequencing (mNGS) confirmed CRAB. The brain, lung, abdominal, and cardiac imaging of the external hospital failed to identify infection site. Despite receiving meropenem (1000 mg tid) and tigecycline (50 mg bid), fever and chills persisted, suggesting a possible persistent bloodstream infection or localized infection. He was therefore referred to our department for further diagnosis and treatment.
Diagnosis of Prosthetic Valve Endocarditis and Persistent CRAB Infection
Due to the diagnosis of CRAB infection, the patient underwent isolation upon admission. Physical examination revealed palpebral conjunctiva haemorrhage, skin petechiae and ecchymoses, and a diastolic murmur over the aortic valve. Laboratory examination showed moderate anemia (87 g/L), leukocytosis (19.41×109/L), positive rheumatoid factor (44.43 IU/mL), and elevated C-reactive protein (184.57 mg/L) (Table S1). Initial therapy with cefoperazone/sulbactam (3000 mg bid) combined with polymyxin B (700,000 U bid) was administered based on coagulation status and antimicrobial susceptibility results (Table 1), but symptoms persisted. Lung CT revealed an opacity in the right lung (Figure 1A), while transthoracic echocardiography (TTE) suggested potential bioprosthetic valve restenosis. The patient subsequently developed somnolence, and brain CT showed cerebellar hemorrhage (Figure 1B), leading to discontinuation of warfarin and postponement of transesophageal echocardiography (TEE). According to the 2023 Duke-ISVID criteria,21 he met one primary criterion (≥3 positive blood cultures) and four secondary criteria (valve surgery history, fever, hemorrhage, and positive rheumatoid factor), establishing IE diagnosis, particularly with prosthetic valve endocarditis (PVE). Surgical intervention was deferred due to the high operative risk following recent valve surgery. Given concerns about nephrotoxicity with polymyxin B and amikacin, a combination of eravacycline (70 mg bid) and sulbactam (2000 mg tid) was employed to treat the persistent CRAB bloodstream infection.
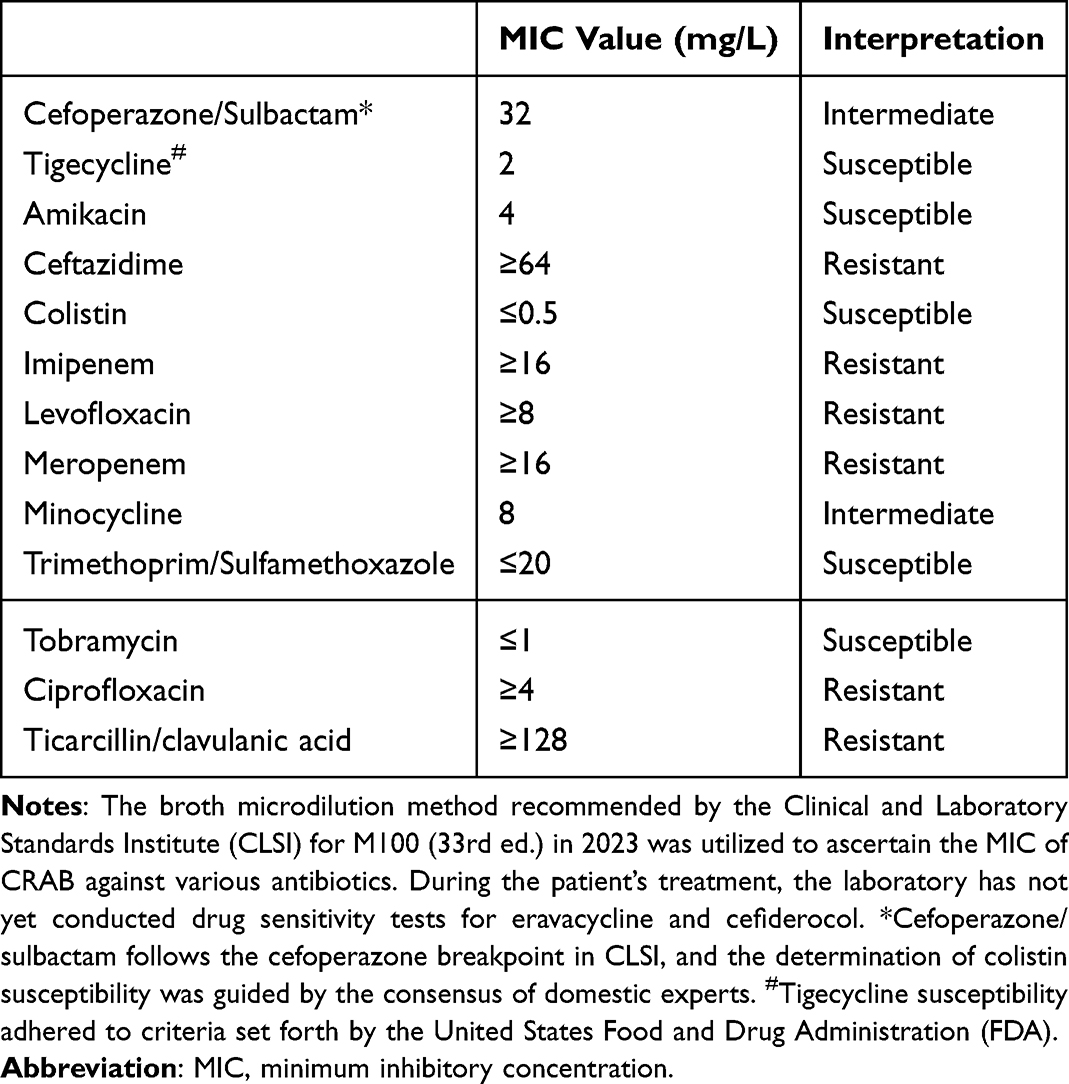 |
Table 1 Antimicrobial Susceptibility Testing Results for the Isolate in the Study |
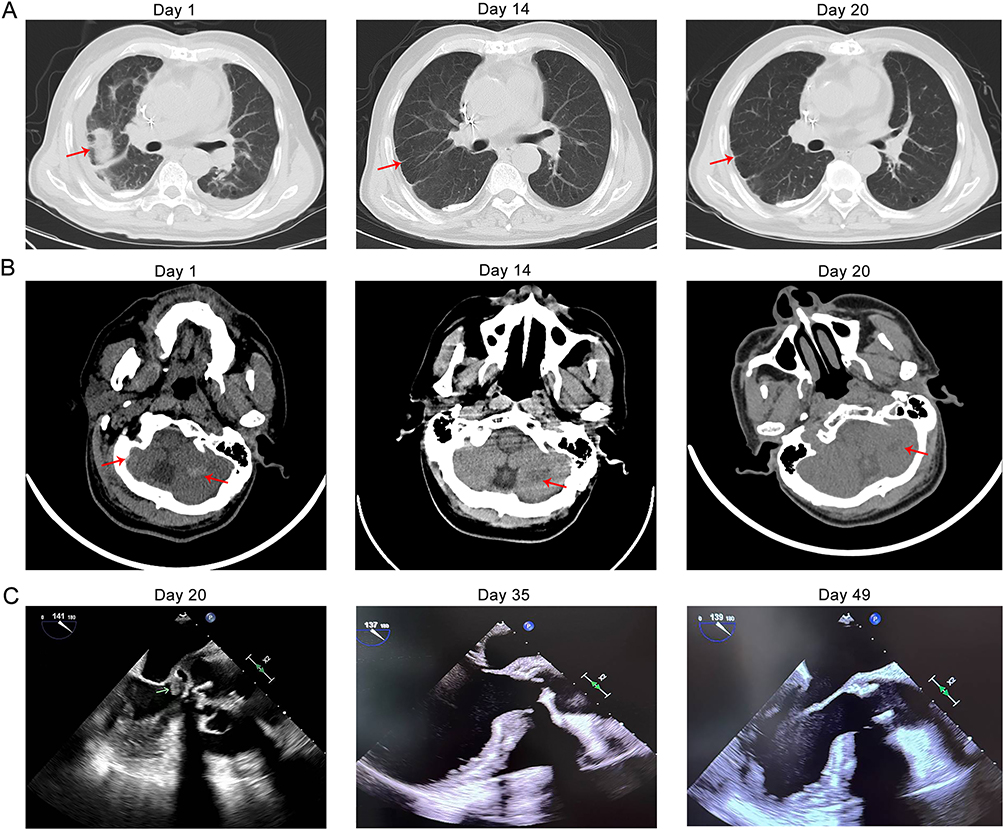 |
Figure 1 Images of the patient before and after treatment. (A) Upon admission, the lung CT plain scan revealed opacity in the right lung (red arrow); on day 14 and day 20, the right lung patchy was observed to be absorbed (red arrow). (B) Upon admission, brain CT scan revealed the presence of bilateral cerebellar hemisphere cerebral hemorrhage (red arrow); on day 14 and day 20, a notable regression in the size of the hemorrhage foci was observed. (C) On day 20, transesophageal echocardiography revealed the presence of aortic valve vegetation (green arrow); on day 35 and day 49, reexamination by transesophageal echocardiography revealed the absence of vegetation. |
Eravacycline–Cefiderocol Combination Therapy with Clinical Improvement
On hospital day 6, abnormal coagulation functions prompted the discontinuation of cefoperazone/sulbactam. Although three blood cultures obtained at our hospital were negative, blood mNGS detected 44 Acinetobacter baumannii sequences (Table S2). On day 11, worsening skin itching and renal impairment (creatinine peak 216 µmol/L) led to discontinuation of polymyxin B, and antimicrobial therapy was adjusted to sulbactam (1000 mg tid), eravacycline, and cefiderocol (1000 mg tid). Imaging on day 14 revealed resolution of right lung lesion (Figure 1A) and reduction of cerebellar hemorrhage (Figure 1B), alongside improvements in body temperature, inflammatory markers, and coagulation function (Table S1).
From days 15 to 19, the patient exhibited psychiatric symptoms (insomnia and irritability), and was diagnosed with hypernatremia (peak sodium level of 156.1 mmol/L). Subsequent mNGS still revealed 5 Acinetobacter baumannii sequences (Table S2). Due to sulbactam’s high sodium content and the improved coagulation function, it was replaced with cefoperazone/sulbactam (3000 mg bid), and cefiderocol was increased to 1500 mg tid, resulting in normalization of sodium levels and improvement of consciousness. TEE on day 20 identified aortic valve vegetation (Figure 1C), further supporting the previous diagnosis of IE. The dosage of cefiderocol was increased to 2000 mg tid, but two days later, psychiatric symptoms re-emerged. After reducing cefiderocol to 1500 mg tid, the psychiatric symptoms resolved.
Effective Infection Control but Subsequent Relapse
On hospital day 26, negative mNGS result indicated the elimination of bloodstream infection. By day 35, TTE and TEE showed no vegetation, although a paravalvular leak (shunt 2.5 mm, Figure 1C) was noted. The patient remained afebrile after day 36. However, on day 41, thrombocytopenia (89×109/L) prompted discontinuation of cefoperazone/sulbactam. By day 49, TEE confirmed absence of vegetation, but revealed a paravalvular aortic valve leak (shunt 2.8 mm, Figure 1C). The patient was discharged on hospital day 53 after two weeks of sustained defervescence, with laboratory parameters normalized except for anemia (Table S1, Figure 2).
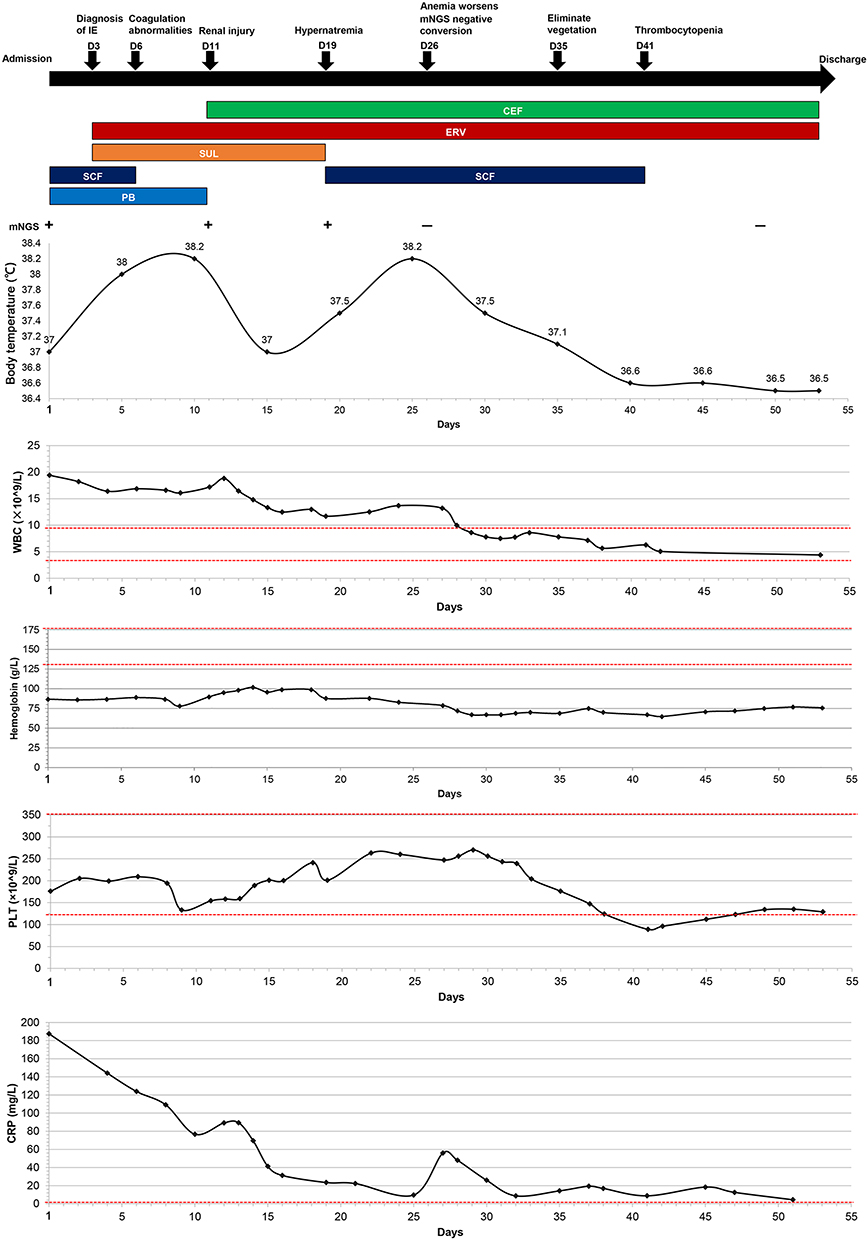 |
Figure 2 The clinical course of the patient after treatment included therapeutic regimen, mNGS, body temperature, WBC, hemoglobin, PLT, and CRP during hospitalization. The “+” indicates mNGS-positive, and “−” indicates mNGS-negative. The red dashed line indicates the normal reference value of the corresponding indices. Abbreviations: IE, infective endocarditis; mNGS, Metagenomics next generation sequencing; CEF, cefiderocol; ERV, Eravacycline; SUL, sulbactam; SCF, Cefoperazone/sulbactam; PB, Polymyxin B; WBC, white blood count; PLT, blood platelet; CRP, C-reactive protein. |
Unfortunately, the patient experienced fever again one week after discharge. Repeat TEE showed further enlargement of the aortic valve leakage, suggesting possible persistent occult infection of the prosthetic valve. Although bloodstream infection and vegetation had resolved during hospitalization, definitive surgical intervention was required for source control. Given the high operative risk after multiple recent valve surgeries, surgery was not feasible. The patient ultimately passed away one month after discharge.
Discussion
CRAB is a highly resistant Gram-negative pathogen forming bacterium that predominantly found in the respiratory tract or within wounds. The incidence of IE attributed to CRAB is remarkably rare and remains difficult to manage because of extensive antimicrobial resistance and the lack of standardized treatment strategies. This study successfully eliminated CRAB bloodstream infection for the first time by employing a novel combined anti-infection regimen, while maintaining safety by timely adjustments to medication and dosages. Moreover, this case emphasizes the critical need for the enhancement of infection control measures.
Diagnostic Challenges in CRAB-IE
The clinical manifestations of IE are complex and varied, with persistent fever being the most common symptom.22 In this case, the patient presented with persistent fever which raised a high clinical suspicion for IE.1 Nevertheless, diagnosis of CRAB-IE in this case was challenging because prior antibiotic exposure resulted in negative blood cultures at our institution. Although blood culture remains the cornerstone of IE diagnosis in the 2023 Duke-ISCVID criteria, molecular methods such as mNGS may provide important complementary value, particularly in blood culture-negative IE.21 mNGS, a high-throughput sequencing technology capable of pathogen detection within approximately 48 hours, has been shown to significantly improve microbiological diagnosis in IE, particularly in blood culture-negative cases.23–26 In our patient, blood mNGS confirmed the presence of Acinetobacter baumannii nucleic acid fragments and supported subsequent antimicrobial management. However, despite reflecting the number of distinct and unique sequences aligned to microorganism’s genome, mNGS results should be interpreted with caution, as non-pathogenic microorganisms may be detected.23 Furthermore, mNGS does not provide antimicrobial susceptibility testing results, and its cost remains relatively expensive at 3500 RMB (approximately 500 USD) per sample. Collectively, although mNGS has not yet become the gold standard for pathogen detection, it may improve microbiological diagnosis in patients with suspected IE and repeatedly negative blood cultures.
In addition, echocardiography serves as the footstone for imaging diagnosis of IE TTE exhibits limited sensitivity, whereas TEE facilitates more comprehensive evaluation of the valve and the extent of infection. Nonetheless, the potential risks of bleeding should be carefully considered.21 In our case, TEE was postponed due to the patient’s new onset of cerebellar hemorrhage. After the alleviation of symptoms, TEE revealed the formation of aortic valve vegetation, which further supported the diagnosis of IE. Despite the anatomical implications of pacemaker leads and artificial heart valves affecting each other, there is currently no evidence of pacemaker lead infections being observed through TEE. In summary, this case highlights the importance of integrating microbiological and imaging modalities in diagnostically complex IE cases.
Therapeutic Challenges and Strategic Management of CRAB-IE
Currently, the treatment of IE relies on clinical features and pathogen detection.27 Initial treatment of IE is generally empirical and requires comprehensive evaluation of patient characteristics and epidemiological factors, with antibiotic selection, dosage, and duration in acute cases guided by the minimum inhibitory concentration (MIC) derived from blood cultures. Indeed, CRAB remains one of the most difficult multidrug-resistant pathogens to treat because of its frequent extensive drug resistance (XDR) and limited susceptibility to available agents.28 According to in vitro sensitivity, polymyxin, tigecycline, and sulbactam are the conventional antimicrobials for CRAB infections.29 However, the emerging resistance to colistin and/or tigecycline has greatly limited the applicability of these traditional agents.30,31 Recent IDSA guidelines recommend sulbactam-containing regimens for CRAB infections, preferably sulbactam/durlobactam in combination with carbapenems, or alternatively high-dose ampicillin/sulbactam combined with another active agent.32 Unfortunately, sulbactam/durlobactam and ampicillin/sulbactam were not available during the treatment of our case. Consistent with international consensus, combination therapy is superior to monotherapy for high-risk CRAB infections owing to antimicrobial synergism.33,34 In alignment with in vitro sensitivity testing and international guidelines, the patient initially received sequential multidrug combination therapy comprising polymyxin B, sulbactam, cefoperazone/sulbactam, and other anti-infective agents. However, persistent fever and positive mNGS indicated unresolved bacteremia. Subsequently, polymyxin B was discontinued owing to the occurrence of skin irritation and renal impairment,35 sulbactam was discontinued due to neurological symptoms linked to hypernatremia,36 and cefoperazone/sulbactam was ceased due to thrombocytopenia.37 During the initial treatment phase, the combination of sulbactam-containing agent, eravacycline, and cefiderocol successfully eradicated the bloodstream infection. In the subsequent phase, eravacycline combined with cefiderocol was continued to stabilize the patient’s condition and avert recurrence, highlighting the potential efficacy of this novel regimen for CRAB-IE. Moreover, our review of the treatment strategies for only four cases of CRAB-IE revealed high mortality despite appropriate antimicrobial therapy with only one patient surviving, and no prior reports have described the use of eravacycline and cefiderocol for CRAB-IE (Table 2).3,10–12 Eravacycline inhibits protein synthesis at the 30S ribosomal subunit, retaining activity against efflux pump and ribosomal protection mechanisms.13 Cefiderocol exploits siderophore-mediated uptake to penetrate the outer membrane and inhibit cell wall synthesis, circumventing β-lactamase and porin loss resistance.38,39 Their complementary targets may theoretically confer synergistic activity and enhanced biofilm penetration. It is noteworthy that the present combination was attempted in this case solely because the guideline-concordant agent was unavailable and empirical therapy had failed. Accordingly, this regimen should be regarded as exploratory rather than standard treatment, and its efficacy and safety require further investigation.
 |
Table 2 Summary of Previously Reported Carbapenem-Resistant Acinetobacter baumannii Infective Endocarditis |
Although the eravacycline combined with cefiderocol was generally tolerated, careful monitoring for adverse reactions remained essential. Unlike a previous report describing acute neutropenia in the treatment during cefiderocol-based therapy for XDR Pseudomonas aeruginosa-induced endocarditis,18 no neutropenia was observed in our patient. However, psychiatric symptoms developed after cefiderocol-dose escalation and resolved following dose reduction, suggesting possible dose-related neurotoxicity.40,41 Moreover, although Phase II/III trials and post-hoc analysis of the APEKS-NP study did not demonstrate significant effects of cefiderocol on iron homeostasis or anemia, Schellong P reported anemia and iron deficiency after prolonged cefiderocol administration for 169 days.42 Similarly, anemia present at admission in our patient appeared to worsen during therapy, highlighting the need for close neurological and hematological monitoring during cefiderocol treatment.
Importance of Early Surgical Intervention in CRAB-IE
Surgical intervention remains crucial in IE caused by CRAB because it can eradicate the infection source, repair the cardiac structure, and reduce embolic complications.43 Although bloodstream infections and vegetation were effectively controlled during hospitalization, the patient developed progressive perivalvular leakage, suggesting ongoing valvular or paravalvular destruction despite microbiological clearance. Furthermore, the patient’s bioprosthetic valve is susceptible to bacterial adhesion, increasing the risk of recurrent infections. Recurrence of fever after discharge and worsening leakage on repeat TEE further indicated progressive enlargement of the paravalvular leak, for which surgical intervention represented the only viable treatment option. However, re-operation was not considered feasible because of the recent prior valve surgery and high surgical risk. This case highlights that, in refractory IE caused by drug-resistant pathogens, timely surgical intervention remains essential even after apparent microbiological improvement, particularly in patients with progressive perivalvular leakage.
One limitation of this study is the relatively small number of reported CRAB-IE cases, which restricts the scope and generalizability of our literature review. While we have summarized published cases from recent years and integrated them with clinical and therapeutic analysis of the present case, large-scale clinical studies are needed to validate the efficacy and safety of this novel combination regimen.
Conclusion
This case report documents a rare instance of infective endocarditis caused by CRAB successfully treated with eravacycline and cefiderocol, with favorable safety maintained through timely medication and dosage adjustment. Our case highlights the growing threat posed by carbapenem-resistant Gram-negative pathogens and the urgent necessity for new antibiotic development. The combination of eravacycline and cefiderocol may provide a promising therapeutic option for refractory drug-resistant infections and help optimize treatment strategies against antimicrobial resistance. Furthermore, in cases of refractory IE caused by drug-resistant bacteria, especially PVE, surgical intervention may be necessary Further clinical studies are warranted to confirm the efficacy and safety of this combination regimen.
Data Sharing Statement
All data generated or analysed during this study are included in this published article and its supplementary information files.
Ethics Approval and Informed Consent
Written informed consent was obtained from the patient’s family for publication of this case report. Institutional review board approval was not required for this single-patient case report, and all identifying details have been removed to maintain confidentiality.
Acknowledgments
We would like to acknowledge and thank the patient’s family who provided written informed consent to publish details of this case.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by funds from Jilin Province Health Science and Technology Capacity Improvement Project (2021JC001) and Jilin Provincial Department of Science and Technology (20200201616JC).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Li M, Kim JB, Sastry BKS, Chen M. Infective endocarditis. Lancet. 2024;404(10450):377–10. doi:10.1016/S0140-6736(24)01098-5
2. Hammond-Haley M, Hartley A, Al-Khayatt BM, et al. Trends in the incidence and mortality of infective endocarditis in high-income countries between 1990 and 2019. Int J Cardiol. 2023;371:441–451. doi:10.1016/j.ijcard.2022.09.061
3. Olut AI, Erkek E. Early prosthetic valve endocarditis due to Acinetobacter baumannii: a case report and brief review of the literature. Scand J Infect Dis. 2005;37(11–12):919–921. doi:10.1080/00365540500262567
4. Ambrosioni J, Hernández-Meneses M, Durante-Mangoni E, et al. Epidemiological changes and improvement in outcomes of infective endocarditis in Europe in the twenty-first century: an International Collaboration on Endocarditis (ICE) prospective cohort study (2000–2012). Infect Dis Ther. 2023;12(4):1083–1101. doi:10.1007/s40121-023-00763-8
5. Sengupta SP, Prendergast B, Laroche C, et al. Socioeconomic variations determine the clinical presentation, aetiology, and outcome of infective endocarditis: a prospective cohort study from the ESC-EORP EURO-ENDO (European infective endocarditis) registry. Eur Heart J Qual Care Clin Outcomes. 2022;9(1):85–96. doi:10.1093/ehjqcco/qcac012
6. Pitsikakis K, Skandalakis M, Fragkiadakis K, Baliou S, Ioannou P. Infective endocarditis by carbapenem-resistant Gram-negative bacteria – a systematic review. Germs. 2024;14(2):149–161. doi:10.18683/germs.2024.1427
7. Müller C, Reuter S, Wille J, et al. A global view on carbapenem-resistant Acinetobacter baumannii. mBio. 2023;14(6):e0226023. doi:10.1128/mbio.02260-23
8. Yang W, Ding L, Han R, et al. Current status and trends of antimicrobial resistance among clinical isolates in China: a retrospective study of CHINET from 2018 to 2022. One Health Adv. 2023;1(1):8. doi:10.1186/s44280-023-00009-9
9. Boutzoukas A, Doi Y. The global epidemiology of carbapenem-resistant Acinetobacter baumannii. JAC Antimicrob Resist. 2025;7(4):dlaf134. doi:10.1093/jacamr/dlaf134
10. Patel G, Perez F, Hujer AM, et al. Fulminant endocarditis and disseminated infection caused by carbapenem-resistantA cinetobacter baumanniiin a renal-pancreas transplant recipient. Transpl Infect Dis. 2015;17(2):289–296. doi:10.1111/tid.12351
11. Chen Q, Cao H, Lu H, Qiu Z-H, He -J-J. Bioprosthetic tricuspid valve endocarditis caused by Acinetobacter baumannii complex, a case report and brief review of the literature. J Cardiothorac Surg. 2015;10(1):149. doi:10.1186/s13019-015-0377-8
12. Durante-Mangoni E, Andini R, Agrusta F, et al. Infective endocarditis due to multidrug resistant gram-negative bacilli: single centre experience over 5years. Eur J Intern Med. 2014;25(7):657–661. doi:10.1016/j.ejim.2014.05.015
13. Chen D, Lan H, Yang W, et al. Comparative in vitro activity and clinical outcomes of eravacycline, tigecycline, and omadacycline against carbapenem-resistant Acinetobacter baumannii and Klebsiella pneumoniae. Infect Drug Resist. 2026;19:583973. doi:10.2147/IDR.S583973
14. Alosaimy S, Morrisette T, Lagnf AM, et al. Clinical outcomes of eravacycline in patients treated predominately for carbapenem-resistant Acinetobacter baumannii. Microbiol Spectr. 2022;10(5):e0047922. doi:10.1128/spectrum.00479-22
15. Karruli A, Migliaccio A, Pournaras S, Durante-Mangoni E, Zarrilli R. Cefiderocol and sulbactam-durlobactam against carbapenem-resistant Acinetobacter baumannii. Antibiotics. 2023;12(12):1729. doi:10.3390/antibiotics12121729
16. Kollef M, Dupont H, Greenberg DE, et al. Prospective role of cefiderocol in the management of carbapenem-resistant Acinetobacter baumannii infections: review of the evidence. Int J Antimicrob Agents. 2023;62(2):106882. doi:10.1016/j.ijantimicag.2023.106882
17. Onorato L, de Luca I, Monari C, Coppola N. Cefiderocol either in monotherapy or combination versus best available therapy in the treatment of carbapenem-resistant Acinetobacter baumannii infections: a systematic review and meta-analysis. J Infect. 2024;88(3):106113. doi:10.1016/j.jinf.2024.01.012
18. Edgeworth JD, Merante D, Patel S, et al. Compassionate use of cefiderocol as adjunctive treatment of native aortic valve endocarditis due to extremely drug-resistant pseudomonas aeruginosa. Clin Infect Dis. 2019;68(11):1932–1934. doi:10.1093/cid/ciy963
19. La Bella G, Salvato F, Minafra GA, et al. Successful treatment of aortic endocarditis by Achromobacter xylosoxidans with cefiderocol combination therapy in a non-hodgkin lymphoma patient: case report and literature review. Antibiotics. 2022;11(12):1686. doi:10.3390/antibiotics11121686
20. Tascini C, Antonelli A, Pini M, et al. Infective endocarditis associated with implantable cardiac device by metallo-β-lactamase-producing pseudomonas aeruginosa, successfully treated with source control and cefiderocol plus imipenem. Antimicrob Agents Chemother. 2023;67:e0131322. doi:10.1128/aac.01313-22
21. Fowler VG, Durack DT, Selton-Suty C, et al. The 2023 duke-international society for cardiovascular infectious diseases criteria for infective endocarditis: updating the modified duke criteria. Clin Infect Dis. 2023;77(4):518–526. doi:10.1093/cid/ciad271
22. Stavropoulou E, Monney P, Tzimas G, et al. Predictors of persistent fever among patients with suspected infective endocarditis: think outside the box. Clin Infect Dis. 2025;80(4):795–803. doi:10.1093/cid/ciae588
23. Haddad SF, DeSimone DC, Chesdachai S, Gerberi DJ, Baddour LM. Utility of metagenomic next-generation sequencing in infective endocarditis: a systematic review. Antibiotics. 2022;11(12):1798. doi:10.3390/antibiotics11121798
24. Wang W, Chen F, Ye L, et al. Enhanced diagnostic yield and clinical impact of metagenomic next-generation sequencing in infective endocarditis: a continuous and prospective surgical cohort study. Int J Surg. 2026;112(2):3372–3387. doi:10.1097/JS9.0000000000003954
25. Wang R, Niu B, Ren J, Zhang L. Infective endocarditis caused by Streptococcus sinensis diagnosed with next-generation sequencing: a case report and literature review. BMC Infect Dis. 2025;25(1):425. doi:10.1186/s12879-025-10837-2
26. Wang Q, Song Y, Han D, et al. The first suspected disseminated Hormographiella aspergillata infection in China, diagnosed using metagenomic next-generation sequencing: a case report and literature review. Emerg Microbes Infect. 2023;12(1):2220581. doi:10.1080/22221751.2023.2220581
27. Sebastian SA, Co EL, Mehendale M, Sudan S, Manchanda K, Khan S. Challenges and updates in the diagnosis and treatment of infective endocarditis. Curr Problems Cardiol. 2022;47(9):101267. doi:10.1016/j.cpcardiol.2022.101267
28. Piperaki E-T, Tzouvelekis LS, Miriagou V, Daikos GL. Carbapenem-resistant Acinetobacter baumannii: in pursuit of an effective treatment. Clin Microbiol Infect. 2019;25(8):951–957. doi:10.1016/j.cmi.2019.03.014
29. Iovleva A, Fowler VG Jr, Doi Y. Treatment approaches for carbapenem-resistant acinetobacter baumannii infections. Drugs. 2025;85(1):21–40. doi:10.1007/s40265-024-02104-6
30. Qureshi ZA, Hittle LE, O’Hara JA, et al. Colistin-resistant Acinetobacter baumannii: beyond carbapenem resistance. Clin Infect Dis. 2015;60(9):1295–1303. doi:10.1093/cid/civ048
31. Iovleva A, McElheny CL, Fowler EL, et al. In vitro activity of sulbactam-durlobactam against colistin-resistant and/or cefiderocol-non-susceptible, carbapenem-resistant Acinetobacter baumannii collected in U.S. hospitals. Antimicrob Agents Chemother. 2024;68(3):e0125823. doi:10.1128/aac.01258-23
32. Tamma PD, Heil EL, Justo JA, Mathers AJ, Satlin MJ, Bonomo RA. Infectious diseases society of America 2024 guidance on the treatment of antimicrobial-resistant gram-negative infections. Clin Infect Dis. 2024;7:ciae403.
33. Schmid A, Wolfensberger A, Nemeth J, Schreiber PW, Sax H, Kuster SP. Monotherapy versus combination therapy for multidrug-resistant gram-negative infections: systematic review and meta-analysis. Sci Rep. 2019;9(1):15290. doi:10.1038/s41598-019-51711-x
34. Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious diseases society of America guidance on the treatment of AmpC β-lactamase-producing enterobacterales, carbapenem-resistant Acinetobacter baumannii, and stenotrophomonas maltophilia infections. Clin Infect Dis. 2022;74(12):2089–2114. doi:10.1093/cid/ciab1013
35. Nang SC, Azad MAK, Velkov T, Zhou QT, Li J. Rescuing the last-line polymyxins: achievements and challenges. Pharmacol Rev. 2021;73(2):679–728. doi:10.1124/pharmrev.120.000020
36. Bamberg M, Menger MM, Thiel JT, Lauer H, Viergutz T, Fontana J. Antibiotics in patients with severe burn injury—A modifiable variable in hypernatremia etiology. Injury. 2024;55(9):111573. doi:10.1016/j.injury.2024.111573
37. Wang W, Liu Y, Yu C, et al. Cefoperazone-sulbactam and risk of coagulation disorders or bleeding: a retrospective cohort study. Expert Opin Drug Saf. 2020;19(3):339–347. doi:10.1080/14740338.2020.1713090
38. Lee YR, Yeo S. Cefiderocol, a new siderophore cephalosporin for the treatment of complicated urinary tract infections caused by multidrug-resistant pathogens: preclinical and clinical pharmacokinetics, pharmacodynamics, efficacy and safety. Clin Drug Investig. 2020;40(10):901–913. doi:10.1007/s40261-020-00955-x
39. Tamma PD, Hsu AJ. Defining the role of novel β-lactam agents that target carbapenem-resistant gram-negative organisms. J Pediatric Infect Dis Soc. 2019;8(3):251–260. doi:10.1093/jpids/piz002
40. Hagiya H, Miyawaki K, Yamamoto N, et al. Ceftriaxone-induced neurotoxicity in a patient after pancreas-kidney transplantation. Intern Med. 2017;56(22):3103–3107. doi:10.2169/internalmedicine.8774-16
41. Bhattacharyya S, Darby RR, Raibagkar P, Gonzalez Castro LN, Berkowitz AL. Antibiotic-associated encephalopathy. Neurology. 2016;86(10):963–971. doi:10.1212/WNL.0000000000002455
42. Schellong P, Wennek-Klose J, Spiegel C, Rödel J, Hagel S. Successful outpatient parenteral antibiotic therapy with cefiderocol for osteomyelitis caused by multi-drug resistant gram-negative bacteria: a case report. JAC Antimicrob Resist. 2023;6(1):dlae015. doi:10.1093/jacamr/dlae015
43. Delgado V, Ajmone Marsan N, de Waha S, et al. 2023 ESC guidelines for the management of endocarditis. Eur Heart J. 2023;44(39):3948–4042. doi:10.1093/eurheartj/ehad193
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.