")
Back to Journals » Adolescent Health, Medicine and Therapeutics » Volume 7
Epilepsy: addressing the transition from pediatric to adult care
Authors Rajendran S, Iyer A
Received 16 November 2015
Accepted for publication 15 April 2016
Published 27 June 2016 Volume 2016:7 Pages 77—87
DOI https://doi.org/10.2147/AHMT.S79060
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Alastair Sutcliffe
Seetha Rajendran, Anand Iyer
Department of Paediatric Neurology, Neurosciences Unit, Alder Hey Children’s NHS Foundation Trust, Liverpool, UK
Abstract: Adolescence is a period of rapid change, both physical and psychosocial for any young person. It can be challenging when they have ongoing health problems and when their care needs to be transitioned to the adult health care system. Transition should be a planned process of addressing the medical and associated comorbid conditions from pediatric to adult care in a coordinated manner. In most cases, the young person and their family are well known to the pediatrics services and have built a relationship based on trust and often friendship over many years. Understandably, there is significant apprehension about moving from this familiar setting to the unknown adult services. Apart from having a sound knowledge of specific childhood epileptic conditions and associated comorbid disorders, it is important that both the pediatric and adult epilepsy teams are motivated to provide a successful and safe transition for these patients. It is essential that transition is seen as a continual process and not as a single event, and good preparation is the key to its success. It is also important that general practitioners are closely engaged to ensure successful transition. An overview of how to effectively address transition in epilepsy, different models of transition, transition of relevant epilepsies, and their management is discussed.
Keywords: epilepsy, transition, adolescence
Introduction
Epilepsy is the most common neurological condition in adolescence, with an incidence of approximately five to seven cases per 10,000 children from birth to 15 years of age, and prevalence of five in 1,000 children.1 Epilepsy in children and young people can be associated with comorbidities, including motor impairments, learning difficulties, behavioral problems, and mental health issues. The British Child and Adolescent Mental Health Survey found that >25% of children with epilepsy between the ages of 5 years and 14 years had emotional, behavioral, and relationship difficulties in comparison to 9% of controls and 11% of children with diabetes, this figure rose to 56% in children with epilepsy and comorbid neurological problems.2 Children with epilepsy may grow up to have significant social problems in adulthood with regard to employment and independent living. These trends have been noted in large population-based long-term follow-up studies in different countries.3 The influence of epilepsy on social outcome was greater than in other childhood chronic disease control groups. Comparison of social outcome of children with childhood absence epilepsy (CAE) and juvenile rheumatoid arthritis revealed that children with CAE had higher rates of unskilled labor and behavioral and psychiatric difficulties.4
In ∼50% of cases, epilepsy with onset in childhood fails to remit.5 There are three recognized patterns of evolution of childhood epilepsy. First, there is epilepsy with onset in childhood, where seizures are likely to remit during adolescence, but the associated comorbidities such as cognitive deficit and behavior disorders may persist into adolescence and adulthood. An example is benign epilepsy with centrotemporal spikes (childhood rolandic epilepsy), which usually remits toward late adolescence. Second, there is epilepsy with onset in early infancy or childhood, which persists as they grow up and is associated with learning difficulties and other comorbidities. An example would be a child with West syndrome and tuberous sclerosis (TS), who continues to have drug-resistant epilepsy during adolescence with learning, psychiatric, and physical disorders. Third, there are epilepsies with onset in adolescence, which persists into adulthood such as juvenile myoclonic epilepsy (JME). This is quite a simplistic view to look at the epilepsies in children and young people and to think about addressing issues during transition. In reality, there are many different types of epilepsies that may not actually fit into these three distinct categories, and each young person with epilepsy would have to have a carefully tailored individual transition plan.
Adolescence is a critical period during development involving key biological and psychosocial elements. It is defined by National Institute for Health and Clinical Excellence (NICE) as “between the ages of 12 years and 17 years”; however, the World Health Organization defines the age as between 10 years and 19 years. In practice, 16 years or 17 years is usually the age when the young person would be transitioned from pediatric to adult services. This is purely an arbitrary figure based on local experience; however, the exact age for considering transition depends on joint agreement between the family and the clinician. Young people with learning difficulties often attend specialist schools till 19 years of age, and this may serve as a trigger for late transition of these patients. Adolescence is often a time of conflict when a young person aspires to develop a sense of identity and self-image. They start to develop cognitive skills such as abstract thinking, experiment with different behaviors, form relationships outside the family, and begin to develop emotional, personal, and financial independence from their parents. Understanding adolescent development is essential in caring for young people with the added burden of chronic disease during this crucial time in their lives.6
Epilepsy in adolescence is therefore an even greater challenge for the young person, their families, and the health care professionals. It interferes with the acquisition of independence and autonomy, as young people with epilepsy may need supervision for activities such as taking a bath, swimming, and going on school trips; and there are restrictions in some cases about drinking alcohol or staying out late in comparison to their peers. There are implications for career choices, leisure activities, driving regulations, pregnancy, contraception, and independent living. The success or failure of safe transition and the ability for health professionals to be able to address all these issues may have long-term implications in the well-being of the adolescent.
Importance of transition
Transition has been defined as a “purposeful planned process that addresses the medical, psychosocial, and educational/vocational needs of young people with chronic physical and medical conditions as they move from child-centered to adult-oriented health care systems”. In contrast to “transfer” of care, which is seen as a single event involving the handover of care from one team to another, “transition” is a dynamic and structured process, which involves planning, preparation, and involvement of a skilled team in ensuring a seamless continuation of care from pediatric to adult services.
The National Services Framework (NSF), UK document Transition: Getting it right for young people states that “young people with neurological disorders and disabilities are the least well served as there is often no service available to take over their care when they leave pediatrics.”7 Transition is an important issue in recent years as there is increased survival to adulthood of children with complex conditions. Adult health care services may have limited knowledge and resources to cope with challenges faced by these young people and families. Effective transition is shown to improve longer term outcomes and the young persons’ experience of the process, which in turn is a positive factor in aiding compliance with care. When poorly planned, there is a risk of nonadherence to treatment and possible loss to follow-up, which can result in serious consequences for the young person in terms of morbidity and mortality. A few key principles of transition planning have been outlined in Table 1 and have been adapted from the document Transition: moving on well published by the Department of Health, UK, in 2008.8
 | Table 1 The key principles of health transition planning Notes: Adapted from Transition: moving on well. Department of Health [UK]. Available from: http://www.bacdis.org.uk/policy/documents/transition_moving-on-well.pdf. Accessed November 16, 2015. © Crown copyright 2008. Contains public sector information licensed under the Open Government Licence v3.0.8 |
Challenges during transition
The transition process can be interrupted by several barriers, one of which being the reluctance of families. This is due to the loss of the longstanding relationship between them and the pediatric team whom they trust and have developed a friendly bond. The care provision in pediatrics is more nurturing and family centered. Pediatric neurologists have a holistic view of the young person’s health, including management of common associated pediatric disorders. The consultation focuses not only on the child and young person but also on several aspects of the impact of epilepsy on the whole family. In most secondary care hospitals across UK, epilepsy in children and young people is managed by pediatricians with expertise in epilepsy and epilepsy nurse specialists, with selective input from the tertiary-based pediatric neurologists for difficult to control epilepsies. However, discussions around independence, sexual health, career choices, and several other aspects do not take precedence and are perceived as inappropriate in presence of parents.
In comparison, the adult setting is more autonomous, and the young person is likely to be seen alone with a structured consultation. They may have less frequent follow-up visits, and the onus is on the young person to seek help independently when required. This will depend on the young person having good knowledge of his/her condition and treatment and recognizing when they need help.3 These changes may have an adverse effect on the care of the young person, if there is an element of learning difficulties and discrepancy between their chronological age and emotional development. Adult health care professionals may not feel adequately trained to communicate with and look after young people with complex neurological disorders and moderate to severe cognitive impairment. This may also pose problems for periods where inpatient care is needed and an adult ward may not be able to recognize the finer aspects of care in complex young people with epilepsy and disabilities, for example, regarding different liquid preparations of antiepileptic medications to be given through the gastrostomy or other assisted feeding devices. In these cases, there also exists the issue of consent and lack of capacity of a young adult with cognitive impairment who will need an advocate to be responsible for consenting to assessment and treatment.
During their time in pediatric care, the young person may not have had much input from the general practitioner (GP) or other primary care professionals, who may now become the first point of contact for a young person in the community. This can cause the young person or the family to feel they are no longer receiving specialist’s care as they had done in pediatric care and may lead to difficulties in establishing a relationship with the primary care team in the longer term.
Therefore, preparing for transition is important, and it is essential that young people and their family have had a chance to reflect on the changes in care and the importance of empowering young people to take charge of their own health. A specific transition program called “Ready Steady Go” has been proposed by a university hospital, which can be used across all subspecialties.9 It is a structured, yet adaptable transition tool that is implemented through a series of questionnaires that assess knowledge of the condition, their treatment, and their clinicians, supports the development of self-advocacy, and encourages the practice of shared decision making at appropriate age. In addition, it also develops an understanding of the issues around a healthy lifestyle, sexual health, and relevant issues, including pregnancy. It also focuses on educational and vocational issues to ensure that the young person has realistic expectations about career options and a plan to achieve their potential. The Ready Steady Go program starts at 11 years of age and goes through different questionnaires for both the young person and their carer during different age groups, including when they are initially seen in the adult clinic. Feedback from young people and carers has been uniformly positive, and this is truly a reflection of adequate preparation in ensuring a successful transition.
Models of transition
There is little evidence to support a clear superior model for transition. However, the most prevalent method used appears to be transfer of care rather than true “transition” to adult clinic or GP.
In UK, there are four options for ongoing care of young people aged 16–19 with epilepsy. First, they can remain under pediatric services; second, be discharged to the care of the GP; third, be transferred to an adult neurologist or physician who may not have an interest in epilepsy; or fourth, be seen in a dedicated epilepsy transition service where specific adolescent and adult issues can be raised and discussed in an appropriate setting.
The first reported specific transition clinic for young people in the UK was in 1991 in Liverpool.10 In addition to providing an appropriate setting, where specific concerns faced by adolescents can be addressed and the process of transition to adult services facilitated, it was an opportunity to review their diagnosis and treatment. In 10%, the diagnosis was not epilepsy, and in 22%, changes were made to their antiepileptic medication. Establishing the correct diagnosis of the seizure type, epilepsy syndrome, comorbidities, and the underlying cause is imperative particularly at a time of transition of care. Failure to do so can lead to potentially lifelong implications for the young person, their life choices, and on-going psychosocial well-being.
A survey of transitional services for adolescents with epilepsy in 23 pediatric tertiary epilepsy centers in UK was conducted in 2011.11 It had a 78% response rate and found that 15 of the 18 units had a transition clinic and half of these were based in an adult neurology/epilepsy unit. In seven of the 15 clinics, the young person was only seen in the transition clinic once before transfer to the adult service. Of the 15 clinics, an adult and pediatric neurologist with a specific epilepsy interest supervised 93% jointly. In contrast, pediatric and adult epilepsy nurse specialists supported only 33% of the clinics jointly and 40% had no epilepsy nurse specialist support. Only five of the 15 clinics provided written information to the young people and their families prior to being seen in the transition service. Thus, this survey shows that despite the recognition of the need for a dynamic and seamless transition process, as endorsed by NSF and NICE, the requirements of this population remain unmet.
There are other models of transition internationally that have proven to be effective in their respective centers.12 In a tertiary specialist pediatric epilepsy center in Toronto, Canada, an adult epileptologist reviews patients ready for transition in a dedicated clinic.13 Before the clinic, an epilepsy fellow provides a written summary of the main problems experienced by the patient. The pediatric neurologist does not attend this clinic, but the pediatric epilepsy specialist nurse usually attends. Subsequent visits take place in the adult hospital and are led only by the adult epileptologist. A unique transition clinic occurs in Halifax, Nova Scotia, which is attended by the pediatric neurologist, adult epileptologist, and the adult epilepsy nurse specialist.3 Before the clinic, the pediatric neurologist prepares a detailed written summary of the medical epilepsy issues, and the family prepares a written summary of the psychosocial issues. The entire team extensively reviews these during the first visit; subsequently, there is one further follow-up visit with the similar team before being promoted to the adult clinic. In Edmonton, Alberta, there is a another transition model clinic that run exclusively by the epilepsy nurse specialists from both pediatrics and adult care – with referral letter detailing the patients’ epilepsy medical issues by the pediatric neurologist. The family discusses a number of key transition issues, and later during another consultation meets the adult epileptologist. Feedback from parents regarding this specific model was positive.14
In Paris, a single, dedicated adult neurologist with a specific interest in transition leads the transition clinic. The process involves a transfer summary from the pediatric neurologist with complete access to all pediatric medical records. An attempt to provide multidisciplinary care for patients with other comorbidities in this clinic has been useful. This center has proven to have implemented a satisfactory transition program for patients with Dravet syndrome.15
Clearly, some of these different models of care could be expensive, although a formal cost–benefit analysis has never been performed. Moreover, these models may not be able to serve the needs of patients who live remotely in rural areas and who may not have access to tertiary or quaternary care centers. A good model of transition, tailored not only to the local population but also to the individual young person, is essential to appropriate management of different epilepsies in adolescence and would in reality be cost effective in terms of longer term outcomes. Ideally, a transition clinic with the presence of both pediatric neurologist and pediatrician with expertise in epilepsy, and adult neurologists reviewing the young person for a few consultations before being promoted to the adult epilepsy clinic has worked well in many centers across the UK.
Transition in specific epilepsies
It is important to acknowledge that “epilepsies” in children have significant etiological and phenotypic heterogeneity, and an understanding of these would be essential for the adult epileptology team participating in the transition process. It also once again justifies the “joint clinic” transition model, where the pediatric neurologist, who would be well versed with the natural history and long-term prognosis of specific epilepsies, could be present to support and educate the adult team, and the patient, and families. A few key aspects of the heterogeneity in pediatric epilepsies and implications for transition will be outlined in this review.
There are a specific group of epilepsies with onset in childhood or adolescence with relatively normal cognition in whom there would be a good chance where the epilepsy may remit in later adulthood or adolescence. Benign epilepsy with centrotemporal spikes (childhood rolandic epilepsy) is one such condition that usually remits within 16 years of age. This fall into the category of nonlesional focal epilepsy in otherwise normal children (NLFN) present with electroclinical focal seizures with normal intellect, clinical examination, and normal neuroimaging, and about two-thirds of these will enter complete remission (defined as 5 years seizure-free and off antiepileptic medications) during adolescence. The risk of relapse following complete remission is <1% per year.16 Most of these epilepsies are pharmacosensitive. Problems with compliance and inappropriate medication choices may lead to poorly controlled epilepsy. Another important group is the adolescents with idiopathic generalized epilepsies, mainly JME. In all, 5%–15% of these individuals may have previously had CAE and may have been in remission before representing.16 Although JME has been considered to be a lifelong disorder with a high rate of recurrence after withdrawal of medications, large case series with longitudinal follow-up have shown that 25% remain seizure free after discontinuing medications.16 This may be linked to maturity and decisions over lifestyle choices such as drinking and sleep deprivation.
There are several genetic epileptic disorders that begin in childhood and persist into adulthood. Each of these has a characteristic phenotype that evolves through adulthood and has specific associated psychiatric, motor, and cognitive comorbidities. Dravet syndrome is the archetypal genetic epileptic encephalopathy, which has been extensively studied within the adult epilepsy centers.17 The epilepsy dampens down in adult life to weekly or monthly nocturnal focal or secondary generalized tonic–clonic seizures. Susceptibility to temperature-induced status epilepticus persists, although these are rare. Focal dyscognitive seizures form the main type of seizures, atypical absence, and myoclonic seizures decrease. A pattern of fluctuating fragmentary myoclonus may emerge in adult life. The changes in behavior occur, with hyperactivity replaced by extreme slowness and perseveration in movements, thinking, and verbal expression. The gait may deteriorate, and attention to supporting the mobility and surveillance for complications such as kyphoscoliosis associated with poor posture is essential. Other commonly encountered monogenic epilepsies include the glucose transporter deficiency syndromes (GLUT1), the phenotypic spectrum of which encompasses movement disorders, and the autosomal dominant nocturnal frontal lobe epilepsies that may be associated with psychiatric comorbidities in adolescence.
Transition for neurocutaneous disorders such as TS complex, in which epilepsy plays a prominent role in childhood and adolescence, is paramount.18 The emphasis of care shifts in adulthood from the epilepsy to renal, pulmonary, and psychiatric problems. Ideally, multidisciplinary specialist TS clinics would be useful in providing comprehensive care to such vulnerable and complex patients; however, operating and maintaining such services may not be cost-effective or even possible. It is likely that many adults with TS may not be independent in view of their learning difficulties, and often the neurologist would be the lead clinician in view of the persistence of epilepsy into adult life. It would be important for these patients to be transitioned appropriately for surveillance and treatment to the respective specialty clinics. Similarly, Sturge Weber syndrome is a condition where the emphasis shifts from epilepsy to management of migraine and follow-up for glaucoma. These individuals often remain independent and may have emotional problems in view of the cosmetic disfiguration, leading to depression and low self-esteem.
Some of the early-onset epilepsies in childhood may be due to diffuse brain abnormalities (disorders of neuronal migration), traumatic brain injury, and acquired brain injuries secondary to encephalitis; and these evolve into Lennox–Gastaut syndrome (LGS). The epilepsies in this group of patients remain refractory, and a good knowledge of the different types of seizures and pragmatic approach to their treatment is important. Similarly, epilepsies related to mitochondrial and other metabolic disorders would need particular attention when being transitioned.19 The epilepsies in mitochondrial disorders may remain refractory to treatment and may exacerbated during periods of intercurrent illnesses or stress. Avoidance of sodium valproate in selected cases is important to recognize.20 Specific conditions such as the GLUT1 deficiency and pyruvate dehydrogenase deficiency may well require continuation of the ketogenic diet. The literature on transition for GLUT1 deficient patients is limited. Many continue to have learning difficulties and remain on the ketogenic diet. It is important to be aware of long-term adverse effects of the diet, including renal calculi, osteoporosis, and impaired growth. In many adult centers, provision of ketogenic diet services by a dedicated adult epileptologist and specialist dietician is not available. Unverricht–Lundborg disease and the other progressive myoclonic epilepsies (Lafora body disease and juvenile neuronal ceroid lipofuscinosis) are neurodegenerative disorders of varying severity, in which epilepsy continues to be active and varying degrees of cognitive and physical deficits also persist. A holistic approach to managing these epilepsies and the coexistent neurodisability with the GP would be beneficial for these vulnerable young people.
Pharmacological and other treatment during transition
Antiepileptic medications remain the mainstay of treatment for epilepsy across all age groups. It is essential to consider whether the current treatment is the most effective one for the specific epilepsy syndrome or condition and whether it would be beneficial to change the medication and how to optimize this. Certain epilepsy syndromes, such as Dravet syndrome, may be treated with medications that have been licensed for use specifically in this condition, for example, stiripentol. This may not be familiar to the adult epileptologist, and it is essential to be updated regarding the pharmacological aspects of these medications and continue to prescribe them. Optimizing medications and taking a “fresh outlook” on treatment of specific epilepsies are beneficial, with consideration of medications that may be “off-label” for use in childhood. Adolescents with disability may require administration of medications through assisted feeding device, such as the percutaneous gastrostomy or jejunostomy. A detailed discussion and involvement of the pharmacy teams may be essential in order to check compatibility of respective formulation through different sites. Similarly, details of rescue medications and dosage, as well as specific care plans for administration during prolonged seizure needs to be reviewed and agreed with the family and carers – including school and respite.21
Potential interactions with contraception, balancing risk of teratogenicity with seizure control, and associated cognitive and psychiatric side effects of respective medication would need to be carefully considered. The Coordination Group for Mutual Recognition and Decentralised Procedures–Human of the European Medicines Agency (EMA) has recently strengthened warnings on the use of valproate in young women of child bearing potential, highlighting its teratogenic potential.22 The Summary of Product Characteristics now states that “valproate should not be used in women of child-bearing potential unless alternative treatments are ineffective or not tolerated”. This does not imply that this category of patients need to try and fail multiple alternative treatment before trying valproate, if valproate is indeed the most effective treatment for her epilepsy. In some cases, this choice is often not provided, given the scare around potential teratogenicity, leading to young women being deprived of making an informed choice regarding the management of their epilepsy.23 The Commission on European Affairs of the International League Against Epilepsy and the European Academy of Neurology have issued recommendations on the clinical use of valproate in young women with epilepsy in the context of these new warnings. They discuss the importance of shared decision making between the clinician and patient based on a careful risk–benefit assessment of reasonable treatment options for the patient’s epilepsy and avoidance of valproate as the first-line treatment of focal epilepsies. In cases where valproate is considered the most appropriate option, every patient must be fully informed of the risks associated with its use during pregnancy as well as of the risks and benefits of alternative treatment options. When used in women, valproate should be prescribed at the lowest effective dose, aiming for doses not >500–600 mg/day, although clinically it may be necessary to prescribe higher doses for optimal seizure control. Women on valproate should utilize effective contraceptive methods to ensure that unplanned pregnancies can be avoided.23,24
Some adolescents with drug-resistant epilepsy, particularly with LGS, may have the vagal nerve stimulator (VNS) as a part of their epilepsy management. It is essential that the settings and details about its efficacy, as well as efficacy of using the “magnet” to terminate specific seizure types is carefully recorded and discussed in the transition clinic. It is also important for the VNS battery and settings to be checked regularly, and alerts be issued about potential interference or loss of VNS efficacy in certain situations, for example, around the operating theater for routine procedures or magnetic resonance imaging. In many centers, dedicated neurosurgical or epilepsy specialist nurses manage the follow-up of patients with VNS with input from the clinical epileptologist.25
Ketogenic diet is a well-recognized treatment for refractory epilepsy and is the treatment of choice for some genetic epilepsy, for example, epilepsy secondary to GLUT1 deficiency. Although this may have been initiated and well managed in childhood, there is a serious lack of adult centers that would be able to continue to support this or initiate this as a new treatment during transition. In the John Hopkins Hospital, Baltimore, an adult epilepsy diet center was established in 2010, chiefly comprising of a specialist dietician and an adult epileptologist with a strong interest in the ketogenic diet, with frequent liaison and support from the pediatric ketogenic diet team.26 They were responsible for recruiting new patients and managing transition of patients already on the diet. It was helpful to have both these centers on the same campus in order to ensure good communication and smooth transition. It is also important to ensure that the service supports independent living, nutritional allowance for the growing and maturing teenager, and managing complications in order to ensure compliance.
Epilepsy surgery has an established role in selected cases, and adolescents should be evaluated early for their suitability for resective surgery. The discussion around weaning of medications, continuing follow-up to review recurrence of seizure, and managing the associated physical and other comorbidities after large resective surgeries (for example, hemispherotomy for Rasmussen’s encephalitis) would need careful evaluation during transition.27
Important lifestyle issues during transition
Driving is an important aspect to be discussed in the transition clinic. For the adolescent, a driver’s license may be the most important stepping stone to adulthood and a marker of independence. It may be required for employment, for leisure, and for transporting family and friends. Therefore, discussion of driving regulations is necessary during transition. In UK, these regulations are similar to the European directive and are summarized in Table 2.28 In most cases, patients need to be seizure free for a year on medication for an ordinary car-driving license. For those with only nocturnal seizures, they need to be having this pattern of seizures for at least 3 years while on medications before they can apply. This poses difficulty in some teenagers who have been seizure free for a reasonable period and who are keen to drive but are also faced with a choice of attempting withdrawal of medication to review if their epilepsy has entered remission. In these cases, one can apply for a license only 6 months after the medication has been stopped. The Driving and Vehicle Licensing Agency (DVLA) review each case closely and liaise with the teenager’s GP and neurologist before authorizing the application for licensing. Provision of license also depends on other associated comorbidities such as attention deficit hyperactivity disorder, obsessive compulsive disorder, and other physical comorbidities such as visual field restriction and learning difficulties, and may add a level of complexity in the decision making for the DVLA.
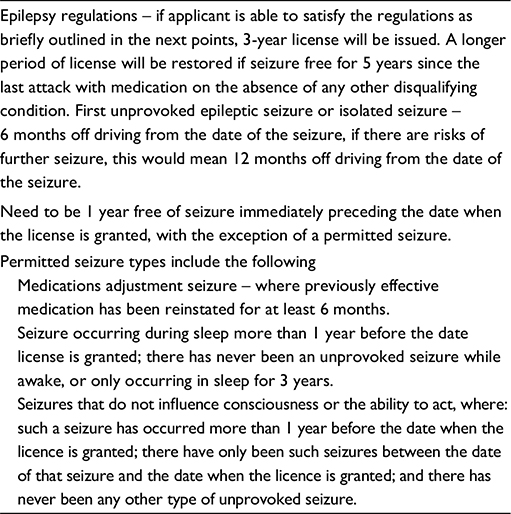 | Table 2 Current DVLA guidelines on driving and epilepsy (requirements for an ordinary licence – group 1 – car and motorcycle) Notes: Adapted from Assessing fitness to drive - a guide for medical professionals. Driver and Vehicle Licensing Agency; UK. Available from: https://www.gov.uk/government/publications/assessing-fitness-to-drive-a-guide-for-medical-professionals. Accessed May 31, 2016. © Crown copyright. Contains public sector information licensed under the Open Government Licence v3.0.37 Abbreviation: DVLA, Driver and Vehicle Licensing Agency, UK. |
Regular exercise for general health improvement is desirable in teenagers with epilepsy who may lead a more sedentary life, thus leading to higher rates of obesity than the general population. Regular walking to educational centers or for work in the absence of a driving license may actually be beneficial. Very rarely, adults with epilepsy have experienced an increase in seizure frequency with exercise. For most other exercises, a degree of common sense is required in ensuring safety. For example, swimming poses the risk of drowning and mandates supervision. The same holds true for other leisure activities such as going to the gym, horse riding, etc; supervision and providing the requisite information to member of the sport staff are crucial. For some sport activities, the person would need to fill out a specific form detailing their type of epilepsy. For extreme sports, such as snowboarding and bungee jumping, there is an element of danger, and one would need to consult their respective governing body about specific regulations. For example, the British Sub-Aqua Club who govern deep water diving mention that one would need to be free from awake seizures and off medication for 5 years before taking up this sport.28
It is important to discuss career choices and the impact of epilepsy on employment at this age. In several community-based cohort studies, it has been noted that unemployment rate in people with epilepsy is at least twice higher than that of the general population.29 This is more in those individuals with difficult to control epilepsy and with frequent generalized tonic–clonic seizures. Moreover, having seizures can have an impact on work performance, thereby leading to problems with career advancement and lost potential. Although previously felt to be a stigma, with improved awareness, this no longer exists, and most people with epilepsy do not experience any specific form of discrimination. Employers may have their own views about epilepsy, more out the concern about dangers faced when individuals with epilepsy are required to perform jobs that are risk, for example, working with machinery. Nevertheless, it is important to disclose epilepsy, as a disability when applying for specific jobs, otherwise this would constitute a breach of trust. There is a need for a specific careers advisor who can discuss different options with the adolescent before embarking on a specific career education. In many cases, once adolescents leave college to work, it may be necessary for a vocational rehabilitation program to support these individuals to find and sustain a suitable employment.
Adolescents on antiepileptic medications face unique challenges, regarding contraception. Combined oral contraceptive (COC) pills and antiepileptic medications can interact bidirectionally and lead to failure of either treatment, in turn leading to unintended pregnancy or worsening seizures. Contraceptive failure and resultant pregnancy are disastrous, particularly due to the teratogenic potential of some medications. Treating adolescent females of child-bearing potential needs careful thought about the choice of antiepileptic medication, ongoing, and accurate counseling, regarding the optimal contraceptive choice and early detection of pregnancy to consider alteration in medications. Long-term enzyme inducing antiepileptic medications (carbamazepine, oxcarbazepine, and phenytoin) may reduce the effectiveness of some combined hormonal oral contraceptive pills (or patch), progesterone only pills (morning-after pill), and progesterone-only implants; and an alternative contraceptive method is recommended.30–32 If the intended choice of contraception is the COC pills, then it is recommended to use two pills containing at least 50 μg of ethinylestradiol and the consistent use of barrier contraceptives at all times. It is advisable to consider a method unaffected by enzyme inducing medications, such as the progesterone-only injection or intrauterine implant. If an emergency contraception is needed, then a copper intrauterine device is recommended or alternatively a single dose of 3 mg of levonorgestrel is recommended. Lamotrigine clearance is increased while taking the COC pills leading to the possibility of loss of seizure control; hence, it is essential to consider increasing the dose of lamotrigine. Alternatively progesterone-only contraception would need to be considered in young women on lamotrigine treatment.
Sudden unexpected death in epilepsy (SUDEP) is extremely rare with population-based epidemiological studies reporting an annual incidence of 1.16 cases per 1,000 patients with epilepsy.33 The risk is increased to 5.9 per 1,000 person years in patients with chronic drug-resistant epilepsy. It remains controversial whether all patients should be routinely informed about SUDEP; however, NICE and the American Epilepsy Society (AES) recommend providing information about SUDEP as a part of a comprehensive epilepsy education and good clinical practice. In a recent survey on SUDEP knowledge and practices, most patients (85%) wished to be informed about SUDEP.33,34 Interestingly, majority of the parents chose to withhold this information from their children, their main reason being to protect their child from distress. Nevertheless, the discussion of SUDEP should be decided on individual patient basis, particularly in those who are at risk of mortality with drug-resistant epilepsy and those who are noncompliant with treatment.
Families and adolescents’ views on transition
In a survey of parental expectations of adolescents with LGS, some expressed their concerns that not only would they feel uncomfortable leaving pediatric care but also had reservations about the knowledge of the adult practitioners in these complex childhood disorders.25 There is no particular recommended time to initiate these discussions; however, several centers have reported better satisfaction when there has been adequate preparation prior to the actual transition. Discussing the model of the transition clinic, staff present, follow-up, and contact details and providing a formal leaflet allows the family to do their research on the much awaited transition clinic appointment and allows them to prepare for this and ask relevant questions during the clinic.
There have been very few studies reviewing the satisfaction of the families following transition to the adult care. One study has used a questionnaire to ascertain the perception of transition in patients with Dravet syndrome.15 Factors that were thought to have positively impacted a smooth transition were the quality of transition preparation, longer duration of follow-up and availability of the pediatric neurologist, transfer into the adult health care system after the age of 18 years, and a stable medical condition before transfer.
Training in adolescent health
In the US, Canada, Australia, and New Zealand, a specialty of adolescent medicine exists, and specific training is offered to health care professionals. In UK however, there is only one department of adolescent medicine in London, and at present, no formal postgraduate training exists. In June 2003, the Royal College of Paediatrics and Child Health (RCPCH) published a document The Intercollegiate Working Party on Adolescent Health: bridging the gaps in health care for adolescents. This acknowledged that young people between the ages of 10 years and 20 years account for 13%–15% of the UK population and recommended that training in adolescent health should be mandatory for all undergraduate and postgraduates who will be involved in the care of young people. All those working in the field of adolescent medicine should be encouraged to obtain a relevant qualification and it is recommended that the European wide training program for trainers in adolescent health (European training in effective adolescent care and health or EuTEACH)35 be adapted for UK training.36
There is a lack of exposure of adult neurology trainees to complex pediatric epilepsies. In addition, there is a lack of awareness of common genetic conditions of which epilepsy and learning difficulties are important comorbidities, Angelman syndrome is one such example. Most would consider a sabbatical of clinic observation for 2 weeks, as adequate exposure to learn about common pediatric epilepsies. Attending dedicated transition clinics and courses about pediatric epilepsies is another way of obtaining further knowledge on relevant transition issues. A survey involving adult neurologists was carried out to check how comfortable they felt in diagnosing and treating epilepsies during transition.13 Most felt confident in treating idiopathic (genetic) generalized epilepsies and adolescents with mesial temporal sclerosis or temporal lobe epilepsies. However, nearly half were not as confident in treating other rare genetic disorders (Dravet syndrome) or epilepsies with comorbid disorders such as autistic spectrum disorder. In many such cases, they acknowledged the benefit from the knowledge and support of the pediatric neurologists. It would be useful to have a systematic approach on reviewing a young person in the transition clinic, and a checklist of essential information to be considered during the initial consultation in the transition clinic is summarized in Table 3.
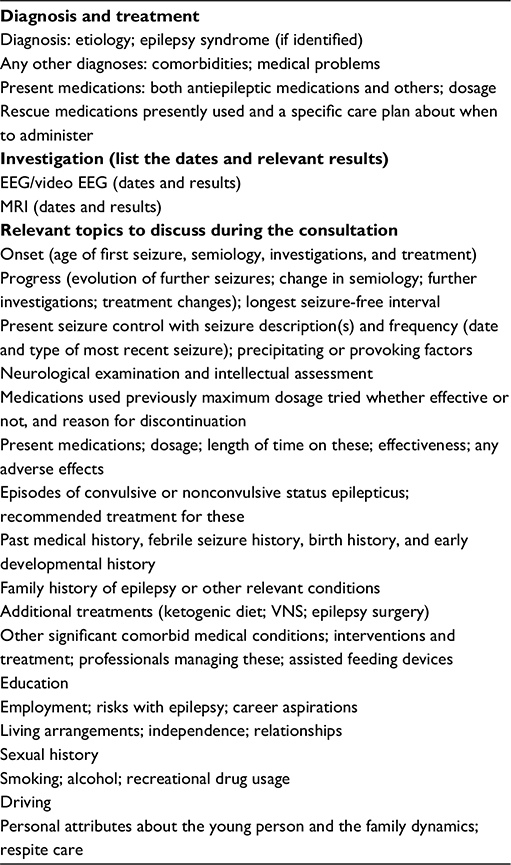 | Table 3 A checklist of relevant issues during transition consultation Abbreviations: EEG, electroencephalography; MRI, magnetic resonance imaging; VNS, vagal nerve stimulator. |
Conclusion
Transition is a major milestone for a young person and his/her family with epilepsy. An effective transition is not just a “handover”, but a planned process of jointly reviewing these complex patients by the pediatric and the adult team, with the view to promoting them to the adult epilepsy clinic at the right time. There are many factors that may jeopardize the continuation of those transition clinics that have been well established, which include personalities and conflicts between staff, financial support, and quality of service. It is paramount that this dedicated transitional care for young people with epilepsy continues and possibly be integrated into clinical services across other areas. Despite the challenges involved in transition, the pediatrician experiences professional satisfaction from helping the young person adapting well to adult life with his/her epilepsy, and from supporting his/her carers through this difficult personal milestone.
Disclosure
The authors report no conflicts of interest in this work.
References
Cowan LD. The epidemiology of the epilepsies in children. Ment Retard Dev Disabil Res Rev. 2002;8(3):171–181. | ||
Davies S, Heyman I, Goodman R. A population survey of mental health problems in children with epilepsy. Dev Med Child Neurol. 2003;45(5):292–295. | ||
Camfield P, Camfield C, Pohlmann-Eden B. Transition from pediatric to adult epilepsy care: a difficult process marked by medical and social crisis. Epilepsy Curr. 2012;12(Suppl 3):13–21. | ||
Cheung C, Wirrell E. Adolescents’ perception of epilepsy compared with other chronic diseases: “through a teenager’s eyes”. J Child Neurol. 2006;21(3):214–222. | ||
Camfield P, Camfield C. Help youth with epilepsy to become competent and happy adults: transition care. Seizure. 2013;22(6):414–415. | ||
Payne D, Martin C, Viner R, Skinner R. Adolescent medicine in paediatric practice. Arch Dis Child. 2005;90(11):1133–1137. | ||
Transition: getting it right for young people. Department of Health [UK]. Available from: http://webarchive.nationalarchives.gov.uk/20130107105354/http:/www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4132149.pdf. Accessed November 16, 2015. | ||
Transition: moving on well. Department of Health [UK]. Available from: http://www.bacdis.org.uk/policy/documents/transition_moving-on-well.pdf. Accessed November 16, 2015. | ||
Nagra A, McGinnity PM, Davis N, Salmon AP. Implementing transition: ready steady go. Arch Dis Child Educ Pract Ed. 2015;100(6):313–320. | ||
Appleton RE. Transition from paediatric clinic to the adult service. J R Soc Med. 2001;94(10):554. | ||
Iyer A, Appleton R. Transitional services for adolescents with epilepsy in the UK: a survey. Seizure. 2013;22(6):433–437. | ||
Carrizosa J, An I, Appleton R, Camfield P, Moers Von A. Models for transition clinics. Epilepsia. 2014;55(Suppl 3):46–51. | ||
Borlot F, Tellez-Zenteno JF, Allen A, Ali A, Snead OC 3rd, Andrade DM. Epilepsy transition: challenges of caring for adults with childhood-onset seizures. Epilepsia. 2014;55(10):1659–1666. | ||
Jurasek L, Ray L, Quigley D. Development and implementation of an adolescent epilepsy transition clinic. J Neurosci Nurs. 2010;42(4):181–189. | ||
Kuchenbuch M, Chemaly N, Chiron C, Dulac O, Nabbout R. Transition and transfer from pediatric to adult health care in epilepsy: a families’ survey on Dravet syndrome. Epilepsy Behav. 2013;29(1):161–165. | ||
Camfield CS, Berg A, Stephani U, Wirrell EC. Transition issues for benign epilepsy with centrotemporal spikes, nonlesional focal epilepsy in otherwise normal children, childhood absence epilepsy, and juvenile myoclonic epilepsy. Epilepsia. 2014;55(Suppl 3):16–20. | ||
Scheffer IE, Dravet C. Transition to adult life in the monogenic epilepsies. Epilepsia. 2014;55(Suppl 3):12–15. | ||
Thiele EA, Granata T, Matricardi S, Chugani HT. Transition into adulthood: tuberous sclerosis complex, Sturge-Weber syndrome, and Rasmussen encephalitis. Epilepsia. 2014;55(Suppl 3):29–33. | ||
Camfield PR, Bahi-Buisson N, Trinka E. Transition issues for children with diffuse cortical malformations, multifocal postnatal lesions, (infectious and traumatic) and Lennox-Gastaut and similar syndromes. Epilepsia. 2014;55(Suppl 3):24–28. | ||
Kossoff EH, Veggiotti P, Genton P, Desguerre I. Transition for patients with epilepsy due to metabolic and mitochondrial disorders. Epilepsia. 2014;55(Suppl 3):37–40. | ||
Chiron C, An I. Pharmacology aspects during transition and at transfer in patients with epilepsy. Epilepsia. 2014;55(Suppl 3):8–11. | ||
Tomson T, Marson A, Boon P, et al. Valproate in the treatment of epilepsy in girls and women of childbearing potential. Epilepsia. 2015;56(7):1006–1019. | ||
Mole TB, Appleton R, Marson A. Withholding the choice of sodium valproate to young women with generalised epilepsy: are we causing more harm than good? Seizure. 2015;24:127–130. | ||
Elger CE. Is valproate contraindicated in young women with epilepsy? No. Epileptology. 2013;1(1):43–45. | ||
Camfield PR, Gibson PA, Douglass LM. Strategies for transitioning to adult care for youth with Lennox-Gastaut syndrome and related disorders. Epilepsia. 2011;52(Suppl 5):21–27. | ||
Kossoff EH, Henry BJ, Cervenka MC. Transitioning pediatric patients receiving ketogenic diets for epilepsy into adulthood. Seizure. 2013;22(6):487–489. | ||
Cross JH, Duchowny M. Transition in lesional focal epilepsy, and following epilepsy surgery. Epilepsia. 2014;55(Suppl 3):34–36. | ||
Nashef L, Capovilla G, Camfield C, Camfield P, Nabbout R. Transition: driving and exercise. Epilepsia. 2014;55(Suppl 3):41–45. | ||
Smeets VMJ, van Lierop BAG, Vanhoutvin JPG, Aldenkamp AP, Nijhuis FJN. Epilepsy and employment: literature review. Epilepsy Behav. 2007;10(3):354–362. | ||
Mody SK, Haunschild C, Farala JP, Honerkamp-Smith G, Hur V, Kansal L. An educational intervention on drug interactions and contraceptive options for epilepsy patients: a pilot randomized controlled trial. Contraception. 2016;93(1):77–80. | ||
Reimers A, Brodtkorb E, Sabers A. Interactions between hormonal contraception and antiepileptic drugs: clinical and mechanistic considerations. Seizure. 2015;28:66–70. | ||
Herzog AG. Differential impact of antiepileptic drugs on the effects of contraceptive methods on seizures: interim findings of the epilepsy birth control registry. Seizure. 2015;28:71–75. | ||
Shankar R, Cox D, Jalihal V, Brown S, Hanna J, McLean B. Sudden unexpected death in epilepsy (SUDEP): development of a safety checklist. Seizure. 2013;22(10):812–817. | ||
Xu Z, Ayyappan S, Seneviratne U. Sudden unexpected death in epilepsy (SUDEP): what do patients think? Epilepsy Behav. 2015;42:29–34. | ||
EuTEACH - European training in effective adolescent care and health [homepage]. Available at: https://www.unil.ch/euteach/en/home.html. Accessed May 31, 2016. | ||
Adolescent Health Programme: Curriculum. Royal College of Paediatrics and Child Health. Available from: http://www.rcpch.ac.uk/ahp. Accessed May 31, 2016. | ||
Assessing fitness to drive - a guide for medical professionals. Driver and Vehicle Licensing Agency; UK. Available from: https://www.gov.uk/government/publications/assessing-fitness-to-drive-a-guide-for-medical-professionals. Accessed May 31, 2016. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.