Back to Journals » Infection and Drug Resistance » Volume 15
Epidemiology of Multidrug Resistant Non-Fermentative Gram Negative Bacilli in Patients with Hospital Acquired Pneumonia: An Alarming Report from Somalia
Authors Adan FN ![]() , Jeele MOO
, Jeele MOO ![]() , Omar NMS
, Omar NMS
Received 24 August 2022
Accepted for publication 27 October 2022
Published 31 October 2022 Volume 2022:15 Pages 6297—6305
DOI https://doi.org/10.2147/IDR.S387370
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Faduma Nur Adan,1,* Mohamed Osman Omar Jeele,2,* Nasteho Mohamed Sheikh Omar3
1Department of Infectious Diseases, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia; 2Department of Internal Medicine, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia; 3Department of Emergency medicine, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia
*These authors contributed equally to this work
Correspondence: Mohamed Osman Omar Jeele, Department of Internal Medicine, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia, Tel +252615775226, Email [email protected]
Introduction: There is a lack of data concerning hospital-acquired pneumonia (HAP) due to multidrug resistant non-fermentative gram-negative bacilli (MDR-NFGNB) in Somalia, and this study will aim to analyze the epidemiology of MDR-NFGNB among HAP patients in tertiary care hospital in Somalia.
Materials and Methods: This is a retrospective study which evaluated the presence of MDR-NFGNB among 2003 HAP patients between June 2017 and May 2022 in a tertiary care hospital in Somalia. NFGNB were cultured on blood agar and eosin methylene blue agar and were then used BBL crystal system and oxidase biochemical assays for identification. Antimicrobial sensitivity and resistance were assessed using Mueller–Hinton agar.
Results: A total of 160 confirmed cases of HAP due to NFGNB were examined. Among these, 114 (71%) were males compared to females (n = 46, 29%). The mean age was 49.49 ± 21.48. The overall prevalence rate of NFGNB among patients with HAP was 8%. It was more common in older patients and in patients with co-morbidities. Acinetobacter baumannii was the most common NFGNB with n = 93 (58%), followed by Pseudomonas aeruginosa (n = 55, 34%), and Stenotrophomonas maltophilia (n = 12, 8%). Regarding the antimicrobial sensitivity rate, Acinetobacter baumannii showed an overall resistance level of 82%, Stenotrophomonas maltophilia (81%), and Pseudomonas aeruginosa (62%). The rate of CR-NFGNB in our study was 79.4%. We found that 68.1% of NFGNB was multidrug resistant (MDR) pathogens. MDR patterns were more common in Acinetobacter baumannii infections (84%). MDR pathogens were strongly associated with ICU admissions (95% CI, 0.202– 0.800, OR, 0.402, p value < 0.009). Finally, the mortality rate of HAP caused by NFGNB in our study was 42.5%.
Conclusion: The prevalence of NFGNB in HAP patients was 8%. These infections were more prevalent among men and the elderly. Acinetobacter baumannii and Stenotrophomonas maltophilia exhibited the highest antibiotic resistance rate. The MDR level of these pathogens was 68.1%.
Keywords: hospital acquired pneumonia, non-fermentative gram negative bacilli, carbapenem resistant non-fermentative gram negative bacilli, multidrug resistance, Somalia
Introduction
The broad definition of hospital-acquired pneumonia (HAP) constitutes an episode of pneumonia that occurs 48 hours or more after hospitalization.1 Patients who are admitted to intensive care units (ICU), especially those who are receiving mechanical ventilation, have an increasing chance of developing a major subset of HAP defined as ventilator-associated pneumonia (VAP).2 HAP is thought to be the most common cause of hospital-acquired infections in Europe and the US, occurring at a rate of 5 to 10 per 1000 hospital admissions and thus increasing the morbidity and mortality rates among hospitalized patients.3 HAP is associated with a nearly 20% mortality rate in ICU patients.4
Despite being regarded as contaminants, non-fermenting gram-negative bacilli (NFGNB) have a well-established pathogenic potential and are one of the major causes of hospital acquired pneumonia.5 Due to the increased antibiotic resistance, this particular bacterial group has become opportunistic pathogens, particularly in immunocompromised hosts, and their treatment is quite challenging.6
There are four major bacteria belonging to this group: Acinetobacter baumannii, Pseudomonas aeruginosa, Stenotrophomonas maltophilia, and Burkholderia cepacia.7 NFGNB infections were previously treated with carbapenems as a last option drug, but recently Carbapenem resistant NFGNB (CR-NFGNB) were reported from various parts of the world.8 Due to their remarkable adaptability and diverse innate and acquired resistance mechanisms, these bacteria are often resistant to key classes of antimicrobial drugs, leaving limited therapy choices.7 Hence, these pathogens constitute a grave threat to global public health since they raise patients morbidity and mortality, as well as hospital stay and expense.
In Somalia, there is an unregulated antibiotic prescribing system, and numerous antibiotics are available on the market to be purchased by anybody without prescription. This, along with the country’s poorly equipped health system, lack of bacterial identification techniques, and lack of patient awareness of antimicrobial resistance, is thought to have contributed to an increase in antibiotic resistance. However, there is a dearth of data concerning HAP caused by multidrug resistant NFGNB, including its prevalence and mortality rates in Somalia. The rate of CR-NFGNB in Somalia is also yet to be determined. Our study aimed to analyze the epidemiology of multidrug resistant non-fermentative gram-negative bacilli among hospital acquired pneumonia patients in tertiary care hospital in Somalia.
Methods and Materials
This is a retrospective, descriptive study which evaluated the presence of multidrug resistant NFGNB among patients with hospital acquired pneumonia. The study was conducted between June 2017 and May 2022 in Mogadishu Somali Turkish Training and Research Hospital. The hospital is the largest tertiary care hospital in Somalia.9 The ethical approval was obtained from the ethical committee board of the Mogadishu Somali Turkish Training and Research Hospital (Approval No, MSTH-7070). The privacy of the patients’ personal information was maintained throughout the study as per the Helsinki Declarations. Codes were used in place of names and ID numbers, to safeguard the patients’ privacy. The ethics committee waived the necessity for informed consent since this study was retrospective in nature.
We enrolled 2003 patients who had been diagnosed with HAP and who had undergone bacterial identification and antibiotic sensitivity testing within the preceding five years. Examined were a total of 160 patients with confirmed HAP due to NFGNB. The socio-demographic data which included the patients age and gender were examined. According to their ages, the patients were divided into four categories, <18 years, 19–40 years, 41–60 years, and >60 years. In addition, co-morbidities such as diabetes, hypertension, chronic kidney disease, heart disease, asthma, and chronic obstructive pulmonary disease (COPD) were assessed. The microbiology culture results and antimicrobial sensitivity results were also assessed. The admission site (intensive care unit, inpatient department), duration of hospital stay (days), and the outcome were also examined. The aforementioned variables were extracted from the hospital information system (HIS) using dates and ICD-10 codes.
Regarding the sample collection, it was categorized into sputum and endotracheal aspiration. After collection, the samples were immediately sent to the microbiology unit within 30 minutes using sterile sample container. The samples were then cultured on blood agar and Eosin methylene blue agar (EMB). Gram staining was performed on all specimens, and they were read at x100 magnification with oil immersion. The samples were then incubated aerobically for 24–72 hours at 37°C room temperature. The samples that showed growth were then put through the BBL crystal system (Becton Dickinson Microbiology Systems, Cockeysville, panel viewer, USA) and an oxidase biochemical tests for bacterial identification.
Antimicrobial sensitivity tests were performed following CLSI guidelines by using the Kirby Bauer disk diffusion method.10 The organisms were tested on Mueller–Hinton agar against Amoxicillin/clavulanic acid (20/10 mcg), Piperacillin (100mcg), Piperacillin/tazobactam (100/10 mcg), Cefoperazone/sulbactam (75/10 mcg), Cefuroxime (30 mcg), Ceftriaxone (30 mcg), Ceftazidime (30 mcg), Cefepime (30 mcg), Trimethoprim/sulfamethoxazole (1.25/23.75 mcg), Ciprofloxacin (5 mcg), Levofloxacin (5 mcg), Amikacin (30 mcg), Meropenem (10 mcg), Imipenem (10 mcg), Colistin (10 mcg), Tigecycline (15 mcg).
The Statistical Package for the Social Sciences (SPSS) (IBM Corporation, Armonk, NY, USA version 26) was used to conduct statistical analyses. Means, standard deviations, and medians were used to display descriptive data. The proportions were presented utilizing frequency and percentage tables. Chi-square and Fisher’s tests were used to compare the categorical variables. The associations between variables were evaluated using bivariate correlation. A p-value less than 0.05 was regarded as statistically significant. The odds ratio and confidence intervals were calculated using binary logistic regression.
Results
Of the total of 2003 patients that were enrolled in this study, 160 cases of confirmed HAP due to NFGNB were identified and examined. The prevalence rate of NFGNB among patients with HAP was 8%. The mean age of our patients was 49.49 ± 21.48. The maximum age was 94 years old, while the minimum age was 11 months old. Regarding the age group, NFGNB were more common in patients aged more than 60 years (n = 52, 32.5%) followed by 19–40 years old (n = 51, 31.9%), 41–60 years old (n = 49, 30.6%), and <18 years old (n = 8, 5%), respectively. A male predominance was noted among our patients with n = 114 (71%) compared to females (n = 46, 29%). More than two-third of the patients with NFGNB infection were males (Table 1).
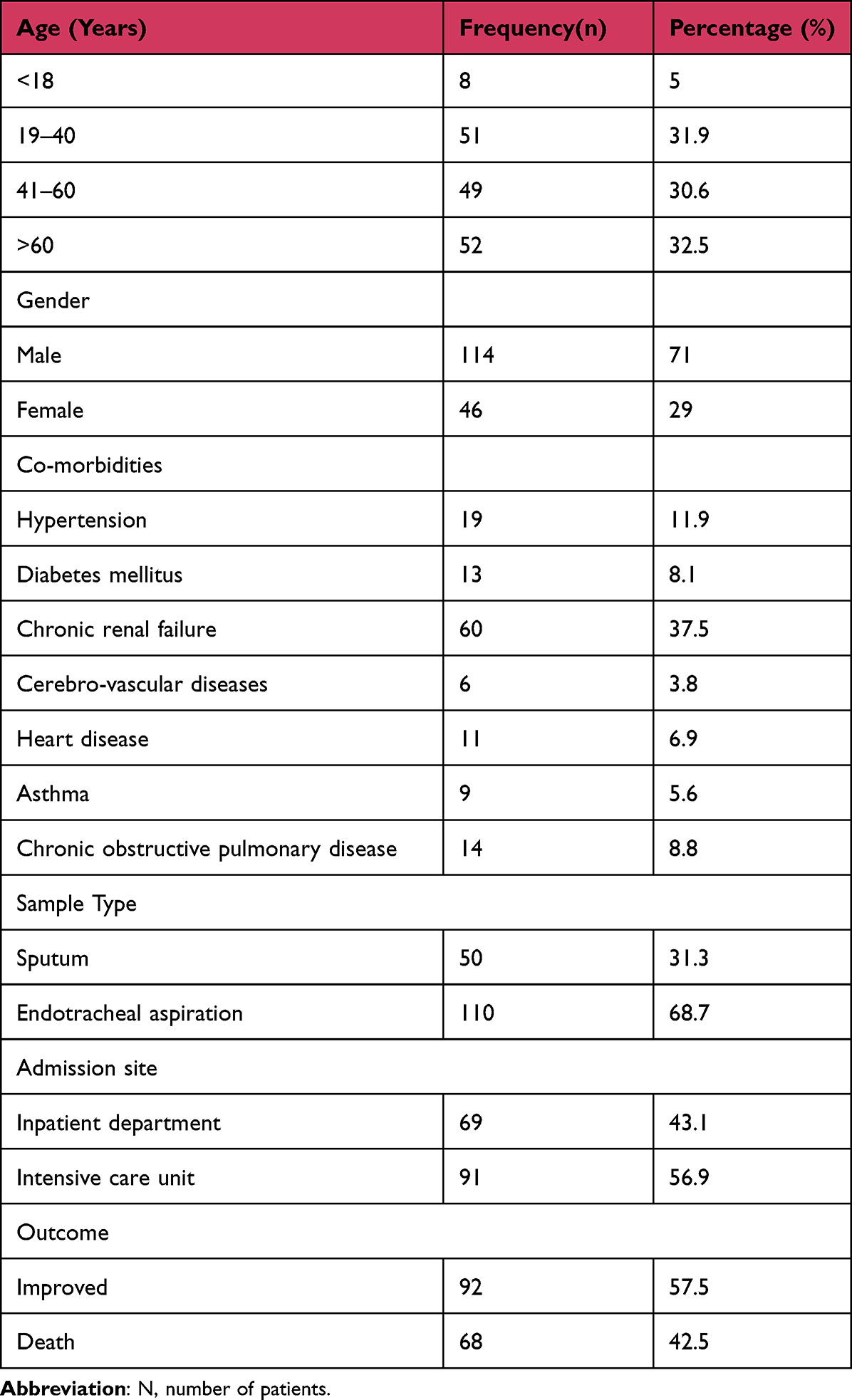 |
Table 1 Demographic and Clinical Characteristic of the Patients |
The co-morbidities of the patients were assessed; the most common co-morbidity was chronic renal disease (n = 60, 37.5%), followed by hypertension (n = 19, 11.9%) and COPD (n = 14, 8.8%). The least common of co-morbidities in our patients was cerebrovascular diseases (n = 6, 3.8%).
Acinetobacter baumannii was the most common NFGNB causing hospital-acquired pneumonia in our study with n = 93 (58%), followed by Pseudomonas aeruginosa with n = 55 (34%), and Stenotrophomonas maltophilia with n = 12 (8%). NFGNB were mostly isolated from endotracheal aspirations; Acinetobacter baumannii (77.4%), Pseudomonas aeruginosa (56%), Stenotrophomonas maltophilia (58%) (Table 2). Acinetobacter baumannii was more common in patients admitted to ICU (67%), while (56%) of Pseudomonas aeruginosa and (64%) of Stenotrophomonas maltophilia were isolated from the inpatient department. Patients with co-morbidities have shown higher rates of NFGNB infection compared to patients without any known co-morbidities.
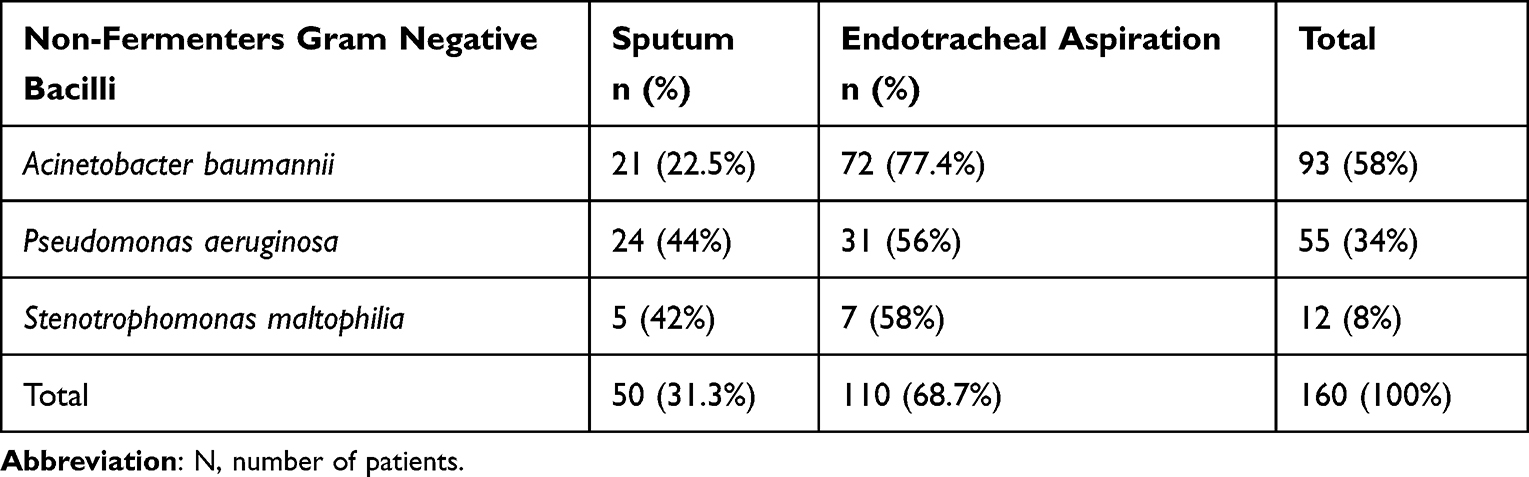 |
Table 2 Frequency of Non-Fermentative Gram Negative Bacilli Among Hospital Acquired Pneumonia |
In this study, we evaluated the antimicrobial sensitivity rate of 16 different antibiotics towards NFGNB. Acinetobacter baumannii showed an overall resistance level of 82% to all antibiotics tested against while Stenotrophomonas maltophilia and Pseudomonas aeruginosa showed a resistance rate of 81%, 62%, respectively. Acinetobacter baumannii and Pseudomonas aeruginosa exhibited a 100% resistance rate to five different antibiotics. Acinetobacter baumannii was 100% resistant to Co-trimoxazole, 96% resistant to penicillin-derived antibiotics, 97% resistant to cephalosporins, and 96% resistant to fluoroquinolones. Pseudomonas aeruginosa, on the other hand, was 100% resistant to Co-trimoxazole, 72% resistant to penicillin-derived antibiotics, 66% resistant to cephalosporins, and fluoroquinolones (53%). Stenotrophomonas maltophilia was 9% resistant to Co-trimoxazole, 97% resistant to penicillin-derived antibiotics, 98% resistant to cephalosporins, and fluoroquinolones (18%). Stenotrophomonas maltophilia also showed a higher resistance rate to individual antibiotics, including 100% resistance rate to Amoxicillin/clavulanic acid, Piperacillin, Ceftriaxone, Cefuroxime, cefepime, and ceftazidime and 92% resistant rate to imipenem and meropenem. Furthermore, it showed a 91% resistance rate to Colistin, Tigecycline, Cefoperazone/sulbactam, and Piperacillin/tazobactam. We also found that Amoxicillin/clavulanic acid, Piperacillin, Ceftriaxone, and Cefuroxime showed the highest resistance rates in all NFGNB (90–100%). Furthermore, Tigecycline is facing a growing resistance rate among individual NFGNB (65%) and this could increase the morbidity and mortality of patients with NFGNB infections. Colistin and Amikacin were shown to have the greatest overall sensitivity rates in all NFGNB infections (68%) and (50.4%), respectively (Table 3).
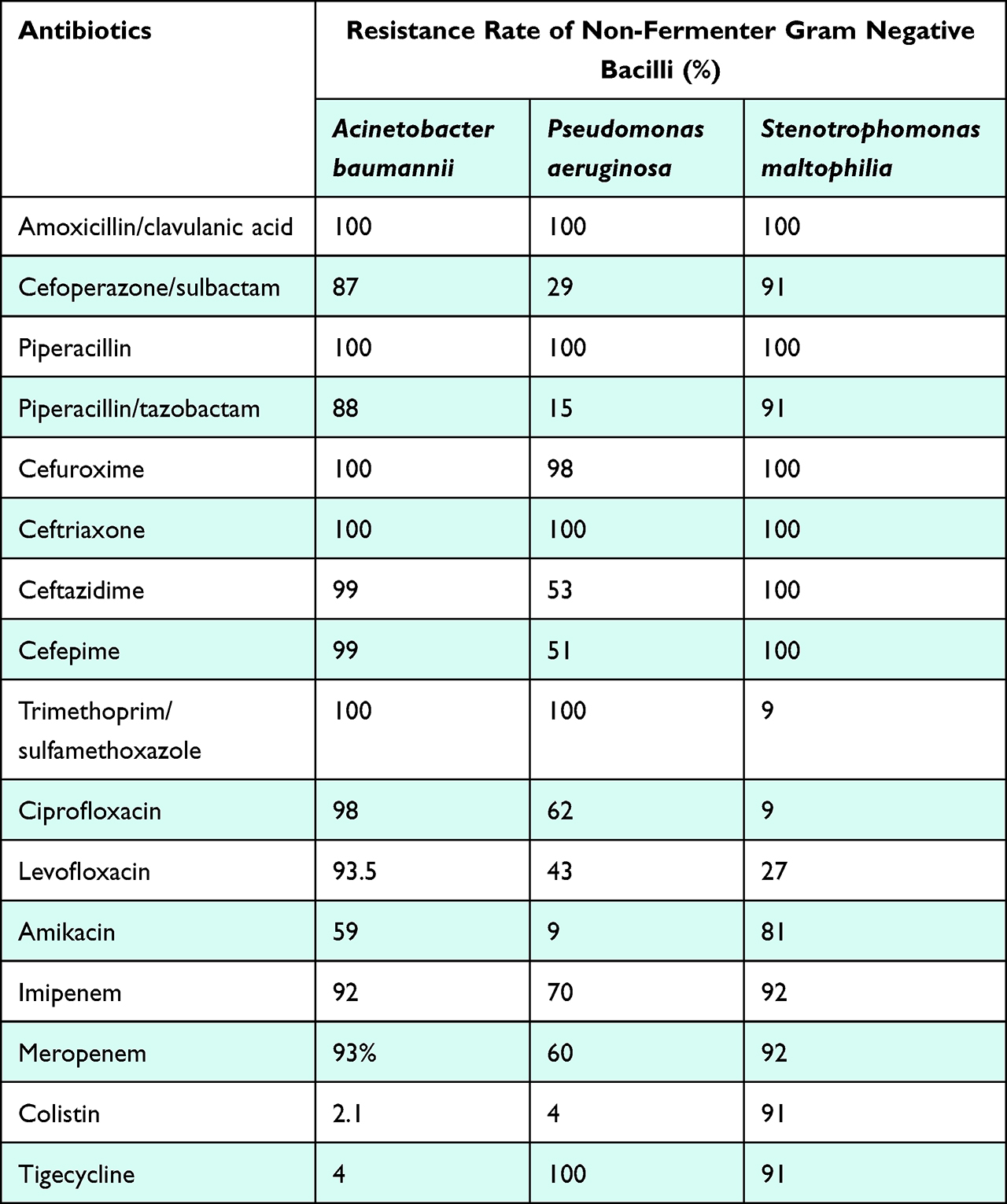 |
Table 3 Antimicrobial Resistance Rate Among Non-Fermentative Gram Negative Bacilli |
We also analyzed the rate of CR-NFGNB in our patients. The rate of CR-NFGNB in our patients was 79.4%. Acinetobacter baumannii had an overall resistance rate of 93% against carbapenem drugs. It had 94% resistant rate to meropenem and 92.4% to imipenem. Pseudomonas aeruginosa was 60% resistant to meropenem and 71% resistant to imipenem. Stenotrophomonas maltophilia was observed to have overall 92% resistance rate against carbapenem drugs specially meropenem and imipenem (Table 4).
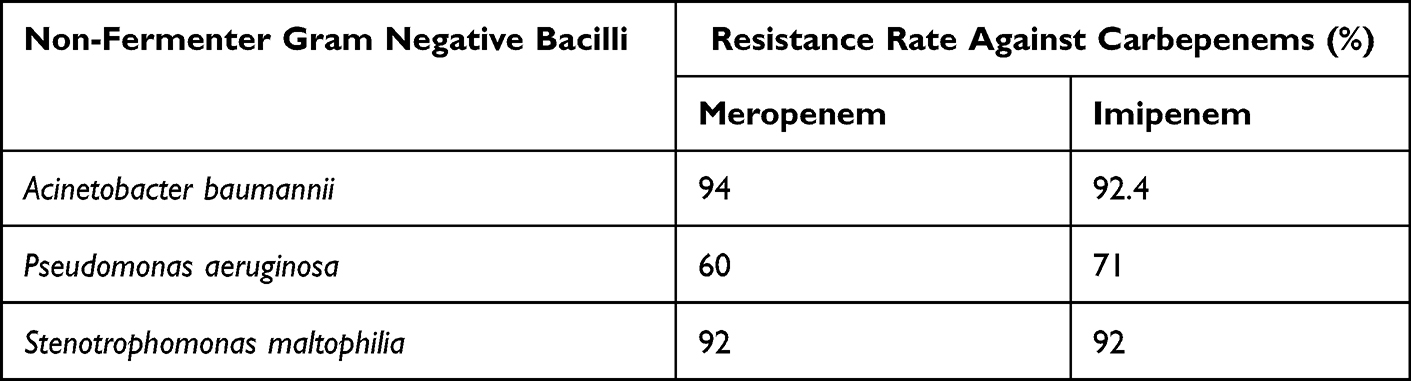 |
Table 4 The Rate of Carbapenem-Resistant Non-Fermentative Gram Negative Bacilli Among Hospital Acquired Pneumonia Patients |
Regarding the distribution of multidrug resistance (MDR), ie, organisms exhibiting resistance to at least three or more antibiotic classes, NFGNB among HAP, the prevalence of MDR showing NFGNB in our study was 68.1%. The MDR patterns were more common in Acinetobacter baumannii related cases (84%). Stenotrophomonas maltophilia and Pseudomonas aeruginosa had MDR patterns of 83% and 38%, respectively. The prevalence of MDR pathogens was strongly associated with ICU admissions (95% CI, 0.202–0.800, OR, 0.402, p value <0.009). MDR exhibiting NFGNB was also found to be more common in males (69%) and patients who have co-morbidities (77%), but these numbers were not enough to represent statistically significant associations between gender and MDR (95% CI, 0.634–3.168, OR, 1.418, p value <0.395) and between comorbidities and MDR (95% CI, 0.601–3.089, OR, 1.363, p value <0.458) (Table 5).
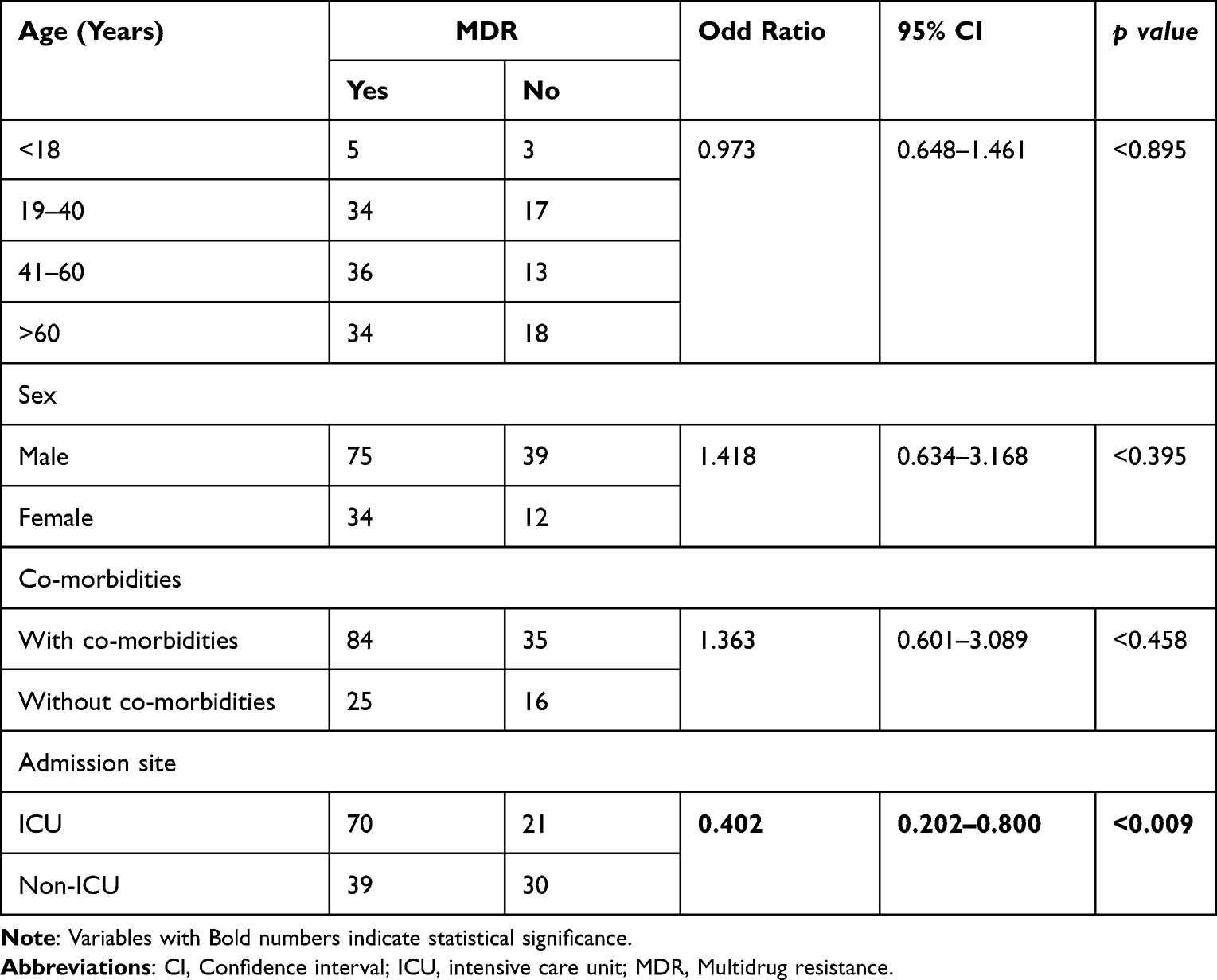 |
Table 5 Relationship Between Multidrug Resistance Pattern and Patient-Related Factors |
The mean duration of the hospital stay in our study was 19.54 ± 16.99. Regarding the outcome of the patients, 57.5% improved and were discharged in good condition. The mortality rate in our study was 42.5%. Death was more common in males, patients over the age of 65, those with MDR, those admitted to ICU, and those with co-morbidities (Figure 1). Death was strongly associated with ICU admissions (95% CI, 24.70–579.55, OR, 119.64, p value <0.0005). Patients admitted to the ICU were 119 times more likely to die than patients in inpatient units.
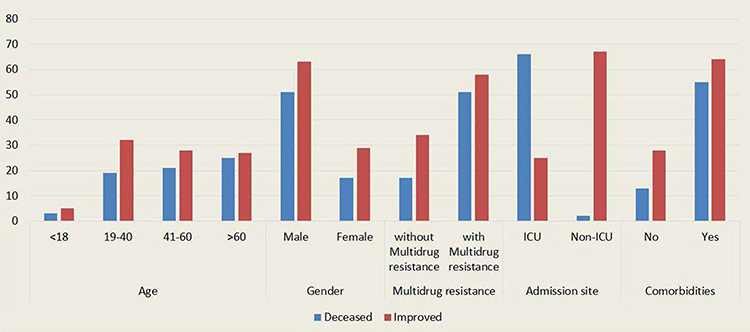 |
Figure 1 Mortality rate and its distribution to patient factors. |
Discussion
Non-fermentative Gram-negative bacteria (NFGNB) are a heterogeneous group of Proteobacteria that are incapable of fermenting sugars to produce energy for their essential cellular functions.11 NFGNB constitutes nearly 15% of all gram negative bacterial infections and can cause severe nosocomial infections in immunocompromised patients, such as the elderly, intensive care patients, and patients with co-morbidities.12,13 The increasing resistance of these bacterial group to multiple antibiotic classes, which ultimately leads to MDR strains, poses a therapeutic challenge for many healthcare systems around the globe.14 The rate of HAP caused by NFGNB, the level of antimicrobial resistance of individual bacteria of NFGNB, the rate of MDR pathogens among NFGNB, and the rate of CR-NFGNB in Somalia have yet to be determined despite the growing threat of highly infectious and incurable diseases due to NFGNB. Our study is therefore the first to describe the epidemiology of multidrug-resistant NFGNB in HAP in Somalia.
In the presenting study, we studied 160 patients with confirmed HAP caused by NFGNB in a 5-year period. The overall prevalence of NFGNB among HAP patients in our study was 8%. We demonstrated a male predominance in NFGNB infections in our study with 71%, while females constitute (28.8%). The prevalence of NFGNB was more common in patients older than 65 years (32.5%), patients with co-morbidities (74.4%), and patients admitted to ICU (56.9%). We noted that the risk of infection with NFGNB increases with age. In 2013, a study from India by Chawla et al found a prevalence of NFGNB in respiratory samples at (16.4%).15 Another study in 2014 by Sharma et al on nosocomial infections due to NFGNB revealed (25.6%) of occurrence.5 Furthermore, another study from 2010 by Sidhu et al about prevalence of NFGNB infection in seriously ill patients. They noted a (45.9%) of NFGNB infection among these patients.16 Regarding to this finding, Somalia has less prevalence rate of NFGNB in respiratory specimens. Gajdács et al worked on the resistance level and epidemiology of NFGNB in patients with urinary tract infection in 2019. They reported a NFGNB rate of 6.43%.14
The most common NFGNB organism in HAP patients in our study was Acinetobacter baumannii in 58% of cases, followed by Pseudomonas aeruginosa in 34%, and Stenotrophomonas maltophilia with 7%. We did not find any other type of less frequent NFGNB in HAP patients in our study. Acinetobacter baumannii was the most frequently identified pathogen from endotracheal tube samples (77.4%), ICU patients (67%) and patients over the age of 60 (58.5%). In consistency to our study, a recent study involving 6216 clinical specimens from Nepal by Yadav et al demonstrated Acinetobacter baumannii as the most common pathogen isolated in 44% followed by Pseudomonas aeruginosa in 40%.12 Our study is also in agreement with findings of the study by Gul et al which reported that Acinetobacter baumannii was the most predominant NFGNB despite being equal to the isolated numbers of Burkholderia cepacia complex.17 We did not find any HAP cases related to Burkholderia cepacia in our study. In contrary to our finding, a study in 2010 by Rahbar et al demonstrated Pseudomonas aeruginosa (42%) as the most common isolated NFGNB followed by Acinetobacter baumannii in 32%.18 This could indicate that Acinetobacter baumannii infections increased over the past decade and may now account for the majority of NFGNB infections.
This study demonstrated a higher antimicrobial resistance rate of Acinetobacter baumannii and Stenotrophomonas maltophilia to all antibiotic therapies tested against, 82% and 81%, respectively. Pseudomonas aeruginosa had showed a resistance rate of 62%. We also found a highly resistant Stenotrophomonas maltophilia strains to Tigecycline in our study (91%). Zhao et al concluded in a study from China that due to increased resistant rate of Tigecycline, it should be used with caution to prevent MDR strains of Stenotrophomonas maltophilia.19 This high level of antibiotic resistance in our study could be explained by the indiscriminate use of several antibiotics in the general population. The use of unprescribed antibiotics is at an all-time high in Somalia as the country has yet to develop a system that supervises the use of antibiotics among the population.
Carbapenem-resistant Acinetobacter baumannii (CRAB) and Carbapenem-resistant Pseudomonas aeruginosa (CRPA) are on the World Health Organization’s (WHO) list of antibiotic-resistant “priority pathogens” that pose the greatest risk to humankind.20 According to the National Healthcare Safety Network (NHSN) in the United States, carbapenem resistance among Acinetobacter species increased from 33% in 2006 to 2007 to more than 60% in 2009 to 2010.21 Over the past decade, the prevalence of CR-NFGNB has increased significantly worldwide.22 In the presenting study, we demonstrated the rate of CR-NFGNB to be (79.4%). CRAB was noted at 93% and CRPA was at 66%. We also found that Stenotrophomonas maltophilia was 92% resistant to carbapenem drugs specially meropenem and imipenem. Agarwal et al worked on the emergence of CR-NFGNB in ICU patients.23 They stated that Acinetobacter baumannii was 90.5% resistant to imipenem and 95.2% to meropenem. They also found that Pseudomonas aeruginosa was 52% resistant to imipenem and 56% resistant to meropenem, while Stenotrophomonas maltophilia was 100% resistant to carbapenems. In contrast to this finding, we found a higher rate of CRAB and CRPA.
In May 2016, the British Government anticipated that by 2050 approximately 10 million people worldwide would die annually as a result of antimicrobial resistance (AMR), more than currently die from cancer.24 Our analysis revealed the prevalence of MDR exhibiting NFGNB in HAP in Somalia to be 68.1%. Acinetobacter baumannii exhibited MDR patterns in 84% of cases, Stenotrophomonas maltophilia had MDR patterns of and 83%, and Pseudomonas aeruginosa showed MDR patterns in 38% of cases. This is very unpleasant reality as the country’s health system is not well equipped and unprepared to face the challenges poses by these MDR pathogens. We observed that MDR cases were more prevalent in intensive care unit (ICU) patients due to reduced immunity, male gender, and patients with chronic conditions such as diabetes, hypertension, heart disease, and COPD. Patients in ICU were more likely to have MDR strains of NFGNB compared to patients admitted to inpatient units. The mortality rate of HAP caused by NFGNB in our study was 42.5%. Mortality was very high in older patients, ICU patients, patients infected with MDR pathogens, and patients with co-morbidities.
Before evaluating the findings of this study, its limitations must be taken into account. First, the study is a retrospective study and only focused in single tertiary care hospital. Second, the study includes a limited number of antibiotics, which may not accurately represent the antimicrobial resistance level of NFGNB in Somalia. Colistin resistance was measured by disk diffusion method due to limited medical resources in our country, and the true resistance level against Colistin may be misrepresented. On the other hand, it should be noted as a strength that our study represents the first reported data regarding the antimicrobial susceptibility rate of NFGNB infections in Somalia. In addition, information regarding these pathogens in sub-Saharan Africa is scarce, and this study will fill the gap in the literature.
Conclusion
In this study, a higher incidence of multidrug-resistant (MDR) NFGNB infections was seen in HAP patients. These infections are more prevalent among men and the elderly. In our analysis, Acinetobacter baumannii was the most frequently isolated NFGNB. Acinetobacter baumannii and Stenotrophomonas maltophilia exhibited the highest antibiotic resistance rate. There is also an increased incidence of CR-NFGNB in HAP patients. Hospital infection control measurements should be enhanced in order to decrease the mounting danger posed by these pathogens. The Somali Health Ministry should also immediately implement measures to combat the growing antibiotic resistance in the country.
Abbreviations
AMR, Antimicrobial resistance; CI, Confidence interval; CLSI, Clinical & Laboratory Standards Institute; COPD, Chronic obstructive pulmonary disease; CRAB, Carbapenem resistant Acinetobacter baumannii; CR-NFGNB, Carbapenem resistant Non-fermentative gram-negative bacilli; CRPA, Carbapenem resistant Pseudomonas aeruginosa; EMB, Eosin methylene blue agar; HAP, Hospital acquired pneumonia; HIS, Hospital information system; ICU, Intensive care units; MDR, Multidrug resistance; N, Number of patients; NFGNB, Non-fermentative gram-negative bacilli; NHSN, National Healthcare Safety Network; OR, Odds ratio; SPSS, Statistical Package for Social Sciences; VAP, Ventilator-associated pneumonia.
Acknowledgment
We thank the medical microbiology unit of Mogadishu Somali Turkish Training and Research Hospital for their contribution to this study.
Disclosure
The authors declare no competing interests in relation to this study.
References
1. Kumar ST, Yassin A, Bhowmick T, Dixit D. Recommendations from the 2016 guidelines for the management of adults with hospital-acquired or ventilator-associated pneumonia. P T. 2017;42(12):767–772. PMID, 29234216; PMCID, PMC5720490.
2. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia, 2016 clinical practice guidelines by the infectious diseases society of America and the American thoracic society. Clin Infect Dis. 2016;63(5):e61–111. doi:10.1093/cid/ciw353
3. Shebl E, Gulick PG. Nosocomial Pneumonia. In: StatPearls. StatPearls Publishing; 2021.
4. Melsen WG, Rovers MM, Groenwold RH, et al. Attributable mortality of ventilator-associated pneumonia, a meta-analysis of individual patient data from randomised prevention studies. Lancet Infect Dis. 2013;13(8):665–671. doi:10.1016/S1473-3099(13)70081-1
5. Sharma D, Vyas N, Sinha P, Mathur A. Non fermentative gram negative bacilli as nosocomial pathogens, Identification and antibiotic sensitivity in clinical samples of indoor patients. Nepal J Med Sci. 2014;3(2):101–105. doi:10.3126/njms.v3i2.13452
6. Whistler T, Sangwichian O, Jorakate P, et al. Identification of Gram negative non-fermentative bacteria, How hard can it be? PLoS Negl Trop Dis. 2019;13(9):e0007729. doi:10.1371/journal.pntd.0007729
7. Enoch DA, Birkett CI, Ludlam HA. Non-fermentative Gram-negative bacteria. Int J Antimicrob Agents. 2007;1(29):S33–41. doi:10.1016/S0924-8579(07)72176-3
8. Ozenen GG, Bal ZS, Umit Z, et al. Nosocomial non-fermentative gram negative bacteria bloodstream infections in children; Risk factors and clinical outcomes of carbapenem resistance. J Infect Chemother. 2021;27(5):729–735. doi:10.1016/j.jiac.2020.12.024
9. Jeele MO, Addow RO, Adan FN, Jimale LH. Prevalence and risk factors associated with hepatitis B and hepatitis C infections among patients undergoing hemodialysis, A single-centre study in Somalia. Int J Nephrol. 2021;2021. doi:10.1155/2021/1555775
10. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. CLSI supplement M100; 2017.
11. Gilad J, Schwartz D, Amsalem Y. Clinical features and laboratory diagnosis of infection with the potential bioterrorism agents Burkholderia mallei and Burkholderia pseudomallei. Int J Biomed Sci. 2007;3(3):144.
12. Yadav SK, Bhujel R, Mishra SK, Sharma S, Sherchand JB. Emergence of multidrug-resistant non-fermentative gram negative bacterial infection in hospitalized patients in a tertiary care center of Nepal. BMC Res Notes. 2020;13(1):1–6. doi:10.1186/s13104-020-05163-6
13. Su SC, Vaneechoutte M, Dijkshoorn L, Wei YF, Chen YL, Chang TC. Identification of non-fermenting Gram-negative bacteria of clinical importance by an oligonucleotide array. J Med Microbiol. 2009;58(5):596–605. doi:10.1099/jmm.0.004606-0
14. Gajdács M, Burián K, Terhes G. Resistance levels and epidemiology of non-fermenting gram-negative bacteria in urinary tract infections of inpatients and outpatients (RENFUTI), a 10-year epidemiological snapshot. Antibiotics. 2019;8(3):143. doi:10.3390/antibiotics8030143
15. Chawla K, Vishwanath S, Munim FC. Nonfermenting gram-negative bacilli other than pseudomonas aeruginosa and Acinetobacter spp. Causing respiratory tract infections in a tertiary care center. J Glob Infect Dis. 2013;5(4):144.
16. Sidhu S, Arora U, Devi P. Prevalence of nonfermentative gram negative bacilli in seriously ill patients with bacteraemia. Jk Sci. 2010;12(4):168.
17. Gul J, Javed I, Mushtaq S, Anwar MS. Antimicrobial Susceptibility, Antimicrobial Susceptibility Pattern and Percentage of Non-Fermenter Gram Negative Bacilli (NFGNB) in Our Setup. Int Prof J Med. 2019;26(03):409–415.
18. Rahbar M, Mehregan H, Haji AA. Prevalence of drug resistance in nonfermenter gram-negative bacilli; 2010.
19. Zhao J, Liu Y, Liu Y, et al. Frequency and genetic determinants of tigecycline resistance in clinically isolated Stenotrophomonas maltophilia in Beijing, China. Front Microbiol. 2018;26(9):549. doi:10.3389/fmicb.2018.00549
20. Tacconelli E, Carrara E, Savoldi A, et al. Discovery, research, and development of new antibiotics, the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis. 2018;18(3):318–327. doi:10.1016/S1473-3099(17)30753-3
21. Sievert DM, Ricks P, Edwards JR, et al. Antimicrobial-resistant pathogens associated with healthcare-associated infections summary of data reported to the national healthcare safety network at the centers for disease control and prevention, 2009–2010. Infect Control Hosp Epidemiol. 2013;34(1):1–4. doi:10.1086/668770
22. Gniadek TJ, Carroll KC, Simner PJ. Carbapenem-resistant non-glucose-fermenting Gram-negative bacilli, the missing piece to the puzzle. J Clin Microbiol. 2016;54(7):1700–1710. doi:10.1128/JCM.03264-15
23. Agarwal S, Kakati B, Khanduri S, Gupta S. Emergence of carbapenem resistant non-fermenting gram-negative bacilli isolated in an ICU of a tertiary care hospital. J Clin Diagnostic Res. 2017;11(1):DC04.
24. El Chakhtoura NG, Saade E, Iovleva A, et al. Therapies for multidrug resistant and extensively drug-resistant non-fermenting gram-negative bacteria causing nosocomial infections, a perilous journey toward ‘molecularly targeted’therapy. Expert Rev Anti Infect Ther. 2018;16(2):89–110. doi:10.1080/14787210.2018.1425139
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.