")
Back to Journals » Infection and Drug Resistance » Volume 16
Epidemiological and Clinical Characteristics of COVID-19 Outbreak in a Mental Hospital in Wenzhou, China, December 2022–January 2023
Authors Zhou Y, Huang Y, Wu C, Yang H, Shan C, Zhou Z
Received 10 April 2023
Accepted for publication 10 August 2023
Published 30 August 2023 Volume 2023:16 Pages 5719—5728
DOI https://doi.org/10.2147/IDR.S416565
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Yiwei Zhou,1 Yu Huang,2 Chunhua Wu,2 Hongsheng Yang,2 Chunyan Shan,2 Zumu Zhou2
1Business School, University of Shanghai for Science and Technology, Shanghai, People’s Republic of China; 2The Affiliated Kangning Hospital of Wenzhou Medical University Zhejiang Provincial Clinical Research Center for Mental Disorders, Wenzhou, People’s Republic of China
Correspondence: Zumu Zhou, The Affiliated Kangning Hospital of Wenzhou Medical University Zhejiang Provincial Clinical Research Center for Mental Disorders, 1 Shengjin Road, Huanglong Residential District, Wenzhou, 325007, People’s Republic of China, Tel +86-13857709701, Fax +86-577-88789117, Email [email protected]
Background: Coronavirus disease (COVID-19) mainly caused by the Omicron virus strain currently is still prevalent worldwide, and many medical institutions have experienced COVID-19 outbreaks in the past three years.
Objective: This article reported COVID-19 outbreak among health care workers in a mental hospital to clarify the epidemiological and clinical characteristics of COVID-19 outbreak in a medical institution, to assess the susceptible factors related to COVID-19 among these personnel and to evaluate the effect of COVID-19 vaccine on the medical workers.
Methods: A uniform questionnaire was used to investigate all employees, including age, gender, department, time of onset, clinical symptoms, vaccination status. At the same, the results of laboratory testing, chest computed tomography (CT) and/or X-ray examination were collected.
Results: Among 1047 hospital employees, 842 cases were diagnosed as COVID-19, with a total attack rate of 80.42%. The attack rate of doctors, nurses, medical technicians, and administrators (83.50– 90.67%) was higher than that of logistics departments (56.81%). Out of the 842 patients, 9 were hospitalized; 833 were non-hospitalized patients who belong to mild or moderate cases. No deaths were reported. The full vaccination rate and booster rate of COVID-19 vaccine were 78.26% and 80.87%, respectively. There was no significant correlation between the attack rate and COVID-19 vaccine (χ2 = 3.41 P > 0.05).
Conclusion: This is an outbreak of COVID-19 with a high attack rate among employees in a mental hospital. The attack rate of medical personnel is higher than that of logistics personnel, which may be related to opportunities and duration of contact with infected individuals. COVID-19 vaccine has no significant protective effect on patients with mild or moderate symptoms 13 months after the full vaccination. It is suggested that they should be timely boostered with COVID-19 vaccine to maintain their immunity to the disease.
Keywords: COVID-19, outbreak, health care workers, mental hospital
Introduction
Coronavirus disease (COVID-19) caused by Severe Acute Respiratory Syndrome-Coronavirus-2 (SARS-CoV-2) has been prevalent globally for more than three years, affecting almost all countries, with varying degrees of COVID-19 pandemic.1,2 Since the pandemic of COVID-19, China has been taking strict prevention and control measures, achieving satisfactory results. Compared with most other countries, COVID-19 epidemics or outbreaks have occurred on a small scale and in a small number, with fewer deaths in China. At the end of 2022, China adjusted, optimized, and relaxed the prevention and control measures against COVID-19,3 based on the epidemiological characteristics, pathogen changes, and clinical characteristics of the disease. Subsequently, a new wave of COVID-19 epidemic occurred. While the COVID-19 epidemic occurred in communities, many institutions also experienced COVID outbreaks.
The researches showed that the epidemiological characteristics (such as the spatial, temporal and population distributions) and clinical characteristics (such as clinical manifestations, disease severity) of COVID-19 among medical personnel in different regions, periods, and medical institutions were different,4–9 based on the variation of SARS CoV-2 virus, as well as the changes in medical system and prevention and control strategies, population density and mobility, medical resources, COVID-19 vaccination and antibody levels of population etc.10
Hospitals are vulnerable to COVID-19 outbreaks. Since the initial outbreak of the COVID-19 in Wuhan at the end of December 2019, in the past three years, outbreaks of nosocomial COVID-19 infections have occurred in many countries, such as Malaysia, Spain, Switzerland, Germany, Italy, and Vietnam.4–11 However, the epidemiological and clinical characteristics of these outbreaks are not all the same, their morbidity and case fatality rates and the scale of the outbreaks varies. In China, the government has adopted stringent COVID-19 prevention and control measures until November 2022, with low morbidity and mortality, and few large-scale COVID-19 outbreaks in hospitals.
After China’s prevention and control measures were adjusted from very strict to optimized and relaxed policy, an outbreak of COVID-19 occurred among medical personnel in a mental hospital in Wenzhou, China from December 2022 to Januray 2023. Then, an epidemiological survey of this COVID-19 outbreak in the mental hospital was carried out. The aim of the present study is to illuminate the epidemiological and clinical characteristics of the COVID-19 outbreak, to assess the susceptible factors related to COVID-19 among these personnel and to evaluate the effect of COVID-19 vaccination on the occurrence of disease among the medical workers.
Subjects and Methods
Subjects
The investigation into this outbreak was a cross-sectional survey. The subjects of this outbreak investigation was all medical personnel in the hospital during the outbreak. All 1047 employees in the mental hospital were surveyed during the outbreak. These employees include 641 medical personnel (175 doctors, 303 nurses, 163 medical technicians), logistics personnel (213 cases), and administrative management personnel (193 cases).
Case Definition
Employees who worked in the mental hospital from December 8, 2022 to January 2, 2023, had a history of contact to COVID-19 patient, and had acute an onset of fever and cough or had an acute onset of any three or more of the following signs or symptoms: fever, cough, general fatigue, myalgia, nasal congestion, runny nose, decreased sense of smell and taste, diarrhea, conjunctivitis, etc.12 Or imaging features of pneumonia in chest; Or laboratory testing for nucleic acid positive by real-time polymerase chain reaction (RT-PCR); At the same time, other diseases are excluded. If only nucleic acid is positive by RT-PCR without clinical symptoms, he/she will not be considered as a COVID-19 case.
Questionnaire
The questionnaire was designed by ourselves, as shown in the Supplementary Material. The clinical symptoms in the questionnaire were referred to WHO document.12 The questionnaire includes general demography, epidemiology, clinical, laboratory and imaging data. The infection control department of hospital notified the uniformly designed questionnaire to each employee of hospital through WeChat network. Each employee directly fills in an epidemiological questionnaire on their mobile phone or computer, recording their onset and related conditions during the period from December 8, 2022 to January 2, 2023, including age, gender, department, onset time, clinical symptoms, vaccination status. The results of laboratory testing, chest CT and/or X-ray examination were also collected, and the medical records were reviewed if necessary. After completing the questionnaire, they send it back to the Sojump software platform through WeChat network.
Laboratory Examination
Pharyngeal swab samples were collected from COVID-19 cases at the early stage of the outbreak, and SARS-COV-2 nucleic acid was detected by RT-PCR. At the same time, a selective examination of some cases in this outbreak was made for detection of SARS-COV-2 antigen.
Statistical Method
Excel software was used to analyze the collected data. The data was expressed in case number, percentage or rate, and the percentage or rate in different groups were compared by Chi square test. The difference was statistically significant when P value was < 0.05.
Ethical Approval
The current study was approved by the Ethics Committee of The Affiliated Kangning Hospital of Wenzhou Medical University, Wenzhou, China (No 2023017). All participants included in the study provided informed consent. The research was conducted in line with the Declaration of Helsinki and Good Clinical Practice. The aim and scope of the research were explained at the beginning of the survey in the questionnaire. A sentence on voluntary informed consent was added at the beginning of the questionnaire and participants who did not give voluntary informed consent were not allowed to continue the survey.
Results
Time Distribution of COVID-19 Cases
The first case of this COVID-19 outbreak among hospital employees was a 27 years old female who began to develop symptoms such as fever, dry cough, fatigue, nasal congestion, runny nose, and myalgia on December 8, 2022. CT examination of the chest revealed inflammatory imaging features. The onset date of the last case of this outbreak was January 2, 2023. The outbreak of 842 cases lasted 26 days. From the onset date of the first case to December 12, there were a small number of sporadic cases. From December 13 to December 18, the number of cases with COVID-19 gradually increased, and the outbreak reached its peak time from December 19 to 23. The total number of cases in the four days was 417 cases, accounting for 48.52% of the total number of cases in this outbreak; the highest number of cases occurred on December 22, reaching 116 cases. Subsequently, the number of cases gradually decreased, and no cases occurred after January 3, 2023. Finally, the outbreak ended. See Figure 1.
 |
Figure 1 Time distribution of COVID-19 cases. |
Incidence Rates by Gender and Age
Of the 1047 hospital employees surveyed, 842 cases were affected, with a total attack rate of 80.42%. Of the 355 male employees, 273 were affected, with an attack rate of 76.90%; Of 692 female employees, 569 were affected, with an attack rate of 82.22%; The attack rate in women was slightly higher than that in men, with a statistically significant difference (χ2 = 4.22 P < 0.05). There was also a significant difference in attack rate among different age groups (χ2 = 62.63 P < 0.05); The attack rate in the 20–49 year old group was higher than that in the over 50 year old group (χ2 = 4.22 P < 0.05). See Table 1.
 |
Table 1 Attack Rate of Employees by Age |
Incidence Rates for Different Types of Work
There is a statistically significant difference in the attack rate among different types of employees (χ2 = 98.96 P < 0.01); The attack rate of doctors, nurses, medical technicians, and administrative personnel (83.50% − 90.67%) is higher than that of logistics personnel (56.81%), with a statistically significant difference (χ2 = 94.68 P < 0.01). See Table 2.
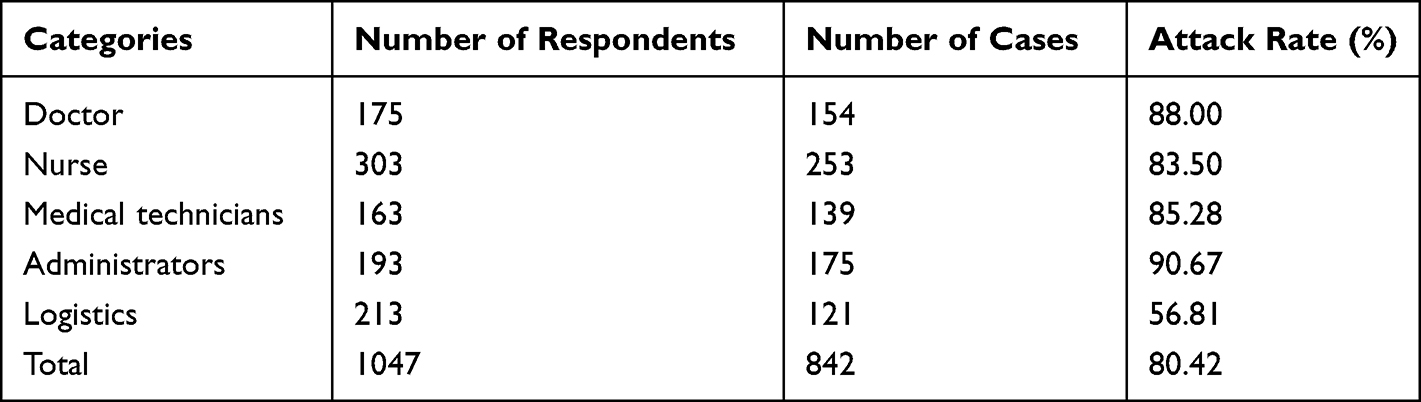 |
Table 2 Attack Rate of Different Categories of Employees |
Clinical Manifestations
Out of the 842 patients, 750 had fever, and namely, the infected patients had the highest proportion of fever, accounting for 89.07%; Other symptoms in turn were fatigue, dry cough, myalgia, nasal congestion, runny nose, decreased sense of smell (taste), and diarrhea, conjunctivitis. See Table 3. Out of the 842 patients, 9 were hospitalized, including 6 mild cases, 1 moderate case, and 2 severe cases; One of the two severe patients has been transferred to another hospital for further treatment. Eight hundred and thirty-three non-hospitalized cases were mild to moderate in severity, and no deaths were reported. Some cases have a long duration of dry cough, with a few patients’ coughing for about a month.
 |
Table 3 Main Clinical Manifestations of COVID-19 Patients |
Laboratory and Chest Imaging Examination
Out of the 1047 hospital employees surveyed, 418 (39.93%) were SARS-CoV-2 nucleic acid positive for RT-PCR; 473 cases (45.18%) were positive for SARS-CoV-2 antigen; 92 cases (8.79%) had inflammatory manifestations on chest imaging.
Attack Rate for Different Doses of Vaccine
Out of the 1047 hospital employees surveyed, among whom 161 people were fully-vaccinated, with 2 doses, and out of these 161 people, there were 126 cases with a attack rate of 78.26%; out of these 1047 hospital employees surveyed, among whom 847 people were vaccinated with 3 doses or more (booster vaccination), out of these 847 people, there were 685 cases with a attack rate of 80.87%. There was no significant difference in the attack rate between the unvaccinated group and the different dose vaccination groups (χ2 = 3.41 P > 0.05); There was also no significant difference in the attack rate between the group of 2 dose (full vaccination) recipients or more (booster vaccination) and the group of unvaccinated or only 1 dose recipients (χ2 = 0.36 P > 0.05). See Table 4.
 |
Table 4 Attack Rate in Vaccine Recipients by Dose(s) |
Prevention and Control Measures
The hospital paid great attention to this outbreak and had established a special epidemic control team in response to the epidemic. It has held multiple prevention and control meetings, strengthened the infection management and epidemic reporting mechanism in hospital, implemented various measures such as disinfection, and strengthened medical personnel’s washing hands, wearing masks, and ventilation of the room. Due to a relatively lack of medical personnel to diagnose and care for patients during COVID-19 outbreak at that time, the isolation measures for medical personnel in small number of wards could not keep pace with the requirements. In consequence, strict isolation was not achieved, making it difficult to achieve the required isolation time. In addition, because some medical personnel have mild clinical symptoms and no obvious discomfort, they have also participated in some diagnosis and treatment work even under strict personal protection, and a few of these medical personnel in this outbreak may have infected other personnel or patients.
Discussion
On January 20, 2020, China began to implement strict Class A prevention and control measures for infectious diseases against COVID-19.13 For three years, the National Health Commission has always adhered to optimizing and adjusting the prevention and control policies and measures according to the time and situation, effectively coordinated the epidemic prevention and control and economic and social development, successfully avoided the widespread epidemic of SARS-CoV-2 strains with its strong pathogenicity and high mortality, and effectively protected people’s life and health. Given that the country has effectively responded to the impact of five successive waves of global epidemics, greatly reducing severe and fatal cases, and also winning valuable time for the development and application of vaccines and drugs, as well as the preparation of medical and other resources. Through the joint efforts of all parties, China has maintained the lowest level of epidemic cases and deaths in the world.
Currently, the Omicron mutant has become a dominant epidemic strain globally, with faster transmission speed, stronger concealment, and greater difficulty in prevention and control, as compared to previous other variants. According to the changes in the epidemic situation and the characteristics of virus mutation, the country has continuously optimized and improved its prevention and control policies, making them more scientific and accurate, so as to not only prevent the epidemic, but also minimize the impact on economic and social development and people’s livelihood. On November 11, 2022, the joint prevention and control mechanism of the State Council of China made a number of adjustments to the epidemic prevention and control policy.3 In addition, China’s announcement to downgrade its management of the infectious disease of COVID-19 from Class A to Class B, starting from January 8, 2023, that is a major shift in COVID-19 prevention and control policy.14 As China adjusts and optimizes its prevention and control policies, a new wave of COVID-19 epidemics has emerged, affecting a wide range of people and causing a large number of infections. COVID-19 outbreaks have occurred in most communities and certain institutions. An outbreak of COVID-19 has also occurred among medical personnel in a mental hospital in Wenzhou, China.
Given that the epidemic of COVID-19 occurred in local communities and many institutions in Wenzhou, China, there occurred some group-based typical COVID-19 clinical manifestations such as fever, cough, headache, fatigue, myalgia, decreased sense of smell (taste), nasal congestion, runny nose, and diarrhea among hospital employees in the mental hospital in a short period of time. Most of the employees were positive for SARS-CoV-2 nucleic acid by RT-PCR and positive for antigen tests, and some employees had typical imaging features of pulmonary inflammation. Based on the above epidemiological characteristics, clinical features, and laboratory test results, it is believed that this was an outbreak of COVID-19 among employees in a mental hospital.
The source of infection for COVID-19 outbreaks among medical personnel may come from communities outside of the work place.15,16 In fact, a number of studies using genome sequencing have shown that healthcare workers may be infected in the community, which has contributed to a major COVID-19 outbreak in medical institutions. An epidemiological survey conducted in three hospitals in the Netherlands with genetic data showed that the comprehensive community spread of SARS CoV-2 and super transmission events such as carnivals may be the source of infection for some medical personnel.16 The present investigation of infectious source found that on December 3 before this outbreak, a female employee suffered from COVID-19 in the his community. After her condition was discovered, she was isolated at home and was unable to go to work in the hospital. However, before the case was discovered, many cases had occurred in the community where she lived, and there were also cases in neighbors. In the hospital, she might have had contact with other employees within her incubation period before illness, which might be transmitted to other employees as a source of infection. In addition, before the outbreak of COVID-19 in the hospital, in fact, many COVID cases had occurred in some communities and families. As the interface between hospitals and communities, medical personnel are likely to become the source of infection for the cross transmission of SARS-CoV-2.16,17 Some patients who come to the hospital from the community may also bring SARS-CoV-2 caused DOVID-19 into the hospital and spread it to other medical personnel, thereby becoming the source of infection for this outbreak.
Research has shown that patients who suffered from a severe case or death are often older, with the majority of people over the age of 70, and often have comorbidities or complications. However, in this outbreak, people under the age of 60 accounted for 96.85% of the total number of employees, and workers in the 20 − 39 age group accounted for 67.24% of the total number of employees. These medical workers were young, usually healthy, and basically without complications. In addition, as the epidemic continues, the virulence of the virus will gradually decrease. The virulence of the recently prevalent Omicron strain has decreased as compared to the past, resulting in a decrease in the number of severe cases, a decrease in the proportion of them, and an increase in the proportion of mild cases. This investigation showed that the cases of outbreak were mainly mild, and a few patients (1.07%) needed to be hospitalized. Some of them recovered after treatment, while others recovered without treatment. There were no severe cases or deaths in this outbreak. It can be seen that the majority of mild cases in this outbreak may be related to the young age of the employees and to and pathogen mutations, and the vast majority of young people without comorbidities or complications, stronger resistance than the elderly.
According to a survey, the occurrence of COVID-1 is related to gender. The COVID-19 infection rate (71.6%) among female medical personnel is higher than that among male medical personnel.18,19 The present survey showed that the attack rate of female medical personnel (82.22%) is higher than that of male (76.90%), which may be related to the more exposure of women to the virus. For example, nurses often have a longer contact with patients than other health care workers, and more frequent contacts with patients than them.
According to reports, the total infection rate among hospital medical personnel was 9.20% (14,058/152,888), with the highest number of COVID-19 infections in the 50 − 59 age group, accounting for 34.23% (4812/14,058); The group aged over 70 has the lowest morbidity rate, but this age group also has a high case fatality rate.19–21 However, morbidity data for medical personnel by age group in hospitals in most countries are often difficult to obtain. This outbreak survey showed that the attack rate in the 50–59 age group was the lowest, at 55.37%, which was lower than the attack rate in other age groups, and was different from the report by Gómez-Ochoa et al.19
According to a report, the attack rate of medical personnel in 6 outbreaks was 21.7 ± 17.4%.19 During the COVID-19 outbreak, 85% of medical personnel experienced symptoms, mainly in the upper respiratory tract, but 15% of medical personnel remained asymptomatic. Fever (85%) is the most common symptom of COVID-19. Other symptoms include headache (85%), cough (80%), and discomfort (70%), while nausea/vomiting (9%) and other symptoms appear less frequently.18 Other studies have reported that the attack rates of different symptoms after COVID-19 infection were: fever 57% − 85%, headache 7% − 81%, cough 56% − 80%, chills 4.5%, diarrhea 7% − 18%, dyspnea 20%, fatigue 38%, hemoptysis 7%, discomfort 43% − 70%, myalgia 17.8% − 48%, nausea/vomiting 7% − 9%, shortness of breath 22%, and sore throat 20.7%.18 In addition, some patients have olfactory disorders.19 Our survey showed that the attack rates of fever, fatigue and dry cough among patients were 89.07%, 80.88%, and 77.91% respectively. The others were nasal congestion (60.45%), myalgia (56.18%), runny nose (50.48%), decreased or disappeared sense of smell and taste (41.81%), diarrhea (15.44%), and conjunctivitis (3.21%). The present survey showed that the proportion of fatigue and myalgia is higher, the duration of cough was longer, and other symptoms are basically similar as compared to the symptoms reported in the other studies mentioned above.
This survey of the outbreak showed that COVID-19 is highly contagious among medical personnel in the mental hospital, with the vast majority of employees becoming ill within a short period of time and a high attack rate. Among the 1047 employees in the hospital, 842 people have become ill, with an attack rate of up to 80%. Moreover, the transmission speed is also very fast, with over 80% of the personnel suffering from disease within just 26 days.
It was reported that medical personnel working on the front line had a high infection rate through direct contact with COVID-19 patients.18,22,23 Among medical workers with different roles, nurses had the highest infection rate, ranging from 38.6% to 48%; The doctors had the infection rate of 25% (95% CI: 12% − 36%), and the other medical personnel had 23%.18 In countries seriously affected by the epidemic, such as Europe and the Americas, the proportion of infections among medical personnel was high. The infection rates among medical personnel and the ordinary people were 14.5% and 8.5%, respectively. According to the available survey results, the infection rate among female medical personnel and nurses was higher. The high infection rate among nursing staff may be related to the nature of nursing responsibilities, including 24-hour care for infected patients. In addition, nurses were medical personnel primarily involved in screening patients. So they were prone to exposure to SARS-CoV-2 before diagnosis.14 Our investigation shows that in this outbreak of COVID-19, the attack rate of medical personnel was higher than that of logistics personnel, while the incidence rate of doctors and nurses was similar. The reason may be related to the fact that medical personnel (including doctors, nurses and medical technicians) had more contact opportunities with COVID-19 patients than logistics personnel, longer contact time, and longer exposure time in indoor environments. There was no statistically significant difference in the attack rate between doctors and nurses, which may be related to similar exposure opportunities at work.
The findings of the current research indicate that during the COVID-19 pandemic, medical personnel are highly likely to be exposed to SARS-CoV-2.16,18 The COVID-19 outbreak is mainly characterized by respiratory droplets and contact transmissions.2,24 And this outbreak is also believed to be transmitted in this manner. Personal protection should be strengthened to reduce risk, and infection control measures should be implemented to reduce transmission within the hospital.25 In order to prevent COVID-19 infection among healthcare workers in medical institutions, to detect cases early, and reduce the transmission of COVID-19 to colleagues and patients with other diseases,18 RT-PCR should be used to conduct SARS-CoV-2 nucleic acid screening, while implementing various other infection control measures, such as wearing masks, washing hands, opening windows for ventilation, and restricting visits to patients. Performing SARS-CoV-2 nucleic acid screening is one of the most important preventive measures during the COVID-19 pandemic, as medical personnel may not know that they have acquired infection before receiving testing. After this outbreak occurred, the hospital immediately took many control measures, but due to multiple reasons and the simultaneous implementation of these measures, it is difficult to determine which measures are effective for this outbreak.
It is reported that most of the vaccines used globally have poor efficacy, and the resulting immune duration is not long.26 COVID-19 vaccine only has a certain effect on preventing severe cases and deaths in the short term, but has no significant effect on mild cases.27 The present survey showed that the vaccination rate of hospital employees is high, reaching 97.80%; The full vaccination rate (including booster vaccination) was 96.28%. In November 2021, the hospital organized a collective COVID-19 booster vaccination, which has been 13 months before this COVID-19 outbreak. In addition, as the produced antibodies after vaccination gradually decrease over time, the effectiveness of prevention will also decrease. Although the COVID-19 vaccine previously administered has a high vaccination rate and sufficient doses, it may not have played a preventive role in this outbreak due to the fact that it was administered more than a year ago.
This outbreak investigation examines the epidemiological and clinical characteristics of the COVID-19 outbreak among medical staff in a mental hospital in Wenzhou and impacts of vaccination received by medical staff on the attack rate of COVID-19 after optimizing, adjusting and relaxing COVID-19 prevention and control measures in China, In addition, results of this investigation will also help provide a scientific basis for the formulation of COVID-19 prevention and control policies and disease diagnosis and treatment.
Our study has some limitations. First, due to human, material and financial resources, serological test of COVID-19 for health care workers was not conducted. In this outbreak investigation, the identification of cases was mainly based on epidemiology, clinical manifestations, RP-PCR and antigen examination, while the results of serological test were not included. Generally speaking, in an outbreak of COVID-19, there may be some subclinical infected individuals who have no clinical symptoms but are infectious and can transmit SARS-CoV-2 to others. Serological test can be used to detect asymptomatic subclinical infections. Due to the lack of serological testing, it is possible to omit the inapparent infected individuals during the investigation. Second, the vaccine recipients in this outbreak did not undergo SARS-CoV-2 antibody tests after vaccination, so it is difficult to know the serological reaction after vaccination and the seroconversion rate over time.
When carrying out epidemiological investigations of COVID-19 outbreak in the future, it is necessary to increase serological examination of the respondents to determine the antibody response to SARS-CoV-2 of the subjects under investigation, to identify subclinical infections and the infection spectrum of the disease. In addition, it is necessary that the serological response and antibody positive conversion rate be evaluated among vaccine recipients.
Conclusion
This study reported the epidemiological and clinical features of COVID-19 outbreak among the medical staff of a mental hospital in Wenzhou, China, from December 2022 to January 2023, with a high attack rate. The attack rate of women is higher than that of men, and the attack rate of medical personnel is higher than that of logistics personnel. The investigation showed that in this outbreak among medical staff in the mental hospital, SARS CoV-2 was highly contagious and spread rapidly. Since COVID-19 vaccine among the medical care workers in the hospital were inoculated more than a year ago, it has no significant protective effect on health care workers with mild or moderate symptoms. Therefore, it is very important to booster the COVID-19 vaccine for medical personnel in time to maintain the their immunity to the disease. Additionally, this survey will help inform the prevention and control of similar outbreaks, and the development of COVID-19 vaccine in the future.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Statement
The study protocol was reviewed and approved by Ethics Committee of the Affiliated Kangning Hospital of Wenzhou Medical University (No 2023017). The research was conducted in line with the Declaration of Helsinki and Good Clinical Practice. Before conducting the investigation, each respondent was informed that the information collected during this survey will be kept confidential and will not be disclosed; The data was kept by a special person. The respondents were aware of the use of this information; If patients was not willing to accept the survey, they may not fill in the questionnaire.
Acknowledgments
We would like to express our heartfelt gratitude to all staff at The Affiliated Kangning Hospital of Wenzhou Medical University who were involved in the epidemiological investigation.
Funding
This work was financially supported by 2022 Ministry of Education of China Humanities and Social Science Youth Foundation Project (22YJC790189) and Shanghai University Young Teachers Cultivation and Support Project.
Disclosure
The authors declare that they have no competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Zhou Z-M, Zhou H-Z, Lin X-D, et al. Outbreak of COVID-19 in a family, Wenzhou, China. Epidemiol Infect. 2020;148:e103. doi:10.1017/S0950268820001089
2. Zhou Y, Xiang F, Ni C, et al. Travel-associated outbreak of COVID-19 in a departmental store, Wenzhou, China. J Infect Dev Ctries. 2022;16(5):752–758. doi:10.3855/jidc.15670
3. National Health Commission of the People’s Republic of China. Notice on further optimizing the prevention and control measures of COVID-19 and carrying out prevention and control work scientifically and accurately. Available from: http://www.nhc.gov.cn/xcs/zhengcwj/202211/ed9d123bbfe14e738402d846290049ea.shtml.
4. Chong DW, Jayaraj VJ, Ng CW, et al. Propagation of a hospital-associated cluster of COVID-19 in Malaysia. BMC Infect Dis. 2021;21(1):1238. doi:10.1186/s12879-021-06894-y
5. Giesen C, Diez-Izquierdo L, Saa-Requejo CM, et al.; COVID Epidemiological Surveillance and Control Study Group. Epidemiological characteristics of the COVID-19 outbreak in a secondary hospital in Spain. Am J Infect Control. 2021;49(2):143–150. doi:10.1016/j.ajic.2020.07.014
6. Zeeb M, Weissberg D, Rampini SK, et al. Identifying contact risks for SARS-CoV-2 transmission to healthcare workers during outbreak on COVID-19 ward. Emerg Infect Dis. 2022;28(10):2134–2137. doi:10.3201/eid2810.220266
7. Wolfensberger A, Kufner V, Zaheri M, et al. Nosocomial COVID-19 incidence and secondary attack rates among patients of tertiary care center, Zurich, Switzerland. Emerg Infect Dis. 2022;28(10):2087–2090. doi:10.3201/eid2810.220321
8. Schwierzeck V, König JC, Kühn J, et al. First reported nosocomial outbreak of Severe Acute Respiratory Syndrome Coronavirus 2 in a pediatric dialysis unit. Clin Infect Dis. 2021;72(2):265–270. doi:10.1093/cid/ciaa491
9. Lucey M, Macori G, Mullane N, et al. Whole-genome sequencing to track severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2) transmission in nosocomial outbreaks. Clin Infect Dis. 2021;72(11):e727–e735. doi:10.1093/cid/ciaa1433
10. Piapan L, De Michieli P, Ronchese F, et al. COVID-19 outbreaks in hospital workers during the first COVID-19 wave. Occup Med. 2022;72(2):110–117. doi:10.1093/occmed/kqab161
11. Duy C, Nong VM, Van Ngo A, et al. Nosocomial coronavirus disease outbreak containment, Hanoi, Vietnam, March–April 2020. Emerg Infect Dis. 2021;27(1):10–17. doi:10.3201/eid2701.202656
12. World Health Organization. WHO COVID-19 case definition: updated in public health surveillance for COVID-19. Available from: https://www.who.int/publications/i/item/WHO-2019-nCoV-Surveillance_Case_Definition-2022.1.
13. National Health Commission of the People’s Republic of China. Pneumonia caused by novel Coronavirus is included in notifiable infectious disease management. Available from: http://www.nhc.gov.cn/xcs/zhengcwj/202001/44a3b8245e8049d2837a4f27529cd386.shtml3.
14. Global Times. From prevention to treatment, COVID diagnosis and treatment protocol pursues ‘optimal solution’: global Times editorial; 2023. Available from: https://www.globaltimes.cn/page/202301/1283361.shtml.
15. Tan LF. Preventing the transmission of COVID-19 amongst healthcare workers. J Hosp Infect. 2020;105(2):364–365. doi:10.1016/j.jhin.2020.04.008
16. Sikkema RS, Pas SD, Nieuwenhuijse DF, et al. COVID-19 in health-care workers in three hospitals in the south of the Netherlands: a cross-sectional study. Lancet Infect Dis. 2020;20(11):1273–1280. doi:10.1016/S1473-3099(20)30527-2
17. Mimura K, Oka H, Sawano M. A perspective on hospital-acquired (nosocomial) infection control of COVID-19: usefulness of spatial separation between wards and airborne isolation unit. J Breath Res. 2021;15(4). doi:10.1088/1752-7163/ac1721
18. Chutiyami M, Bello UM, Salihu D, et al. COVID-19 pandemic-related mortality, infection, symptoms, complications, comorbidities, and other aspects of physical health among healthcare workers globally: an umbrella review. Int J Nurs Stud. 2022;129:104211. doi:10.1016/j.ijnurstu.2022.104211
19. Gómez-Ochoa SA, Franco OH, Rojas LZ, et al. COVID-19 in health-care workers: a living systematic review and Meta-analysis of prevalence, risk factors, clinical characteristics, and outcomes. Am J Epidemiol. 2021;190(1):161–175. doi:10.1093/aje/kwaa191
20. Cyh N, Lim NA, Bao LXY, et al. Mitigating SARS-CoV-2 transmission in hospitals: a systematic literature review. Public Health Rev. 2022;43:1604572. doi:10.3389/phrs.2022.1604572
21. Bandyopadhyay S, Baticulon RE, Kadhum M, et al. Infection and mortality of healthcare workers worldwide from COVID-19: a systematic review. BMJ Glob Health. 2020;5(12):e003097. doi:10.1136/bmjgh-2020-003097
22. Shepard J, Kling SMR, Lee G, et al. The prevalence of COVID-19 in healthcare personnel in an adult and pediatric academic medical center. Am J Infect Control. 2021;49(5):542–546. doi:10.1016/j.ajic.2021.01.004
23. Huang L, Lin G, Tang L, et al. Special attention to nurses’ protection during the COVID-19 epidemic. Crit Care. 2020;24(1):120. doi:10.1186/s13054-020-2841-7
24. Al-Tawfifiq JA, Zumla A, Memish ZA. Travel implications of emerging coronaviruses: SARS and MERS-CoV. Travel Med Infect Dis. 2014;12(5):422–428. doi:10.1016/j.tmaid.2014.06.007
25. Li J. Prevention is key to reducing the spread of COVID-19 in long-term care facilities. Infect Drug Resist. 2022;15:6689–6693. doi:10.2147/IDR.S386429
26. Fan Y, Li X, Zhang L, et al. SARS-CoV-2 Omicron variant: recent progress and future perspectives. Signal Transduct Target Ther. 2022;7(1):141. doi:10.1038/s41392-022-00997-x
27. Li J, Jiang N, Zeng QL, et al. The epidemiological, clinical features and outcomes of imported Chinese COVID-19 patients following inactivated vaccines injection. Infect Drug Resist. 2022;15:2115–2125. doi:10.2147/IDR.S35646
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.