")
Back to Journals » Infection and Drug Resistance » Volume 16
Enterococcus casseliflavus Infection: A Review of Clinical Features and Treatment
Authors Yoshino Y
Received 22 November 2022
Accepted for publication 16 January 2023
Published 20 January 2023 Volume 2023:16 Pages 363—368
DOI https://doi.org/10.2147/IDR.S398739
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Yusuke Yoshino
Teikyo University, School of Medicine, Department of Microbiology and Immunology, Tokyo, Japan
Correspondence: Yusuke Yoshino, Teikyo University, School of Medicine, Department of Microbiology and Immunology, 2-11-1, Kaga, Itabashi, Tokyo, 173-8605, Japan, Tel +81-3-3964-1211, Email [email protected]
Abstract: Some Enterococcus species, including Enterococcus faecalis and E. faecium, are increasingly becoming a common cause of nosocomial infections, accounting for the majority of human enterococcal infections, while other species, such as E. casseliflavus, have also been shown to be pathogenic to humans due to the increase in immunocompromised patients. These infections vary widely in their mode of transmission, symptoms, and other characteristics. Treatment is difficult in some cases because enterococci are resistant to numerous antimicrobial agents. Enterococcus faecalis and E. faecium are the best-known opportunistic pathogens, but others, including E. casseliflavus, occasionally cause opportunistic infections. This review summarizes the clinical features of E. casseliflavus infections and discusses effective therapeutic strategies. Bacteremia was the most common form of E. casseliflavus infections. Because E. casseliflavus carries the VanC gene, which confers resistance to vancomycin, less resistant drugs such as ampicillin were found more effective in treating the bacteremia. The second most common form of E. casseliflavus infection was trauma-induced endophthalmitis. This was commonly reported in active young to middle-aged patients. Vitreoretinal surgery and local or systemic administration of sensitive antimicrobial agents seem to be key to successful treatment. Other conditions such as infective endocarditis, meningitis, peritonitis, and pyothorax have also been reported as forms of E. casseliflavus infection. This review clarifies the clinical features of E. casseliflavus infection and provides important insights into its treatment.
Keywords: nosocomial infections, bacteremia, endophthalmitis, vancomycin
Introduction
Enterococci, a group of widespread Gram-positive facultative anaerobic bacteria, have more than 40 described species. Although previously considered to belong to the Streptococci group, DNA homology studies have suggested that Enterococcus is a distinct genus.1 These bacteria are usually found in the intestines of humans and animals, on the surfaces of plants, and in dairy products.2 They persist in the environment because of their ability to survive under a range of conditions, including drying, extreme temperatures, high osmolarity, and the presence of disinfectants.3 Moreover, enterococci are also used in food production as probiotic products to monitor fecal contamination.4
However, some species of the bacteria are an increasingly common cause of nosocomial infections, such as Enterococcus faecalis and E. faecium, accounting for the majority of human enterococcal infections, while others like E. casseliflavus have also been shown to be pathogenic to humans.5 E. casseliflavus has been assigned the species status in 1984; it is a motile bacterium that produces a yellow pigment.6 E. casseliflavus is rarely found in clinical samples (< 1.3%);7 however, it is an opportunistic pathogen that targets individuals who are immunocompromised or chronically ill and is sometimes nosocomially acquired.8 Although uncommon, E. casseliflavus infection can be seriously invasive. Yet, few studies have summarized the characteristics of these infections.
Here, reports of E. casseliflavus infections and their features are reviewed. Furthermore, I summarize commonly reported manifestations of E. casseliflavus infections, along with discussions of case studies and clinical therapies. All E. casseliflavus-related clinical manuscripts written in English listed on PubMed (https://pubmed.ncbi.nlm.nih.gov/) were included.
Bacteremia
Bacteremia was the most common form of E. casseliflavus infection. Eleven case reports and 12 retrospective cohort studies/case series of E. casseliflavus bacteremia were reviewed.9–31 The treatment courses of all 11 reported cases were summarized in Table 1. Specific background factors of bacteremia cases, including cirrhosis, chronic obstructive pulmonary disease, cancers (including those on chemotherapy) and its complications, advanced age, and steroid use, were identified in the case reports. Ten of eleven patients had at least one of these background factors. Retrospective cohort studies showed that 40.12–48.8% of the patients with bacteremia due to E. casseliflavus had solid tumors as a complication.27,30 A study evaluating E. casseliflavus and E. gallinarum bacteremia cases showed that malignancy (70.0%) and diabetes mellitus (20.0%) were the most common complications in these bacteremia cases.31 These results indicate that E. casseliflavus bacteremia is more likely to occur in immunocompromised hosts. Case reports suggest that the susceptible age for this bacteremia is mainly 60–80 years; however, neonatal cases have also been reported.14
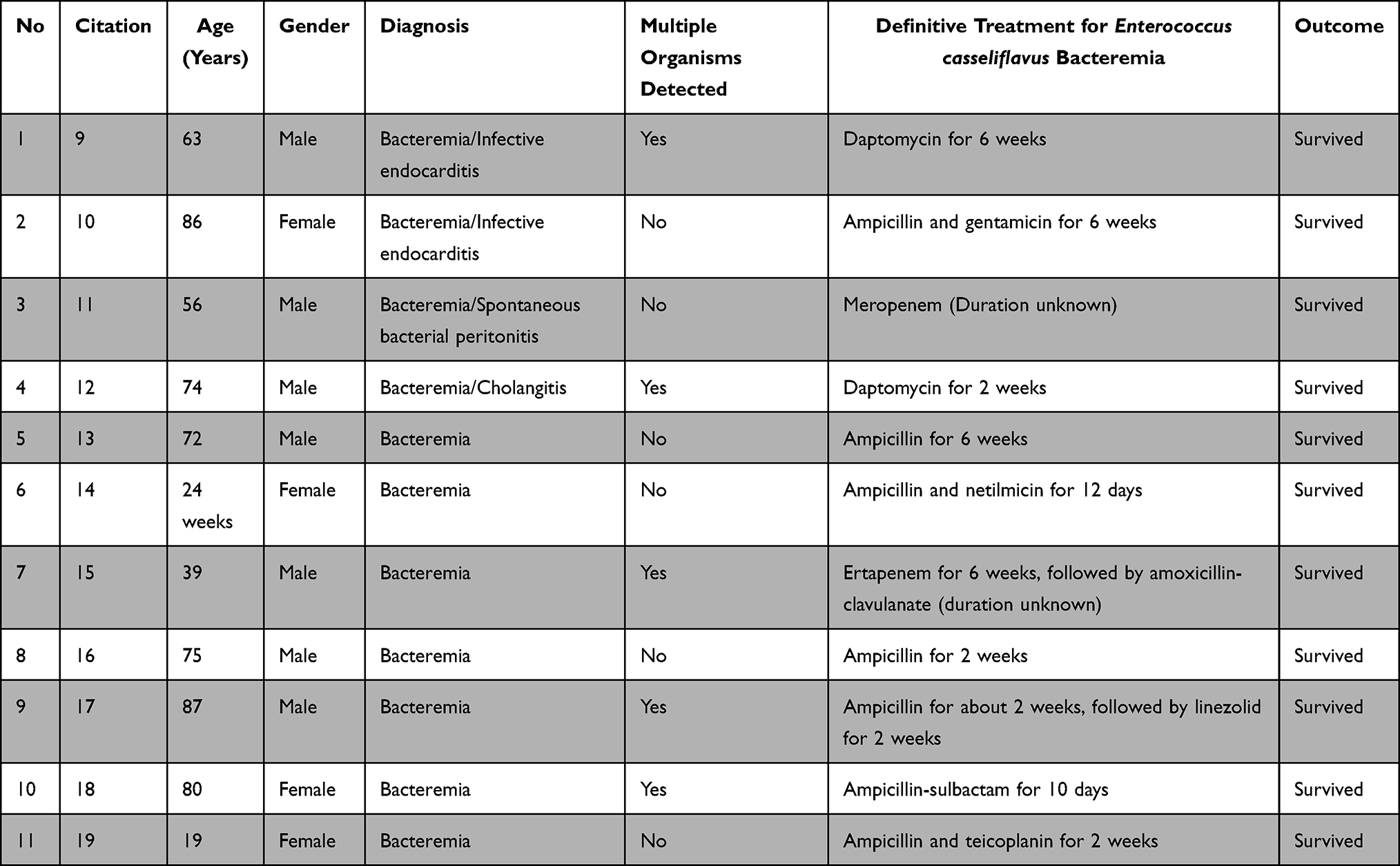 |
Table 1 Summary of the Treatment Courses for All Reported Bacteremia Cases |
The most important organs related to E. casseliflavus bacteremia are the biliary tract and liver. Infective endocarditis was the primary infection site in two cases,9,10 and cholangitis was reported as the primary infection site in one case.12 A retrospective cohort study of biliary infections with bacteremia found that E. casseliflavus constituted 12.5% of the Gram-positive bacteremia.20 Three of the eleven patients had biliary tract infections prior to the onset of E. casseliflavus bacteremia.16,18,19 In one case, surgery of the biliary system had been performed before the onset of E. casseliflavus bacteremia.15 A retrospective cohort study of post-liver transplant cases found 7.8% of the patients to be infected with enterococcal bacteremia.21 These results suggest that this microbe has a high affinity for the biliary system.
E. casseliflavus carries the VanC gene intrinsically and is moderately resistant to vancomycin (VCM).32 Owing to this moderate resistance, the Clinical and Laboratory Standards Institute (CLSI) considers VCM concentrations below 4 mg/dL to be susceptible for Enterococcus species; therefore, the drug is not actively recommended in E. casseliflavus bacteremia treatment.33 Indeed, a VCM minimum inhibitory concentration (MIC) of 4 mg/dL in three cases, 8 mg/dL in one case, and 3 mg/dL in two cases, were demonstrated.10,13,14,16,18,19 It is important to note that even if microbiological tests show that this microorganism is susceptible to VCM, the actual therapeutic effect of VCM is likely to be low. In the case reports reviewed, all 11 patients were treated with antimicrobial agents other than VCM and survived. While five patients were treated with ampicillin-sulbactam or carbapenem from the beginning, five patients had been switched from VCM to ampicillin, and one patient had been switched from VCM to daptomycin, which had a favorable sensitivity result.9,10,13,14,16,17 Some retrospective cohort studies report E. casseliflavus to be 79.5–100% sensitive to VCM, while others report VCM MICs as high as 4 mg/dL.26–28 However, ampicillin was reported to have a 96% success rate against E. casseliflavus in a summary of 41 cases, indicating that this drug is a viable treatment option.30
Of the 11 case reports reviewed, five presented with bacteremia caused by E. casseliflavus and other organisms.9,12,15,17,18 Cohort studies reported a high proportion (41.5–66.1%) of E. casseliflavus bacteremia cases with multiple bacterial species present, primarily other Gram-negative Enterobacteriaceae.27,28,30 This feature is probably specific to E. casseliflavus bacteremia. Although all reported cases demonstrated favorable outcomes, E. casseliflavus bacteremia is typically accompanied by multiple bacterial species and consequently might have a poor prognosis.22,25 The mortality rates have been reported as 24.4–24.8% for enterococcal bacteremia, 27.3–28.7% for non-faecalis non-faecium bacteremia, and 12.8–25.0% for E. casseliflavus bacteremia.22,23,27–30 However, the mortality rate of E. casseliflavus bacteremia has only been reported in a small number of studies and it is not clear whether there is any difference in prognosis compared to other enterococci. Either way, enterococcal bacteremia, including that caused by E. casseliflavus, is associated with an overall poor prognosis.
Based on these results, when E. casseliflavus is identified by blood culture, the biliary system should be evaluated, the antimicrobial susceptibility of the organism should be confirmed, and an effective antimicrobial agent other than VCM, such as ampicillin, should be administered promptly. Particularly, if multiple organisms are identified, attention should be paid to the choice of antimicrobial agents and the treatment course. In several reports summarizing enterococcal bacteremia due to nosocomial infections, risk factors for poor prognosis included catheter-related bloodstream infections, steroid-associated immunosuppression, severe illness at onset, and advanced age. These factors may also require evaluation at the time of diagnosis.22–24,27
Endophthalmitis
Endophthalmitis is the second most frequently reported type of E. casseliflavus infection. Six reports of endophthalmitis caused by E. casseliflavus and one retrospective cohort study were reviewed.34–40 In the cohort study, 14 (48.3%) of 29 cases of enterococcal endophthalmitis were attributed to this organism, suggesting that intraocular tissues were particularly susceptible to E. casseliflavus.40 The case reports showed that most of the cases were traumatic endophthalmitis, with a wide range of trauma types, including attacks from domestic animals, such as pigs and horses, water gunshot wounds, among others.34,36–39 A farm-related component was identified in three of six cases, such as trauma related to lawnmowers and attacks from livestock. Therefore, in farm injury-based endophthalmitis, it is necessary to consider the possibility that this microorganism is the causative agent.34,38,39 No specific risk factors for infection were identified in these cases. Endophthalmitis caused by E. casseliflavus occurs in a wide age range (4–54); the incidence seems to be higher among active young and middle-aged individuals.
In five of the six cases, vitreoretinal surgery was performed, followed by intraocular administration of VCM/ceftazidime and steroids, followed by other more effective antimicrobial agents after the strain was identified. One patient initially refused vitreoretinal surgery, with the surgery being finally performed after the disease worsened. This suggests that endophthalmitis caused by E. casseliflavus requires vitreoretinal surgery.39
VCM is routinely administered intraocularly for endophthalmitis; however, if the organism is identified, additional measures, such as systemic or intraocular administration of an appropriate antimicrobial agent may be required. One cohort study showed that as an endophthalmitis pathogen, E. casseliflavus was resistant to new quinolones, including 64.3% resistance to ciprofloxacin and 100% resistance to VCM. Administration of systemic ampicillin was required as treatment in two cases and systemic linezolid in one case after intraocular administration of VCM and ceftazidime.36–38 As noted previously, E. casseliflavus possesses an intrinsic VanC gene; therefore, VCM should not be used as a therapeutic agent for endophthalmitis caused by this species. Furthermore, three of the six patients underwent reoperation for vitreoretinal extraction, indicating the need for appropriate postoperative follow-up.34,35,38 Although proposing an appropriate treatment is challenging due to the paucity of case reports, the optimal approach for managing E. casseliflavus-caused endophthalmitis seems to be through vitreoretinal surgery, systemic administration of the suitable antimicrobial (eg, ampicillin) based on antimicrobial susceptibility testing, and adequate postoperative follow-up.
Others
As mentioned previously, two bacteremia cases also resulted in infective endocarditis.9,10 Although chronic kidney disease (CKD) was common to both cases and other risks such as age and being immunosuppressed were apparent, no clear common risk was identified. Vegetation was observed on the aortic valve in both cases. In both cases, the causative microorganism was assumed to be resistant to VCM, although MIC of VCM was 4 mg/dL in one report and that of VCM was unknown in the other report. Both cases resulted in recovery; one case was treated with daptomycin based on the susceptibility results and the other was treated with ampicillin. These two cases suggest that this organism, although rare, may be a causative agent of infective endocarditis.
Two cases of infectious meningitis have also been reported.41,42 No similarities in background diseases or causes were observed. Moreover, VCM resistance was observed in both cases; one patient was treated with linezolid and the other with meropenem and ampicillin-sulbactam, both resulting in full recovery.
Two cases of peritonitis were also reviewed.11,43 One patient had spontaneous bacterial peritonitis associated with alcoholic cirrhosis and ascites, and the other had peritonitis associated with peritoneal dialysis. E. casseliflavus can colonize the intestine and cause peritonitis. Finally, one case report was found of empyema caused by E. casseliflavus in association with a chronic expanding hematoma, but the details were not clear in this case.43
Conclusion
This review clarified that E. casseliflavus can be a causative microorganism in various infections, including bacteremia and endophthalmitis. A review of cases also revealed that the bacterium intrinsically possesses the VanC gene and can be mildly to moderately resistant to VCM, highlighting the importance of selecting appropriate antimicrobial agents. In most cases, the organism demonstrated sensitivity to ampicillin, which has been recommended as one of the most suitable antimicrobial agents for E. casseliflavus infections.
Acknowledgments
I would like to thank Editage for English language editing.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Yuen GJ, Ausubel FM. Enterococcus infection biology: lessons from invertebrate host models. J Microbiol. 2014;52(3):200–210. doi:10.1007/s12275-014-4011-6
2. Pasquaroli S, Di Cesare A, Vignaroli C, Conti G, Citterio B, Biavasco F. Erythromycin- and copper-resistant Enterococcus hirae from marine sediment and co-transfer of erm(B) and tcrB to human Enterococcus faecalis. Diagn Microbiol Infect Dis. 2014;80(1):26–28. doi:10.1016/j.diagmicrobio.2014.06.002
3. Kuch A, Willems RJ, Werner G, et al. Insight into antimicrobial susceptibility and population structure of contemporary human Enterococcus faecalis isolates from Europe. J Antimicrob Chemother. 2012;67(3):551–558. doi:10.1093/jac/dkr544
4. Palmer KL, Godfrey P, Griggs A, et al. Comparative genomics of enterococci: variation in Enterococcus faecalis, clade structure in E faecium, and defining characteristics of E gallinarum and E. casseliflavus. mBio. 2012;3(1):e00318–e00311. doi:10.1128/mBio.00318-11
5. Facklam RR, Collins MD. Identification of Enterococcus species isolated from human infections by a conventional test scheme. J Clin Microbiol. 1989;27(4):731–734. doi:10.1128/jcm.27.4.731-734.1989
6. Liu Y, Wang Y, Dai L, Wu C, Shen J. First report of multiresistance gene cfr in Enterococcus species casseliflavus and gallinarum of swine origin. Vet Microbiol. 2014;170(3–4):352–357. doi:10.1016/j.vetmic.2014.02.037
7. Liu Y, Liu K, Lai J, Wu C, Shen J, Wang Y. Prevalence and antimicrobial resistance of Enterococcus species of food animal origin from Beijing and Shandong Province, China. J Appl Microbiol. 2013;114(2):555–563. doi:10.1111/jam.12054
8. Abamecha A, Wondafrash B, Abdissa A. Antimicrobial resistance profile of Enterococcus species isolated from intestinal tracts of hospitalized patients in Jimma, Ethiopia. BMC Res Notes. 2015;8:213. doi:10.1186/s13104-015-1200-2
9. Motie I, Burns K, Thompson R, et al. Acinetobacter radioresistens and Enterococcus casseliflavus co-infection with endocarditis, bacteremia, and pneumonia. IDCases. 2022;30:e01622. doi:10.1016/j.idcr.2022.e01622
10. Okumura N, Watanabe T, Teranishi S, et al. Successful treatment of aortic valve endocarditis caused by Enterococcus casseliflavus: a case report. BMC Infect Dis. 2021;21(1):447. doi:10.1186/s12879-021-06160-1
11. Narciso-Schiavon JL, Borgonovo A, Marques PC, et al. Enterococcus casseliflavus and Enterococcus gallinarum as causative agents of spontaneous bacterial peritonitis. Ann Hepatol. 2015;14(2):270–272. doi:10.1016/S1665-2681(19)30791-4
12. Prasad V, Barouni B, Khiatah B, Saeed M, Rare A. Case of Raoultella planticola and Enterococcus casseliflavus coinfection. Case Rep Infect Dis. 2022;2022:3377331. doi:10.1155/2022/3377331
13. Vasilakopoulou A, Vourli S, Siafakas N, Kavatha D, Tziolos N, Pournaras S. Enterococcus casseliflavus bacteraemia in a patient with chronic renal disease. Infect Dis Rep. 2020;12(3):70–73. doi:10.3390/idr12030015
14. Ruess M, Sander A, Hentschel R, Berner R. Enterococcus casseliflavus septicaemia in a preterm neonate. Scand J Infect Dis. 2002;34(6):471–472. doi:10.1080/003655402320170327
15. Heda RP, Savage Y, Nair SP, Verma R. Enterococcus casseliflavus, Streptococcus equinus and Klebsiella oxytoca septicaemia associated with perinephric haematoma in a post-liver transplant patient with allograft cirrhosis. BMJ Case Rep. 2019;12:8. doi:10.1136/bcr-2019-230096
16. Verma R, Baroco AL. Enterococcus casseliflavus septicaemia associated with hepatobiliary infection in a 75-year-old man. BMJ Case Rep. 2017;2017. doi:10.1136/bcr-2017-219636
17. Saumya B, Abhijeet Y, Nagpal S, Sartor O. An unusual case of sepsis with both Vibrio vulnificus and Enterococcus casseliflavus. J La State Med Soc. 2010;162(3):153–154.
18. Pappas G, Liberopoulos E, Tsianos E, Elisaf M. Enterococcus casseliflavus bacteremia. Case report and literature review. J Infect. 2004;48(2):206–208. doi:10.1016/j.jinf.2003.08.001
19. Van Goethem GF, Louwagie BM, Simoens MJ, Vandeven JM, Verhaegen JL, Boogaerts MA. Enterococcus casseliflavus septicaemia in a patient with acute myeloid leukaemia. Eur J Clin Microbiol Infect Dis. 1994;13(6):519–520. doi:10.1007/BF01974649
20. Jo IH, Kim YJ, Chung WC, et al. Microbiology and risk factors for gram-positive Cocci bacteremia in biliary infections. Hepatobiliary Pancreat Dis Int. 2020;19(5):461–466. doi:10.1016/j.hbpd.2020.05.006
21. Kim YJ, Jun YH, Choi HJ, et al. Impact of enterococcal bacteremia in liver transplant recipients. Transplant Proc. 2019;51(8):2766–2770. doi:10.1016/j.transproceed.2019.02.064
22. Falcone M, Tiseo G, Dentali F, et al. Early alert from the microbiology laboratory improves the outcome of elderly patients with Enterococcus spp bloodstream infection: results from a multicentre prospective study. J Glob Antimicrob Resist. 2019;18:139–144. doi:10.1016/j.jgar.2019.02.014
23. Suzuki H, Hase R, Otsuka Y, Hosokawa N. A 10-year profile of enterococcal bloodstream infections at a tertiary-care hospital in Japan. J Infect Chemother. 2017;23(6):390–393. doi:10.1016/j.jiac.2017.03.009
24. Zheng JX, Li H, Pu ZY, et al. Bloodstream infections caused by Enterococcus spp: a 10-year retrospective analysis at a tertiary hospital in China. J Huazhong Univ Sci Technol Med Sci. 2017;37(2):257–263. doi:10.1007/s11596-017-1725-9
25. Britt NS, Potter EM. Clinical epidemiology of vancomycin-resistant Enterococcus gallinarum and Enterococcus casseliflavus bloodstream infections. J Glob Antimicrob Resist. 2016;5:57–61. doi:10.1016/j.jgar.2015.12.002
26. Jain S, Kumar A, Kashyap B, Kaur IR. Clinico-epidemiological profile and high-level aminoglycoside resistance in enterococcal septicemia from a tertiary care hospital in east Delhi. Int J Appl Basic Med Res. 2011;1(2):80–83. doi:10.4103/2229-516X.91149
27. Tan CK, Lai CC, Wang JY, et al. Bacteremia caused by non-faecalis and non-faecium enterococcus species at a Medical center in Taiwan, 2000 to 2008. J Infect. 2010;61(1):34–43. doi:10.1016/j.jinf.2010.04.007
28. Koganemaru H, Hitomi S. Bacteremia caused by VanC-type enterococci in a university hospital in Japan: a 6-year survey. J Infect Chemother. 2008;14(6):413–417. doi:10.1007/s10156-008-0644-x
29. de Perio MA, Yarnold PR, Warren J, Noskin GA. Risk factors and outcomes associated with non-Enterococcus faecalis, non-Enterococcus faecium enterococcal bacteremia. Infect Control Hosp Epidemiol. 2006;27(1):28–33. doi:10.1086/500000
30. Choi SH, Lee SO, Kim TH, et al. Clinical features and outcomes of bacteremia caused by Enterococcus casseliflavus and Enterococcus gallinarum: analysis of 56 cases. Clin Infect Dis. 2004;38(1):53–61. doi:10.1086/380452
31. Reid KC, Cockerill IF, Patel R. Clinical and epidemiological features of Enterococcus casseliflavus/flavescens and Enterococcus gallinarum bacteremia: a report of 20 cases. Clin Infect Dis off Publ Infect Dis Soc Am. 2001;32(11):1540–1546. doi:10.1086/320542
32. Navarro F, Courvalin P. Analysis of genes encoding D-alanine–D-alanine ligase-related enzymes in Enterococcus casseliflavus and Enterococcus flavescens. Antimicrob Agents Chemother. 1994;38(8):1788–1793. doi:10.1128/AAC.38.8.1788
33. CLSI supplement M100. Clinical and laboratory standards institute; 2018.
34. Khurana RN, Leder HA, Nguyen QD, Do DV. Enterococcus casseliflavus endophthalmitis associated with a horse tail injury. Arch Ophthalmol. 2009;127(11):1551–1552. doi:10.1001/archophthalmol.2009.282
35. Sambhav K, Mathai A, Reddy AK, Reddy BV, Bhatia K, Balne PK. Endogenous endophthalmitis caused by Enterococcus casseliflavus. J Med Microbiol. 2011;60(5):670–672. doi:10.1099/jmm.0.016675-0
36. Low JR, Teoh CS, Chien JM, Huang EH. Enterococcus casseliflavus endophthalmitis due to metallic intraocular foreign body. Eye. 2015;29(6):840–841. doi:10.1038/eye.2014.332
37. Berenger BM, Kulkarni S, Hinz BJ, Forgie SE. Exogenous endophthalmitis caused by Enterococcus casseliflavus: a case report and discussion regarding treatment of intraocular infection with vancomycin-resistant enterococci. Can J Infect Dis Med Microbiol. 2015;26(6):330–332. doi:10.1155/2015/784910
38. Nguyen J, Hartnett ME. Successful management of post-traumatic vancomycin-resistant enterococcus endophthalmitis. Am J Ophthalmol Case Rep. 2017;5:117–118. doi:10.1016/j.ajoc.2016.12.022
39. Bao QD, Liu TX, Xie M, Tian X. Exogenous endophthalmitis caused by Enterococcus casseliflavus: a case report. World J Clin Cases. 2019;7(22):3904–3911. doi:10.12998/wjcc.v7.i22.3904
40. Dave VP, Pathengay A, Braimah IZ, et al. ENTEROCOCCUS endophthalmitis: clinical settings, antimicrobial susceptibility, and management outcomes. Retina. 2020;40(5):898–902. doi:10.1097/IAE.0000000000002462
41. Li MC, Guo HC, Chen G, Kong F, Zhang QH. Meningitis caused by Enterococcus casseliflavus with refractory cerebrospinal fluid leakage following endoscopic endonasal removal of skull base chondrosarcoma. Chin Med J. 2011;124(20):3440.
42. Iaria C, Stassi G, Costa GB, Di Leo R, Toscano A, Cascio A. Enterococcal meningitis caused by Enterococcus casseliflavus. First case report. BMC Infect Dis. 2005;5(1):3. doi:10.1186/1471-2334-5-3.
43. Nzana VB, Rohit A, George D, et al. Twenty-one episodes of peritonitis in a continuous ambulatory peritoneal dialysis patient: what is the root cause? Indian J Med Microbiol. 2018;36(2):282–284. doi:10.4103/ijmm.IJMM_18_225
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.