Back to Journals » Nursing: Research and Reviews » Volume 15
Enhancing Surgical Precision Through Awareness: An Assessment of Nurses’ Adherence to WHO Surgical Safety Guidelines in the Operating Rooms
Authors Elmansy FM ![]() , Elbqry MG
, Elbqry MG ![]() , Qalawa SAA
, Qalawa SAA ![]() , Elgazzar SE
, Elgazzar SE ![]() , Ashmieg FSO
, Ashmieg FSO ![]() , Abdelbaqi HSM
, Abdelbaqi HSM
Received 18 July 2025
Accepted for publication 4 November 2025
Published 15 November 2025 Volume 2025:15 Pages 193—204
DOI https://doi.org/10.2147/NRR.S554660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ferry Efendi
Fatma Mohamed Elmansy,1 Mohamed Goda Elbqry,1 Shereen Ahmed A Qalawa,1 Samia Eaid Elgazzar,1 Fatima SO Ashmieg,1 Hebah Said M Abdelbaqi2
1Department of Medical and Surgical, College of Nursing, Qassim University, Buraydah City, Saudi Arabia; 2Department of Operating Room, Medical City, Qassim University, Buraydah City, Saudi Arabia
Correspondence: Fatma Mohamed Elmansy, Department of Medical and Surgical, College of Nursing, Qassim University, P.O. Box: 52571, Buraydah, Saudi Arabia, Tel +966542235580, Email [email protected]
Background: Ensuring surgical safety is a global healthcare priority, with the World Health Organization (WHO) introducing the Surgical Safety Checklist to reduce errors and improve patient outcomes. Nurses play a critical role in implementing these guidelines, particularly in the operating theatre. However, their level of awareness and adherence to such protocols remains researchable.
Aim: To evaluate the level of awareness, understanding, and engagement of nurses with the World Health Organization’s Surgical Safety Guidelines in the operating theatre at Qassim University Medical City.
Methods: A cross-sectional survey of 66 conveniently selected nurses was conducted between February and May 2024 using a validated and reliable online tool.
Results: The majority of nurses had received prior training (93.9%) and reported the presence of the WHO Surgical Safety Checklist in their workplace (97%). Nearly half demonstrated good knowledge (45%) and adequate practice (39.2%) levels. A significant positive correlation (r = 0.58, p < 0.05) was found between knowledge and practice, with gender, experience, education, and work setting showing significant associations.
Conclusion: This study highlights that while nurses demonstrate high awareness and training regarding WHO Surgical Safety Guidelines, their practical adherence remains moderate, underscoring the need for continuous institutional support and targeted improvement strategies. Continuous training, targeted interventions, and supportive work environments are essential to enhance compliance and ensure safer surgical outcomes.
Keywords: nurses, patient safety, perioperative care, safety management
Introduction
Surgical safety remains a critical concern globally due to the significant risk of adverse events during operative procedures. According to the World Health Organization (WHO), surgical complications contribute substantially to morbidity and mortality worldwide, particularly in low- and middle-income countries where healthcare resources are limited. In response, the WHO developed the Surgical Safety Checklist in 2008 to standardize safety practices and reduce preventable surgical errors, including wrong-site surgery, retained surgical items, and anesthesia complications.1 Estimates indicate that major surgeries in developing nations have a mortality rate of 5–10%, with approximately 7 million patients experiencing major complications annually, resulting in 1 million deaths during or immediately following surgery—nearly half of which could be prevented.2 Implementation of the checklist has been shown to improve patient outcomes by fostering teamwork and communication among surgical teams, thereby enhancing the overall safety culture in operating theaters. Moreover, checklist use has been associated with reductions in mortality from 1.5% to 0.8% and in serious complications from 11% to 7%.1,2 Despite widespread endorsement, studies reveal variability in adoption and adherence across healthcare settings and professional groups, including nurses, who play a pivotal role in perioperative care.3
In the Kingdom of Saudi Arabia (KSA), rapid advancements in healthcare infrastructure and increasing surgical volumes have underscored the need to maintain high safety standards in operative environments. The Ministry of Health and other healthcare organizations have promoted quality improvement initiatives, including the integration of WHO surgical safety protocols to enhance patient outcomes.4 Nevertheless, evidence from recent regional studies indicates inconsistencies in knowledge, awareness, and compliance with the WHO checklist among healthcare professionals, particularly nursing staff in operating rooms.5 Nurses’ engagement with safety protocols is crucial, as they are responsible for multiple essential roles during surgery, including patient preparation, monitoring, and intraoperative communication.6 Addressing gaps in nurse awareness and practice regarding WHO safety measures is therefore fundamental to improving surgical safety culture and reducing preventable surgical complications in KSA healthcare facilities.7
Although several international studies have examined WHO Surgical Safety Checklist implementation, few have specifically evaluated nurses’ individual adherence behaviors, attitudes, and the contextual factors influencing checklist compliance within Saudi Arabia. For instance, Alsadun et al (2021) assessed operating room staff perceptions in Riyadh over time, demonstrating improved awareness of the checklist and patient safety culture.8 Alrasheadi et al (2022) surveyed nurses in medical-surgical units in the Qassim region regarding general safety culture but did not analyze checklist adherence in the operating theatre.9 Rawas and Abou Hashish (2023) explored predictors of nurses’ safety culture in Jeddah, highlighting leadership, communication, and error reporting, but without detailed investigation of checklist adherence.10 International studies similarly identify facilitators and barriers—such as workload, training, leadership, and institutional support—that influence how nurses comply with the checklist.11,12 These gaps suggest that, while safety culture and awareness have been studied, there is limited evidence on how nurses in a Saudi academic tertiary hospital perceive, engage with, and adhere to the WHO Surgical Safety Checklist in daily practice. This study is therefore novel focusing on nurses’ awareness, attitudes, and checklist adherence at Qassim University Medical City, providing context-specific insights to inform training, policy, and safety culture improvements both nationally and internationally.
Nurses are central to surgical safety implementation, as they oversee patient preparation, intraoperative coordination, monitoring, and documentation throughout surgery.13,14 Their adherence to the WHO Surgical Safety Checklist is critical to ensure that each safety step is completed accurately and communicated effectively among the multidisciplinary team. Investigating nurses’ adherence within the context of Qassim University Medical City, a tertiary academic hospital integrating clinical service, education, and training is particularly important, as these factors may uniquely influence safety behaviors and compliance culture. Understanding how nurses in this environment perceive and apply surgical safety protocols provides valuable insight into the interaction between educational settings and clinical practice.15 Furthermore, examining these dynamics contributes to the broader body of knowledge by generating context-specific evidence that can inform national and international strategies to enhance surgical safety culture, guide the development of tailored educational interventions, and support Saudi Arabia’s Vision 2030 objectives for healthcare quality and patient safety.
Methods
Study Design and Setting
This study employed a descriptive design conducted from February to April 2024 to evaluate the level of awareness, understanding, and engagement of nurses with the World Health Organization’s Surgical Safety Guidelines in the operating theatre at Qassim University Medical City.
The Study Population
The study targeted registered nurses working in the operating theatre at Qassim University Medical City. A purposive sampling method was used to select 66 nurses who agreed to take part during the data collection phase. Both male and female registered nurses Saudi Commission for Health Sciences, at least six months of experience and who were willing to participate by providing informed consent were included. Nursing interns, students, and nurses who were on leave or otherwise unavailable during the study period were excluded. The required sample size was estimated using the single population proportion formula, assuming a 50% prevalence of adequate adherence to the WHO Surgical Safety Checklist (to maximize sample size), a 95% confidence level, and a 10% margin of error. Although the calculation yielded a sample size of 96, a total of 66 nurses were recruited due to the limited number of eligible staff in the operating theatre, representing the majority of the accessible population. This sample size provides sufficient power to detect meaningful trends in nurses’ awareness, attitudes, and adherence to surgical safety protocols within this setting. This size is sufficient for descriptive analysis, though statistical power for subgroup comparisons may be limited.
Data Collection
A self-administered online survey was developed and distributed to participants via their official QUMC Email addresses. The questionnaire, available in both Arabic and English, was adapted by the researcher from validated instruments found in relevant previous studies,15–17 ensuring clarity and comprehensiveness regarding awareness, understanding, and engagement of nurses with the World Health Organization’s Surgical Safety Guidelines in the operating theatre at Qassim University Medical City. The survey comprised three parts. The first section consisted of a demographic data sheet comprising seven items designed to assess the nurses’ demographic characteristics, including age, gender, marital status, educational background, years of experience, operating room specialty, and the availability of surgical safety guidelines. The second section was a 15-item knowledge assessment sheet aimed at evaluating nurses’ understanding of the World Health Organization (WHO) surgical safety measures during intraoperative care. The items addressed key aspects such as the definition, components, significance, and influencing factors of surgical safety protocols. The scoring system was used to evaluate the nurses’ level of knowledge regarding WHO surgical safety measures. Each correct response was awarded one point, with a total possible score of 15. The final score was converted into a percentage. A score of less than 75% was considered indicative of unsatisfactory knowledge, while a score of 75% or higher was deemed satisfactory. These thresholds were adapted from WHO guidelines on surgical safety practices and supported by prior studies assessing nurses’ knowledge and adherence to surgical safety protocols.2,4
The third part of the tool was the WHO Surgical Safety Checklist, which was utilized to assess nurses’ adherence to intraoperative surgical safety protocols. This checklist is a standardized instrument that facilitates the observation of safety practices during three critical stages of surgical procedure. To ensure inter-rater reliability, two trained observers independently assessed a subset of surgical procedures, and agreement between observers was measured using Cohen’s kappa. Any discrepancies were discussed and resolved through consensus before final data entry, ensuring consistency and reproducibility of the observational findings. It is twenty-two items divided to the first section, “Before Induction of Anesthesia”, including seven items related to patient identity verification, anesthesia equipment checks, and assessment of patient-specific risks. The second section, “Before Skin Incision”, consists of ten items covering team introductions, discussion of anticipated critical events, and confirmation of necessary prophylactic interventions. The final section, “Before the Patient Leaves the Operating Room”, comprises five items focusing on the verification of instrument, sponge, and needle counts, proper labeling of surgical specimens, and discussion of key recovery concerns. This checklist served as a reliable measure of compliance with internationally recognized surgical safety standards. The scoring system for the WHO Surgical Safety Checklist was designed to evaluate the level of nurses’ adherence to intraoperative safety practices. Each item on the checklist was scored as either “done” (1 point) or “not done” (0 points). The total score was calculated by summing the points across all 22 items. The total adherence score was then converted into a percentage. A score > 75% was higher was classified as adequate adherence, indicating satisfactory compliance with WHO surgical safety measures, while from 51–75 was neutral adherence. In contrast, a score of less than <50% was considered non-adequate adherence, reflecting suboptimal compliance. This classification was adapted from WHO guidelines and supported by similar research in surgical safety compliance.1–7
To ensure the validity of the survey, the questionnaire was reviewed by a panel of five experts in perioperative nursing and patient safety, who assessed the content for clarity, relevance, and comprehensiveness. Items were modified based on their feedback to ensure that all aspects of nurses’ awareness, knowledge, and adherence to WHO surgical safety protocols were adequately captured. The instrument was also pilot-tested with a small group of six operating theatre nurses who were not part of the main study sample, to confirm readability, clarity, and the time required for completion. Regarding reliability, internal consistency was evaluated using Cronbach’s alpha, which yielded values of 0.82 for the knowledge assessment section and 0.87 for the WHO Surgical Safety Checklist adherence section, indicating good reliability. These steps ensured that the survey provided consistent, accurate, and meaningful measurements of nurses’ knowledge and adherence to surgical safety standards.
Data Collection Protocol
Approval of conducting the study was obtained by submitting all relevant documents to the Ethics Committee and the Head of the Research Department at Qassim University. Once permission was granted, the adopted instruments were subjected to expert review to ensure validity and were pilot tested to confirm their reliability within the local context. Official letters were then prepared, clearly stating the purpose of the study and the ethical considerations and were submitted to the Director of the Medical City at Qassim University in the Qassim region to initiate data collection. Data were collected using a validated and confidential online questionnaire, developed in both English and Arabic to ensure cultural appropriateness. Nurses’ practices related to surgical safety measures were observed directly without informing the participants in advance, to preserve the objectivity and authenticity of the observations. The validity and reliability of the tools were confirmed. Informed consent was obtained from all participating nurses, and confidentiality and privacy were strictly maintained throughout the study.
Once approval was secured, the researchers coordinated with area supervisors to schedule appropriate times and dates for data collection. During these scheduled periods, the researchers met with the nurses, explained the study objectives in simple terms, and provided access to the online survey link. In accordance with institutional policies and protocols, efforts were made to maximize participation. The survey, created using Microsoft Forms through there official Email QUMC, was designed to be completed within 4–7 minutes. To enhance accessibility, the link was shared electronically, allowing participants to complete it at a time and place convenient for them. In parallel, the observational checklist was also developed using Microsoft Forms and was used to evaluate whether each step of surgical safety practice was completed or not, within an average observation time of 3–5 minutes per nurse. After completion of both the questionnaire and the observation, data collection tools were coded and securely stored in sealed envelopes in preparation for data entry into SPSS for statistical analysis. Participants were reminded of their right to withdraw at any time without penalty, and their anonymity and confidentiality were fully protected. Verbal consent was accepted, and no incentives or consequences were associated with participation.
Statistical Analysis
Data were analyzed using SPSS version 20.0 (IBM Corp, 2011). Continuous variables met assumptions of normality (Shapiro–Wilk test) and homogeneity of variance (Levene’s test), allowing the use of parametric tests. Descriptive statistics summarized demographics and survey responses, with knowledge and adherence scores classified using a 75% cutoff. Chi-square tests examined associations between categorical variables, t-tests compared two groups, ANOVA compared multiple groups, and Pearson’s correlation assessed relationships between continuous variables. A p-value < 0.05 indicated statistical significance.
Results
Results are Presented in Table 1
Table 1 displays that the majority of participants were non-Saudi nationals (83.3%), with a smaller proportion of Saudi students (16.7%). Most students were within the 29–38 age group (66.7%), with a mean age of 24.5 years (SD = 2.28). In terms of gender, females represented the larger proportion (66.7%), compared to males (24.2%). Regarding marital status, nearly 69.7% were married. For the working place, over half of the students (56%) were working in surgical wards, while 44% were in the operating room. The vast majority held a bachelor’s degree (83.4%), with only (9.1%) having postgraduate qualifications. Regarding work experience, most students had between 5 to 9 years of experience (42.4%), followed by those with 10 or more years (39.4%), and (18.2%) with less than 5 years.
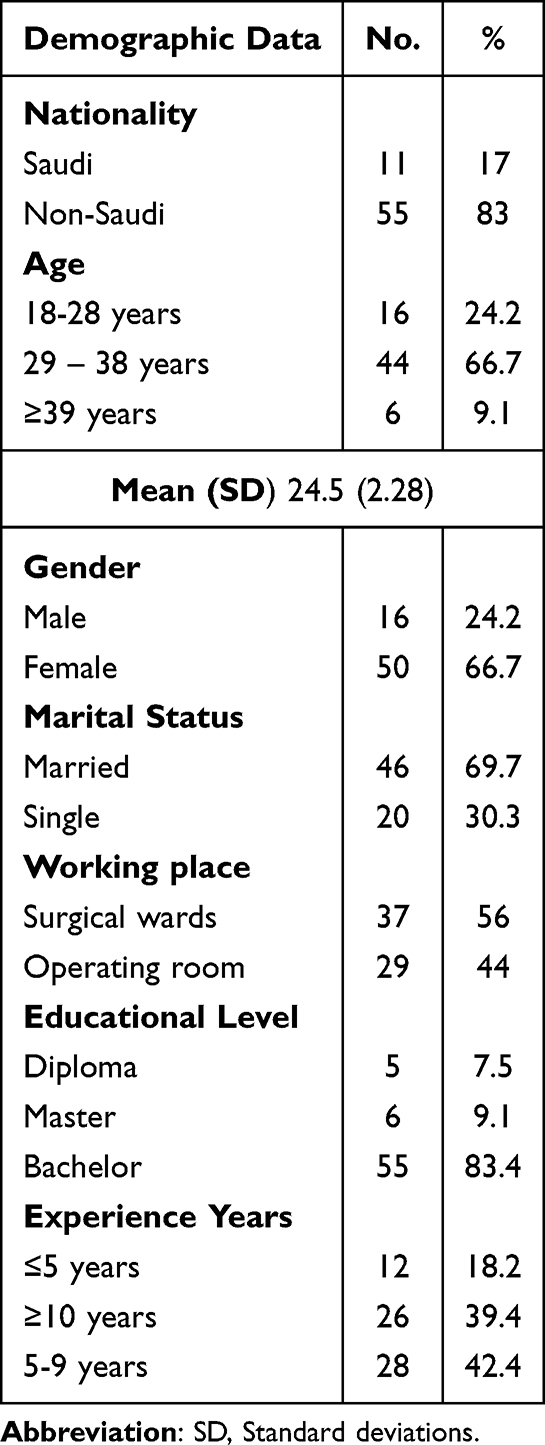 |
Table 1 The Studied Students’ Demographic Data. (n = 66) |
As shown in Figure 1, 45% of the nurses demonstrated good knowledge of the WHO Surgical Safety Guidelines, while 36% had a moderate level of knowledge, and only 19% exhibited poor knowledge.
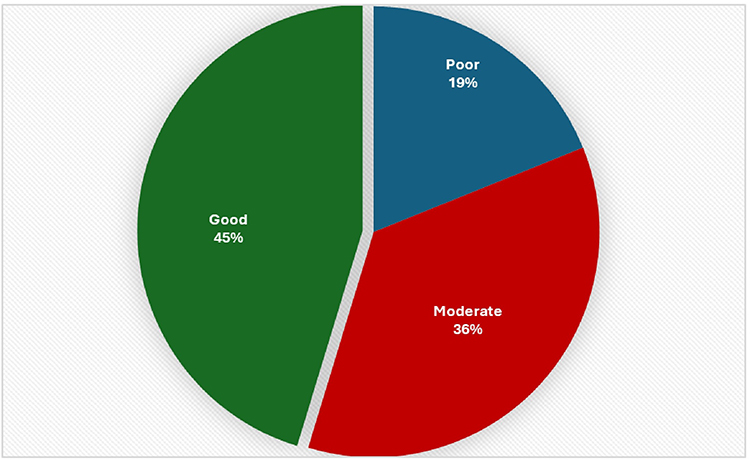 |
Figure 1 Knowledge level of the studied nurses toward WHO surgical safety guidelines in the operating theatre. (n= 66). |
Table 2 presents the correlation between the knowledge and practice levels of the studied nurses regarding WHO surgical safety guidelines. The results show a moderate positive correlation between knowledge and practice, with a Pearson correlation coefficient (r) of 0.58, which is statistically significant (p < 0.05). This finding suggests that higher levels of knowledge among nurses are associated with better adherence to safe surgical practices.
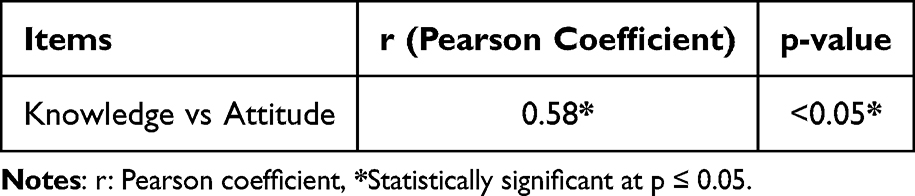 |
Table 2 Correlation Between Knowledge vs Practice’s Level of the Studied Nurses. (n = 66) |
Table 3 revealed that several demographic factors were significantly associated with nurses’ knowledge and practice scores. Gender showed a notable difference, with female nurses scoring significantly higher than males in both knowledge and practice (p = 0.01 and 0.02, respectively). Similarly, years of experience were significantly linked to performance, with nurses having 5–9 years of experience achieving the highest scores in both domains (p = 0.01 and 0.05). Educational level also had a significant impact (p = 0.01), with bachelor’s degree holders demonstrating superior practice scores. Furthermore, the working place influenced outcomes, as nurses in surgical wards scored significantly higher in knowledge and practice than those in operating rooms (p = 0.01 and 0.05). In contrast, nationality and age did not show statistically significant associations with knowledge or practice levels (p > 0.05). These findings suggest that professional background and work environment play a more influential role than personal demographics in shaping nurses’ knowledge and practice.
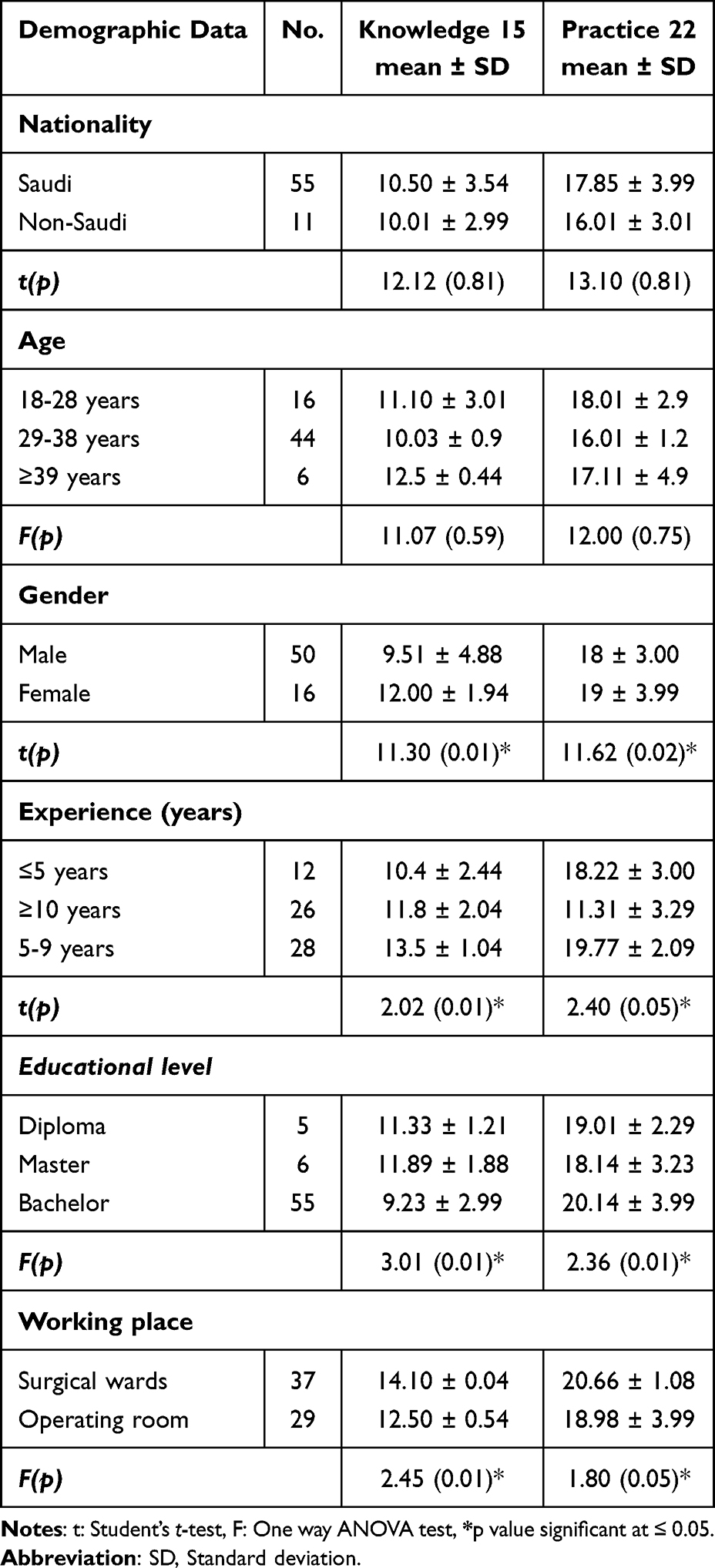 |
Table 3 Relation Between Total Knowledge and Practice Score of the Studied Nurses with Demographic Data. (n = 66) |
Discussion
The demographic profile of participants (Table 1) in this study indicates that the majority were non-Saudi nationals (83.3%), predominantly female (66.7%), and aged between 29–38 years, with most holding a bachelor’s degree and possessing moderate to extensive work experience. These findings align with those of Alrasheadi et al, who reported that the majority of surgical nurses in Saudi Arabia were male and aged between 30–40 years, reflecting the increasing male participation in surgical nursing roles in the region.12 Similarly, a study by Hawsawi et al also found that most participants held bachelor’s degrees and had 5–10 years of clinical experience, emphasizing the role of mid-career professionals in surgical settings.13 However, our findings contrast with those of Shubayr who found a higher proportion of female surgical nurses and a more balanced distribution across different age groups in a Brazilian context.14 This discrepancy may be attributed to cultural and systemic differences in nursing workforce composition and gender roles across countries. Furthermore, the predominance of Saudi nationals in our sample may reflect local hiring policies and nationalization efforts in the Saudi healthcare sector.15 The high proportion of participants with experience in surgical wards and operating rooms indicates appropriate participant selection for evaluating engagement with the WHO Surgical Safety Guidelines. The educational background and professional experience suggest a workforce capable of implementing surgical safety protocols, though actual adherence may vary and warrants further behavioral and system-level analysis.
The findings (Figure 2) indicate a high level of institutional support and nurse engagement with the WHO Surgical Safety Checklist (SSC) at Qassim University Medical City. A significant majority of the nurses (93.9%) reported having received prior training on the SSC, and 97% confirmed the availability of the checklist in the operating theatre. These findings suggest a proactive institutional culture that supports surgical safety, consistent with the global push by the WHO to implement standardized safety protocols.16 Moreover, the knowledge assessment (Figure 1) revealed that 45% of nurses had good knowledge of the SSC, 36% had a moderate level, and 19% exhibited poor knowledge. This distribution reflects a generally strong awareness among the nursing staff, likely reinforced by the high rates of prior training and institutional availability of guidelines. Comparable results were reported in a study by Leone where over 90% of nurses in tertiary hospitals had received SSC training, and 48% demonstrated high knowledge levels.17 Similarly, Alqahtani et al who found that training significantly influenced SSC knowledge and compliance in Saudi hospitals.18 In contrast, a study conducted by Bhardwaj et al in India reported lower training rates (68%) and a higher proportion of nurses with inadequate SSC knowledge, attributing the gap to inconsistent in-service education and lack of institutional enforcement.19 This comparison highlights the importance of continuous training and strong leadership support in fostering effective SSC implementation. The current findings reinforce the need for ongoing education and monitoring to sustain high levels of adherence and promote a culture of surgical safety. Despite encouraging figures, the presence of nurses with poor knowledge (19%) indicates room for improvement through targeted interventions and refresher training programs.
 |
Figure 2 Frequency and distribution of the studied nurses according to the presence of SSC guidelines and receiving previous training program regarding SSC. (n = 66). Notes: Regarding previous training on the Surgical Safety Checklist (SSC), it shows that more than half 93.9% of the studied nurses reported having received such training, while 6.1% had not. However, approximately 97% of the studied nurses revealed the presence of SSC guidelines in the OR, while only 3% had not. |
The practice levels (Figure 3) of nurses toward the WHO Surgical Safety Guidelines, as shown in Figure 3, indicate a mixed but generally positive pattern. While 44.3% of the participants demonstrated adequate practice in the “Before Induction of Anesthesia” phase, the “Before Skin Incision” and “Before the Patient Leaves the Operating Room” phases had relatively higher adequate to neutral practice levels (40.6% and 41.4%, respectively). Overall, 39.2% of nurses exhibited adequate practice across all components, underscoring the need for targeted quality assurance efforts to improve consistency in guideline adherence. These findings align with those of Paterson et al, who reported similar variability in compliance across checklist phases, with the highest adherence noted during the anesthesia induction stage and lower consistency during sign-out procedures.20 The authors attributed this to the heightened attention given to anesthesia safety and comparatively less structured oversight during later procedural stages. Moreover, studies by Mondal et al also reported similar intermediate levels of practice, emphasizing that while awareness and training may be high, consistent practice remains a challenge without continuous monitoring and institutional support.21 For example, Poveda et al noted that despite 85% of nurses receiving training, only 42% consistently followed all checklist steps in practice.22 In contrast, higher levels of adherence were observed in structured and accreditation-driven healthcare systems. A study by Ribeiro et al in the United Kingdom demonstrated that when hospitals incorporated surgical safety checklist adherence into performance metrics and daily briefings, compliance across all phases exceeded 80%.23 This suggests that the presence of institutional mandates and leadership support plays a critical role in enhancing practice consistency. Therefore, while the current findings reflect a moderately engaged nursing workforce, further improvement is required through structured audit systems, regular simulation-based training, and strong interdisciplinary collaboration to ensure complete implementation of the WHO guidelines at every surgical phase.
 |
Figure 3 Practice level of the studied nurses toward WHO surgical safety guidelines in the operating theatre. (n= 66). Notes: demonstrates the distribution of nurses’ practice levels toward WHO surgical safety guidelines in the operating theatre. Notably, most nurses (44.3%) demonstrated an adequate level of practice regarding the “Before Induction of Anesthesia” phase. Additionally, (40.6%) showed an adequate level of practice during the “Before Skin Incision” phase. Concerning the “Before the Patient Leaves the Operating Room” phase, (41.4%) of the nurses also fell into the neutral practice category. Overall, more than one-third of the nurses (39.2%) demonstrated an adequate level of practice across all components of the WHO surgical safety guidelines. |
The results presented in (Table 2) demonstrate a moderate positive correlation (r = 0.58, p < 0.05) between nurses’ knowledge and practice levels regarding the WHO Surgical Safety Guidelines. This statistically significant relationship indicates that as nurses’ knowledge of surgical safety increases, their adherence to proper practices in the operating theatre tends to improve correspondingly. This finding reinforces the critical role of knowledge acquisition in shaping clinical behavior and supports ongoing investment in targeted educational interventions. This result is consistent with findings by Lemos and Poveda who reported a significant correlation (r = 0.61, p < 0.01) between surgical safety knowledge and practice among perioperative nurses, emphasizing the importance of theoretical understanding in promoting compliance with safety protocols.24 Similarly, a study conducted by Cabral and Pereira revealed a comparable positive correlation, further supporting the link between cognitive preparedness and behavioral adherence in surgical settings.25
However, other studies have reported weaker associations between knowledge and practice, suggesting that knowledge alone may not always translate into action. For example, Oliveira et al found only a mild correlation (r = 0.32) in an Indian tertiary hospital, highlighting the influence of environmental factors such as team dynamics, administrative support, and workload pressure on practice implementation.26 This discrepancy underscores the multifactorial nature of clinical compliance and the need to address both individual competencies and systemic enablers. Overall, the moderate correlation found in the current study highlights that while enhancing knowledge is essential, it should be complemented by supportive policies, team-based reinforcement, and regular audits to ensure consistent application of surgical safety protocols in daily practice. Furthermore, While the study demonstrates a positive association between nurses’ knowledge and adherence to WHO Surgical Safety Guidelines, it is important to note that high knowledge levels do not always result in consistent practice. This discrepancy may be influenced by systemic barriers within the clinical environment, such as heavy workload pressures, team dynamics, and the broader organizational culture that may not fully support strict adherence to safety protocols. Addressing these barriers through institutional support, targeted training, and workflow optimization is crucial to ensure that knowledge effectively translates into safe and consistent surgical practices.
Furthermore, in (Table 3) there is significant relation between demographic characteristics and the knowledge and practice levels of nurses regarding WHO Surgical Safety Guidelines. Notably, female nurses outperformed male counterparts in both knowledge and practice (p = 0.01 and 0.02, respectively). This finding aligns with a study by Santana et al who also reported significantly higher compliance and attentiveness among female surgical nurses, attributing the difference to communication style and attention to detail.27 Years of experience were also positively associated with performance, particularly among those with 5–9 years of clinical exposure. This intermediate experience bracket may reflect a balance between theoretical knowledge and sufficient clinical exposure, as supported by research from Faria et al, who noted similar patterns in Saudi and Emirati surgical units.28 Nurses with more than 10 years of experience, while experienced, sometimes showed stagnation in updating practices, as echoed in earlier literature.29 Educational level was another strong predictor of practice, with bachelor’s degree holders outperforming others, possibly due to formal exposure to safety protocols in academic curricula. This is consistent with findings from a study by Roscani ar et al, which emphasized the role of formal education in shaping evidence-based surgical practices among nurses in sub-Saharan Africa.30 Interestingly, nurses working in surgical wards had significantly higher knowledge and practice scores compared to those in the operating room (p = 0.01 and 0.05), suggesting that ward-based protocols and routine documentation may reinforce guideline application more frequently than high-pressure OR environments. This finding somewhat contrasts with the study of Batista et al, who found higher compliance in operating theatres due to the presence of multidisciplinary oversight.31 The inconsistency may be due to differences in institutional emphasis or resource allocation between settings. Conversely, age and nationality showed no significant association with knowledge or practice, suggesting that professional factors such as education, training, and environment are more influential than personal demographics. This reinforces the idea that structured continuing education and supportive work environments are crucial for enhancing surgical safety compliance across all nurse categories. This study has several limitations. The use of purposive sample and a relatively small sample size may limit the generalizability of the findings. The self-administered online survey could introduce response bias, and while observations were conducted without prior notification to minimize bias, the possibility of the Hawthorne effect cannot be excluded. Additionally, the cross-sectional design captures only a single point in time, and observational data were limited to accessible operating theatres. Finally, the classification of knowledge and adherence scores, though based on established cutoffs, may not fully reflect nuanced performance differences. Despite these limitations, the study provides valuable, context-specific insights into nurses’ awareness, attitudes, and adherence to surgical safety protocols.
Conclusions
This study demonstrates that nurses at Qassim University Medical City generally exhibit good awareness and training regarding the WHO Surgical Safety Guidelines; however, variations in knowledge and practical adherence persist across different surgical phases. The moderate positive correlation between knowledge and practice indicates that enhanced education improves compliance with safety protocols. Associations with gender, experience, education level, and workplace setting further highlight the influence of professional background and environment on safe surgical practices. Despite these positive findings, the presence of nurses with inadequate knowledge and inconsistent adherence underscores the need for ongoing quality improvement efforts. Addressing these gaps requires tailored educational programs, institutional support mechanisms, and policy-level interventions. Nursing educators should integrate the WHO Surgical Safety Checklist into both academic curricula and clinical training, while healthcare institutions should provide refresher courses, simulation training, and competency assessments. Creating a culture of safety that empowers nurses to advocate for protocol adherence, alongside reducing barriers such as workload pressures and resource limitations, is critical. Collectively, these measures can enhance teamwork, minimize surgical errors, improve patient outcomes, and strengthen the overall quality of perioperative care in the Saudi context.
The findings of this study have several practical implications. Hospital administrators should consider implementing regular training programs and refresher courses to reinforce nurses’ knowledge and adherence to WHO Surgical Safety Guidelines. Policymakers can support the development of standardized monitoring systems and protocols to ensure consistent compliance across operating theatres. Educators in nursing programs should emphasize the integration of surgical safety principles into both theoretical and clinical curricula, promoting a culture of patient safety. Additionally, addressing systemic barriers such as workload management, team communication, and institutional support can help translate knowledge into consistent, safe practice, ultimately enhancing surgical outcomes.
Institutional Review Board Statement
The study received ethical approval from the Research Ethics Committee and Medical City at Qassim University in January 2024 (reference code No. 24/71/03). Approval was also obtained from the Dean of Academic Affairs at the research site. Participants were thoroughly informed about the study’s objectives, and their privacy and confidentiality were rigorously protected.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Informed Consent Statement
Permission obtained from all participants before data collection.
Acknowledgments
The researchers would like to thank the Deanship of Graduate Studies and Scientific Research at Qassim University for financial support (QU-APC-2025). The researchers sincerely thank all the participants for their valuable time and contribution. We also gratefully acknowledge the support and cooperation of the participating colleges at QUMC, which greatly assisted in facilitating the data collection process.
Author Contributions
All authors significantly contributed to the conception and design of the study, as well as the execution, data collection, analysis, and interpretation of the results. They were actively involved in drafting, revising, and critically reviewing the manuscript. The authors have approved the final version for publication, agree with the choice of the journal for submission, and accept full responsibility for the accuracy and integrity of the work.
Disclosure
The authors report no conflicts of interest related to this study.
References
1. World Health Organization WHO. WHO surgical safety checklist and implementation manual. Geneva: 2024. Available from: https://www.who.int/teams/integrated-health-services/patient-safety/research/safe-surgery.
2. Alsadoun L, Sanipini S, Khleif R, et al. Evaluating the impact of the world health organization’s surgical safety checklist on clinical outcomes and implementation strategies: a systematic review. Cureus. 2024;16(9).
3. Dirie NI, Elmi AH, Ahmed AM, et al. Implementation of the WHO surgical safety checklist in resource-limited Somalia: a new standard in surgical safety. Patient Safety Surg. 2024;18(1):30. doi:10.1186/s13037-024-00410-2
4. Al-Qahtani EM, Alzahrani AA, Omran NA, et al. Exploring the relationship between patient safety and quality of care in Saudi Arabia. J Int Crisis Risk Communication Res. 2024;7(S6):939.
5. Yaseen SJ, Taha S, Alkaiyat A, Zyoud SE. Multicenter audit of operating room staff compliance with the surgical safety checklist: a cross-sectional study from a low-and middle-income country. BMC Health Serv Res. 2025;25(1):103. doi:10.1186/s12913-025-12288-6
6. Hawsawi OA, Brnawi HB, Al-Husawi HA, et al. Nurses’ compliance with surgical safety protocols for patients having abdominal surgery in Saudi Arabia. J Int Crisis Risk Communication Res. 2024;7(S6):173.
7. El-Sayed WMA, Eldeeb IEM, Khater MK, Morsy TA. Operating room and patient safety: an overview. J Egyptian Soc Parasitol. 2021;51(2):391–404. doi:10.21608/jesp.2021.193325
8. Alsadun D, Arishi H, Alhaqbani A, et al. Do we feel safe about the surgical safety checklist? A cross-sectional study between two periods. Global J Quality Safety Healthcare. 2021;4(4):135–140. doi:10.36401/JQSH-20-46
9. Alrasheadi BA, Alamri MS, Aljohani KA, et al. nurses’ perception of safety culture in medical− surgical units in hospitals in Saudi Arabia. Medicina. 2022;58(7):897. doi:10.3390/medicina58070897
10. Rawas H, Abou Hashish EA. Predictors and outcomes of patient safety culture at King Abdulaziz Medical City, Jeddah, Saudi Arabia. A nursing perspective. BMC Nurs. 2023;22(1):229. doi:10.1186/s12912-023-01391-w
11. Melekie TB, Getahun GM. Compliance with surgical safety checklist completion in the operating room of university of gondar hospital, Northwest Ethiopia. BMC Res Notes. 2015;8(1):361. doi:10.1186/s13104-015-1338-y
12. Habtewold YW, Getnet MA, Genetu KB, Woretaw AW. Nurses’ knowledge, perceived practice, and associated factors towards sterile techniques in major operation rooms at public hospitals in Addis Ababa, Ethiopia, 2022: a cross-sectional study. BMC Nurs. 2024;23(1):794. doi:10.1186/s12912-024-02462-2
13. Rydenfält C, Johansson G, Odenrick P, Åkerman K, Larsson PA. Compliance with the WHO surgical safety checklist: deviations and possible improvements. Int J Qual Health Care. 2013;25(2):182–187. doi:10.1093/intqhc/mzt004
14. Shubayr N. Operating room radiation safety measures: awareness, compliance, and perceived risks among nurses and other healthcare workers. Int Nurs Rev. 2024;2024.
15. Manamela LM, Rasweswe MM, Mooa RS. Factors contributing to non-adherence of the peri-operative surgical team to WHO surgical safety checklist in the Kingdom of Saudi Arabia. Perioperative Care Operating Room Management. 2022;29:100292. doi:10.1016/j.pcorm.2022.100292
16. Gasoma EB, Marouf MA. Enhancing surgical outcomes: evaluating the impact of implementing the world health organization surgical safety checklist—a prospective cross-sectional study. Surgery J. 2024;10(04):e53–9. doi:10.1055/s-0044-1800917
17. Leone S. Assessing utilization and barriers to effective implementation of the WHO surgical safety checklist at princess Christian maternity hospital, Freetown. Surgeon. 40.
18. Alqahtani MA, Nabrawi MA, Alharbi SA, et al. A review of enhancing operating room safety: protocols, practices, and preventative measures. J Int Crisis Risk Communication Res. 2024;7(S8):2621.
19. Squires K, Pilkington M, Clément L, Brindle ME. Healthcare priorities for surgical care in Canada. Ann Surg Open. 2025;6(2):e561. doi:10.1097/AS9.0000000000000561
20. Paterson C, Mckie A, Turner M, Kaak V. Barriers and facilitators associated with the implementation of surgical safety checklists: a qualitative systematic review. J Adv Nurs. 2024;80(2):465–483. doi:10.1111/jan.15841
21. Mondal SC, Lahiri S, Mudi S. Knowledge, attitude, and practices of health care providers regarding the implementation of world health organization surgical safety checklist at malda medical college and hospital. Front Health Informatics. 2024;13(5).
22. Poveda VD, Lemos CD, Lopes SG, Pereira MC, Carvalho RD. Implementation of a surgical safety checklist in Brazil: cross-sectional study. Revista Brasileira de Enfermagem. 2021;74(2):e20190874. doi:10.1590/0034-7167-2019-0874
23. Ribeiro L, Fernandes GC, Souza EG, Souto LC, Santos AS, Bastos RR. Safe surgery checklist: filling adherence, inconsistencies, and challenges. Revista Do Colégio Brasileiro de Cirurgiões. 2019;46(5):e20192311. doi:10.1590/0100-6991e-20192311
24. Lemos CD, Poveda VD. Effect of implementing an anesthesia nurse checklist in a safety and teamwork climate: quasi-experimental study. Revista da Escola de Enfermagem da USP. 2022;56:e20210471. doi:10.1590/1980-220x-reeusp-2021-0471en
25. Cabral DB, Pereira ML, Fernandes MS, Fincatto S, Kuczmainski AG, Korb A. Auditable criteria for implementing best practices in adhering to the surgical safety checklist. Acta Paulista de Enfermagem. 2021;34:eAPE00515. doi:10.37689/acta-ape/2021AO00515
26. Oliveira JL, Silva SV, Santos PR, Matsuda LM, Tonini NS, Nicola AL. Patient safety: knowledge between multiprofessional residents. Einstein. 2017;15(1):50–57. doi:10.1590/s1679-45082017ao3871
27. Santana HT, de Freitas MR, Ferraz EM, Evangelista MS. WHO safety surgical checklist implementation evaluation in public hospitals in the Brazilian federal district. J Infection Public Health. 2016;9(5):586–599. doi:10.1016/j.jiph.2015.12.019
28. Faria LR, Moreira TR, Carbogim FD, Bastos RR. Effect of the surgical safety checklist on the incidence of adverse events: contributions from a national study. Revista Do Colégio Brasileiro de Cirurgiões. 2022;49:e20223286. doi:10.1590/0100-6991e-20223286_en
29. de Almeida RE, Rodrigues MC. Filling in the surgical safety checklist in Brazilian hospitals. Rev Rene. 2018;19(1):69.
30. Roscani AN, Ferraz EM, Oliveira Filho AG, Freitas MI. Validation of surgical checklist to prevent surgical site infection. Acta Paulista de Enfermagem. 2015;28(6):553–565. doi:10.1590/1982-0194201500092
31. Batista J, Cruz ED, Alpendre FT, Rocha DJ, Brandão MB, Maziero EC. Prevalence and avoidability of surgical adverse events in a teaching hospital in Brazil. Revista Latino-Americana de Enfermagem. 2019;27:e2939. doi:10.1590/1518-8345.2939.3171
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Experience of Nurses with Intravenous Fluid Monitoring for Patient Safety: A Qualitative Descriptive Study
Park J, You SB, Kim H, Park C, Ryu GW, Kwon S, Kim Y, Lee S, Lee K
Risk Management and Healthcare Policy 2022, 15:1783-1793
Published Date: 22 September 2022
The Association of Transformational Leadership on Safety Practices Among Nurses: The Mediating Role of Patient Safety Culture
Hamdan M, Jaaffar AH, Khraisat O, Issa MR, Jarrar M
Risk Management and Healthcare Policy 2024, 17:1687-1700
Published Date: 26 June 2024
Instruments for Measuring Healthcare Professionals’ Medication Safety Competence: A Scoping Review
Stephan C, Kloor D, Wurmbach VS, Mahler C
Journal of Multidisciplinary Healthcare 2025, 18:1745-1758
Published Date: 25 March 2025
Improving Surgical Safety in Somalia a Closed-Loop Audit Study of WHO Surgical Safety Checklist Adherence
Yusuf FY, Hussein AM, Elmi AH, Mohamed DA, Abdi AO
Risk Management and Healthcare Policy 2025, 18:4003-4010
Published Date: 24 December 2025
Managerial Challenges in the Clinical Use of Checklists: Proven Benefits, Yet Untapped Potential?
Palm M, Braut GS
Journal of Healthcare Leadership 2026, 18:567303
Published Date: 15 January 2026