Back to Journals » Risk Management and Healthcare Policy » Volume 19
Enhancing Crisis Preparedness in Healthcare Facilities: A Risk-Based Assessment Tool for Preventing Targeted Violent Attacks
Authors Zajíc M ![]() , Tušer I
, Tušer I ![]() , Jánský J
, Jánský J
Received 27 July 2025
Accepted for publication 26 January 2026
Published 18 February 2026 Volume 2026:19 551849
DOI https://doi.org/10.2147/RMHP.S551849
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Gulsum Kaya
Miloš Zajíc,1 Irena Tušer,1 Jiří Jánský2
1Department of Security Management, AMBIS University, Praha, Czech Republic; 2Faculty of Military Technology, University of Defence, Brno, Czech Republic
Correspondence: Irena Tušer, AMBIS University, Lindnerova 1, Praha, 180 00, Czech Republic, Email [email protected]
Introduction: Terrorist and other deliberate attacks on outpatient healthcare facilities pose a serious threat to the health and safety of the population. Strengthening the resilience of outpatient healthcare facilities to violent incidents requires a comprehensive approach that includes physical security, technological measures, staff preparedness, and effective emergency management. According to World Health Organization estimates, between 8% and 38% of healthcare workers experience physical violence during their professional career, highlighting the substantial magnitude and seriousness of this problem across healthcare systems.
Objective: The study focuses on establishing a hierarchy of key dimensions of crisis preparedness. A second objective is to propose a methodological procedure that healthcare facilities can use to determine their own hierarchy of preparedness aspects and that is sufficiently flexible to be applied across different types of facilities and healthcare systems.
Methods: The research was conducted as a mixed-methods study combining qualitative and quantitative approaches. The quantitative part used the Analytic Hierarchy Process with 30 experts from 30 different outpatient healthcare facilities. Expert inputs were obtained through pairwise comparisons provided by these thirty crisis preparedness specialists and healthcare professionals.
Results: The research revealed key shortcomings in the crisis preparedness of the analysed outpatient healthcare facilities. Six main preparedness dimensions were identified, three of which were rated as having the highest priority in the expert assessment. Based on these, the authors proposed a tool for assessing the current level of crisis preparedness, which can be applied within the internal audit of similar types of facilities.
Conclusion: The proposed tool contributes to the protection of soft targets in the healthcare sector and supports systematic planning of security measures. The study also provides a methodological framework usable by junior professionals and healthcare policy makers.
Plain Language Summary: The research focused on the physical and technical security measures of buildings and on the security documentation of outpatient healthcare facilities. The study did not involve human or animal subjects and therefore did not require formal ethics committee approval. All respondents (members of the expert panel) were solely involved in pairwise comparisons of criteria necessary for the application of the AHP method.
Prior to providing their assessments, all members of the expert panel were duly informed about the purpose of the study, the procedures used, and the processing and storage of the input data for the AHP method. They explicitly provided their informed consent to participate in the study before its commencement. For these reasons, the AMBIS University Ethics Committee granted an ethics waiver, recorded under reference number EC 04/2025.
Keywords: crisis preparedness, outpatient healthcare facilities, risk management, violent attacks, active attacker, preventive measures, public health, patient safety, health policy
Introduction
The pursuit of a safe environment is a natural and universal human endeavor. Its provision is a pillar of social trust and the stable functioning of public institutions.1 This need is particularly relevant in outpatient healthcare settings providing care to vulnerable populations, where safety breaches may have serious consequences for health, patient trust, and the functioning of the healthcare system as a whole.2,3 The patient, as a person temporarily or permanently dependent on professional care, naturally finds himself in a role when in contact with the healthcare system that creates the need for assurances of a safe environment and competent care.4
However, in recent years, outpatient healthcare facilities have faced increasing security risks. They are increasingly becoming targets of physical attacks, aggressive behavior, or vandalism.5,6 These facilities, especially outpatient facilities, are often referred to as soft targets, ie publicly accessible places with limited physical protection options.7 According to a report by the European Crime Prevention Network,8 attacks on such public facilities are increasing in the European Union countries, with healthcare facilities increasingly being identified as vulnerable. Data from the UK9 show that more than 14% of healthcare workers have experienced physical assault in the past year. In Germany, the Federal Statistical Office10 recorded a more than 25% increase in violent incidents in healthcare between 2017 and 2020, largely in the outpatient sector. The Dutch Healthcare Authority11 highlights the increasing risk of aggression in waiting rooms and emergency rooms.
Laws in developed countries, whose subject matter is emergency management,12–14 impose an obligation to develop a crisis preparedness plan (CPP) on designated entities, which are hospitals and acute care facilities. However, outpatient facilities that provide primary health care,15,16 are not directly called upon to create crisis plans, remaining outside the mainstream of emergency planning – and thus outside the systematic control of their crisis preparedness. This disproportion between legislative regulation and real security risks creates space for professional interest and practical interventions.
Experience shows that patients increasingly consider not only the professional level of care provided, but also other factors. These include the availability of hospitals,17,18 but also subjectively perceived safety, and the organization of care as a whole. This is also confirmed by the conclusions of a systematic literature review,19 which identified safety, transparency, and trust as key factors influencing patient satisfaction and provider choice. Methods for quantifying population safety are also described, for example, in.20
The presented study responds to these challenges by proposing a methodology that enables the assessment of the crisis preparedness of outpatient and polyclinic facilities against violent incidents such as “amok” and similar emergencies. The research is based on six key areas of security, which include physical and technical protection, personnel competence, planning for crisis scenarios, and the use of international experience. The authors’ objective is not to substitute legal regulation, but to create an expertly based framework that can be adapted across different healthcare systems and serve as a tool to strengthen the protection of soft targets in healthcare.
Materials and Methods
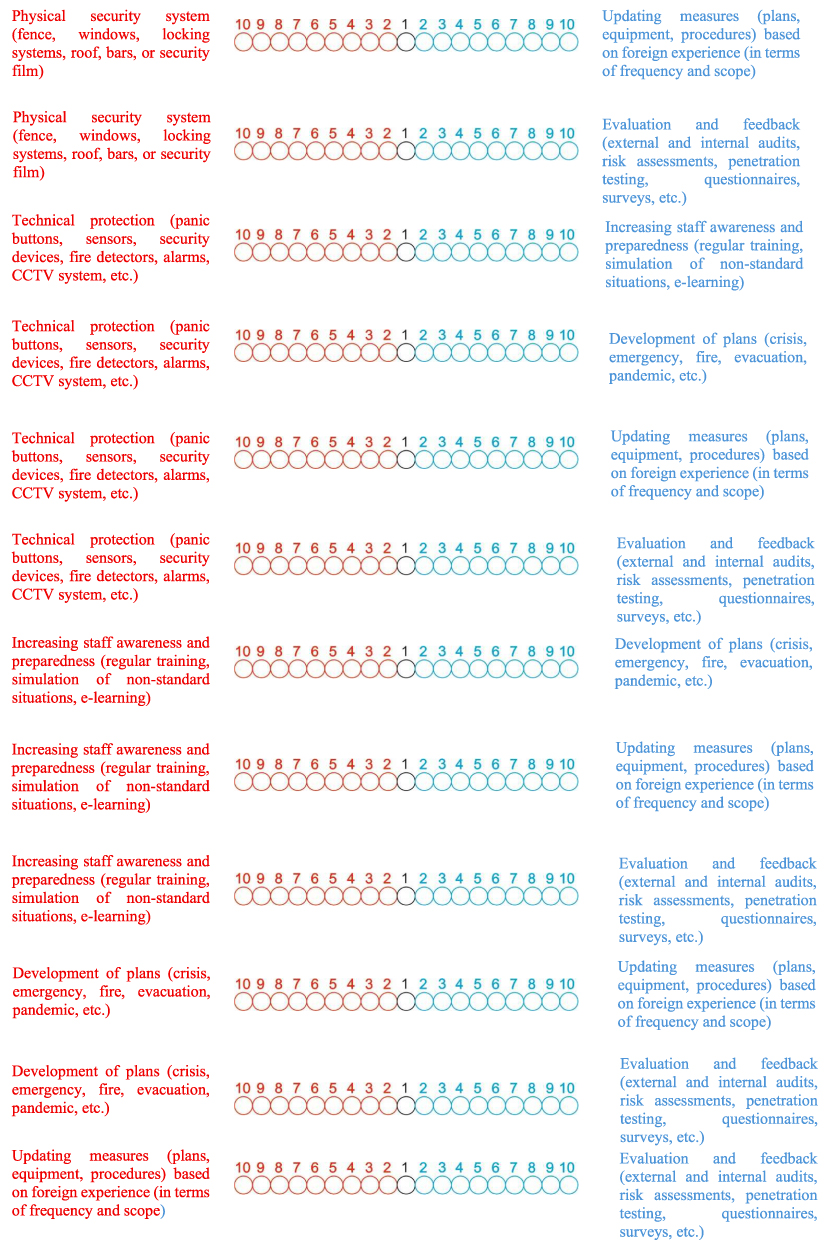
The research was designed as a combination of empirical survey and application of a multi-criteria decision-making model. In the first phase, a questionnaire was created, the structure of which was based on six main areas of research identified based on the practical experience of the authors and expert recommendations in the field of healthcare facility safety (Figure 1).
Figure 1 Continued. Figure 1 Questionnaire of the Conducted Research.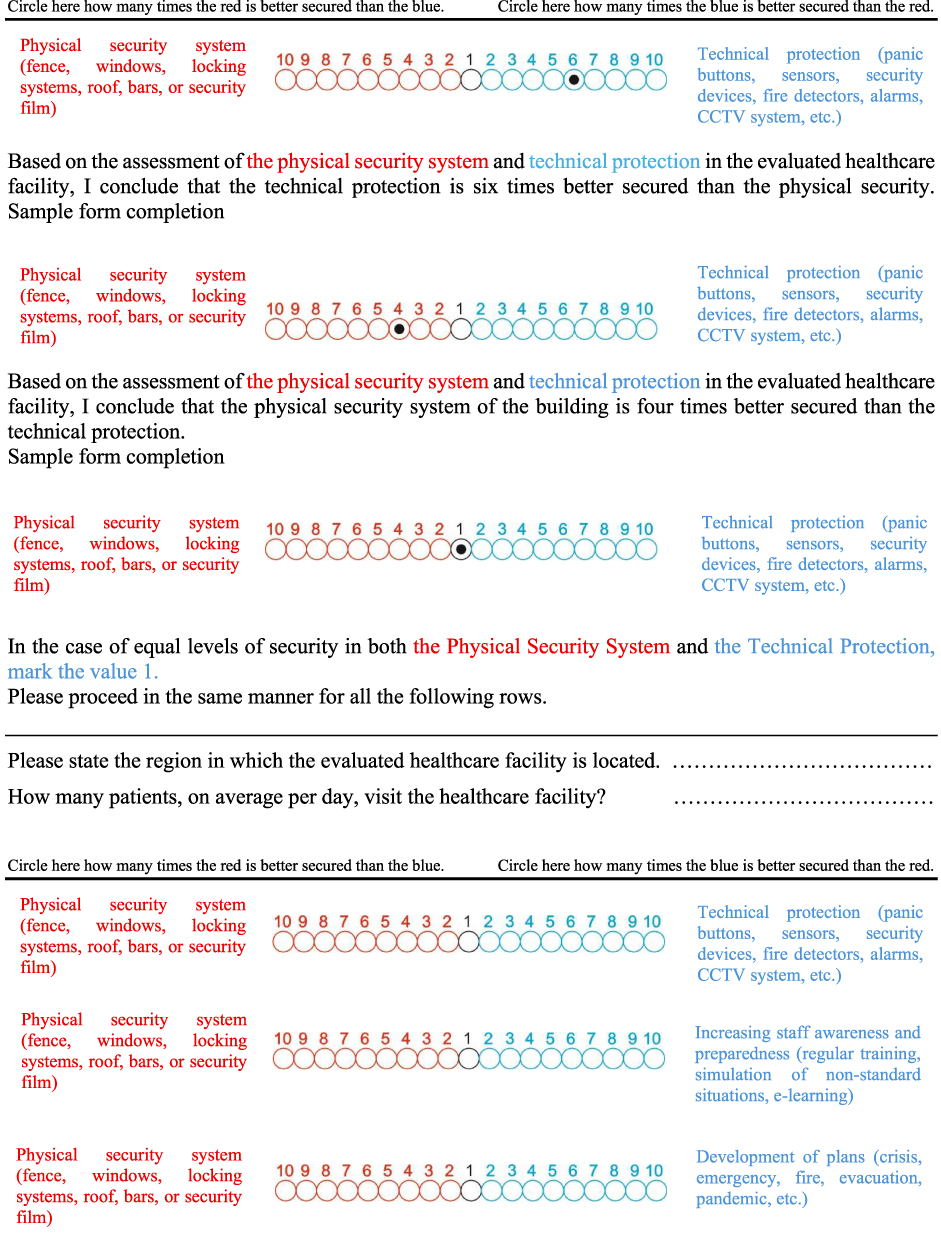
These areas included:
- physical security system (A1) – primary protection of a facility, protection of entry points, property, and persons against unauthorized entry or violent acts,
- technical protection (A2) – technological means to detect and prevent threats,
- increasing staff awareness and preparedness (A3) – the ability of healthcare workers to adequately respond to unexpected events, crisis training, and regular exercises,
- processing of plans (A4) – creating plans for dealing with non-standard, emergency events and crisis situations - introduction of at least minimal scenarios, procedures, and contacts for emergency management,
- updating existing measures based on experience from abroad (A5) – using knowledge from the international environment, where the crisis preparedness of healthcare entities is systematically developed,
- evaluation and feedback (A6) – systematic verification of the effectiveness of security measures through tools such as internal and external audits, risk assessments, penetration testing, questionnaire surveys, and polls; the results of these tools are used to identify weaknesses, assess preparedness, and continuously improve emergency management and physical and technical security.
The questionnaire was designed in the form of a pairwise comparison of individual areas, which is an approach corresponding to methodology of the Analytic Hierarchy Process (AHP). The respondents were asked to express the mutual importance of individual areas in terms of security of the healthcare facility. The comparison was made on a scale of 1–10, where the value 1 meant equal importance of both criteria, while the values 2–10 expressed different degrees of preference of one criterion over the other (or their inverse values in the case of the opposite preference). Instructions for filling in were demonstrated on a specific example shown at the beginning of the questionnaire. In this way, the respondents compared all relevant combinations of questionnaire areas. More precisely, each respondent in the questionnaire compared all pairs of areas Ai,Aj, where  .
.
The questionnaire was distributed to 30 specialized healthcare facilities across the Czech Republic. The respondents consisted of 30 experts. For the purposes of this study, an “expert” was defined as an individual with direct experience in managing the crisis preparedness of an outpatient healthcare facility and at least three years of relevant professional practice. All respondents met these criteria, which supports the validity of the expert inputs obtained. Before completing the questionnaire, a short, targeted interview was conducted with each respondent (expert), the purpose of which was to eliminate interpretative excesses and ensure a correct understanding of the evaluation methodology. This significantly increased the validity of the data obtained and representativeness of the results.
To analyze the completed questionnaires, the Analytic Hierarchy Process (AHP) method, developed by Thomas L. Saaty21 – this method allows for hierarchical structuring of the decision-making problem, quantification of subjective preferences, and objective evaluation of options. In healthcare settings, this method can be effectively used, for example, for evaluating security options of an ambulance (eg installation of security doors, camera system, presence of security guards, changes in the layout of the interior) with regard to criteria such as security benefits, financial requirements, operational impacts, and acceptability by patients.
After receiving all completed questionnaires, the data from each respondent was transformed into a Saaty pairwise comparison matrix, which formed the basis for the next phase of analysis. This matrix allowed the calculation of weighted priorities of individual respondents in the given areas. Then, by synthesizing the preferences of all respondents, the resulting weights of the individual options were calculated.
The following section describes the principles of the AHP method, its application in outpatient healthcare facilities, and an example of a model decision-making problem focused on selecting an optimal combination of safety measures for outpatient surgical settings.
Table 1 below illustrates how the questionnaire data was processed. It is a representation of a table filled in from one questionnaire, which represents the results of a pairwise comparison of preferences between individual safety areas at a specific healthcare facility. This data served as an input matrix for calculating weights using AHP and subsequent synthesis of priorities within the overall assessment.
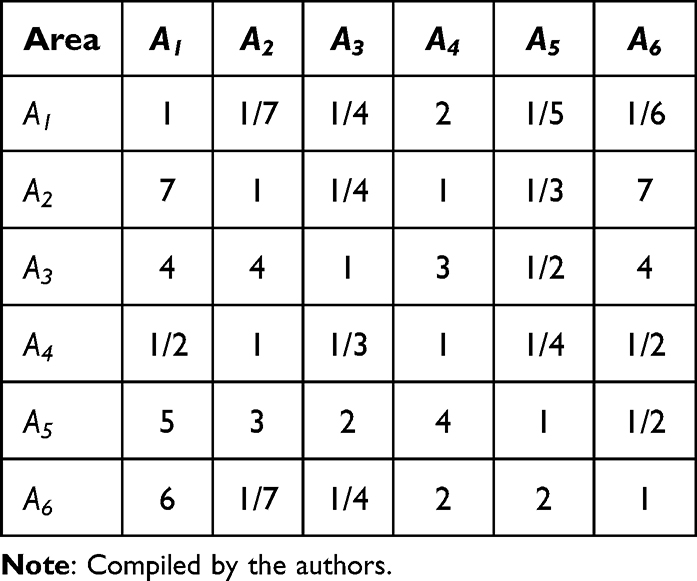 |
Table 1 Pairwise Comparison of Preferences Between Individual Areas of Security |
The first row and first column of Table 1 list the criteria being compared. The rest of Table 1 lists the values filled in by the user. These values form a matrix, which we will denote by the symbol Q. Matrix Q is reciprocal, which means that for its elements it holds  for all
for all  . However, it does not satisfy the condition
. However, it does not satisfy the condition  for all
for all  and is therefore not consistent. Now, using the elements of the matrix Q, it is necessary to estimate the elements of the decision vector W=(w1,w2,…w6). The most common method to obtain the vector W is to find it as a solution to the equation
and is therefore not consistent. Now, using the elements of the matrix Q, it is necessary to estimate the elements of the decision vector W=(w1,w2,…w6). The most common method to obtain the vector W is to find it as a solution to the equation  , where
, where  is the largest eigenvalue. However, this method is recommended only if the consistency ratio is
is the largest eigenvalue. However, this method is recommended only if the consistency ratio is  where RI is the average consistency index given by the tabular values discussed in the articles.22,23 However, for the matrix Q shown in Table 1 it holds that CR>0.1, and therefore does not satisfy this condition. That is the reason why in this paper the decision vector W was estimated using a different method described in the paper.23 It is known that if Q is the reciprocal of the matrix, then the matrix L defined as
where RI is the average consistency index given by the tabular values discussed in the articles.22,23 However, for the matrix Q shown in Table 1 it holds that CR>0.1, and therefore does not satisfy this condition. That is the reason why in this paper the decision vector W was estimated using a different method described in the paper.23 It is known that if Q is the reciprocal of the matrix, then the matrix L defined as
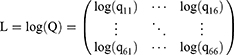
is a Skew-Hermitian matrix. It is a matrix whose elements have the property  for all
for all  . For this type of matrices, a simple algorithm for calculating a consistent matrix using orthogonal projection was described in the article.23 According to this algorithm, a square
. For this type of matrices, a simple algorithm for calculating a consistent matrix using orthogonal projection was described in the article.23 According to this algorithm, a square  with six rows is first constructed, whose elements are only ones.
with six rows is first constructed, whose elements are only ones.
matrix  is constructed. At the end of the mentioned algorithm, the matrix M is constructed
is constructed. At the end of the mentioned algorithm, the matrix M is constructed
which is the closest consistent matrix to the matrix Q.
By applying the above algorithm to the matrix Q, we obtain a consistent matrix M of the form:
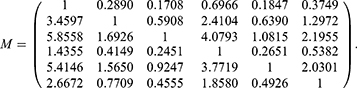
For this consistent matrix, the desired weight vector W1 (ie, the normalized Perron eigenvector) is in the form of  .
.
The other completed questionnaires were also processed in the same way as described above. The decision vectors for respondents 1, 2, 3, and 30 are marked with symbols  and are listed in Table 2. The resulting decision vector of weights
and are listed in Table 2. The resulting decision vector of weights

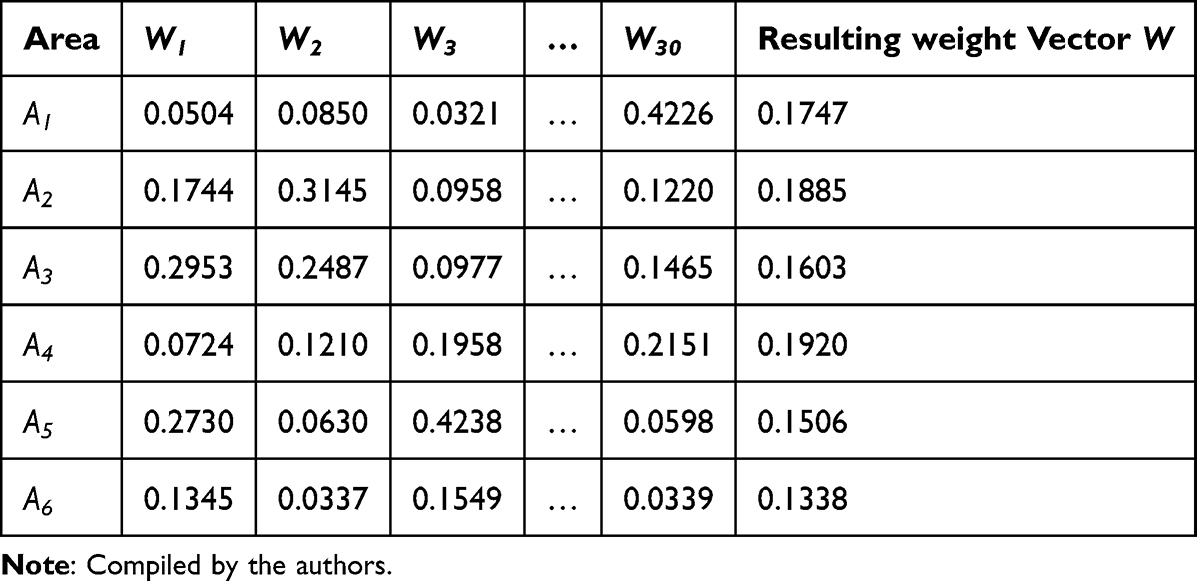 |
Table 2 Values of Weight Vectors Wi for Respondents 1, 2, 3, and 30, and the Resulting Weight Vector W |
was obtained as the average of the relevant elements of the decision vectors Wi, obtained from individual respondents, and is also shown in the last column of Table 2.
The weights in vector W determine the importance that individual areas have in ensuring security.
Results and Recommendations
As part of the empirical survey, 30 healthcare facilities from different regions of the Czech Republic were approached, with each respondent being explained the methodology in an initial interview, which contributed to increasing the reliability and validity of the results. Using the orthogonal projection method and subsequently the Analytic Hierarchy Process,21 preferences for six basic areas of crisis preparedness of healthcare facilities were evaluated. These preferences are listed in Table 3.
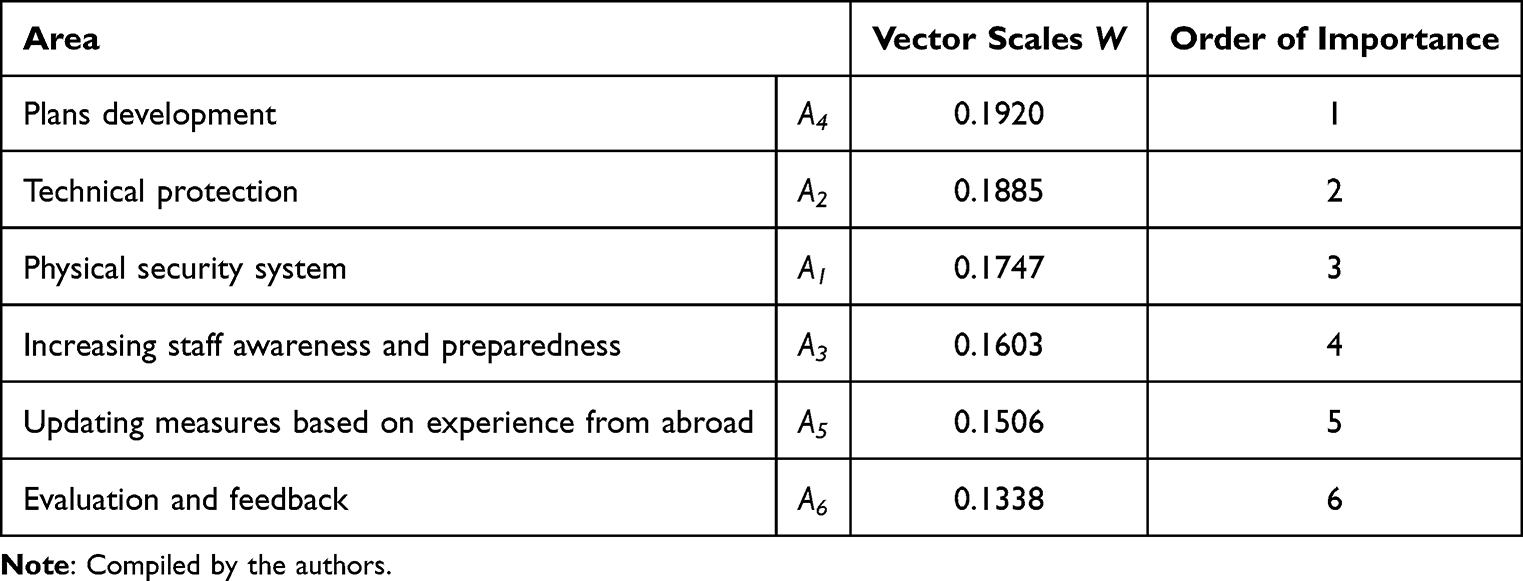 |
Table 3 Ranking of Areas Studied by Importance |
Table 3 shows that respondents consider the following areas to be the most important in terms of ensuring the safety of outpatient facilities:
1. Plans development,
2. Technical protection,
3. Physical security system.
On the contrary, areas such as updating measures based on experience from abroad and evaluation and feedback were assessed as lower priority, but still not negligible. The resulting weighted decision vector (Table 3) showed balanced preferences between “soft” (organizational-behavioral) and “hard” (technical) elements of crisis preparedness, which corresponds to international findings on the protection of soft targets in healthcare.7,8
The above result is consistent with professional literature, which has long highlighted the need to develop worker competencies as a key element of security in healthcare,19,24 and at the same time supports the trend of a comprehensive approach to crisis preparedness that integrates organizational, human, and technological components.16
The research has several limitations that need to be considered when interpreting the results. The AHP method uses subjective expert evaluation, which can be influenced by the individual experiences of respondents despite standardized instructions. The selection of six main areas of crisis preparedness was based on expert recommendations and the authors’ practice but does not cover all possible dimensions of evaluation. In the future, it would be beneficial to supplement the model with economic indicators or links to the integrated rescue system. Another limitation is that the research does not evaluate the empirical impact of specific measures on security incidents in practice. The absence of quantitative evaluation reduces the possibility of accurately determining the effectiveness of the proposed solutions.
Despite the limitations mentioned, this study can be a valuable practical tool for the professional community, as it offers a structured approach to assessing the crisis preparedness of outpatient (healthcare) facilities and supports the implementation of preventive measures against targeted violent attacks.
Discussion
The results obtained confirm the growing importance of crisis preparedness in outpatient healthcare facilities, with expert evaluations strongly preferring the areas of staff education and emergency planning. This conclusion corresponds to international recommendations that emphasize building organizational resilience and the ability of healthcare staff to respond effectively to unexpected situations.16,22 However, from the perspective of foreign approaches, while the Czech model emphasizes the human factor, some systems – especially in the USA or the Netherlands – place greater emphasis on technological measures and standardized procedures for protecting entrances, zoning, and detecting dangerous individuals.9,11 In this regard, a certain discrepancy can be identified between the respondents’ emphasis on staff preparedness and the technocratic concept of security applied abroad.
From a methodological point of view, the use of the AHP tool has proven to be an effective approach for synthesizing expert evaluation. However, the selection of six main safety areas, although supported by literature,7,8 can be considered partially reductive considering international studies. For example, Ferreira et al (2023)19 draw attention to the importance of patient experience and perceived safety as a factor influencing the quality of care and trust in the healthcare system. This aspect was not included in our research and could significantly enrich the interpretation and selection of priority areas in follow-up research.
It is also worth mentioning the fact that the results of the pilot study reflect the subjective views of experts from one national system. Although the effort to transfer the conclusions to other countries was taken into account by the design of a flexible model, it cannot be overlooked that the safety frameworks, legislation, and operational capacities of outpatient facilities differ from country to country. WHO (2020)16 and OECD (2023)25 state in their reviews that, for example, the degree of digitalization, support for risk management, and the financial availability of preventive technologies differ fundamentally between Western and Central Europe. In this sense, the design of the assessment tool should be interpreted as a basic framework that needs to be localized according to the operational and legal context of the target country. The findings of this study represent an expert-perceived level of preparedness rather than the empirically measured effectiveness of specific measures. The results should therefore be understood primarily as a framework for setting priorities in crisis management.
The lack of a quantitative assessment of the effectiveness of the measures can also be considered a relevant challenge for future research, which distinguishes this study from some foreign approaches that evaluate the impacts of security interventions on incident reduction (eg.9,10). Given that our study worked exclusively with expert judgment, the actual benefit of the recommended measures cannot be assessed without additional longitudinal analysis.
However, the results discussed point to the pragmatic value of the research. The proposed approach provides a structured and understandable tool that allows managers of healthcare facilities to quickly identify weak points and propose priority interventions without complex analyses or external audits. In this regard, the AHP approach is advantageous not only for its methodological transparency, but also for the possibility of adjusting weighted preferences according to the specific needs of the institution. This makes the model suitable for internal use and in an international environment, where a centralized crisis planning system for all healthcare facilities is not available.
It can be stated that, despite certain limitations, the research represents a practically usable contribution to risk management in healthcare, which enriches the current discussionon the protection of soft targets and preparedness for targeted violent attacks in the public healthcare sector.
The results of this study are based on an expert assessment of the crisis preparedness of thirty outpatient healthcare facilities and therefore reflect a perceived level of resilience rather than empirically measured performance. As the analysis was conducted within a single national healthcare system, the application of the proposed tool in other settings may require context-specific adaptation.
Conclusion
The presented study identified a significant gap in the area of risk management in the healthcare sector, specifically in the crisis preparedness of outpatient healthcare facilities, which, despite their vulnerability, are often neglected in formal emergency planning. Using the Analytic Hierarchy Process method, a structured tool was created to enable assessment and prioritization of key areas of preparedness. The research showed that healthcare professionals consider staff training and emergency planning to be the most important factors strengthening the resilience of institutions, while not neglecting the importance of technical and organizational measures.
Despite some limitations, such as the subjectivity of expert input and the national scope of the research, the proposed model represents a practically usable tool. It allows healthcare facility managers to systematically assess the current level of preparedness and implement preventive measures based on clearly defined and quantifiable criteria. The model is flexible and scalable, and therefore suitable for use in various types of outpatient facilities across healthcare systems and countries, regardless of whether they are subject to a formal legislative obligation for emergency planning.
This research contributes to the international discussion on healthcare system resilience and security policy by offering a transferable methodology to support the identification of organizational vulnerabilities and targeted risk reduction measures. The study results are therefore fully consistent with the objective of supporting population health improvement and risk reduction at all levels of care.
As this study represents the first phase of a broader research programme, it is designated as a pilot. Its aim was to verify the structure of the assessment framework, the clarity of the criteria, and the practical applicability of the AHP method in the context of outpatient healthcare facilities. In subsequent phases of the research project, the tool will be applied to a larger sample of facilities, and its effectiveness will be further evaluated through simulation scenarios and long-term monitoring of changes in crisis preparedness.
In conclusion, the presented tool has the potential to strengthen risk management in the outpatient healthcare sector by supporting informed decision-making, effectively prioritizing safety investments, and harmonizing preparedness efforts within the broader framework of public health protection. Future research should focus on the practical validation of the effectiveness of the proposed measures, for example through simulation exercises or the analysis of objective performance indicators.
Disclosure
The authors report no conflicts of interest in this work.
References
1. OECD. OECD Survey on Drivers of Trust in Public Institutions – 2024 Results: building Trust in a Complex Policy Environment [Internet]. Paris: OECD Publishing; 2024 [cited June 7, 2025]. Available from: https://www.oecd.org/en/publications/oecd-survey-on-drivers-of-trust-in-public-institutions-2024-results_9a20554b-en/full-report/trust-in-government-on-complex-policy-issues_036c7ccd.html.
2. Eller E, Frey D. Psychological Perspectives on Perceived Safety: social Factors of Feeling Safe. In: Raue M, Streicher B, Lermer E, editors. Perceived Safety: A Multidisciplinary Perspective. Cham: Springer; 2019:43–10. doi:10.1007/978-3-030-11456-5_4
3. Gottschalk-Mazouz N. Philosophical Perspectives on Safety and Risk. In: Raue M, Streicher B, Lermer E, editors. Perceived Safety. Cham: Springer; 2019. doi:10.1007/978-3-030-11456-5_3.
4. Kabat-Zinn J. Life Is a Disaster: How to Cope with Stress, Illness, and Pain Using the Wisdom of Body and Mind. In Czech: Život Samá Pohroma: Jak Čelit Stresu, Nemoci a Bolesti Pomocí Moudrosti Těla a Mysli. Brno: Jan Melvil Publishing; 2016. ISBN: 978-80-7555-012-5.
5. HFT – International Association for Healthcare Security and Safety Foundation. Healthcare crime and violent incidents by the numbers [Internet]. Healthcare Facilities Today. 2023 Mar 15, [cited June 7, 2025]. Available from: https://www.healthcarefacilitiestoday.com/posts/Healthcare-Crime-and-Violent-Incidents-by-the-Numbers--30080.
6. World Health Organization. Preventing violence against health workers [Internet]. Geneva: WHO; 2025 [cited June 7, 2025]. Available from: https://www.who.int/activities/preventing-violence-against-health-workers.
7. Kalvach Z. Basics Soft Targets Protection – guidelines [Internet]. Prague: Ministry of the Interior, Soft Targets Protection Institute, z.ú.; 2016 [cited June 7, 2025]. Available from: https://mv.gov.cz/chh/clanek/ke-stazeni-10-principu-zodolneni-mekkeho-cile.aspx.
8. European Crime Prevention Network. Soft Target Protection – thematic paper [Internet]. Brussels: EUCPN; 2022 [cited June 7, 2025]. Available from: https://eucpn.org/document/eucpn-thematic-paper-soft-target-protection.
9. Royal College of Nursing. Violence and aggression in the NHS: estimating the size and the impact of the problem: interim report [Internet]. London: Royal College of Nursing; 2018 [cited June 7, 2025]. Available from: https://www.rcn.org.uk/professional-development/publications/pub-007301.
10. Statistisches Bundesamt. Unfälle und Gewaltvorfälle in Pflege- und Gesundheitsberufen [Internet]. Wiesbaden: Destatis; 2021 [cited June 7, 2025]. Available from: https://www.destatis.de.
11. Dutch Healthcare Authority. Healthcare sector safety and aggression reports [Internet]. Utrecht: NZa; 2020 [cited June 7, 2025]. Available from: https://www.nza.nl.
12. European Centre for Disease Prevention and Control. Recommendations for Preparedness Planning for Public Health Threats []. Stockholm: ECDC; 2025. doi:10.2900/7416543.
13. International Federation of Red Cross and Red Crescent Societies. Guidance on Law and Public Health Emergency Preparedness and Response. [Internet]. Geneva: IFRC; 2021 [cited 2025 Jun 7]. Available from: https://disasterlaw.ifrc.org/sites/default/files/media/disaster_law/2021-09/Guidance%20on%20Law%20and%20PHE%20Preparedness%20and%20Response%20-%20Pilot%20Version%20%28FINAL%29.pdf.
14. World Health Organization. Hospital emergency response checklist: an all-hazards tool for hospital administrators and emergency managers [Internet]. Geneva: WHO; 2011 [cited June 7, 2025]. Available from: https://www.who.int/docs/default-source/documents/publications/hospital-emergency-response-checklist.pdf.
15. Centers for Medicare & Medicaid Services. Ambulatory Surgical Center (ASC) Payment [Internet]. Baltimore (MD): CMS; 2024 [cited 2025 Jun 7]. Available from: https://www.cms.gov/medicare/payment/prospective-payment-systems/ambulatory-surgical-center-asc.
16. World Health Organization. Primary health care: closing the gap between public health and primary care through integration [Internet]. Geneva: World Health Organization; 2018 [cited June 7, 2025]. Available from: https://iris.who.int/handle/10665/326458iris.who.int+2.
17. Jekl J, Jánský J. Geographical Distribution Analysis of Field Hospitals Along the Frontline: 2SFCA method-based approach. In: Bekesiene S, editor. Challenges to National Defence in Contemporary Geopolitical Situation. Vol. 4. Brno: General Jonas Zemaitis Military Academy of Lithuania; 2024: 403–410. doi:10.3849/cndcgs.2024.403.
18. Jekl J, Jánský J. Composite index for 2SFCA based accessibility comparison and field hospitals distribution analysis along the frontline. Adv Mil Technol. 2025;19(2):329–344. doi:10.3849/aimt.01910
19. Ferreira DC, Vieira I, Pedro MI, Caldas P, Varela M. Patient satisfaction with healthcare services and the techniques used for its assessment: a systematic literature review and a bibliometric analysis. Healthcare. 2023;11(5):639. doi:10.3390/healthcare11050639
20. Jekl J, Jánský J. Security challenges and economic-geographical metrics for analyzing safety to achieve sustainable protection. Sustainability. 2022;14(22):15161. doi:10.3390/su142215161
21. Saaty TL. The Analytic Hierarchy Process: Planning, Priority Setting, Resource Allocation. New York: McGraw-Hill; 1980. ISBN 10:70543712.
22. Donegan HA, Dodd FJ. A note on Saaty’s random indexes. Math Comput Model. 1991;15(10):135–137. doi:10.1016/0895-7177(91)90098-R
23. Benítez J, Izquierdo J, Pérez-García R, Ramos-Martínez E. A simple formula to find the closest consistent matrix to a reciprocal matrix. Appl Math Model. 2014;38:3968–3974. doi:10.1016/j.apm.2014.01.007
24. Agency for Healthcare Research and Quality. CAHPS Ambulatory Care Improvement Guide [Internet]. Rockville (MD): AHRQ; [cited July 6, 2025]. Available from: https://www.ahrq.gov/cahps/quality-improvement/improvement-guide/improvement-guide.html.
25. OECD. Health at a Glance 2023: OECD Indicators [Internet]. Paris: OECD Publishing; 2023. [cited June 7, 2025]. doi:10.1787/7a7afb35-en
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.