Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Enhanced Nursing Care for Improving the Self-Efficacy & Health-Related Quality of Life in Patients with a Urostomy
Received 22 October 2022
Accepted for publication 10 January 2023
Published 29 January 2023 Volume 2023:16 Pages 297—308
DOI https://doi.org/10.2147/JMDH.S394515
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Tian Zhang,1 Xiangxiu Qi2
1The First Internal Medicine Comprehensive Ward, Shengjing Hospital of China Medical University, Shenyang, People’s Republic of China; 2Department of Nursing, Shengjing Hospital of China Medical University, Shenyang, People’s Republic of China
Correspondence: Xiangxiu Qi, Department of Nursing, Shengjing Hospital of China Medical University, No. 36 Sanhao Street, Heping District, Shenyang City, Shenyang, 110004, People’s Republic of China, Email [email protected]
Background: Bladder cancer is the most predominant cancer of the lower urinary tract and is the most common cause for urostomy or urinary diversion. Urostomy immensely affect the patient’s everyday life from minor physical activity to social relations. Nurse-led interventions have been evaluated for improvement in quality of life in patients with urostomy.
Objective: The main objective of this study was to review the medical literature in a systematic way to evaluate the nursing role in improving the health-related quality of life of patients undergoing urostomy.
Methods: A systematic search of the PubMed, CINAHL, Embase, and Science Direct databases was carried out to identify studies that have evaluated the effect of nurse-led intervention on the self-efficacy and health-related quality of life in patients with urostomy. In addition, studies for factor affecting the quality of life were also investigated.
Results: Overall, 10 studies were identified as suitable for inclusion in this review. Health-related quality of life was lower in these patients as compared to population norms and several factors such as age, employment, and living status were identified as the contributing factors. Preoperative education was critical in meeting the psychological needs while postoperative intervention was instrumental in improving the self-efficacy and health-related quality of life particularly when a continued nursing-patient interaction was existent.
Conclusion: A comprehensive nurse-led intervention consisting of preoperative and postoperative components aimed at ostomy-related education, psychological counseling and compliant with patient factors is feasible and may result in greater improvement in self-efficacy and health-related quality of life in patients with urostomy. Larger clinical trials are warranted to validate these results.
Keywords: bladder cancer, nursing, urostomy education, quality of life, perioperative care
Introduction
Stoma is a surgical opening of an organ to communicate with the outside of the body to facilitate the excretion of waste products (faeces or urine) from the body.1 Ostomy is usually performed in patients with malignancy and other benign conditions, such as trauma, obstruction, ischemia, and inflammatory diseases.2,3 The most common types of stoma include the colostomy, ileostomy, and urostomy; and the most common causes for these ostomies in respective order are colorectal cancer, inflammatory bowel disease and bladder cancer.3,4 Bladder cancer is the most predominant cancer of the lower urinary tract and depending on the presentation its therapeutic management may involve surgery (transurethral resection or radical cystectomy), radiation therapy, chemotherapy, and immunotherapy in the form of immune checkpoint blockade and intravesical immunotherapy also termed as BCG (bacillus Calmette-Guérin).5–7 Radical cystectomy is offered when bladder cancer invades the muscle wall and is termed as muscle-invasive bladder cancer (MIBC).5–7 In such instance, a urinary diversion or urostomy is created for urine to leave the body.7,8 Urinary diversions are of three types including incontinent conduit (IC), continent cutaneous diversion (CCD), and orthotopic neobladder (ONB).8 In incontinent conduit (IC), urine is emptied into an ostomy bag via a stoma on the abdominal wall while an intermittent catheterization of the stoma is required in the continent cutaneous diversion (CCD). In ONB surgery involves the creation of a pouch in the pelvis constructed from a portion of the small bowel and anastomosed to the urethra to allow normal micturition.8
Urostomy, or stoma in general, immensely affect the patient’s everyday life from minor physical activity to social relations.4 Various factors, such as loss of control over the urine elimination, pouch leaks, bad odor, flatulence, not only can negatively influence the self-esteem and confidence of the patients but also compromise the social well-being.9–12 Moreover, proper functioning needs continued care for several physiological reasons including skin inflammation, electrolyte imbalances, stoma necrosis and parastomal hernias, and retraction or prolapse.13,14 In a study interviewing 11 patients living with urostomy identified six themes that described their perception of the major concerns including 1) surgery impact, 2) body image, 3) daily and social-life activities, 4) stoma and sexuality, 5) managing stoma education, 6) family and friends’ support.15 Hence, enhanced nursing care and nursing-patient interaction based on the scientific research is essential to assist these patients and achieve a better quality of life. To address this issue, we have carried out a systematic review of the literature to highlight the recent updates in the nursing management of urostomy and reflect on the progress in this regard.
Methods
This systematic-review and meta-analysis was carried out following the updated version 2020 of PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (Supplementary Table 1).16
Eligibility Criteria
Target Population and Treatment
Patients with urostomy who were administered with preoperative or postoperative nursing care or nurse-led education programs.
Outcome of Interest
Main outcome of this study included the improvement in the self-efficacy or quality of life of patients with urostomy. Other outcomes included individual and treatment-related factors adversely affecting the quality of life for which studies published between 2012 and 2022 were considered.
Study Design and Language Restrictions
Only studies with prospective, cross-sectional, and descriptive designs, as well as, randomized clinical trials were included. Studies with retrospective designs, case studies, conference abstracts, letters to the editor, literature reviews, and systematic reviews and meta-analysis were excluded. Only studies published in English were included.
Research Strategy and Study Selection
PubMed, CINAHL, Embase, and Science Direct were formally searched with several key terms until June 30, 2022. The following search terms were used singularly or in combination in all fields: “urostomy”, “urinary diversion”, “nursing care”, “nursing-led education program” and “quality of life” (Supplementary Table 2). Further potential studies were identified through screening references of relevant articles. A step-wise procedure comprising retrieving, organizing, and screening was followed by two reviewers to select studies meeting the eligibility criteria. Disagreements were solved after mutual consultation.
Data Extraction and Synthesis
Characteristics of the included studies and attributes of participants were extracted that included first author, publication year, study design, number and type of participants, details of intervention and quality of life assessment. Participants’ attributes included age, gender, disease type, married status, and type of urinary diversion. The extracted data were transformed into a table form.
Results
Initial database search with key terms identified 562 studies. Interestingly, PubMed database search with key term “urostomy” only identified 342 studies. The number of studies per year on the topic only reached to a maximum of 24 studies in 2021 (Figure 1). Screening for title and abstract and duplicates removed 552 studies. Further scrutiny for eligibility criteria resulted in the final selection of 11 studies (n = 871) including 5 randomized controlled trials (RCT) for qualitative analysis (Figure 2). Bladder cancer patients constituted the majority of the participants (85%) followed by prostate cancer (10%) (Figure 3). The most common type of urinary diversion was the construction of an ileal conduit (91%) followed by neobladder (4%) (Figure 4). Male was the predominant gender type constituting between 71% and 93% of the study participants. Mean age ranged between 63.25 and 73.6 years old. Detailed characteristics are outlined in Table 1. Characteristic details of intervention and assessment are summarized in Tables 2 and 3.
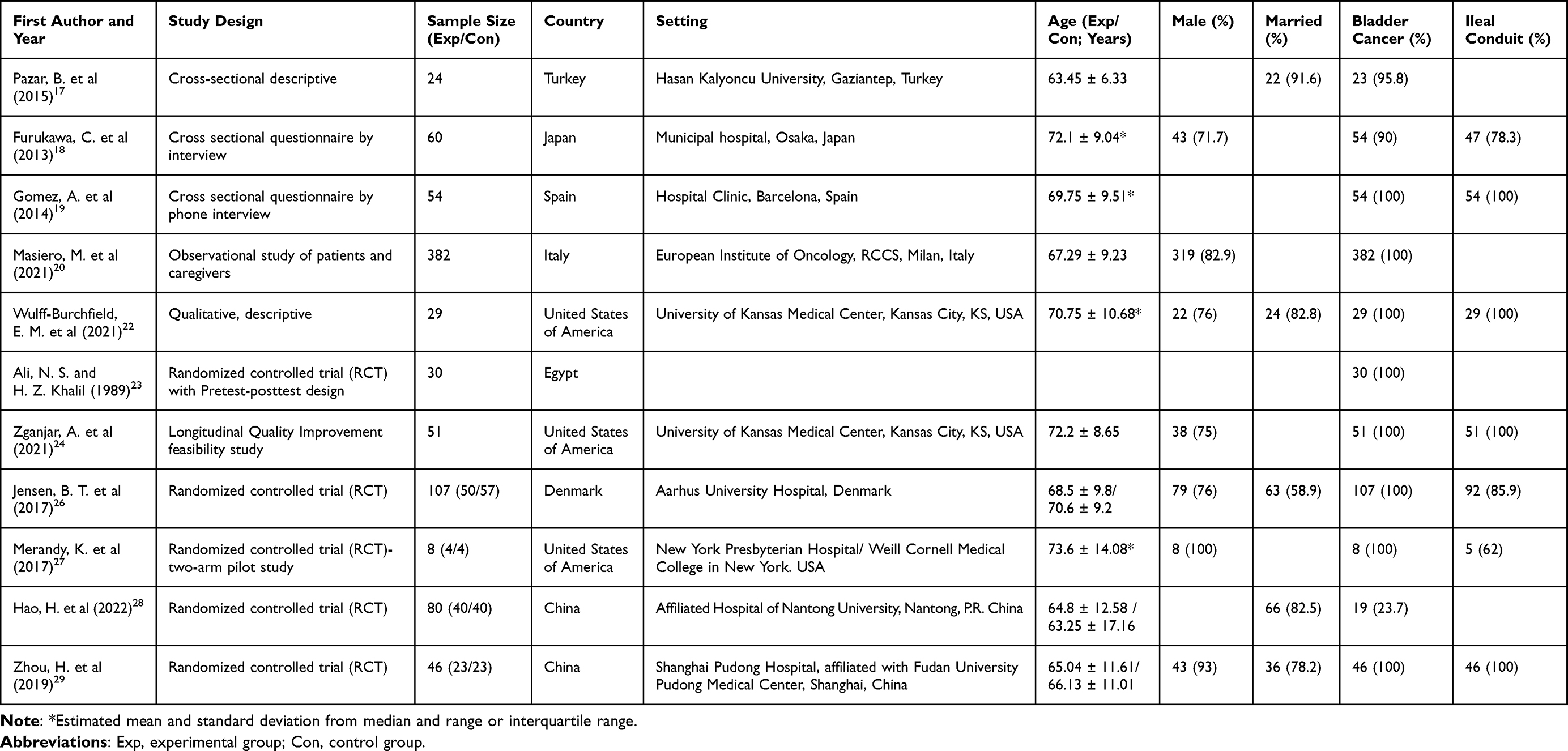 |
Table 1 General Characteristics of Studies and Participants |
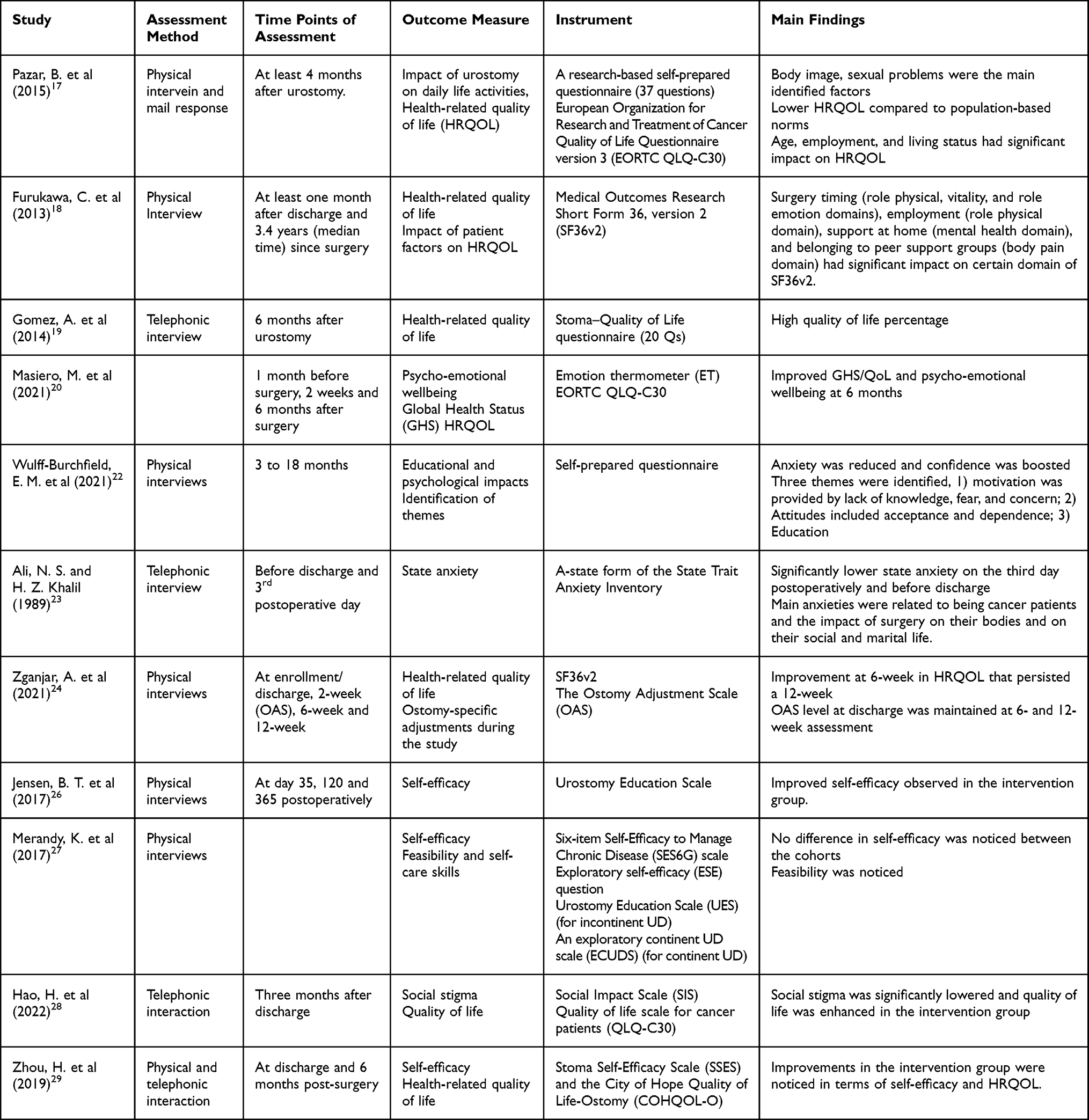 |
Table 2 Outcome Assessment and Main Findings |
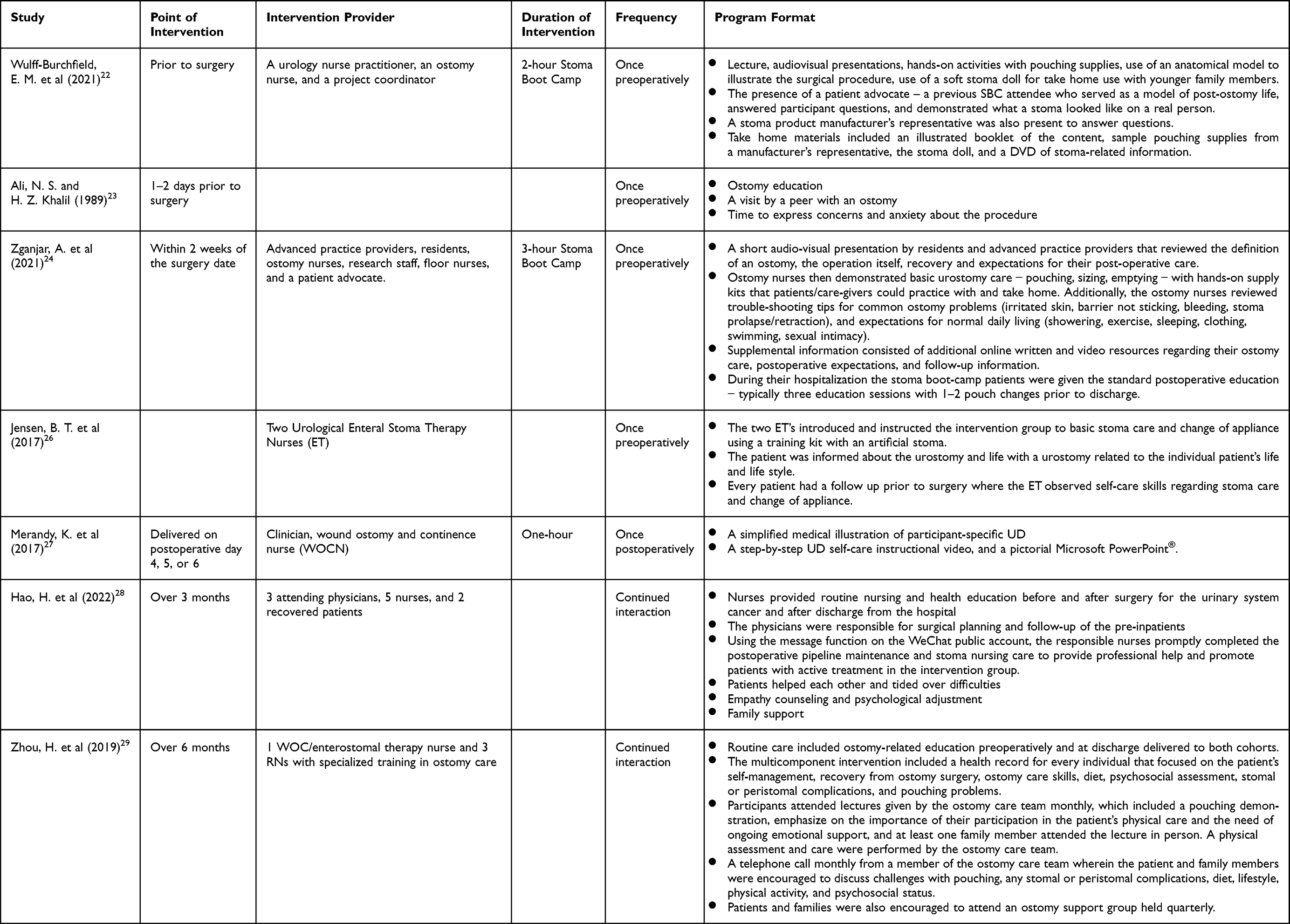 |
Table 3 Intervention Details |
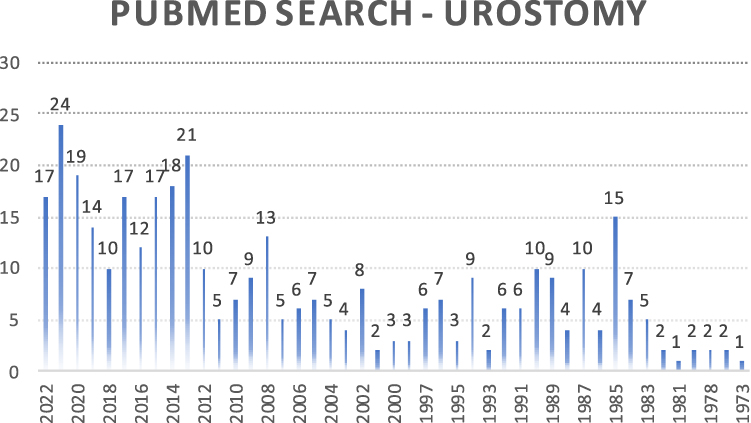 |
Figure 1 PubMed search outcome with key term “Urostomy” from 1973 to 2022. |
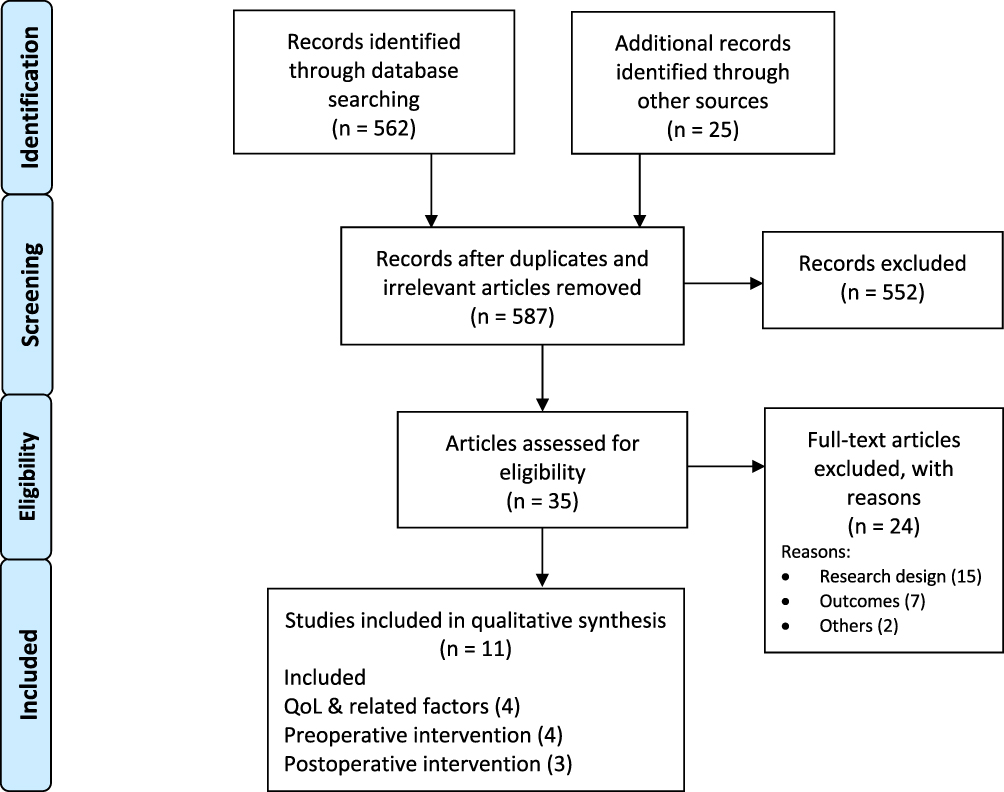 |
Figure 2 Research strategy and study selection. |
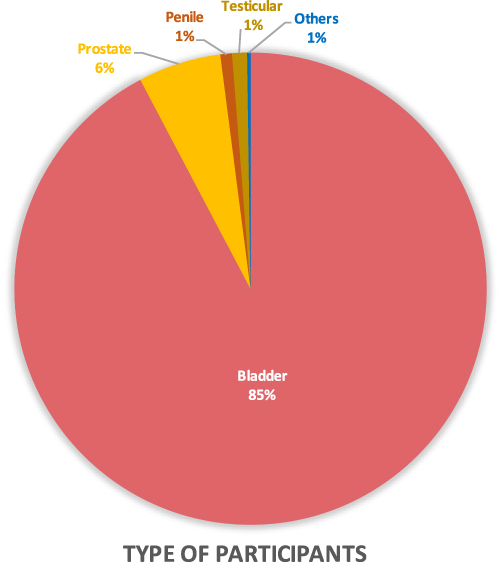 |
Figure 3 Primary disease of the participants. |
 |
Figure 4 Type of urinary diversion constructed for participants. |
Factors Affecting Health-Related Quality of Life (HRQOL)
Assessment of quality of life in patients living with a urostomy is an essential tool to determine the overall level of satisfaction of the patients with the treatment (surgical procedure and nursing care), and, in doing so, could also identify the various factors that are negatively affecting their health-related quality of life. Moreover, determining the patients’ problems can provide essential assistance in designing appropriate nursing approaches and education programs. A cross-sectional descriptive study involving 24 patients with urostomy, who were interviewed at least four months after urostomy, revealed that life-style factors affected by urostomy included dressing habits (83.4%), sleep patterns (91.7%), family life (91.7%), participation in social activities (91.7%), and occupation (75.0%).17 Body image and sexual relationship were identified as the main concerns in these patients. Health-related quality of life, as determined by EORTC-QLQ-C30 scores, demonstrated lower mean scores for general wellness, functional condition, and symptomatic condition domains (54.16 ± 15.29, 44.07 ± 9.62, and 64.31 ± 12.56, respectively) in comparison to the population-based norms.17 Age (>65 and ≤65; Symptomatic condition: 67.20 vs 55.98; p < 0.05), working status before operation (Yes and No; Functional condition: 46.37 vs 41.77; p < 0.05), and living status (alone, wife, and wife and children) had significant influence on the functional condition and symptomatic condition domain of the EORTC-QLQ-C30. Patients living alone performed better on symptomatic condition domain as compared to those who were living with their spouse or spouse and children both (mean scores: 75.42 versus 67.09 versus 50.64; p < 0.05). A rather opposite situation was apparent for the functional condition domain of the EORTC-QLQ-C30 (mean scores: 31.85 versus 42.07 versus 44.29; p < 0.05).17
Another study conducted in Japan also reported HRQOL in patients living with urostomy based on the 8 domains of the Medical Outcomes Research Short Form 36, version 2 (SF36v2).18 Only the body pain domain exceeded the mean 50 score (standard mean score) indicating better quality in this domain. Bladder cancer patients undergoing urostomy reported significantly higher score on the social function domain compared to urostomies performed for other causes (47.8 ± 9.8 vs others 35.7 ± 10.8; P<0.01). Significantly lower mental health domain score was associated with presence of a support person at home (yes: 41.8 ± 8.8 vs no: 46.9 ± 8.; P<0.05), and participation in ostomy support groups was associated with a lower score on body pain domain (yes: 47.4 ± 11.7 vs no: 53.9 ± 7.4; P < 0.01). In this study, duration from the surgery was identified as a significant factor affecting the patient’s quality of life. In comparison to patients living with urostomy for more than four years, patients with urostomy who had surgery during the last four years demonstrated significantly lower health-related quality of life scores (role physical: <4 years: 42.9 ± 10.2 vs >4 years: 8.4 ± 9.7, p<0.05; vitality: <4 years 45.3 ± 8.1 vs >4 years 50.4 ± 7.9, p<0.01; role emotion: <4 years 42.8 ± 10.0 vs >4 years 48.8 ± 9.0, p<0.001).18 Similarly, HRQOL assessed with Stoma–Quality of Life questionnaire by telephone 6 months after urostomy surgery was ranked as good by 95% of the participants (mean score 68.54, range 64–73).19 It appears that the patients with urostomy interviewed within short period of time following urostomy demonstrate a low HRQOL. Correspondingly, global health status/quality of life (GHS/QoL) was recovered to pre-hospitalization level at 6 months (T2) after an initial decline at 2 weeks after surgery (T1) in a study involving bladder cancer patients undergoing urostomy and neobladder (GHS/QoL: T0: 71.61 ± 20.89; T1 62.91 ± 19.98; T2: 75.66 ± 19.12).20 Overall, a general improvement in the HRQOL and global health status/QoL from T0 (1 month before surgery) to T2 was demonstrated (p < 0.001).20 It is suggested that patients face difficulty in the early post-surgery period in adjusting to the new life but with time they acquire knowledge, expertise and acceptance permitting them to more independence.21 Nonetheless, patients were in contact with nurse during these 6 months and 32 out of 35 respondents (91.4%) contacted or visited the ostomy nurse’s office at least once, which may have had a positive impact on their life quality as well.19 Moreover, distinct questionnaires were used in these studies which may have an impact on the overall outcome of these studies.
Preoperative Nurse-Led Interventions
There have been very few studies on the efficacy of nurse-led education interventions programs in the management of bladder cancer patients with urostomy. A qualitative study aimed at improving the self-management and post-ostomy life of bladder cancer patients was carried out by Wulff-Burchfield et al at the University of Kansas Health System (KUHS) Urology Department.22 The Stoma Bootcamp (SBC) education program, developed by a team of specialists including a urology nurse practitioner, an ostomy nurse, and a project coordinator, comprised of important components such as psychosocial care, pre-operative timing, and lay and peer teachers with the goal of improving patients’ and caregivers’ abilities to care for the stoma physically and psychologically. Overall, 16 patients, 18 caregivers and 3 program educators completed the interviews from 3 to 18 months post-program. In general, the SBC program was well received and termed as effective and timely by patients whose expectations of post-ostomy life were transformed from anxiety to that of confidence. Unfortunately, no quantitative data was provided regarding the efficacy of the education program. Nonetheless, lack of knowledge, fear and concern about the procedure were cited as motivation for the education program participation, which suggest the need for such programs to be performed preoperatively as well. In coherence with the first study, an RCT with pretest-posttest design conducted by Ali and Khalil involving Egyptian patients with urinary diversion demonstrated quantitative evidence of benefit in the postoperative anxiety levels in the experimental group at discharge and on day 3 postoperatively (p < 0.05).23 The study also identified the main anxiety contributors, which included being cancer patients and the impact of surgery on their bodies and on their social and marital life. The study was aimed at assessing the effects of a preoperative psycho-educational training program on the postoperative anxiety levels, which consisted of ostomy education, a visit by a peer with an ostomy, and time to express concerns and anxiety about the procedure. These outcomes indicate that preoperative stoma education programs can successfully lower the anxiety levels of the patients by improving their knowledge about the procedure and self-management.
A recent longitudinal and quality-improvement feasibility study performed at the University of Kansas Health System evaluated the efficacy of a preoperative “stoma boot camp”, a 3-hour group session within 2 weeks of the surgery date, on the health-related quality of life of bladder cancer patients scheduled for radical cystectomy with ileal conduit formation (RCIC).24 The education content included a short presentation regarding the procedure, recovery and expectations for their post-operative care by residents and advanced practice providers. Moreover, basic urostomy care was demonstrated by ostomy nurses that comprised of pouching, sizing, emptying and trouble-shooting tips for common ostomy problems. The patients (n = 51) achieved an average ostomy adjustment score (OAS) of 150.4 (95% CI 142.0, 158.8) at discharge which showed no decline over a 12-weeks duration. Numerical improvements in the Short-form 36 (SF-36) scores were also observed in each category at 6 week which persisted at the 12-week mark. Although the categorical scores were higher to published population norms (for SF-36 scores for US general population), the study lacked a direct control group and hence no comparative efficacy superiority of the program can be established.25 In a recently concluded RCT, bladder cancer patients in the intervention group showed a significantly better stoma self-care (2.7 [95% CI: 0.9; 4.], 4.3 [95% CI: 2.1; 6.5] and 5.1 [95% CI: 2.3; 7.8] at day 35, 120 and 365 postoperatively) measured on “The Urostomy Education Scale” as compared to standard.26 In their study, the intervention group was instructed to a preoperative standardized stoma-education program that consisted of areas recognized necessary to change a stoma appliance. This is the first study to report a positive efficacy of a short-term preoperative stoma intervention based on the RCT-design.
Postoperative Nurse-Led Interventions
Postoperative efficacy of nurse-led education programs has been well established in stoma patients; however, there were not many studies in the urostomy cohorts evaluating the postoperative efficacy. In a two-arm randomized controlled trial, self-efficacy (SE) or self-care in patients with bladder cancer requiring urinary diversion (UD) was investigated based on the intervention of a supplemental multimethod educational program.27 Study reported no difference in self-care independence (p = 0.4286) between the treatment arms assessed with Six-item Self-Efficacy to Manage Chronic Disease (SES6G) scale, and no change in pre- versus post-SES6G score in the intervention group (p = 0.125) was noticed. Only two participants from the control group demonstrated self-care independence in the entire sample. It must be pointed out that the control group was younger in age which further stresses the point that age is an important factor in determining the outcome of such educational programs and must be taken into consideration in designing these educational programs. Nonetheless, feasibility and acceptability were shown for integration of such programs in these patients. Moreover, a need for ongoing post-discharge support and education support was noted. In another randomized controlled trial involving 80 urinary system cancer patients, the effects of a nurse-led education program via an online interactive platform “Wechat” for education of patients with urostomy was evaluated.28 Intervention group was provided with psychological intervention as compared to the control group who received routine nursing care. The Chinese version of social impact and quality of life scales were used which indicated a significantly lower score for stigma (p < 0.01) and higher score for quality of life in the observation group (p < 0.01). A third randomized controlled trial using the Chinese language versions of the Stoma Self-Efficacy Scale (SSES) and the City of Hope Quality of Life-Ostomy (COHQOL-O) questionnaire assessed the effect of a nurse-led multicomponent intervention on ostomy-related complications, self-efficacy, and health-related quality of life in 46 patients who underwent radical cystectomy with an ileal conduit.29 Results indicated significant decrease in the incidence of complications at 6 months (4.35% vs 30.43%, P = 0.047). Additionally, greater self-efficacy in stoma care (107.13 ± 11.87 vs 85.65 ± 12.87, P = 0.000) and higher health-related quality of life (154.48 ± 16.01 vs 138.26 ± 13.42, P = 0.001) were also indicated.
Discussions
In this study, we have reviewed the medical literature in a systematic way to rationalize the need for perioperative care in patients undergoing urostomy in order to improve their health-related quality of life. The literature research yielded very limited results indicating that this particular group of patients is neglected, which stresses the need for more robust attention. Health-related quality of life was lower in these patients as compared to population norms and several factors, such as age, employment and living status, were identified as the contributing factors. Preoperative education was critical in meeting the psychological needs while postoperative intervention was instrumental in improving the self-efficacy and health-related quality of life particularly when a continued nursing-patient interaction was existent.
Our study identified three major essential components for designing a comprehensive nurse-led education program (Figure 5). The main component of ostomy education intervention, which was constant across studies, was the ostomy-related care skills education that consisted of oral and practical presentation.22–24,26–29 The results indicated that both preoperative and postoperative intervention are helpful tools in improving the self-care skills and HRQOL in the intervention group as compared to patients receiving routine care.26–29 It could be debated whether the combination of two periods might further enhance the outcomes of these interventions? For example, post-operative period is essential as the patients had just undergone the surgery and they might be vulnerable and in need of assistance. Intervention at this stage can improve their confidence and self-care skills; however, patients’ compliance can be an issue to select the right window period for intervention.27 On the other hand, preoperative period might be vital as stoma-related care skills could be practiced on a mannequin in advance. In doing so, dexterity of the participants could also be assessed and, hence, vulnerable participants could be identified who need more attention.27 Moreover, patients have demonstrated augmented motivation before the procedure driven by lack of knowledge about the procedure which could further improve participation.22 Therefore, preoperative period can be the right time for ostomy-related educational intervention. Post-operative period can be rather essential for continued care through nursing-patient interaction as has been demonstrated in these studies.28–30 In fact, postoperative intervention has been critical in the prevention of stoma-related complications which has shown to affect the HRQOL adversely.21,29,30 Moreover, timing of assessment is also critical as early (few weeks) and late (6 months onwards) assessment may influence the outcome of interventions.18,20 Hence, multiple assessment points may be necessary to measure the efficacy of interventions and further detect inadequacies.
 |
Figure 5 Triangle of Perioperative care for patients with urostomy. Three major ingredients include ostomy-related education, psychological counseling and patient’s factors. Point of intervention starts from preoperative to postoperative in the form continued care to enhance the self-efficacy and quality of life in these patients. |
In this study, two main problems that may be alleviated with psychological counseling were the body image and sexual relationship.17 Body image is the self-perception of one’s physical well-being in terms of attractiveness and function and its disturbance can be manifested in the form of dissatisfaction, concern, and distress.12,31 Stoma patients have been reported for experiencing a negative body image, particularly in patients with younger age, overweight, and temporary stoma.9–12,32 Psychological counseling of the patients and family members in this regard could be an essential tool to cope with the discomfort and boost their self-confidence. In fact, psycho-emotional wellbeing of the caregivers has also been associated with global health status and quality of life of the patients.20 Therefore, improving the psycho-emotional wellbeing of primary caregivers might boost QoL in patients. Another severely affected aspect of urostomy on patients is their dysfunctional sexual life. Sexual problems experienced by the patients include no desire, erectile dysfunction, anorgasmia in female, and even inability to generate a penile erection.10,17
Identification of vulnerable patients who might need special consideration and attention should be carried before the initiation of intervention. Three main factors that were identified contributing to various aspects of the quality of life included age, living status, and employment status. Age (older participants) had significant impact on the patient’s dexterity affecting self-care independence but was associated with enhanced acceptance.17,21 Age (younger participants) was also identified as contributing factor to the negative perception of body image.18 Hence, different age groups would require special kind of consideration in terms of education and psychological counseling. Similarly, patients with previous employment may face difficulty in coping with the new life as compared to the ones with no previous employment.17 Therefore, differential psychological input would be desirable to assist such patients. Living status (alone, with wife, or wife and children) has also demonstrated to differentially affect the outcomes of quality of life scores.17,18
Several factors limit the outcomes of outcomes of our study. The studies included were from diverse geo locations and some consisted of small number of participants. There was no detailed information about the type of urinary diversion. Moreover, distinctive instruments were employed to assess self-efficacy and health-related quality of life. Likewise, the point of assessments also varied from study to study.
Conclusions
Urostomy enormously affect the quality of life which can be improved via preoperative nurse-led personalized education consisting of physical and psychological components with a postoperative continued and planned interactive educational course respecting the patients’ needs. Our study emphasizes the need for a comprehensive structured perioperative educational program led by nurses to adequately support the patients with urostomy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hyland J. The basics of ostomies. Gastroenterol Nurs. 2002;25(6):241–4; quiz 4–5. doi:10.1097/00001610-200211000-00003
2. Mo J, Wendel CS, Sloan JA, et al. Stoma location and ostomy-related quality of life among cancer survivors with ostomies: a pooled analysis. Am J Surg. 2022;223(5):963–968. doi:10.1016/j.amjsurg.2021.09.023
3. Golicki D, Styczen P, Szczepkowski M. Quality of life in stoma patients in Poland: multicentre cross-sectional study using WHOQOL-BREF questionnaire. Przegl Epidemiol. 2013;67(3):491–6, 589–93.
4. Dabirian A, Yaghmaei F, Rassouli M, Tafreshi MZ. Quality of life in ostomy patients: a qualitative study. Patient Prefer Adherence. 2010;5:1–5. doi:10.2147/PPA.S14508
5. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
6. Saginala K, Barsouk A, Aluru JS, Rawla P, Padala SA, Barsouk A. Epidemiology of bladder cancer. Med Sci. 2020;8(1):15.
7. Lenis AT, Lec PM, Chamie K, Mshs MD. Bladder cancer: a review. JAMA. 2020;324(19):1980–1991. doi:10.1001/jama.2020.17598
8. Lee RK, Abol-Enein H, Artibani W, et al. Urinary diversion after radical cystectomy for bladder cancer: options, patient selection, and outcomes. BJU Int. 2014;113(1):11–23. doi:10.1111/bju.12121
9. Jenks JM, Morin KH, Tomaselli N. The influence of ostomy surgery on body image in patients with cancer. Appl Nurs Res. 1997;10(4):174–180. doi:10.1016/S0897-1897(97)80548-4
10. Kiliç E, Taycan O, Belli A, Ozmen M. The effect of Permanent Ostomy on Body Image, Self-Esteem, Marital Adjustment, and Sexual Functioning. Turk J Psychiatry. 2007;18(4):302–310. Turkish.
11. Hong KS, Oh BY, Kim EJ, Chung SS, Kim KH, Lee RA. Psychological attitude to self-appraisal of stoma patients: prospective observation of stoma duration effect to self-appraisal. Ann Surg Treat Res. 2014;86(3):152–160. doi:10.4174/astr.2014.86.3.152
12. Jayarajah U, Samarasekera DN. Psychological adaptation to alteration of body image among stoma patients: a descriptive study. Indian J Psychol Med. 2017;39(1):63–68. doi:10.4103/0253-7176.198944
13. Babakhanlou R, Larkin K, Hita AG, Stroh J, Yeung SC. Stoma-related complications and emergencies. Int J Emerg Med. 2022;15(1):17. doi:10.1186/s12245-022-00421-9
14. Bafford AC, Irani JL. Management and complications of stomas. Surg Clin North Am. 2013;93(1):145–166. doi:10.1016/j.suc.2012.09.015
15. Villa G, Manara DF, Brancato T, et al. Life with a urostomy: a phenomenological study. Appl Nurs Res. 2018;39:46–52. doi:10.1016/j.apnr.2017.10.005
16. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. PLoS Med. 2021;18(3):e1003583. doi:10.1371/journal.pmed.1003583
17. Pazar B, Yava A, Başal Ş. Health-related quality of life in persons living with a urostomy. J Wound Ostomy Continence Nurs. 2015;42(3):264–270. doi:10.1097/WON.0000000000000110
18. Furukawa C, Sasaki Y, Matsui K, Morioka I. Health-related quality of life and its relevant factors in Japanese patients with a urostomy. J Wound Ostomy Continence Nurs. 2013;40(2):165–170. doi:10.1097/WON.0b013e31827e8339
19. Gomez A, Barbera S, Lombraña M, Izquierdo L, Baños C. Health-related quality of life in patients with urostomies. J Wound Ostomy Continence Nurs. 2014;41(3):254–256. doi:10.1097/WON.0000000000000026
20. Masiero M, Busacchio D, Guiddi P, et al. Quality of life and psycho-emotional wellbeing in bladder cancer patients and their caregivers: a comparative analysis between urostomy versus ileal orthotopic neobladder. Ecancermedicalscience. 2021;15:1163. doi:10.3332/ecancer.2021.1163
21. Cerruto MA, D’Elia C, Cacciamani G, et al. Behavioural profile and human adaptation of survivors after radical cystectomy and ileal conduit. Health Qual Life Outcomes. 2014;12:46. doi:10.1186/1477-7525-12-46
22. Wulff-Burchfield EM, Potts M, Glavin K, Mirza M. A qualitative evaluation of a nurse-led pre-operative stoma education program for bladder cancer patients. Support Care Cancer. 2021;29(10):5711–5719. doi:10.1007/s00520-021-06093-0
23. Ali NS, Khalil HZ. Effect of psychoeducational intervention on anxiety among Egyptian bladder cancer patients. Cancer Nurs. 1989;12(4):236–242. doi:10.1097/00002820-198908000-00006
24. Zganjar A, Glavin K, Mann K, et al. Intensive preoperative ostomy education for the radical cystectomy patient. Urol Oncol. 2021;40:11481–11486.
25. Ware JE. SF-36 Health Survey: Manual and Interpretation Guide Health Institute. England Medical Center; 1993.
26. Jensen BT, Kiesbye B, Soendergaard I, Jensen JB, Kristensen SA. Efficacy of preoperative uro-stoma education on self-efficacy after radical cystectomy; secondary outcome of a prospective randomized controlled trial. Eur J Oncol Nurs. 2017;28:41–46. doi:10.1016/j.ejon.2017.03.001
27. Merandy K, Morgan MA, Lee R, Scherr DS. Improving self-efficacy and self-care in adult patients with a urinary diversion: a pilot study. Oncol Nurs Forum. 2017;44(3):E90–E100. doi:10.1188/17.ONF.E90-E100
28. Hao H, Yang X, Zhu H, Wang Z, Zhang H, Huang C. Effect of the whole seamless connection of nursing from WeChat interactive platform on stigma and quality of life in patients with urinary system cancer. Digit Health. 2022;8:20552076221102772. doi:10.1177/20552076221102772
29. Zhou H, Ye Y, Qu H, Zhou H, Gu S, Wang T. Effect of ostomy care team intervention on patients with ileal conduit. J Wound Ostomy Continence Nurs. 2019;46(5):413–417. doi:10.1097/WON.0000000000000574
30. Jin Y, Tian X, Li Y, Jiménez-Herrera M, Wang H. Effects of continuous care on health outcomes in patients with stoma: a systematic review and meta-analysis. Asia Pac J Oncol Nurs. 2022;9(1):21–31. doi:10.1016/j.apjon.2021.12.006
31. McLellan A. Patient satisfaction: public engagement with service information is key test of choice. Health Serv J. 2012;122(6308):3.
32. Morrall SE. The shock of the new. Altered body image after creation of a stoma. Prof Nurse. 1990;5(10):529–537.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Fluid and Caffeine Management on Quality of Life in Older Women with Overactive Bladder in Rural Korea: A Pilot Study
Park J, Lee K, Lee K
Journal of Multidisciplinary Healthcare 2024, 17:1549-1559
Published Date: 10 April 2024
Caregiver Burden in Bladder Cancer Patients with Urinary Diversion Post-Radical Cystectomy and the Need for Comprehensive Nursing Education: A Narrative Literature
Zhang T, Qi X
Journal of Multidisciplinary Healthcare 2024, 17:3825-3834
Published Date: 7 August 2024
The Impact of Cognitive-Behavioral Intervention (CBI) on Enhancing Mental Health and Quality of Life in Lung Cancer Patients Undergoing Chemotherapy Nursing
Fan M, Wei X
Journal of Multidisciplinary Healthcare 2025, 18:3299-3309
Published Date: 8 June 2025