Back to Journals » International Journal of Nanomedicine » Volume 21
Engineering Nanocarriers for Dopamine Stabilization and Targeted Brain Delivery: Mechanisms, Approaches and Translational Challenges
Received 4 March 2026
Accepted for publication 9 June 2026
Published 12 June 2026 Volume 2026:21 606830
DOI https://doi.org/10.2147/IJN.S606830
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Yan Shen
Sandip Patra,1,2,* Aakash Nathani3,*
1Department of Chemistry, Hunter College, City University of New York, New York, NY, USA; 2Department of Chemistry, CUNY Graduate Center, New York, NY, USA; 3College of Pharmacy and Pharmaceutical Sciences, Florida A&M University, Tallahassee, FL, USA
*These authors have contributed equally to this work
Correspondence: Aakash Nathani, College of Pharmacy and Pharmaceutical Sciences, Florida A&M University, Tallahassee, FL, USA, Tel +1 850 559 3315, Email [email protected]; [email protected]
Abstract: Dopamine plays a central role in motor control, cognition, reward signaling, and neuroendocrine regulation, and its dysregulation is strongly associated with neurological disorders such as Parkinson’s disease. However, conventional dopaminergic therapies remain limited by poor blood–brain barrier (BBB) penetration, rapid systemic metabolism, short half-life, peripheral toxicity, and dopamine oxidation-induced neurotoxicity. Nanomedicine-based drug delivery systems have emerged as promising strategies to overcome these limitations by enhancing dopamine stability, improving BBB transport, enabling controlled release, and facilitating targeted delivery to dopaminergic brain regions. This review comprehensively summarizes current advances in dopamine-targeted nanotherapeutics, including polymeric nanoparticles, liposomes, solid lipid nanoparticles, dendrimers, inorganic nanoparticles, exosomes, and biomimetic vesicles. Particular emphasis is placed on the dual role of nanocarriers in both facilitating dopamine delivery and protecting dopamine from oxidative degradation and reactive oxygen species-associated toxicity. Among currently investigated platforms, polymeric nanoparticles, lipid-based nanocarriers, and exosome-inspired vesicles appear particularly promising due to their ability to improve dopamine stability, facilitate controlled release, enhance BBB penetration, and enable targeted brain delivery. The review additionally discusses receptor-mediated targeting strategies, intranasal delivery approaches, translational barriers, manufacturing scalability, long-term safety considerations, and regulatory challenges associated with clinical implementation. Finally, emerging future directions involving AI-assisted nanocarrier engineering, precision-targeted delivery systems, and stimuli-responsive nanomedicine are highlighted as promising approaches for the development of next-generation therapies for neurodegenerative disorders.
Keywords: dopamine, blood-brain barrier, nanomedicine, targeted drug delivery, dopamine receptors, neurodegenerative diseases
Introduction
Dopamine is a central neurotransmitter that regulates numerous physiological processes in the central nervous system, including motor control, motivation, cognition, reward processing, and neuroendocrine signaling. Dopaminergic neurons originate primarily in the midbrain and project through several major pathways, including the nigrostriatal, mesolimbic, mesocortical, and tuberoinfundibular systems. These circuits collectively coordinate voluntary movement, emotional behavior, reinforcement learning, and hormonal regulation. Because of this widespread functional role, disturbances in dopaminergic signaling are implicated in a broad spectrum of neurological and psychiatric disorders, including Parkinson’s disease, schizophrenia, attention deficit disorders, and substance addiction. As a result, dopaminergic pathways have long been a central focus of neuropharmacological research and therapeutic development.1–4
Despite decades of progress in dopaminergic pharmacology, achieving precise and sustained modulation of dopamine signaling remains a major therapeutic challenge.5 One of the fundamental difficulties arises from the intrinsic biochemical properties of dopamine itself. Dopamine contains a catechol moiety that is highly susceptible to oxidation under physiological conditions.6,7 Exposure to oxygen or reactive species readily leads to the formation of dopamine quinones and other reactive intermediates. These oxidative products not only reduce the availability of functional dopamine but may also contribute to neuronal damage through the generation of reactive oxygen species and oxidative stress. This inherent instability significantly limits the direct therapeutic use of dopamine. In addition to oxidative instability, dopamine is subject to rapid metabolic degradation. Enzymes such as monoamine oxidase and catechol-O-methyltransferase rapidly convert dopamine into inactive metabolites, tightly regulating its extracellular concentration within synaptic environments. While this metabolic control is essential for normal neurotransmission, it poses a substantial barrier to therapeutic intervention because exogenously administered dopamine is quickly degraded before reaching its target sites within the brain.8,9 Consequently, direct dopamine administration rarely produces sustained therapeutic effects when delivered systemically.10,11 Another major obstacle in dopaminergic therapy is the presence of the blood-brain barrier (BBB), a specialized physiological interface that tightly regulates the movement of molecules between the bloodstream and the brain. The BBB is composed of endothelial cells connected by tight junctions, supported by pericytes, astrocytes, and extracellular matrix components that together form the neurovascular unit. In addition, active efflux transporters such as P-glycoprotein and other ATP-binding cassette transporters further limit the accumulation of therapeutic molecules within the brain. As a result, the BBB remains one of the most significant barriers to effective treatment of central nervous system disorders.12,13
Because of these physiological constraints, most clinical strategies for dopaminergic therapy do not rely on direct dopamine administration. Instead, they utilize dopamine precursors or receptor-modulating drugs. The dopamine precursor levodopa remains the most widely used treatment for Parkinson’s disease because it can cross the BBB via amino acid transport systems and is subsequently converted into dopamine within the brain.14,15 Although levodopa therapy provides significant symptomatic relief, long-term treatment is frequently associated with complications such as motor fluctuations, dyskinesia, and reduced therapeutic responsiveness. Dopamine receptor agonists and antagonists are also commonly used to treat various neurological and psychiatric disorders, yet these drugs often exhibit limited receptor subtype selectivity and may interact with other G-protein-coupled receptors throughout the body. Such off-target interactions can produce undesirable systemic effects, including cardiovascular complications, metabolic disturbances, and neuropsychiatric symptoms.10 The widespread distribution of dopamine receptors throughout both central and peripheral tissues further complicates therapeutic intervention. Dopamine receptors belong to the G-protein-coupled receptor superfamily and are typically classified into D1-like and D2-like receptor families.1 These receptor subtypes regulate intracellular signaling pathways that influence neuronal excitability, synaptic plasticity, and gene expression. However, the broad expression of these receptors across multiple organ systems means that systemic administration of dopaminergic drugs can lead to unintended physiological effects outside the brain. Achieving selective targeting of dopaminergic pathways therefore requires not only improved pharmacological selectivity but also delivery strategies that enable spatial control of drug distribution within the body.
In recent years, nanomedicine has emerged as a promising approach to overcome many of the biological and pharmacological barriers associated with dopamine therapy. Nanocarrier systems offer several advantages that are particularly relevant for central nervous system drug delivery. By encapsulating dopamine or dopaminergic drugs within nanoscale structures, these systems can protect unstable molecules from enzymatic degradation and oxidative damage during systemic circulation. Nanocarriers can also be engineered to provide controlled or sustained drug release, allowing more stable therapeutic concentrations in target tissues. Importantly, nanoparticles can be designed to interact with specific transport pathways across the BBB, enabling enhanced penetration of therapeutic agents into the brain. Advances in nanotechnology have led to the development of a wide range of nanoscale delivery platforms with distinct physicochemical properties and therapeutic capabilities.16–18 Polymeric nanoparticles composed of biodegradable materials can provide controlled release and improved drug stability. Liposomes and lipid-based nanocarriers offer excellent biocompatibility and efficient encapsulation of both hydrophilic and lipophilic molecules. Dendrimers provide highly tunable surface chemistry that allows multivalent targeting and functionalization. Inorganic nanoparticles offer unique optical and magnetic properties that enable simultaneous therapeutic delivery and imaging. More recently, biologically derived nanocarriers such as extracellular vesicles and exosomes have gained attention for their ability to naturally cross biological barriers and deliver therapeutic cargo to neuronal cells. Beyond improving drug stability and brain penetration, nanomedicine platforms also enable more sophisticated therapeutic strategies. Targeted nanoparticles can be functionalized with ligands that recognize receptors expressed on brain endothelial cells, facilitating receptor-mediated transport across the BBB.19 Intranasal nanoparticle delivery has also emerged as a promising non-invasive strategy for bypassing the BBB through olfactory and trigeminal nerve pathways. Furthermore, multifunctional nanomaterials can integrate therapeutic and diagnostic capabilities, enabling nanotheranostic systems that monitor drug distribution and treatment response in real time. These innovations highlight the growing potential of nanotechnology to transform the treatment of neurological disorders by enabling more precise and efficient modulation of dopaminergic signaling. Despite encouraging experimental outcomes, most dopamine-targeted nanomedicine approaches remain at the preclinical stage, with limited clinical validation currently available.
In this review, we examine the major biological and pharmacological barriers that limit conventional dopaminergic therapies and discuss emerging nanomedicine strategies designed to overcome these challenges. We first summarize key aspects of dopamine biology relevant to therapeutic development and describe the limitations of existing pharmacological approaches. We then review advances in nanoparticle-based delivery systems for dopamine and dopaminergic drugs, including polymeric nanoparticles, lipid-based carriers, dendrimers, inorganic nanomaterials, and extracellular vesicles. Finally, we discuss safety considerations, translational challenges, and emerging technological directions that may enable the development of clinically viable nanomedicine platforms for the treatment of dopamine-related neurological disorders. Unlike previous reviews focused primarily on dopaminergic pharmacology or general CNS nanomedicine approaches, this review uniquely integrates dopamine stabilization, oxidative protection, blood–brain barrier transport strategies, and translational nanotherapeutic development within a unified nanomedicine framework.
Dopamine Biology, Chemistry and Therapeutic Targets
Dopamine is an essential catecholamine neurotransmitter involved in numerous physiological and behavioral functions, including movement, learning, motivation, reward perception, cognition, and hormonal regulation. Dopaminergic neurons are primarily concentrated within the midbrain and communicate with different regions of the brain through several well-defined neural circuits. Among these are the nigrostriatal pathway, which governs motor coordination and voluntary movement; the mesolimbic pathway, which is central to reward and reinforcement behaviors; the mesocortical pathway, which influences executive function and emotional processing; and the tuberoinfundibular pathway, which regulates endocrine activity through the pituitary gland. Because these pathways control diverse aspects of brain function, disturbances in dopaminergic neurotransmission have been linked to a variety of neurological and psychiatric disorders.20–25
The major biosynthetic and biodegradation pathway for dopamine is given in Figure 1. Dopamine is synthesized from the amino acid tyrosine through a tightly regulated enzymatic pathway. Tyrosine is first converted to L-3,4-dihydroxyphenylalanine (L-DOPA) by the enzyme tyrosine hydroxylase, which represents the rate-limiting step in dopamine biosynthesis.26 L-DOPA is then decarboxylated by aromatic L-amino acid decarboxylase to generate dopamine. Newly formed dopamine is packaged into synaptic vesicles through the action of vesicular monoamine transporter 2 (VMAT2), allowing it to be stored until neuronal stimulation triggers its release into the synaptic cleft. Once released, dopamine interacts with specific receptors on neighboring neurons, initiating signaling events that influence neuronal communication and network activity.27–29 To maintain proper neurotransmission, extracellular dopamine levels must be carefully regulated. One major mechanism involves reuptake through the dopamine transporter (DAT), which removes dopamine from the synaptic cleft and returns it to presynaptic neurons for reuse or degradation. Dopamine can also undergo enzymatic metabolism by monoamine oxidase (MAO) and catechol-O-methyltransferase (COMT), yielding metabolites such as 3,4-dihydroxyphenylacetic acid (DOPAC) and homovanillic acid. Together, these processes ensure tight control of dopamine concentrations within the nervous system. However, they also present obstacles for therapeutic applications because externally administered dopamine is rapidly eliminated or metabolized before reaching target tissues.30–33
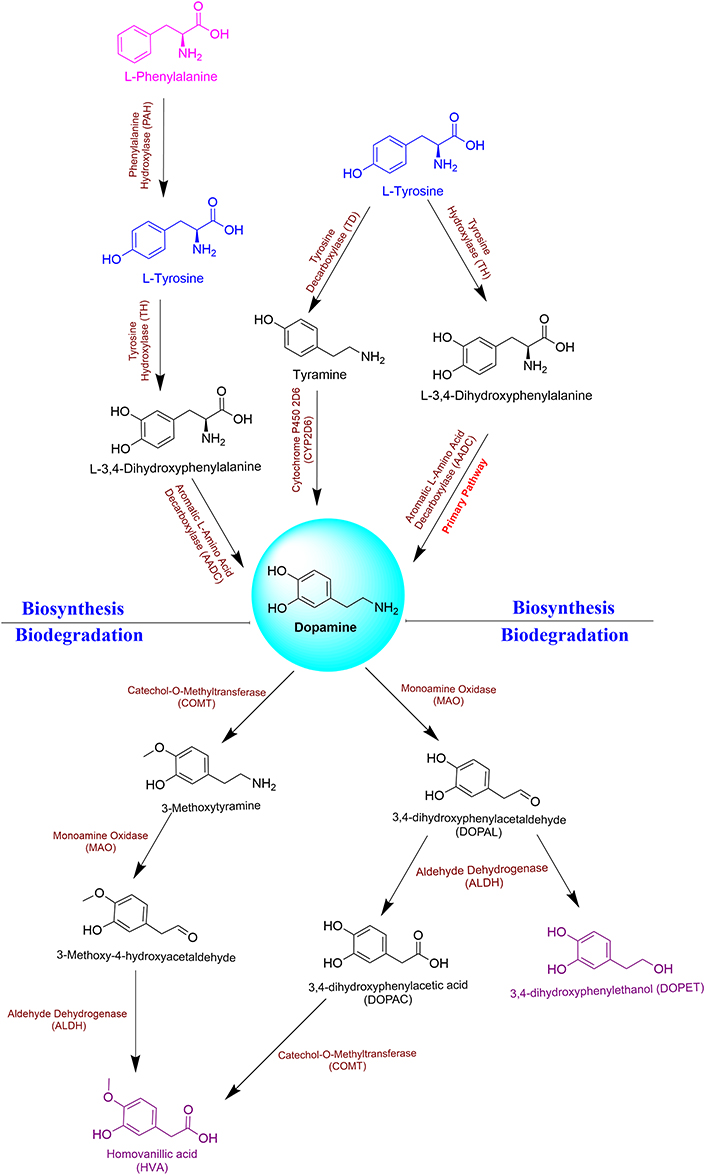 |
Figure 1 Overview of dopamine synthesis, signaling, transport, and metabolism within the central nervous system. Dopamine is synthesized from tyrosine through enzymatic conversion to L-DOPA followed by decarboxylation to dopamine. Newly synthesized dopamine is packaged into synaptic vesicles through vesicular monoamine transporter 2 (VMAT2) and released into the synaptic cleft upon neuronal stimulation. Dopamine subsequently interacts with D1-like and D2-like receptor families to regulate motor function, cognition, reward signaling, mood, and neuroendocrine activity. Following receptor activation, dopamine is cleared through dopamine transporter (DAT)-mediated reuptake and enzymatic degradation by monoamine oxidase (MAO) and catechol-O-methyltransferase (COMT). Dysregulation of dopaminergic signaling is strongly associated with neurodegenerative disorders such as Parkinson’s disease. Colors were used to facilitate visualization of the dopamine metabolic network. Brown labels indicate enzymes and catalytic reactions, blue structures represent major biosynthetic intermediates, pink structures denote precursor, purple structures indicate terminal metabolic products, and black structures represent key intermediates within dopamine synthesis and degradation pathways (Created with BioRender.com). |
The physiological effects of dopamine are mediated through five G protein-coupled receptor subtypes that are divided into two functional groups. The D1-like receptor family, consisting of D1 and D5 receptors, generally stimulates adenylate cyclase activity through Gs proteins, leading to increased intracellular cyclic AMP (cAMP) levels. In contrast, the D2-like receptor family, which includes D2, D3, and D4 receptors, is typically coupled to Gi proteins and suppresses adenylate cyclase activity, thereby reducing cAMP production.1 Through these signaling mechanisms, dopamine receptors influence neuronal firing, synaptic remodeling, and gene expression. The widespread distribution of dopamine receptor subtypes contributes to the complexity of dopaminergic signaling. D1 and D2 receptors are highly expressed within the striatum, where they play critical roles in regulating movement and basal ganglia circuitry. Abnormal signaling through these receptors is strongly associated with disorders such as Parkinson’s disease and other movement-related conditions. Receptors located within the mesolimbic and mesocortical systems contribute to motivation, emotional regulation, and cognitive performance, and dysfunction within these circuits has been implicated in schizophrenia, substance use disorders, and other psychiatric illnesses. Because dopamine receptors are found throughout both central and peripheral tissues, therapies that broadly activate dopaminergic pathways frequently produce undesirable side effects due to limited selectivity.34–37
An additional challenge in dopamine biology is its inherent chemical instability. Under physiological conditions, dopamine can undergo oxidation to generate quinones and other reactive species capable of inducing oxidative stress and cellular injury.38 These reactions are particularly relevant in neurodegenerative diseases such as Parkinson’s disease, where oxidative stress and mitochondrial dysfunction are believed to play important roles in disease progression. Consequently, strategies that protect dopamine from oxidation or regulate its controlled release may offer therapeutic advantages. The tightly regulated processes of dopamine synthesis, release, receptor signaling, reuptake, and metabolism create a complex neurochemical system that is difficult to modulate using conventional pharmacological approaches.39,40 Effective therapies must address challenges such as rapid metabolism, oxidative instability, and the difficulty of selectively targeting specific neural circuits. These limitations have motivated the development of advanced drug delivery technologies. In particular, nanomedicine-based systems have emerged as promising strategies for enhancing dopamine stability, improving transport across the blood–brain barrier, enabling controlled release, and facilitating targeted delivery to affected regions of the brain.41
Limitations of Conventional Dopaminergic Therapies
Although considerable progress has been made in understanding dopamine signaling and developing dopaminergic medications, current treatment approaches remain constrained by several biological and pharmacological challenges. Most available therapies do not deliver dopamine directly but instead utilize dopamine precursors, receptor agonists, or receptor antagonists to modulate dopaminergic activity. While these strategies can alleviate symptoms in a range of neurological and psychiatric disorders, they often lack the ability to provide sustained, localized, and physiologically regulated dopamine signaling. Key obstacles include dopamine’s inherent chemical instability, rapid metabolic breakdown, limited penetration into the brain, and the broad distribution of dopamine receptors throughout the body.
Dopamine Instability
A major hurdle in dopamine-based therapy is the molecule’s susceptibility to chemical degradation. The catechol moiety present in dopamine is readily oxidized under physiological conditions, particularly in the presence of oxygen and reactive oxygen species. This oxidation process generates dopamine quinones and other reactive byproducts that not only reduce the amount of active dopamine available but can also contribute to oxidative stress within neural tissues. The resulting reactive intermediates have been implicated in neuronal injury and may accelerate pathological processes associated with neurodegenerative diseases, including Parkinson’s disease. Consequently, dopamine instability remains one of the principal barriers to its direct therapeutic application.42 In addition to nonenzymatic oxidation, dopamine is rapidly metabolized by enzymes such as monoamine oxidase (MAO) and catechol-O-methyltransferase (COMT). These enzymes convert dopamine into inactive metabolites in both peripheral organs and the central nervous system, substantially shortening its biological half-life. As a result, systemically administered dopamine is cleared quickly and generally fails to maintain therapeutically relevant concentrations within the brain, limiting its clinical utility for neurological disorders.33
To overcome these shortcomings, treatment strategies have largely focused on the use of dopamine precursors. The most widely used example is levodopa (L-DOPA), which can cross the blood-brain barrier through amino acid transport systems and subsequently be converted into dopamine within the brain. Levodopa remains the gold-standard symptomatic treatment for Parkinson’s disease and is highly effective at improving motor symptoms, particularly during the early stages of therapy.43,44 However, prolonged administration frequently leads to complications such as motor fluctuations, dyskinesia, and reduced therapeutic responsiveness over time.45 These complications are believed to arise from pulsatile stimulation of dopamine receptors and progressive degeneration of dopaminergic neurons, which disrupt normal regulatory mechanisms within basal ganglia circuits.46 Dopamine receptor agonists represent another important therapeutic class. These compounds directly activate dopamine receptors and are often employed either as alternatives to levodopa or in combination with it. Although receptor agonists can improve symptom management and delay the need for higher levodopa doses, their use is frequently accompanied by adverse effects such as nausea, orthostatic hypotension, impulse-control disorders, hallucinations, and other neuropsychiatric complications.47,48 These adverse effects arise in part because dopamine receptors are widely distributed in both central and peripheral tissues, making it difficult to achieve selective activation of specific neural circuits using systemic pharmacological agents.
Blood-Brain Barrier Restriction
Another critical limitation of conventional dopaminergic therapies is the restricted delivery of therapeutic molecules across the blood-brain barrier.49–51 The BBB is formed by specialized endothelial cells connected through tight junctions that severely restrict the movement of molecules from the bloodstream into the brain. In addition, active transport systems and efflux pumps further limit the accumulation of many drugs within neural tissues. Consequently, numerous dopaminergic compounds exhibit poor brain uptake following systemic administration.52 Even when a drug is capable of crossing the BBB, achieving sufficient concentrations in specific brain regions can remain challenging. In many cases, therapeutics distribute broadly throughout the central nervous system, affecting multiple dopaminergic pathways rather than selectively targeting the circuit involved in disease. Such nonspecific distribution may reduce therapeutic efficiency while increasing the likelihood of adverse effects arising from unintended pathway activation.53–55
Collectively, these challenges illustrate the limitations of conventional dopaminergic pharmacotherapy. Successful therapeutic intervention requires strategies that simultaneously address several barriers, including dopamine oxidation, rapid metabolic elimination, inadequate BBB penetration, and poor spatial selectivity within the brain. These unmet needs have driven growing interest in advanced drug delivery technologies capable of overcoming the shortcomings of traditional treatments. In particular, nanomedicine-based platforms have emerged as promising tools for enhancing dopamine stability, improving transport into the brain, prolonging drug exposure, and enabling targeted delivery to specific neural regions. Such approaches may ultimately provide more precise and effective modulation of dopaminergic signaling than currently available therapies. Furthermore, despite their widespread clinical use, existing dopaminergic medications continue to suffer from issues including limited selectivity, systemic adverse effects, and long-term treatment complications. The major characteristics, clinical applications, and limitations of these therapies are summarized in Table 1.
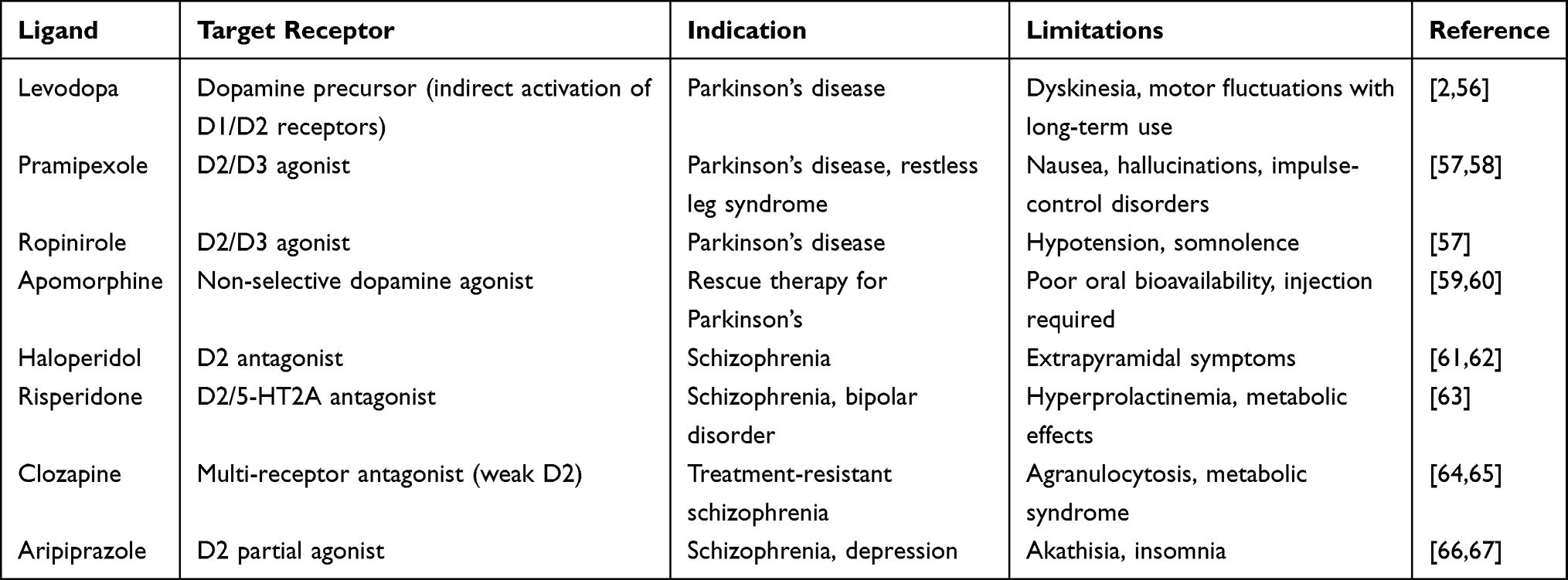 |
Table 1 Clinically Used Dopaminergic Drugs and Key Therapeutic Limitations |
Blood-Brain Barrier as the Central Delivery Challenge
The BBB is one of the most significant physiological obstacles to effective treatment of neurological disorders as shown in Figure 2. While the BBB plays a crucial protective role by maintaining the homeostasis of the central nervous system, it simultaneously restricts the delivery of many potentially beneficial therapeutic agents. This barrier prevents the entry of toxins, pathogens, and circulating molecules into the brain, but it also limits the transport of numerous drugs designed to treat neurological diseases. As a result, many pharmacological compounds that demonstrate promising activity in vitro fail to achieve adequate therapeutic concentrations within the brain.68,69
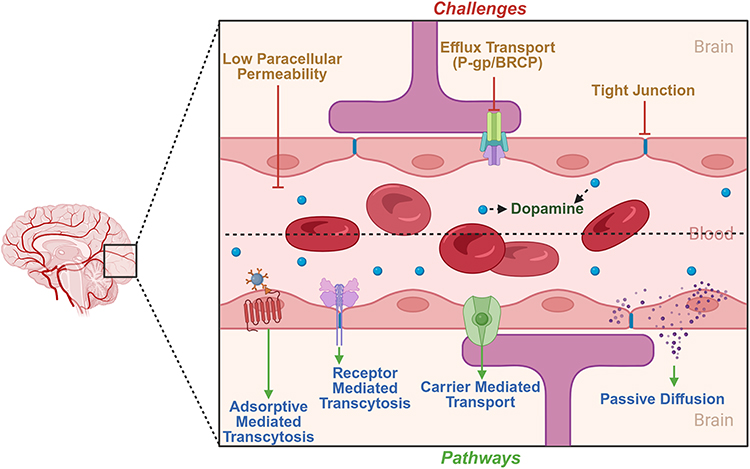 |
Figure 2 Structure of the blood–brain barrier (BBB) and major transport mechanisms involved in CNS drug delivery. The BBB is composed of tightly connected endothelial cells supported by astrocytic end-feet, pericytes, and the basement membrane, forming a highly selective physiological barrier that restricts entry of most therapeutic agents into the brain. Major transport pathways include passive diffusion, carrier-mediated transport, receptor-mediated transcytosis, and adsorptive-mediated transcytosis. Efflux transporters such as P-glycoprotein (P-gp) and breast cancer resistance protein (BCRP) further limit CNS drug accumulation by actively transporting xenobiotics out of brain endothelial cells. These physiological barriers represent a major challenge for effective dopamine delivery and motivate the development of targeted nanomedicine strategies capable of enhancing BBB penetration and brain-specific therapeutic delivery. Green arrows represent positive regulation, activation, or induction of downstream signaling events, while red lines/arrows represent negative regulation, inhibition, or suppression of molecular targets and pathways. (Created with BioRender.com). |
Structural Organization of the BBB
The BBB is primarily formed by specialized endothelial cells that line cerebral microvessels. Unlike endothelial cells in peripheral tissues, brain endothelial cells are tightly connected by complex networks of tight junction proteins, including claudins, occludins, and junctional adhesion molecules. These structures restrict paracellular diffusion and create a highly selective interface between the bloodstream and neural tissue.52 Beyond endothelial cells, the BBB is part of a larger functional unit known as the neurovascular unit, which includes pericytes, astrocytic end-feet, neurons, and extracellular matrix components. Pericytes embedded within the vascular basement membrane regulate vascular stability and permeability, while astrocytes extend specialized processes that surround the capillary walls and contribute to the maintenance of BBB integrity.70 These cellular interactions coordinate vascular signaling, nutrient transport, and immune surveillance within the brain. Together, the components of the neurovascular unit maintain a tightly regulated microenvironment that is essential for proper neuronal function. However, this sophisticated structural organization also creates a formidable barrier that restricts the entry of many therapeutic molecules.
Transport Mechanisms Across the BBB
Although the BBB restricts the passive diffusion of most molecules, several physiological transport mechanisms allow essential nutrients and signaling molecules to enter the brain. These transport processes include passive diffusion, carrier-mediated transport, receptor-mediated transcytosis, and adsorptive-mediated transcytosis. Small lipophilic molecules may cross the BBB through passive diffusion across endothelial membranes.71,72 However, many pharmacological agents, including dopamine, are hydrophilic and therefore exhibit poor passive permeability. Carrier-mediated transport systems facilitate the movement of specific molecules such as glucose, amino acids, and nucleosides through specialized membrane transporters. For example, the dopamine precursor L-DOPA can cross the BBB through amino acid transport systems, which explains its therapeutic use in Parkinson’s disease.73 Receptor-mediated transcytosis represents another important pathway for the transport of macromolecules across the BBB. In this process, circulating ligands bind to specific receptors expressed on brain endothelial cells, triggering vesicular transport across the endothelial layer.74 Examples of receptors involved in this mechanism include transferrin receptors, insulin receptors, and low-density lipoprotein receptors. Adsorptive-mediated transcytosis, in contrast, occurs through electrostatic interactions between positively charged molecules and negatively charged endothelial surfaces, leading to endocytosis and vesicular transport across the barrier. While these transport pathways allow the selective entry of certain molecules, they are often insufficient for delivering therapeutic concentrations of many drugs to the brain.75,76
Efflux Transporters and Drug Clearance
In addition to restricting molecular entry, the BBB contains active efflux transport systems that remove many xenobiotics from the brain. These transporters belong primarily to the ATP-binding cassette (ABC) transporter family and include proteins such as P-glycoprotein (P-gp), breast cancer resistance protein (BCRP), and multidrug resistance-associated proteins. These transporters actively pump numerous drugs back into the bloodstream, thereby limiting their accumulation within the brain.77 Efflux transporters represent a major barrier to CNS drug delivery because even compounds capable of crossing endothelial membranes may be rapidly expelled before reaching therapeutic concentrations within neural tissues. Consequently, many dopaminergic drugs exhibit poor central nervous system bioavailability despite favorable pharmacological properties.
Implications for Dopaminergic Therapy
The combined effects of tight junction restriction, selective transport systems, and active efflux mechanisms significantly limit the ability of dopaminergic drugs to reach target sites within the brain. Dopamine itself is particularly affected by these barriers because it is both hydrophilic and rapidly metabolized in peripheral tissues.78 Even when dopamine precursors or receptor agonists are used, achieving consistent and region-specific drug delivery remains difficult. Furthermore, systemic administration of dopaminergic drugs often results in widespread distribution throughout the body rather than selective accumulation within specific neural circuits.79 This lack of spatial targeting contributes to many of the adverse effects associated with dopaminergic therapies, including cardiovascular complications, gastrointestinal disturbances, and neuropsychiatric symptoms. Because of these challenges, improving the delivery of dopaminergic therapeutics requires strategies that can overcome the structural and functional barriers of the BBB while minimizing systemic toxicity.
Rationale for Nanomedicine-Based Delivery Strategies
Nanomedicine-based drug delivery systems offer promising opportunities to address many of the limitations imposed by the BBB. Nanocarriers can be engineered to protect therapeutic molecules from degradation, prolong systemic circulation, and enhance transport across biological barriers. Nanoparticles can be functionalized with targeting ligands that interact with receptors expressed on brain endothelial cells, thereby exploiting receptor-mediated transcytosis pathways for improved BBB penetration. In addition, nanoscale carriers can be designed to control drug release, allowing sustained therapeutic exposure within the brain while reducing systemic toxicity. Surface modification strategies such as polyethylene glycol coating can improve nanoparticle stability and reduce immune clearance, further enhancing their circulation time and delivery efficiency. These capabilities make nanomedicine an attractive strategy for improving the delivery of dopamine and dopaminergic drugs to the central nervous system. The following section discusses major nanoparticle platforms that have been developed to overcome the biological barriers associated with dopaminergic therapy.80–82
Nanomedicine Strategies for Dopamine Delivery and Oxidative Stabilization
Nanotechnology-based drug delivery systems have emerged as promising approaches to overcome the limitations associated with conventional dopamine therapies, particularly poor BBB penetration, systemic toxicity, and rapid drug metabolism.51 Nanocarriers can encapsulate dopamine or dopaminergic drugs, protect them from degradation, and facilitate controlled release within the brain. In addition, nanoscale systems can be engineered with targeting ligands and surface modifications that enhance BBB transport and neuronal uptake. Important nanocarrier systems and their benefits for dopamine delivery have been summarized in Figure 3.
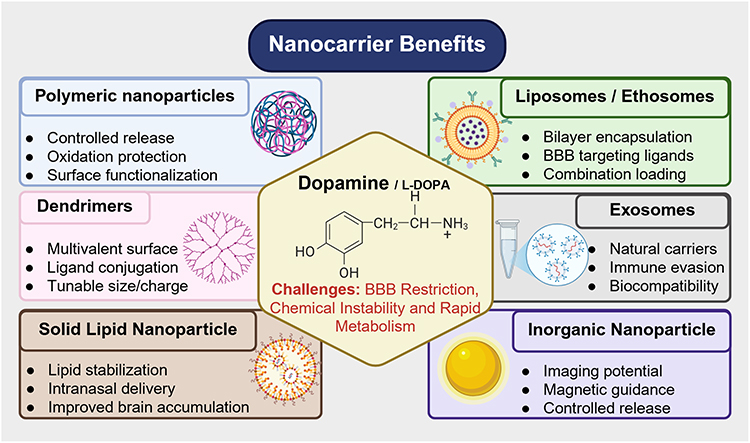 |
Figure 3 Major nanocarrier platforms investigated for dopamine delivery and stabilization in neurological disorders. Polymeric nanoparticles, liposomes, solid lipid nanoparticles (SLNs), nanostructured lipid carriers (NLCs), dendrimers, inorganic nanoparticles, and exosome-inspired vesicles are illustrated as representative nanosystems developed to overcome the limitations of conventional dopaminergic therapies. These nanocarriers improve dopamine stability, reduce peripheral degradation, enhance blood–brain barrier penetration, facilitate controlled drug release, and improve targeting to dopaminergic brain regions. Each platform possesses distinct advantages and limitations with respect to biocompatibility, scalability, targeting efficiency, oxidative protection, and translational feasibility. Emerging multifunctional and biomimetic nanosystems are increasingly being explored to integrate delivery enhancement with antioxidant and neuroprotective properties. (Created with BioRender.com). |
Polymeric Nanoparticles
Polymeric nanoparticles, particularly those based on poly (lactic-co-glycolic acid) (PLGA) and PEG-modified PLGA, represent one of the most extensively investigated nanocarrier systems for central nervous system drug delivery. PLGA is biodegradable, biocompatible, and approved for clinical use, making it highly suitable for controlled drug delivery applications. Its polymer matrix can encapsulate both hydrophilic and lipophilic drugs, allowing protection of sensitive molecules and prolonged release profiles.
Controlled Release
Experimental work demonstrated that PLGA nanoparticles can deliver dopamine across the blood-brain barrier and restore dopaminergic signaling in animal models of Parkinson’s disease.83 A key advantage of PLGA systems is their ability to provide controlled and sustained drug release. Encapsulation of dopamine or L-DOPA within PLGA nanoparticles slows drug diffusion and reduces rapid degradation in physiological environments, thereby maintaining therapeutic concentrations over extended periods. Studies have shown that dopamine entrapped in PLGA nanoparticles is released gradually while maintaining elevated dopamine levels in the brain compared with free drug administration.83
Oxidation Protection
Polymeric nanoparticles also offer protection against oxidative degradation of dopamine, which is a major limitation in conventional therapy. Research has demonstrated that encapsulation within PLGA nanoparticles decreases dopamine autoxidation and reduces formation of reactive quinone intermediates, ultimately lowering cellular toxicity.83,84 In this study, the nanoparticle formulation improved neurobehavioral outcomes and reduced dopamine oxidation compared with free dopamine administration.83 More recently, in vitro BBB models have confirmed that dopamine-loaded PLGA nanoparticles exhibit efficient transport across endothelial barriers and show strong binding to neuronal tissues, supporting their therapeutic potential.85
Surface Engineering
Surface modification strategies have further enhanced the performance of polymeric nanoparticles. For example, albumin-functionalized PLGA nanosystems have demonstrated improved receptor-mediated transport across the BBB and enhanced accumulation in dopaminergic brain regions.86 Polymeric nanoparticles can also be PEGylated, a modification that increases circulation time, reduces immune recognition, and improves systemic stability, thereby increasing the probability of brain delivery.87 Particle size is a critical parameter influencing BBB penetration and biodistribution. Nanoparticles in the 50–200 nm range have been shown to exhibit optimal circulation behavior and efficient cellular uptake, whereas larger particles are more rapidly cleared by the reticuloendothelial system.
Liposomes
Liposomes are spherical vesicles composed of one or more phospholipid bilayers that can encapsulate therapeutic molecules within both an aqueous core and a lipid membrane. This dual-compartment structure allows hydrophilic drugs to be contained within the internal aqueous space while lipophilic compounds are incorporated within the phospholipid bilayer, providing a versatile platform for drug delivery. Experimental studies of lipid self-assembly demonstrate that phospholipid molecules spontaneously organize into bilayer vesicles in aqueous environments, with hydrophilic head groups oriented outward and hydrophobic tails forming the membrane interior, creating a stable compartment capable of drug encapsulation.88,89
Bilayer Encapsulation
This bilayer architecture offers important advantages for dopamine delivery because it can protect unstable molecules from enzymatic degradation and oxidative reactions while allowing controlled release. Liposomes can simultaneously load hydrophilic and lipophilic agents, enabling combination therapies and improving pharmacokinetics.90,91 Recent studies have demonstrated that liposomal encapsulation can significantly improve brain delivery of dopaminergic drugs. For example, dopamine-loaded liposomes functionalized with targeting ligands have shown improved uptake in brain endothelial cells and enhanced penetration across the blood-brain barrier.92,93
RVG29/Transferrin Targeting
More advanced studies have demonstrated that dopamine-loaded liposomes can significantly improve drug delivery to the brain. In a 2024 study, receptor-targeted liposomes modified with the RVG29 peptide enhanced BBB penetration and increased dopamine accumulation in the striatum and substantia nigra in animal models of Parkinson’s disease.94 These liposomal formulations also prolonged systemic circulation and improved neuroprotective effects compared with free dopamine. Liposomes can also be engineered with targeting ligands such as transferrin, lactoferrin, or peptides derived from viral glycoproteins, which facilitate receptor-mediated transport across the BBB.
Solid Lipid Nanoparticles
Lipid-based nanocarriers such as solid lipid nanoparticles (SLNs) and nanostructured lipid carriers (NLCs) have attracted considerable attention for central nervous system drug delivery because of their biocompatibility, ability to protect labile molecules, and potential to improve brain targeting. These systems consist of physiological lipids that remain solid at body temperature, forming a matrix capable of encapsulating drugs and controlling their release. Compared with conventional nanoparticles, SLNs and NLCs offer improved drug stability and reduced toxicity due to the use of biodegradable lipids. Additionally, the lipid matrix can enhance drug permeability across biological membranes and improve pharmacokinetic profiles.
Intranasal Delivery
The intranasal route has emerged as a promising strategy for delivering dopaminergic therapeutics directly to the brain while bypassing the blood–brain barrier. Lipid-based nanoparticles can exploit olfactory and trigeminal nerve pathways to transport drugs from the nasal cavity to the central nervous system. Experimental studies evaluating dopamine-loaded SLNs demonstrated successful nose-to-brain delivery, resulting in increased dopamine levels in the striatum of animal models and improved neurological outcomes.95,96
Recent investigations have also shown that lipid nanocarriers administered intranasally significantly enhance brain accumulation compared with conventional drug formulations. Encapsulation within SLNs or NLCs improves drug residence time in the nasal cavity, promotes uptake by olfactory neurons, and facilitates transport to brain tissues.97,98 For example, a recent study demonstrated that intranasal nanostructured lipid carriers increased drug concentration in the brain and improved therapeutic efficacy compared with systemic administration, highlighting their potential for treating neurodegenerative diseases.99
Lipid Stabilization
Another major advantage of SLNs and NLCs is their ability to stabilize therapeutic molecules within a lipid matrix. The solid lipid core protects drugs from enzymatic degradation, chemical instability, and premature metabolism during circulation. This feature is particularly important for dopamine and other neurotransmitters that are highly susceptible to oxidation and degradation.
Nanostructured lipid carriers were developed as a second-generation system to overcome limitations associated with SLNs. By incorporating both solid and liquid lipids, NLCs create imperfections in the lipid matrix that improve drug loading capacity and reduce drug leakage during storage.97 Recent experimental work has demonstrated that dopamine co-loaded lipid nanoparticles can improve drug stability and therapeutic outcomes in models of Parkinson’s disease. Encapsulation within SLNs protects dopamine from degradation while enabling sustained drug release and improved brain targeting.100 These findings suggest that lipid-based nanocarriers provide an effective platform for stabilizing dopaminergic drugs and enhancing their delivery to the brain.
Dendrimers
Dendrimers are highly branched nanoscale polymers with a well-defined architecture consisting of a central core, repetitive branching units, and numerous surface functional groups. Their unique structure provides a high degree of control over particle size, surface chemistry, and drug loading capacity, making them attractive candidates for drug delivery applications. Early investigations demonstrated that poly(amidoamine) (PAMAM) dendrimers can effectively transport therapeutic molecules and interact with biological membranes because of their multivalent surface functionality.101
Surface Functionalization and Targeted Delivery
One of the most important advantages of dendrimers is the ability to modify their surface with targeting ligands, polymers, or therapeutic molecules. This surface engineering enables improved stability, selective targeting, and enhanced delivery across biological barriers. Studies investigating peptide-modified PAMAM dendrimers demonstrated that conjugation of targeting ligands significantly improves drug delivery efficiency and facilitates transport across the blood-brain barrier.102 Recent experimental work has also shown that modification of dendrimer surfaces can improve brain targeting and reduce systemic toxicity. For example, functionalized dendrimers engineered for central nervous system delivery demonstrated improved accumulation within brain tissue compared with unmodified nanoparticles.103 In addition, modern engineering strategies now incorporate polymers, peptides, or biomolecules onto dendrimer surfaces to enhance cellular uptake and drug loading efficiency. These approaches take advantage of the multivalent surface of dendrimers, which allows simultaneous attachment of targeting ligands and therapeutic cargo.104
Charge-Dependent Toxicity
Despite their advantages, dendrimers can exhibit cytotoxicity that depends strongly on surface charge and molecular generation. Cationic dendrimers interact electrostatically with negatively charged cellular membranes, which can disrupt membrane integrity and induce cell damage. Experimental studies have shown that increasing dendrimer generation and surface charge enhances cellular uptake but may also increase cytotoxicity. More recent research confirms that reducing positive surface charge through chemical modification can significantly decrease dendrimer toxicity. For instance, studies of PAMAM-based nanostructures reported that lowering zeta potential through surface modification resulted in reduced cellular toxicity while maintaining delivery efficiency.105 Additionally, recent investigations into dendrimer-based drug delivery systems emphasize the importance of balancing particle size and surface charge to achieve effective cellular targeting while minimizing adverse biological effects.106
Inorganic Nanoparticles
Inorganic nanoparticles have emerged as promising platforms for neurological drug delivery due to their structural stability, tunable physicochemical properties, and multifunctional capabilities. Unlike polymeric systems, inorganic nanomaterials can provide additional imaging, magnetic guidance, or controlled drug release functions, enabling theranostic applications in neurological disorders. Recent studies demonstrate that inorganic nanoparticles can enhance drug transport across the blood-brain barrier (BBB) and improve therapeutic targeting in brain diseases.107
Gold Nanoparticles
Gold nanoparticles (AuNPs) are among the most extensively studied inorganic nanomaterials for brain delivery because of their high biocompatibility, chemical stability, and ease of surface functionalization. Their large surface area enables conjugation of drugs, peptides, and antibodies that facilitate transport across the BBB and targeting of diseased brain regions.108 Experimental studies have demonstrated that functionalized gold nanoparticles can cross the BBB and deliver therapeutic cargo in intracranial tumor models, highlighting their potential for brain-targeted drug delivery.109 More recent investigations also indicate that ultrasmall gold nanoparticles can penetrate the BBB and enhance transport of biomolecules to neural tissue, supporting their use in treating neurodegenerative diseases.107 In addition, alternative delivery routes such as intranasal administration have shown improved targeting efficiency, where gold nanoparticles delivered through the nasal cavity accumulated more effectively in brain tissues compared with intravenous administration.110 These findings demonstrate that gold nanoparticles offer a versatile platform capable of combining drug delivery, imaging, and therapeutic applications.
Magnetic Nanoparticles
Magnetic nanoparticles, particularly iron oxide nanoparticles, have attracted significant attention for brain delivery due to their ability to be guided using external magnetic fields. This feature enables spatial control of drug delivery and potentially improves targeting efficiency within the central nervous system. Experimental studies demonstrated that magnetic nanoparticles could cross the BBB and accumulate in brain tissue when guided by an external magnetic field, illustrating their potential for targeted neurological therapy. Further investigations confirmed that magnetically guided nanocarriers can deliver therapeutic agents to brain regions with minimal neurotoxicity, making them promising candidates for both treatment and imaging applications.111 Recent developments in magnetic nanoparticle engineering have also enabled multifunctional platforms capable of drug delivery, imaging, and hyperthermia therapy, highlighting their potential as theranostic systems for neurological diseases.112
Silica Nanoreservoirs
Mesoporous silica nanoparticles (MSNs) represent another important class of inorganic nanocarriers due to their highly ordered pore structure, large surface area, and tunable particle size. These properties allow efficient drug loading and controlled release, making them suitable nanoreservoirs for neurological therapeutics. Experimental studies evaluating mesoporous silica nanoparticles demonstrated their ability to cross in vitro BBB models and deliver therapeutic agents to brain cells.113 Further work has shown that silica nanoparticles can permeate the BBB and transport drugs into brain tissue, suggesting potential applications for treating neurological disorders.114 More recent research highlights that engineered silica nanoparticles with tunable size and surface chemistry can improve BBB transport and enhance targeted drug delivery.115 However, studies also indicate that silica nanoparticles may influence neuronal signaling and neurotransmitter levels, emphasizing the need for careful evaluation of their neurotoxicity and long-term safety.116
Exosomes and Biomimetic Vesicles
Extracellular vesicles such as exosomes have emerged as a promising class of natural nanocarriers for drug delivery to the central nervous system. Exosomes are nanosized membrane vesicles secreted by many cell types that mediate intercellular communication by transporting proteins, lipids, and nucleic acids. Because their lipid bilayer structure originates from biological membranes, exosomes exhibit high biocompatibility and improved interactions with biological barriers compared with many synthetic nanomaterials. These properties have stimulated intense research into their use for neurological drug delivery.
Natural Blood-Brain Barrier Crossing
One of the most important advantages of exosomes is their inherent ability to cross the BBB. A landmark experimental study demonstrated that engineered exosomes could deliver small interfering RNA to the mouse brain following systemic administration, providing direct evidence that these vesicles can transport therapeutic cargo across the BBB.117 Subsequent studies confirmed that extracellular vesicles can traverse BBB models through transcellular transport mechanisms and deliver functional cargo to neuronal cells.118 More recent investigations have further highlighted the potential of exosome-based systems for brain drug delivery, showing that these vesicles can be engineered with targeting ligands to enhance selective uptake by neural tissues and improve therapeutic efficacy in neurological disease models.119,120 These findings suggest that exosomes represent a promising natural platform for transporting drugs and genetic therapeutics into the brain.
Immune Evasion and Biocompatibility
Another key advantage of exosomes is their ability to evade immune recognition. Because they originate from endogenous cellular membranes, exosomes generally exhibit lower immunogenicity than synthetic nanoparticles and are less likely to trigger rapid clearance by the immune system. Experimental studies have shown that exosome-based carriers can deliver RNA molecules to brain tissue without inducing significant immune responses, highlighting their suitability for therapeutic applications.117 In addition, the lipid composition and surface proteins of exosomes contribute to improved cellular uptake and enhanced biological stability, enabling efficient delivery of therapeutic molecules across physiological barriers.121,122 Because of these properties, exosomes are increasingly being investigated as natural delivery vehicles for neurodegenerative diseases and other central nervous system disorders.
Scalability and Manufacturing Challenges
Despite their promising biological properties, the large-scale clinical application of exosome-based drug delivery systems remains challenging. Production of exosomes typically requires cell culture systems, and isolation procedures such as ultracentrifugation or chromatography can be labor-intensive and difficult to standardize. These limitations can affect reproducibility and scalability during therapeutic development. Recent research has therefore explored engineered or biomimetic vesicles that mimic natural exosomes but can be produced more efficiently. For example, exosome-mimetic nanovesicles generated from cell membranes have been developed to improve large-scale manufacturing while maintaining efficient brain targeting capabilities.123 These biomimetic approaches aim to combine the biological advantages of natural exosomes with the scalability required for clinical translation.
Dopamine Oxidation Shielding by Nanocarriers
A major limitation of dopamine-based therapy is the rapid oxidation of dopamine into quinone intermediates, which leads to the generation of reactive oxygen species (ROS) and loss of therapeutic activity. Nanocarrier systems have therefore been investigated not only as delivery vehicles but also as protective platforms that can stabilize dopamine and reduce oxidative degradation. Recent experimental work demonstrates that nanoparticle-based systems can preserve dopamine activity, reduce oxidative stress, and enhance therapeutic outcomes in neurological disease models.84 Dopamine stabilization benefits have been summarized in the Figure 4.
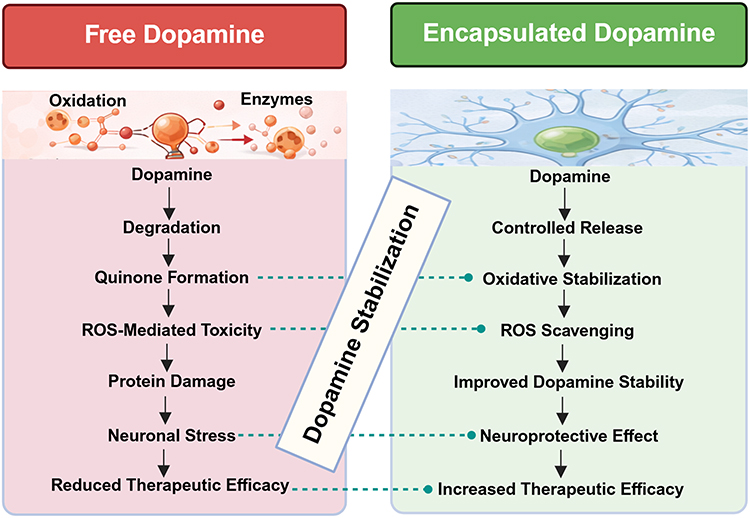 |
Figure 4 Nanocarrier-mediated protection against dopamine oxidation and reactive oxygen species (ROS)-associated neurotoxicity. Free dopamine is highly susceptible to autoxidation under physiological conditions, resulting in the formation of dopamine quinones, reactive oxygen species, and oxidative stress-associated neuronal injury. Encapsulation of dopamine within nanocarrier systems provides a protective microenvironment that reduces direct exposure to oxidative conditions, thereby limiting quinone formation and improving dopamine stability. Controlled release properties further minimize rapid extracellular dopamine accumulation and prolong therapeutic activity within the brain. Certain nanomaterials additionally exhibit intrinsic antioxidant and ROS-scavenging properties that may further reduce oxidative stress and neuroinflammation. These combined effects improve dopamine bioavailability, reduce neurotoxicity, and enhance the overall therapeutic potential of dopamine-targeted nanomedicine approaches. (Created with BioRender.com). |
Protection From Dopamine Quinone Formation
Dopamine is highly susceptible to autoxidation in physiological environments, producing dopamine-quinones that can damage cellular proteins and contribute to neurotoxicity. Encapsulation of dopamine within nanocarriers limits exposure to oxygen and enzymatic degradation, thereby reducing quinone formation and improving molecular stability. For example, dopamine-loaded nanoparticle systems have been shown to deliver dopamine across the blood–brain barrier and restore dopaminergic signaling while protecting the molecule from rapid degradation in Parkinson’s disease models.84 Nanostructured delivery systems also provide a physical barrier between dopamine and the extracellular environment, allowing gradual release of the drug and preventing immediate oxidation. This controlled release helps maintain therapeutic dopamine concentrations in the brain and reduces the formation of reactive quinone intermediates that are associated with neuronal damage.
Reduction of Reactive Oxygen Species (ROS)
Beyond protecting dopamine, certain nanomaterials actively reduce oxidative stress through intrinsic antioxidant properties. Polydopamine-based nanoparticles, for instance, have demonstrated strong ROS-scavenging activity and can protect cells from oxidative damage. Experimental studies showed that dopamine-derived nanoparticles significantly reduce intracellular oxidative stress and restore antioxidant enzyme activity in treated cells.124 Additional work has demonstrated that polydopamine nanoparticles eliminate multiple reactive species and protect neuronal cells from oxidative injury by lowering cellular ROS levels.125 More recent studies continue to confirm these antioxidant capabilities, showing that polydopamine nanomaterials can neutralize ROS and modulate inflammatory responses in disease models.126 Because oxidative stress plays a central role in neurodegenerative diseases, these ROS-scavenging properties represent an important therapeutic advantage of nanocarrier systems.
Stability Improvement and Neuroprotective Effects
Nanocarriers not only protect dopamine from chemical degradation but also enhance its pharmacological stability and therapeutic efficacy. In vivo experiments using dopamine-loaded nanoparticles demonstrated restoration of monoamine levels and improved neurological outcomes in experimental models of Parkinson’s disease.127 Furthermore, advances in nanoparticle engineering have produced multifunctional systems capable of combining dopamine delivery with antioxidant and anti-inflammatory activity, thereby addressing multiple pathological mechanisms simultaneously. Recent research highlights that such nanosystems can improve drug stability, prolong circulation time, and enhance accumulation within dopaminergic brain regions.
To summarize representative nanotechnology approaches developed for dopaminergic therapy, key experimental studies are compiled in Table 2. These studies illustrate how diverse nanocarrier platforms, including polymeric nanoparticles, liposomes, lipid nanoparticles, dendrimers, inorganic nanomaterials, and extracellular vesicles, have been engineered to improve dopamine stability, enhance blood–brain barrier transport, and increase therapeutic efficacy in neurological disease models. These studies collectively highlight the versatility of nanocarrier platforms in addressing the challenges associated with dopamine delivery. Continued advances in nanoparticle design, targeting strategies, and translational development may enable more effective therapies for dopamine-related neurological disorders.
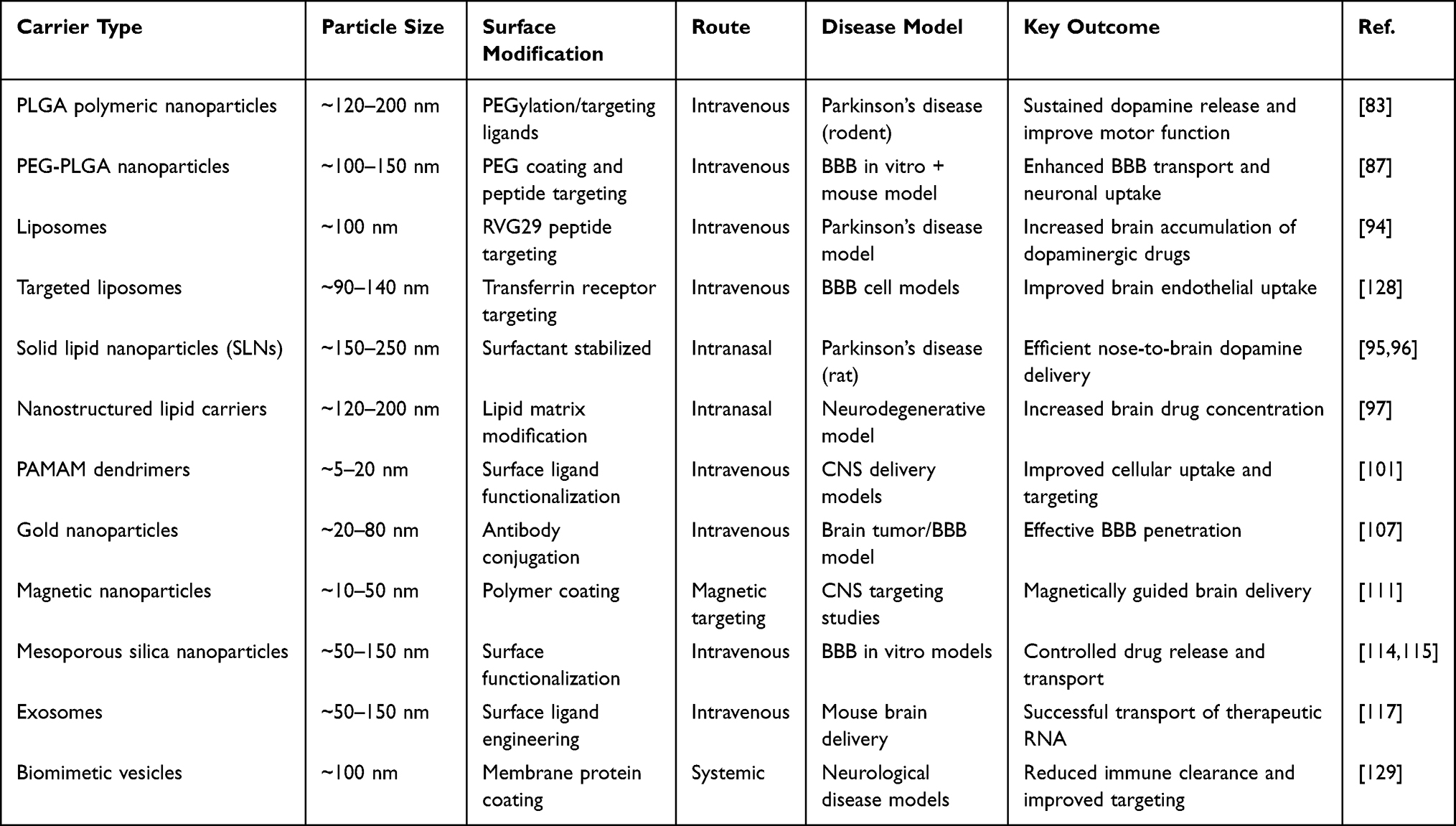 |
Table 2 Nanocarriers for Dopamine Delivery |
Although multiple nanocarrier platforms have demonstrated considerable potential for dopamine delivery to the brain, each system possesses distinct advantages and limitations that influence its translational applicability. Polymeric nanoparticles, particularly PLGA-based systems, offer excellent structural stability, controlled drug release, and protection against dopamine oxidation, making them among the most extensively investigated platforms for CNS delivery.130 Their biodegradability and FDA-approved polymer composition further support their translational potential.131 However, polymeric systems may exhibit relatively complex manufacturing processes and batch-to-batch variability that can affect reproducibility and scalability during large-scale production.132 Liposomes and lipid-based nanocarriers, including solid lipid nanoparticles (SLNs) and nanostructured lipid carriers (NLCs), provide superior biocompatibility, efficient encapsulation of both hydrophilic and lipophilic therapeutics, and enhanced BBB penetration, particularly through intranasal administration routes.133 Nevertheless, these systems may suffer from limited long-term stability, drug leakage during storage, and comparatively lower structural rigidity than polymeric formulations.134 Current evidence suggests that polymeric nanoparticles provide strong dopamine stabilization and controlled release properties, whereas lipid-based nanocarriers demonstrate superior biocompatibility and efficient BBB penetration, particularly through intranasal delivery strategies.135 Exosome-inspired vesicles exhibit exceptional biological compatibility and inherent BBB-crossing capability, making them highly promising for future translational CNS applications.136,137
Dendrimers provide unique advantages due to their highly tunable architecture, multivalent surface functionality, and ability to incorporate targeting ligands, imaging agents, and therapeutic molecules simultaneously. These features enable highly efficient receptor-mediated targeting and improved cellular uptake.138 However, dendrimer-associated cytotoxicity, particularly in highly cationic systems, remains a major limitation requiring careful surface engineering and charge optimization.139 Inorganic nanoparticles such as gold nanoparticles, magnetic nanoparticles, and mesoporous silica nanoparticles offer additional theranostic capabilities including imaging, magnetic guidance, and stimulus-responsive drug release. Despite these multifunctional properties, concerns regarding long-term accumulation, biodegradability, and neurotoxicity continue to limit their clinical translation.140 Exosomes and biomimetic vesicles represent one of the most biologically compatible nanocarrier systems due to their endogenous membrane composition, intrinsic BBB-crossing ability, and reduced immunogenicity. However, large-scale production, isolation standardization, cargo loading efficiency, and manufacturing reproducibility remain significant challenges for clinical application.141
Collectively, these findings suggest that no single nanocarrier system is universally optimal for dopamine delivery. Instead, the selection of an appropriate nanoplatform must be tailored to the intended therapeutic objective, whether prioritizing oxidative stabilization, controlled release, targeting specificity, biocompatibility, or translational scalability. Future advances will likely involve hybrid and multifunctional nanosystems that integrate the strengths of multiple carrier platforms while minimizing their individual limitations. Emerging approaches involving AI-assisted nanocarrier engineering, precision-targeted ligand design, and stimuli-responsive delivery systems may further enhance the clinical feasibility and therapeutic efficacy of dopamine-targeted nanomedicine. Despite encouraging preclinical outcomes, major translational challenges remain, including manufacturing scalability, reproducibility, long-term safety evaluation, regulatory standardization, and limited clinical validation of dopamine-targeted nanotherapeutics.
Dopamine Targeted Nanotherapies
Recent advances in nanotechnology have enabled the development of targeted nanotherapeutic systems designed to deliver dopamine or dopaminergic drugs directly to the brain. These strategies aim to improve drug stability, enhance blood-brain barrier (BBB) penetration, enable sustained drug release, and reduce systemic toxicity. Several nanoparticle-based approaches have been explored, including levodopa nanocarriers and ligand-decorated nanoparticles capable of targeting specific receptors expressed on brain endothelial cells.
Levodopa Nanoparticles
Levodopa (L-DOPA), the metabolic precursor of dopamine, remains the most widely used treatment for Parkinson’s disease, but its therapeutic efficacy is limited by peripheral metabolism and fluctuating brain concentrations. Encapsulation of levodopa within nanoparticles has been investigated as a strategy to improve pharmacokinetics and CNS delivery. For example, tannic-acid/polyvinyl-alcohol nanoparticles successfully encapsulated L-DOPA and enabled non-invasive delivery to the brain, leading to increased dopamine and tyrosine hydroxylase levels in Parkinsonian animal models.142 Similarly, self-assembled polymeric nanodrugs containing L-DOPA demonstrated gradual enzymatic release of the drug and significantly improved symptoms in MPTP-induced Parkinson’s disease mice compared with conventional L-DOPA therapy.143
More recent work has continued to improve levodopa delivery systems. Nanoparticle-based carriers have been shown to enhance brain delivery of levodopa while simultaneously reducing oxidative stress and neuronal damage in experimental models of Parkinson’s disease.144 These studies demonstrate that nanoparticle encapsulation can increase drug stability, prolong circulation time, and provide sustained release, thereby improving the therapeutic potential of levodopa.
Dopamine Nanoparticles
Direct delivery of dopamine using nanoparticles has also been explored to bypass limitations associated with dopamine instability and rapid metabolism. A landmark study developed dopamine-loaded PLGA nanoparticles capable of crossing the BBB and restoring dopaminergic function in Parkinsonian rats.83 These nanoparticles released dopamine in a controlled manner and reduced dopamine oxidation and plasma clearance, highlighting the potential of polymeric nanocarriers for neurotransmitter delivery. More recently, engineered nanocarriers and biomimetic vesicles have been investigated to enhance targeted dopamine delivery and improve therapeutic outcomes in neurodegenerative disease models.145
Receptor-Targeted Nanoparticles
One of the most promising strategies in dopamine nanomedicine involves decorating nanoparticles with ligands that interact with receptors expressed on the BBB. This approach promotes receptor-mediated transcytosis and improves delivery efficiency as shown in Figure 5.
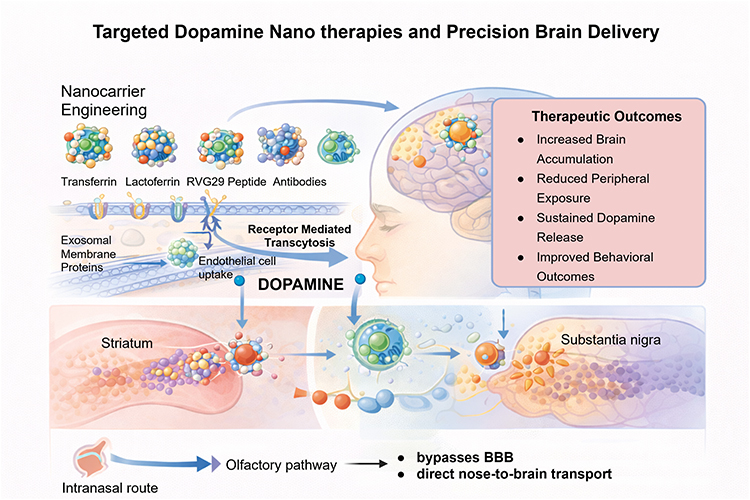 |
Figure 5 Targeted nanotherapeutic strategies for precision dopamine delivery across the blood–brain barrier. Surface-engineered nanocarriers functionalized with targeting ligands such as transferrin, lactoferrin, peptides, antibodies, and receptor-specific molecules facilitate receptor-mediated transcytosis across brain endothelial cells and improve selective accumulation within dopaminergic brain regions including the striatum and substantia nigra. Various delivery approaches including intravenous administration, intranasal transport, and biomimetic vesicle-mediated delivery are illustrated. These targeted nanosystems enhance BBB penetration, improve dopamine stability, enable controlled release, and reduce peripheral toxicity. Emerging strategies involving AI-assisted ligand optimization, stimuli-responsive nanocarriers, and biomimetic exosome-inspired vesicles may further improve precision targeting and translational potential for future neurodegenerative disease therapies. (Created with BioRender.com). |
Transferrin-Targeted Nanoparticles
Transferrin receptors are highly expressed on brain endothelial cells and have therefore been widely exploited for targeted drug delivery. Transferrin-functionalized liposomes carrying dopamine have been shown to cross the BBB and improve brain drug accumulation, demonstrating enhanced therapeutic potential for Parkinson’s disease treatment.92 Other experimental studies have shown that nanoparticles conjugated with transferrin receptor antibodies exhibit increased uptake by brain endothelial cells and improved transport across the BBB.146
Lactoferrin-Modified Nanoparticles
Lactoferrin is another targeting ligand capable of facilitating nanoparticle transport across the BBB through receptor-mediated endocytosis. Lactoferrin-decorated nanoparticles have demonstrated improved brain accumulation and enhanced neuroprotective effects in preclinical models of neurodegenerative diseases.147
Antibody-Functionalized Nanoparticles
Antibody-based targeting strategies have also gained attention for delivering nanotherapeutics to specific brain regions. Nanoparticles functionalized with antibodies directed against BBB transport receptors have demonstrated efficient uptake by endothelial cells and improved transcytosis across the BBB.146
Ligand-Decorated Nanoparticles for Targeted Delivery
Ligand-decorated nanoparticles provide several advantages compared with conventional drug formulations. By attaching targeting molecules such as peptides, proteins, or antibodies to nanoparticle surfaces, researchers can improve drug accumulation in specific brain regions while reducing systemic exposure. These functionalized nanoparticles can interact with endothelial receptors and exploit endogenous transport mechanisms to enter the brain.146 Additionally, biomimetic carriers such as exosomes have been shown to utilize transferrin-mediated pathways to reach the brain and deliver dopamine effectively in Parkinson’s disease models.145
Preclinical investigations of dopamine- and levodopa-loaded nanocarriers demonstrate improved BBB penetration, enhanced stability, and superior therapeutic outcomes compared with conventional formulations, as summarized in Table 3. Despite promising preclinical outcomes, no dopamine-loaded nanoparticle system has yet reached advanced clinical trials, highlighting the translational challenges associated with CNS nanomedicine.
 |
Table 3 Dopamine and Levodopa Nanomedicine Studies (Preclinical) |
Nanotheranostics in Dopamine Disorders
Nanotheranostics combines diagnostic imaging and therapeutic intervention within a unified nanoscale platform, offering a promising strategy for managing dopamine-related neurological disorders. By integrating imaging agents with targeted nanocarriers, these systems enable simultaneous drug delivery and disease monitoring. This approach allows researchers and clinicians to visualize dopaminergic pathways, track disease progression, and assess treatment efficacy in real time. Advanced imaging modalities, including positron emission tomography (PET), magnetic resonance imaging (MRI), and fluorescence-based techniques, have significantly enhanced our understanding of dopamine signaling and its role in neurological function in vivo.150
Imaging of Dopaminergic Systems
Visualization of the dopaminergic system has played a critical role in advancing our understanding of neurological and psychiatric disorders, including Parkinson’s disease, schizophrenia, and substance use disorders (Table 4). Early positron emission tomography (PET) investigations utilized radiolabeled ligands such as 11C-raclopride and 11C-SCH23390 to map dopamine receptor distribution in the human brain, enabling in vivo quantification of D2 and D1 receptor binding.151 As imaging technologies progressed, additional radiotracers were developed to assess other aspects of dopaminergic function, including neurotransmitter synthesis and transporter activity. For example, 18F-FDOPA and 11C-raclopride have been extensively employed in both clinical and preclinical studies to measure dopamine production, release, and receptor occupancy.152
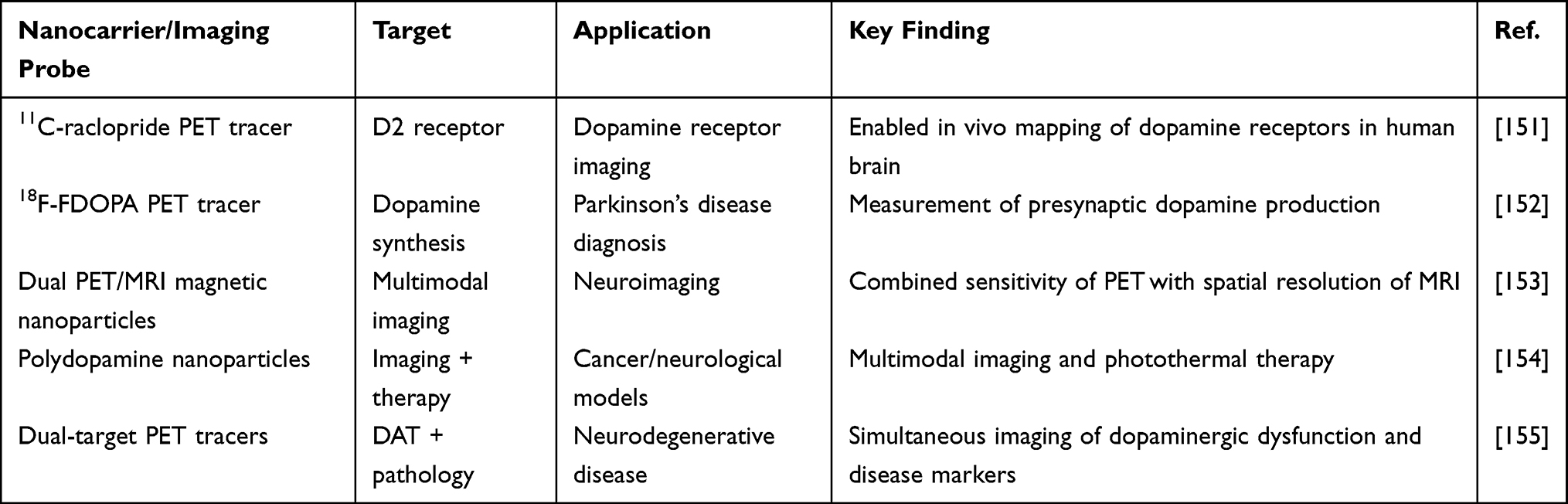 |
Table 4 Summary of Dopamine Imaging Pathways |
More recent PET imaging studies have combined multiple tracers to simultaneously assess dopamine synthesis capacity and receptor availability across brain regions, revealing correlations between dopaminergic activity and behavioral processes.156 Beyond conventional PET imaging, emerging nanotechnology-driven imaging tools are expanding the ability to monitor neurotransmitter activity with greater sensitivity and spatial precision. Examples include fluorescence-based dopamine sensors, magnetic nanoparticle platforms, and multifunctional imaging probes capable of tracking dopamine dynamics in living biological systems.150
Diagnostic Nanoparticles
Nanoparticle-based imaging agents have emerged as valuable tools for the diagnosis and monitoring of neurological diseases. Among these, magnetic nanoparticles and multifunctional nanoprobes have gained particular attention because they can integrate multiple imaging modalities, such as positron emission tomography (PET) and magnetic resonance imaging (MRI), into a single platform. This combination offers the high sensitivity of PET together with the superior anatomical resolution of MRI. In one preclinical investigation, a dual-imaging system was developed by incorporating PET radioisotopes onto superparamagnetic iron oxide nanoparticles, resulting in effective in vivo imaging performance.153 Recent advances have further improved these technologies through the development of surface-engineered magnetic nanoparticles that selectively recognize disease-related biomarkers associated with neurodegenerative disorders. By targeting pathological proteins, these nanoplatforms enable visualization of disease progression at the molecular level and may contribute to the earlier detection of Parkinson’s disease and other neurodegenerative conditions.157
In addition to magnetic nanomaterials, polydopamine-based nanoparticles have attracted considerable interest as theranostic platforms because of their excellent biocompatibility, strong photothermal activity, and versatile surface chemistry. Their structure allows the incorporation of imaging agents, therapeutic cargos, and targeting molecules, creating multifunctional systems capable of both disease diagnosis and treatment. Experimental studies have demonstrated the potential of these nanoparticles to serve as integrated imaging and therapeutic tools in a variety of disease models.154
PET Tracers Targeting Dopaminergic Systems
Positron emission tomography (PET) continues to be one of the most valuable imaging techniques for investigating dopaminergic function in the living brain. By utilizing radiolabeled compounds that bind to dopamine receptors or transporters, PET enables the assessment of receptor expression, neurotransmitter dynamics, and disease-related changes in dopaminergic pathways. Early tracer development focused on cocaine-derived molecules that selectively bind to the dopamine transporter (DAT), a critical regulator of dopamine reuptake and synaptic signaling.158 These tracers provided important insights into dopaminergic dysfunction in both healthy and diseased states. Advances in radiochemistry have since led to the development of more selective PET tracers capable of targeting individual dopamine receptor subtypes. For example, recently developed D1 receptor agonist tracers allow researchers to evaluate receptor activation and signaling in vivo, providing a more detailed understanding of dopaminergic function in primate models.159
Current research is also expanding toward multimodal and dual-target imaging approaches that can simultaneously assess dopaminergic abnormalities and other pathological features of neurodegenerative disease. In a recent preclinical study, investigators employed complementary PET tracers to examine both dopamine transporter function and amyloid plaque accumulation within the same model. This strategy provided a more comprehensive evaluation of disease pathology and may enhance the accuracy of diagnostic imaging for neurodegenerative disorders.155
Future Potential of Dopamine Nanotheranostics
The integration of targeted nanocarriers with advanced imaging technologies is expected to significantly enhance the diagnosis and treatment of dopamine-related disorders. Nanoparticles capable of carrying therapeutic agents while simultaneously providing imaging contrast could allow clinicians to monitor drug delivery, track disease progression, and personalize treatment strategies. Continued progress in nanoparticle engineering, radiochemistry, and molecular imaging will likely expand the role of nanotheranostics in neurology and precision medicine.
Safety and Regulatory Considerations
Despite the significant potential of nanomedicine to overcome many limitations of conventional brain drug delivery, concerns regarding biocompatibility, long-term safety, and regulatory acceptance remain important obstacles to clinical translation. Nanoparticles possess unique physicochemical properties that facilitate transport across biological barriers; however, these same properties may also promote unforeseen biological interactions, including cytotoxic effects, immune system activation, and tissue retention. Therefore, comprehensive evaluation of nanoparticle safety profiles is essential to ensure the successful translation of dopamine-targeted nanomedicines into clinical practice.
Nanoparticle Toxicity
The biological effects and potential toxicity of nanoparticles are strongly influenced by their physicochemical properties, including size, morphology, surface charge, and material composition. Research has demonstrated that some nanoparticles can trigger oxidative stress, disrupt mitochondrial function, and cause DNA damage, ultimately impairing cellular health and, in severe cases, leading to apoptosis. These adverse effects are often linked to the excessive production of reactive oxygen species (ROS) following nanoparticle internalization by cells.160 Metal-based nanoparticles, such as silver or gold nanoparticles, have attracted particular attention because of their potential to interact with proteins and intracellular components. Small nanoparticles can enter cellular compartments and interfere with normal biochemical pathways, while heavy-metal particles may induce oxidative stress and inflammation within neural tissues.
Experimental in vivo studies have demonstrated that exposure to engineered nanoparticles may result in neurotoxicity and systemic toxicity depending on the material composition and dosage. For example, carbon nanotubes have been reported to cause pulmonary, cardiovascular, and neurological toxicities in animal models following systemic exposure.161 More recent experimental investigations continue to highlight the importance of dose and nanoparticle formulation. More recent investigations continue to emphasize the importance of comprehensive safety evaluations. A 2025 in vivo study examining various inorganic nanoparticles identified measurable immune and systemic responses following exposure, highlighting the need for rigorous toxicological assessment before these materials can be safely translated into clinical applications.162
Immune Responses to Nanoparticles
The interaction of nanoparticles with the immune system remains a significant concern in the development of nanomedicine-based therapies. Upon entering the bloodstream, nanoparticles are rapidly surrounded by circulating plasma proteins, forming a so-called protein corona. This adsorbed protein layer can substantially alter the nanoparticle’s biological behavior, influencing its biodistribution, cellular uptake, and recognition by immune cells.
Numerous studies have shown that nanoparticle exposure can activate immune pathways and provoke inflammatory responses, particularly in the case of certain inorganic nanomaterials. Internalization of nanoparticles by macrophages and other immune cells may stimulate the production of pro-inflammatory cytokines, potentially leading to both systemic and neuroinflammatory effects.163 Nevertheless, advances in nanoparticle design have demonstrated that these immune responses can be mitigated through appropriate surface modification strategies. For instance, functionalized mesoporous silica nanoparticles have been reported to exhibit efficient cellular uptake while eliciting minimal cytokine secretion and inflammatory signaling, underscoring the critical role of surface engineering in enhancing nanoparticle biocompatibility and safety.164
Long-Term Accumulation and Biodistribution
Another critical concern in nanoparticle-based drug delivery is the potential for long-term accumulation in tissues. Because certain nanomaterials are not biodegradable, they may persist within organs such as the liver, spleen, or brain for extended periods of time. Persistent accumulation can interfere with normal physiological processes and may lead to chronic toxicity.
Studies investigating gold nanoparticles have demonstrated that although these materials are generally considered biocompatible, their long-term biological effects remain under debate. Experimental animal studies have shown that accumulation of gold nanoparticles in tissues may produce histological alterations and physiological changes depending on particle size, coating, and dose.165,166 Earlier work on carbon nanoparticles also demonstrated accumulation within brain structures such as the olfactory bulb following inhalation exposure, which was associated with inflammatory activation of microglial cells.167 These findings highlight the importance of evaluating nanoparticle biodistribution and clearance mechanisms when developing CNS-targeted nanotherapies.
Barriers to Clinical Translation and Regulation
Despite encouraging results in preclinical studies, relatively few nanoparticle-based therapeutics have successfully progressed to clinical use. One major obstacle is the lack of standardized regulatory frameworks for evaluating nanoparticle safety and efficacy. Because nanomaterials behave differently from conventional pharmaceuticals, traditional toxicological testing methods may not adequately predict their biological effects. Continued collaboration among researchers, regulatory agencies, and industry will therefore be essential for translating dopamine-targeted nanomedicine from laboratory studies to clinical practice.
Several lipid-based and polymer-assisted delivery systems have demonstrated clinical utility in improving drug pharmacokinetics, stability, and tissue distribution; however, translation of dopamine-targeted nanotherapeutics remains largely at the experimental stage. One of the major barriers limiting clinical progression is the complexity associated with large-scale manufacturing and reproducibility of nanocarrier systems. Variability in particle size distribution, surface charge, cargo loading efficiency, and long-term storage stability can significantly influence therapeutic performance and regulatory approval outcomes. In addition, the biological behavior of nanoparticles within the central nervous system remains incompletely understood, particularly regarding long-term biodistribution, clearance mechanisms, immunogenicity, and potential neurotoxicity following repeated administration.
Regulatory agencies also require extensive characterization of nanocarrier composition, batch consistency, pharmacokinetics, toxicity, and manufacturing quality control prior to clinical approval. These requirements can be particularly challenging for biologically derived systems such as exosomes and biomimetic vesicles, where heterogeneity and scalability remain major concerns. Cost-effectiveness and manufacturing scalability further influence translational feasibility, as highly engineered nanosystems often require complex production and purification processes that may limit widespread clinical adoption. Consequently, future progress in dopamine-targeted nanomedicine will depend not only on improving therapeutic efficacy and BBB targeting efficiency but also on developing standardized, reproducible, scalable, and regulatory-compliant manufacturing strategies capable of supporting large-scale clinical translation.
Future Perspectives
Although significant progress has been made in dopamine pharmacology and nanomedicine-based drug delivery, several emerging technologies are expected to reshape future therapeutic strategies for dopamine-related disorders. Advances in artificial intelligence, structure-guided receptor targeting, gene therapy, and precision nanomedicine are opening new directions for improving treatment efficacy while minimizing adverse effects. However, future advances in this field will likely involve AI-assisted nanocarrier engineering, precision-targeted and stimuli-responsive delivery systems, biomimetic vesicles, and patient-specific therapeutic strategies capable of adapting to disease-specific CNS microenvironments.
AI-Guided Dopamine Ligand Design
Artificial intelligence (AI) and machine learning are increasingly transforming the discovery of dopaminergic therapeutics by enabling rapid identification and optimization of receptor-selective ligands and prediction of pharmacokinetic properties. Traditional drug discovery approaches rely heavily on trial-and-error screening, whereas AI-driven platforms can analyze large chemical datasets, predict ligand-receptor interactions, and design novel compounds with desired biological activity. Recent advances in deep learning and generative models now allow exploration of vast chemical space and facilitate the design of molecules with optimized binding affinity, selectivity, and brain penetration potential.168,169
Improving Dopamine Receptor Subtype Selectivity
Achieving selectivity among dopamine receptor subtypes (D1-D5) remains one of the central challenges in dopaminergic drug development. Machine-learning-based molecular modeling has recently been used to analyze large datasets of dopamine receptor ligands and predict subtype-specific binding patterns. For example, graph neural network models trained on thousands of dopamine receptor ligands have demonstrated strong predictive performance for receptor selectivity, enabling identification of compounds with preferential activity at specific receptor subtypes.170 Complementary computational studies combining in-silico screening with experimental validation have identified ligands with high affinity and selectivity for D2/D3 receptor subtypes, demonstrating the value of AI-guided approaches for rational ligand design.171
More broadly, AI-driven drug discovery platforms can integrate structural biology, molecular docking, and predictive modeling to accelerate the optimization of dopamine receptor ligands and reduce development timelines.172
BBB Permeability Prediction Modeling
In addition to optimizing receptor binding, AI methods are increasingly applied to predict whether candidate molecules can cross the blood-brain barrier (BBB), a critical requirement for therapies targeting neurological disorders. Recent deep-learning models have been developed to classify compounds as BBB-permeable or non-permeable using molecular descriptors and structural features, enabling early identification of brain-penetrant drug candidates.173
Machine-learning approaches such as random forest, neural networks, and ensemble algorithms have shown strong performance in predicting BBB permeability and guiding lead optimization during drug discovery.174,175 For example, quantitative models such as LogBB-Pred have demonstrated high accuracy in predicting BBB permeability of drug-like compounds, illustrating the potential of computational tools to accelerate CNS drug development.176
The integration of AI-guided ligand discovery with predictive BBB modeling represents a powerful strategy for developing next-generation dopaminergic therapeutics. By combining molecular design, pharmacokinetic prediction, and receptor selectivity optimization, AI-driven approaches have the potential to significantly accelerate the discovery of safer and more effective treatments for dopamine-related neurological disorders.
Receptor Subtype-Selective Targeting
One of the longstanding challenges in dopamine pharmacology is the development of ligands that selectively target individual receptor subtypes. Structural biology has provided critical insights that are now guiding medicinal chemistry efforts. Chien et al solved the crystal structure of the human dopamine D3 receptor bound to an antagonist, revealing key binding interactions responsible for ligand recognition and subtype selectivity.177 More recently, another study determined the structure of the dopamine D2 receptor in complex with the Gi protein, providing a detailed view of receptor activation and signaling mechanisms.178 These structural advances are enabling rational drug design approaches aimed at developing ligands with improved specificity for D1-like or D2-like receptor families, which may reduce off-target effects associated with current therapies.
Gene Delivery Strategies
Gene therapy represents another promising direction for treating dopamine-related neurological disorders, particularly Parkinson’s disease. One early clinical study demonstrated that adeno-associated virus (AAV)-mediated delivery of the aromatic L-amino acid decarboxylase gene to the striatum improved motor function in Parkinson’s disease patients.179 These approaches aim to provide long-term therapeutic effects by enabling neurons to produce dopamine continuously rather than relying on repeated drug administration. More recent advances in nanotechnology have also introduced nanoparticle-based gene delivery systems capable of transporting nucleic acids across biological barriers, including the blood-brain barrier. These systems may provide safer and more controllable alternatives to viral vectors for treating dopamine-related disorders.
Smart Stimuli-Responsive Nanocarriers
Recent advances in nanomedicine have led to the development of smart stimuli-responsive nanocarriers capable of releasing therapeutic agents in response to specific biological signals. Unlike conventional drug delivery systems, these platforms remain relatively stable during circulation but undergo structural or chemical changes when exposed to physiological triggers such as pH shifts, enzyme activity, or oxidative stress. Such systems enable controlled and site-specific drug release, thereby improving therapeutic efficacy while minimizing systemic toxicity.180,181
pH-Sensitive Nanocarriers
pH-responsive nanocarriers are among the most extensively studied smart delivery systems. These nanoparticles are designed to remain stable under physiological pH but undergo structural changes or polymer degradation under acidic conditions, which are commonly observed in diseased tissues and intracellular compartments such as endosomes and lysosomes. Research has demonstrated that pH-responsive nanosystems can selectively release therapeutic cargo in acidic microenvironments, improving drug accumulation at target sites while reducing off-target exposure.182,183
Recent developments have focused on engineering polymers and lipid systems that undergo charge conversion, membrane destabilization, or bond cleavage under mildly acidic conditions. Such mechanisms allow nanoparticles to enhance intracellular drug release and improve therapeutic performance in various disease models.184
Enzyme-Responsive Nanocarriers
Another promising strategy involves nanocarriers that respond to enzyme activity associated with pathological environments. These systems incorporate enzyme-cleavable linkers or coatings that remain stable during circulation but degrade when exposed to disease-related enzymes, enabling controlled drug release at the target site. Recent research highlights that enzyme-responsive materials can be designed to respond to specific biological signals and trigger localized drug release, thereby increasing therapeutic precision.185 Such systems are particularly attractive for neurological disorders and cancer, where specific enzymes are overexpressed and can act as biological triggers for drug activation.
ROS-Triggered Drug Release
Reactive oxygen species (ROS) are increasingly recognized as important internal triggers for smart drug delivery systems. Elevated ROS levels are commonly observed in pathological conditions such as neurodegeneration, inflammation, and cancer. Consequently, ROS-responsive nanocarriers have been developed that undergo chemical bond cleavage or structural changes when exposed to oxidative environments, resulting in targeted drug release.186,187
Recent studies suggest that ROS-responsive systems may be particularly useful in neurological disorders, where oxidative stress plays a central role in disease progression. By exploiting disease-associated ROS levels, these nanocarriers can provide site-specific drug delivery and improved therapeutic outcomes.188 Furthermore, multifunctional ROS-responsive nanoplatforms are being developed that combine drug delivery with antioxidant or imaging capabilities, representing an important direction for future nanomedicine research.
Personalized Nanomedicine
Advances in genomics, biomarker discovery, and precision medicine are enabling more individualized approaches to the treatment of neurological diseases. Nanoparticle drug delivery systems can be engineered to respond to specific molecular signals present in diseased tissues, allowing targeted drug release and reduced systemic toxicity. Densely PEG-coated nanoparticles could penetrate brain tissue more effectively than conventional particles, illustrating how nanocarrier design can be tailored to overcome biological barriers was demonstrated by Nance et al189 Similarly, Saraiva et al developed targeted nanoparticles capable of delivering therapeutic agents across the blood-brain barrier, highlighting the potential of precision nanomedicine strategies for treating neurological disorders.190 In the future, integrating patient-specific genetic and molecular information with advanced nanotechnology may enable customized treatment approaches for disorders involving dopaminergic dysfunction.
Clinical Outlook: Why Translation Remains Difficult
Despite significant progress in nanomedicine and dopaminergic drug delivery, translation from preclinical research to successful clinical therapies remains challenging. Numerous nanocarrier systems have demonstrated promising results in animal models; however, only a limited number of nanomedicine platforms have reached clinical application for neurological diseases. Several biological, technological, and regulatory factors continue to limit successful translation.
Rodent vs Human Blood-Brain Barrier Differences
One major barrier to translation arises from fundamental physiological differences between animal models and humans. Many nanomedicine strategies are validated in rodents, yet the structure and function of the blood-brain barrier (BBB) vary across species. Comparative studies show differences in transporter expression and barrier permeability between rodents and humans, which can significantly influence drug distribution in the brain. For instance, research indicates that expression and activity of the efflux transporter P-glycoprotein differ between species, affecting central nervous system drug exposure and therapeutic outcomes.191
Experimental evidence also suggests that BBB permeability and transport mechanisms are not identical between rodents and humans, meaning that drug delivery results obtained in animal models may not directly translate to clinical settings.192 These interspecies differences complicate the prediction of therapeutic efficacy and highlight the need for improved translational models, including humanized systems and advanced in vitro BBB platforms.
Manufacturing and Scaling Challenges
Another major limitation in the translation of nanomedicine is the difficulty of scaling up nanoparticle production while maintaining reproducibility and quality. Laboratory-scale synthesis methods often rely on complex multistep processes that are difficult to standardize for industrial manufacturing. Studies examining the development of nanomedicine platforms emphasize that reproducible large-scale production, robust characterization methods, and regulatory compliance remain major hurdles for clinical development.193,194
In addition, the physicochemical properties of nanoparticles, such as size distribution, surface chemistry, and stability, can change during scale-up, potentially altering their biological behavior and therapeutic performance. These challenges must be addressed before nanomedicine formulations can move from experimental studies to clinical trials.
Clinical Trial Design Complexity
Clinical evaluation of nanomedicines presents unique challenges compared with traditional small-molecule drugs. The complexity of nanoparticle systems introduces additional variables related to biodistribution, immune interactions, and pharmacokinetics. Reviews of translational nanomedicine research highlight that inadequate understanding of disease heterogeneity, difficulties in patient selection, and regulatory uncertainty can complicate clinical trial design and interpretation.193,195
Furthermore, many preclinical studies rely on simplified disease models that do not fully replicate the complexity of human neurological disorders. As a result, promising experimental therapies may fail during clinical evaluation.
Dose Translation from Animals to Humans
Determining appropriate dosing strategies represents another critical challenge in translating nanomedicine therapies. Nanoparticle biodistribution is influenced by multiple factors including particle size, surface chemistry, and interactions with biological proteins, making dose extrapolation from animal models difficult. Differences in BBB transport, metabolism, and clearance between species further complicate dose prediction and therapeutic optimization. Because nanocarriers often exhibit nonlinear pharmacokinetics, conventional dose scaling approaches used for small molecules may not accurately predict human responses. Improved computational models and translational pharmacology approaches are therefore needed to guide dose selection during clinical development.
Long-Term Safety and Biological Interactions
Long-term safety remains one of the most important considerations for nanomedicine therapies targeting the brain. Nanoparticles can accumulate in tissues, interact with immune cells, and potentially induce chronic toxicity or inflammation. Studies analyzing clinical translation emphasize that incomplete understanding of nanoparticle-biological interactions and long-term biodistribution remains a major barrier to regulatory approval.193,196 In addition, subtle differences in nanoparticle composition, surface charge, and ligand decoration can significantly influence safety profiles, making standardized evaluation essential for clinical development.
Together, these challenges illustrate that successful translation of dopaminergic nanotherapies requires more than promising preclinical results. Advances in human-relevant disease models, scalable manufacturing technologies, improved clinical trial design, and comprehensive safety assessment will be essential for bridging the gap between experimental nanomedicine research and effective therapies for neurological disorders.
Conclusion
Nanomedicine-based strategies have demonstrated substantial potential for overcoming the major limitations associated with conventional dopaminergic therapies, including poor BBB penetration, rapid metabolism, oxidative degradation, and systemic toxicity. Among the various nanosystems investigated, polymeric nanoparticles, lipid-based nanocarriers, and exosome-inspired vesicles appear particularly promising due to their ability to enhance dopamine stability, facilitate controlled release, improve BBB transport, and enable targeted delivery to dopaminergic brain regions. Importantly, these nanocarriers not only improve dopamine delivery efficiency but also function as protective microenvironments that reduce dopamine oxidation and reactive oxygen species (ROS)-associated neurotoxicity, thereby improving therapeutic stability and neuroprotective potential. Despite encouraging preclinical outcomes, major translational challenges remain, including manufacturing scalability, reproducibility, long-term safety evaluation, regulatory standardization, and limited clinical validation of dopamine-targeted nanotherapeutics. Future advances in this field will likely involve AI-assisted nanocarrier engineering, precision-targeted and stimuli-responsive delivery systems, biomimetic vesicles, and patient-specific therapeutic strategies capable of adapting to disease-specific CNS microenvironments. Continued interdisciplinary collaboration among nanotechnologists, neuroscientists, clinicians, and regulatory agencies will be essential for translating these emerging nanomedicine approaches into safe and clinically effective therapies for neurodegenerative disorders such as Parkinson’s disease.
Data Sharing Statement
No new data was generated or analyzed in the preparation of this review article.
Acknowledgments
All figures in this manuscript were created using BioRender.com.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Disclosure
The authors declare that they have no competing financial interests or personal relationships that could have influenced the work reported in this paper.
References
1. Neve KA. The dopamine receptors. In: The Receptors.
2. Poewe W, Seppi K, Tanner CM, et al. Parkinson disease. Nat Rev Dis Primers. 2017;3(1):17013. doi:10.1038/nrdp.2017.13
3. Speranza L, Miniaci MC, Volpicelli F. The role of dopamine in neurological, psychiatric, and metabolic disorders and cancer: a complex web of interactions. MDPI. 2025;13:492.
4. Klein MO, Battagello DS, Cardoso AR, Hauser DN, Bittencourt JC, Correa RG. Dopamine: functions, signaling, and association with neurological diseases. Cell Mol Neurobiol. 2019;39(1):31–32. doi:10.1007/s10571-018-0632-3
5. Pardridge WM. Drug transport across the blood–brain barrier. J Cereb Blood Flow Metab. 2012;32(11):1959–1972. doi:10.1038/jcbfm.2012.126
6. Pattison DI, Dean RT, Davies MJ. Oxidation of DNA, proteins and lipids by DOPA, protein-bound DOPA, and related catechol (amine) s. Toxicology. 2002;177(1):23–37. doi:10.1016/S0300-483X(02)00193-2
7. Patra S, Namballa HK, Gudipally AR, Xie L, Xie L, Harding WW. Discovery of a selective α2C-AR scaffold from a molecular hybridization approach. Bioorg Med Chem. 2025;131:118424. doi:10.1016/j.bmc.2025.118424
8. Niazi SK. Non-invasive drug delivery across the blood–brain barrier: a prospective analysis. Pharmaceutics. 2023;15(11):2599. doi:10.3390/pharmaceutics15112599
9. Kaur S, Singh S, Jaiswal G, et al. Pharmacology of dopamine and its receptors. In: Frontiers in Pharmacology of Neurotransmitters. Springer; 2020:143–182.
10. Myslivecek J. Dopamine and dopamine-related ligands can bind not only to dopamine receptors. Life. 2022;12(5):606. doi:10.3390/life12050606
11. LeWitt PA. Rethinking the role of continuous dopaminergic stimulation in Parkinson disease therapy. Parkinsonism Related Disord. 2025;139:107354. doi:10.1016/j.parkreldis.2025.107354
12. Domínguez A, Álvarez A, Hilario E, Suarez-Merino B, Goñi-de-Cerio F. Central nervous system diseases and the role of the blood-brain barrier in their treatment. Neurosci Discov. 2013;1(1):3. doi:10.7243/2052-6946-1-3
13. Bors LA, Erdő F. Overcoming the blood–brain barrier. challenges and tricks for CNS drug delivery. Scientia Pharmaceut. 2019;87(1):6. doi:10.3390/scipharm87010006
14. Haddad F, Sawalha M, Khawaja Y, Najjar A, Karaman R. Dopamine and levodopa prodrugs for the treatment of Parkinson’s disease. Molecules. 2017;23(1):40. doi:10.3390/molecules23010040
15. Riederer P, Strobel S, Nagatsu T, et al. Levodopa treatment: impacts and mechanisms throughout Parkinson’s disease progression: p. Riederer et al. J Neural Transm. 2025;132(6):743–779. doi:10.1007/s00702-025-02893-4
16. Saraswathi TS, Mothilal M, Bukke SPN, Thalluri C, Chettupalli AK. Recent advances in potential drug nanocarriers for CNS disorders: a review. Biomed Eng Online. 2025;24(1):137. doi:10.1186/s12938-025-01474-6
17. Toader C, Dumitru AV, Eva L, Serban M, Covache-Busuioc R-A, Ciurea AV. Nanoparticle strategies for treating CNS disorders: a comprehensive review of drug delivery and theranostic applications. Int J Mol Sci. 2024;25(24):13302. doi:10.3390/ijms252413302
18. Senanayake D, Yapa P, Dabare S, Munaweera I. Precision targeting of the CNS: recent progress in brain-directed nanodrug delivery. RSC Adv. 2025;15(32):25910–25928. doi:10.1039/D5RA03578C
19. Moura RP, Martins C, Pinto S, Sousa F, Sarmento B. Blood-brain barrier receptors and transporters: an insight on their function and how to exploit them through nanotechnology. Expert Opin Drug Delivery. 2019;16(3):271–285. doi:10.1080/17425247.2019.1583205
20. Nieoullon A, Coquerel A. Dopamine: a key regulator to adapt action, emotion, motivation and cognition. Curr Opin Neurol. 2003;16 Suppl 2(S3–9):S3–9.
21. Berridge KC, Kringelbach ML. Pleasure systems in the brain. Neuron. 2015;86(3):646–664. doi:10.1016/j.neuron.2015.02.018
22. Hussain T, Lokhandwala MF. Renal dopamine receptors and hypertension. Exp Biol Med. 2003;228(2):134–142. doi:10.1177/153537020322800202
23. Rubi B, Maechler P. Minireview: new roles for peripheral dopamine on metabolic control and tumor growth: let’s seek the balance. Endocrinology. 2010;151(12):5570–5581. doi:10.1210/en.2010-0745
24. Buttarelli FR, Fanciulli A, Pellicano C, Pontieri FE. The dopaminergic system in peripheral blood lymphocytes: from physiology to pharmacology and potential applications to neuropsychiatric disorders. Curr Neuropharmacol. 2011;9(2):278–288. doi:10.2174/157015911795596612
25. Brodde OE. Vascular dopamine receptors: demonstration and characterization by in vitro studies. Life Sci. 1982;31(4):289–306. doi:10.1016/0024-3205(82)90406-4
26. Meiser J, Weindl D, Hiller K. Complexity of dopamine metabolism. Cell Commun Signal. 2013;11(1):34. doi:10.1186/1478-811X-11-34
27. Hiroi T, Imaoka S, Funae Y. Dopamine formation from tyramine by CYP2D6. Biochem Biophys Res Commun. 1998;249(3):838–843. doi:10.1006/bbrc.1998.9232
28. Bromek E, Haduch A, Golembiowska K, Daniel WA. Cytochrome P450 mediates dopamine formation in the brain in vivo. J Neurochem. 2011;118(5):806–815. doi:10.1111/j.1471-4159.2011.07339.x
29. Elsworth JD, Roth RH. Dopamine synthesis, uptake, metabolism, and receptors: relevance to gene therapy of Parkinson’s disease. Exp Neurol. 1997;144(1):4–9. doi:10.1006/exnr.1996.6379
30. Eriksen J, Jorgensen TN, Gether U. Regulation of dopamine transporter function by protein-protein interactions: new discoveries and methodological challenges. J Neurochem. 2010;113(1):27–41. doi:10.1111/j.1471-4159.2010.06599.x
31. Uhl GR, Hall FS, Sora I. Cocaine, reward, movement and monoamine transporters. Mol Psych. 2002;7(1):21–26. doi:10.1038/sj.mp.4000964
32. Gainetdinov RR, Sotnikova TD, Caron MG. Monoamine transporter pharmacology and mutant mice. Trends Pharmacol Sci. 2002;23(8):367–373. doi:10.1016/s0165-6147(02)02044-8
33. Eisenhofer G, Kopin IJ, Goldstein DS. Catecholamine metabolism: a contemporary view with implications for physiology and medicine. Pharmacol Rev. 2004;56(3):331–349. doi:10.1124/pr.56.3.1
34. Ye N, Neumeyer JL, Baldessarini RJ, Zhen X, Zhang A. Update 1 of: recent progress in development of dopamine receptor subtype-selective agents: potential therapeutics for neurological and psychiatric disorders. Chem Rev. 2013;113(5):PR123–78. doi:10.1021/cr300113a
35. Harris J, Stanford PM, Oakes SR, Ormandy CJ. Prolactin and the prolactin receptor: new targets of an old hormone. Ann Med. 2004;36(6):414–425. doi:10.1080/07853890410033892
36. Bostwick JR, Guthrie SK, Ellingrod VL. Antipsychotic-induced hyperprolactinemia. Pharmacotherapy. 2009;29(1):64–73. doi:10.1592/phco.29.1.64
37. Maguire GA. Prolactin elevation with antipsychotic medications: mechanisms of action and clinical consequences. J Clin Psychiatry. 2002;63 Suppl 4:56–62.
38. Monzani E, Nicolis S, Dell’Acqua S, et al. Dopamine, oxidative stress and protein–quinone modifications in Parkinson’s and other neurodegenerative diseases. Angew Chem Int Ed. 2019;58(20):6512–6527. doi:10.1002/anie.201811122
39. Tansey MG, McCoy MK, Frank-Cannon TC. Neuroinflammatory mechanisms in Parkinson’s disease: potential environmental triggers, pathways, and targets for early therapeutic intervention. Exp Neurol. 2007;208(1):1–25. doi:10.1016/j.expneurol.2007.07.004
40. Cenci MA, Lundblad M. Post- versus presynaptic plasticity in L-DOPA-induced dyskinesia. J Neurochem. 2006;99(2):381–392. doi:10.1111/j.1471-4159.2006.04124.x
41. Yang Y. Functional selectivity of dopamine D1 receptor signaling: retrospect and prospect. Int J Mol Sci. 2021;22(21):11914. doi:10.3390/ijms222111914
42. Graham DG. Oxidative pathways for catecholamines in the genesis of neuromelanin and cytotoxic quinones. Mol Pharmacol. 1978;14(4):633–643. doi:10.1016/S0026-895X(25)13535-9
43. Salat D, Tolosa E. Levodopa in the treatment of Parkinson’s disease: current status and new developments. J Parkinsons Dis. 2013;3(3):255–269. doi:10.3233/JPD-130186
44. Obeso JA, Olanow CW, Nutt JG. Levodopa motor complications in Parkinson’s disease. Trends Neurosci. 2000;23:S2–S7. doi:10.1016/S1471-1931(00)00031-8
45. Mueller T, Russ H. Levodopa, motor fluctuations and dyskinesia in Parkinson’s disease. Expert Opi Pharmacother. 2006;7(13):1715–1730. doi:10.1517/14656566.7.13.1715
46. van Laar T. Levodopa-induced response fluctuations in patients with Parkinson’s disease: strategies for management. CNS Drugs. 2003;17(7):475–489. doi:10.2165/00023210-200317070-00002
47. Borovac JA. Side effects of a dopamine agonist therapy for Parkinson’s disease: a mini-review of clinical pharmacology. Yale J Biol Med. 2016;89(1):37.
48. Weintraub D, Koester J, Potenza MN, et al. Impulse control disorders in Parkinson disease: a cross-sectional study of 3090 patients. Arch Neurol. 2010;67(5):589–595. doi:10.1001/archneurol.2010.65
49. Jiao Y, Yang L, Wang R, et al. Drug delivery across the blood–brain barrier: a new strategy for the treatment of neurological diseases. Pharmaceutics. 2024;16(12):1611. doi:10.3390/pharmaceutics16121611
50. Harini K, Durgadevi P, Girigoswami K, Girigoswami A. Transitioning from conventional therapies to nanomedicine-based therapeutics for major depressive disorder. Biomed Res Ther. 2025;12(12):8072–8099. doi:10.15419/z5q8dv72
51. Qin L, Wang X, Liang T, et al. Research progress of blood-brain barrier penetrating and brain diseases therapy by natural biopolymer-based nanomedicine delivery systems. Mater Today Bio. 2026;2026:102849.
52. Brightman M, Reese T. Junctions between intimately apposed cell membranes in the vertebrate brain. J Cell Biol. 1969;40(3):648–677. doi:10.1083/jcb.40.3.648
53. Bourdy R, Sanchez-Catalan MJ, Kaufling J, et al. Control of the nigrostriatal dopamine neuron activity and motor function by the tail of the ventral tegmental area. Neuropsychopharmacology. 2014;39(12):2788–2798. doi:10.1038/npp.2014.129
54. Tepper JM, Lee CR. GABAergic control of substantia nigra dopaminergic neurons. Prog Brain Res. 2007;160:189–208. doi:10.1016/S0079-6123(06)60011-3
55. Kravitz AV, Kreitzer AC. Striatal mechanisms underlying movement, reinforcement, and punishment. Physiology. 2012;27(3):167–177. doi:10.1152/physiol.00004.2012
56. Olanow CW, Stern MB, Sethi K. The scientific and clinical basis for the treatment of Parkinson disease (2009). Neurology. 2009;72(21_supplement_4):S1–S136. doi:10.1212/WNL.0b013e3181a1d44c
57. Schapira A. Present and future drug treatment for Parkinson’s disease. J Neurol Neurosurg. 2005;76(11):1472–1478. doi:10.1136/jnnp.2004.035980
58. Jenner P. Dopamine agonists, receptor selectivity and dyskinesia induction in Parkinson’s disease. Current Opin Neurol. 2003;16:S3–S7. doi:10.1097/00019052-200312001-00002
59. van Laar T, Borgemeester R. The need for non-oral therapy in Parkinson’s disease; a potential role for apomorphine. Parkinsonism Related Disord. 2016;33:S22–S27. doi:10.1016/j.parkreldis.2016.11.019
60. Trenkwalder C, Chaudhuri KR, Ruiz PJG, et al. Expert consensus group report on the use of apomorphine in the treatment of Parkinson’s disease–clinical practice recommendations. Parkinsonism Related Disord. 2015;21(9):1023–1030. doi:10.1016/j.parkreldis.2015.06.012
61. Kapur S, Mamo D. Half a century of antipsychotics and still a central role for dopamine D2 receptors. Prog Neuro Psychopharmacol Biol Psychiatry. 2003;27(7):1081–1090. doi:10.1016/j.pnpbp.2003.09.004
62. Kim DH, Stahl SM. Antipsychotic drug development. Behav Neurobiol Schizophrenia Treatment. 2010;2010:123–139.
63. Meltzer HY. Update on typical and atypical antipsychotic drugs. Annual Rev Med. 2013;64(1):393–406. doi:10.1146/annurev-med-050911-161504
64. Miyamoto S, Duncan GE, Marx CE, Lieberman JA. Treatments for schizophrenia: a critical review of pharmacology and mechanisms of action of antipsychotic drugs. Mol Psychiatry. 2005;10(1):79–104. doi:10.1038/sj.mp.4001556
65. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic: a double-blind comparison with chlorpromazine. Arch Gen Psychiatry. 1988;45(9):789–796. doi:10.1001/archpsyc.1988.01800330013001
66. Kd B, Molski TF, Xu C. Aripiprazole, a novel antipsychotic, is a high-affinity partial agonist at human dopamine D2 receptors. J Pharmacol Exp Ther. 2002;302:381–389. doi:10.1124/jpet.102.033175
67. Lieberman JA. Dopamine partial agonists: a new class of antipsychotic. CNS Drugs. 2004;18(4):251–267. doi:10.2165/00023210-200418040-00005
68. Zha S, Liu H, Li H, Li H, Wong K-L, All AH. Functionalized nanomaterials capable of crossing the blood–brain barrier. ACS Nano. 2024;18(3):1820–1845. doi:10.1021/acsnano.3c10674
69. Mokarram N, Case A, Hossainy NN, Lyon JG, MacDonald TJ, Bellamkonda R. Device-assisted strategies for drug delivery across the blood-brain barrier to treat glioblastoma. Communicat Mater. 2025;6(1):5. doi:10.1038/s43246-024-00721-y
70. Armulik A, Genové G, Mäe M, et al. Pericytes regulate the blood–brain barrier. Nature. 2010;468(7323):557–561. doi:10.1038/nature09522
71. Fong CW. Permeability of the blood–brain barrier: molecular mechanism of transport of drugs and physiologically important compounds. J Membrane Biol. 2015;248(4):651–669. doi:10.1007/s00232-015-9778-9
72. Liu J, Wang T, Dong J, Lu Y. The blood–brain barriers: novel nanocarriers for central nervous system diseases. J Nanobiotechnol. 2025;23(1):146. doi:10.1186/s12951-025-03247-8
73. Wade L, Katzman R. Synthetic amino acids and the nature of L‐DOPA transport at the blood‐brain barrier. J Neurochem. 1975;25(6):837–842. doi:10.1111/j.1471-4159.1975.tb04415.x
74. Friden PM, Walus LR, Watson P, et al. Blood-brain barrier penetration and in vivo activity of an NGF conjugate. Science. 1993;259(5093):373–377. doi:10.1126/science.8420006
75. Lu W. Adsorptive-mediated brain delivery systems. Current Pharm Biotechnol. 2012;13(12):2340–2348. doi:10.2174/138920112803341851
76. Ding L, Kshirsagar P, Agrawal P, Murry DJ. Crossing the blood–brain barrier: innovations in receptor-and transporter-mediated transcytosis strategies. Pharmaceutics. 2025;17(6):706. doi:10.3390/pharmaceutics17060706
77. Schinkel A, Smit J, van Tellingen M, et al. Disruption of the mouse mdr1a P-glycoprotein gene leads to a deficiency in the blood-brain barrier and to increased sensitivity to drugs. Cell. 1994;77(4):491–502. doi:10.1016/0092-8674(94)90212-7
78. Hardebo JE, Owman C. Barrier Mechanisms for Neurotransmitter Monoamines and Their Precursors at the Blood‐brain Interface. Wiley Online Library; 1980:1–11.
79. Juarez B, Han M-H. Diversity of dopaminergic neural circuits in response to drug exposure. Neuropsychopharmacology. 2016;41(10):2424–2446. doi:10.1038/npp.2016.32
80. Razavi R, Khajouei G, Divsalar F, Dawi E, Amiri M. Recent advances on brain drug delivery via nanoparticles: alternative future materials for neuroscience applications; a review. Rev Neurosci. 2025;36(4):405–430. doi:10.1515/revneuro-2024-0086
81. Kulkarni M, Patel K, Patel A, et al. Nanomaterials as drug delivery agents for overcoming the blood-brain barrier: a comprehensive review. ADMET DMPK. 2024;12(1):63–105. doi:10.5599/admet.2043
82. Kochman U, Sitka H, Kuźniar J, et al. Targeted nanoparticles for drug delivery across the blood–brain barrier in early and late stages of Alzheimer’s disease: a review. Mol Neurobiol. 2026;63(1):75. doi:10.1007/s12035-025-05417-z
83. Pahuja R, Seth K, Shukla A, et al. Trans-blood brain barrier delivery of dopamine-loaded nanoparticles reverses functional deficits in parkinsonian rats. ACS Nano. 2015;9(5):4850–4871. doi:10.1021/nn506408v
84. Monge-Fuentes V, Biolchi Mayer A, Lima MR, et al. Dopamine-loaded nanoparticle systems circumvent the blood–brain barrier restoring motor function in mouse model for Parkinson’s Disease. Sci Rep. 2021;11(1):15185. doi:10.1038/s41598-021-94175-8
85. Danz K, Fleddermann J, Koch M, et al. Evaluation of the transport and binding of dopamine-loaded PLGA nanoparticles for the treatment of Parkinson’s disease using in vitro model systems. Pharmaceutics. 2024;16(5):571. doi:10.3390/pharmaceutics16050571
86. Lababidi JM, HME-S A. Revamping Parkinson’s disease therapy using PLGA-based drug delivery systems. NPJ Parkinson’s Dis. 2025;11(1):248. doi:10.1038/s41531-025-01081-1
87. Zhi K, Raji B, Nookala AR, et al. PLGA nanoparticle-based formulations to cross the blood–brain barrier for drug delivery: from R&D to cGMP. Pharmaceutics. 2021;13(4):500. doi:10.3390/pharmaceutics13040500
88. Awad NS, Paul V, AlSawaftah NM, Husseini GA. Effect of phospholipid head group on ultrasound-triggered drug release and cellular uptake of immunoliposomes. Sci Rep. 2023;13(1):16644. doi:10.1038/s41598-023-43813-4
89. Pattni BS, Chupin VV, Torchilin VP. New developments in liposomal drug delivery. Chem Rev. 2015;115(19):10938–10966. doi:10.1021/acs.chemrev.5b00046
90. Akbarzadeh A, Rezaei-Sadabady R, Davaran S, et al. Liposome: classification, preparation, and applications. Nanoscale Res Lett. 2013;8(1):102. doi:10.1186/1556-276X-8-102
91. Drescher S, van Hoogevest P. The phospholipid research center: current research in phospholipids and their use in drug delivery. Pharmaceutics. 2020;12(12):1235. doi:10.3390/pharmaceutics12121235
92. Lopalco A, Cutrignelli A, Denora N, Lopedota A, Franco M, Laquintana V. Transferrin functionalized liposomes loading dopamine HCl: development and permeability studies across an in vitro model of human blood–brain barrier. Nanomaterials. 2018;8(3):178. doi:10.3390/nano8030178
93. Qu M, Lin Q, He S, et al. A brain targeting functionalized liposomes of the dopamine derivative N-3, 4-bis (pivaloyloxy)-dopamine for treatment of Parkinson’s disease. J Control Release. 2018;277:173–182. doi:10.1016/j.jconrel.2018.03.019
94. Liang Y, Feng L, Zheng Y, et al. Targeted liposomal co-delivery dopamine with 3-n-butylphthalide for effective against parkinson’s disease in mice model. Int J Nanomed. 2024;Volume 19:12851–12870. doi:10.2147/IJN.S483595
95. Dazzi L, Talani G, Trapani G, et al. Nose-to-brain delivery of dopamine to the striatum of rats using neurotransmitter-loaded solid lipid nanoparticles: an in vivo study by brain microdialysis. Neuropharmacology. 2026;287:110830. doi:10.1016/j.neuropharm.2026.110830
96. Trapani A, De Giglio E, Cometa S, et al. Dopamine-loaded lipid based nanocarriers for intranasal administration of the neurotransmitter: a comparative study. Eur J Pharm Biopharm. 2021;167:189–200. doi:10.1016/j.ejpb.2021.07.015
97. Zheng Y, Cui L, Lu H, et al. Nose to brain: exploring the progress of intranasal delivery of solid lipid nanoparticles and nanostructured lipid carriers. Int J Nanomed. 2024;Volume 19:12343–12368. doi:10.2147/IJN.S497480
98. Taha E, Nour SA, Mamdouh W, et al. Cod liver oil nano-structured lipid carriers (Cod-NLCs) as a promising platform for nose to brain delivery: preparation, in vitro optimization, ex vivo cytotoxicity & in vivo biodistribution utilizing radioiodinated zopiclone. Int J Pharm X. 2023;5:100160. doi:10.1016/j.ijpx.2023.100160
99. Sonawane D, Pokharkar V. Nose to brain targeting of the donepezil nanostructured lipid carrier in situ gel: formulation, in vitro, ex vivo, in vivo pharmacokinetic and pharmacodynamic characterization. RSC Pharmaceut. 2024;1(4):820–840. doi:10.1039/D4PM00174E
100. Castellani S, Iaconisi GN, Tripaldi F, et al. Dopamine and citicoline-co-loaded solid lipid nanoparticles as multifunctional nanomedicines for Parkinson’s disease treatment by intranasal administration. Pharmaceutics. 2024;16(8):1048. doi:10.3390/pharmaceutics16081048
101. Abedi-Gaballu F, Dehghan G, Ghaffari M, et al. PAMAM dendrimers as efficient drug and gene delivery nanosystems for cancer therapy. Appl Mater Today. 2018;12:177–190. doi:10.1016/j.apmt.2018.05.002
102. Zarebkohan A, Najafi F, Moghimi HR, Hemmati M, Deevband MR, Kazemi B. Synthesis and characterization of a PAMAM dendrimer nanocarrier functionalized by SRL peptide for targeted gene delivery to the brain. Eur J Pharm Sci. 2015;78:19–30. doi:10.1016/j.ejps.2015.06.024
103. Srinageshwar B, Peruzzaro S, Andrews M, et al. PAMAM dendrimers cross the blood–brain barrier when administered through the carotid artery in C57BL/6J mice. Int J Mol Sci. 2017;18(3):628. doi:10.3390/ijms18030628
104. Ly P-D, Ly K-N, Phan H-L, Nguyen HH, Duong V-A, Nguyen HV. Recent advances in surface decoration of nanoparticles in drug delivery. Front Nanotechnol. 2024;6:1456939. doi:10.3389/fnano.2024.1456939
105. Kołodziejczyk AM, Grala M, Kołodziejczyk Ł. Evaluation of PAMAM dendrimer-stabilized gold nanoparticles: two-stage procedure synthesis and toxicity assessment in MCF-7 breast cancer cells. Molecules. 2025;30(9):2024. doi:10.3390/molecules30092024
106. Alamos-Musre S, Beltrán-Chacana D, Moyano J, et al. From structure to function: the promise of PAMAM dendrimers in biomedical applications. Pharmaceutics. 2025;17(7):927. doi:10.3390/pharmaceutics17070927
107. Sokolova V, Mekky G, van der Meer SB, Seeds MC, Atala AJ, Epple M. Transport of ultrasmall gold nanoparticles (2 nm) across the blood–brain barrier in a six-cell brain spheroid model. Sci Rep. 2020;10(1):18033. doi:10.1038/s41598-020-75125-2
108. Arellano A, Palma-Florez S, Cabrera P, et al. Attenuation of blood-brain barrier dysfunction by functionalized gold nanoparticles against amyloid-β peptide in an Alzheimer’s disease-on-a-chip model. Mater Today Bio. 2025;35:102453. doi:10.1016/j.mtbio.2025.102453
109. Cheng Y, Dai Q, Morshed RA, et al. Blood‐brain barrier permeable gold nanoparticles: an efficient delivery platform for enhanced malignant glioma therapy and imaging. Small. 2014;10(24):5137–5150. doi:10.1002/smll.201400654
110. Gallardo-Toledo E, Tapia-Arellano A, Celis F, et al. Intranasal administration of gold nanoparticles designed to target the central nervous system: fabrication and comparison between nanospheres and nanoprisms. Int J Pharm. 2020;590:119957. doi:10.1016/j.ijpharm.2020.119957
111. Kong SD, Lee J, Ramachandran S, et al. Magnetic targeting of nanoparticles across the intact blood–brain barrier. J Control Release. 2012;164(1):49–57. doi:10.1016/j.jconrel.2012.09.021
112. Qiao R, Fu C, Forgham H, et al. Magnetic iron oxide nanoparticles for brain imaging and drug delivery. Adv Drug Delivery Rev. 2023;197:114822. doi:10.1016/j.addr.2023.114822
113. Baghirov H, Karaman D, Viitala T, et al. Feasibility study of the permeability and uptake of mesoporous silica nanoparticles across the blood-brain barrier. PLoS One. 2016;11(8):e0160705. doi:10.1371/journal.pone.0160705
114. Jampilek J, Zaruba K, Oravec M, et al. Preparation of silica nanoparticles loaded with nootropics and their in vivo permeation through blood‐brain barrier. Biomed Res Int. 2015;2015(1):812673. doi:10.1155/2015/812673
115. Lin C-K, Yang Y-S, Liu T-P, et al. Tailored mesoporous silica nanoparticles and the chick chorioallantoic membrane: a promising strategy and model for efficient blood-brain barrier crossing. ACS Appl Mater Interfaces. 2025;17(20):29437–29454. doi:10.1021/acsami.5c05429
116. Wu J, Wang C, Sun J, Xue Y. Neurotoxicity of silica nanoparticles: brain localization and dopaminergic neurons damage pathways. ACS Nano. 2011;5(6):4476–4489. doi:10.1021/nn103530b
117. Alvarez-Erviti L, Seow Y, Yin H, Betts C, Lakhal S, Wood MJ. Delivery of siRNA to the mouse brain by systemic injection of targeted exosomes. Nature Biotechnol. 2011;29(4):341–345. doi:10.1038/nbt.1807
118. Chen CC, Liu L, Ma F, et al. Elucidation of exosome migration across the blood–brain barrier model in vitro. Cell Mol Bioeng. 2016;9(4):509–529. doi:10.1007/s12195-016-0458-3
119. Onohuean H, Naik Bukke SP, Thalluri C, Abass KS, Choonara YE. Exosome engineering for targeted therapy of brain-infecting pathogens: molecular tools, delivery platforms, and translational advances. Front Med Technol. 2025;7:1655471. doi:10.3389/fmedt.2025.1655471
120. Kim HI, Park J, Zhu Y, Wang X, Han Y, Zhang D. Recent advances in extracellular vesicles for therapeutic cargo delivery. Exp Mol Med. 2024;56(4):836–849. doi:10.1038/s12276-024-01201-6
121. Khatami SH, Karami N, Taheri-Anganeh M, et al. Exosomes: promising delivery tools for overcoming blood-brain barrier and glioblastoma therapy. Mol Neurobiol. 2023;60(8):4659–4678. doi:10.1007/s12035-023-03365-0
122. Palakurthi SS, Shah B, Kapre S, et al. A comprehensive review of challenges and advances in exosome-based drug delivery systems. Nanoscale Adv. 2024;6(23):5803–5826. doi:10.1039/D4NA00501E
123. Lee Y, Kim M, Ha J, Lee M. Brain‐targeted exosome‐mimetic cell membrane nanovesicles with therapeutic oligonucleotides elicit anti‐tumor effects in glioblastoma animal models. Bioeng Transl Med. 2023;8(2):e10426. doi:10.1002/btm2.10426
124. Zhong G, Yang X, Jiang X, et al. Dopamine-melanin nanoparticles scavenge reactive oxygen and nitrogen species and activate autophagy for osteoarthritis therapy. Nanoscale. 2019;11(24):11605–11616. doi:10.1039/C9NR03060C
125. Lou X, Hu Y, Zhang H, Liu J, Zhao Y. Polydopamine nanoparticles attenuate retina ganglion cell degeneration and restore visual function after optic nerve injury. J Nanobiotechnol. 2021;19(1):436. doi:10.1186/s12951-021-01199-3
126. Lin W, Miao H, Zhang J, et al. Regulation of the antioxidant structure of polydopamine nanomaterials: mechanisms, strategies, and applications in reactive oxygen species-mediated diseases. Next Mat. 2025;9:101253. doi:10.1016/j.nxmate.2025.101253
127. Ahmed-Farid OA, Taha M, Bakeer RM, et al. Effects of bee venom and dopamine-loaded nanoparticles on reserpine-induced Parkinson’s disease rat model. Sci Rep. 2021;11(1):21141. doi:10.1038/s41598-021-00764-y
128. Kawak P, Sawaftah NMA, Pitt WG, Husseini GA. Transferrin-targeted liposomes in glioblastoma therapy: a review. Int J Mol Sci. 2023;24(17):13262. doi:10.3390/ijms241713262
129. You Q, Liang F, Wu G, et al. The landscape of biomimetic nanovesicles in brain diseases. Adv Mater. 2024;36(7):2306583. doi:10.1002/adma.202306583
130. Cunha A, Gaubert A, Latxague L, Dehay B. PLGA-based nanoparticles for neuroprotective drug delivery in neurodegenerative diseases. Pharmaceutics. 2021;13(7):1042. doi:10.3390/pharmaceutics13071042
131. Alsaab HO, Alharbi FD, Alhibs AS, et al. PLGA-based nanomedicine: history of advancement and development in clinical applications of multiple diseases. Pharmaceutics. 2022;14(12):2728. doi:10.3390/pharmaceutics14122728
132. VandenBerg MA, Dong X, Smith WC, et al. Learning from the future: towards continuous manufacturing of nanomaterials. AAPS Open. 2025;11(1):7. doi:10.1186/s41120-025-00111-9
133. Waheed I, Ali A, Tabassum H, Khatoon N, Lai W-F, Zhou X. Lipid-based nanoparticles as drug delivery carriers for cancer therapy. Front Oncol. 2024;14:1296091. doi:10.3389/fonc.2024.1296091
134. Ezike TC, Okpala US, Onoja UL, et al. Advances in drug delivery systems, challenges and future directions. Heliyon. 2023;9(6):e17488. doi:10.1016/j.heliyon.2023.e17488
135. Naki T, Peter S, Alven S. Polymeric nanocarrier-based drug formulations for enhancing nose-to-brain delivery. Pharmaceutics. 2025;17(10):1242. doi:10.3390/pharmaceutics17101242
136. Jin Y, Zhang Y, Song M, Zhou J, Zhang H, Ding Y. Engineered exosomes as precision tools for brain-targeted drug delivery and treatment of central nervous system diseases. Cell Biomat. 2026;2026:1.
137. Berry D, Ene J, Nathani A, Singh M, Li Y, Zeng C. Effects of physical cues on stem cell-derived extracellular vesicles toward neuropathy applications. Biomedicines. 2024;12(3):489. doi:10.3390/biomedicines12030489
138. Fadaei MR, Fadaei MS, Kheirieh AE, et al. Overview of dendrimers as promising drug delivery systems with insight into anticancer and anti-microbial applications. Int J Pharm X. 2025;10:100390. doi:10.1016/j.ijpx.2025.100390
139. Janaszewska A, Lazniewska J, Trzepiński P, Marcinkowska M, Klajnert-Maculewicz B. Cytotoxicity of dendrimers. Biomolecules. 2019;9(8):330. doi:10.3390/biom9080330
140. Liu Y, Zhao M, Zhang M, Yang B, Qi Y-K, Fu Q. Mesoporous silica nanoparticle-based nanomedicine: preparation, functional modification, and theranostic applications. Mater Today Bio. 2025;34:102223. doi:10.1016/j.mtbio.2025.102223
141. Sanadgol N, Abedi M, Hashemzaei M, et al. Exosomes as nanocarriers for brain-targeted delivery of therapeutic nucleic acids: advances and challenges. J Nanobiotechnol. 2025;23(1):453. doi:10.1186/s12951-025-03528-2
142. Nie T, He Z, Zhu J, et al. Non-invasive delivery of levodopa-loaded nanoparticles to the brain via lymphatic vasculature to enhance treatment of Parkinson’s disease. Nano Res. 2021;14(8):2749–2761. doi:10.1007/s12274-020-3280-0
143. Vong LB, Sato Y, Chonpathompikunlert P, Tanasawet S, Hutamekalin P, Nagasaki Y. Self-assembled polydopamine nanoparticles improve treatment in Parkinson’s disease model mice and suppress dopamine-induced dyskinesia. Acta Biomater. 2020;109:220–228. doi:10.1016/j.actbio.2020.03.021
144. Liang K, Yang L, Kang J, et al. Improving treatment for Parkinson’s disease: harnessing photothermal and phagocytosis-driven delivery of levodopa nanocarriers across the blood-brain barrier. Asian J Pharm Sci. 2024;19(6):100963. doi:10.1016/j.ajps.2024.100963
145. Qu M, Lin Q, Huang L, et al. Dopamine-loaded blood exosomes targeted to brain for better treatment of Parkinson’s disease. J Control Release. 2018;287:156–166. doi:10.1016/j.jconrel.2018.08.035
146. Thomsen MS, Johnsen KB, Kucharz K, Lauritzen M, Moos T. Blood–brain barrier transport of transferrin receptor-targeted nanoparticles. Pharmaceutics. 2022;14(10):2237. doi:10.3390/pharmaceutics14102237
147. Tang S, Wang A, Yan X, et al. Brain-targeted intranasal delivery of dopamine with borneol and lactoferrin co-modified nanoparticles for treating Parkinson’s disease. Drug Delivery. 2019;26(1):700–707. doi:10.1080/10717544.2019.1636420
148. Argitekin E, Ersoz-Gulseven E, Cakan-Akdogan G, Akdogan Y. Dopamine-conjugated bovine serum albumin nanoparticles containing pH-responsive catechol-V (III) coordination for in vitro and in vivo drug delivery. Biomacromolecules. 2023;24(8):3603–3618. doi:10.1021/acs.biomac.3c00363
149. Padilla-Godínez FJ, López-Goerne T, Calvillo-Muñoz EY, et al. Dopamine stabilized in ultra-nanoreservoirs for controlled delivery in Parkinson’s disease. Nanomedicine. 2025;20(6):543–557. doi:10.1080/17435889.2025.2460228
150. Post MR, Sulzer D. The chemical tools for imaging dopamine release. Cell Chem Biol. 2021;28(6):748–764. doi:10.1016/j.chembiol.2021.04.005
151. Farde L, Halldin C, Stone-Elander S, Sedvall G. PET analysis of human dopamine receptor subtypes using 11C-SCH 23390 and 11C-raclopride. Psychopharmacology. 1987;92(3):278–284. doi:10.1007/BF00210831
152. Elsinga PH, Hatano K, Ishiwata K. PET tracers for imaging of the dopaminergic system. Curr Med Chem. 2006;13(18):2139–2153. doi:10.2174/092986706777935258
153. Thomas G, Boudon J, Maurizi L, et al. Innovative magnetic nanoparticles for PET/MRI bimodal imaging. ACS Omega. 2019;4(2):2637–2648. doi:10.1021/acsomega.8b03283
154. Liang Y, Shen G, He K, et al. Multimodal imaging by polydopamine nanoparticles for effective pre-and intra-operative lymph-node screening in gastric cancer using mice model. Int J Nanomed. 2026;2026:1–18.
155. Park B-N, Kim S-M, An Y-S. Combining dopamine transporter and amyloid PET tracer: a preclinical study on dual-target imaging. Mol Imaging Biol. 2025;27(4):578–586. doi:10.1007/s11307-025-02033-0
156. Ianni AM, Eisenberg DP, Boorman ED, et al. PET-measured human dopamine synthesis capacity and receptor availability predict trading rewards and time-costs during foraging. Nat Commun. 2023;14(1):6122. doi:10.1038/s41467-023-41897-0
157. Pan H, Balbirnie M, Hou K, et al. Liganded magnetic nanoparticles for magnetic resonance imaging of α-synuclein. NPJ Parkinson’s Dis. 2025;11(1):88. doi:10.1038/s41531-025-00918-z
158. Chalon S, Vercouillie J, Payoux P. The story of the dopamine transporter PET tracer LBT-999: from conception to clinical use. Front Med. 2019;6:90. doi:10.3389/fmed.2019.00090
159. Barret O, Zhang L, Alagille D, et al. Dopamine D1 receptor agonist PET tracer development: assessment in nonhuman primates. J Nucl Med. 2021;62(9):1307–1313. doi:10.2967/jnumed.120.256008
160. Xuan L, Ju Z, Skonieczna M, Zhou PK, Huang R. Nanoparticles‐induced potential toxicity on human health: applications, toxicity mechanisms, and evaluation models. MedComm. 2023;4(4):e327. doi:10.1002/mco2.327
161. Sharma S, Parveen R, Chatterji BP. Toxicology of nanoparticles in drug delivery. Curr Pathobiol Rep. 2021;9(4):133–144. doi:10.1007/s40139-021-00227-z
162. Payoe KS, Gadar K, Flahaut E, McCarthy RR, Stenbeck G. Nanoparticle-induced systemic toxicity and immune response in Galleria mellonella larvae. Front Pharmacol. 2025;16:1625472. doi:10.3389/fphar.2025.1625472
163. Maria MF, Thangam T, Prakashini RS, Hemamalani A, Parthasarathy K, Phoebe M. Evaluating nanoparticle-induced cytotoxicity: mechanisms and methods. Nano Biomed Eng. 2025;17(4):481–504. doi:10.26599/NBE.2025.9290129
164. Heidegger S, Gößl D, Schmidt A, et al. Immune response to functionalized mesoporous silica nanoparticles for targeted drug delivery. Nanoscale. 2016;8(2):938–948. doi:10.1039/C5NR06122A
165. Jakic K, Selc M, Razga F, et al. Long-term accumulation, biological effects and toxicity of BSA-coated gold nanoparticles in the mouse liver, spleen, and kidneys. Int J Nanomed. 2024;Volume 19:4103–4120. doi:10.2147/IJN.S443168
166. Zhang L, Ma Y, Wei Z, Wang L. Toxicity of gold nanoparticles complicated by the co-existence multiscale plastics. Front Microbiol. 2024;15:1447046. doi:10.3389/fmicb.2024.1447046
167. Teleanu DM, Chircov C, Grumezescu AM, Volceanov A, Teleanu RI. Impact of nanoparticles on brain health: an up to date overview. J Clin Med. 2018;7(12):490. doi:10.3390/jcm7120490
168. Atz K, Cotos L, Isert C, et al. Prospective de novo drug design with deep interactome learning. Nat Commun. 2024;15(1):3408. doi:10.1038/s41467-024-47613-w
169. Özçelik R, Brinkmann H, Criscuolo E, Grisoni F. Generative deep learning for de novo drug design─ a chemical space odyssey. J Chem Inf Model. 2025;65(14):7352–7372. doi:10.1021/acs.jcim.5c00641
170. Aghdam MF, Solout MV, Amini F, et al. Using machine learning in the in-silico design of selective dopamine receptor ligands: advancements in targeted therapies for neurological and psychiatric disorders. Res Chem. 2025;2025:102915.
171. Zell L, Bretl A, Temml V, Schuster D. Dopamine receptor ligand selectivity—an in silico/in vitro insight. Biomedicines. 2023;11(5):1468. doi:10.3390/biomedicines11051468
172. Nguyen AT, Nguyen DT, Koh HY, et al. The application of artificial intelligence to accelerate G protein‐coupled receptor drug discovery. Br J Pharmacol. 2024;181(14):2371–2384. doi:10.1111/bph.16140
173. Huang ET, Yang J-S, Liao KY, et al. Predicting blood–brain barrier permeability of molecules with a large language model and machine learning. Sci Rep. 2024;14(1):15844. doi:10.1038/s41598-024-66897-y
174. Nabi AE, Pouladvand P, Liu L, Hua Y, Ayubcha C. Machine learning in drug development for neurological diseases: a review of blood brain barrier permeability prediction models. Mol Inform. 2025;44(3):e202400325. doi:10.1002/minf.202400325
175. Zhu B, Liu S. Feature-guided machine learning for studying passive blood–brain barrier permeability to aid drug discovery. Int J Mol Sci. 2025;26(22):11228. doi:10.3390/ijms262211228
176. Shaker B, Lee J, Lee Y, et al. A machine learning-based quantitative model (LogBB_Pred) to predict the blood–brain barrier permeability (logBB value) of drug compounds. Bioinformatics. 2023;39(10):btad577. doi:10.1093/bioinformatics/btad577
177. Chien EY, Liu W, Zhao Q, et al. Structure of the human dopamine D3 receptor in complex with a D2/D3 selective antagonist. Science. 2010;330(6007):1091–1095. doi:10.1126/science.1197410
178. Yin J, Chen K-YM, Clark MJ, et al. Structure of a D2 dopamine receptor–G-protein complex in a lipid membrane. Nature. 2020;584(7819):125–129. doi:10.1038/s41586-020-2379-5
179. LeWitt PA, Rezai AR, Leehey MA, et al. AAV2-GAD gene therapy for advanced Parkinson’s disease: a double-blind, sham-surgery controlled, randomised trial. Lancet Neurol. 2011;10(4):309–319. doi:10.1016/S1474-4422(11)70039-4
180. Luo S, Lv Z, Yang Q, Chang R, Wu J. Research progress on stimulus-responsive polymer nanocarriers for cancer treatment. Pharmaceutics. 2023;15(7):1928. doi:10.3390/pharmaceutics15071928
181. Wang T, Wu C, Hu Y, Zhang Y, Ma J. Stimuli-responsive nanocarrier delivery systems for Pt-based antitumor complexes: a review. RSC Adv. 2023;13(24):16488–16511. doi:10.1039/D3RA00866E
182. Karimi M, Eslami M, Sahandi‐Zangabad P, et al. pH‐Sensitive stimulus‐responsive nanocarriers for targeted delivery of therapeutic agents. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2016;8(5):696–716. doi:10.1002/wnan.1389
183. Bhattacharya S, Prajapati BG, Singh S. A critical review on the dissemination of PH and stimuli-responsive polymeric nanoparticular systems to improve drug delivery in cancer therapy. Crit Rev Oncol/Hematol. 2023;185:103961. doi:10.1016/j.critrevonc.2023.103961
184. Parra‐Nieto J, de Carcer IA, García Del Cid MA, Jimenez‐Falcao S, Gónzalez‐Larre J, Baeza A. Stimuli‐Responsive nanocarriers as active enhancers of antitumoral immunotherapy. Adv Mater Interfaces. 2024;11(30):2400343. doi:10.1002/admi.202400343
185. Yadav N, Debnath N, Das S, Huang Y, Wu A, Zhao P. Stimuli-responsive nanocarriers for targeted mRNA therapeutics: a paradigm shift in mRNA delivery for biomedical applications. Drug Delivery Transl Res. 2026;16:1–27. doi:10.1007/s13346-025-01943-4
186. Cao Z, Li D, Wang J, Yang X. Reactive oxygen species-sensitive polymeric nanocarriers for synergistic cancer therapy. Acta Biomater. 2021;130:17–31. doi:10.1016/j.actbio.2021.05.023
187. Ballance WC, Qin EC, Chung HJ, Gillette MU, Kong H. Reactive oxygen species-responsive drug delivery systems for the treatment of neurodegenerative diseases. Biomaterials. 2019;217:119292. doi:10.1016/j.biomaterials.2019.119292
188. Boyuklieva R, Zahariev N, Simeonov P, Penkov D, Katsarov P. Next-generation drug delivery for neurotherapeutics: the promise of stimuli-triggered nanocarriers. Biomedicines. 2025;13(6):1464. doi:10.3390/biomedicines13061464
189. Nance E, Zhang C, Shih T-Y, Xu Q, Schuster BS, Hanes J. Brain-penetrating nanoparticles improve paclitaxel efficacy in malignant glioma following local administration. ACS Nano. 2014;8(10):10655–10664. doi:10.1021/nn504210g
190. Saraiva C, Praça C, Ferreira R, Santos T, Ferreira L, Bernardino L. Nanoparticle-mediated brain drug delivery: overcoming blood–brain barrier to treat neurodegenerative diseases. J Control Release. 2016;235:34–47. doi:10.1016/j.jconrel.2016.05.044
191. Verscheijden LF, Koenderink JB, de Wildt SN, Russel FG. Differences in P-glycoprotein activity in human and rodent blood–brain barrier assessed by mechanistic modelling. Arch Toxicol. 2021;95(9):3015–3029. doi:10.1007/s00204-021-03115-y
192. Wasielewska JM, Chaves JCDS, White AR, Oikari L. Modeling the Blood–Brain Barrier to Understand Drug Delivery in Alzheimer’s Disease. Exon Publications; 2020:117–134.
193. Agrahari V, Agrahari V. Facilitating the translation of nanomedicines to a clinical product: challenges and opportunities. Drug Discovery Today. 2018;23(5):974–991. doi:10.1016/j.drudis.2018.01.047
194. Paliwal R, Babu RJ, Palakurthi S. Nanomedicine scale-up technologies: feasibilities and challenges. AAPS Pharm Sci Tech. 2014;15(6):1527–1534. doi:10.1208/s12249-014-0177-9
195. Metselaar JM, Lammers T. Challenges in nanomedicine clinical translation. Drug Delivery Transl Res. 2020;10(3):721–725. doi:10.1007/s13346-020-00740-5
196. Hua S, De Matos MB, Metselaar JM, Storm G. Current trends and challenges in the clinical translation of nanoparticulate nanomedicines: pathways for translational development and commercialization. Front Pharmacol. 2018;9:790. doi:10.3389/fphar.2018.00790
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Recent Advancements in Lipid Nanoparticles-Based Phytoactives Delivery Systems for Neurodegenerative Diseases

Dirir AM, Ali A, Hachem M
International Journal of Nanomedicine 2025, 20:10279-10300
Published Date: 25 August 2025
How Effective are Nanotechnology-Based Therapeutics to Treat Autoimmune Diseases
Barakat M, Abu Ershaid JM, Alzaghari LF, Abdulrazzaq SB, Raad D, Hasen E, Al-Qudah RA, Chellappan DK, Athamneh T, Al-Najjar MAA, Ashames A
International Journal of Nanomedicine 2026, 21:562959
Published Date: 20 January 2026
Nanomaterial-Based Drug Delivery Systems for Ischemic Stroke: From Blood-Brain Barrier Crossing to Neuroprotection
He Y, Qu M, Yu L, Lu Y, Hong J, Sun M, Yang H, Mi W, Guo H, Ma Y
International Journal of Nanomedicine 2026, 21:588499
Published Date: 11 February 2026
Surface-Engineered Precision Nano-Systems for Targeted Treatment of Huntington’s Disease: A Review of Recent Advancements
Zhang J, Nie L, Ma J, Wang X
International Journal of Nanomedicine 2026, 21:548892
Published Date: 20 February 2026
Peptide-Based Nanocarriers for Targeted Drug Delivery: Recent Advances, Strategies, and Therapeutic Frontiers
Adnan SB, Lim F, Ahmad H, Maarof M, Fauzi MB, Md Fadilah NI
International Journal of Nanomedicine 2026, 21:588558
Published Date: 27 March 2026