Back to Journals » International Journal of Nanomedicine » Volume 21
Nanomaterial-Based Drug Delivery Systems for Ischemic Stroke: From Blood-Brain Barrier Crossing to Neuroprotection
Authors He Y, Qu M, Yu L, Lu Y, Hong J, Sun M, Yang H, Mi W ![]() , Guo H, Ma Y
, Guo H, Ma Y ![]()
Received 12 December 2025
Accepted for publication 3 February 2026
Published 11 February 2026 Volume 2026:21 588499
DOI https://doi.org/10.2147/IJN.S588499
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Eng San Thian
Yanan He,1,* Mengyao Qu,1,* Lu Yu,1,* Yiuxn Lu,1 Jin Hong,1 Miao Sun,1 Huikai Yang,1 Weidong Mi,1 Hang Guo,2 Yulong Ma1
1Department of Anesthesiology, the First Medical Center of Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China; 2Department of Anesthesiology, the Seventh Medical Center of Chinese PLA General Hospital, Beijing, 100700, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yulong Ma, Email [email protected] Weidong Mi, Email [email protected]
Abstract: Ischemic stroke remains a leading cause of mortality and long-term disability worldwide, largely due to limited therapeutic options and the restrictive nature of the blood–brain barrier (BBB). Nanomaterial-based drug delivery systems have emerged as promising strategies to enhance brain-targeted therapy by facilitating BBB penetration and enabling multi-pathway neuroprotection. This review provides a mechanism-driven overview of recent advances in stroke nanomedicine, classifying nanotherapeutic strategies into four major categories: reactive oxygen species–scavenging nanomaterials, glutamate-modulating systems, anti-inflammatory nanocarriers, and neuroprotective or neuroregenerative delivery platforms. Representative nanoplatforms within each category are discussed with respect to their BBB-crossing mechanisms, therapeutic potential, and translational relevance. In addition, the current clinical trial landscape, key translational bottlenecks, and emerging artificial intelligence–assisted approaches for optimizing nanocarrier design and supporting translational decision-making are highlighted. Overall, this review aims to provide a structured, clinically oriented framework to guide the rational design and translational development of nanomaterial-based drug delivery systems for ischemic stroke.
Keywords: ischemic stroke, nanomedicine, blood-brain barrier, neuroprotection, drug delivery
Introduction
Ischemic stroke remains a leading cause of mortality and long-term disability worldwide, imposing substantial health and socioeconomic burdens.1,2 Although advances in acute reperfusion therapies, including intravenous thrombolysis and mechanical thrombectomy, have markedly improved outcomes in selected patients, their overall clinical impact remains constrained by narrow therapeutic windows, limited patient eligibility, and the persistent risk of hemorrhagic complications.3,4 Consequently, there is a critical unmet need for adjunctive and neuroprotective strategies capable of extending therapeutic opportunities beyond reperfusion and promoting sustained neurological recovery.
A major obstacle to effective stroke therapy is the blood–brain barrier (BBB), which restricts the brain delivery of most pharmacological agents.5,6 While ischemic injury and subsequent reperfusion can induce BBB disruption, this process is neither uniform nor sustained.7 BBB permeability evolves dynamically over time and space, differing across the ischemic core, peri-infarct penumbra, and non-affected regions, and is further influenced by reperfusion status and clinical interventions.8 Transient increases in BBB permeability may occur during acute and early subacute phases, particularly following thrombolysis or thrombectomy, creating narrow but clinically relevant windows for therapeutic delivery. These features underscore the importance of aligning drug delivery strategies with realistic clinical workflows rather than assuming persistent or homogeneous BBB opening.9
In addition to temporal and spatial BBB heterogeneity, clinical variability among stroke patients represents a critical translational consideration.10,11 Accumulating evidence indicates that biological sex and aging influence BBB integrity, inflammatory responses, and post-stroke recovery trajectories.12 Furthermore, common comorbidities such as hypertension, diabetes, and hyperlipidemia are known to exacerbate BBB dysfunction and neuroinflammation, potentially altering nanocarrier biodistribution, therapeutic efficacy, and safety profiles.13 Consideration of these patient-specific factors is therefore essential for the rational design and clinical translation of brain-targeted therapies for ischemic stroke.14
Within this context, nanomaterial-based drug delivery systems have emerged as promising platforms to enhance brain-targeted therapy.15,16 Owing to their tunable physicochemical properties, nanocarriers can be engineered to improve systemic stability, facilitate BBB transport, and enable spatiotemporally controlled drug release.17 Beyond functioning as passive carriers, many nanoplatforms are designed to engage specific pathological pathways, offering opportunities to coordinately modulate oxidative stress, excitotoxic signaling, neuroinflammatory responses, and post-stroke repair processes.18
Despite substantial preclinical progress, the clinical translation of stroke nanomedicine remains limited. Key barriers include incomplete characterization of long-term biodistribution and clearance, immunogenicity and complement activation, protein corona variability, and off-target toxicity.19,20 In parallel, challenges related to scalable manufacturing, batch-to-batch reproducibility, and chemistry, manufacturing, and controls (CMC) compliance continue to impede regulatory advancement. These translational constraints help explain why many sophisticated nanoplatforms have not progressed beyond preclinical evaluation despite encouraging experimental efficacy.
To address these challenges and provide a clinically grounded perspective, this review adopts a mechanism-based framework to organize nanomaterial-based strategies according to their primary therapeutic actions rather than carrier type alone. In addition, the review integrates current insights from the emerging clinical trial landscape and highlights the growing role of artificial intelligence and machine learning approaches in optimizing nanocarrier design, patient stratification, and translational decision-making. By explicitly bridging mechanistic understanding with clinical feasibility, this review aims to offer a structured and translationally relevant overview of nanomaterial-based drug delivery systems for ischemic stroke.
Pathophysiology of Ischemic Stroke and Barriers to Drug Delivery
Ischemic stroke, accounting for approximately 80–90% of all stroke cases globally, represents a leading cause of mortality and long-term disability worldwide. The pathophysiology of ischemic stroke encompasses a complex series of molecular and cellular events initiated by the sudden interruption of cerebral blood flow. During the acute phase, oxygen and glucose deprivation triggers a devastating cascade of pathological processes, including excitotoxicity, oxidative stress, mitochondrial dysfunction, and neuroinflammation. These interconnected mechanisms collectively contribute to rapid neuronal death within the ischemic core and progressive injury in the surrounding penumbra. Furthermore, the blood-brain barrier (BBB), a highly specialized neurovascular interface that normally protects the central nervous system, presents formidable obstacles to therapeutic drug delivery while simultaneously undergoing structural and functional disruption during stroke. The narrow therapeutic window for current interventions, primarily limited to 4.5 hours for intravenous thrombolysis, severely restricts treatment eligibility and underscores the urgent need for innovative therapeutic approaches that can overcome these biological barriers and extend the treatment timeframe.
Pathological Cascades in Ischemic Stroke: Oxidative Stress, Excitotoxicity, and Neuroinflammation
The pathological cascade following cerebral ischemia is characterized by three major interconnected mechanisms: oxidative stress, excitotoxicity, and neuroinflammation. Upon blood flow reduction, the depletion of adenosine triphosphate (ATP) leads to energy failure and ionic imbalance, triggering membrane depolarization and excessive release of excitatory neurotransmitters, particularly glutamate. Beyond acute energy failure, accumulating evidence indicates that ischemic stroke induces profound metabolic reprogramming, characterized by excessive glycolytic activation and dysregulated lipid metabolism, which together exacerbate mitochondrial dysfunction, oxidative stress, and inflammatory signaling cascades.21 The subsequent overactivation of N-methyl-D-aspartate receptors (NMDARs) results in massive calcium influx, initiating excitotoxicity and downstream cell death pathways.22 Concurrently, mitochondrial dysfunction during ischemia generates excessive reactive oxygen and nitrogen species (RONS), including superoxide anion, hydrogen peroxide, and peroxynitrite, which overwhelm endogenous antioxidant defense systems comprising superoxide dismutase, catalase, and glutathione peroxidase.23 These free radicals directly damage cellular macromolecules, including lipids, proteins, and DNA, while also activating redox-sensitive transcription factors such as nuclear factor kappa-B (NF-κB), thereby amplifying inflammatory responses.24
Oxidative stress plays a particularly devastating role during both the ischemic and reperfusion phases of stroke. Recent studies have demonstrated that malondialdehyde (MDA), a biomarker of lipid peroxidation, is significantly elevated in acute ischemic stroke patients and correlates with increased mortality rates and poor functional outcomes.25 Furthermore, the expression of antioxidant enzymes such as peroxiredoxin 1 (PRDX1) and peroxiredoxin 6 (PRDX6) is upregulated following stroke as a compensatory cellular response to oxidative injury, with PRDX6 demonstrating neuroprotective effects through multiple mechanisms including phospholipid hydroperoxide reduction and membrane repair.26 The interplay between oxidative stress and ferroptosis, an iron-dependent form of regulated cell death characterized by lipid peroxidation, has emerged as a critical pathway in ischemic brain injury, with glutathione peroxidase 4 (GPX4) serving as a key regulator.27
Neuroinflammation represents the third pillar of post-ischemic pathology, manifesting as both beneficial and detrimental processes depending on timing and magnitude. Within hours of stroke onset, resident microglia undergo rapid activation and morphological transformation, releasing pro-inflammatory cytokines including interleukin-1β (IL-1β), interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α), which further recruit peripheral immune cells such as neutrophils and monocytes into the injured brain parenchyma.28 IL-6, in particular, has emerged as a critical prognostic biomarker, with elevated serum levels associated with increased stroke severity, larger infarct volumes, and worse functional outcomes at 90 days.29 The inflammatory response also triggers matrix metalloproteinase (MMP) activation, particularly MMP-2 and MMP-9, which degrade the extracellular matrix and tight junction proteins, exacerbating BBB breakdown and facilitating hemorrhagic transformation.30 This inflammatory cascade creates a self-amplifying cycle wherein oxidative stress promotes neuroinflammation, which in turn generates additional RONS, perpetuating tissue injury and expanding the infarct zone beyond the initial ischemic core. These interconnected pathological cascades—oxidative stress, excitotoxicity, neuroinflammation, and BBB breakdown—collectively contribute to progressive neuronal injury following ischemic stroke (Figure 1).
 |
Figure 1 Pathophysiological cascades following ischemic stroke. Cerebral ischemia triggers four interconnected pathological mechanisms: oxidative stress with mitochondrial ROS production, excitotoxicity from excessive glutamate release, neuroinflammation involving microglial activation and neuronal degeneration, and BBB breakdown permitting peripheral immune cell infiltration. |
Blood-Brain Barrier: Structural Features and Challenges for Drug Delivery
The blood-brain barrier represents the most formidable obstacle to successful pharmacotherapy for ischemic stroke, restricting the passage of approximately 98% of small-molecule drugs and nearly 100% of large biomolecules, including therapeutic proteins, antibodies, and nucleic acids.31 This highly selective barrier is formed by specialized brain microvascular endothelial cells interconnected by complex tight junction proteins, including claudins, occludins, and zonula occludens, which severely limit paracellular diffusion. These endothelial cells exhibit remarkably low pinocytic activity and express high levels of efflux transporters, particularly P-glycoprotein and breast cancer resistance protein, which actively pump out xenobiotics and many therapeutic agents.32 Additionally, the BBB endothelium is surrounded by pericytes embedded within the basement membrane and astrocytic endfeet, forming a sophisticated neurovascular unit that maintains brain homeostasis through precise regulation of ion transport, metabolite exchange, and immune surveillance.33
During ischemic stroke, the BBB undergoes dynamic and heterogeneous disruption that paradoxically presents both opportunities and challenges for drug delivery. Contrary to earlier assumptions that BBB disruption uniformly enhances drug penetration, recent evidence demonstrates that the relationship between barrier breakdown and therapeutic access is complex and time-dependent. Dynamic contrast-enhanced magnetic resonance imaging studies in acute ischemic stroke patients reveal that BBB permeability increases continuously from symptom onset, with peak disruption occurring between 6–48 hours post-stroke, though this leakage persists for up to 90 hours in some cases.34 However, this BBB compromise is primarily localized to the infarct core and immediate penumbra, with the salvageable tissue often retaining significant barrier function.35 Critically, extensive BBB disruption correlates with poor clinical outcomes rather than improved drug delivery, as it facilitates the infiltration of peripheral leukocytes, neutrophils, and pro-inflammatory mediators that exacerbate neuroinflammation and increase the risk of hemorrhagic transformation.36
The molecular mechanisms underlying BBB disruption during stroke involve multiple interconnected pathways. MMP-9, upregulated within hours of ischemia onset through inflammatory cytokine signaling (particularly TNF-α and IL-1β), degrades basement membrane components and tight junction proteins, leading to increased vascular permeability and edema formation.37 Simultaneously, oxidative stress generated by NADPH oxidase activation and mitochondrial dysfunction directly damages endothelial cells and compromises tight junction integrity.38 The pleiotropic cytokine macrophage migration inhibitory factor (MIF) further contributes to BBB dysfunction by inducing endothelial autophagy, promoting inflammatory cytokine production, and disrupting tight junction protein expression. These pathological changes create a therapeutic dilemma: while some degree of BBB opening might theoretically facilitate drug delivery to the ischemic brain, excessive disruption leads to edema, hemorrhage, and worse clinical outcomes, necessitating drug delivery strategies that can either cross the intact barrier or selectively target regions of controlled permeability while preserving overall barrier function.
Therapeutic Window and Limitations of Conventional Treatments
The therapeutic window for acute ischemic stroke is governed by the principle that “time is brain”, with approximately 1.9 million neurons lost every minute during untreated cerebral ischemia. Currently, intravenous tissue plasminogen activator (tPA) remains the only FDA-approved pharmacological treatment, demonstrating established efficacy within 3 hours of symptom onset and extended approval in selected patients up to 4.5 hours.39 Importantly, recent meta-analyses of randomized clinical trials demonstrate that, under advanced imaging-based selection, intravenous thrombolysis can confer functional benefit beyond the conventional 4.5-hour window, challenging rigid time-based treatment paradigms.40 However, the narrow therapeutic window reflects the delicate balance between thrombolytic benefits and hemorrhagic complications, with treatment efficacy diminishing progressively over time and symptomatic intracranial hemorrhage occurring in approximately 6% of treated patients.41 Mechanical thrombectomy has emerged as a complementary intervention with a somewhat extended window, demonstrating efficacy up to 6 hours for large vessel occlusions and even up to 24 hours in highly selected patients identified through advanced perfusion imaging that reveals favorable penumbral patterns. Nevertheless, these interventions are limited to only 3–5% of all stroke patients due to stringent time constraints, imaging requirements, and eligibility criteria.42
The fundamental limitations of current treatments extend beyond temporal constraints to several critical issues that underscore the need for innovative therapeutic approaches. First, despite successful recanalization, many patients experience reperfusion injury characterized by secondary reactive oxygen species generation, inflammatory cell infiltration, and BBB disruption when blood flow is restored. Second, both tPA and thrombectomy address only the proximal cause of stroke without directly targeting downstream pathological cascades of excitotoxicity, oxidative stress, and neuroinflammation that continue expanding the infarct into the penumbra. Third, numerous neuroprotective agents showing promise in preclinical studies have failed in clinical trials, largely due to inadequate brain penetration, inappropriate dosing, delayed administration, and heterogeneous patient populations.43 Finally, the absence of reliable biomarkers to identify patients most likely to benefit from specific interventions further hampers personalized treatment approaches.44 These limitations highlight the critical need for advanced drug delivery systems capable of extending therapeutic windows, enhancing neuroprotective agent penetration across the BBB, targeting multiple pathological pathways simultaneously, and providing sustained therapeutic effects in the evolving post-ischemic environment.
Strategies for Blood-Brain Barrier Penetration and Brain Targeting
The development of effective strategies to overcome the blood-brain barrier (BBB) represents a critical challenge in central nervous system drug delivery, as this highly selective barrier restricts approximately 98% of small-molecule drugs and nearly all large-molecule therapeutics from entering the brain parenchyma. Current approaches to enhance BBB penetration can be broadly categorized into passive targeting strategies that exploit physicochemical properties and nanocarrier characteristics, active targeting mechanisms that utilize receptor-mediated transcytosis pathways, and stimuli-responsive systems that enable spatiotemporal control of drug release. Recent advances in nanotechnology and molecular engineering have significantly expanded the therapeutic arsenal for brain-targeted drug delivery, offering promising solutions to enhance therapeutic efficacy while minimizing systemic toxicity in the treatment of neurodegenerative diseases, brain tumors, and neuropsychiatric disorders.45,46
Passive Targeting: Size Optimization and Surface Modification (PEGylation, Charge Modulation)
Passive targeting strategies primarily rely on the optimization of nanoparticle physicochemical properties to enhance BBB permeability and brain accumulation through mechanisms such as enhanced permeation and retention (EPR) effect and adsorptive-mediated transcytosis. Size optimization plays a crucial role in BBB penetration, with nanoparticles in the range of 10–100 nm demonstrating optimal brain uptake due to their ability to navigate through endothelial fenestrations while avoiding rapid clearance by the reticuloendothelial system. Recent studies have shown that ultrasmall nanoparticles (<10 nm) can achieve improved BBB crossing through transcellular pathways, while larger particles (>200 nm) tend to accumulate in peripheral organs and exhibit limited brain bioavailability.47 Furthermore, the polydispersity index significantly influences biodistribution patterns, with monodisperse formulations showing more predictable pharmacokinetic profiles and enhanced brain targeting efficiency compared to heterogeneous size distributions.48
Surface modification through PEGylation has emerged as a gold standard strategy to prolong circulation time and reduce protein adsorption, thereby enhancing the probability of BBB interaction and transcytosis. The incorporation of polyethylene glycol (PEG) chains creates a hydrophilic corona that minimizes opsonization and immune recognition, effectively evading the mononuclear phagocyte system and extending blood circulation half-life from minutes to hours or even days. Recent investigations have revealed that PEG molecular weight, grafting density, and chain architecture critically influence stealth properties and BBB permeability, with PEG chains of 2–5 kDa demonstrating optimal balance between circulation longevity and tissue penetration.49 However, emerging concerns regarding accelerated blood clearance (ABC) phenomenon upon repeated administration and the development of anti-PEG antibodies have prompted researchers to explore alternative hydrophilic polymers such as poly(2-oxazoline), zwitterionic polymers, and polysarcosine as next-generation stealth coatings.50
Charge modulation represents another critical parameter in passive BBB targeting, as surface charge significantly influences nanoparticle interactions with the negatively charged glycocalyx and tight junction proteins of brain endothelial cells. While cationic nanoparticles can promote adsorptive-mediated transcytosis through electrostatic interactions with the negatively charged BBB, excessive positive charge often leads to rapid plasma protein adsorption, complement activation, and hemolytic toxicity. Conversely, neutral or slightly negative surfaces demonstrate improved biocompatibility and reduced toxicity but may exhibit lower cellular uptake efficiency. Recent advances have focused on developing charge-reversible nanoparticles that maintain neutral or negative charge in systemic circulation to minimize non-specific interactions, then undergo charge conversion to positive under specific microenvironmental conditions (such as acidic pH in tumor or inflammatory tissues) to facilitate enhanced cellular internalization and BBB penetration.51 Additionally, zwitterionic surface modifications combining both positive and negative charges have shown promise in achieving ultra-low fouling properties while maintaining sufficient BBB interaction capabilities.52
Active Targeting: Ligand-Mediated Transport (Transferrin, Lactoferrin, Peptide Conjugation)
Active targeting strategies exploit the overexpression of specific receptors on brain endothelial cells to facilitate receptor-mediated transcytosis, offering significantly enhanced BBB penetration efficiency and brain specificity compared to passive approaches. Among the most extensively investigated receptor-targeting ligands, transferrin (Tf) has demonstrated remarkable potential due to the high expression of transferrin receptors (TfR) on the BBB, which physiologically mediate iron transport into the brain. Conjugation of therapeutic nanocarriers with transferrin or anti-TfR antibodies can trigger clathrin-mediated endocytosis followed by transcytosis across the BBB, achieving brain drug concentrations several-fold higher than non-targeted formulations. Recent clinical investigations have validated the translational potential of transferrin-targeted nanoparticles, with liposomal doxorubicin conjugated to anti-TfR antibody demonstrating improved survival in glioblastoma patients in Phase II trials.53 However, challenges remain regarding competition with endogenous transferrin, potential receptor saturation at high doses, and the need for optimizing ligand density to balance binding affinity with transcytosis efficiency.54
Lactoferrin represents an alternative iron-binding glycoprotein that interacts with lactoferrin receptors highly expressed on brain endothelial cells, offering advantages including lower endogenous competition compared to transferrin and additional anti-inflammatory and neuroprotective properties. Lactoferrin-modified nanoparticles have shown superior BBB penetration in various preclinical models, with studies demonstrating up to 5-fold enhancement in brain accumulation compared to unmodified carriers and significant improvements in therapeutic outcomes for Alzheimer’s disease and Parkinson’s disease models.55 The multifunctional nature of lactoferrin extends beyond mere targeting, as it can modulate BBB permeability through interactions with tight junction proteins and provide intrinsic therapeutic benefits through its anti-oxidant and anti-apoptotic activities.56 Recent developments have focused on engineering lactoferrin-functionalized stimuli-responsive nanocarriers that combine active targeting with controlled drug release, achieving synergistic enhancements in both brain delivery efficiency and therapeutic efficacy.
Peptide-based targeting ligands have emerged as highly versatile alternatives to protein-based targeting moieties, offering advantages including smaller size, lower immunogenicity, ease of synthesis and modification, and the ability to be rationally designed for specific receptor interactions. Cell-penetrating peptides (CPPs) such as TAT, penetrating, and angiopep-2 have demonstrated remarkable BBB-crossing capabilities through both receptor-mediated and adsorptive-mediated mechanisms, with angiopep-2 showing particular promise through its specific interaction with low-density lipoprotein receptor-related protein 1 (LRP1) highly expressed on brain endothelial cells.57 Beyond classical CPPs, recent peptide engineering efforts have identified novel BBB-targeting sequences through phage display, in vivo screening, and computational design approaches, yielding peptides with enhanced specificity, reduced toxicity, and improved transcytosis efficiency. Furthermore, dual-targeting strategies combining BBB-penetrating peptides with disease-specific targeting moieties (such as tumor-homing peptides or amyloid-binding sequences) have demonstrated synergistic improvements in both brain delivery and disease site accumulation, opening new avenues for precision nanomedicine in neurodegenerative and neuro-oncological applications.58
Stimuli-Responsive Systems: Ultrasound, Magnetic, and pH-Sensitive Nanomaterials
Stimuli-responsive nanocarriers represent an innovative paradigm in brain drug delivery by enabling spatiotemporal control of BBB penetration and drug release in response to external or internal stimuli, thereby maximizing therapeutic efficacy while minimizing off-target effects. Focused ultrasound (FUS) combined with microbubbles has emerged as a leading non-invasive approach to transiently disrupt the BBB through mechanical effects including acoustic cavitation, microstreaming, and radiation force, creating reversible opening of tight junctions that allows enhanced penetration of circulating therapeutics. Recent clinical trials have demonstrated the safety and feasibility of MRI-guided focused ultrasound for BBB opening in patients with Alzheimer’s disease, brain tumors, and Parkinson’s disease, with temporal BBB disruption lasting 4–6 hours followed by complete restoration without apparent neurotoxicity.59 The integration of ultrasound-responsive nanoparticles loaded with both therapeutic agents and contrast agents enables real-time monitoring of BBB opening and drug delivery, while also providing opportunities for triggered drug release through ultrasound-induced cavitation and hyperthermia effects.
Magnetic nanoparticles, particularly superparamagnetic iron oxide nanoparticles (SPIONs) and magnetite nanoparticles, offer dual functionality as both therapeutic carriers and contrast agents for magnetic resonance imaging, while enabling magnetic field-guided targeting to specific brain regions. Under external magnetic field application, magnetic nanoparticles can be actively directed toward target sites, overcoming the limitations of passive diffusion and achieving significantly enhanced local drug concentrations at desired brain regions.60 Furthermore, alternating magnetic fields can induce localized hyperthermia through magnetic nanoparticle oscillation, enabling both magnetic hyperthermia therapy for tumor ablation and thermally-triggered drug release from temperature-sensitive carriers. Recent advances in magnetic targeting have incorporated magnetoelectric nanoparticles that can respond to magnetic fields by generating local electric fields, potentially modulating neuronal activity and opening tight junctions through electromagnetic effects without requiring microbubbles or ultrasound.61 The combination of magnetic guidance with surface functionalization using targeting ligands has demonstrated synergistic improvements in brain-specific delivery, with preclinical studies showing up to 10-fold enhancement in tumor accumulation and significant improvements in survival in glioblastoma models.62
pH-sensitive nanomaterials exploit the pH gradients present in pathological brain conditions, including the acidic tumor microenvironment (pH 6.5–6.8) and endosomal compartments (pH 5.0–6.0), to trigger drug release or undergo structural transformations that enhance therapeutic activity. pH-responsive polymers such as poly(β-amino esters), poly(histidine), and chitosan exhibit protonation-dependent solubility changes that can trigger nanoparticle disassembly, membrane destabilization, or drug release under acidic conditions.63 Advanced pH-sensitive systems have been designed with dual-stage responsiveness: neutral or negative charge in blood circulation to minimize non-specific interactions, followed by charge reversal to positive upon encountering acidic environments to enhance cellular uptake and endosomal escape. Recent innovations include pH-sensitive peptide-polymer conjugates that can undergo conformational changes from random coil to α-helix structures under acidic conditions, facilitating membrane insertion and cytosolic drug delivery.64 Moreover, pH-responsive systems can be combined with other targeting strategies, such as incorporating both pH-sensitive linkages and BBB-targeting ligands, to achieve multi-stage targeting that sequentially navigates systemic circulation, crosses the BBB, accumulates at disease sites, and releases drugs in response to local pH changes.65 These diverse BBB penetration strategies, including passive targeting, active targeting, and stimuli-responsive systems, are summarized in Table 1.
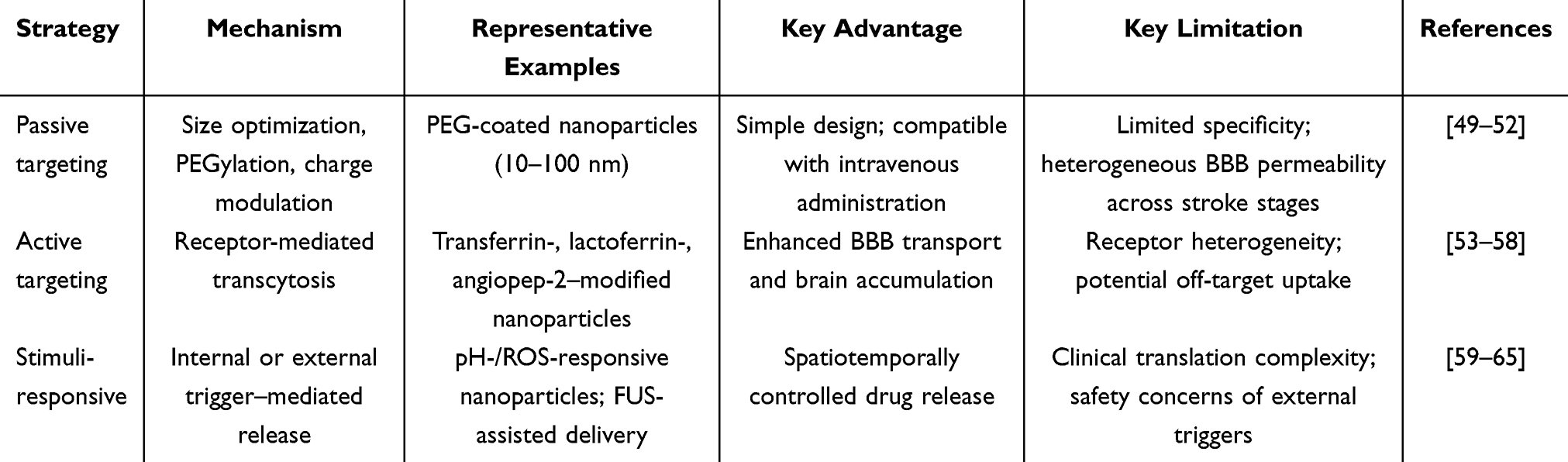 |
Table 1 Strategies for Blood-Brain Barrier Penetration in Ischemic Stroke Nanotherapy |
Mechanism-Based Classification of Nanomaterials for Ischemic Stroke Therapy
The pathophysiological complexity of ischemic stroke, characterized by overlapping cascades of oxidative stress, excitotoxicity, neuroinflammation, and neurodegeneration, necessitates therapeutic interventions that can simultaneously address multiple injury mechanisms. Nanomaterial-based delivery systems have emerged as promising platforms capable of targeting these distinct yet interconnected pathological processes through diverse mechanisms of action. Based on their primary therapeutic mechanisms, nanomaterials for ischemic stroke can be classified into four major categories: ROS-scavenging systems that directly neutralize oxidative damage, glutamate-modulating platforms that intervene in excitotoxic cascades, anti-inflammatory formulations that suppress neuroinflammatory responses, neuroprotective and neuroregenerative carriers that deliver neurotrophic factors. This mechanism-based classification provides a systematic framework for understanding how nanomaterials can be rationally designed to target specific pathophysiological processes while offering the versatility to combine complementary therapeutic modalities for enhanced neuroprotection. In this section, we comprehensively examine each category of nanomaterials, highlighting their mechanisms of action, representative examples, and therapeutic efficacy in preclinical stroke models, with particular emphasis on recent advances that have been reported in the past five years. Based on their primary therapeutic mechanisms, nanomaterials for ischemic stroke can be classified into four major categories: ROS-scavenging, glutamate-modulating, anti-inflammatory, and neuroprotective systems (Figure 2 and Table 2).
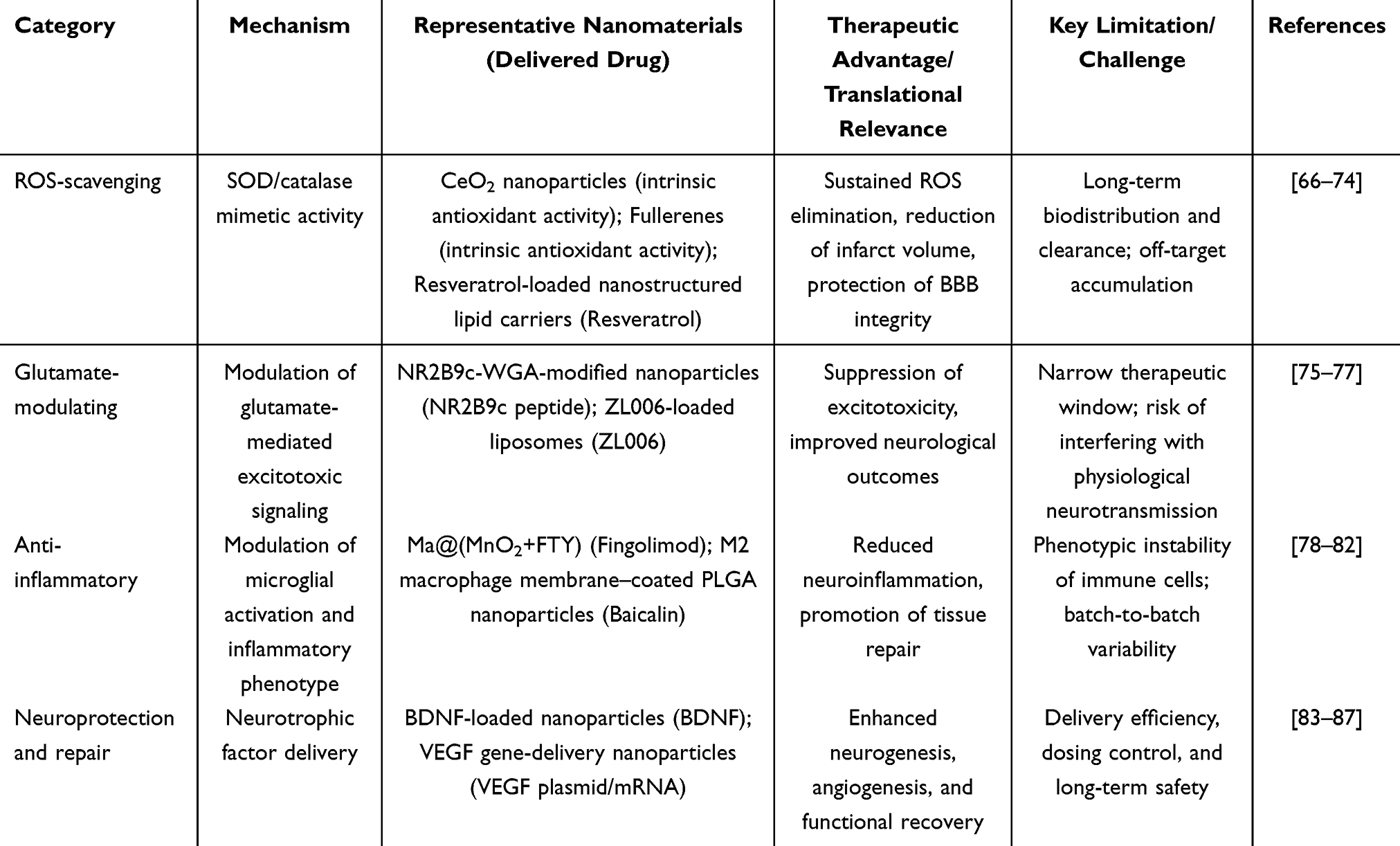 |
Table 2 Mechanism-Based Classification of Nanomaterials for Ischemic Stroke Therapy |
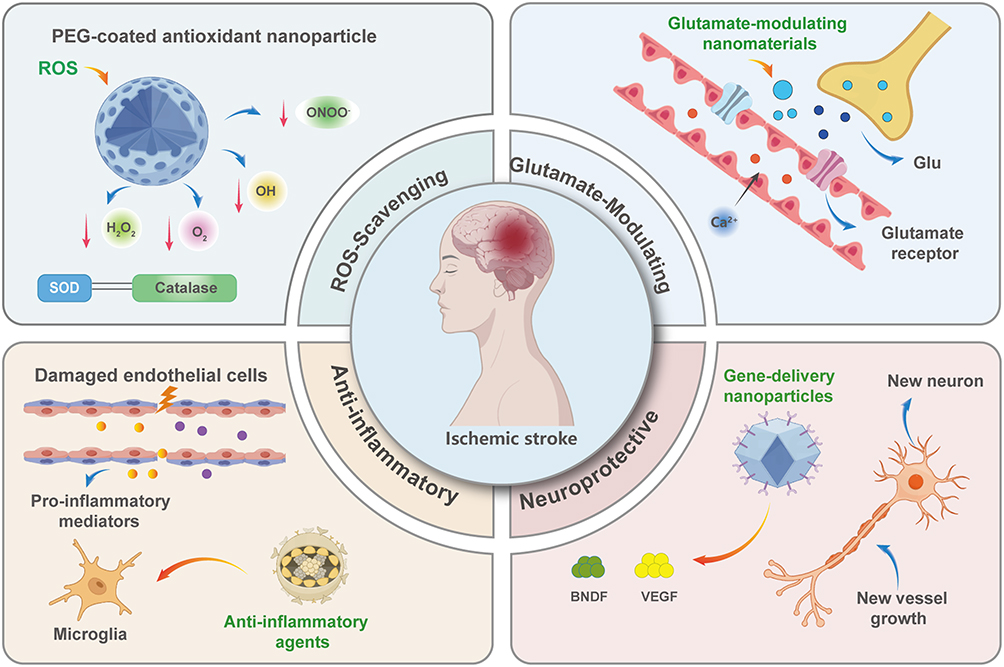 |
Figure 2 Mechanism-based classification of nanomaterials for ischemic stroke therapy. The schematic illustrates four representative therapeutic strategies: (i) ROS-scavenging nanomaterials exhibiting antioxidant activity through enzyme-mimetic mechanisms; (ii) nanomaterials designed to modulate glutamate-mediated excitotoxicity; (iii) anti-inflammatory nanoplatforms reported to regulate post-stroke neuroinflammatory responses, including effects on microglial activation; and (iv) neuroprotective nanocarriers delivering neurotrophic factors such as BDNF and VEGF to support neuronal survival, neurogenesis, and angiogenesis. Upward arrows indicate increased levels or activation, while downward arrows indicate decreased levels or inhibition of the corresponding pathological processes. |
ROS-Scavenging Nanomaterials: Cerium Oxide, Fullerene, and Antioxidant-Loaded Systems
Representative ROS-scavenging nanomaterials are discussed based on the robustness of their antioxidant mechanisms, in vivo neuroprotective efficacy, and potential relevance to clinically realistic delivery windows. Carbon-based nanomaterials, particularly fullerenes and their derivatives, constitute another important class of ROS-scavenging agents with distinctive advantages. Fullerenes (C60), characterized by their spherical structure with abundant conjugated double bonds and low-lying lowest unoccupied molecular orbital (LUMO), exhibit high reactivity toward radical species and can function as “free radical sponges” without being consumed in the reaction.66 Polyhydroxylated fullerenes (fullerenols) have demonstrated remarkable neuroprotective effects in middle cerebral artery occlusion (MCAO) models, with pre-treatment and post-treatment administration reducing infarct volume by 53% and 81%, respectively, while simultaneously decreasing malondialdehyde (MDA) and nitrate contents and enhancing superoxide dismutase activity and glutathione levels in ischemic hemispheres.67 The antioxidant activity of fullerenes is critically dependent on their surface functionalization; carboxyfullerenes, for instance, have shown a 75% reduction in brain infarction when administered at the time of ischemia in permanent MCAO models, with therapeutic effects remaining significant even when administered 6 hours post-occlusion.68 Recent investigations have revealed that fullerenol nanoparticles can protect blood-brain barrier integrity and attenuate brain edema after cerebral ischemia-reperfusion injury, potentially through reduction of interleukin-6 (IL-6) and matrix metalloproteinase-9 (MMP-9) transcription, thereby addressing both oxidative stress and neuroinflammation.69
Beyond nanomaterials with inherent antioxidant properties, polymeric and lipid-based nanocarriers have been extensively explored for delivering conventional antioxidant agents with improved pharmacokinetics and brain targeting capabilities. Nanostructured lipid carriers encapsulating resveratrol have demonstrated significantly enhanced therapeutic efficacy compared to free resveratrol, with encapsulated formulations showing 40–160 times greater effectiveness in reducing oxidative stress through increased glutathione levels and preservation of antioxidant enzyme activity in MCAO models.70 Similarly, edaravone, the only neuroprotective drug approved for clinical use in acute ischemic stroke in Japan, has been formulated into various nanoparticle systems to overcome its limited BBB penetration and short half-life.71 Recent advances include the development of ROS-responsive nanocarriers that selectively release antioxidant payloads in the oxidative microenvironment of ischemic tissue, enabling spatiotemporally controlled therapy. These intelligent nanoplatforms represent a significant advancement over conventional antioxidant delivery by minimizing systemic exposure while maximizing therapeutic concentrations at sites of oxidative injury.
Among metal and metal oxide nanoparticles investigated for ischemic stroke therapy, cerium oxide nanoparticles (CeO2 NPs) have been most extensively studied due to their unique redox cycling between Ce3⁺ and Ce4⁺ states, which enables sustained and self-regenerative scavenging of multiple reactive oxygen species.72,73 In contrast, other metal or metal oxide nanoparticles, such as iron oxide, manganese dioxide, and zinc oxide nanoparticles, have primarily been explored as imaging agents, enzyme-mimetic systems, or drug carriers, with comparatively fewer studies demonstrating intrinsic neuroprotective efficacy in ischemic stroke models. Therefore, CeO2 NPs were emphasized in this review as a representative and well-characterized example of metal oxide–based nanotherapeutics for ischemic stroke. Cerium oxide nanoparticles exhibit superoxide dismutase- and catalase-mimetic activity via reversible Ce3⁺/Ce4⁺ redox cycling, thereby enabling efficient scavenging of multiple reactive oxygen species.74
In addition to cerium oxide nanoparticles and fullerenes, several other nanomaterial-based free radical scavenger delivery systems have demonstrated therapeutic potential in ischemic stroke models. For example, Prussian blue nanoparticles and manganese dioxide–based nanoplatforms have been reported to effectively eliminate excessive reactive oxygen species while simultaneously alleviating oxidative stress–induced neuronal damage.88,89 Moreover, polymeric and lipid-based nanoparticles encapsulating antioxidant agents such as edaravone, resveratrol, and N-acetylcysteine derivatives have shown enhanced brain accumulation, prolonged circulation, and improved neuroprotective efficacy compared with free drugs. These studies further support the versatility of nanomaterial-based systems for targeted free radical scavenging in ischemic stroke therapy.90,91
Glutamate-Modulating Nanomaterials: Functional Nanoparticles for Excitotoxicity Intervention
Representative glutamate-modulating nanoplatforms are highlighted based on their mechanistic specificity in attenuating excitotoxicity, demonstrated efficacy in preclinical stroke models, and feasibility for targeted delivery to the ischemic brain. Glutamate excitotoxicity, triggered by excessive activation of N-methyl-D-aspartate receptors (NMDARs) and subsequent massive calcium influx, represents a critical early mechanism of neuronal injury following ischemic stroke. Nanomaterial-based delivery systems targeting excitotoxic pathways have emerged as promising strategies to interrupt this devastating cascade. Recent advances have focused on delivering NMDAR antagonists or disrupting the NMDAR-mediated signaling complex without completely blocking physiological NMDAR function, which is essential for normal synaptic transmission.75 One notable approach involves targeting the protein-protein interaction between postsynaptic density protein-95 (PSD-95) and neuronal nitric oxide synthase (nNOS), thereby selectively inhibiting NMDAR-dependent excitotoxicity while preserving normal NMDAR activity. Li et al developed wheat germ agglutinin (WGA)-modified nanoparticles carrying NR2B9c peptide (NR2B9c-WGA-NPs), which demonstrated strong BBB crossing capability due to WGA’s high affinity for neuronal surface receptors.76 These nanoparticles effectively protected cultured primary cortical neurons from NMDA-induced excitotoxicity, reduced focal ischemic damage in rat brain, and improved neurological function after stroke, highlighting the therapeutic potential of peptide-based excitotoxicity interventions delivered via targeted nanocarriers.
Another innovative strategy for modulating excitotoxicity involves the delivery of small molecule inhibitors that disrupt the nNOS-PSD-95 interaction. Zhao et al developed dual-targeted PEGylated liposomes conjugated with both T7 peptide and SHp peptide (T7&SHp-P-LPs) for targeted delivery of ZL006, a selective nNOS-PSD-95 uncoupler, to ischemic brain tissue.77 In vivo imaging studies demonstrated efficient BBB crossing and accumulation in the ischemic area of MCAO rats, with the treatment significantly reducing infarct size, improving neurological function, and alleviating histopathological damage. Cellular studies further confirmed enhanced BBB crossing and cellular uptake, with the nanoformulation effectively reducing glutamate-induced cell apoptosis.77 These findings underscore the advantage of nanoparticle-based delivery in overcoming the BBB penetration challenges that have hindered the clinical translation of many glutamate receptor antagonists. The targeted delivery approach not only enhances drug concentration at the ischemic site but also minimizes systemic exposure and potential side effects, representing a significant advancement over conventional systemic administration of excitotoxicity inhibitors.92
Anti-Inflammatory Nanomaterials: Targeting Microglial Activation and Cytokine Release
Representative anti-inflammatory nanomaterials are selected based on their ability to modulate post-stroke neuroinflammation, particularly microglial polarization, as well as their translational relevance and in vivo validation. Neuroinflammation, characterized by rapid microglial activation and peripheral immune cell infiltration, represents a critical therapeutic target in ischemic stroke. Microglia, the resident immune cells of the central nervous system, exhibit phenotypic polarization into pro-inflammatory M1 and anti-inflammatory M2 states following ischemic injury, with their activation pattern critically influencing stroke outcomes.78 Recent nanomedicine strategies have focused on modulating microglial polarization to favor neuroprotective M2 phenotypes while suppressing detrimental M1 responses. Li et al developed macrophage membrane-encapsulated manganese dioxide (MnO2) nanoparticles loaded with fingolimod (Ma@(MnO2+FTY)), which demonstrated multifaceted anti-inflammatory effects: (1) enhanced targeting to the inflammatory brain microenvironment via macrophage membrane recognition, (2) ROS scavenging through MnO2-mediated catalytic activity while generating oxygen in situ to rescue hypoxic neurons, and (3) promotion of M2 microglial polarization through STAT3 activation by fingolimod.79 Specifically, the Ma@(MnO2+FTY) system has been reported to suppress pro-inflammatory microglial activation by promoting M2 polarization via STAT3 signaling, thereby attenuating post-stroke neuroinflammatory responses.This biomimetic approach exemplifies the integration of cell membrane camouflage technology with therapeutic nanoparticles to achieve superior brain targeting and immune evasion. Furthermore, Zhang et al engineered M2 macrophage membrane-coated PLGA nanoparticles loaded with baicalin (M2M@BANPs), which demonstrated remarkable synergistic therapeutic effects by combining the intrinsic anti-inflammatory properties of M2-derived membrane components with the neuroprotective activity of baicalin, effectively reprogramming microglia from M1 to M2 phenotype, reducing neutrophil infiltration, and inhibiting neuronal apoptosis.80
Beyond microglial modulation, nanotechnology-based approaches have been developed to directly target inflammatory mediators and signaling pathways. Wang et al demonstrated the potential of C3-siRNA-encapsulated nanoparticles (NPsiC3) to suppress complement component C3 expression in microglia, effectively reducing C3b accumulation on neurons and alleviating microglia-induced neuronal injury. Following intravenous administration, NPsiC3 successfully crossed the BBB and delivered C3-siRNA to the ischemic penumbra, decreasing inflammatory cell infiltration, reducing pro-inflammatory cytokine levels, minimizing neuronal apoptosis, and reducing infarct size while improving functional recovery in ischemia/reperfusion models. Additionally, Jin et al developed ROS-sensitive 18β-glycyrrhetinic acid-conjugated DEAE-dextran nanoparticles (DGA) for targeted delivery of glycyrrhetinic acid, which suppressed high mobility group box 1 (HMGB1) and promoted anti-inflammatory M2 microglial phenotypes in stroke mice, resulting in smaller infarct volumes, improved motor function, and enhanced neurogenesis.81 Recent innovations also include the development of lipid nanoparticles for mRNA delivery to modulate microglial polarization. Gao et al developed M2 microglia-targeting lipid nanoparticles (MLNPs) that selectively deliver mRNA encoding interleukin-10 (IL-10) to the ischemic brain, creating a beneficial feedback loop that promotes microglial polarization toward the protective M2 phenotype and improves BBB integrity following ischemic stroke.82 These diverse anti-inflammatory nanotherapeutic strategies highlight the potential of nanotechnology to precisely modulate complex neuroinflammatory processes and promote tissue repair following cerebral ischemia.
Neuroprotective and Neuroregenerative Nanomaterials: BDNF/VEGF Delivery Systems
Representative neuroprotective and neuroregenerative delivery systems are highlighted based on their capacity to promote neuronal survival and functional recovery, together with considerations of delivery feasibility and translational maturity. Neurotrophic factors, particularly brain-derived neurotrophic factor (BDNF) and vascular endothelial growth factor (VEGF), play essential roles in promoting neuronal survival, stimulating neurogenesis, and facilitating angiogenesis in the ischemic brain. However, their clinical translation has been severely limited by poor BBB penetration, short biological half-lives, and rapid enzymatic degradation in the systemic circulation.83 Nanoparticle-based delivery systems have emerged as promising strategies to overcome these limitations and enable effective neurotrophic factor delivery to the injured brain. Rodriguez-Frutos et al demonstrated that ultrasound-targeted microbubble destruction (UTMD) technology could successfully deliver BDNF to the brain, promoting functional recovery associated with restoration of fiber tract connectivity, increased oligodendrocyte markers, and enhanced myelin regeneration in ischemic stroke models.84 This approach combines the targeting capability of focused ultrasound with the drug-carrying capacity of microbubbles to achieve site-specific BDNF delivery while transiently enhancing BBB permeability. Beyond direct protein delivery, innovative gene therapy approaches have been developed to achieve sustained neurotrophic factor expression. Jiang et al fabricated ROS-responsive charge-reversal poly[(2-acryloyl)ethyl (p-boronic acid benzyl) diethylammonium bromide] (B-PDEA) polymer nanocarriers that efficiently transfected neural stem cells (NSCs) with BDNF-encoding genes. Ischemic stroke mice receiving these transfected NSCs via tail vein injection exhibited significantly elevated BDNF expression levels and remarkably improved survival rates in vivo, demonstrating the potential of combining stem cell therapy with nanotechnology-mediated gene transfer to enhance therapeutic outcomes.85
For VEGF delivery, Oshikawa et al developed laminin-rich porous sponges that immobilize histidine-tagged VEGF through affinity interactions, creating a biomaterial scaffold that provides sustained VEGF release to support angiogenesis in the injured brain.86 When transplanted into mouse stroke models, these VEGF-immobilized sponges produced significantly greater angiogenic activity compared to sponges containing soluble VEGF, highlighting the importance of controlled, localized growth factor presentation for optimal therapeutic effects. Stem cell-based approaches have also been enhanced through nanotechnology. Numerous preclinical and clinical studies have demonstrated that stem cell transplantation provides neuroprotection and enhances motor function recovery following cerebral ischemia, with therapeutic effects primarily mediated by stem cell migration to damaged brain areas and subsequent release of beneficial factors including IL-6, IL-10, VEGF, nerve growth factor (NGF), and BDNF.87 Engineering stem cells to overexpress these therapeutic cytokines using nanoparticle-mediated gene delivery represents an emerging strategy to amplify their regenerative potential. The integration of magnetic nanoparticles with stem cells has enabled real-time tracking of cell migration and homing to ischemic tissues using magnetic resonance imaging, while simultaneously providing magnetic field-guided targeting to enhance therapeutic cell accumulation at injury sites. These diverse neuroprotective and neuroregenerative nanotherapeutic approaches demonstrate the versatility of nanotechnology in delivering or enhancing endogenous neurotrophic signaling to promote tissue repair and functional recovery following ischemic stroke.
Conclusions and Future Directions
This review provides a mechanism-based overview of nanomaterial-based drug delivery systems for ischemic stroke, focusing on BBB crossing strategies and multi-target neuroprotection. Diverse nanoplatforms—including ROS-scavenging, glutamate-modulating, anti-inflammatory, and neurotrophic factor delivery systems—demonstrate the capacity of nanotechnology to address the complex pathophysiology of ischemic stroke. The emergence of multifunctional and biomimetic nanocarriers represents a significant advancement toward integrated therapeutic paradigms.
Despite encouraging preclinical progress, clinical translation remains limited. Key translational bottlenecks include patient heterogeneity, narrow therapeutic windows, incomplete long-term safety characterization, and challenges in scalable manufacturing and regulatory compliance. The spatial and temporal heterogeneity of post-stroke BBB disruption further complicates the design of clinically realistic delivery strategies.
To guide future development, we propose the following recommendations: (i) go/no-go criteria should include reproducible efficacy across multiple stroke models, demonstrated benefit within clinically achievable time windows (≤6 hours), and robust safety profiles; (ii) delivery strategies should prioritize intravenous administration compatible with acute stroke workflows and standard reperfusion therapies; and (iii) trial-relevant endpoints should extend beyond infarct volume to include functional recovery, imaging-based biomarkers, and safety outcomes. Additionally, artificial intelligence and machine learning approaches offer promising tools for optimizing nanocarrier design, predicting BBB transport, and supporting patient stratification, thereby potentially reducing translational attrition.
In summary, three key take-home messages emerge from this review: first, multi-mechanistic targeting is essential given the interconnected pathological cascades in ischemic stroke; second, nanocarrier design must align with clinical realities including feasible delivery routes and therapeutic time windows; and third, integration of AI-assisted optimization with clearly defined translational criteria may accelerate clinical development. A translational roadmap summarizing these considerations is provided in Figure 3.
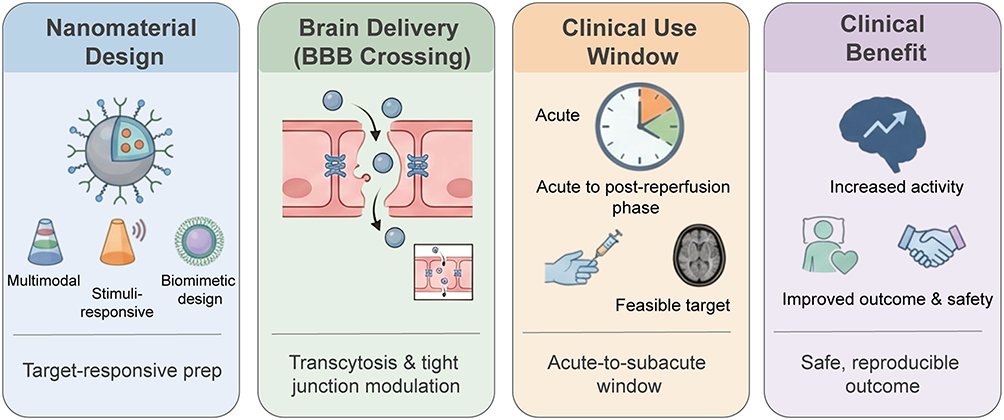 |
Figure 3 Translational roadmap for nanomaterial-based therapy in ischemic stroke. The figure summarizes key translational steps from nanomaterial design and BBB crossing to clinically feasible treatment windows and patient-relevant outcomes. |
Abbreviations
BBB, blood–brain barrier; BDNF, brain-derived neurotrophic factor; CeO2, cerium oxide; FUS, focused ultrasound; MCAO, middle cerebral artery occlusion; NMDAR, N-methyl-D-aspartate receptor; NPs, nanoparticles; PEG, polyethylene glycol; ROS, reactive oxygen species; TfR, transferrin receptor; VEGF, vascular endothelial growth factor.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (No. 82171464, 82371469).
Disclosure
The authors declare no conflict of interest.
References
1. GBD. Stroke collaborators. global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global burden of disease study 2019. Lancet Neurol. 2021;20(10):795–17.
2. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics-2023 update: a report from the American heart association. Circulation. 2023;147(8):e93–e621. doi:10.1161/CIR.0000000000001123
3. Tsivgoulis G, Katsanos AH, Sandset EC, et al. Thrombolysis for acute ischaemic stroke: current status and future perspectives. Lancet Neurol. 2023;22(5):418–429. doi:10.1016/S1474-4422(22)00519-1
4. Zubair AS, Sheth KN. Hemorrhagic Conversion of acute ischemic stroke. Neurotherapeutics. 2023;20(3):705–711. doi:10.1007/s13311-023-01377-1
5. Blase A, Di Girasole CG, Benjamin L, Turowski P. Phased blood-brain barrier disruption in ischaemic stroke: implications for therapy?. Fluids Barriers CNS. 2025;22(1):90. doi:10.1186/s12987-025-00701-5
6. Ezzaki C, Chaari A, Al-Othman A. Recent advances on chitosan-based nanoparticles for brain drug delivery. Polymers. 2025;17(22):3055. doi:10.3390/polym17223055
7. Liang Y, Jiang Y, Liu J, et al. Blood-brain barrier disruption and imaging assessment in stroke. Transl Stroke Res. 2025;16(4):1400–1411. doi:10.1007/s12975-024-01300-6
8. Vignoli A, Sticchi E, Piccardi B, et al. Predicting reperfusion injury and functional status after stroke using blood biomarkers: the STROKELABED study. J Transl Med. 2025;23(1):491. doi:10.1186/s12967-025-06498-z
9. Wang RF, Liu J, Chen CH. Vascular recanalization exacerbates BBB permeability after ischemic stroke. Front Neurol. 2025;16:1682748. doi:10.3389/fneur.2025.1682748
10. Alaqel SI, Imran M, Khan A, Nayeem N. Aging, vascular dysfunction, and the blood-brain barrier: unveiling the pathophysiology of stroke in older adults. Biogerontology. 2025;26(2):67. doi:10.1007/s10522-025-10209-y
11. Cheng F, Yan B, Liao P, et al. Ischemic stroke and the biological hallmarks of aging. Aging Dis. 2024;16(5):2908–2936. doi:10.14336/AD.2024.1059
12. Niu P, Li L, Zhang Y, et al. Immune regulation based on sex differences in ischemic stroke pathology. Front Immunol. 2023;14:1087815. doi:10.3389/fimmu.2023.1087815
13. Chen C, Xu X, Lu J, Xiang Y, Shi L, Liu D. Hyperglycemia-induced blood-brain barrier dysfunction: mechanisms and therapeutic interventions. Microvasc Res. 2025;160:104820. doi:10.1016/j.mvr.2025.104820
14. Chen JXY, Vipin A, Sandhu GK, et al. Blood-brain barrier integrity disruption is associated with both chronic vascular risk factors and white matter hyperintensities. J Prev Alzheimers Dis. 2025;12(2):100029. doi:10.1016/j.tjpad.2024.100029
15. Saraiva C, Praça C, Ferreira R, Santos T, Ferreira L, Bernardino L. Nanoparticle-mediated brain drug delivery: overcoming blood-brain barrier to treat neurodegenerative diseases. J Control Release. 2016;235:34–47. doi:10.1016/j.jconrel.2016.05.044
16. Fisher M, Savitz SI. Pharmacological brain cytoprotection in acute ischaemic stroke — renewed hope in the reperfusion era Rev Neurol. 2022;18(4):193–202. doi:10.1038/s41582-021-00605-6
17. Zhang L, Li W, Xu Z, et al. Promoting transcellular traversal of the blood–brain barrier by simultaneously improving cellular uptake and accelerating lysosomal escape. Nanoscale. 2025;17(11):6780–6792. doi:10.1039/D4NR05134C
18. Zhang Y, Zhang H, Zhao F, et al. Mitochondrial-targeted and ROS-responsive nanocarrier via nose-to-brain pathway for ischemic stroke treatment. Acta Pharm Sin B. 2023;13(12):5107–5120. doi:10.1016/j.apsb.2023.06.011
19. Joyce P, Allen CJ, Alonso MJ, et al. A translational framework to DELIVER nanomedicines to the clinic. Nat Nanotechnol. 2024;19(11):1597–1611. doi:10.1038/s41565-024-01754-7
20. Fu F, Crespy D, Landfester K, Jiang S. In situ characterization techniques of protein Corona around nanomaterials. Chem Soc Rev. 2024;53(22):10827–10851.
21. Wang Y, Ge M, Wang J, Xu Y, Wang N, Xu S. Metabolic reprogramming in ischemic stroke: when glycolytic overdrive meets lipid storm. Cell Death Dis. 2025;16(1):788. doi:10.1038/s41419-025-08114-w
22. Chen H, He Y, Chen S, Qi S, Shen J. Therapeutic targets of oxidative/nitrosative stress and neuroinflammation in ischemic stroke: applications for natural product efficacy with omics and systemic biology. Pharmacol Res. 2020;158:104877. doi:10.1016/j.phrs.2020.104877
23. Salaudeen MA, Bello N, Danraka RN, Ammani ML. Understanding the pathophysiology of ischemic stroke: the basis of current therapies and opportunity for new ones. Biomolecules. 2024;14(3):305. doi:10.3390/biom14030305
24. Orellana-Urzúa S, Rojas I, Líbano L, Rodrigo R. Pathophysiology of ischemic stroke: role of oxidative stress. Curr Pharm Des. 2020;26(34):4246–4260. doi:10.2174/1381612826666200708133912
25. Elhamrawy EA, Shoman H, Abdel-Tawab H, et al. Oxidative stress and early mortality in acute ischemic stroke: a prospective cohort study. Neurol Res. 2023;45(11):1003–1010. doi:10.1080/01616412.2023.2252284
26. Pawluk H, Tafelska-Kaczmarek A, Sopońska M, et al. the influence of oxidative stress markers in patients with ischemic stroke. Biomolecules. 2024;14(9):1130. doi:10.3390/biom14091130
27. Li C, Xing Y, Zhang Y, Hua Y, Hu J, Bai Y. Neutrophil extracellular traps exacerbate ischemic brain damage. Mol Neurobiol. 2022;59(1):643–656. doi:10.1007/s12035-021-02635-z
28. Vahidinia Z, Karimian M, Joghataei MT. Neurosteroids and their receptors in ischemic stroke: from molecular mechanisms to therapeutic opportunities. Pharmacol Res. 2020;160:105163. doi:10.1016/j.phrs.2020.105163
29. Pawluk H, Woźniak A, Tafelska-Kaczmarek A, et al. The Role of IL-6 in ischemic stroke. Biomolecules. 2025;15(4):470. doi:10.3390/biom15040470
30. Qin C, Yang S, Chu Y-H, et al. Signaling pathways involved in ischemic stroke: molecular mechanisms and therapeutic interventions. Signal Transduct Target Ther. 2022;7(1):215. doi:10.1038/s41392-022-01064-1
31. Rust R, Yin H, Achón Buil B, Sagare AP, Kisler K. The blood-brain barrier: a help and a hindrance. Brain. 2025;148(7):2262–2282.
32. Zhang X, Fu M, Wang Y, Wu T. Strategies for delivering drugs across the blood-brain barrier for the treatment of neurodegenerative diseases. Front Drug Deliv. 2025;5:1644633. doi:10.3389/fddev.2025.1644633
33. D’Souza A, Dave KM, Stetler RA, et al. Targeting the blood-brain barrier for the delivery of stroke therapies. Adv Drug Deliv Rev. 2021;171:332–351. doi:10.1016/j.addr.2021.01.015
34. Leigh R, Knutsson L, Zhou J, van Zijl PC. Imaging the physiological evolution of the ischemic penumbra in acute ischemic stroke. J Cereb Blood Flow Metab. 2018;38(9):1500–1516. doi:10.1177/0271678X17700913
35. Dong X. Current strategies for brain drug delivery. Theranostics. 2018;8(6):1481–1493. doi:10.7150/thno.21254
36. Achar A, Myers R, Ghosh C. Drug delivery challenges in brain disorders across the blood–brain barrier: novel methods and future considerations for improved therapy. Biomedicines. 2021;9(12):1834. doi:10.3390/biomedicines9121834
37. Yang Y, Rosenberg GA. Blood–brain barrier breakdown in acute and chronic cerebrovascular disease. Stroke. 2011;42(11):3323–3328. doi:10.1161/STROKEAHA.110.608257
38. Chamorro Á, Dirnagl U, Urra X, Planas AM. Neuroprotection in acute stroke: targeting excitotoxicity, oxidative and nitrosative stress, and inflammation. Lancet Neurol. 2016;15(8):869–881. doi:10.1016/S1474-4422(16)00114-9
39. Warner JJ, Harrington RA, Sacco RL, Elkind MSV. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke. Stroke. 2019;50(12):3331–3332. doi:10.1161/STROKEAHA.119.027708
40. Günkan A, Ferreira MY, Vilardo M, et al. Thrombolysis for ischemic stroke beyond the 4.5-hour window: a meta-analysis of randomized clinical trials. Stroke. 2025;56(3):580–590. doi:10.1161/STROKEAHA.124.048536
41. Emberson J, Lees KR, Lyden P, et al. Stroke Thrombolysis Trialists’ Collaborative Group. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet. 2014;384(9958):1929–1935. doi:10.1016/S0140-6736(14)60584-5
42. Nogueira RG, Jadhav AP, Haussen DC, et al. Dawn trial investigators. thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 2018;378(1):11–21. doi:10.1056/NEJMoa1706442
43. Goyal M, Menon BK, van Zwam WH, et al. HERMES collaborators. endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387(10029):1723–1731. doi:10.1016/S0140-6736(16)00163-X
44. Sutherland BA, Neuhaus AA, Couch Y, et al. The transient intraluminal filament middle cerebral artery occlusion model as a model of endovascular thrombectomy in stroke. J Cereb Blood Flow Metab. 2016;36(2):363–369. doi:10.1177/0271678X15606722
45. Patel MM, Patel BM. Crossing the blood–brain barrier: recent advances in drug delivery to the brain. CNS Drugs. 2017;31(2):109–133. doi:10.1007/s40263-016-0405-9
46. Teleanu DM, Niculescu A-G, Lungu II, et al. An overview of oxidative stress, neuroinflammation, and neurodegenerative diseases. Int J Mol Sci. 2022;23(11):5938. doi:10.3390/ijms23115938
47. Zheng M, Tao W, Zou Y, Farokhzad OC, Shi B. Nanotechnology-based strategies for siRNA brain delivery for disease therapy. Trends Biotechnol. 2018;36(5):562–575. doi:10.1016/j.tibtech.2018.01.006
48. Chen Y, Liu L. Modern methods for delivery of drugs across the blood-brain barrier. Adv Drug Deliv Rev. 2012;64(7):640–665. doi:10.1016/j.addr.2011.11.010
49. Suk JS, Xu Q, Kim N, Hanes J, Ensign LM. PEGylation as a strategy for improving nanoparticle-based drug and gene delivery. Adv Drug Deliv Rev. 2016;99(Pt A):28–51. doi:10.1016/j.addr.2015.09.012
50. Knop K, Hoogenboom R, Fischer D, Schubert US. Poly(ethylene glycol) in drug delivery: pros and cons as well as potential alternatives. Angew Chem Int Ed Engl. 2010;49(36):6288–6308. doi:10.1002/anie.200902672
51. Du J-Z, Sun T-M, Song W-J, Wu J, Wang J. A tumor-acidity-activated charge-conversional nanogel as an intelligent vehicle for promoted tumoral-cell uptake and drug delivery. Angew Chem Int Ed Engl. 2010;49(21):3621–3626. doi:10.1002/anie.200907210
52. Schlenoff JB. Zwitteration: coating surfaces with zwitterionic functionality to reduce nonspecific adsorption. Langmuir. 2014;30(32):9625–9636. doi:10.1021/la500057j
53. Johnsen KB, Burkhart A, Thomsen LB, Andresen TL, Moos T. Targeting the transferrin receptor for brain drug delivery. Prog Neurobiol. 2019;181:101665. doi:10.1016/j.pneurobio.2019.101665
54. Wiley DT, Webster P, Gale A, Davis ME. Transcytosis and brain uptake of transferrin-containing nanoparticles by tuning avidity to transferrin receptor. Proc Natl Acad Sci USA. 2013;110(21):8662–8667. doi:10.1073/pnas.1307152110
55. Ci T, Chen L, Yu L, Ding J. Tumor regression achieved by encapsulating a moderately soluble drug into a polymeric thermogel. Sci Rep. 2014;4(1):5473. doi:10.1038/srep05473
56. Cutone A, Rosa L, Ianiro G, et al. Lactoferrin’s anti-cancer properties: safety, selectivity, and wide range of action. Biomolecules. 2020;10(3):456. doi:10.3390/biom10030456
57. Demeule M, Régina A, Ché C, et al. Identification and design of peptides as a new drug delivery system for the brain. J Pharmacol Exp Ther. 2008;324(3):1064–1072. doi:10.1124/jpet.107.131318
58. Oller-Salvia B, Sánchez-Navarro M, Giralt E, Teixidó M. Blood–brain barrier shuttle peptides: an emerging paradigm for brain delivery. Chem Soc Rev. 2016;45(17):4690–4707. doi:10.1039/C6CS00076B
59. Lipsman N, Meng Y, Bethune AJ, et al. Blood–brain barrier opening in Alzheimer’s disease using MR-guided focused ultrasound. Nat Commun. 2018;9(1):2336. doi:10.1038/s41467-018-04529-6
60. Tapeinos C, Battaglini M, Ciofani G. Advances in the design of solid lipid nanoparticles and nanostructured lipid carriers for targeting brain diseases. J Control Release. 2017;264:306–332. doi:10.1016/j.jconrel.2017.08.033
61. Kaushik A, Jayant RD, Sagar V, Nair M. The potential of magneto-electric nanocarriers for drug delivery. Expert Opin Drug Deliv. 2014;11(10):1635–1646. doi:10.1517/17425247.2014.933803
62. Ulbrich K, Holá K, Šubr V, Bakandritsos A, Tuček J, Zbořil R. Targeted drug delivery with polymers and magnetic nanoparticles: covalent and noncovalent approaches, release control, and clinical studies. Chem Rev. 2016;116(9):5338–5431. doi:10.1021/acs.chemrev.5b00589
63. Shen Y, Tang H, Radosz M, Van Kirk E, Murdoch WJ. pH-responsive nanoparticles for cancer drug delivery. Methods Mol Biol. 2008;437:183–216. doi:10.1007/978-1-59745-210-6_10
64. Yin T, Wang P, Li J, et al. Tumor-penetrating codelivery of siRNA and paclitaxel with ultrasound-responsive nanobubbles hetero-assembled from polymeric micelles and liposomes. Biomaterials. 2014;35(22):5932–5943. doi:10.1016/j.biomaterials.2014.03.072
65. Liu J, Huang Y, Kumar A, et al. pH-sensitive nano-systems for drug delivery in cancer therapy. Biotechnol Adv. 2014;32(4):693–710. doi:10.1016/j.biotechadv.2013.11.009
66. Song G, Zhao M, Chen H, et al. The role of nanomaterials in stroke treatment: targeting oxidative stress. Oxid Med Cell Longev. 2021;2021(1):8857486. doi:10.1155/2021/8857486
67. Vani JR, Mohammadi MT, Foroshani MS, Jafari M. Polyhydroxylated fullerene nanoparticles attenuate brain infarction and oxidative stress in rat model of ischemic stroke. EXCLI J. 2016;15:378–390. doi:10.17179/excli2016-309
68. Lin AM, Fang SF, Lin SZ, Chou CK, Luh TY, Ho LT. Local carboxyfullerene protects cortical infarction in rat brain. Neurosci Res. 2002;43(4):317–321. doi:10.1016/S0168-0102(02)00056-1
69. Sarami Foroshani M, Sobhani ZS, Mohammadi MT, Aryafar M. Fullerenol nanoparticles decrease blood-brain barrier interruption and brain edema during cerebral ischemia-reperfusion injury probably by reduction of interleukin-6 and matrix metalloproteinase-9 transcription. J Stroke Cerebrovasc Dis. 2018;27(11):3053–3065. doi:10.1016/j.jstrokecerebrovasdis.2018.06.042
70. Nozohouri S, Sifat AE, Vaidya B, Abbruscato TJ. Novel approaches for the delivery of therapeutics in ischemic stroke. Drug Discov Today. 2020;25(3):535–551. doi:10.1016/j.drudis.2020.01.007
71. Zhang J, Chen Z, Chen Q. Advanced nano-drug delivery systems in the treatment of ischemic stroke. Molecules. 2024;29(8):1848. doi:10.3390/molecules29081848
72. Wu Y, Ta HT. Different approaches to synthesising cerium oxide nanoparticles and their corresponding physical characteristics, and ROS scavenging and anti-inflammatory capabilities. J Mater Chem. 2021;9(36):7291–7301. doi:10.1039/d1tb01091c
73. Amaldoss MJN, Mehmood R, Yang JL, et al. Anticancer therapeutic effect of cerium-based nanoparticles: known and unknown molecular mechanisms. Biomater Sci. 2022;10(14):3671–3694. doi:10.1039/d2bm00334a
74. Corsi F, Di Meo E, Lulli D, et al. Safe-shields: basal and anti-UV protection of human keratinocytes by redox-active cerium oxide nanoparticles prevents UVB-induced mutagenesis. Antioxidants. 2023;12(3):757. doi:10.3390/antiox12030757
75. Blinova E, Turovsky E, Eliseikina E, et al. Novel hydroxypyridine compound protects brain cells against ischemic damage in vitro and in vivo. Int J Mol Sci. 2022;23(21):12953. doi:10.3390/ijms232112953
76. Chen J, Jin J, Li K, Shi L, Wen X, Fang F. Progresses and prospects of neuroprotective agents-loaded nanoparticles and biomimetic material in ischemic stroke. Front Cell Neurosci. 2022;16:868323. doi:10.3389/fncel.2022.868323
77. Zhao Y, Jiang Y, Lv W, et al. Dual targeted nanocarrier for brain ischemic stroke treatment. J Control Release. 2016;233:64–71. doi:10.1016/j.jconrel.2016.04.038
78. Xia X, Chen W, Zhou T, et al. TEPP-46 inhibits glycolysis to promote M2 polarization of microglia after ischemic stroke. Int Immunopharmacol. 2025;149:114148. doi:10.1016/j.intimp.2025.114148
79. Lei SY, Yang YQ, Liu JC, et al. Nanodrug delivery systems for regulating microglial polarization in ischemic stroke treatment: a review. J Tissue Eng. 2024;15:20417314241237052. doi:10.1177/20417314241237052
80. Zhang S, Li R, Song M, Han J, Fan X. Exploration of M2 macrophage membrane as a biotherapeutic agent and strong synergistic therapeutic effects in ischemic stroke. J Control Release. 2025;378:476–489. doi:10.1016/j.jconrel.2024.11.033
81. Jin K, Luo Z, Zhang B, Pang Z. Biomimetic nanoparticles for inflammation targeting. Acta Pharm Sin B. 2018;8(1):23–33. doi:10.1016/j.apsb.2017.12.002
82. Gao M, Li Y, Ho W, et al. Targeted mRNA nanoparticles ameliorate blood–brain barrier disruption postischemic stroke by modulating microglia polarization. ACS Nano. 2024;18(4):3260–3275. doi:10.1021/acsnano.3c09817
83. Manickam DS, Brynskikh AM, Kopanic JL, et al. Well-defined cross-linked antioxidant nanozymes for treatment of ischemic brain injury. J Control Release. 2012;162(3):636–645. doi:10.1016/j.jconrel.2012.07.044
84. Rodríguez-Frutos B, Otero-Ortega L, Ramos-Cejudo J, et al. Enhanced brain-derived neurotrophic factor delivery by ultrasound and microbubbles promotes white matter repair after stroke. Biomaterials. 2016;100:41–52. doi:10.1016/j.biomaterials.2016.05.028
85. Jiang XC, Xiang JJ, Wu HH, et al. Neural stem cells transfected with reactive oxygen species–responsive polyplexes for effective treatment of ischemic stroke. Adv Mater. 2019;31(10):e1807591. doi:10.1002/adma.201807591
86. Oshikawa M, Okada K, Kaneko N, Sawamoto K, Ajioka I. Affinity-immobilization of VEGF on laminin porous sponge enhances angiogenesis in the ischemic brain. Adv Healthc Mater. 2017;6(11). doi:10.1002/adhm.201700183
87. Nakajima M, Nito C, Sowa K, et al. Mesenchymal stem cells overexpressing interleukin-10 promote neuroprotection in experimental acute ischemic stroke. Mol Ther Methods Clin Dev. 2017;6:102–111. doi:10.1016/j.omtm.2017.06.005
88. Zhao Y, Song C, Wang H, et al. Polydopamine-cloaked nanoarchitectonics of prussian blue nanoparticles promote functional recovery in neonatal and adult ischemic stroke models. Biomater Res. 2024;28:0079. doi:10.34133/bmr.0079
89. Wang J, Guo Y, Wu X, et al. A cascade reaction nanoplatform with magnetic resonance imaging capability for combined photothermal/chemodynamic/gas cancer therapy. J Pharm Anal. 2025;15(9):101223. doi:10.1016/j.jpha.2025.101223
90. Mozafari F, Rashidzadeh H, Bijani S, et al. Enhancing the neuroprotection potential of edaravone in transient global ischemia treatment with glutathione- (GSH-) conjugated poly(methacrylic acid) nanogel as a promising carrier for targeted brain drug delivery. Oxid Med Cell Longev. 2023;2023:7643280.
91. Jiang Z, Chen Q, Yang H. Drug delivery strategies for neuroprotective therapy in ischemic stroke: application of nanotechnology. Neural Regen Res. 2026;21(5):1793–1808. doi:10.4103/NRR.NRR-D-24-01383
92. Chen W, Jiang L, Hu Y, et al. Nanomedicines, an emerging therapeutic regimen for treatment of ischemic cerebral stroke: a review. J Control Release. 2021;340:342–360. doi:10.1016/j.jconrel.2021.10.020
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multiomic Profiling and Neuroprotective Bioactivity of Salvia Hairy Root-Derived Extracellular Vesicles in a Cellular Model of Parkinson’s Disease

Vestuto V, Conte M, Vietri M, Mensitieri F, Santoro V, Di Muro A, Alfieri M, Moros M, Miranda MR, Amante C, Delli Carri M, Campiglia P, Dal Piaz F, Del Gaudio P, De Tommasi N, Leone A, Moltedo O, Pepe G, Cappetta E, Ambrosone A
International Journal of Nanomedicine 2024, 19:9373-9393
Published Date: 11 September 2024
Drug Delivery System Targeting Cancer-Associated Fibroblast for Improving Immunotherapy
Zhang Z, Wang R, Chen L
International Journal of Nanomedicine 2025, 20:483-503
Published Date: 11 January 2025
Research and Application Prospect of Nanomedicine in Kidney Disease: A Bibliometric Analysis From 2003 to 2024

Meng Y, Sui L, Xu T, Zhao H, Yuan Q, Sun L
International Journal of Nanomedicine 2025, 20:3007-3030
Published Date: 12 March 2025
Recent Advances in Nanozymes for the Treatment of Atherosclerosis
Zou Z, Bi X, Ma H, Chen L, Jin H, Gong S, Li X, Liu X
International Journal of Nanomedicine 2025, 20:9447-9472
Published Date: 29 July 2025
Phytochemical and Anti-Ischemic Stroke Properties from the Vitex L. Genus
Xie C, Wu J, Huang P
Drug Design, Development and Therapy 2026, 20:585338
Published Date: 11 February 2026