Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Endothelial Function in Obese Patients Treated with Bariatric Surgery
Authors Borzì AM ![]() , Buscemi C, Corleo D
, Buscemi C, Corleo D ![]() , Randazzo C
, Randazzo C ![]() , Rosafio G
, Rosafio G ![]() , Pantuso G, Buscemi S
, Pantuso G, Buscemi S ![]()
Received 12 September 2019
Accepted for publication 23 January 2020
Published 4 February 2020 Volume 2020:13 Pages 247—256
DOI https://doi.org/10.2147/DMSO.S230684
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Antonio Maria Borzì,1,2,* Carola Buscemi,3,4,* Davide Corleo,3,4 Cristiana Randazzo,3,4 Giuseppe Rosafio,3,4 Gianni Pantuso,5 Silvio Buscemi3,4
1Department of Clinical and Experimental Medicine, Specialization School in Geriatrics, University of Catania, Catania, Italy; 2Specialization School in Geriatrics, Catania, Italy; 3Dipartimento di Promozione della Salute, Materno-Infantile, Medicina Interna e Specialistica di Eccellenza (PROMISE), University of Palermo, Palerno, Italy; 4Unit of Malattie Endocrine, del Ricambio e della Nutrizione, Policlinico University Hospital, Palermo, Italy; 5Dipartimento di Discipline Chirurgiche e Odontostomatologiche (DICHIRONS), Unit of Chirurgia Oncologica, Policlinico University Hospital, Palermo, Italy
*These authors contributed equally to this work
Correspondence: Silvio Buscemi
Unit of Malattie Endocrine, del Ricambio e della Nutrizione, Policlinico University Hospital, Piazza delle cliniche 2, Palermo 90127, Italy
Email [email protected]
Purpose: Bariatric surgery (BS) is becoming an increasingly frequent treatment option especially in people with morbid obesity, demonstrating that it is able to reduce total mortality and cardiovascular (CV) risk. Despite endothelial dysfunction is an essential requisite contributing to atherosclerosis and predicting CV events, only some studies have investigated the effects of BS on endothelial function with controversial results. In this study, the effects of weight loss on endothelial function were investigated in obese patients after BS and compared with patients after medical nutrition treatment (MNT).
Patients and Methods: Seventeen obese patients who underwent BS procedures (9 adjustable gastric bands, 3 gastric by-passes and 5 biliopancreatic diversions) were included in the study and compared with 18 obese individuals who underwent MNT. Endothelial function was investigated by flow-mediated dilation (FMD) of the brachial artery. Also, carotid intima-media thickness (c-IMT) was measured as a marker of subclinical atherosclerosis.
Results: At the end of follow-up, the mean weight loss was 18.8% in the BS group and 7.0% in the MNT group. After treatment, FMD significantly decreased in the BS group (mean ± SD before: 9.0 ± 4.7; after: 6.1 ± 2.9%; P= 0.04); however, no significant change was observed in the MNT group (before: 9.4 ± 5.8; after: 8.3 ± 5.3; P= 0.41). The modification of endothelial function was negatively correlated with c-IMT change in the BS group (r= − 0.63; P < 0.007).
Conclusion: A significant endothelial dysfunction occurred following BS but not after MNT. Furthermore, the decline of endothelial function observed in the BS group might have contributed to atherosclerosis.
Keywords: obesity, endothelial function, bariatric surgery, medical nutrition therapy
Introduction
Obesity is a multifactorial disease that develops following a sufficiently prolonged period of time in which energy intake exceeds energy expenditure. Parallel to progressive urbanization, the prevalence of overweight/obesity is continuously rising1 even among children and adolescents.2 Therefore, obesity represents a real emergency in the Western world due to its association with many health problems among which reduced life expectancy,3 compromised quality of life,4 increased metabolic complications such as diabetes and cardiovascular (CV) morbidity and mortality.5 The global burden of obesity is also associated with high costs and represents a serious threat to the sustainability of health systems.6 Therefore, both effective preventive strategies and treatment approaches are urgently needed. At present, the gold standard for the treatment of obesity is medical nutrition treatment (MNT), based on a cognitive behavioral approach aimed at changing lifestyle with appropriate dietary habits and an adequate level of physical activity.7 However, the MNT is often followed by frequent regain of weight loss especially in people with morbid obesity. In the latter cases, bariatric surgery (BS) is becoming an increasingly frequent treatment option. Despite its costs and possible side effects, BS is now acknowledged to be a relatively safe treatment that is more effective than MNT at least in terms of the amount of weight loss.8 Although a large body of epidemiological evidence suggests the association between obesity and CV morbidity and mortality, it has not been definitively established that reducing body weight is associated with significant prevention of these outcomes, especially in the case of MNT. However, there is some evidence that BS reduces both CV mortality and CV events.8,9 All conditions, including obesity, that are associated with increased CV risk are characterized by endothelial dysfunction10 which is an established requisite condition for atherosclerosis.11 Currently, the reference method for in-vivo investigation of endothelial function consists in measuring the ability of dilating the brachial artery after the stimulus of both hypoxia and increasing blood flow, namely flow-mediated dilation (FMD).12 A large body of evidence has demonstrated that low FMD strongly predicts CV events.13 To date, only few studies have investigated the effects of BS on endothelial function in terms of FMD demonstrating in general that FMD improves after BS.14 However, some controversial results have also been reported and some studies have failed to confirm these conclusions.15–17 Therefore, in this present study, we investigated the consequences of weight loss on endothelial function, measured as FMD, in obese patients with available data after BS who were compared with obese patients after MNT.
Materials and Methods
Participants
Seventeen obese patients were included in the study among those with available data who underwent BS procedures in the period from 2007 to 2012 at the Surgical Oncology Unit and at the Minimally Invasive Surgery Unit of the Policlinico “P. Giaccone” University Hospital in Palermo (Italy). Different BS procedures were performed according to SICOB guidelines:18 9 adjustable gastric banding (GB) procedures, 3 gastric by-passes (GBP) and 5 biliopancreatic diversions (BPD). These patients were compared with a group of 18 obese patients who in the same period were referred to the Laboratory of Metabolism and Clinical Nutrition of the Dipartimento Biomedico di Medicina Interna e Specialistica (DIBIMIS; University of Palermo, Italy) for medical nutritional treatment (MNT) of obesity consisting in a hypocaloric diet [20 kcal/kg body weight of which: 55% carbohydrates, 25% fats (20% saturated, 65% monounsaturated and 15% polyunsaturated fats) and 20% proteins; the daily intakes of fibers and cholesterol were 30 g and ≤250 mg, respectively. No supplementation of vitamins, antioxidants or minerals was prescribed and general advice aiming at increasing the habitual level of physical activity. For both BS and MNT patients, inclusion criteria were age of 18–65 years, body mass index (BMI; body weight/height2) ≥28.0 kg/m2 for MNT patients and ≥35.0 kg/m2 for BS patients. Exclusion criteria were major complications following BS and significant comorbidities, including heart failure, coronary heart disease, stroke, chronic kidney disease, liver cirrhosis, chronic respiratory failure and diabetes under medical treatment (with the exclusion of metformin), pregnancy and lactation, lack of release of informed consent.
All participants were examined before (0–1 month) and after BS (6–24 months) or MNT (3–18 months). The assignment of the medical intervention was not at the discretion of the investigators and measurements performed were part of clinical procedures of the center. The institutional Ethics Committee (“Palermo 1” of the Policlinico “P. Giaccone” University Hospital) approved the study protocol. All participants accepted informed consent form.
Anthropometric Measurements
All measurements were performed in the morning, after overnight fasting. Height and body weight were measured with subjects lightly dressed and without shoes. Fat mass (FM %) and fat-free mass (FFM, kg) body composition were measured by the Bioelectrical Impedance Analysis method (BIA-103, RJL, Detroit, MI, USA/Akern, Florence, Italy) following the manufacturer’s equations, as elsewhere described.19 Body circumference (waist circumference) was measured at the umbilical level as a surrogate measure of visceral adipose tissue.
Cardiovascular Measurement
Echographic scans of both extracranial carotid artery walls were performed with a high-resolution ultrasound 10-MHz linear array transducer (Sonoline G50; Siemens, Germany); the best longitudinal ultrasound scan was stored on digital support. Measurements of intima-media thickness (c-IMT) were later accomplished. The end-diastolic c-IMT of the far wall of right and left common carotid arteries was measured as elsewhere described.20 The mean value between both carotid c-IMT was calculated according to guidelines.21 A trained operator performed all the ultrasonographic measurements. A 12-lead electrocardiogram was performed for each participant and the main parameters were obtained automatically using an integrated auto-diagnostic software (Esaote; Firenze, Italy); furthermore, the corrected QT interval for heart rate (QTc) was also evaluated.
Endothelial Function
The endothelial function was evaluated through FMD measurement of the brachial artery A high-resolution ultrasound linear probe (10 MHz, Sonoline G50; Siemens, Germany) was used. A stereotactic clamp with micrometer alignment (EDI Progetti e Sviluppo; Pisa, Italy) immobilized the probe during the test to guarantee image reliability. A sphygmomanometer was cuffed at 220–250 mmHg 2 cm below the antecubital fossa for 300 s to occlude the artery and establish reactive hyperemia. Twenty minutes later FMD measurement, 300 μg of sublingual glyceryl-trinitrate (GTN) was administered to evaluate endothelium-independent dilation. A real-time computed video-analysis of B-mode ultrasound images (FMD Studio; Institute of Physiology CNR; Pisa, Italy) recorded the brachial artery diameter variations. The diameter is detected with subpixel precision with a rate of 25 frames per second. The brachial artery diameters were represented on a graphical interface over a time scale of 9 min. The mean of the measures obtained during the first minute set the baseline vessel size. Both FMD and GTN were calculated as the maximum percentage increase of brachial artery diameter over baseline. These procedures are explained elsewhere.10,22 All the FMD tests were performed by the same operator. A trained operator who was blinded to the participant’s treatment classification performed all the ultrasonographic measurements. Our intra-observer coefficient of variation for FMD is 2.9%.
Laboratory Analysis
All participants underwent blood sampling in the morning, after overnight fasting. Fasting plasma glucose (FPG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), triglycerides (Tg) and uric acid concentrations were measured using standard clinical chemistry methods (Glucose HK UV; Tot. cholesterol Mod P/D; HDL cholesterol gen 3 mod P/917; Triglycerides; Uric acid MOD P/917; Roche Diagnostics; Monza, Italy). Friedewald’s equation was used to determine low-density lipoprotein (LDL) cholesterol serum.23
Statistical Analysis
Data are reported as mean values ± SD or as prevalence. The independent samples Student’s t-test was used to compare the two groups; otherwise, Pearson’s χ2 test was used when appropriate. The effect of BS and MNT was assessed by paired samples Student’s t-test. The simple linear regression coefficient r was calculated to study the correlations among variables. A two-tailed P value <0.05 was considered significant. All analyses were performed with Systat (Windows version 11.0; San Jose, CA, USA).
Results
A total of 35 patients (17 undergoing BS and 18 undergoing MNT) were selected. The demographic and clinical characteristics of the 2 groups are shown in Tables 1 and 2. The length of follow-up of the BS group was higher than that of the MNT group (P< 0.001). The MNT group was older than the BS group (P= 0.01), the BS group showed higher BMI (P< 0.001), body weight (P< 0.001), waist circumference (P< 0.001) and FFM-kg (P< 0.001) than the MNT group. The blood concentrations of FPG (P< 0.05), TC (P< 0.05) and LDL cholesterol (P< 0.05) were higher in the MNT group than in the BS group. At the end of follow-up, the mean weight loss was 18.8% in the BS group and 7.0% in the MNT group. Pre-treatment FMD was not different between the groups (P= NS); however, after treatment, FMD was significantly reduced in the BS group (P= 0.04), whereas no significant change was observed in the MNT group (P= 0.41) (Table 2 and Figure 1). Contrary to the average trend of FMD in the BS group, four patients of this group (2 GBP and 2 BPD) exhibited a significant increase of FMD following the surgical procedure. Both studied groups had similar values of GTN and c-IMT. The change in endothelial function (∆ FMD) was negatively correlated with c-IMT change (∆ c-IMT) in the BS group (r= −0.63; P <0.007; Figures 1 and 2).
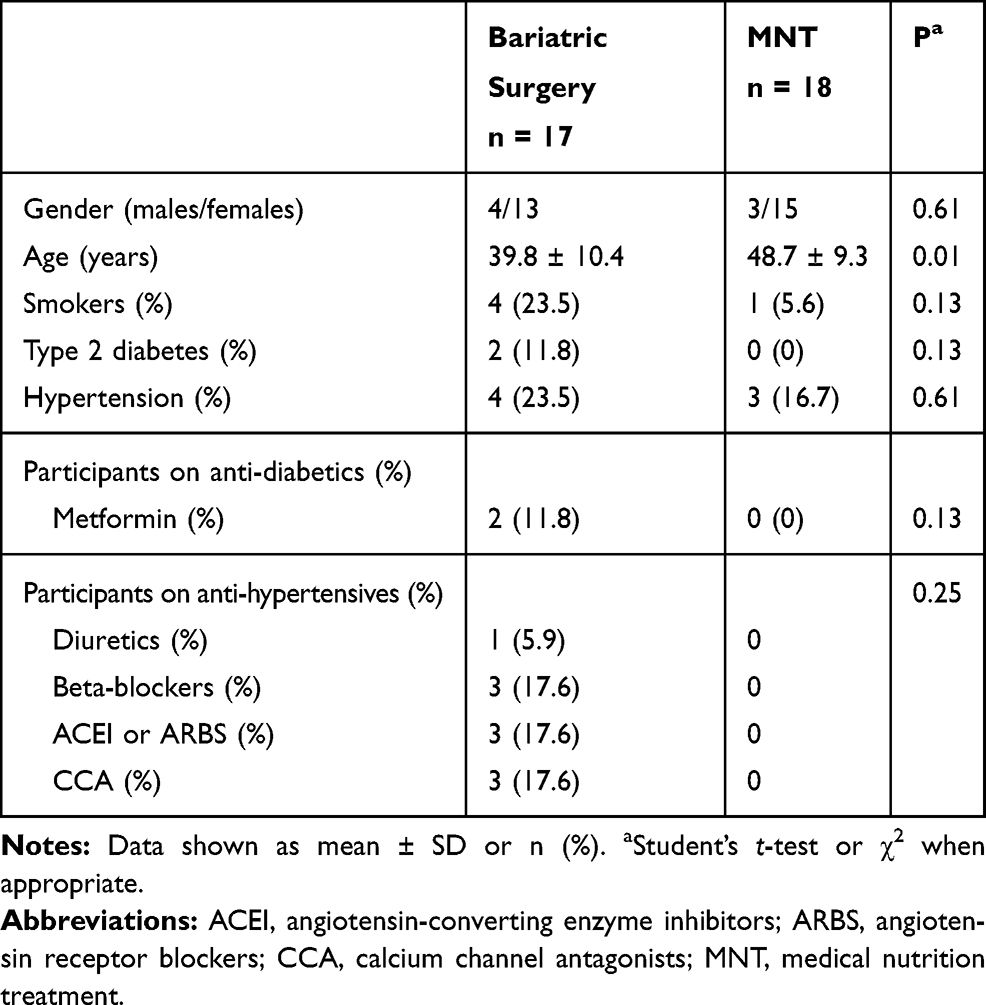 |
Table 1 Characteristics of the Studied Groups |
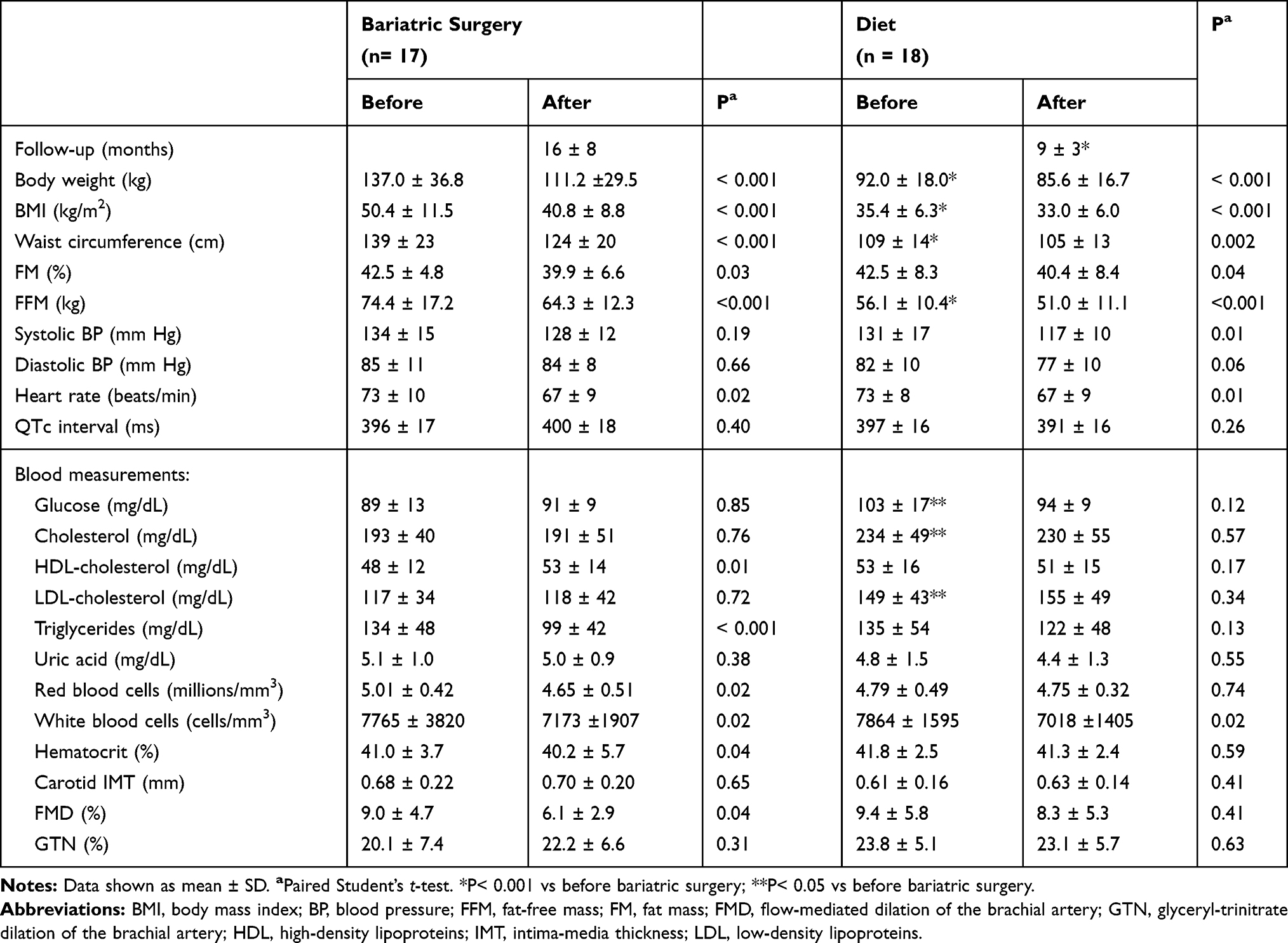 |
Table 2 Changes in Clinical and Physical Measurements After Surgical or Medical Treatment |
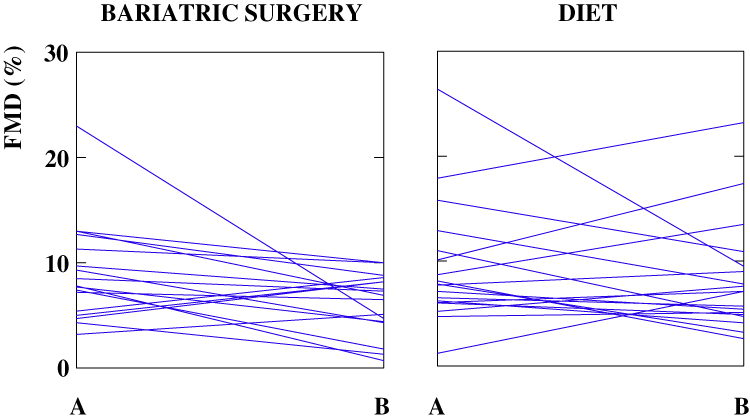 |
Figure 1 Endothelial function (FMD) before (A) and after (B) surgical or dietary treatment in each patient. |
 |
Figure 2 Correlation between the change of endothelial function (∆ FMD) and the change of carotid IMT (∆ c-IMT) in patients treated with bariatric surgery. |
Discussion
In this study, a significant endothelial dysfunction, measured as FMD, generally occurred following BS to treat obesity. On the contrary, the FMD in obese patients did not change after MNT. Furthermore, the decline of endothelial function that we observed in the BS group might have contributed to atherosclerosis, as suggested by the significant inverse correlation between the change of FMD and that of carotid IMT. Our results generally disagree with the few available data according to which endothelial function improves following BS,14 even though not sufficiently robust methods probably supported much of this evidence (Table 3). Williams et al observed a significant improvement in FMD following BS, but their study included only 8 patients undergoing GB, with a short-term follow-up of 6 months.24 Another study by Saleh et al reported that FMD improved considerably following GBP in 47 individuals;25 nevertheless, this study did not include a control group, the follow-up duration was just 10 months and the post-surgery FMD reached a very high value (18.9%) that is uncommon in clinical practice. Similar data were provided by Nerla et al who found that the FMD increased shortly after (3 months) surgical procedure.26 In agreement with previous studies, Tschoner et al reported that BS was associated with an improved FMD in 52 individuals 5 years after the surgical procedure (mostly GBP);27 however, no control group was included and the FMD was measured in a non-described subgroup of 36 patients. Bigornia et al demonstrated that FMD increased following weight loss but, unfortunately, they included both patients undergoing BS and MNT in the same cohort so that it was not possible to clearly demonstrate the efficacy of surgery.28 Interestingly, Tarzia et al recently demonstrated, in a cohort of obese individuals undergoing BS, that the improvement in FMD first observed at 3 months was maintained even after follow-up at 4 years;29 however, of the original sample of 50 patients, only 19 agreed to continue the long-term follow-up; thus, data regarding the remaining part of the cohort are missing. Furthermore, consistent with these results, three studies described a significant increase of FMD after the intervention.30–32 These findings are supported in part by a meta-analysis, performed including 8 studies (269 patients) and that demonstrated an improvement of FMD after surgical treatment.14 On the contrary, two studies investigating the role of BS in mediating the FMD response have not reported any change in follow-up at 1, 6 and 12 months after treatment.15,16 Furthermore, Flores et al observed no improvement in endothelial function in a cohort of 33 individuals with obesity undergoing BS.17
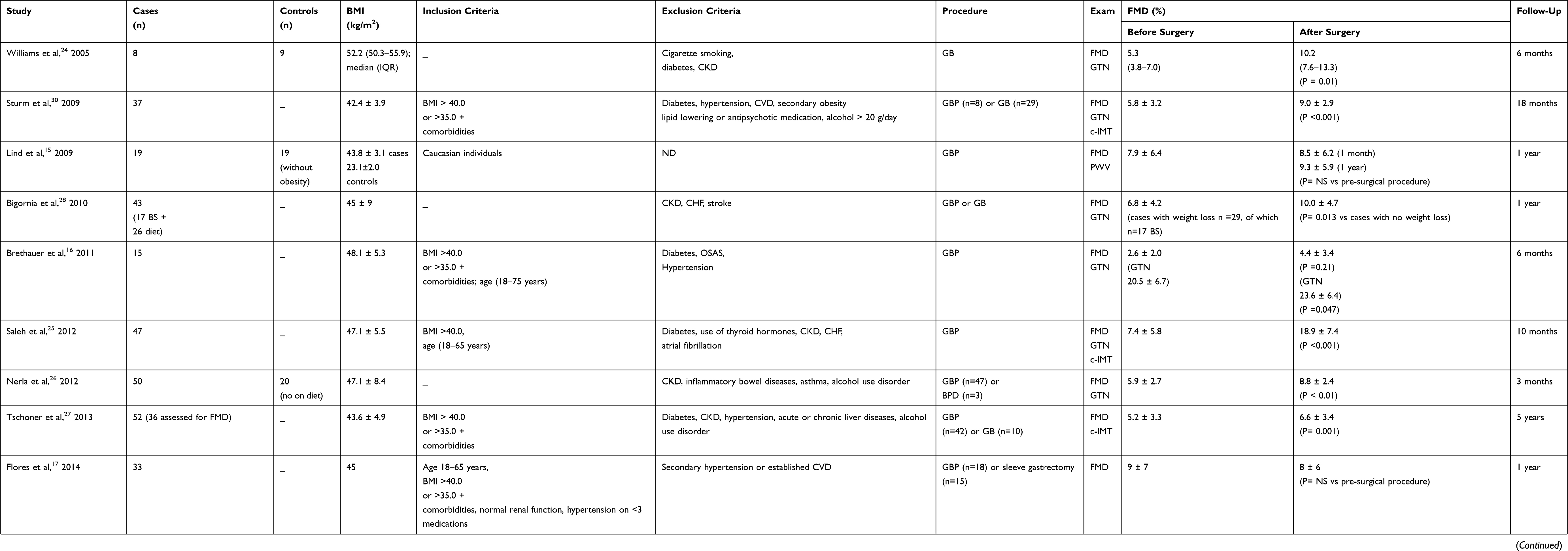 |
Table 3 Studies That Investigated Endothelial Function in Patients Treated with Bariatric Surgery |
Interestingly, there is no clear evidence that intentional weight loss with MNT in overweight or obese people is associated with a reduction in CV mortality risk.33 Surprisingly, some epidemiologic studies have paradoxically shown that weight loss is associated with an increased incidence of cardiovascular events,34 even in subjects who were overweight or obese at baseline.35,36 On the contrary, despite some methodological limitations, it has been demonstrated, especially from the Swedish cohort of the SOS study, that bariatric surgery is associated with a significant reduction in the risk of both CV events and mortality.37 Compromised endothelial function has been associated with unfavorable CV risk as well as with increased overall mortality risk.38 Therefore, our results seem to be in agreement with an increased health risk at least in the nearly 2-year period following the surgical treatment of obesity. Interestingly, it should be observed that in the SOS cohort the benefits of BS became evident about 6 years after surgery, while in the first months a small but significant increase in fatal CV events was observed compared to the control group. On the other hand, CV events are a consequence of progressive vascular disease that develops over time, so it seems plausible that removing obesity-related risk factors takes a few years before reducing CV risk. We do not have a clear explanation for our results. Dietary factors and antioxidants in particular might have an important role in endothelial function. Antioxidants are, in fact, key factors in countering reactive oxygen species whose activation reduces endothelial nitric oxide bioavailability39 and, therefore, normal endothelial function.40 Nutritional deficiencies occur quite frequently following BS,41 so, we cannot exclude that a paucity of micronutrients and antioxidants due either to reduced dietary intake or to post-surgery malabsorption may contribute to endothelial dysfunction. Should this be true, it would provide further evidence that nutritional deficiencies need to be promptly identified and treated after BS. In agreement with our results, a recent study observed that individuals undergoing GBP exhibited increased concentrations of several markers of both inflammation and oxidative stress even after 12 months of follow-up, in spite of vitamin supplementation.42 Similar results were reported by Dadalt et al who observed both a significant decrease in antioxidant concentrations and high levels of inflammatory markers after GBP; they were also able to demonstrate that these values began to improve 2 years after surgery.43 The average length of follow-up of the BS group was less than 2 years (16 months), so our findings may be due to a premature evaluation, before any improvement could be observed. Interestingly, the 4 cases of BS group in which we found improved FMD had a longer follow-up (18, 23, 23, 25 months). Furthermore, these 4 patients in whom endothelial function improved after BS underwent malabsorptive surgical procedures (2 GBP and 2 BPD). On the contrary, patients of the BS group that exhibited a decrease in FMD (n= 13) in most cases underwent GB (n= 9), a restrictive rather than malabsorptive procedure. Therefore, only about 30% of patients who did not obtain an improvement of endothelial function underwent a malabsorptive intervention. Despite the limited number of patients included in this study that do not allow subgroup analysis, our results might be at least in part explained by the fact that according to different studies endocrine, incretin-mediated effects characterize malabsorptive procedures and they probably induce favorable effects on endothelial function independently of weight loss.44 Even more recently, it was reported in rats and in man that Roux-en-Y gastric bypass reverses obesity-induced endothelial dysfunction via GLP-1–mediated weight-independent mechanisms.45 Unlike BS, MNT did not induce any change in FMD. Noteworthy, before undergoing the procedure, neither the BS nor MNT group exhibited endothelial dysfunction. In fact, the pre-treatment mean FMD could be considered in the normal range; therefore, it seems plausible that the beneficial effects of MNT on endothelial function occur when FMD is markedly impaired or with specific nutritional treatments.22
This study has some important limitations. First, the number of patients enrolled is too small and does not allow definitive conclusions. Second, the two study groups differed for some physical characteristics such as age and the degree of obesity, two well-known factors that may influence endothelial function. Furthermore, the individual length of follow-up varied greatly between participants and groups, it was shorter in the MNT group than in the BS group. Also, the BS group was too heterogeneous according to the different types of surgical procedures, and this was another possible confounding factor. Indeed, we did not record any indicator of habitual physical activity, a well-known factor that may potentially influence endothelial function. Finally, we did not measure other biomarkers of oxidative stress or inflammation, vitamins and antioxidant concentrations; their evaluation might have allowed an in-depth interpretation of results. However, our study has also some points of strength. The presence of a control group allowed considering specific aspects of BS. The procedure used to measure FMD is more reliable and accurate than those used in the majority of other studies on this subject in past years; furthermore, a single operator performed all measurements of FMD and this contributed to enhancing the reproducibility of the results. There are many potential confounders when measuring FMD. These include dieting before/after surgery. In addition, ketosis may acutely influence FMD and it may easily occur in patients with morbid obesity; the different measurement techniques (especially those used in past years) may have significant reproducibility problems and the change in arm diameter may allow better measurements after surgery. Our study has the merit of having standardized all these factors at the best of current possibilities. Furthermore, despite a certain heterogeneity regarding follow-up length, the mean duration was one of the longest in studies available in the literature.
Conclusion
Bariatric surgery is a safe and effective treatment for successful management of diabetes and obesity. However, there are still uncertainties about clinical outcomes that need to be fully elucidated. Indeed, medical complications could follow BS, even after a long time, that might be potentially harmful and may require adequate nutritional follow-up. Therefore, in order to attain a better understanding of BS implications, well-controlled trials, with follow-up longer than 5 years, to assess specific issues in groups of accurately enrolled homogeneous individuals are warranted.
Data Sharing Statement
The datasets analyzed in this study are available from the corresponding author Silvio Buscemi upon reasonable request.
Ethics Approval and Consent to Participate
The study protocol was approved by the institutional Ethics Committee (“Palermo 1” of the Policlinico “P. Giaccone” University Hospital) and each participant signed a written informed consent. This study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work. SB took also the general responsibility and supervised the study project.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–781. doi:10.1016/S0140-6736(14)60460-8
2. Buscemi S, Giordano C. Physical activity and cardiovascular prevention: is healthy urban living a possible reality or utopia? Eur J Intern Med. 2017;40:8–15. doi:10.1016/j.ejim.2017.02.007
3. Flegal KM, Graubard BI, Williamson DF, et al. Cause-specific excess deaths associated with underweight overweight, and obesity. JAMA. 2007;298:2028–2037. doi:10.1001/jama.298.17.2028
4. Taylor VH, Forhan M, Vigod SN, et al. The impact of obesity on quality of life. Best Pract Res Clin Endocrinol Metab. 2013;27:139–146. doi:10.1016/j.beem.2013.04.004
5. Gregg EW, Cheng YJ, Cadwell BL, et al. Secular trends in cardiovascular disease risk factors according to body mass index in US adults. JAMA. 2005;293:1868–1874. doi:10.1001/jama.293.15.1868
6. Seidell JC, Halberstadt J. The global burden of obesity and the challenges of prevention. Ann Nutr Metab. 2015;66(S2):7–12. doi:10.1159/000375143
7. Buscemi S, Batsis JA, Verga S, et al. Long-term effects of a multidisciplinary treatment of uncomplicated obesity on carotid intima-media thickness. Obesity. 2011;19:1187–1192. doi:10.1038/oby.2010.313
8. Sjöström L, Lindroos AK, Peltonen M, et al.; Swedish Obese Subjects Study Scientific Group. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683–2693. doi:10.1056/NEJMoa035622
9. Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric surgery versus conventional medical therapy for type 2 diabetes. N Engl J Med. 2012;366:1577–1585. doi:10.1056/NEJMoa1200111
10. Deanfield JE, Halcox JP, Rabelink TJ. Endothelial function and dysfunction: testing and clinical relevance. Circulation. 2007;115:1285–1295. doi:10.1161/CIRCULATIONAHA.106.652859
11. Davignon J, Ganz P. Role of endothelial dysfunction in atherosclerosis. Circulation. 2004;109(S1):1127–1132. doi:10.1161/01.CIR.0000131515.03336.f8
12. Thijssen DH, Black MA, Pyke KE, et al. Assessment of flow-mediated dilation in humans: a methodological and physiological guideline. Am J Physiol Heart Circ Physiol. 2011;300:2–12. doi:10.1152/ajpheart.00471.2010
13. Maruhashi T, Soga J, Fujimura N, et al. Endothelial dysfunction, increased arterial stiffness, and cardiovascular risk prediction in patients with coronary artery disease: FMD-J (Flow-Mediated Dilation Japan) Study A. J Am Heart Assoc. 2018;7:e008588. doi:10.1161/JAHA.118.008588
14. Lupoli R, Di Minno MN, Guidone C, et al. Effects of bariatric surgery on markers of subclinical atherosclerosis and endothelial function: a meta-analysis of literature studies. Int J Obes. 2015;40:395–402. doi:10.1038/ijo.2015.187
15. Lind L, Zethelius B, Sundbom M, et al. Vasoreactivity is rapidly improved in obese subjects after gastric bypass surgery. Int J Obes. 2009;33:1390–1395. doi:10.1038/ijo.2009.188
16. Brethauer SA, Heneghan HM, Eldar S, et al. Early effects of gastric bypass on endothelial function, inflammation, and cardiovascular risk in obese patients. Surg Endosc. 2011;25:2650–2659. doi:10.1007/s00464-011-1620-6
17. Flores L, Núñez I, Vidal J, et al. Endothelial function in hypertensive obese patients: 1 year after surgically induced weight loss. Obes Surg. 2014;24:1581–1584. doi:10.1007/s11695-014-1328-5
18. Available from: http://www.sicob.org/chirurgia/premessa.aspx.
19. Buscemi S, Blunda G, Maneri R, et al. Bioelectrical characteristics of type 1 and type 2 diabetic subjects with reference to body water compartments. Acta Diabetol. 1998;35:220–223. doi:10.1007/s005920050135
20. Buscemi S, Geraci G, Massenti FM, et al. Renal function and carotid atherosclerosis in adults with no known kidney disease. Nutr Metab Cardiovasc Dis. 2017;27:267–273. doi:10.1016/j.numecd.2016.09.013
21. Touboul PJ, Hennerici MG, Meairs S, et al. Mannheim carotid intima-media thickness and plaque consensus (2004-2006-2011). An update on behalf of the advisory board of the 3rd, 4th and 5th watching the risk symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany B. Cerebrovasc Dis. 2004;2012:290e6.
22. Buscemi S, Verga S, Tranchina MR, et al. Effects of hypocaloric very-low-carbohydrate diet vs. Mediterranean diet on endothelial function in obese women. Eur J Clin Invest. 2009;39:339–347. doi:10.1111/j.1365-2362.2009.02091.x
23. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499–502. doi:10.1093/clinchem/18.6.499
24. Williams IL, Chowienczyk PJ, Wheatcroft SB, et al. Endothelial function and weight loss in obese humans. Obes Surg. 2005;15:1055–1060. doi:10.1381/0960892054621134
25. Saleh MH, Bertolami MC, Assef JE, et al. Improvement of atherosclerotic markers in non-diabetic patients after bariatric surgery. Obes Surg. 2012;22:1701–1707. doi:10.1007/s11695-012-0706-0
26. Nerla R, Tarzia P, Sestito A, et al. Effect of bariatric surgery on peripheral flow-mediated dilation and coronary microvascular function. Nutr Metab Cardiovasc Dis. 2012;22:626–634. doi:10.1016/j.numecd.2010.10.004
27. Tschoner A, Sturm W, Gelsinger C, et al. Long-term effects of weight loss after bariatric surgery on functional and structural markers of atherosclerosis. Obesity. 2013;21:1960–1965. doi:10.1002/oby.20357
28. Bigornia SJ, Mott MM, Hess DT, et al. Long-term successful weight loss improves vascular endothelial function in severely obese individuals. Obesity. 2010;18:754–759. doi:10.1038/oby.2009.482
29. Tarzia P, Lanza GA, Sestito A, et al. Long-term effects of bariatric surgery on peripheral endothelial function and coronary microvascular function. Obes Res Clin Pract. 2017;11:114–117. doi:10.1016/j.orcp.2016.12.005
30. Sturm W, Tschoner A, Engl J, et al. Effect of bariatric surgery on both functional and structural measures of premature atherosclerosis. Eur Heart J. 2009;30:2038–2043. doi:10.1093/eurheartj/ehp211
31. Tromba L, Tartaglia F, Carbotta S, et al. The role of sleeve gastrectomy in reducing cardiovascular risk. Obes Surg. 2017;27:1145–1151. doi:10.1007/s11695-016-2441-4
32. de Assunção Machado AC, da Silva AMV, Signori LU, et al. Endothelial function of patients with morbid obesity submitted to Roux-en-Y gastric bypass with and without obstructive sleep apnea-hypopnea syndrome. Obes Surg. 2018;28:3595–3603. doi:10.1007/s11695-018-3403-9
33. Williamson DF, Thompson TJ, Thun M, et al. Intentional weight loss and mortality among overweight individuals with diabetes. Diabetes Care. 2000;23:1499–1504. doi:10.2337/diacare.23.10.1499
34. Nilsson PM, Nilsson JA, Hedblad B, et al. The enigma of increased non-cancer mortality after weight loss in healthy men who are overweight or obese. J Intern Med. 2002;252:70–78. doi:10.1046/j.1365-2796.2002.01010.x
35. Pamuk ER, Williamson DF, Serdula MK, et al. Weight loss and subsequent death in a cohort of U.S. Adults Ann Intern Med. 1993;119:744–748. doi:10.7326/0003-4819-119-7_Part_2-199310011-00023
36. Nissen SE, Nicholls SJ, Wolski K, et al. Effect of rimonabant on progression of atherosclerosis in patients with abdominal obesity and coronary artery disease: the STRADIVARIUS randomized controlled trial. JAMA. 2008;299:1547–1560. doi:10.1001/jama.299.13.1547
37. Sjöström L, Narbro K, Sjöström CD, et al.; Swedish Obese Subjects Study. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357:741–752. doi:10.1056/NEJMoa066254
38. Matsuzawa Y, Kwon TG, Lennon RJ, et al. Prognostic value of flow-mediated vasodilation in brachial artery and fingertip artery for cardiovascular events: a systematic review and meta-analysis. J Am Heart Assoc. 2015;4:e002270. doi:10.1161/JAHA.115.002270;.
39. Hsieh HJ, Liu CA, Huang B, et al. Shear-induced endothelial mechanotransduction: the interplay between reactive oxygen species (ROS) and nitric oxide (NO) and the pathophysiological implications. J Biomed Sci. 2014;21:3. doi:10.1186/1423-0127-21-3
40. Stamler JS, Singel DJ, Loscalzo J. Biochemistry of nitric oxide and its redox-activated forms. Science. 1992;258:1898–1902. doi:10.1126/science.1281928
41. Shankar P, Boylan M, Sriram K. Micronutrient deficiencies after bariatric surgery. Nutrition. 2010;26:1031–1037. doi:10.1016/j.nut.2009.12.003
42. da Silva VR, Moreira EA, Wilhelm-Filho D, et al. Proinflammatory and oxidative stress markers in patients submitted to Roux-en-Y gastric bypass after 1 year of follow-up. Eur J Clin Nutr. 2012;66:891–899. doi:10.1038/ejcn.2012.17
43. Dadalt C, Fagundes RL, Moreira EA, et al. Oxidative stress markers in adults 2 years after Roux-en-Y gastric bypass. Eur J Gastroenterol Hepatol. 2013;25:580–586. doi:10.1097/MEG.0b013e32835d0ae0
44. Salinari S, Bertuzzi A, Asnaghi S, et al. First phase insulin secretion restoration and differential response to glucose load depending on the route of administration in type 2 diabetic subjects after bariatric surgery. Diabetes Care. 2009;32:375–380. doi:10.2337/dc08-1314
45. Osto E, Doytcheva P, Corteville C, et al. Rapid and body weight–independent improvement of endothelial and high-density lipoprotein function after Roux-en-Y gastric bypass. Role of Glucagon-Like Peptide-1. Circulation. 2015;131:871–881. doi:10.1161/CIRCULATIONAHA.114.011791
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.