Back to Journals » Clinical Ophthalmology » Volume 16
Endophthalmitis, Visual Outcomes, and Management Strategies in Eyes with Intraocular Foreign Bodies
Authors Keil JM ![]() , Zhao PY, Durrani AF
, Zhao PY, Durrani AF ![]() , Azzouz L, Huvard MJ, Dedania VS, Zacks DN
, Azzouz L, Huvard MJ, Dedania VS, Zacks DN
Received 12 January 2022
Accepted for publication 24 March 2022
Published 3 May 2022 Volume 2022:16 Pages 1401—1411
DOI https://doi.org/10.2147/OPTH.S358064
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jason M Keil,1 Peter Y Zhao,1 Asad F Durrani,1 Lyna Azzouz,1 Michael J Huvard,1 Vaidehi S Dedania,2 David N Zacks1
1Kellogg Eye Center, Department of Ophthalmology and Visual Sciences, University of Michigan, Ann Arbor, MI, USA; 2Department of Ophthalmology, New York University Langone Health, New York University School of Medicine, New York, NY, USA
Correspondence: David N Zacks, Email [email protected]
Purpose: Ocular trauma with intraocular foreign body (IOFB) can have devastating visual consequences. Management and antimicrobial strategies remain variable due to the infrequency and heterogeneity of presentation. Our goal was to identify risk factors for endophthalmitis and poor visual outcomes in cases of IOFB and investigate management strategies.
Patients and Methods: A retrospective chart review was conducted in 88 eyes of 88 patients suffering traumatic injury with IOFB at the University of Michigan between January 2000 and December 2019. Medical records were reviewed to characterize the injuries and IOFBs as well as how clinical presentation and treatment modalities were associated with outcomes.
Results: Delayed presentation (P=0.016) and organic IOFB (P=0.044) were associated with development of endophthalmitis. Retinal detachment (P=0.012), wound length greater than 5 mm (P=0.041), and poor presenting visual acuity (P=0.003) correlated with poor final visual outcome. Antibiotic prophylaxis was given to all patients, though agents and routes of delivery varied. Endophthalmitis developed in 4.9% of the eyes after initial management, with primary and secondary removal of posterior segment IOFBs associated with similar rates of endophthalmitis (P=1.000).
Conclusion: Poor presenting visual acuity and severity of injury, as measured by large wound and retinal detachment, correlate with poor visual outcome. Prompt globe closure and antimicrobial prophylaxis are critical for infection prevention. In cases where IOFB removal and globe closure cannot be performed concurrently, primary globe closure with aggressive antibiotic prophylaxis offers a reasonable alternative to prevent endophthalmitis.
Keywords: retina, trauma, vitreous, IOFB
Introduction
Open globe injuries with intraocular foreign body (IOFB) can have severe visual consequences. IOFBs cause vision loss through multiple mechanisms including direct mechanical trauma, hemorrhage, inflammation and toxicity from the foreign body, or retinal detachment (RD). One feared and visually devastating complication is endophthalmitis. Entry wounds allow communication between intraocular and external environments, and foreign bodies may seed the eye with microbes. Most studies with retained IOFB injuries found endophthalmitis in 5–17% of cases,1 though rates between 0% and 48% have been reported.2,3 Risk factors include age,4 IOFB in the posterior segment,5 vegetable composition6 or contaminated IOFB,7,8 and delayed globe repair.1,4 Despite these known risk factors and ability to stratify patients by presentation and IOFB characteristics, management strategies remain controversial. Some investigators report low endophthalmitis rates with prompt primary removal of IOFBs during globe closure,9 while others found low rates with early globe closure and delayed secondary IOFB removal.2 Additionally, most practitioners advocate for prompt antimicrobial therapy, though specific agents and routes of delivery vary between institutions and specific trauma scenarios.
Post-traumatic endophthalmitis following IOFB injury necessitates further intervention and is associated with poor visual outcome.10 Therefore, understanding risk factors that predispose to infection and identifying optimal surgical interventions and antimicrobial prophylaxis strategies can decrease vision loss in patients suffering eye trauma. While prospective studies are difficult and costly to conduct due to relative infrequency and heterogeneity, retrospective analyses may identify additional risk factors and treatment strategies that correlate with effective prophylaxis. This study sought to characterize open globe injuries with retained IOFBs that presented to University of Michigan over nearly two decades and analyze factors on presentation and during management that predisposed to endophthalmitis and poor final acuity.
Materials and Methods
Data Collection
We conducted retrospective chart review of open globe injuries with retained IOFBs presenting to the University of Michigan between January 2000 and December 2019. Study protocol was approved by the Institutional Review Board of University of Michigan Medical School, was compliant with the Health Insurance Portability and Accountability Act (HIPAA), and adhered to the Declaration of Helsinki. Informed consent of patients was not required per the Institutional Review Board. Patients were excluded if follow-up was less than 30 days, in cases of primary enucleation, or if secondary enucleation occurred within 30 days without endophthalmitis. Standard open globe care with suspected IOFB included prompt evaluation by the on-call ophthalmology resident with immediate eye shield placement upon confirmation, CT scan with thin orbital slices, tetanus prophylaxis if indicated, coordination with additional teams for other injuries, and urgent globe closure. Intravenous (IV) medications for pain and nausea were administered as needed while awaiting surgical intervention. Strategy for IOFB removal was dictated by the on-call trauma surgeon in coordination with the on-call vitreoretinal surgeon if the IOFB was in the posterior segment. Generally, anterior segment IOFBs were removed during primary closure, while posterior segment IOFBs were removed by either pars plana vitrectomy (PPV) at time of globe closure, or deferred secondary PPV. The routes and antibiotics for endophthalmitis prophylaxis were determined in coordination with other care teams, in context of antibiotics administered prior to globe closure. Intravitreal antimicrobial prophylaxis was considered on an individual basis by on-call trauma and vitreoretinal surgeons depending on injury, IOFB composition, timing, and other infection risk factors. Medical records were reviewed to characterize the injury, IOFB, clinical examination, timing of injury and interventions, surgical procedures, antibiotics, endophthalmitis, and visual acuity measurements. Acuity was converted to logarithm of the minimum angle of resolution (logMAR) scale and counting fingers (CF), hand motion (HM), light perception (LP), and no light perception (NLP) were recoded to logMAR 2.0, 2.3, 2.7, and 3.0, respectively.11 Final visual acuity reflects acuity measured at most recent follow-up appointment. In endophthalmitis cases, microbiological characteristics and additional interventions were noted.
Statistical Analysis
Statistical analysis was performed using R (The R Foundation, Vienna, Austria). Multivariate logistic regression was used to correlate clinical outcomes to features on initial presentation. We examined clinical outcomes of endophthalmitis, good final acuity (corrected acuity 20/40 or better), and poor final acuity (corrected acuity 20/200 or worse). Unpaired t-tests were used to compare continuous variables and Fisher’s exact tests were used to compare categorical variables. Tests of statistical significance were two-tailed and p-values less than 0.05 were considered statistically significant.
Results
Study Cohort
We identified 100 eyes with open globe injuries involving retained IOFBs. Twelve eyes were excluded: six had inadequate follow-up, one required primary enucleation, and five required secondary enucleation within 30 days. Therefore, 88 eyes of 88 patients were included (Table 1). Patients were predominantly male (84:4, 95.5%) with mean age 34.4 years (SD=17.0), and 16/88 (18.2%) presented more than 24 hours after injury. Patients had a wide spectrum of presenting visual acuity with mean logMAR 1.25 (SD=1.04, Snellen equivalent 20/356). Of the 88 eyes, 35 (39.8%) were CF or worse, and five eyes were unable to be tested (5/88, 5.7%). Six patients had endophthalmitis at presentation (6/88, 6.8%), while an additional four of the remaining 82 eyes (4/82, 4.9%) developed endophthalmitis after medical and surgical management. Four eyes were enucleated within this cohort. Three eyes that developed endophthalmitis were enucleated. One eye was enucleated 90 days after presentation, with no evidence of endophthalmitis during treatment course or at time of enucleation.
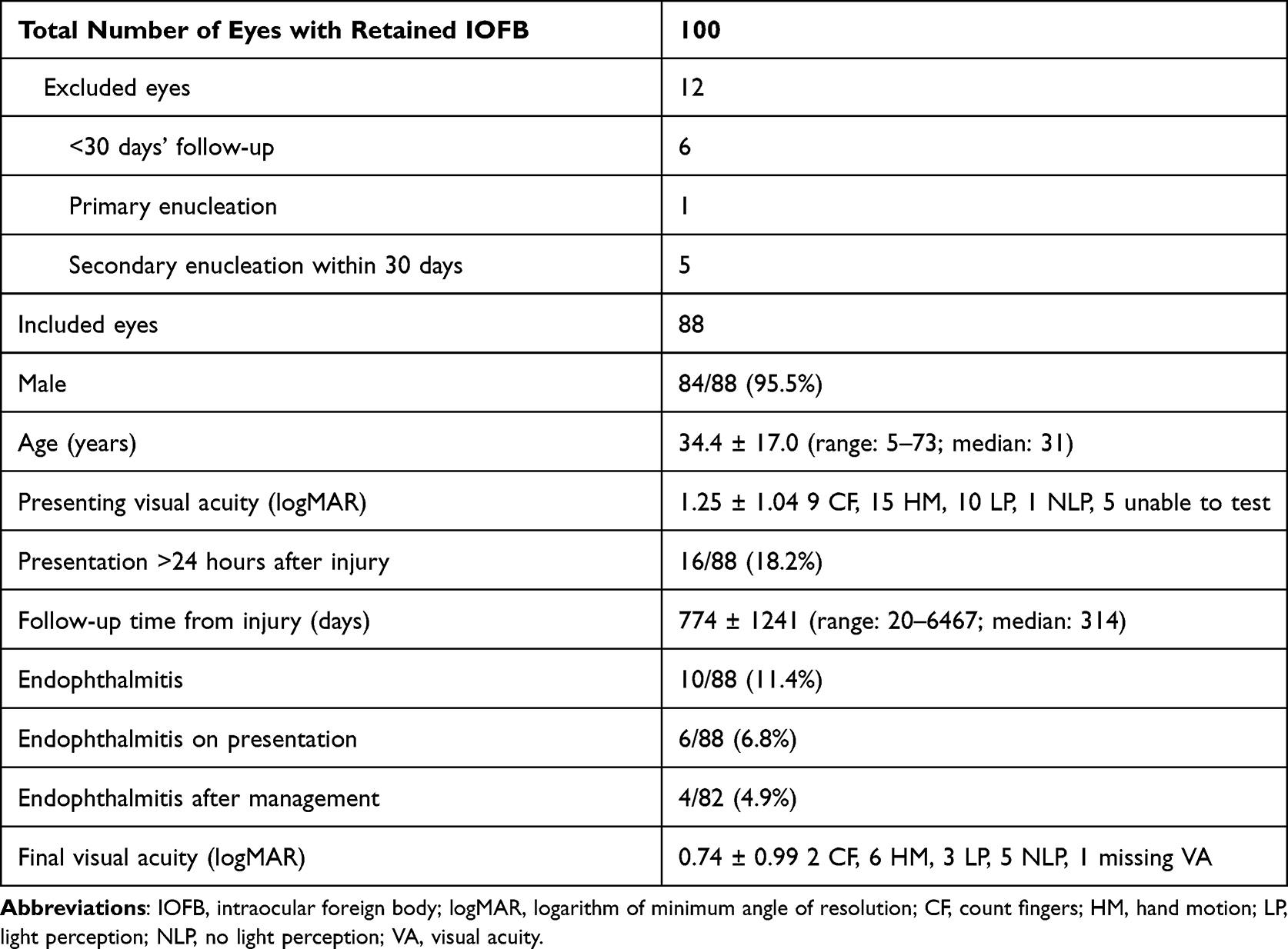 |
Table 1 Summary of Demographics and Clinical Presentation of Eyes Suffering Trauma with IOFB |
IOFB Characteristics
IOFB injuries varied in nature and velocity, entrance wound location and size, and ocular structures affected. Most IOFBs (59/88, 67.0%) entered through Zone 1,12 and a majority (60/88, 68.2%) were found in the posterior segment (Table 2). Consistent with other studies, the majority of IOFBs were metallic (71/88, 80.7%). 20/88 eyes (20.7%) suffered an entrance wound >5 mm. Anterior and posterior segment injuries were common including disruption of the lens capsule (50/88, 56.8%), vitreous hemorrhage (42/88, 47.7%), retinal tears (36/88, 40.9%), and retinal detachment (25/88, 28.4%).
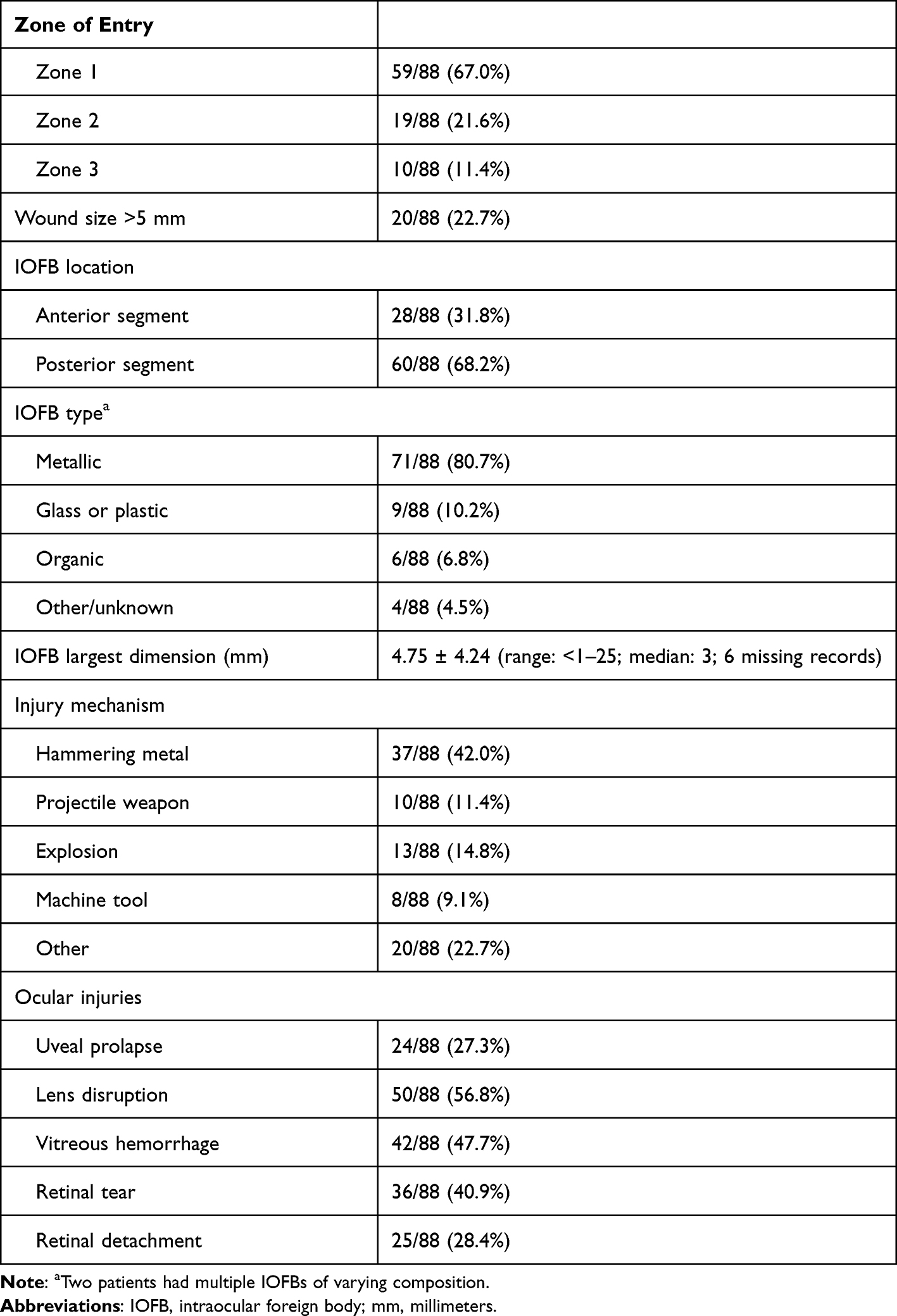 |
Table 2 IOFB Characteristics and Patterns of Injury in 88 Studied Eyes |
Globe Closure and IOFB Removal
Of the 88 eyes, 53 (60.2%) were closed primarily with concurrent IOFB removal, while 34 eyes (38.6%) underwent separate surgeries for globe closure and subsequent IOFB removal (Table 3). IOFBs were removed via an anterior approach at globe closure in 25/88 eyes (28.4%) and in 3/88 eyes (3.4%) in secondary fashion. PPV-facilitated IOFB removal was performed primarily in 28/88 eyes (31.8%) and in 31/88 eyes (35.2%) that underwent secondary IOFB removal. 1/88 eyes (1.1%) had a retained IOFB that was never removed after primary globe closure.
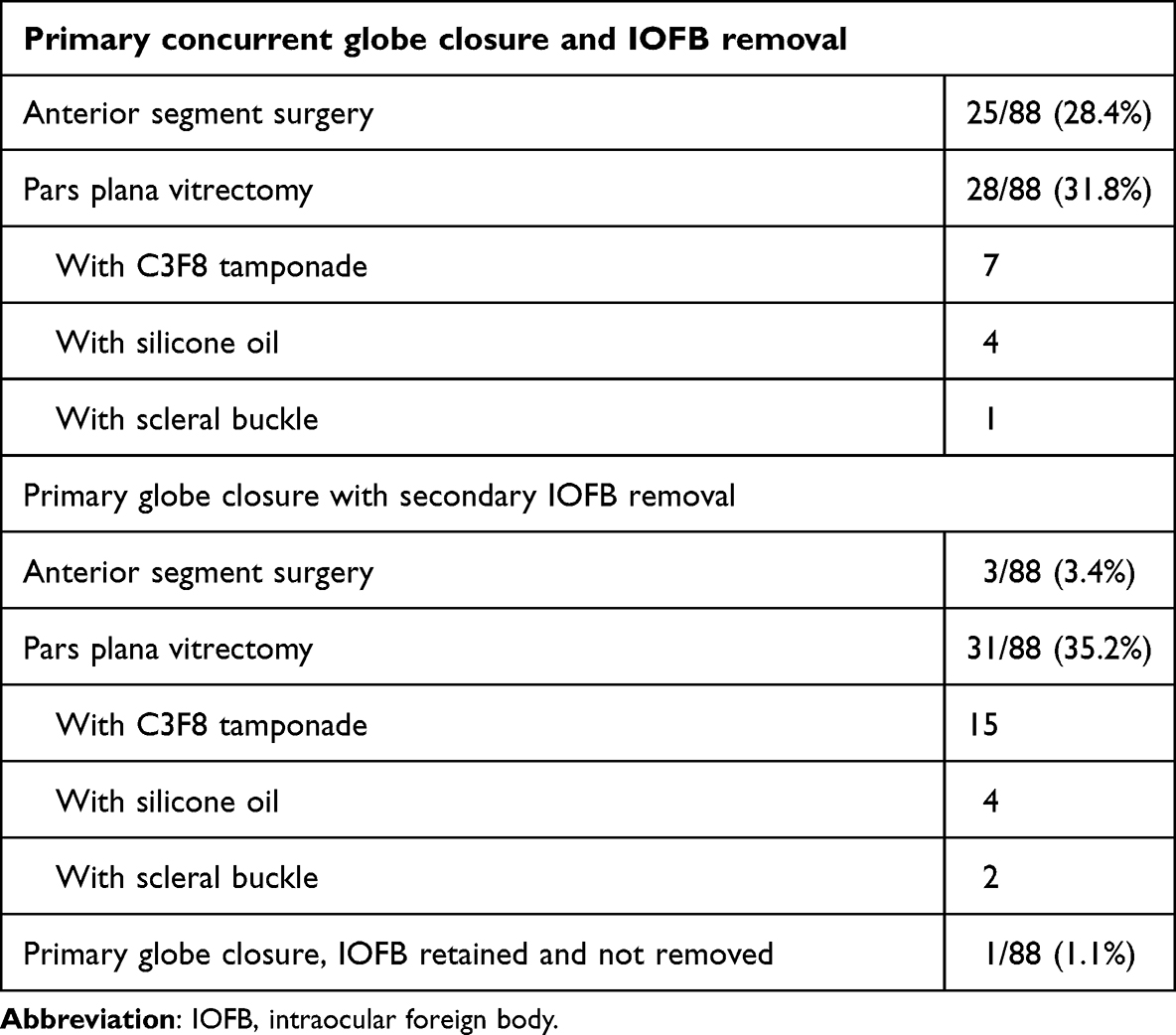 |
Table 3 Timing and Type of Surgical Interventions in 88 Studied Eyes |
Factors Associated with Endophthalmitis and Visual Recovery
Ten of 88 eyes (10/88, 11.4%) developed endophthalmitis. Of these 10 patients, 6 were diagnosed at initial presentation, all which presented >48 hours after initial injury. These six eyes (five with posterior segment IOFBs, one with anterior segment IOFB) were included in analyses of factors associated with endophthalmitis and visual outcome but excluded from analyses of endophthalmitis prophylaxis. Four of the remaining 82 eyes (4/82, 4.9%) developed endophthalmitis after initial management. Of 10 total endophthalmitis patients, 2 had anterior segment (2/10, 20%) and 8 had posterior segment IOFBs (8/10, 80%). Four patients had microbiological evidence of endophthalmitis by gram stain or culture (4/10, 40%), two patients had culture-negative endophthalmitis (2/10, 20%), and four patients had no data available or unsuccessful vitreous taps (4/10, 40%). Final acuity in this group varied widely (mean logMAR 1.67 [Snellen equivalent 20/935], SD 1.36, range: 20/25-NLP) and three patients required enucleation.
Regression analyses demonstrated that organic IOFB and delayed presentation (>24 hours after injury) were positively correlated with endophthalmitis (Figure 1A). We did not find significant association between age, posterior segment IOFB, wound length >5 mm, or severe anterior segment damage (concurrent corneal laceration, uveal prolapse, and lens disruption) and endophthalmitis. Good acuity was associated with absence of retinal detachment, while poor visual outcome was associated with poor presenting acuity, wound length >5 mm, and retinal detachment at presentation identified by clinical examination, B-scan, or during PPV. This cohort demonstrated correlation (Pearson’s R = 0.58) between presenting and final visual acuity (Figure 1B), with 48/88 eyes (54.5%) final visual acuity better compared to presentation. Acuity significantly improved (p=0.0011) from logMAR 1.25 (Snellen equivalent 20/356, SD 1.04) to 0.74 (Snellen equivalent 20/110, SD 0.99). 50/88 eyes (56.8%) achieved good final visual acuity (20/40 or better) while 30/88 eyes (34.1%) had poor final visual acuity (20/200 or worse).
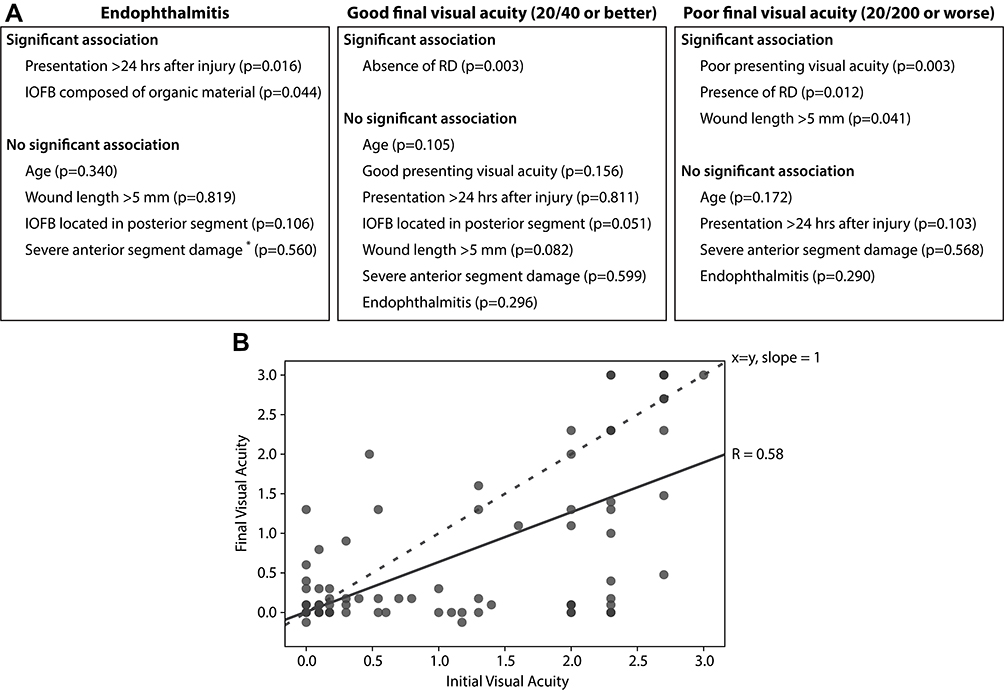 |
Figure 1 Regression analysis of factors associated with endophthalmitis and good or poor final visual acuity. (A) Factors associated with endophthalmitis development and final visual acuity. p < 0.05 significant. *Severe anterior segment damage defined as concurrent corneal laceration, uveal prolapse, and lens disruption. (B) Initial and final visual acuity of eyes presenting with IOFBs, with dashed line slope=1 and continuous trendline demonstrating Pearson’s correlation coefficient (R = 0.58). Points below the dashed line demonstrate eyes with improved visual acuity compared to presentation. |
Primary versus Secondary Removal of Posterior Segment IOFBs
To further define risk factors for endophthalmitis, sub-group analysis of posterior segment IOFBs was conducted, comparing eyes closed primarily with concurrent PPV versus primary closure and secondary deferred PPV for IOFB removal. This analysis excluded six eyes with posterior segment IOFBs from the initial dataset. Five eyes were excluded due to endophthalmitis on initial presentation and one eye had a retained IOFB that was never removed. The remaining 54 eyes presented without signs of infection and enabled subgroup analysis of primary versus deferred IOFB removal. Eyes that underwent primary closure and IOFB removal (n=25) presented with logMAR acuity 0.86 (Snellen equivalent 20/145, SD=1.01), 13/25 (52.0%) had retinal tears, and 7/25 (28.0%) had retinal detachments (Table 4). Eyes that underwent secondary IOFB removal (n=29) presented with logMAR acuity 1.65 (Snellen equivalent 20/893, SD=0.91), 21/29 (72.4%) had retinal tears, and 15/29 (51.7%) had retinal detachments. While presenting visual acuity was significantly different between these groups (p=0.0039), retinal tears (p=0.16) and retinal detachments (p=0.10) were not. Eyes undergoing secondary IOFB removal were usually (25/29, 86.2%) treated with intravitreal antibiotics at globe closure, compared to 9/25 (36.0%) primary IOFB removal eyes. Rates of endophthalmitis (primary, 1/25 [4.0%] vs secondary, 2/29 [6.9%], p=1.00) and enucleation (primary, 2/25 [8.0%] vs secondary, 1/29 [3.4%], p=0.59) were similar between groups. Secondary IOFB removal eyes trended towards higher rates of proliferative vitreoretinopathy (PVR) (secondary, 6/29 [20.7%] vs primary, 1/25 [4.0%], p=0.11), though were not statistically different from eyes undergoing primary IOFB removal. Visual acuity trended toward improvement in both but neither differed significantly (primary-logMAR 0.86 to 0.67; SD=0.98, p=0.19, secondary-logMAR 1.65 to 1.22, SD=1.08, p=0.11).
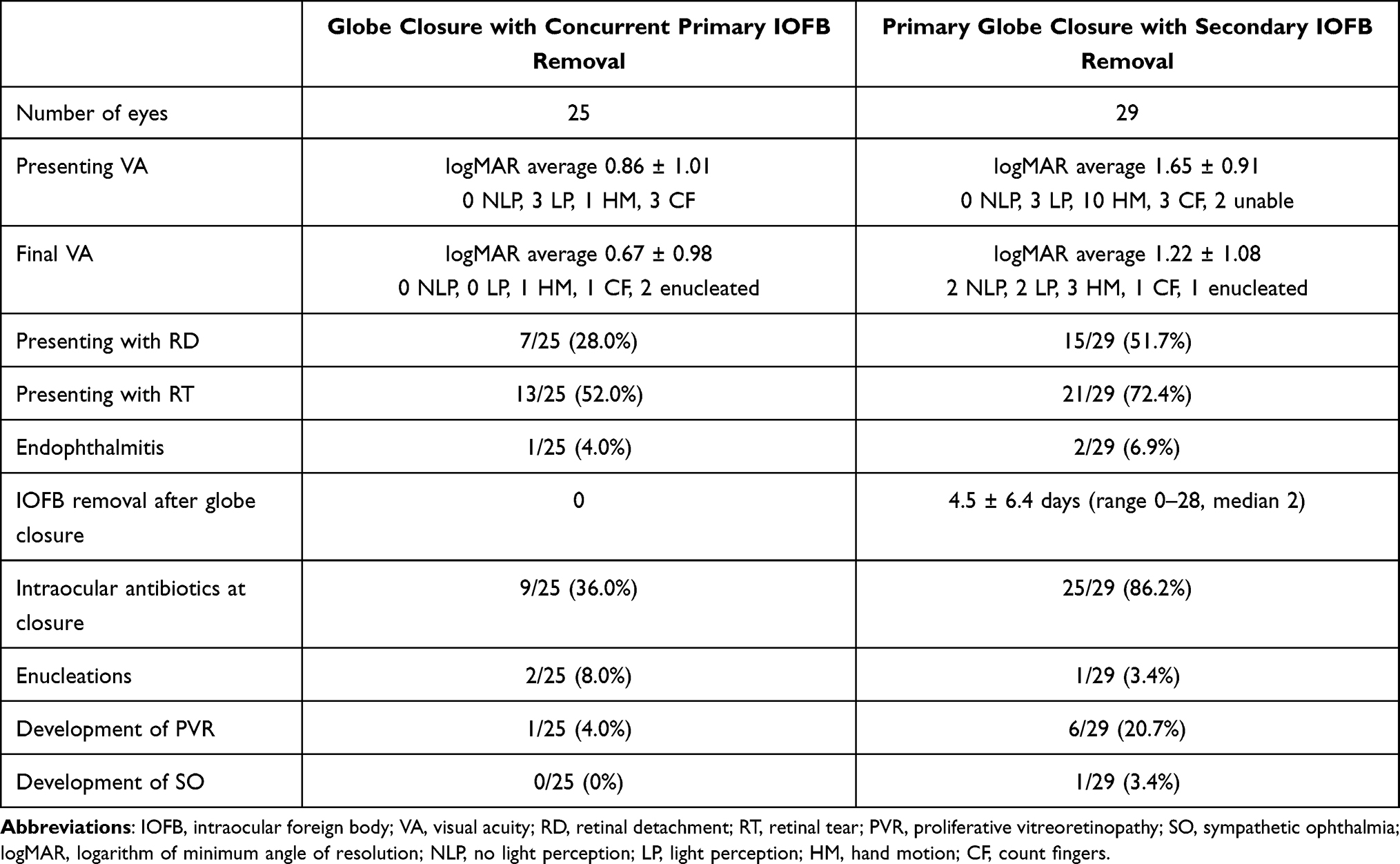 |
Table 4 Primary and Secondary Removal of Posterior Segment IOFBs Including Presenting Characteristics, Treatments, and Outcomes |
Secondary IOFB removal eyes underwent delayed PPV a median 2 days after presentation (mean 4.5, SD 6.4, range 0–28). The majority had PPV and IOFB removal in the same day or within the first 5 days after globe closure (Figure 2). Most commonly, patients underwent globe closure and were seen early the next day in retina clinic to rapidly schedule subsequent PPV and IOFB removal. Further delays were seen in cases of severe corneal edema, complex cases necessitating multiple sub-specialties, severe multi-faceted trauma injuries, blast injuries, or difficult surgeries where IOFB removal was attempted but not possible during initial intervention.
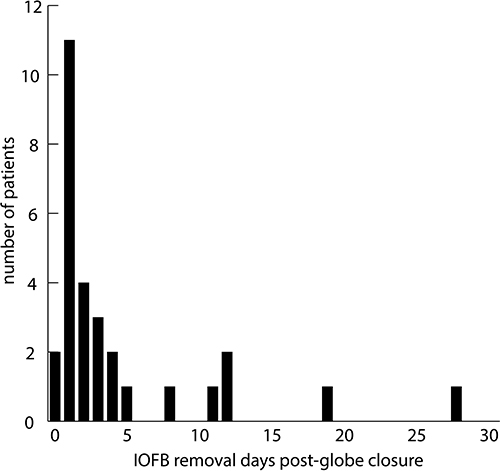 |
Figure 2 Days elapsed between initial globe closure and deferred IOFB removal by PPV. |
Antimicrobial Prophylaxis
All patients received antimicrobial prophylaxis. 71/88 (80.7%) received systemic antibiotics (Figure 3) by IV or per os (PO). 42/88 (47.7%) received a single antibiotic, 29/88 (33.0%) received multiple agents. 46/88 patients (52.3%) received a fluoroquinolone agent, 15/88 (17.0%) received a penicillin or cephalosporin alone, and 29/88 (33.0%) received combination therapy. Most commonly, patients received IV antibiotics at initial presentation and surgical intervention with transition to outpatient PO antibiotics. Forty-four of 88 patients (50.0%) received intravitreal antibiotics, most often vancomycin and ceftazidime, though a few patients received amikacin, cefazolin, or cefuroxime. Intravitreal antibiotics were given in 86.2% of the cases where primary globe closure was completed with a retained IOFB intended for secondary removal, though 36.0% of the cases with concurrent primary closure and IOFB removal received intravitreal antibiotics. A small percentage of eyes (5.0%) received intravitreal voriconazole for antifungal prophylaxis, generally in the presence of contaminated wound or suspected dirty IOFB.
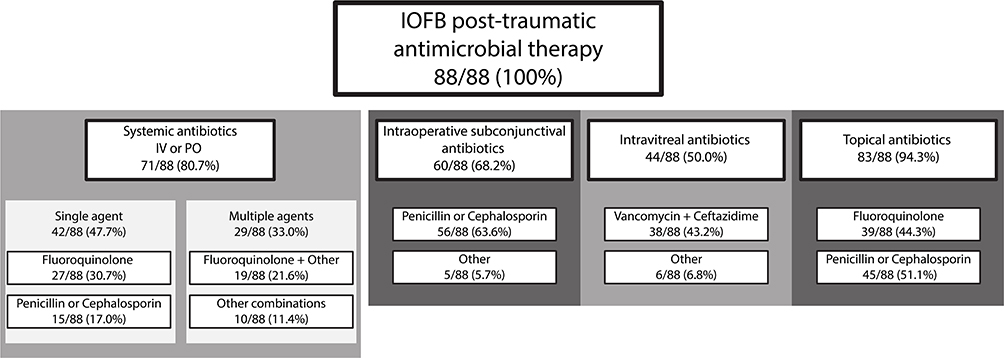 |
Figure 3 Antimicrobial treatment by agent class and route of delivery in patients with IOFBs. |
Endophthalmitis Cases
Four patients developed endophthalmitis after initial intervention. Case 1 was a 39-year-old male patient who presented with a large IOFB and complete RD with giant retinal tears after a fiberglass grinding wheel exploded. The patient was LP on presentation, was treated with multiple doses of IV cefazolin and primary closure of the anterior wound with concurrent PPV-mediated removal of the IOFB with silicone oil tamponade. Despite prompt removal and IV antibiotic therapy, the patient developed endophthalmitis on POD1 due to Bacillus cereus, which necessitated enucleation. Case 2 was a 20-year-old male patient who suffered eye trauma while removing wooden house siding, with RD and giant retinal tears, who was HM on presentation. A wood IOFB was not ascertained during initial exam or globe closure, and was first seen on outpatient B-scan. Despite oral levofloxacin therapy after globe closure, the patient developed endophthalmitis on POD7. This patient was treated with intravitreal vancomycin, ceftazidime, and voriconazole injection with IOFB removal by PPV. Vision remained HM at most recent evaluation. Case 3 was a 23-year-old male patient who presented with a small metallic IOFB in the anterior chamber with traumatic cataract after metal-on-metal hammering. Acuity was HM on presentation and the anterior chamber IOFB was removed primarily at time of globe closure. The patient was treated with IV cefazolin and oral levofloxacin for 7 days, and presented with culture-negative endophthalmitis 49 days after injury. Vitreous tap culture did not yield an organism and the patient most recently had excellent visual recovery to 20/30. Case 4 was an 11-year-old male patient who sustained a corneal laceration with metallic IOFB while hammering a debris pile. On presentation, the patient’s vision was HM and the globe was promptly closed. He was treated with IV levofloxacin, intravitreal vancomycin and ceftazidime injection, and discharged on oral levofloxacin with plans for follow-up removal of IOFB by PPV. On POD2, the patient had worsening exam and clinical findings suggestive of endophthalmitis. PPV enabled IOFB removal (metallic IOFB and intraocular cilia), with cultures later growing Clostridium bifermentans. The patient developed RD and closed-angle glaucoma in a blind, painful eye and was therefore enucleated on POD60. The patient additionally developed sympathetic ophthalmia in the contralateral eye. Although these represent a small number of cases, regression analysis found no association between endophthalmitis and systemic fluoroquinolone therapy (endophthalmitis 6/10 [60%], Others 36/78 [46.2%], p=0.546), intravitreal antibiotics (endophthalmitis 6/10 [60%], Others 38/78 [48.7%], p=0.534), or primary globe closure with concurrent IOFB removal (endophthalmitis 6/10 [60%], Others 47/78 [60.3%], p=0.731).
Discussion
This cohort collected over nearly two decades largely mirrored the demographics of other studies, demonstrating that working-age males are at highest risk for open globe injury with retained IOFB.13–15 Many of these injuries were due to construction work with tools (hammering metal, machine tool failure), firearms, or explosions, consistent with other studies in different regions of the globe.1,4,16 This highlights the need for ocular protection among the general population, especially among working-age males during high-risk activities. As a result of the mechanisms leading to these injuries, IOFBs were mainly metallic and a majority were present in the posterior segment. Six patients presented with endophthalmitis while four additional patients developed endophthalmitis after initial management. Late presentation and organic IOFB were associated with increased endophthalmitis risk, in agreement with prior studies.9,13 These risk factors highlight the need for prompt management and aggressive antimicrobial prophylaxis depending on injury and IOFB. However, we found no association between endophthalmitis and age, anterior segment damage, posterior segment IOFB, or wound length >5 mm, as have been reported.4,5 Poor final acuity was associated with poor presenting acuity,4,10,14 presence of retinal detachment, and large wounds.
One open topic in IOFB management regards timing of foreign body removal relative to globe closure, mainly relevant to posterior segment IOFBs that require a vitreoretinal surgeon for removal via PPV. Some practitioners and institutions advocate for prompt IOFB removal as a combined case concurrent with primary globe repair. Jonas17 found lower endophthalmitis rates with primary removal and Andreoli9 reported low rates of endophthalmitis (3.2% in IOFB eyes) with 48 hours of IV antibiotics and prompt removal. Primary removal decreases the time for an IOFB to seed an infection and aims to sterilize the intraocular environment via antibiotic treatment, while globe repair decreases microbial entrance into the eye. Other studies, however, found no difference in endophthalmitis between primary and secondary removal,18 or found no endophthalmitis cases (0/79 eyes) with prompt broad-spectrum antibiotics and secondary removal days or weeks later.2 This latter study, however, consisted exclusively of American soldiers during Operation Iraqi Freedom, representing a young and healthy patient population who suffered injuries with IOFBs that may have been heat-sterilized due to explosion. Delayed removal generally occurs in cases of life-threatening polytrauma, if a surgeon is not available, or if the injury is complex and deemed to benefit from healing prior to posterior segment surgery. Proponents of delayed removal also advocate for better assessment of anatomic damage and decreased injury-associated inflammation. Often, in cases of secondary removal, systemic and/or intraocular antibiotics are initiated as endophthalmitis prophylaxis, given concern for infection. Delayed removal is often considered a risk factor for other retina-damaging pathologies including PVR.17 Given these considerations, expert recommendations and institutional practices remain inconsistent.
In this cohort, we detected no difference in endophthalmitis incidence between primary (4.0%) or secondary (6.9%) removal of posterior segment IOFBs, with high rates of prophylactic intraocular antibiotic usage in deferred removal cases. While primary removal is often desired, these results suggest that prompt globe closure with appropriate endophthalmitis prophylaxis and secondary IOFB removal may present a reasonable strategy if primary removal is not possible. Final acuity was worse in the secondary removal group; however, these eyes presented with worse acuity and higher rates of retinal damage, complicating the interpretation of these results and further suggesting that injury severity impacts physician management.
In IOFB cases, many practitioners advocate for systemic antibiotic prophylaxis on presentation.13 While the optimal regimen is hard to define, this most commonly includes PO or IV cephalosporins, fluoroquinolones, and/or IV vancomycin, as these drugs achieve therapeutic minimum inhibitory concentration intraocularly, and cover the most common pathogens.13,14 When IOFBs are removed primarily, these patients may be hospitalized for IV antibiotics or transition to PO antibiotics on discharge. More controversial are antimicrobial strategies for IOFBs that are retained after primary globe closure and when to utilize intraocular antimicrobials. Many practitioners recommend intraocular antibiotics in wounds that are deemed high-risk for infection including those obtained in rural accidents or IOFBs that are suspected to be contaminated with soil or vegetable matter, though prospective data are limited. Soheilian19 conducted a double-blinded randomized controlled trial for patients with open globe injuries (with and without IOFBs). In 346 eyes, the authors found a reduction in endophthalmitis in ruptured globes (2.3% to 0.3%) with intraocular antibiotic treatment, and eyes with IOFBs showed a marked reduction from 28% (7/25) to 0% (0/27) endophthalmitis with intravitreal or intracameral antibiotics at globe closure. In the 88 eyes of our cohort, all patients received antibiotics, though delivery route, specific agents, and treatment duration varied, which made identification of trends difficult. In part, this variability stemmed from the long time period of this study as treatment paradigms have evolved. Systemic antibiotic prophylaxis occurred in 80.7% of IOFB cases and intravitreal antibiotics were utilized in 50%, though intravitreal antibiotics were highly prevalent (86.2%) in secondary IOFB removal cases and may represent an important component of endophthalmitis prophylaxis.
Limitations of this study are the retrospective nature and small sample size. The lack of randomized and standardized treatment algorithms can introduce bias, especially given the heterogeneous presentation of ocular trauma. Additionally, due to low incidence, small numbers diminish statistical power to uncover trends. Future coordinated multi-center efforts, meta-analyses, and registries will be critical to continued progress in studying this relatively rare presentation to establish best practices. This study consisted of patients over nearly 20 years, and therefore current management practices may not have been employed in patients who sustained injuries early in the cohort.
Conclusions
Delayed presentation and organic foreign bodies are risk factors for endophthalmitis following open globe injuries with retained IOFBs. Poor presenting visual acuity, large wound size, and retinal detachment at presentation correlated with poor final visual outcomes. Prompt globe closure and intravitreal antibiotic prophylaxis in cases of organic foreign bodies or secondary, delayed IOFB removal may reduce the risk of endophthalmitis in these eyes with already guarded visual potential.
Abbreviations
IOFB, intraocular foreign body; PPV, pars plana vitrectomy; CF, count fingers; HM, hand motion; LP, light perception; NLP, no light perception; PVR, proliferative vitreoretinopathy; SO, sympathetic ophthalmia; RD, retinal detachment; RT, retinal tear; VA, visual acuity; IV, intravenous; PO, per os; POD, post-operative day; logMAR, logarithm of the minimum angle of resolution.
Data Sharing Statement
Data will be made available upon reasonable request to the corresponding author.
Ethics Approval and Informed Consent
This retrospective study was approved by the IRB of the University of Michigan Medical School, conducted in compliance with HIPAA, and adhered to the 1964 Declaration of Helsinki and later amendments. Informed consent was not obtained due to the retrospective nature of the study, and not deemed necessary by the IRB.
Consent for Publication
No images of patients are included in the text. Individuals discussed within the text were anonymized to prevent identification of participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors did not receive support from any organization for this study.
Disclosure
The authors have no relevant financial or non-financial interests to disclose. The abstract of this paper was presented at the 2021 ARVO meeting as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Investigative Ophthalmology & Visual Science, June 2021, Vol.62, 3679: https://iovs.arvojournals.org/article.aspx?articleid=2775931
References
1. Loporchio D, Mukkamala L, Gorukanti K, Zarbin M, Langer P, Bhagat N. Intraocular foreign bodies: a review. Surv Ophthalmol. 2016;61(5):582–596. doi:10.1016/j.survophthal.2016.03.005
2. Colyer MH, Weber ED, Weichel ED, et al. Delayed intraocular foreign body removal without endophthalmitis during Operations Iraqi Freedom and Enduring Freedom. Ophthalmology. 2007;114(8):1439–1447. doi:10.1016/j.ophtha.2006.10.052
3. Kazokoğlu H, Saatçi O. Intraocular foreign bodies: results of 27 cases. Ann Ophthalmol. 1990;22(10):373–376.
4. Thompson JT, Parver LM, Enger CL, Mieler WF, Liggett PE. Infectious endophthalmitis after penetrating injuries with retained intraocular foreign bodies. National Eye Trauma System. Ophthalmology. 1993;100(10):1468–1474. doi:10.1016/s0161-6420(93)31454-5
5. Zhang Y, Zhang M, Jiang C, Qiu HY. Intraocular foreign bodies in China: clinical characteristics, prognostic factors, and visual outcomes in 1421 eyes. Am J Ophthalmol. 2011;152(1):66–73.e1. doi:10.1016/j.ajo.2011.01.014
6. Duan F, Yuan Z, Liao J, Zheng Y, Yang Y, Lin X. Incidence and risk factors of intraocular foreign body-related endophthalmitis in Southern China. J Ophthalmol. 2018;2018:8959108. doi:10.1155/2018/8959108
7. Boldt HC, Pulido JS, Blodi CF, Folk JC, Weingeist TA. Rural endophthalmitis. Ophthalmology. 1989;96(12):1722–1726. doi:10.1016/s0161-6420(89)32658-3
8. Ahmed Y, Schimel AM, Pathengay A, Colyer MH, Flynn HW. Endophthalmitis following open-globe injuries. Eye. 2012;26(2):212–217. doi:10.1038/eye.2011.313
9. Andreoli CM, Andreoli MT, Kloek CE, Ahuero AE, Vavvas D, Durand ML. Low rate of endophthalmitis in a large series of open globe injuries. Am J Ophthalmol. 2009;147(4):601–608.e2. doi:10.1016/j.ajo.2008.10.023
10. Liu Y, Wang S, Li Y, Gong Q, Su G, Zhao J. Intraocular foreign bodies: clinical characteristics and prognostic factors influencing visual outcome and globe survival in 373 eyes. J Ophthalmol. 2019;2019:5208092. doi:10.1155/2019/5208092
11. Lange C, Feltgen N, Junker B, Schulze-Bonsel K, Bach M. Resolving the clinical acuity categories “hand motion” and “counting fingers” using the Freiburg visual acuity test (FrACT). Graefes Arch Clin Exp Ophthalmol. 2009;247(1):137–142. doi:10.1007/s00417-008-0926-0
12. Kuhn F, Morris R, Witherspoon CD. Birmingham Eye Trauma Terminology (BETT): terminology and classification of mechanical eye injuries. Ophthalmol Clin North Am. 2002;15(2):139–143. doi:10.1016/s0896-1549(02)00004-4
13. Bhagat N, Nagori S, Zarbin M. Post-traumatic Infectious Endophthalmitis. Surv Ophthalmol. 2011;56(3):214–251. doi:10.1016/j.survophthal.2010.09.002
14. Yeh S, Colyer MH, Weichel ED. Current trends in the management of intraocular foreign bodies. Curr Opin Ophthalmol. 2008;19(3):225–233. doi:10.1097/ICU.0b013e3282fa75f1
15. Mukkamala LK, Soni N, Zarbin MA, Langer PD, Bhagat N. Posterior segment intraocular foreign bodies: a 10-year review. Ophthalmol Retina. 2017;1(4):272. doi:10.1016/j.oret.2017.01.007
16. Chang T, Zhang Y, Liu L, et al. Epidemiology, clinical characteristics, and visual outcomes of patients with intraocular foreign bodies in southwest china: a 10-year review. Ophthalmic Res. 2021;64(3):494–502. doi:10.1159/000513043
17. Jonas JB, Budde WM. Early versus late removal of retained intraocular foreign bodies. Retina. 1999;19(3):193–197. doi:10.1097/00006982-199905000-00003
18. Ferrari TM, Cardascia N, Di Gesù I, Catella N, Recchimurzo N, Boscia F. Early versus late removal of retained intraocular foreign bodies. Retina. 2001;21(1):92–93. doi:10.1097/00006982-200102000-00026
19. Soheilian M, Rafati N, Mohebbi MR, et al. Prophylaxis of acute posttraumatic bacterial endophthalmitis: a multicenter, randomized clinical trial of intraocular antibiotic injection, report 2. Arch Ophthalmol. 2007;125(4):460–465. doi:10.1001/archopht.125.4.460
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.