Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Endobronchial Valve Replacements in Patients with Advanced Emphysema After Endoscopic Lung Volume Reduction
Authors Brock JM ![]() , Schuster PU, Böhmker F, Eberhardt R, Gompelmann D, Kontogianni K, Trudzinski F
, Schuster PU, Böhmker F, Eberhardt R, Gompelmann D, Kontogianni K, Trudzinski F ![]() , Benjamin N, Herth F
, Benjamin N, Herth F ![]()
Received 15 February 2023
Accepted for publication 30 April 2023
Published 19 May 2023 Volume 2023:18 Pages 933—943
DOI https://doi.org/10.2147/COPD.S408674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Judith Maria Brock,1,2 Paul Ulrich Schuster,3 Felix Böhmker,3 Ralf Eberhardt,4 Daniela Gompelmann,5 Konstantina Kontogianni,1,2 Franziska Trudzinski,1,2 Nicola Benjamin,1 Felix Herth1,2
1Department of Pneumology and Critical Care Medicine, Thoraxklinik at University of Heidelberg, Heidelberg, Germany; 2Translational Lung Research Center Heidelberg (TLRC), German Center for Lung Research (DZL), Heidelberg, Germany; 3Medical Faculty, University of Heidelberg, Heidelberg, Germany; 4Department of Pneumology and Intensive Care Medicine, Asklepios Klinik Barmbek, Hamburg, Germany; 5Department of Internal Medicine II, Division of Pulmonology, Medical University of Vienna, Vienna, Austria
Correspondence: Judith Maria Brock, Department of Pneumology and Critical Care Medicine, Thoraxklinik Heidelberg, University Hospital of Heidelberg, Röntgenstraße 1, Heidelberg, 69126, Germany, Tel +49 6221-3968256, Email [email protected]
Purpose: Up to 41% of patients with endobronchial valve implantation need revision bronchoscopies and valve replacements most likely due to valve dysfunction or lack of benefit. So far, no data is available whether valve replacements lead to the desired lobar volume reduction and therapy benefit.
Patients and Methods: We conducted a single-center retrospective analysis of patients with endobronchial valve implantation and at least one valve replacement. Indications and number of revision bronchoscopies and valve replacements were evaluated. Therapy benefit regarding lung function and exercise capacity as well as development of complete lobar atelectasis was investigated and possible predictors identified.
Results: We identified 73 patients with 1– 12 revision bronchoscopies and 1– 5 valve replacements. The main indication for revision bronchoscopy in this group was lack of therapy benefit (44.2%). Lung function and exercise capacity showed improvements in about one-third of patients even years after the initial implantation. A total of 26% of all patients showed a complete lobar atelectasis at the end of the observation period, 56.2% had developed lung volume reduction. The logistic regression revealed the development of a previous complete lobar atelectasis as predictor for a complete lobar atelectasis at final follow-up. Oral cortisone long-term therapy was also shown as predictive factor. The probability for a final complete lobar atelectasis was 69.2% if a lobar atelectasis had developed before.
Conclusion: Valve replacements are more likely to be beneficial in patients who develop a re-aeration of a previous lobar atelectasis following valve implantation. Every decision for revision bronchoscopy must be taken carefully.
Keywords: endobronchial lung volume reduction, endobronchial valves, valve replacement, revision bronchoscopy, COPD
Introduction
Endoscopic lung volume reduction (ELVR) with valves has become an established procedure for treating advanced emphysema in chronic obstructive pulmonary disease (COPD), but selecting patients and guiding their way in case of therapy-failure remains a challenge. Up to 35% of patients develop complete lobar atelectasis and gain functional therapy benefit, represented by clinical, lung function and exercise improvements.1–3 The development of complete lobar atelectasis is moreover associated with a survival benefit.3 Apart from this “primary successful” group, some patients with lacking therapy benefit or complications need further bronchoscopies.4 Randomized controlled trials report a revision bronchoscopy rate of 19–39% for the first year.5–10 41% of all patients need at least one revision bronchoscopy, mainly in order to investigate valve dysfunction as reason for lacking therapy benefit.11,12 If the bronchoscopist evaluates the endobronchial valves as functional, they are left in place. Whenever valves are observed as dysfunctional, they are explanted and replaced with new valves, preferably in one bronchoscopic session. However, sometimes valve removal and replacement is performed in two sessions due to bleeding, secretions or excessive granulation tissue. Reasons for valve dysfunction are multiple, eg dislocation, dysfunction due to granulation tissue or secretion.4
If patients do not benefit despite several valve replacements, valves will be finally explanted in 17% of all cases.13 For a subgroup of patients, lung volume reduction surgery (LVRS) presents a possible alternative therapy option following valve therapy.14 According to the literature, a revision bronchoscopy with one valve replacement can improve the forced expiratory volume in one second (FEV1) in 63% of patients and the residual volume (RV) in 64%.12 So far, there are no long-term data published for those patients who get one or more valve replacements over months or years and in whom valves remain indefinitely in-situ. Because every revision bronchoscopy can represent a risk for patients with severe emphysema, the question is raised: Are valve replacements worth the risk? We therefore investigated in a retrospective analysis the group of patients with repeated valve replacements regarding therapy benefit. In particular, we tried to identify factors which can predict therapy success.
Materials and Methods
Data Collection
This is a retrospective analysis of patients who received endobronchial valve implantation in the years 2016–2019 at the Thoraxklinik Heidelberg. All patients gave written informed consent for the scientific use of their medical records. The study complies with the Declaration of Helsinki. Patients with at least one valve replacement and valves in situ until the end of the observation period were enrolled in the specific analysis. To avoid selection bias, group comparisons were performed regarding baseline characteristics (all parameters from Table 1 except fissure completeness and emphysema index) between the four patient groups “primary successful group” vs “explantation group” vs “LVRS group” vs “valve replacement group” (Figure 1).
 |
Table 1 Baseline Demographic Data and Characteristics of the Valve Replacement Group |
 |
Figure 1 Patient selection. |
Data were recorded from doctoral letters, questionnaires (mMRC [modified medical research council], CAT [COPD Assessment test]), laboratory, vital data (body mass index [BMI] in kg/m²), 6-minute-walk-distance (6-MWD), body plethysmography (FEV1, RV, VC [vital capacity], TLC [total lung capacity] in l and %) and diffusion capacity (DLCO SB [transfer factor for carbon monoxide] and DLCO/VA [DLCO divided by the alveolar volume]) in %). Chest x-ray and multi-detector computed tomography (MDCT) of the lung were reviewed. Emphysema index was obtained from the Heidelberg-based quantitative computed tomography software Yacta (yet another CT scan analyzer).15 Every bronchoscopy report was reviewed, including Chartis® assessment and reasons for valve replacement as well as valve types (endobronchial valves [EBV] and intrabronchial valves [IBV]). Fissure completeness is evaluated by experienced radiologists at our center and in case of incomplete fissures (80–95%) Chartis® measurement was performed.
Every follow-up visit was recorded (30 days, 90 days, 180 days, 365 days after ELVR – starting new after every valve replacement) until January 2022. The 30-day follow-up after the last valve replacement was the primary endpoint of the analysis (“final follow-up”). Additionally, also data 180 days after the last valve replacement were reviewed. The groups were divided according to their therapy success into “complete lobar atelectasis” vs “lung volume reduction” vs “no volume reduction” and evaluated for group differences regarding all baseline characteristics from Table 1.
Statistical Analysis
All analyses have been performed using IBM SPSS version 27 (SPSS Statistics V27, IBM Corporation, Somers, New York). Data are presented as mean ± standard deviation (SD) or median (min-max and interquartile range [IQR]). Frequency data are presented as n and percentage. Comparison of clinical data between follow-up visit and baseline was performed by two-sided Student’s t-test for paired data. Clinical data were analyzed as continuous variables and for FEV1, RV and 6-MWD as dichotomized variables representing improvement above or below the threshold of minimal clinically important difference (MCID). MCID was defined as +100mL for FEV1, −310mL for RV and +26 ±2m for 6-MWD according to current literature.16–18 Frequency data was compared by chi-square test.
Analysis of predictive factors of complete atelectasis at final follow-up was performed by logistic regression in an univariable analysis with the following variables (selected according to clinical importance): sex, age, nicotine consumption, lung function parameters initially, mMRC, CAT, 6-MWD, cardiovascular risk factors, BMI, oral cortisone long-term therapy, roflumilast, long-acting beta-agonists (LABA), long-acting muscarinic antagonists (LAMA), inhaled corticosteroids (ICS), necessity of Chartis® measurement, emphysema index of the lung and the target lobe, GOLD (Global Initiative for Chronic Obstructive Lung Disease) group, localization of valves, respiratory insufficiency, previous development of atelectasis, eosinophil count, number of valve replacements and revision bronchoscopies, atelectasis before first revision bronchoscopy and at 90 days. Parameters with more than 15% missing values were excluded (CAT, atelectasis at 90 days). Due to the explorative nature of the study, p-values were interpreted descriptively. No adjustment for multiple testing was performed. p-values <0.05 were considered statistically significant.
Results
Patient Selection
In the years 2016–2019, 244 patients underwent endobronchial valve implantation at the Thoraxklinik Heidelberg. Clinical and functional data did not significantly differ between the four patient groups “primary successful” vs “explantation” vs “LVRS” vs “valve replacement” (Figure 1). The left lower lobe (LLL) was most often the treated target lobe in all groups. In the primary successful group, the left upper lobe (LUL) was more frequently treated compared to the valve replacement group (34.9% vs 12.3%) and the LLL less frequently (38.5% vs 58.9%) (p=0.002). This was also significant (p=0.021) when comparing the primary successful group (34.9% LUL, 38.5% LLL) with the other three groups (14.8% LUL, 51.1% LLL). Moreover, FEV1 and VC were lower in the primary successful group, compared to the other three groups (FEV1 0.75 l vs 0.81 l, p= 0.049; VC 2.12 l vs 2.41 l, p=0.004; VC 64.3% vs 69.6%, p=0.023).
We identified 73 patients that underwent at least one valve replacement and valves remained in situ until the end of the observation period. All further analysis was performed for this group.
Revision Bronchoscopies and Valve Replacements
Baseline parameters of the valve replacement group are presented in Table 1. The mean time interval between valve implantation and the first revision bronchoscopy was 172 ± 148 days (2–737 days, median 129.5 days, IQR 131.5). The maximum time interval between valve implantation and last revision bronchoscopy was 1822 days (5 years) for a patient with 12 revision bronchoscopies. The mean time interval between valve placement and final follow-up was 507 ± 403 days. A total of 218 revision bronchoscopies (1–12 per patient) and 107 valve replacements (1–5 per patient) were performed in total. Most of the patients (34.2%) received two revision bronchoscopies and one valve replacement (67.1%) (Figure 2). Lacking therapy benefit presents the main indication for revision bronchoscopies (Figure 3). Further information about characteristics of the revision bronchoscopies is available in Table S1.
 |
Figure 2 Total number of revision bronchoscopies and valve replacements per patient. |
 |
Figure 3 Indications for revision bronchoscopy. The term “reimplantation” includes the following indications: reimplantation after former explantation (when reimplantation was not possible in the same bronchoscopy or after pneumothorax) or reimplantation of expectorated valves. In nine patients, valves had to be replaced once because they were expectorated, in four patients this had to be done twice, in two patients three times. |
Therapy Success
Clinical and Functional Outcome
In comparison to the baseline data, few statistically significant improvements were found for lung function and exercise capacity at various timepoints (Table 2). At final follow-up, VC in l and % (p=0.008, p=0.036), TLC in l (p=0.003) and RV in % (p=0.033) improved significantly. At 90-day-follow-up 32.8% of patients reached MCID for FEV1, 56.3% reached MCID for 6-MWD, nobody reached MCID for RV. At final follow-up, it was 29.2% for FEV1, 35.6% for 6-MWD, and none for RV.
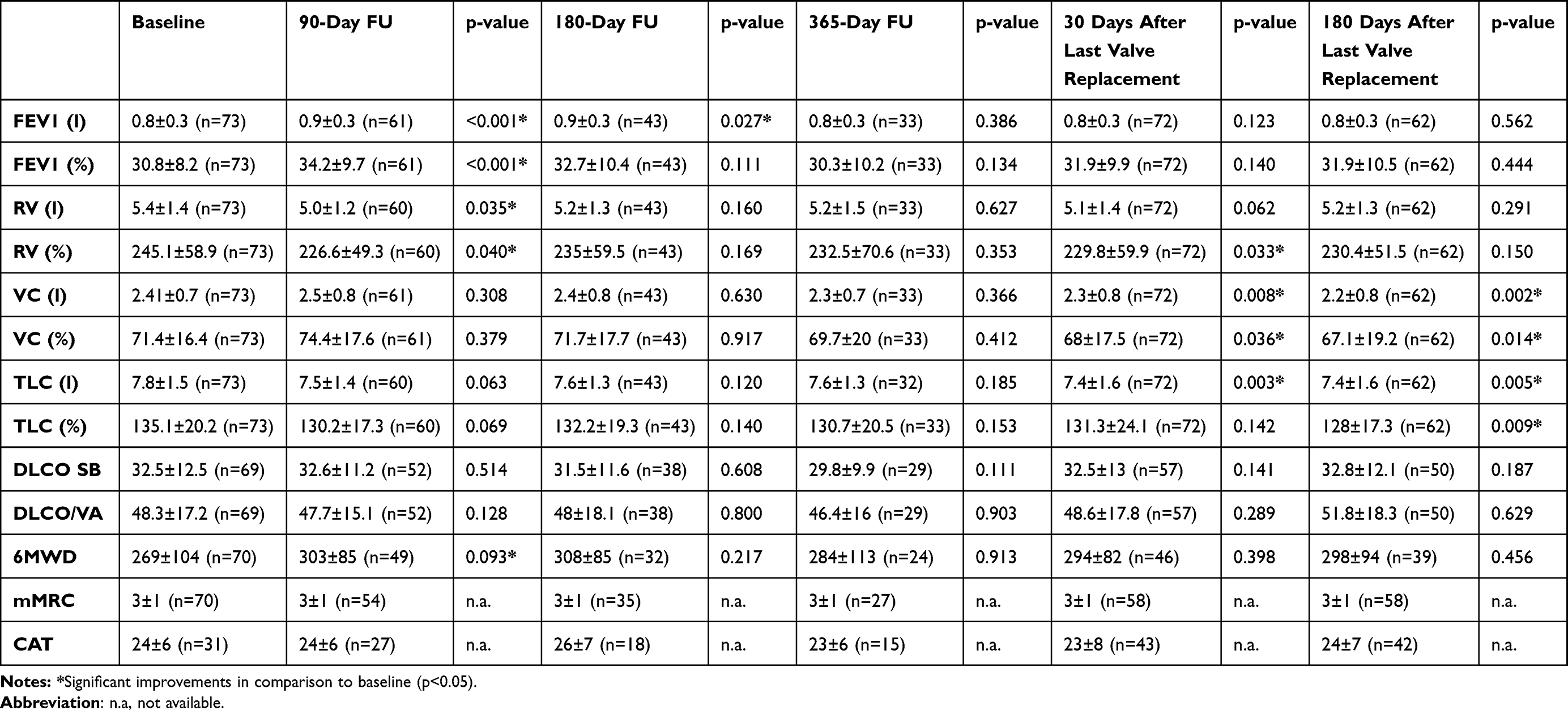 |
Table 2 Course of Functional and Clinical Outcome Parameters of the Valve Replacement Group at All Follow-Up Timepoints |
Radiological Outcome
At 90-days follow-up, 11.1% of the patients showed a complete lobar atelectasis of the target lobe (Table 3). The rate for complete lobar atelectasis was 13.6% for the 180-days follow-up and 12.1% for the 365-days follow-up. Before the first revision bronchoscopy, 15.1% had once developed a complete lobar atelectasis that had re-opened and indicated the revision bronchoscopy. A total of 11% of the patients never had developed any visible lung volume reduction before the first revision bronchoscopy. Twenty-six patients (35.6%) have developed a complete lobar atelectasis over the observation time at least once. At the final follow-up, 19 patients (26%) had complete lobar atelectasis, 56.2% showed visible lung volume reduction. Only 5 of these 19 patients had an atelectasis before the first revision bronchoscopy. Two more patients developed complete lobar atelectasis 180 days after the last valve replacement. The lobar atelectasis group underwent 1–6 revision bronchoscopies and 1–3 valve replacements.
 |
Table 3 Atelectasis Rate at All Follow-Up Timepoints |
Group Differences
The group of patients with complete lobar atelectasis at final follow-up (n=19) had more often an oral cortisone long-term therapy initially (42.1%) than the group with lung volume reduction only (17.1%, p=0.011). However, no difference was found in comparison to the group with no lung volume reduction. When comparing the patients with complete lobar atelectasis vs those without, no statistically significant differences could be found regarding all baseline characteristics. All outcome parameters at all follow-up timepoints can be viewed for the group with complete lobar atelectasis in Table S2.
Predictors for Therapy Success
After exclusion of missing values, the logistic regression showed the development of a previous complete lobar atelectasis as main and only predictor (p<0.001) of a complete lobar atelectasis finally. A total of 18 of 26 patients (69.2%) that had developed a complete atelectasis in the meantime, also showed a complete atelectasis at final follow-up. Only one out of 47 patients that never had atelectasis before showed atelectasis finally. In order to investigate further factors, an additional regression analysis without knowledge on previous atelectasis was performed. This revealed the presence of oral cortisone long-term therapy as predicting factor (p=0.003). A total of 8 of 15 patients (53.3%) with oral cortisone long-term therapy developed a complete atelectasis vs 11 of 58 (19%) patients without.
Discussion
To our knowledge, this is the first analysis evaluating the benefit of several valve replacements. We observed that 30% of all patients (73 out of 244) with endobronchial valve implantation underwent one or more valve replacements over an observation time up to 6 years and valves remained in-situ. Because a long observation period was reported, the occurrence of indications and complications differs from the results of studies with shorter observation periods. The rate of valve replacements is reported 17% in the STELVIO trial10 and 21.2% in a prospective cohort study of Roodenburg et al.12 The latter reported a second revision bronchoscopy in 24 patients and a third in six patients; further bronchoscopies were not evaluated. Final valve explantation (with possibly later LVRS) was conducted in 25% of all cases in our study, which is higher than previously reported rates of 13–17%.12,13,19
Lacking therapy benefit was the main indication for revision bronchoscopy in 44.2% of our cases vs 74.3% in the study of Roodenburg et al.12 Rates for poststenotic pneumonia (0.9 vs 1.5%) and hemoptysis (7% vs 12.1%) were similar in these trials, while we report a higher rate for expectorated valves (20.5% vs 4.1%).
We found no significant differences regarding baseline characteristics in the four different “success” groups except that valves seem to work better in the left upper than the left lower lobe. Therefore, predicting whether valve implantation will be successful will remain a challenge.
This study showed only moderate improvements of lung function. This was expected due to the inhomogeneous follow-up timepoints that were disrupted by revision bronchoscopies and prolonged over a long time period until the final follow-up. Meanwhile emphysema progression and annual decline of FEV1 took place and blurred therapy effects. However, clinically meaningful improvements could be observed for the whole group regarding FEV1 and 6-MWD at 90 days and even at the end of the observation period. It is quite surprising and encouraging that lung function parameters still show improvements at these timepoints.
The development of complete lobar atelectasis is associated with prolonged survival with a 5-year survival rate of 65.3% for patients with vs 43.9% for patients without lobar atelectasis.3 Therefore and also because lobar atelectasis is a clear-to-evaluate parameter, the development of complete lobar atelectasis was chosen as primary outcome. We observed that 26% of patients who underwent valve replacements developed a complete lobar atelectasis. This is nearly as high as already reported atelectasis rates of 5–34.8% in other trials.1–3,20
Logistic regression revealed the development of previous complete atelectasis as strong predictor for therapy success. The probability of final atelectasis was 69.2% for patients with previous atelectasis. While this is not surprising, this is to our knowledge the first study to prove this clinical observation. Interpreting these results, we believe it is beneficial to replace valves, whenever a complete atelectasis had developed before and in the further course was re-aerated. In this study, a maximum of 3 valve replacements was needed for final success.
More surprising is that in this study cohort, other factors did not seem to influence the development of complete lobar atelectasis, even not emphysema index of the target lobe or the necessity of Chartis® measurement (which was necessary in 26% of patients due to visually incomplete fissures). The reported diagnostic accuracy for visual-based fissure interpretation is 77%, for quantitative computed tomography software analysis 78.8–96.4% and for Chartis® measurement 74–83.3%.21 Discordant results are seen comparing visual analysis vs Chartis® measurement in 31.9%. This leaves room for false-negative collateral ventilation results and could therefore also explain missing therapy benefit. However, the results from this study may imply that the methods to exclude collateral ventilation seem good enough to not be a relevant factor for missing atelectasis.
In contrary to our results, low VC, high RV, low 6-MWD and heterogeneity index have been identified as predictors for lung function improvements in patients with complete atelectasis.22 Furthermore, ICS use and higher emphysema index were shown as predictors for inferior outcome.23 No analysis regarding the outcome specific for patients with valve replacements has been done so far.
The presence of oral cortisone long-term therapy as predictive factor for therapy success is difficult to interpret. Oral cortisone long-term therapy might prevent exacerbations and formation of granulation tissue and therefore could secure valve function, but this hypothesis needs further evaluation.
The presented study has some obvious limitations. This is due to the retrospective design of the study and the inhomogeneous follow-up time points. The heterogeneity of this patient cohort caused difficulties for adequate endpoint analysis. Conclusions for lung function results should only be drawn carefully because of multiple testing problems.
Finally, despite the challenging design of this retrospective analysis, reliable results regarding development of atelectasis could be obtained and represent a building block in the decision-making for patients with primary ELVR failure.
Conclusion
Valve replacements are successful procedures with a final 26% complete atelectasis rate and are promising, when complete atelectasis has once occurred and was lost in the further course. The price for complete atelectasis is quite high, as often many valve replacements are required for full therapy benefit. Patients should be treated in experienced centers that have the availability to offer revision bronchoscopies and are able to recognize and treat possible complications. Every valve replacement should be an individual decision between the expert team and the well-informed patient.
Abbreviations
6-MWD, 6-minute-walk difference; BMI, body mass index; CAT, COPD assessment test; COPD, Chronic Obstructive Pulmonary Disease; DLCO SB, transfer factor for carbon monoxide; DLCO/VA, DLOC divided by the alveolar volume; EBV, endobronchial valves; ELVR, Endoscopic Lung Volume Reduction; FEV1, forced expiratory volume in 1 second; GOLD, Global Initiative for Chronic Obstructive Lung Disease; IBV, intrabronchial valves; ICS, inhaled corticosteroid; LABA, long-acting-beta-agonist; LAMA, long-acting-muscarinic antagonist; LLL, left lower lobe; LUL, left upper lobe; LVRS, Lung volume reduction surgery; MCID, minimal clinically important difference; MDCT, multi-detector computed tomography; mMRC, modified Medical Research Council; RV, residual volume; TLC, total lung capacity; VC, vital capacity; Yacta, yet another CT scan analyzer.
Data Sharing Statement
The data that support the findings of this study are available in the Supplementary Materials of this article.
Ethics Approval Declaration
The study protocol was reviewed and approved by the institute’s ethics committee of Heidelberg (S-304/2021). All patients gave written informed consent for the scientific use of their medical records. This study complies with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There were no funding sources for this project.
Disclosure
Judith Brock has received honoraria and consultation fees from Boehringer Ingelheim, Astra Zeneca, streamed up!, Intuitive Surgical Inc, Berlin Chemie, outside the submitted work. Paul Ulrich Schuster, Felix Böhmker, and Nicola Benjamin have no conflicts of interest to report for this work. Prof. Dr. Ralf Eberhardt reports honoraria or payment for lectures and presentations from Broncus, Olympus, Pentax, Pulmonx, Astra Zeneca. He joins the data safety monitoring board for Intuitive Surgical Inc, outside the submitted work. Prof. Dr. Daniela Gompelmann reports fees for lectures and travel from Pulmonx, Chiesi, Boehringer Ingelheim, Astra Zeneca, Berlin Chemie, Erbe, Novartis, Olympus, outside the submitted work. Konstantina Kontogianni has received honoraria for lectures from Berlin-Chemie, Astra Zeneca and Boston Scientific, outside the submitted work. Franziska Trudzinski has received honoraria for lectures from Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Grifols, Novartis, CSL Behring. She participates in an Advisory Board for CSL Behring, GlaxoSmithKline and Boehringer Ingelheim, outside the submitted work. Felix Herth reports Research Support from Olympus Medical, Pulmonx, Broncus, Uptake Medical, Roche Diagnostics, BMBF, DFG, EU, Klaus-Tschira Stiftung, BMG; Lecturing honoraria from Pulmonx, Uptake Medical, Roche Diagnostics, Astra Zeneca, Boehringer Ingelheim, Novartis, Berlin Chemie, Chiesi, Medupdate, Erbe, GSK and consulting activities for Olympus Medical, Pulmonx, Broncus – Uptake Medical, Roche Diagnostics, Astra Zeneca, J&J, Karger, LÄK, Boston Scientific, Dinova, Nanovation, Free Flow Medical, Erbe, outside the submitted work.
References
1. Davey C, Zoumot Z, Jordan S, et al. Bronchoscopic lung volume reduction with endobronchial valves for patients with heterogeneous emphysema and intact interlobar fissures (the BeLieVeR-HIFi study): a randomised controlled trial. Lancet. 2015;386(9998):1066–1073. doi:10.1016/S0140-6736(15)60001-0
2. Hopkinson NS, Kemp SV, Toma TP, et al. Atelectasis and survival after bronchoscopic lung volume reduction for COPD. Eur Respir J. 2011;37(6):1346–1351. doi:10.1183/09031936.00100110
3. Gompelmann D, Benjamin N, Bischoff E, et al. Survival after endoscopic valve therapy in patients with severe emphysema. Respiration. 2019;97(2):145–152. doi:10.1159/000492274
4. Koster TD, Klooster K, Ten Hacken NH, Nick HT, van Dijk M, Slebos D-J. Endobronchial valve therapy for severe emphysema: an overview of valve-related complications and its management. Expert Rev Respir Med. 2020;14(12):1235–1247. doi:10.1080/17476348.2020.1813571
5. Hartman JE, Lowie EGW, van Rikxoort EM, Klooster K, Slebos D-J. Endobronchial valves for severe emphysema. Eur Respir Rev. 2019;28:152. doi:10.1183/16000617.0121-2018
6. Valipour A, Slebos D-J, Herth F, et al. Endobronchial valve therapy in patients with homogeneous emphysema. Results from the IMPACT study. Am J Respir Crit Care Med. 2016;194(9):1073–1082. doi:10.1164/rccm.201607-1383OC
7. Klooster K, Ten Hacken NH, Nick HT, et al. Endobronchial valves for emphysema without interlobar collateral ventilation. N Engl J Med. 2015;373(24):2325–2335. doi:10.1056/NEJMoa1507807
8. Criner GJ, Sue R, Wright S, et al. A multicenter randomized controlled trial of zephyr endobronchial valve treatment in heterogeneous emphysema (LIBERATE). Am J Respir Crit Care Med. 2018;198(9):1151–1164. doi:10.1164/rccm.201803-0590OC
9. Kemp SV, Slebos D-J, Kirk A, et al. A multicenter randomized controlled trial of zephyr endobronchial valve treatment in heterogeneous emphysema (TRANSFORM). Am J Respir Crit Care Med. 2017;196(12):1535–1543. doi:10.1164/rccm.201707-1327OC
10. Klooster K, Hartman JE, Ten Hacken H, Nick HT, Slebos D-J. One-year follow-up after endobronchial valve treatment in patients with emphysema without collateral ventilation treated in the STELVIO trial. Respiration. 2017;93(2):112–121. doi:10.1159/000453529
11. Slebos D-J, Shah PL, Herth FJF, Valipour A. Endobronchial valves for endoscopic lung volume reduction: best practice recommendations from expert panel on endoscopic lung volume reduction. Respiration. 2017;93(2):138–150. doi:10.1159/000453588
12. Roodenburg SA, Klooster K, Hartman JE, Koster TD, van Dijk M, Slebos D-J. Revision bronchoscopy after endobronchial valve treatment for emphysema: indications, findings and outcomes. Int J Chron Obstruct Pulmon Dis. 2021;16:1127–1136. doi:10.2147/COPD.S302662
13. Gompelmann D, Gerovasili V, Kontogianni K, et al. Endoscopic valve removal 180 days since implantation in patients with severe emphysema. Respiration. 2018;96(4):348–354. doi:10.1159/000489887
14. Eichhorn ME, Gompelmann D, Hoffmann H, et al. Consolidating lung volume reduction surgery after endoscopic lung volume reduction failure. Ann Thorac Surg. 2021;111(6):1858–1865. doi:10.1016/j.athoracsur.2020.06.148
15. Achenbach T, Weinheimer O, Buschsieweke C, Heussel CP, Thelen M, Kauczor HU. Fully automatic detection and quantification of emphysema on thin section MD-CT of the chest by a new and dedicated software. Rofo. 2004;176(10):1409–1415. doi:10.1055/s-2004-813530
16. Hartman JE, Ten Hacken NH, Nick HT, et al. The minimal important difference for residual volume in patients with severe emphysema. Eur Respir J. 2012;40(5):1137–1141. doi:10.1183/09031936.00219111
17. Donohue JF. Minimal clinically important differences in COPD lung function. COPD. 2005;2(1):111–124. doi:10.1081/copd-200053377
18. Puhan MA, Chandra D, Mosenifar Z, et al. The minimal important difference of exercise tests in severe COPD. Eur Respir J. 2011;37(4):784–790. doi:10.1183/09031936.00063810
19. Leppig JA, Song L, Voigt DC, et al. When treatment of pulmonary emphysema with endobronchial valves did not work: evaluation of quantitative CT analysis and pulmonary function tests before and after valve explantation. Int J Chron Obstruct Pulmon Dis. 2022;17:2553–2566. doi:10.2147/COPD.S367667
20. Venuta F, Anile M, Diso D, et al. Long-term follow-up after bronchoscopic lung volume reduction in patients with emphysema. Eur Respir J. 2012;39(5):1084–1089. doi:10.1183/09031936.00071311
21. Saccomanno J, Hübner RH, Witzenrath M, et al. Bronchoscopic Measurement of Collateral Ventilation: state of the Art. Respiration. 2023;102(4):296–307. doi:10.1159/000528419
22. Gompelmann D, Hofbauer T, Gerovasili V, et al. Predictors of clinical outcome in emphysema patients with atelectasis following endoscopic valve therapy: a retrospective study. Respirology. 2016;21(7):1255–1261. doi:10.1111/resp.12819
23. Polke M, Brugger J, Rötting M, et al. Inhaled steroids, sex and emphysema index - clinical parameters with impact on the effectiveness of valve implantation in patients with severe emphysema. Int J Chron Obstruct Pulmon Dis. 2022;17:1423–1430. doi:10.2147/COPD.S361256
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.