")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 17
Emotional Distress is Associated with Lower Health-Related Quality of Life Among Patients with Diabetes Using Antihypertensive and/or Antihyperlipidemic Medications: A Multicenter Study in Indonesia
Authors Alfian SD , Annisa N, Iskandarsyah A , Perwitasari DA , Denig P , Hak E , Abdulah R
Received 28 July 2021
Accepted for publication 10 October 2021
Published 7 December 2021 Volume 2021:17 Pages 1333—1342
DOI https://doi.org/10.2147/TCRM.S329694
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Sofa D Alfian,1,2 Nurul Annisa,1,3 Aulia Iskandarsyah,4 Dyah A Perwitasari,5 Petra Denig,6 Eelko Hak,7 Rizky Abdulah1,2
1Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jatinangor, Indonesia; 2Center of Excellence in Higher Education for Pharmaceutical Care Innovation, Universitas Padjadjaran, Jatinangor, Indonesia; 3Unit of Clinical Pharmacy and Community, Faculty of Pharmacy, Universitas Mulawarman, Samarinda, Indonesia; 4Department of Clinical Psychology, Faculty of Psychology, Universitas Padjadjaran, Jatinangor, Indonesia; 5Department of Clinical Pharmacy, Faculty of Pharmacy, Universitas Ahmad Dahlan, Yogyakarta, Indonesia; 6Department of Clinical Pharmacy and Pharmacology, University of Groningen, University Medical Centre Groningen, Groningen, The Netherlands; 7Unit of Pharmaco-Therapy, Epidemiology & Economics, Groningen Research Institute of Pharmacy, University of Groningen, Groningen, The Netherlands
Correspondence: Sofa D Alfian
Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jl. Raya Jatinangor, KM 21, Jatinangor, Sumedang, Indonesia
Tel/Fax +62 22-7796200
Email [email protected]
Objective: To evaluate the associations between different types of diabetes distress and health-related quality of life (HRQOL) among patients with type 2 diabetes (T2DM) using antihypertensive and/or antihyperlipidemic medications in Indonesia and to explore the differences between those using only antihypertensive, only antihyperlipidemic, or both medications.
Methods: A multicenter cross-sectional study was conducted in Community Health Centers in three cities in Indonesia among patients with T2DM aged at least 18 years who were using antihypertensive and/or antihyperlipidemic medications. Diabetes distress subscales (emotional, regimen-related, interpersonal, and physician-related distress) and HRQOL were assessed using a validated diabetes distress scale-17 and EQ-5D-5L scale, respectively. Multiple linear regression models were used to evaluate the associations between different types of diabetes distress and HRQOL adjusting for confounders.
Results: Most of the 503 participants were females (67.6%) and aged 60– 69 years (40.8%). Emotional distress was negatively associated with HRQOL among the whole group of patients (β: − 0.08; 95% confidence interval (CI): − 0.10, − 0.05; p < 0.001). This association was similar across all therapeutic subgroups. Regimen-related distress (β: − 0.06; 95% CI: − 0.09, − 0.03; p < 0.001) and interpersonal distress (β: − 0.02; 95% CI: − 0.05, − 0.01; p = 0.022) were negatively associated, whereas physician-related distress (β: 0.04; 95% CI: 0.01, 0.07; p = 0.037) was positively associated with HRQOL among the whole group. These associations were also observed among those using only antihypertensive medication.
Conclusion: Emotional distress affects HRQOL in T2DM patients treated for cardiovascular comorbidities, independent of antihypertensive and/or antihyperlipidemic medication use.
Keywords: diabetes distress, quality of life, lipid-lowering medication, blood pressure-lowering medication
Highlights
What is already known about the topic?
- Diabetes distress is reportedly one of the important determinants associated with lower health-related quality of life (HRQOL). Therefore, assessing and monitoring diabetes distress is recommended as part of clinical care in several national guidelines in developed countries.
- The guidelines in Indonesia lack emphasis on the importance of addressing different types of diabetes distress during patient counseling.
What does the paper add to existing knowledge?
- Emotional distress was negatively associated with HRQOL among patients with type 2 diabetes mellitus (T2DM) using antihypertensive and/or antihyperlipidemic medications in Indonesia.
- This association was similar among T2DM patients using only antihypertensive, only antihyperlipidemic, or both medications.
What insights does the paper provide for informing healthcare-related decision-making?
- Emotional distress should be addressed in tailored interventions among patients with T2DM, independent of the use of antihypertensive and/or antihyperlipidemic medications to improve their HRQOL further.
Introduction
Type 2 diabetes mellitus (T2DM) needs a lifetime self-management plan and complex care activities, including regular blood glucose monitoring, healthy diet, physical exercise, and long-term medication.1 In Indonesia, 10.3 million patients with diabetes were reported in 2017, and this number is estimated to increase to 16.7 million patients by 2045.2 About a quarter of such patients experience diabetes distress in developed countries,3 but this number is expected to be higher in developing countries.4
Diabetes distress, a psychological condition reflecting the stress and burden associated with the management of diabetes, was reported to be one of the important determinants associated with lower health-related quality of life (HRQOL).5,6 Previous studies show that diabetes distress varies from general mental health problems, such as depression, and is more salient than depression and crucial to address in patients with diabetes.7,8 Different types of diabetes distress, including emotional, regimen-related, physician-related, and interpersonal distress, represent different sources of distress.9 Routine screening, early support, and the use of medication for diabetes distress can improve patients’ hemoglobin A1c (HbA1c), blood pressure, and cholesterol levels.10 Therefore, monitoring diabetes distress is recommended as part of clinical care in many national guidelines in developed countries.11,12 The guidelines in Indonesia lack emphasis on the importance of addressing diabetes distress during patient visits. This requires more attention, particularly in primary care settings where patients are more likely to report diabetes distress.13
Previous studies highlighted the importance of addressing diabetes distress to improve patients’ HRQOL among T2DM patients.14,15 Patients’ HRQOL is considered an important health outcome in T2DM patients.16 HRQOL is defined as a multidimensional construct that incorporates physical, mental, emotional, and social well-being. T2DM patients diagnosed with dyslipidemia were found to have lower HRQOL, particularly psychological quality of life, than those diagnosed with hypertension.5 Another study indicated that both hypertension and hyperlipidemia as comorbidities among T2DM patients were associated with lower HRQOL in general. Particularly, hypertension had more harmful effects on the mental health of patients.17 Although different HRQOL questionnaires were used in these studies,5,17 the findings indicate adverse effects of hypertension and/or hyperlipidemia on HRQOL in T2DM patients. Low HRQOL among T2DM patients is related to poor treatment response, worse disease progression, and mortality.18,19 Therefore, it is imperative to maintain and optimize patients’ HRQOL.
Currently, there is limited evidence on the association between diabetes distress and HRQOL in T2DM patients with hypertension and/or hyperlipidemia. The treatment of T2DM patients with these comorbidities may be more complicated owing to difficulties in managing their time, attention, and resources.20 Therefore, further studies are warranted to obtain insights into the association between different types of diabetes distress and HRQOL in T2DM patients with these comorbidities. Such information will be helpful for pharmacists and other healthcare providers to provide tailored interventions according to the individual patient’s requirements.
The primary objective of this study was to evaluate the associations between different types of diabetes distress and HRQOL among T2DM patients using antihypertensive and/or antihyperlipidemic medications in Indonesia. The secondary objective was to explore whether there were differences between those using only antihypertensive, only antihyperlipidemic, or both medications.
Methods
This study was reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies (Table S1).21
Study Design, Setting, and Patient Recruitment
A multicenter cross-sectional survey was conducted in three cities in Indonesia (Bandung, Samarinda, and Yogyakarta) from October 2018 to September 2019. Patients were recruited from purposively selected Community Health Centers (CHCs) according to the required number of T2DM patients diagnosed with hypertension and/or hyperlipidemia. CHCs are primary healthcare centers staffed with doctors, nurses, midwives, and pharmacists. One of the main programs of CHCs is to provide integrated chronic disease management at the sub-district level. Patients aged at least 18 years, diagnosed with type 2 diabetes for over one year, using antihypertensive and/or antihyperlipidemic medications, and literate in the Indonesian language were eligible to participate. Patients who were unable to take their medication, with severe physical or mental constraints, or pregnant or in the lactation period were excluded. This study was approved by the Health Research Ethics Committee of Universitas Padjadjaran (No. 1137/UN6.KEP/EC/2018) and was conducted according to the Declaration of Helsinki. Written informed consent was obtained from all patients who participated in this study.
Measures
Diabetes Distress
Distress about the burden of diabetes and its management was measured using the Diabetes Distress Scale−17 (DDS−17).9 The DDS comprises 17 statements evaluating the distress experienced by patients in the previous month using four subscales measuring different types of distress: emotional burden (five items, eg, “feeling angry, scared, and/or depressed when I think about living with diabetes”), physician-related distress (four items, eg, “feeling that my doctor doesn’t take my concerns seriously enough”), regimen-related distress (five items, eg, “feeling that I am often failing with my diabetes routine”), and interpersonal distress (three items, eg, “feeling that friends or family don’t appreciate how challenging living with diabetes can be”).9 All items of the DDS-17 and its subscales are available in the paper by Polonsky et al.9 Patients indicated how profound the experience of their distress was on a 6-point Likert scale ranging from “not a problem” to “a very serious problem”.9 The patients’ responses in each subscale were added and then divided using the number of statements in that particular subscale. The Indonesian version of the DDS-17 has been previously reported to be valid and reliable.22
HRQOL
Patients’ HRQOL was measured using the EuroQol 5-Dimension (EQ-5D) questionnaire. Two versions of the EQ-5D are available: 3-level (EQ-5D-3L) and 5-level (EQ-5D-5L).23 The EQ-5D-5L was used in this study because it shows better measurement and scoring properties in Indonesian T2DM patients.24 The EQ-5D-5L assesses the health status of patients using five statements regarding their mobility, self-care, usual activities, pain/discomfort, and anxiety/depression and is available in the paper by Rabin and De Charro.23 Each of these dimensions is recorded as “no problems (1)”, “slight problems (2)”, “moderate problems (3)”, “severe problems (4)”, and “extreme problems (5)”.25 One number from each of these dimensions results in a five-digit number that can be converted into a single EQ-5D-5L index using a formula that assigns different weights to each of the five-digit numbers of the health status.23 The specific set of weights (value set) we used was according to a representative general population of Indonesia.26 An EQ-5D-5L index of “1” indicates a perfect health status, whereas “0” indicates the worst possible health status.23 Although not diabetes-specific, the EQ-5D-5L is reported to be relevant for T2DM patients.27,28 The EQ-5D-5L questionnaire has been translated and validated for T2DM patients in Indonesia.24,26
Sociodemographic Covariates
The patient’s sociodemographic factors included sex, age, education level (no formal education or elementary school, junior and senior high school, or university), and health insurance type. The health insurance type was categorized as patients who could not afford to pay the health insurance premium (BPJS-PBI), patients who could afford to pay the health insurance premium (BPJS-Non PBI), and patients without health insurance. A structured case report form was used to record the duration of diabetes, hypertension, and/or hyperlipidemia (years).
Data Collection
The pharmacists screened patients’ eligibility at the CHCs. The pharmacist asked the researcher or trained research assistant to approach the eligible patient, briefly describe the study to the patient, and ask the patient to provide informed consent. Patients were asked to independently complete a self-reported questionnaire. In some cases, however, some elderly patients who could not read and/or answer the questionnaires themselves were interviewed by trained research assistants.
Sample Size Calculation
According to the minimum sample size formula for multiple linear regression analysis, as suggested by Green et al,29 a sample size of 122 patients per therapeutic subgroup was required when using 9 potential independent variables in the multivariate analysis.
Data Analysis
Descriptive statistics were used to report the patients’ characteristics. Multicollinearity was analyzed using the variance inflation factor. Data distribution was assessed to determine whether adjustments were required because of skewed distributions. Complete-case analyses were conducted because some data was observed to be missing. Multiple linear regression was conducted to evaluate the associations between different types of diabetes distress and HRQOL, adjusting for age, sex, health insurance type, education, and duration of diabetes, hypertension, and/or hyperlipidemia. First, the main analysis was conducted for the whole group of T2DM patients using antihypertensive and/or antihyperlipidemic medications. Second, the analyses per therapeutic subgroup were conducted, that is, among T2DM patients using only antihypertensive, only antihyperlipidemic, or both antihypertensive and antihyperlipidemic medications. The duration of hypertension and/or hyperlipidemia was included only for the relevant therapeutic subgroup. The adjusted associations were obtained from multiple linear regression models and regression coefficients, 95% confidence interval (CI), p-values, and adjusted R2 are reported. All statistical analyses were performed using SPSS software version 25.0 (IBM, Armonk, NY, USA).
Results
Patient Characteristics
A total of 503 T2DM patients (response rate 96.7%) using antihypertensive (439 patients), antihyperlipidemic (197 patients), or both antihypertensive and antihyperlipidemic medications (133 patients) participated in this study. The patients were from Bandung (6 CHCs; 132 patients), Samarinda (5 CHCs; 162 patients), and Yogyakarta (18 CHCs; 209 patients). Characteristics of the patients are presented in Table 1. Most patients were females and were aged 60–69 years (Table 1).
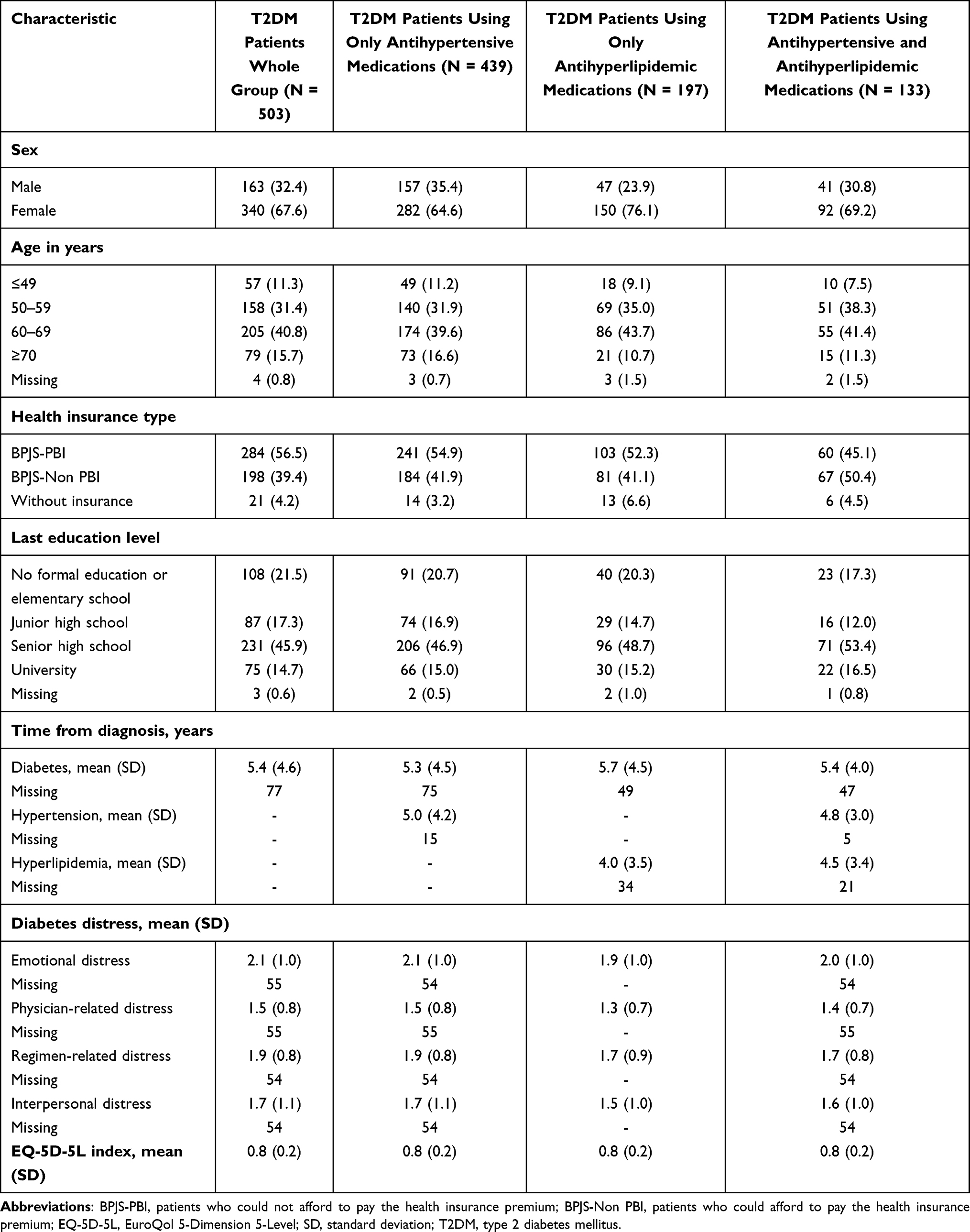 |
Table 1 Characteristics of T2DM Patients Using Antihypertensive and/Or Antihyperlipidemic Medications per Therapeutic Subgroup |
Among the different types of diabetes distress, the highest mean score was noted for emotional distress in the whole group of patients (2.1 ± 1.0). Similar mean scores were observed for those using only antihypertensive (2.1 ± 1.0), only antihyperlipidemic (1.9 ± 1.0), and both antihypertensive and antihyperlipidemic medications (2.0 ± 1.0). Physician-related distress exhibited the lowest mean score in the whole group of patients (mean 1.5 ± 0.8). A similar mean score was observed for those using only antihypertensive medications (1.5 ± 0.8), and slightly lower mean scores were observed for those using only antihyperlipidemic (1.3 ± 0.7) and both antihypertensive and antihyperlipidemic medications (1.4 ± 0.7). The mean score for regimen-related distress was 1.9 ± 0.8, which was similar for those using only antihypertensive medications (1.9 ± 0.8) and slightly lower for those using only antihyperlipidemic (1.7 ± 0.9) and both antihypertensive and antihyperlipidemic medications (1.7 ± 0.8). Finally, the mean score for interpersonal-related distress was 1.7 ± 1.1, which was similar for those using only antihypertensive medications (1.7 ± 1.1) and lower for those using only antihyperlipidemic (1.5 ± 1.) and both antihypertensive and antihyperlipidemic medications (1.6 ± 1.0) (Table 1).
A relatively high mean HRQOL (mean EQ-5D-5L index of 0.8) was noted in the whole group of T2DM patients using antihypertensive and/or antihyperlipidemic medications. This was similar to the mean HRQOL among those using only antihypertensive, only antihyperlipidemic, and both antihypertensive and antihyperlipidemic medications (Table 1). Additionally, having a problem with pain or discomfort was the most common HRQOL dimension experienced by all patients (Table 2).
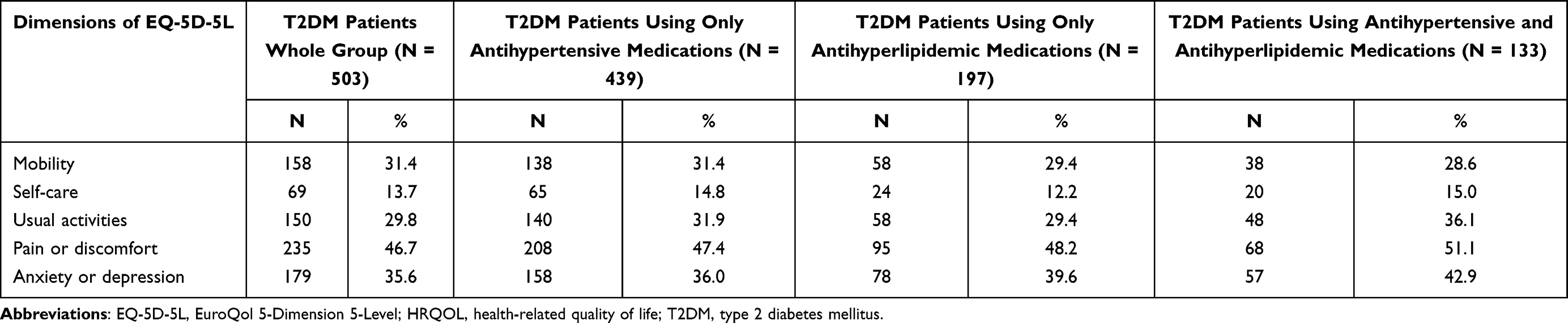 |
Table 2 HRQOL of T2DM Patients Using Antihypertensive and/Or Antihyperlipidemic Medications per Therapeutic Subgroup |
Associations Between Different Types of Diabetes Distress and HRQOL
No significant multicollinearity among different types of diabetes distress and sociodemographic factors was observed (variance inflation factors > 1). The HRQOL data were negatively skewed but considered acceptable to prove normal distribution (between −2 and +2).30,31 Adjusted analyses were conducted for age, sex, health insurance type, education level, and duration of diabetes, hypertension, and/or hyperlipidemia. Higher emotional distress was significantly associated with lower HRQOL among the whole group of patients (β: −0.08; 95% CI: −0.10, −0.05; p < 0.001) (Table 3). This association was observed among the subgroups of patients using only antihypertensive (β: −0.08; 95% CI: −0.10, −0.05; p < 0.001), only antihyperlipidemic (β: −0.10; 95% CI: −0.14, −0.06; p < 0.001), or both antihypertensive and antihyperlipidemic medications (β: −0.10; 95% CI: −0.16, −0.05; p < 0.001) (Table 4).
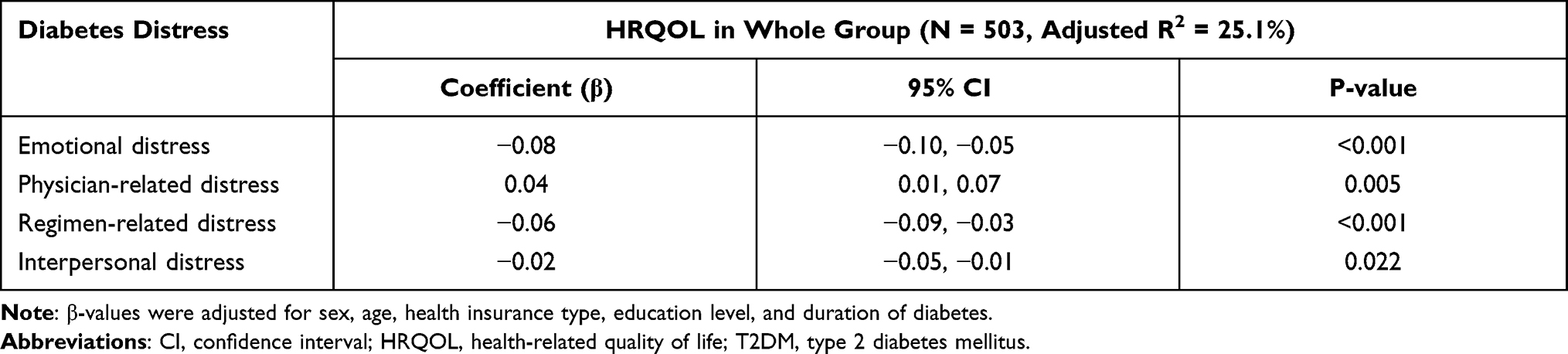 |
Table 3 Associations Between Different Types of Diabetes Distress and HRQOL in T2DM Patients Using Antihypertensive and/Or Antihyperlipidemic Medications |
 |
Table 4 Associations Between Different Types of Diabetes Distress and HRQOL per Therapeutic Subgroup Estimated from Multiple Linear Regression Analyses |
Higher regimen distress (β: −0.06; 95% CI: −0.09, −0.03; p < 0.001) and interpersonal distress (β: −0.02; 95% CI: −0.05, −0.01; p = 0.022) were associated with lower HRQOL among the whole group of patients (Table 3). These associations were also observed among those using only antihypertensive medication (Table 4). Surprisingly, higher physician distress was associated with higher HRQOL among the whole group of patients (β: 0.04; 95% CI: 0.01, 0.07, p = 0.005) (Table 3) and those using only antihypertensive medication (β: 0.04; 95% CI: 0.01, 0.07, p = 0.037) (Table 4).
Discussion
Emotional distress was the most common type of distress reported in T2DM patients using antihypertensive and/or antihyperlipidemic medications. This type of distress was significantly associated with lower HRQOL among the whole group and across the three therapeutic subgroups. Regimen-related and interpersonal distress were associated with lower HRQOL, whereas physician-related distress was associated with higher HRQOL among the whole group and those using only antihypertensive medication.
In this study, we found that emotional distress is the dominant type of diabetes distress among T2DM patients using antihypertensive and/or antihyperlipidemic medications. This finding is similar to that reported in a previous study in the US that demonstrated that T2DM patients with comorbidities experienced higher levels of emotional burden.32 This distress might partly be explained by patients feeling overwhelmed or frightened about the complexity of their treatment, including changes in treatment regimen or switching or adding medications.33 Although the distress levels were relatively similar, the lowest distress levels were seen in patients using only antihyperlipidemic medications. This is likely the group with a more simple treatment regimen compared with the treatment regimen of those using antihypertensive medications.
A relatively high HRQOL (mean EQ-5D-5L index of 0.8) was observed among the whole group and across all three therapeutic subgroups, indicating that patients did not experience severe problems regarding their mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. A previous study reported that the minimally important difference estimates of EQ-5D-5L in adults with type 2 diabetes were 0.043, 0.040, and 0.045 for all changes, improvement, and deterioration, respectively,34 indicating that meaningful improvements in our study population are still possible. The mean EQ-5D-5L index of 0.8 in our study is similar to that of patients with diabetes in Vietnam,35 but higher than that of such patients in Saudi Arabia.36 This can be partly explained by the inclusion of patients from primary healthcare settings, who are relatively healthy.
It was observed that the association between higher emotional distress and lower HRQOL among T2DM patients was independent of the use of antihypertensive and/or antihyperlipidemic medications. This indicates that emotional distress is relevant for patients’ HRQOL regardless of the type of comorbidity or medication. Previous studies reported conflicting results regarding whether hypertension or hyperlipidemia has more harmful effects on the psychological status of T2DM patients.5,17 However, patients with both hypertension and hyperlipidemia were excluded from those studies, which might have caused the differences in the findings. Furthermore, different HRQOL measures were used in those studies, which might hinder comparisons between study populations.37,38
Higher regimen-related and interpersonal distress were associated with lower HRQOL in the whole group and those using only antihypertensive medication. This indicates that focusing on reducing regimen complexity and increasing family support are relevant in addressing regimen-related and interpersonal distress experienced by patients with T2DM. Surprisingly, regimen-related distress was somewhat lower in those using both antihypertensive and antihyperlipidemic medications. Perhaps these patients already received more support. Also, no association with HRQOL was observed for this group. This can be partly explained by the lower distress score and the lower number of patients, thereby resulting in lower statistical power. Finally, it was observed that higher physician-related distress was associated with higher HRQOL in the whole group, which was an unexpected result and could be considered, in the light of our limitations, to be influenced by an unmeasured confounder or a chance finding.
The strength of this study is that the differences and similarities in associations of different types of diabetes distress with HRQOL were analyzed across different therapeutic subgroups. Furthermore, we were able to better understand which specific type of diabetes distress was associated with HRQOL and needs further attention. The high response rate in this study indicates that our findings are generalizable for T2DM patients who visit CHCs in Indonesia. Moreover, this study was conducted as a multicenter survey in different cities in Indonesia, further strengthening the generalizability of our findings.
Nevertheless, some limitations need to be addressed. We may have underestimated diabetes distress and overestimated HRQOL owing to social desirability and recall bias. Due to the cross-sectional study approach, no causal association between diabetes distress and HRQOL can be made. Moreover, our models had a relatively low adjusted R2. This implies that other unmeasured factors may be associated with HRQOL to varying degrees, for example, the severity of each chronic condition, the number of medications, other comorbidities, lifestyle advice, or personal circumstances. Such information could not be obtained herein. Additionally, most patients who participated in our study were those who regularly visited the CHCs and did not have severe diabetes distress or very low HRQOL. Further studies should evaluate the association between different types of diabetes distress and HRQOL in less controlled T2DM patients using antihypertensive and/or antihyperlipidemic medications. Finally, multiple testing, which may lead to chance findings, was conducted. However, the associations for emotional and interpersonal distress in our main analysis showed significance levels of p < 0.001.
These findings emphasize the urgent need for developing interventions to prevent and reduce diabetes distress in T2DM patients with comorbidities to improve their HRQOL. These could be tailored interventions considering that diabetes distress is highly responsive to such interventions.39 Screening for diabetes distress, in particular patients’ emotional distress, is needed for managing diabetes and its comorbidities.
Conclusion
Emotional distress affects HRQOL in T2DM patients treated for cardiovascular comorbidities, independent of the use of antihypertensive and/or antihyperlipidemic medications.
Role of the Funder
The funding body did not have any role in designing the study, in collecting data, in analyzing and interpreting data, in drafting the manuscript, and in deciding to submit the manuscript for publication.
Acknowledgment
We thank all patients and research assistants for their support and contribution.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Universitas Padjadjaran (No: 1427/UN6.RKT/LT/2019) to RA.
Disclosure
The authors report no conflicts of interest for this work.
References
1. American Diabetes Association. 9. Cardiovascular disease and risk management: standards of medical care in diabetes-2018. Diabetes Care. 2018;41(Suppl 1):S86–104. doi:10.2337/dc18-S009
2. International Diabetes Federation (IDF). IDF Diabetes Atlas. 2017. http://www.diabetesatlas.org/resources/2017-atlas.html.
3. Dennick K, Sturt J, Hessler D, et al. High rates of elevated diabetes distress in research populations: a systematic review and meta-analysis. Int Diabetes Nurs. 2015;12(3):93–107. doi:10.1080/20573316.2016.1202497
4. Chew BH, Vos R, Mohd-Sidik S, Rutten GE. Diabetes-Related distress, depression and Distress-Depression among adults with type 2 diabetes mellitus in Malaysia. PLoS One. 2016;11(3):e0152095. doi:10.1371/journal.pone.0152095
5. Chew BH, Mohd-Sidik S, Shariff-Ghazali S. Negative effects of diabetes-related distress on health-related quality of life: an evaluation among the adult patients with type 2 diabetes mellitus in three primary healthcare clinics in Malaysia. Health Qual Life Outcomes. 2015;13(1). doi:10.1186/s12955-015-0384-4
6. Bruno BA, Choi D, Thorpe KE, Yu CH. Relationship among diabetes distress, decisional conflict, quality of life, and patient perception of chronic illness care in a cohort of patients with type 2 diabetes and other comorbidities. Diabetes Care. 2019;42(7):1170–1177. doi:10.2337/dc18-1256
7. Fisher L, Mullan JT, Arean P, Glasgow RE, Hessler D, Masharani U. Diabetes distress but not clinical depression or depressive symptoms is associated with glycemic control in both cross-sectional and longitudinal analyses. Diabetes Care. 2010;33(1):23–28. doi:10.2337/dc09-1238
8. Fisher L, Skaff MM, Mullan JT, et al. Clinical depression versus distress among patients with type 2 diabetes: not just a question of semantics. Diabetes Care. 2007;30(3):542–548. doi:10.2337/dc06-1614
9. Polonsky WH, Fisher L, Earles J, et al. Assessing psychosocial distress in diabetes: development of the Diabetes Distress Scale. Diabetes Care. 2005;28(3):626–631. doi:10.2337/diacare.28.3.626
10. Young-Hyman D, De Groot M, Hill-Briggs F, Gonzalez JS, Hood K, Peyrot M. Psychosocial care for people with diabetes: a position statement of the American diabetes association. Diabetes Care. 2016;39(12):2126–2140. doi:10.2337/dc16-2053
11. Johnson EL, Feldman H, Butts A, et al. Standards of medical care in diabetes—2019 abridged for primary care providers. Clin Diabetes. 2019;37(1):11–34.
12. Skinner TC, Joensen L, Parkin T. Twenty‐five years of diabetes distress research. Diabet Med. 2019;37(3):
13. Arifin B, van Asselt ADI, Setiawan D, Atthobari J, Postma MJ, Cao Q. Diabetes distress in Indonesian patients with type 2 diabetes: a comparison between primary and tertiary care. BMC Health Serv Res. 2019;19(1):773. doi:10.1186/s12913-019-4515-1
14. Gómez-Pimienta E, González-Castro TB, Fresan A, et al. Decreased quality of life in individuals with type 2 diabetes mellitus is associated with emotional distress. Int J Environ Res Public Health. 2019;16(15):2652. doi:10.3390/ijerph16152652
15. Carper MM, Traeger L, Gonzalez JS, Wexler DJ, Psaros C, Safren SA. The differential associations of depression and diabetes distress with quality of life domains in type 2 diabetes. J Behav Med. 2014;37:501–510. doi:10.1007/s10865-013-9505-x
16. Trikkalinou A, Papazafiropoulou AK, Melidonis A. Type 2 diabetes and quality of life. World J Diabetes. 2017;8(4):120. doi:10.4239/wjd.v8.i4.120
17. Papadopoulos AA, Kontodimopoulos N, Frydas A, Ikonomakis E, Niakas D. Predictors of health-related quality of life in type II diabetic patients in Greece. BMC Public Health. 2007;7(1):186. doi:10.1186/1471-2458-7-186
18. Daher AM, AlMashoor SAH, Winn T. Glycaemic control and quality of life among ethnically diverse Malaysian diabetic patients. Qual Life Res. 2015;24(4):951–958. doi:10.1007/s11136-014-0830-5
19. Landman GWD, Van Hateren KJJ, Kleefstra N, Groenier KH, Gans ROB, Bilo HJG. Health-related quality of life and mortality in a general and elderly population of patients with type 2 diabetes (ZODIAC-18). Diabetes Care. 2010;33(11):2378–2382. doi:10.2337/dc10-0979
20. Pentakota SR, Miller DR, Rajan M, et al. Does diabetes care differ by type of chronic comorbidity?: an evaluation of the Piette and Kerr framework. Diabetes Care. 2012;35(6):1285–1292. doi:10.2337/dc11-1569
21. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
22. Farm BAS, Perwitasari DA, Thobari JA, Cao Q, Krabbe PFM, Postma MJ. Translation, revision, and validation of the Diabetes Distress Scale for Indonesian type 2 diabetic outpatients with various types of complications. Value Heal Reg Issues. 2017;12:63–73. doi:10.1016/j.vhri.2017.03.010
23. Rabin R, De Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med. 2001;33(5):337–343. doi:10.3109/07853890109002087
24. Arifin B, Purba FD, Herman H, et al. Comparing the EQ-5D-3 L and EQ-5D-5 L: studying measurement and scores in Indonesian type 2 diabetes mellitus patients. Health Qual Life Outcomes. 2020;18(1):22. doi:10.1186/s12955-020-1282-y
25. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727–1736. doi:10.1007/s11136-011-9903-x
26. Purba FD, Hunfeld JAM, Iskandarsyah A, et al. The Indonesian EQ-5D-5L Value Set. Pharmacoeconomics. 2017;35(11):1153–1165. doi:10.1007/s40273-017-0538-9
27. Sayah F, Qiu W, Xie F, Johnson JA. Comparative performance of the EQ-5D-5L and SF-6D index scores in adults with type 2 diabetes. Qual Life Res. 2017;26(8):2057–2066. doi:10.1007/s11136-017-1559-8
28. Mulhern B, Meadows K. The construct validity and responsiveness of the EQ-5D, SF-6D and Diabetes Health Profile-18 in type 2 diabetes. Health Qual Life Outcomes. 2014;12(1):1–10. doi:10.1186/1477-7525-12-42
29. Green SB. How many subjects does it take to do a regression analysis? Multivariate Behav Res. 1991;26(3):499–510. doi:10.1207/s15327906mbr2603_7
30. Gravetter FJ, Wallnau LB. Essentials of Statistics for the Behavioral Sciences. Belmont, CA: Wadsworth; 2014.
31. George D, Paul Mallery W. SPSS for Windows Step by Step a Simple Guide and Reference Fourth Edition (11.0 Update) Answers to Selected Exercises. Boston: Pearson; 2010.
32. Baek RN, Tanenbaum ML, Gonzalez JS. Diabetes burden and diabetes distress: the buffering effect of social support. Ann Behav Med. 2014;48(2):145–155. doi:10.1007/s12160-013-9585-4
33. Tran VT, Montori VM, Ravaud P. Is my patient overwhelmed?: determining thresholds for acceptable burden of treatment using data from the ComPaRe e-Cohort. Mayo Clin Proc. 2020;95(3):504–512. doi:10.1016/j.mayocp.2019.09.004
34. McClure N, Sayah F, Ohinmaa A, Johnson J. Minimally Important Difference of the EQ-5D-5L Index Score in Adults with Type 2 Diabetes. Value Health. 2018;21(9):1090–1097. doi:10.1016/j.jval.2018.02.007
35. Thi H, Nguyen T, Luong LH. Health-related quality of life in elderly diabetic outpatients in Vietnam. Patient Prefer Adherence. 2018;12:1347–1354. doi:10.2147/PPA.S162892
36. Al-Aboudi I, Hassali M, Aa S. Knowledge, attitudes, and quality of life of type 2 diabetes patients in Riyadh, Saudi Arabia. J Pharm Bioallied Sci. 2016;8(3):195–202. doi:10.4103/0975-7406.171683
37. Pequeno NPF, Pequeno NPF. Quality of life assessment instruments for adults: a systematic review of population-based studies. Health Qual Life Outcomes. 2020;18(1):208. doi:10.1186/s12955-020-01347-7
38. Haraldstad K, Wahl A, Andenæs R, et al. A systematic review of quality of life research in medicine and health sciences. Qual Life Res. 2019;28(10):2641–2650. doi:10.1007/s11136-019-02214-9
39. Fisher L, Hessler D, Glasgow RE, et al. REDEEM: a pragmatic trial to reduce diabetes distress. Diabetes Care. 2013;36(9):2551–2558. doi:10.2337/dc12-2493
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.