Back to Journals » Journal of Pain Research » Volume 19
Emergency Department Presentations for Jellyfish Stings in Southern China: A Cross-Sectional Analysis of Pain Severity and Treatment Timing
Authors Li X, Wang H, Guo X, Huo C, Jiang M, Zhang J
Received 3 November 2025
Accepted for publication 15 March 2026
Published 19 March 2026 Volume 2026:19 576516
DOI https://doi.org/10.2147/JPR.S576516
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Xin Li,1,2,* Huiying Wang,3,* Xiaoyang Guo,4,* Cong Huo,5 Mingyue Jiang,6 Jie Zhang6,7
1Graduate School, Chinese People’s Liberation Army Medical School, Beijing, People’s Republic of China; 2Department of Respiratory Critical Care Unit, The Second Medical Center and National Clinical Research Center for Geriatric Diseases of Chinese People’s Liberation Army General Hospital, Beijing, People’s Republic of China; 3Department of Medical Services, the Sixth Medical Center of Chinese People’s Liberation Army General Hospital, Beijing, People’s Republic of China; 4Department of Ultrasound, the 305 Hospital of Chinese People’s Liberation Army, Beijing, People’s Republic of China; 5Department of Pulmonary and Critical Care Medicine, Hainan Hospital of Chinese People’s Liberation Army General Hospital, Sanya, Hainan, People’s Republic of China; 6School of Nursing, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 7Department of Nursing, the Ninth Medical Center of Chinese People’s Liberation Army General Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jie Zhang, Department of Nursing, the Ninth Medical Center of Chinese People’s Liberation Army General Hospital, No. 9, Anxiang Beili Street, Chaoyang District, Beijing, People’s Republic of China, Tel +86 15011477062, Email [email protected]
Purpose: To analyze and discuss the clinical characteristics of jellyfish stings in the South China Sea and to identify factors associated with post-sting pain.
Patients and Methods: The study population included individuals stung by jellyfish along the coasts of Hainan and Guangdong Provinces, recruited from two regional hospital emergency departments.A cross-sectional study was conducted using a structured questionnaire. Univariate and multivariate logistic regression analyses were performed on the collected data. Pain intensity was assessed using the Numerical Rating Scale (NRS) and used as the basis for grouping participants. Receiver operating characteristic (ROC) curve analysis was applied to determine the optimal time interval between sting occurrence and medical treatment.
Results: A total of 436 questionnaires were distributed, and 376 were returned (response rate: 87.6%). After screening, 316 valid questionnaires were included in the final analysis (validity rate: 84.0%). Based on NRS scores, participants were categorized into three groups: Group 1 (mild pain, NRS 0– 3), Group 2 (moderate pain, NRS 4– 6), and Group 3 (severe pain, NRS 7– 10). Baseline characteristics were comparable across the three groups. Univariate analysis identified eight factors associated with NRS scores: sting on the face or neck, sting on the chest or abdomen, skin edema, skin wound bleeding, skin wound infection, seawater rinsing, hot compress/hot water immersion, and time interval from sting to medical treatment (all P < 0.05). Multivariate logistic regression revealed six independent predictors of higher pain scores: sting on the face or neck, skin edema, skin wound bleeding, seawater rinsing, and hot compress/hot water immersion (all P < 0.05). ROC curve analysis indicated that receiving medical treatment within 28 minutes of the sting was associated with significant pain relief. However, it may be delayed due to logistics and transportation time.
Conclusion: Multiple factors influence pain severity following jellyfish stings. Prompt and appropriate initial non-pharmacological management, followed by timely medical treatment preferably within 28 minutes can help alleviate pain and improve clinical outcomes.
Keywords: jellyfish sting, risk factor, post-sting pain, numerical rating scale
Introduction
Jellyfish are marine invertebrates belonging to the phylum Cnidaria. They exhibit remarkable species diversity and large population sizes and are widely distributed across all major oceans worldwide.1 Numerous nematocysts containing toxins are located on the surface of their tentacles. When humans come into contact with these tentacles, the nematocysts rapidly discharge their stinging threads, which penetrate the skin and inject toxins.2 Jellyfish venom is characterized by complex and diverse biochemical components with potent biological activity. It can induce a wide range of clinical manifestations of varying severity, including pain of different intensities, local erythema and edema, cardiovascular reactions, dyspnea, Irukandji syndrome, acute systemic allergic responses, anaphylactic shock, and, in severe cases, death. These effects can result in varying degrees of health impairment among affected individuals.3–5
In recent years, the number of reported jellyfish sting cases has risen sharply in many coastal cities worldwide. This trend may be associated with global warming and the deterioration of marine environments resulting from industrial activities.6–8 It is estimated that approximately 150 million jellyfish stings occur globally each year.9 In Australia, 6,769 emergency cases related to marine animal stings were reported during 2022–2023.10 Countries such as Thailand, Malaysia, and the Philippines have also reported varying numbers of jellyfish sting cases, including fatalities.11,12 China, with its extensive coastline of 32,000 kilometers and numerous coastal beaches, also experiences a high incidence of jellyfish stings. For instance, in Qinhuangdao—a popular coastal tourist destination in northern China—approximately 2,724 cases were documented during the summer seasons between 2017 and 2019.13 The rising incidence not only adversely affects tourism but also poses a significant public health burden, contributing to increased medical expenditures, as evidenced by reports from Italy where medical expenses associated with stings reached up to 400,000 euros over five years.14,15
Despite the growing public health concern, data on the clinical characteristics of jellyfish stings in the southern marine regions of China remain limited. Specifically, there is a lack of comprehensive analysis regarding the risk factors that contribute to the severity of sting symptoms, particularly post-sting pain, in areas like Hainan and Guangdong Provinces. Understanding these local epidemiological and clinical features is crucial for developing targeted treatment strategies and public health interventions.
Therefore, this study aims to investigate the clinical characteristics of patients stung by Portuguese man-of-war and jellyfish (Cyanea) in Hainan and Guangdong Provinces, located in the southern marine regions of China, and to identify the risk factors associated with the severity of post-sting pain.
Methods
Study Design and Participants
This cross-sectional study was conducted from August 2023 to October 2024. Participants were recruited from two large medical institutions in southern China, both located within the South China Sea region: the Hainan Hospital of the PLA General Hospital (Hainan Province) and the 196th Hospital of the PLA (Guangdong Province). Questionnaires were distributed on-site to patients who presented to the emergency departments (EDs) of these hospitals for medical treatment following a jellyfish sting. The surveys were administered with nurse assistance, and relevant data were collected retrospectively at the time of medical consultation.
Inclusion criteria: Participants were eligible if they (1) were aged 18–60 years, (2) sought ED treatment for a clinically confirmed jellyfish sting, and (3) voluntarily provided informed consent to participate in the questionnaire survey. Exclusion criteria: Participants were excluded if they (1) were pregnant or lactating, (2) were unable to complete the questionnaire independently, or (3) had a history of mental illness or other conditions that could interfere with pain assessment.
This study was reviewed and approved by the Ethics Committee of the Sixth Medical Center of the Chinese PLA General Hospital. Written informed consent was obtained from all participants prior to data collection. The study was registered at ClinicalTrials.gov (Registration Number: ChiCTR2400093701).
Outcome Measurement and Group Setting
Outcome Measurement
The primary outcome measure of this cross-sectional study was pain intensity following a jellyfish sting, derived from the “pain level” item in the questionnaire. This served as the key indicator reflecting the severity of sting-related discomfort. Pain intensity was quantified using the NRS a validated and widely used instrument for clinical pain assessment. Participants were asked to rate their maximum pain intensity within one hour of presentation to the ED on an 11-point scale, where 0 represented “no pain at all” and 10 indicated “the worst pain imaginable.”
Secondary outcome measures included the following: (1) Sting site: categorized by common anatomical regions (eg., face/neck, chest/abdomen, back/waist, limbs) based on participants’ self-report and nurse verification. (2) Local symptoms: recorded as binary variables (yes/no) for manifestations including skin erythema, skin edema, skin wound bleeding, and skin wound infection. (3) Systemic symptoms: recorded as binary variables (yes/no) for symptoms such as fever, dyspnea, and abdominal pain, nausea, or vomiting. (4) Time interval from sting to medical treatment: defined as the duration between sting occurrence and receipt of medical care in the ED. (5) Non-pharmacological interventions: recorded as binary variables (yes/no) for first-aid measures applied before ED presentation, including seawater rinsing, fresh water rinsing, vinegar rinsing, hot compress or hot water immersion, and ice compress or cold water immersion.
Group Setting
Participants were stratified according to the core outcome indicator pain intensity as assessed by the NRS to compare differences in other outcome variables across varying levels of pain severity. Based on established clinical pain classification standards and the distribution characteristics of jellyfish sting–related pain, participants were divided into three groups: (1) mild pain group, NRS score 0–3; (2) moderate pain group, NRS score 4–6; and (3) severe pain group, NRS score 7–10.16
This grouping approach was both objective and quantifiable, consistent with the assessment logic of the primary outcome measure. It provided a robust framework for subsequent analyses of factors associated with pain severity among jellyfish sting patients.
Questionnaire
A self-administered questionnaire was used to collect data on jellyfish sting–related information and participant characteristics. Two formats online and offline were implemented to accommodate different participant needs.
Questionnaire Content
The questionnaire was organized into two sections to ensure systematic data collection. The first section, demographic and baseline characteristics, included items such as gender, age, body mass index (BMI), marital status, occupational category, education level, smoking habits, and drinking habits. The second section, jellyfish sting-specific information, focused on details of the sting event and subsequent outcomes, including pain level (quantified using the Numerical Rating Scale, NRS), sting site, local and systemic symptoms, time interval from sting occurrence to initiation of medical treatment, non-pharmacological interventions applied, treatment type (outpatient or inpatient), and length of hospital stay for inpatients.
Questionnaire Administration
The online version was implemented via Questionnaire Star, a free and widely used online survey platform in China. Researchers designed and edited the questionnaire on the platform’s official website, which automatically generated a unique QR code. Participants were instructed to scan the QR code using WeChat China’s primary social media and messaging application to complete the survey electronically. The offline version consisted of traditional paper-based questionnaires, which participants completed on-site in the emergency departments of the participating hospitals. All questionnaires were reviewed immediately upon completion by trained nurses to check for missing data or logically inconsistent responses, thereby enhancing data completeness and accuracy.
Questionnaire Data Collection
For the online data, participant responses were automatically uploaded to the official Questionnaire Star database upon completion. Researchers accessed the collected data through the platform and downloaded an Excel file containing all survey items and corresponding responses. For the offline data, designated staff at the participating hospitals were responsible for collecting the completed paper-based questionnaires. These questionnaires were then uniformly mailed to the corresponding author’s affiliated institution, where members of the research team securely stored and entered the data into Microsoft Excel for digitization. Finally, the online and offline datasets were merged to form the final raw dataset used for statistical analysis.
Statistical Analysis
Continuous variables with a normal distribution were expressed as the mean ± standard deviation (SD), while non-normally distributed continuous variables were presented as the median and interquartile range (IQR). Continuous variables were compared using the Student’s t-test, and categorical variables were expressed as frequencies or percentages and analyzed using the chi-square test. For univariate and multivariate analyses, all participants were categorized into three groups according to their NRS pain scores. The mild pain group served as the reference category for comparisons with the moderate pain and severe pain groups. Statistical analyses were performed using SPSS version 24.0 (IBM Corp., Armonk, NY, USA). Initially, univariate analyses were conducted for each variable, and those with P < 0.10 were subsequently included in the multivariate logistic regression analysis. A P-value < 0.05 was considered statistically significant.
Result
Data Collection and Sample Screening
Between August 2023 and October 2024, a total of 436 questionnaires were distributed. Of these, 376 were returned, yielding a response rate of 87.6%. After screening, 316 questionnaires containing complete and valid data were included in the final analysis. The remaining 60 questionnaires were excluded: 42 due to incomplete data and 18 because the respondents did not meet the inclusion or exclusion criteria (Figure 1).
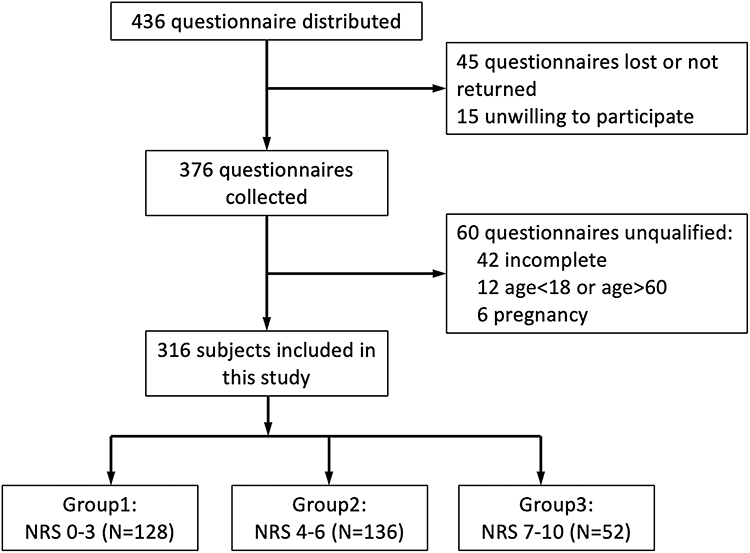 |
Figure 1 Flow chart of participant enrollment and screening. |
Baseline Characteristics
All participants assessed pain intensity using the NRS, an 11-point scale ranging from 0 (no pain) to 10 (the most severe pain imaginable).16 Participants were stratified into three groups based on NRS scores: mild pain (0–3), moderate pain (4–6), and severe pain (7–10). Detailed characteristics of respondents are summarized in Table 1.
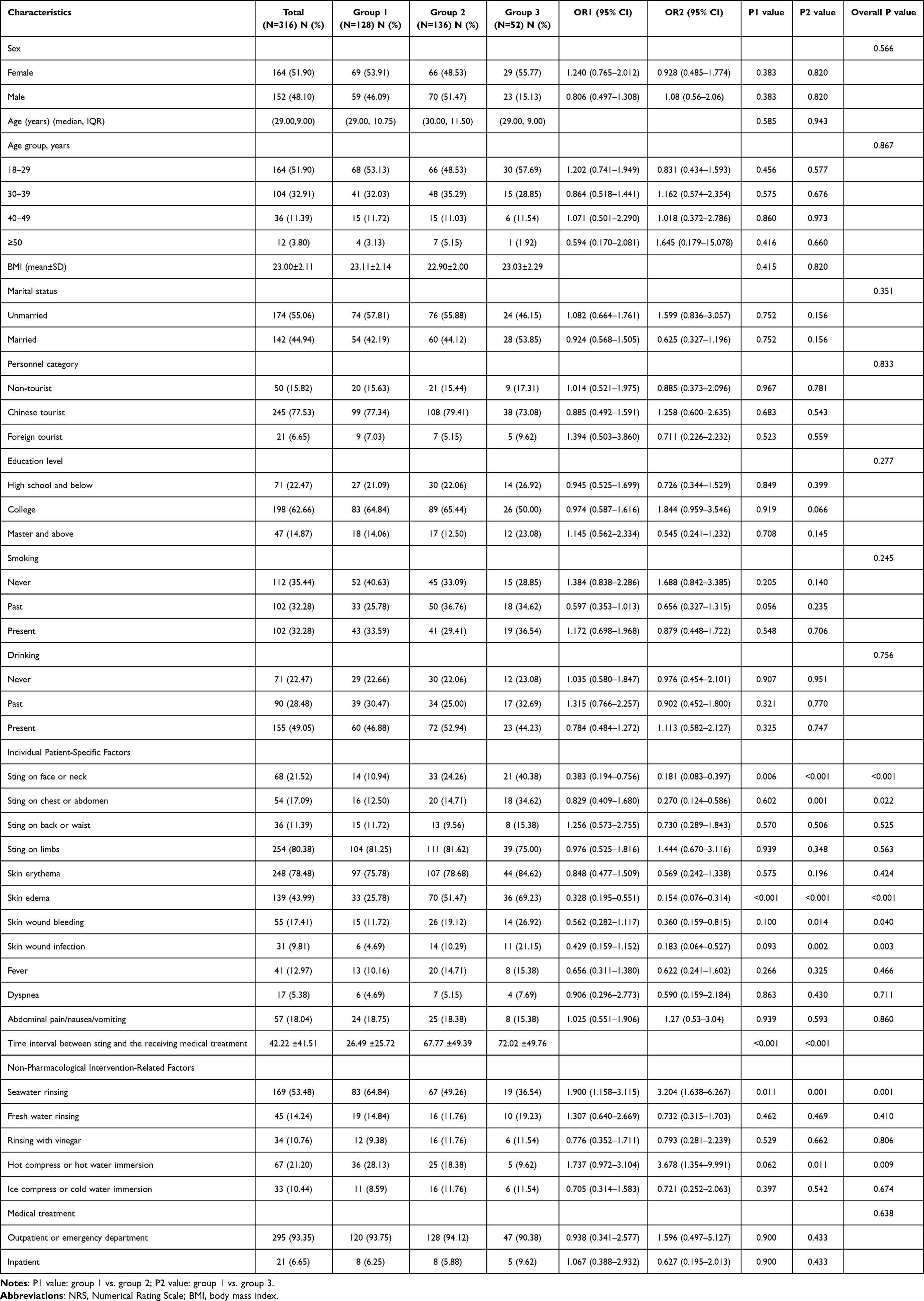 |
Table 1 Univariate Analysis of the Associations Between Three Groups According to NRS |
Among the 316 participants, 152 were male (48.10%) and 164 were female (51.90%). The median age was 29 years (range 18–57 years), with 51.90% aged 18–29, 32.91% aged 30–39, 11.39% aged 40–49, and 3.80% aged ≥50. The mean BMI was 23.00 ± 2.11 kg/m2. Most participants (84.18%, 266/316) were tourists, including 245 Chinese tourists (77.53%) and 21 foreign tourists (6.65%). The remaining 15.82% (50/316) were non-tourists, such as divers, fishermen, or members of maritime rescue teams.
As shown in Table 1, there were no statistically significant differences among the three pain groups regarding gender, age group, marital status, personnel category, education level, smoking habits, or drinking habits (all P > 0.05).
Univariate Analysis
Univariate analysis identified eight variables significantly associated with NRS pain scores (P < 0.05). The detailed results are presented below.
Sting Site
Face or neck stings: Among all participants, 21.52% (68/316) sustained stings to the face or neck. The proportion was highest in the severe pain group at 40.38% (21/52), significantly higher than in the mild pain group (10.94%, 14/128) and the moderate pain group (24.26%, 33/136). Compared with the severe pain group, the odds of face or neck stings were lower in the mild pain group (OR = 0.383, 95% CI: 0.194–0.765, P = 0.006) and in the moderate pain group (OR = 0.181, 95% CI: 0.083–0.397, P < 0.001) (Supplementary Figure 1).
Chest and abdomen stings: The overall incidence was 17.09% (54/316). In the severe pain group, 34.62% (18/52) of participants reported stings at these sites, which was significantly higher than in the mild pain group (12.50%, 16/128) and moderate pain group (14.71%, 20/136). The odds of chest or abdomen stings were lower in the mild pain group compared with the severe pain group (OR = 0.270, 95% CI: 0.124–0.586, P = 0.001).
Back and waist stings: The overall incidence was 11.39% (36/316). No significant differences were observed among the three groups (overall P = 0.525).
Arms and legs stings: The overall incidence was 80.38% (254/316), with no significant differences across groups (overall P = 0.563) (Supplementary Figure 2).
Local Symptoms
Skin edema: The overall incidence of skin edema was 43.99% (139/316). The proportion was highest in the severe pain group at 69.23% (36/52), significantly higher than in the mild pain group (25.78%, 33/128) and the moderate pain group (51.47%, 70/136). Compared with the severe pain group, the odds of skin edema were lower in the mild pain group (OR = 0.328, 95% CI: 0.195–0.551, P < 0.001) and in the moderate pain group (OR = 0.154, 95% CI: 0.076–0.314, P < 0.001).
Skin wound bleeding: The overall incidence was 17.41% (55/316). No significant difference was observed between the mild pain and moderate pain groups (OR = 0.562, 95% CI: 0.282–1.117, P = 0.100). However, compared with the severe pain group, the incidence of skin wound bleeding was lower in the mild pain group (OR = 0.360, 95% CI: 0.159–0.815, P = 0.014). Overall, skin wound bleeding differed significantly among the three groups.
Skin wound infection: The overall incidence was 9.81% (31/316), with 21.15% (11/52) in the severe pain group. Compared with the severe pain group, the odds of wound infection were lower in the mild pain group (OR = 0.183, 95% CI: 0.064–0.527, P = 0.002), whereas no significant difference was observed between the mild and moderate pain groups (OR = 0.429, 95% CI: 0.159–1.152, P = 0.093).
Skin erythema: The overall incidence was 78.48% (248/316), with no significant differences among the three groups (overall P = 0.424).
Systemic Symptoms
No significant intergroup differences were found in fever (41/316, 12.97%), dyspnea (17/316, 5.38%), or abdominal pain/nausea/vomiting (57/316, 18.04%) (all P > 0.05).
Time Interval from Sting to Medical Treatment
The mean time from sting occurrence to receiving medical treatment across all participants was 42.22 ± 41.51 minutes. Stratified by pain severity, the mean interval was 26.49 ± 25.72 minutes in the mild pain group, 67.77 ± 49.39 minutes in the moderate pain group, and 72.02 ± 49.76 minutes in the severe pain group. Both the moderate and severe pain groups had significantly longer intervals compared with the mild pain group (P < 0.001 for both comparisons).
Non-Pharmacological Intervention–Related Factors
Seawater sinsing: The proportion of participants receiving seawater rinsing was highest in the mild pain group (64.84%, 83/128), compared with 49.26% (67/136) in the moderate pain group and 36.54% (19/52) in the severe pain group. Compared with the severe pain group, the odds of seawater rinsing were higher in the mild pain group (OR = 1.900, 95% CI: 1.158–3.115, P = 0.011) and the moderate pain group (OR = 3.204, 95% CI: 1.638–6.267, P = 0.001).
Hot compress or hot water immersion: The proportion in the mild pain group was 28.13% (36/128), higher than in the moderate (18.38%, 25/136) and severe (9.62%, 5/52) pain groups. Compared with the severe pain group, the odds were higher in the mild pain group (OR = 3.678, 95% CI: 1.354–9.991, P = 0.011). The difference between the mild and moderate pain groups was marginally significant (OR = 1.737, 95% CI: 0.972–3.104, P = 0.062).
For fresh water rinsing (45/316, 14.24%), vinegar rinsing (34/316, 10.76%), and ice compress or cold water immersion (33/316, 10.44%): no significant intergroup differences were observed (all P > 0.05).
Seawater rinsing and hot compresses have a certain protective effect, possibly because hot compresses denature venom proteins, while seawater rinsing prevents nematocyst discharge, thereby alleviating pain and limiting local tissue damage.
Treatment Type
Among all participants, 295 cases (93.35%) received outpatient or emergency department care, including 120/128 (93.75%) in the mild pain group, 128/136 (94.12%) in the moderate pain group, and 47/52 (90.38%) in the severe pain group.
A total of 21 cases (6.65%) required inpatient treatment, comprising 8/128 (6.25%) in the mild pain group, 8/136 (5.88%) in the moderate pain group, and 5/52 (9.62%) in the severe pain group. No significant differences were observed among the groups in treatment type (P = 0.638).
Multivariate Analysis
To correct for potential confounding factors identified in the univariate analysis and to independently assess the association of each factor with pain severity, a multivariate ordinal logistic regression analysis was conducted. In accordance with the study objectives, all variables with P < 0.10 in the univariate analysis were included in the multivariate model. Simultaneously, to control for the potential confounding effects of demographic characteristics and behavioral habits, variables such as gender, age, marital status, personnel category (tourist/non-tourist), education level, smoking, and drinking habits were also incorporated into the model for adjustment. Variable selection for the final model was performed using a forward stepwise regression method based on maximum likelihood estimation. The analysis results are detailed in Table 2.
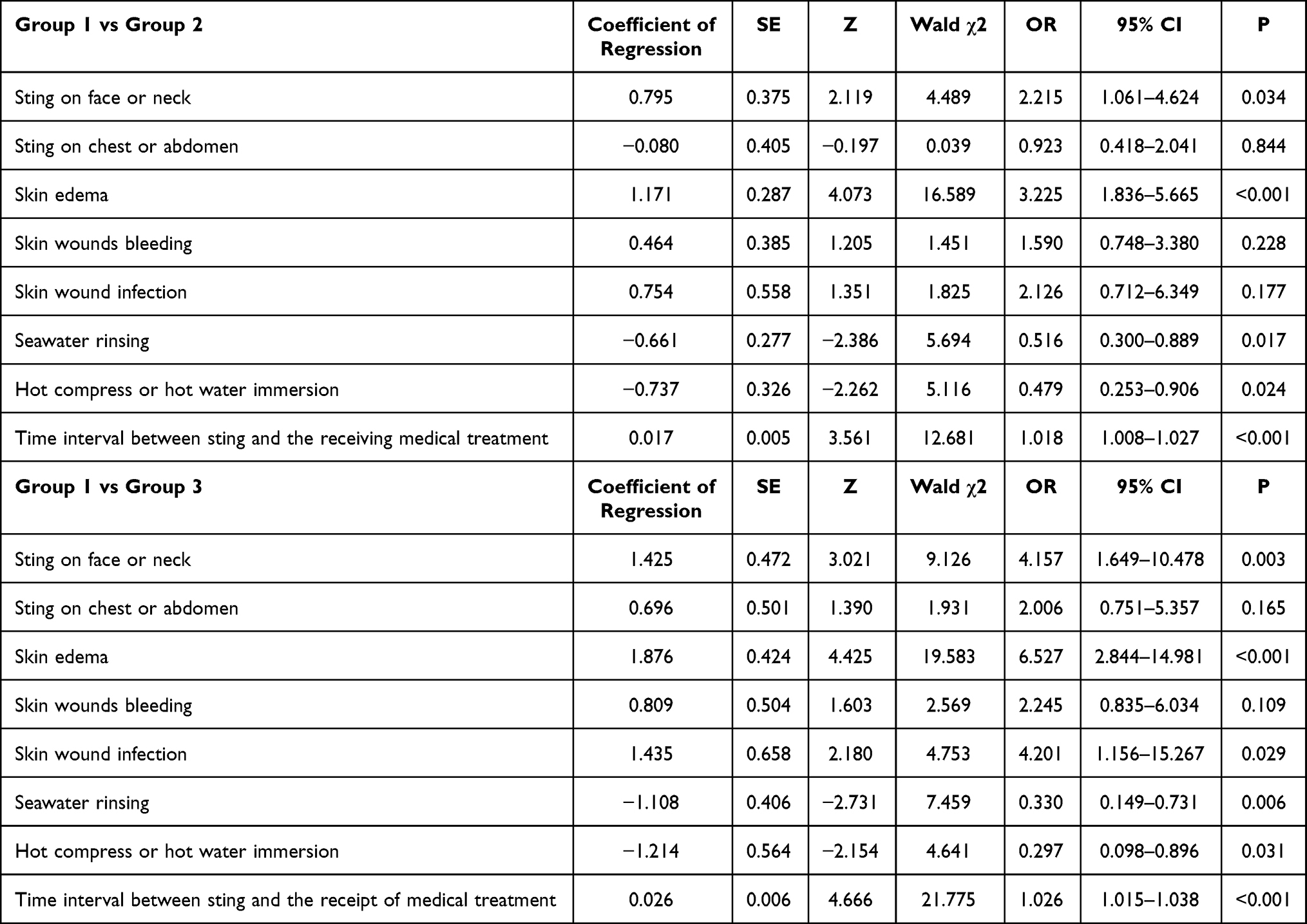 |
Table 2 Multivariate Logistics Analysis of the Association Between Potentially Significant Factors and NRS |
Group 1 vs Group 2
Five factors were independently associated with higher pain in the moderate pain group compared with the mild pain group: Sting on face or neck (OR = 2.215, 95% CI: 1.061–4.624, P = 0.034); Skin edema (OR = 3.225, 95% CI: 1.836–5.665, P < 0.001); Seawater rinsing (OR = 0.516, 95% CI: 0.300–0.889, P = 0.017); Hot compress or hot water immersion (OR = 0.479, 95% CI: 0.253–0.906, P = 0.024); Time interval from sting to medical treatment (OR = 1.018, 95% CI: 1.008–1.027, P < 0.001).
Group 1 vs. Group 3
Six factors were independently associated with higher pain in the severe pain group compared with the mild pain group: Sting on face or neck (OR = 4.157, 95% CI: 1.649–10.478, P = 0.003); Skin edema (OR = 6.527, 95% CI: 2.844–14.981, P < 0.001); Skin wound infection (OR = 4.201, 95% CI: 1.156–15.267, P = 0.029); Seawater rinsing (OR = 0.330, 95% CI: 0.149–0.731, P = 0.006); Hot compress or hot water immersion (OR = 0.297, 95% CI: 0.098–0.896, P = 0.031); Time interval from sting to medical treatment (OR = 1.026, 95% CI: 1.025–1.038, P < 0.001).
ROC Curve and Cut-off Value
ROC curve analysis was performed to evaluate the discriminative ability of the time interval from sting to medical treatment in predicting pain severity. Mild vs. moderate pain (Group 1 vs. Group 2): The area under the curve (AUC) was 0.654 (95% CI: 0.589–0.719, P < 0.001). The optimal cut-off value for the time interval was 28.0 minutes, corresponding to a sensitivity of 0.618 and a specificity of 0.609. Mild vs. severe pain (Group 1 vs. Group 3): The AUC was 0.846 (95% CI: 0.787–0.904, P < 0.001), indicating stronger discriminative power compared with the mild vs. moderate comparison. The optimal cut-off value remained 28.0 minutes, with a higher sensitivity of 0.904 and specificity of 0.609 (Figure 2; Table 3).
 |
Table 3 ROC Curve of the Time Interval Between Sting Occurrence and the Receiving Medical Treatment Among Three Groups (Min) |
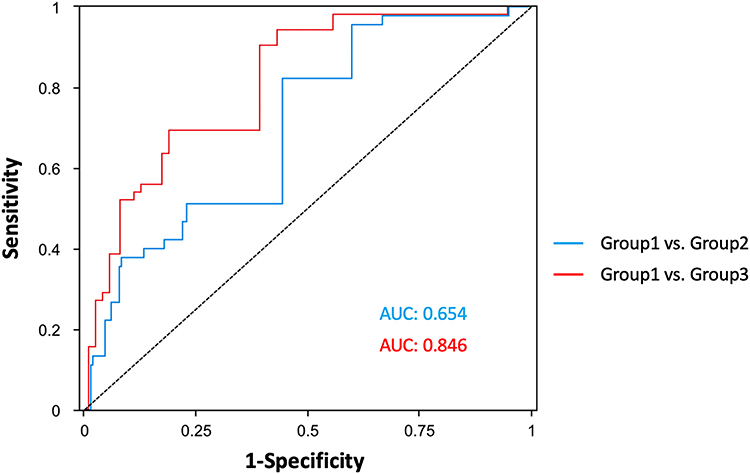 |
Figure 2 ROC curve for the time interval between sting and the receiving medical treatment among three groups. |
Discussion
Jellyfish stings can induce a range of symptoms resulting from the human immune response to jellyfish venom, which acts as an allergen. Jellyfish toxins are broadly categorized into three types: protein-like toxins, non-protein toxins, and bioactive enzymes. These bioactive components exhibit diverse biological toxicities, including skin damage, inflammation, allergic reactions, and adverse effects on the cardiovascular and nervous systems.17,18 Typically, following a jellyfish sting, the victim initially experiences stinging pain, followed by the development of erythema and papules on the skin, often with linear or rope-like marks resembling jellyfish tentacles.19 Patients may also experience varying degrees of pain, itching, burning, or numbness. In severe cases, the skin can develop blisters, bleeding, ulcers, or even necrosis.5,20 When a large amount of venom enters the bloodstream, systemic symptoms such as dyspnea, dizziness, nausea, and vomiting may occur, potentially leading to acute, life-threatening complications including cardiac arrest and hepatic-renal failure.21,22
Individual Patient-Specific Factors
Regarding the site of the sting, stings on the face or neck were associated with higher pain intensity in both univariate and multivariate analyses, whereas stings on the chest or abdomen were significant only in univariate analysis. This difference may be explained by anatomical characteristics. The skin of the face, neck, and chest is relatively thin and contains less subcutaneous tissue compared with the limbs, lacking the protective thickness of the stratum corneum and abundant adipose tissue especially in the head and neck. This thin skin, coupled with minimal subcutaneous fat, allows jellyfish venom to rapidly penetrate the skin barrier, directly stimulating nociceptors and triggering intense pain. Additionally, the head, face, and neck have a denser distribution of nerves (eg., the trigeminal nerve in the face) compared with the limbs and lumbodorsal region, leading to faster and more intense pain perception.23 In contrast, the relatively sparse distribution of pain-sensing nerves in the chest and abdomen may explain why stings in these areas were significant only in univariate analysis.
Our survey also showed that 78.48% (248/316) of participants developed skin erythema, making it the most common symptom. However, erythema did not significantly affect pain perception. The development of erythema may involve jellyfish venom components such as histamine, 5-hydroxytryptamine, and kinins, which act on the skin to induce non-specific cutaneous lesions, including allergic contact dermatitis, resulting in erythema and papules.5,20
The second most common symptom was skin edema, which differed significantly among the three pain groups in both univariate (P < 0.001) and multivariate analyses (P < 0.001 or P = 0.001). The occurrence of skin edema may be related to kinin-like components in jellyfish venom, which act on small veins and capillaries in the local skin area, causing vasodilation and increased vascular permeability. This leads to plasma exudation into the interstitial space and results in localized edema.24
In this study, 17.41% (55/316) of patients experienced skin wound bleeding. This variable showed a statistically significant association with pain in the univariate analysis but was not significant in the multivariate analysis. Additionally, 9.81% (31/316) of patients developed skin wound infections of varying severity, which were significant in both univariate and multivariate analyses. Several factors may contribute to wound infection, including the sting site and the time interval before medical treatment. Our analysis indicated that patients with wound infections had a longer interval from sting occurrence to medical care compared with those without infection (P = 0.021) (Supplementary Table 1).
Non-Pharmacological Intervention-Related Factors
Our study found that seawater rinsing was beneficial for reducing pain in patients, as demonstrated in both univariate and multivariate analyses. Previous studies have shown that the nematocysts of Chrysaora quinquecirrha, Chiropsalmus quadrumanus, Physalia physalis, Nemopilema nomurai, and Carybdea brevipedalia do not discharge in seawater.25,26 In vitro experiments by Pyo et al26 confirmed that seawater did not induce nematocyst discharge in Nemopilema nomurai and Carybdea mora (a type of box jellyfish). In human skin tests, rinsing with seawater alleviated erythema and pain at the sting site, supporting the recommendation of seawater as a safe and effective first-aid solution for jellyfish stings. Seawater rinsing helps prevent further nematocyst discharge by maintaining osmotic balance around undischarged nematocysts. However, Doyle’s study reported that seawater rinsing could significantly increase venom secretion from Cyanea capillata.27 Although our results indicated that fresh water rinsing had no effect on patients’ skin pain, its use is still not recommended.
Regarding vinegar (acetic acid) application, Fenner reported that 4–6% acetic acid can inhibit nematocyst discharge in several common box jellyfish species, including Chironex fleckeri and Carybdea rastoni.28 Wilcox et al29 also found that vinegar could inhibit nematocyst discharge in certain Physalia species. Conversely, other studies have shown that vinegar may trigger nematocyst discharge and exacerbate pain.25,26,30 A systematic review including 19 studies on jellyfish sting management concluded that vinegar application generally worsened pain from stings caused by most jellyfish species, although it alleviated pain from stings by Physalia species.8
Our study revealed that hot compress or hot water immersion could relieve pain for jellyfish sting both in univariate and multivariate analysis. Loten’s randomised controlled trial (RCT) showed that immersion in water at 45° C for 20 minutes is an effective treatment for relieving pain from compared with ice pack application.31 Compared with cold or ice treatment, hot compresses are safer and more effective in alleviating localized pain.20,32 Ward et al believed that for common jellyfish stings in North America and Hawaii, hot compresses could improve the symptoms of the patients stung by jellyfish8 A meta-analysis of seven trials (435 participants) showed that hot water more effectively relieved pain from stings by Physalia species (portuguese man-of-war or bluebottle jellyfish).1 However, Isbister et al RCT conducted that hot water immersion was no more effective than icepacks for reducing the acute pain of box jellyfish stings33 Hot compresses may denature thermolabile proteins in jellyfish venom, thereby alleviating pain and limiting local tissue damage. Despite the high quality of Isbister’s study, its sample size was small (with only 42 cases in total). Therefore, the use of hot compresses is still recommended.
This study reveled that the aggravation of pain is also associated with the prolong of time interval between sting and medical treatment (P < 0.001 both in univariate and multivariate analysis). An ROC curve with AUC of 0.654 and 0.846 and a cut-off value of 28.000 (min) indicating that patients stung by jellyfish should receive medical treatment as soon as possible. However, this may be delayed due to logistics and transportation time. Although no study reported the shorten and appropriate time interval between sting and medical treatment, Wang’s study illustrated that the delayed jellyfish envenomation syndrome (DJES) with severe multiple organ dysfunction or systemic damage usually occurs 2 hours after being stung by a jellyfish.34
Pharmacological Treatment
DeClerck et al35 conducted studies using both human and in vitro models and found that wet compresses with sodium bicarbonate solution for 30 to 60 minutes not only prevented nematocyst discharge but also significantly reduced skin erythema. Other studies have confirmed that sodium bicarbonate solution can inhibit nematocyst discharge in Nemopilema nomurai and demonstrates therapeutic efficacy for jellyfish stings.2,20,36 Pek et al’s systematic review and meta-analysis further indicated that topical application of lidocaine gel can alleviate local skin symptoms, including pain.37 Similarly, Birsa et al25 reported that applying 10% or 15% lidocaine hydrochloride solution to the skin of sting victims provided immediate pain relief and significantly reduced the area of erythema and swelling. In the present study, data on pharmacological interventions administered during emergency department treatment were not collected. Therefore, future research should focus on evaluating the effects of pharmacological therapies on pain management in patients with jellyfish stings.
Given that tourists constitute the majority of affected individuals, specific preventive measures should be implemented in high-risk areas. These include: (1) installing warning signs at beaches during peak jellyfish seasons to alert visitors of potential hazards; (2) providing easily accessible first-aid stations with clear instructions for appropriate initial management; (3) training lifeguards and beach personnel in proper jellyfish sting first aid; and (4) distributing educational materials to tourists upon beach entry, emphasizing the importance of protective clothing and appropriate response protocols. Such targeted interventions may help reduce the incidence and severity of jellyfish stings among this vulnerable population.
Limitation
This study has several limitations. The study population design limits causal inference, as the associations identified between risk factors and pain severity should be interpreted as correlational rather than causal. First, the cross-sectional design limits causal inference, as the associations identified between risk factors and pain severity should be interpreted as correlational rather than causal. Second, participants’ understanding of the pain index may have varied, highlighting the need for trained personnel to educate and assist patients in completing the assessment accurately. Third, all data were self-reported, which may be subject to recall bias. Fourth, this study did not identify the specific jellyfish species responsible for the stings, which is a significant limitation given that different species possess venoms with varying compositions, toxicities, and optimal treatment approaches. Fifth, the non-pharmacological interventions recorded in this study were self-administered by patients before presenting to the hospital, and there was no standardization of these first-aid measures in terms of duration, technique, or water temperature for hot immersion. This lack of standardization may have introduced variability in the effectiveness of these interventions. Sixth, patients’ self-treatment decisions may have been influenced by their pain levels, prior knowledge, or access to first-aid resources at the beach, potentially introducing selection bias.
Conclusion
This cross-sectional survey revealed that jellyfish stings are a common occurrence on the beaches of the South China Sea in China, with tourists comprising the majority of affected individuals. This finding may be attributable to tourists’ limited awareness of local marine hazards and their tendency to engage in recreational water activities without adequate protective measures.
To reduce pain and prevent complications, several practical recommendations emerge from our findings. First, individuals entering the sea should wear protective clothing, with particular attention to the face, neck, and chest —areas identified in our multivariate analysis as being independently associated with more severe pain. The vulnerability of these anatomical sites likely relates to thinner skin and higher nerve ending density, which may amplify pain perception upon envenomation.
Second, following a sting, the affected area should be rinsed with seawater (rather than fresh water, which may trigger further nematocyst discharge), and hot compresses or hot water immersion can be applied to alleviate pain. The therapeutic effect of heat is biologically plausible, as elevated temperatures can denature the thermolabile proteins in jellyfish venom, thereby reducing pain and limiting local tissue damage.
Third, the time interval from sting to medical treatment emerged as a critical modifiable factor. For patients presenting with skin edema or bleeding, prompt medical treatment —preferably within the 28-minute window identified by our ROC analysis—is strongly recommended to reduce pain and prevent secondary infection. This finding underscores the importance of timely access to professional care and supports the establishment of first-aid protocols at coastal recreational areas.
Data Sharing Statement
Data sharing is not applicable to this article, as no datasets were generated or analyzed specifically for sharing beyond the current study. The data supporting the findings of this study are available from the corresponding author upon reasonable request and subject to institutional ethics approval.
Ethics Approval
This study was reviewed and approved by the Ethics Committee of the Sixth Medical Center of the Chinese PLA General Hospital (No. HZKY-PJ-2024-61). Our study was registered with ClinicalTrials.gov (ChiCTR2400093701). Our study complies with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Disclosure
All authors report no conflicts of interest in this work.
References
1. McGee RG, Webster AC, Lewis SR, et al. Interventions for the symptoms and signs resulting from jellyfish stings. Cochrane Database Syst Rev. 2023;6(6):CD009688. doi:10.1002/14651858.CD009688.pub3
2. Cegolon L, Heymann WC, Lange JH, et al. Jellyfish stings and their management: a review. Mar Drugs. 2013;11(2):523–14. doi:10.3390/md11020523
3. McIver LJ, Tjhung IG, Parish ST, et al. Irukandji sydrome in the Torres Strait: a series of 8 cases. Wilderness Environ Med. 2011;22(4):338–342. doi:10.1016/j.wem.2011.08.002
4. Nagai H, Takuwa K, Nakao M, et al. Isolation and characterization of a novel protein toxin from the Hawaiian box jellyfish (sea wasp) Carybdea alata. Biochem Biophys Res Commun. 2000;275(2):589–594. doi:10.1006/bbrc.2000.3352
5. Peng X, Liu KT, Chen JB, et al. Jellyfish stings: a review of skin symptoms, pathophysiology, and management. Med Sci Monit. 2024;30:e944265. doi:10.12659/MSM.944265
6. Lee SH, Hwang JS, Kim KY, et al. Contrasting effects of regional and local climate on the interannual variability and phenology of the Scyphozoan, Aurelia coerulea and Nemopilema nomurai in the Korean Peninsula. Diversity. 2021;13(5):214. doi:10.3390/d13050214
7. Hifumi T, Fukuchi Y, Otani N, et al. Clinical characteristics of jellyfish stings in Japan. Acute Med Surg. 2020;7(1):e469. doi:10.1002/ams2.469
8. Ward NT, Darracq MA, Tomaszewski C, et al. Evidence-based treatment of jellyfish stings in North America and Hawaii. Ann Emerg Med. 2012;60(4):399–414. doi:10.1016/j.annemergmed.2012.04.010
9. Monteiro S, Carvalho F, Freitas A, et al. Raising awareness on the clinical and forensic aspects of jellyfish stings: a worldwide increasing threat. Int J Environ Res Public Health. 2022;19(14):8430. doi:10.3390/ijerph19148430
10. Australia Surf Life Saving Annual Report 2022–2023. Available from: https://issuu.com/surflifesavingaustralia/docs/slsa_annualreport_2023?fr=xKAE9_zU1NQ.
11. Mohd Suan MA, Tan WL, Soelar SA, et al. Jellyfish stings on Langkawi Island, Malaysia. Med J Malaysia. 2016;71(4):161–165.
12. Premmaneesakul H, Sithisarankul P. Toxic jellyfish in Thailand. Int Marit Health. 2019;70(1):22–26. doi:10.5603/IMH.2019.0004
13. Wang YH, Li F, He JJ, et al. Investigation and prevention and control analysis of jellyfish stings along the Qinhuangdao waters during the summer vacation in 2017-2019. China J Emerg Resuscitation Disaster Med. 2022;17(12):1656–1658. (In Chinese).
14. De Donno A, Idolo A, Bagordo F, et al. Impact of stinging jellyfish proliferations along south Italian coasts: human health hazards, treatment and social costs. Int J Environ Res Public Health. 2014;11(3):2488–2503. doi:10.3390/ijerph110302488
15. Bosch-Belmar M, Giomi F, Rinaldi A, et al. Concurrent environmental stressors and jellyfish stings impair caged European sea bass (Dicentrarchus labrax) physiological performances. Sci Rep. 2016;6(6):27929. doi:10.1038/srep27929
16. Chiarotto A, Maxwell LJ, Ostelo RW, et al. Measurement properties of visual analogue scale, numeric rating scale, and pain severity subscale of the brief pain inventory in patients with low back pain: a systematic review. J Pain. 2019;20(3):245–263. doi:10.1016/j.jpain.2018.07.009
17. Jouiaei M, Yanagihara AA, Madio B, et al. Ancient venom systems: a review on cnidaria toxins. Toxins. 2015;7(6):2251–2271. doi:10.3390/toxins7062251
18. Yang F, Yang K, Wang Y, et al. Insights into the discovery and intervention of metalloproteinase in marine hazardous jellyfish. J Hazard Mater. 2024;472:134526. doi:10.1016/j.jhazmat.2024.134526
19. Kimball AB, Arambula KZ, Stauffer AR, et al. Efficacy of a jellyfish sting inhibitor in preventing jellyfish stings in normal volunteers. Wilderness Environ Med. 2004;15(2):102–108. doi:10.1580/1080-6032(2004)015[0102:EOAJSI]2.0.CO;2
20. Remigante A, Costa R, Morabito R, et al. Impact of scyphozoan venoms on human health and current first aid options for stings. Toxins. 2018;10(4):133. doi:10.3390/toxins10040133
21. D’Ambra I, Lauritano C. A review of toxins from cnidaria. Mar Drugs. 2020;18(10):507. doi:10.3390/md18100507
22. Gaudio FG, Johnson DE, DiLorenzo K, et al. Wilderness medical society clinical practice guidelines on anaphylaxis. Wilderness Environ Med. 2022;33(1):75–91. doi:10.1016/j.wem.2021.11.009
23. Wang J, Li Y, Wang M, et al. Localization of the center of the intramuscular nerve dense region of the suboccipital muscles: an anatomical study. Front Neurol. 2022;13:863446. doi:10.3389/fneur.2022.863446
24. Erin NM, Geoffrey KI. Jellyfish stings; 2024 [April 04, 2025]. Available from: https://www.uptodate.cn/contents/jellyfish-stings.
25. Birsa LM, Verity PG, Lee RF. Evaluation of the effects of various chemicals on discharge of and pain caused by jellyfish nematocysts. Comp Biochem Physiol C Toxicol Pharmacol. 2010;151(4):426–430. doi:10.1016/j.cbpc.2010.01.007
26. Pyo MJ, Lee H, Bae SK, et al. Modulation of jellyfish nematocyst discharges and management of human skin stings in Nemopilema nomurai and Carybdea mora. Toxicon. 2016;109:26–32. doi:10.1016/j.toxicon.2015.10.019
27. Doyle TK, Headlam JL, Wilcox CL, et al. Evaluation of Cyanea capillata sting management protocols using ex vivo and in vitro envenomation models. Toxins. 2017;9(7):215. doi:10.3390/toxins9070215
28. Fenner PJ, Williamson J, Callanan VI, et al. Further understanding of, and a new treatment for, “Irukandji” (Carukia barnesi) stings. Med J Aust. 1986;145(11–12):569,572–574. doi:10.5694/j.1326-5377.1986.tb139500.x
29. Wilcox CL, Headlam JL, Doyle TK, et al. Assessing the efficacy of first-aid measures in Physalia sp. envenomation, using solution- and blood agarose-based models. Toxins. 2017;9(5):149. doi:10.3390/toxins9050149
30. Fenner PJ, Williamson JA, Burnett JW, et al. First aid treatment of jellyfish stings in Australia. Response to a newly differentiated species. Med J Aust. 1993;158(7):498–501. doi:10.5694/j.1326-5377.1993.tb137588.x
31. Loten C, Stokes B, Worsley D, et al. A randomised controlled trial of hot water (45 degrees C) immersion versus ice packs for pain relief in bluebottle stings. Med J Aust. 2006;184(7):329–333. doi:10.5694/j.1326-5377.2006.tb00265.x
32. Wilcox CL, Yanagihara AA. Heated debates: hot-water immersion or ice packs as first aid for cnidarian envenomations? Toxins. 2016;8(4):97. doi:10.3390/toxins8040097
33. Isbister GK, Palmer DJ, Weir RL, et al. Hot water immersion v icepacks for treating the pain of Chironex fleckeri stings: a randomised controlled trial. Med J Aust. 2017;206(6):258–261. doi:10.5694/mja16.00990
34. Wang B, Zhang L, Zheng J, et al. Multiple organ dysfunction: a delayed envenomation syndrome caused by tentacle extract from the jellyfish Cyanea capillata. Toxicon. 2013;61:54–61. doi:10.1016/j.toxicon.2012.11.003
35. DeClerck MP, Bailey Y, Craig D, et al. Efficacy of topical treatments for Chrysaora chinensis species: a human model in comparison with an in vitro model. Wilderness Environ Med. 2016;27(1):25–38. doi:10.1016/j.wem.2015.10.008
36. Chinese Society of Toxicology. Chinese Expert Consensus on treatment of jellyfish envenomation. Clin Misdiagnosis Misther. 2014;27(10):1–5.
37. Pek JH, Lim SH, Ong GY, et al. First aid treatment of jellyfish stings: a systematic review. Cureus. 2025;17(5):e84289. doi:10.7759/cureus.84289
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.