")
Back to Journals » Infection and Drug Resistance » Volume 16
Emergence of a ST248Pasteur-ST1068Oxford Carbapenem Resistance Acinetobacter pittii Clinical Isolate in China, Co-Harboring OXA-58 and OXA-500 Carbapenemases
Authors Tian C, Song J, Huang D, Wang S, Zhao Y, Fu L, Fan X, Ma T, Bai Y
Received 11 July 2023
Accepted for publication 24 August 2023
Published 29 August 2023 Volume 2023:16 Pages 5681—5684
DOI https://doi.org/10.2147/IDR.S426182
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Sandip Patil
Chongmei Tian,1,* Jianqin Song,2,* Delian Huang,3 Siwei Wang,4 Yaping Zhao,1 Liping Fu,1 Xueyu Fan,5 Tianhong Ma,6 Yongfeng Bai5
1Department of Pharmacy, Shaoxing Hospital of Traditional Chinese Medicine Affiliated to Zhejiang Chinese Medical University, Shaoxing, Zhejiang, 312000, People’s Republic of China; 2Department of Traditional Chinese Medicine, Hangzhou Linping District Hospital of Integrated Chinese and Western Medicine, Hangzhou, People’s Republic of China; 3School of Medical Technology and Information Engineering, Zhejiang Chinese Medical University, Hangzhou, 310053, People’s Republic of China; 4Core Facility, The Quzhou Affiliated Hospital of Wenzhou Medical University, Quzhou People’s Hospital, Quzhou, 324000, People’s Republic of China; 5Department of Clinical Laboratory, The Quzhou Affiliated Hospital of Wenzhou Medical University, Quzhou People’s Hospital, Quzhou, 324000, People’s Republic of China; 6Department of Pharmacy, Jiaxing Hospital of Traditional Chinese Medicine, Jiaxing, 314001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yongfeng Bai; Tianhong Ma, Email [email protected]; [email protected]
Acinetobacter pittii is a crucial pathogen that mainly causes healthcare-associated infections, including pneumonia, bloodstream infections (BSIs) and urinary tract infections (UTIs).1 Carbapenem-resistant A. pittii (CRAP) poses a huge challenge in clinical settings. CRAP is increasingly recognized as a significant pathogen of hospital-acquired infections in the hospital.2 Carbapenem resistance in A. pittii is mainly caused by the production of carbapenem-hydrolyzing class D β-lactamases (CHDLs) including OXA-23-like, OXA-58-like, and OXA-24-like enzymes.3 Until now, the genomic features of rare sequence type (ST) A. pittii have not been well studied.
Here, one ST248Pasteur-ST1068Oxford CRAP clinical strain (TCM2) was collected from sputum in 2018 in China, and its genomic characteristics were described based on Illumina whole-genome sequencing (WGS) and bioinformatic analysis. Antimicrobial susceptibility tests (AST), including imipenem, meropenem, ciprofloxacin, colistin and tigecycline, were conducted using broth microdilutions and results were interpreted according to Clinical and Laboratory Standards Institute (CLSI) guidelines. Conjugation experiments were performed using film mating method with a rifampicin-resistant derivative of A. baumannii ATCC 17978 as the recipient strain as described previously.4 Transconjugants were selected on Mueller–Hinton agar plates containing rifampicin (60 µg/mL) and meropenem (4 µg/mL). WGS was performed using the Illumina platform. Sequenced raw reads were assembled using Shovill pipeline, version 0.9. Sequences annotation was performed using National Center for Biotechnology Information (NCBI) Prokaryotic Genome Annotation Pipeline (PGAP) (http://www.ncbi.nlm.nih.gov/genome/annotation_prok/) and rapid annotations were conducted using the subsystems technology (RAST) server.5,6 Multilocus sequence typing (MLST) was performed using Pasteur and Oxford schemes with PubMLST (https://pubmlst.org/). Identification of acquired antibiotic resistance genes using ResFinder database and KmerResistance-2.2.7,8 Bacterial virulence factors were predicted using virulence factor database (VFDB).9 Capsular polysaccharide (KL) and lipoolygosaccharide (OCL) were tested using Kaptive.10 Plasmid replicon analysis was conducted using the A. baumannii PCR-based replicon typing (AB-PBRT) method.11 Comparison between the p17-84_OXA plasmid and TCM2 genome was performed using Circoletto.12 Closely related plasmids were predicted using the Bacterial Isolate Genome Sequence Database (BIGSdb).13
AST results revealed that the TCM2 strain was resistant to imipenem and meropenem, with minimal inhibitory concentrations (MIC) of 8 and 16 mg/L, respectively. It was also resistant to ciprofloxacin (32 mg/L) but was still susceptible to colistin (0.5 mg/L) and tigecycline (0.5 mg/L). According to the RAST results, 3816 genes belonging to 311 subsystems were annotated. Most of these belong to various metabolic functions (465), amino acids, and derivatives (305). In addition, 58 subsystems were sorted into the virulence, disease, and defense categories (Figure 1A). The specific sequence assembly statistics (Size, GC content, N50, L50 and number of contigs) are shown in Supplementary Table 1.
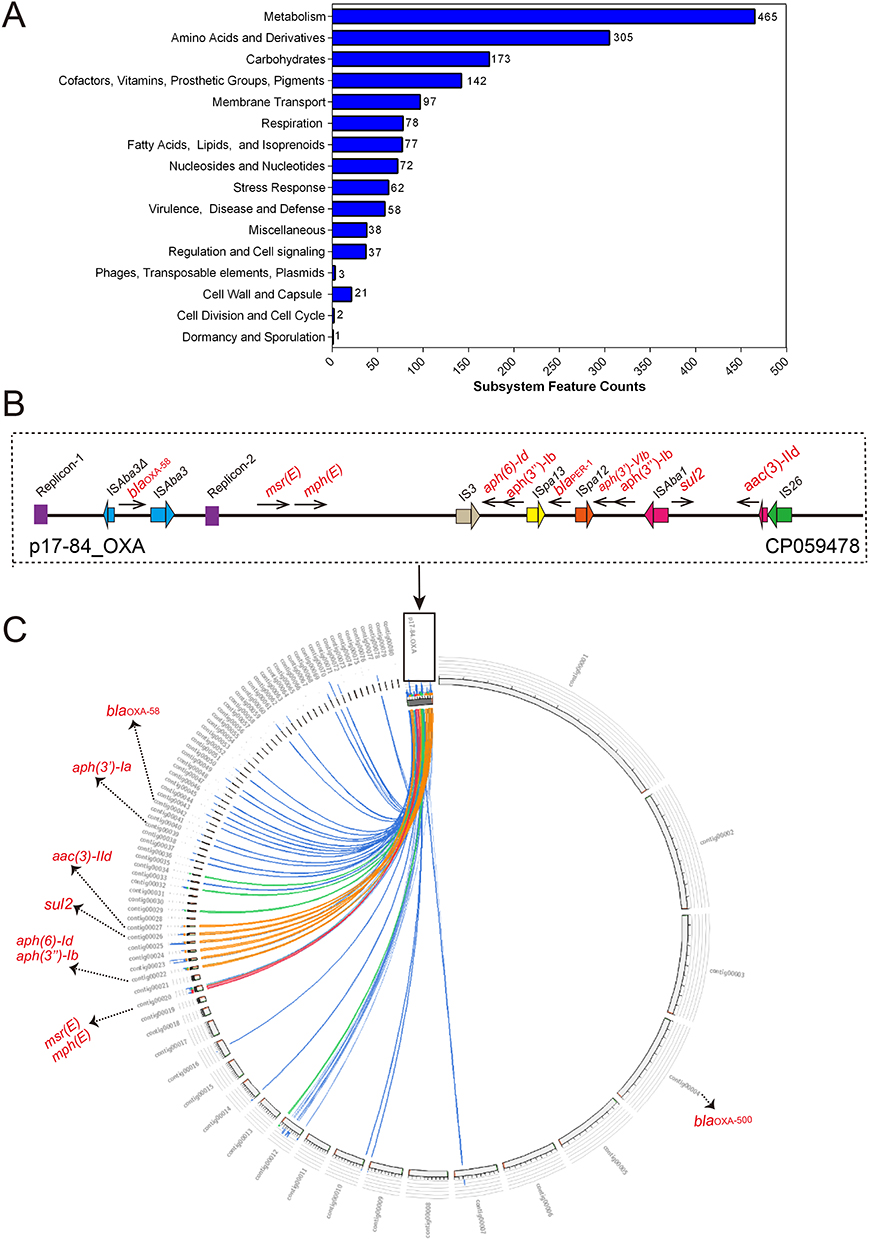 |
Figure 1 RAST annotation, p17-84_OXA plasmid structure and mapped to the genome of A. pittii TCM2 clinical isolate. (A) Counts of subsystem based on RAST annotation. The number of each subsystem category is shown on the right of column. (B) Structure of p17-84_OXA plasmid (GenBank accession number: CP059478). Resistance genes (black arrows with red names), replicons (purple), and ISs with different colors are shown. (C) Comparison between p17-84_OXA plasmid and A. pittii TCM2 strain genome. The lines with different colors represent homologous regions with high identity. Resistance genes located in distinct contigs and labeled with red names. |
Analysis of the resistance genes profile of A. pittii TCM2 strain showed that, in addition to co-harbouring blaOXA-58 and blaOXA-500, a series of genes, including aac(3)-IId, aph(3″)-Ib, aph(3′)-Ia, aph(6)-Id, sul2 and msr(E)-mph(E), were also identified, which was matched with the resistance phenotypes. The results of resistance genes profile were identical using ResFinder database and KmerResistance-2.2. Moreover, a mutation of serine to lysine at amino acid residue 81 (S81L) of the gyrA-encoded DNA gyrase confers resistance to fluoroquinolones.14 In the present study, the putative plasmid was non-typeable by AB-PBRT and no transconjugants were identified for blaOXA-58. Various virulence factors have been predicted in the TCM2 strain, such as pilus-related csuABCDE, acinetobactin-encoding gene clusters (bauBCDEF, basABCDFGHIJ and barAB), and bfmRS. Based on genome analysis, A. pittii TCM2 was ST248Pasteur-ST1068Oxford with KL84 and OCL6, respectively. We further mapped our genome to the p17-84_OXA plasmid (accession number: CP059478) (Figure 1B), which is located in an ST63 pandrug-resistant A. pittii.15 High nucleotide sequence identity was observed for some of the contigs in the TCM2 genome with p17-84_OXA (Figure 1C). Consequently, we concluded that there was a blaOXA-58-bearing plasmid in the TCM2 strain, which was probably obtained from other A. pittii and A. nosocomialis strains collected in China in 2012 and 2014, respectively (Supplementary Table 2). Moreover, there is a likelihood that other genes listed above are also plasmid-encoded based on the sequence identities with p17-84_OXA. blaOXA-58 gene was flanked by one truncated ISAba3 (upstream) and one complete ISAba3 (downstream) with different orientations, which was similar to previous report.16 Further research of long-read sequencing using Oxford Nanopore Technologies (ONT) platform should be performed to validate the structure of this putative plasmid.
To our knowledge, this is the first report of the genomic characteristics of a ST248Pasteur-ST1068Oxford CRAP clinical isolate that co-produces OXA-58 and OXA-500 in China. Identified resistance genes were correlated with the actual antimicrobial resistance phenotype of the strain and a blaOXA-58-bearing plasmid should be harbored by the TCM2 strain. Therefore, early detection is recommended to prevent further spread in the healthcare settings.
Data Sharing Statement
The draft genome sequence of A. pittii TCM2 strain was deposited in GenBank under the Bioproject PRJNA943463, Biosample SAMN33728593, with the accession number JARJKM000000000.
Ethical Approval
Ethical approval was not required due to this study was part of the routine hospital laboratory procedure and this study was only focused on the bacterial genome and not the patient’s data.
Funding
This work was supported by the Medical Health Science and Technology Project of Zhejiang Provincial Health Commission (2023KY1270, 2022RC278), Zhejiang Province Traditional Chinese Medicine Science and Technology Project (2023ZL729), Natural Science Foundation of Zhejiang Province (LQ19H160002), and Quzhou Technology Projects, China (2019K36).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chopjitt P, Putthanachote N, Ungcharoen R, et al. Genomic characterization of clinical extensively drug-resistant Acinetobacter pittii isolates. Microorganisms. 2021;9(2):242. doi:10.3390/microorganisms9020242
2. Chusri S, Chongsuvivatwong V, Rivera JI, et al. Clinical outcomes of hospital-acquired infection with Acinetobacter nosocomialis and Acinetobacter pittii. Antimicrob Agents Chemother. 2014;58(7):4172–4179. doi:10.1128/AAC.02992-14
3. Ayibieke A, Kobayashi A, Suzuki M, et al. Prevalence and characterization of carbapenem-hydrolyzing class D beta-lactamase-producing acinetobacter isolates from Ghana. Front Microbiol. 2020;11:587398. doi:10.3389/fmicb.2020.587398
4. Jin L, Wang R, Wang X, et al. Emergence of mcr-1 and carbapenemase genes in hospital sewage water in Beijing, China. J Antimicrob Chemother. 2018;73:84–87.
5. Tatusova T, DiCuccio M, Badretdin A, et al. NCBI prokaryotic genome annotation pipeline. Nucleic Acids Res. 2016;44(14):6614–6624. doi:10.1093/nar/gkw569
6. Overbeek R, Olson R, Pusch GD, et al. The SEED and the Rapid Annotation of microbial genomes using Subsystems Technology (RAST). Nucleic Acids Res. 2014;42:D206–D214.
7. Zankari E, Hasman H, Cosentino S, et al. Identification of acquired antimicrobial resistance genes. J Antimicrob Chemother. 2012;67(11):2640–2644. doi:10.1093/jac/dks261
8. Clausen PT, Zankari E, Aarestrup FM, Lund O. Benchmarking of methods for identification of antimicrobial resistance genes in bacterial whole genome data. J Antimicrob Chemother. 2016;71:2484–2488.
9. Liu B, Zheng D, Zhou S, Chen L, Yang J. VFDB 2022: a general classification scheme for bacterial virulence factors. Nucleic Acids Res. 2022;50(D1):D912–D917. doi:10.1093/nar/gkab1107
10. Wyres KL, Cahill SM, Holt KE, Hall RM, Kenyon JJ. Identification of Acinetobacter baumannii loci for capsular polysaccharide (KL) and lipooligosaccharide outer core (OCL) synthesis in genome assemblies using curated reference databases compatible with Kaptive. Microb Genom. 2020;6:e000339.
11. Bertini A, Poirel L, Mugnier PD, Villa L, Nordmann P, Carattoli A. Characterization and PCR-based replicon typing of resistance plasmids in Acinetobacter baumannii. Antimicrob Agents Chemother. 2010;54:4168–4177.
12. Darzentas N. Circoletto: visualizing sequence similarity with circos. Bioinformatics. 2010;26(20):2620–2621. doi:10.1093/bioinformatics/btq484
13. Tian C, Xing M, Fu L, Zhao Y, Fan X, Wang S. Emergence of uncommon KL38-OCL6-ST220 carbapenem-resistant Acinetobacter pittii strain, co-producing chromosomal NDM-1 and OXA-820 carbapenemases. Front Cell Infect Microbiol. 2022;12:943735.
14. Korzheva N, Davies TA, Goldschmidt R. Novel Ser79Leu and Ser81Ile substitutions in the quinolone resistance-determining regions of ParC Topoisomerase IV and GyrA DNA gyrase subunits from recent fluoroquinolone-resistant streptococcus pneumoniae clinical isolates. Antimicrob Agents Chemother. 2005;49(6):2479–2486. doi:10.1128/AAC.49.6.2479-2486.2005
15. Yang L, Dong N, Xu C, Ye L, Chen S. Emergence of ST63 pandrug-resistant acinetobacter pittii isolated from an AECOPD patient in China. Front Cell Infect Microbiol. 2021;11:739211.
16. Wang J, Wang Y, Wu H, et al. Coexistence of bla (OXA-58) and tet(X) on a novel plasmid in Acinetobacter sp. from Pig in Shanghai, China. Front Microbiol. 2020;11:578020. doi:10.3389/fmicb.2020.578020
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.