Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Elevated Serum Complement C1q Levels After Traumatic Brain Injury and Its Association with Poor Prognosis
Authors Yan XJ ![]() , Li YB, Liu W
, Li YB, Liu W ![]() , Wu HY, Yu GF
, Wu HY, Yu GF
Received 16 November 2021
Accepted for publication 26 December 2021
Published 8 January 2022 Volume 2022:18 Pages 47—55
DOI https://doi.org/10.2147/NDT.S348682
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Xin-Jiang Yan,1 Yang-Bo Li,1 Wei Liu,1 Hua-Yong Wu,2 Guo-Feng Yu1
1Department of Neurosurgery, The Quzhou Affiliated Hospital of Wenzhou Medical University, Quzhou People’s Hospital, Quzhou, People’s Republic of China; 2Neurosurgical Intensive Care Unit, The Quzhou Affiliated Hospital of Wenzhou Medical University, Quzhou People’s Hospital, Quzhou, People’s Republic of China
Correspondence: Guo-Feng Yu Tel +86 570 3055179
Email [email protected]
Objective: Complement C1q is implicated in neuroinflammation. We intended to discern the relationship between serum C1q levels and severity in addition to prognosis following traumatic brain injury (TBI).
Methods: In this prospective, observational study, serum C1q levels were quantified in 188 TBI patients and 188 healthy controls. Glasgow coma scale (GCS) and Rotterdam computed tomography (CT) classification were used as clinical and radiological indicators of severity. Patients with extended Glasgow outcome scale (GOSE) score of 1– 4 at 6 months after trauma were considered to have a poor outcome. Multiple logistic regression model was built to ascertain the independent association of serum C1q levels with 6-month poor outcome. Receiver operating characteristic (ROC) curve was configured for analysis of prognostic capability with respect to serum C1q levels.
Results: TBI patients exhibited substantially higher serum C1q levels than controls (median, 223.9 mg/l versus 75.4 mg/l). Serum C1q levels of patients were tightly correlated with GCS score (r = − 0.671), Rotterdam CT classification (r = 0.604) and GOSE score (r = − 0.581). An area under the ROC curve was yielded of 0.793 (95% confidence interval = 0.728– 0.849), and serum C1q levels above 345.5 mg/l discriminated the risk of 6-month poor outcome with 59.6% sensitivity and 92.6% specificity. Serum C1q levels above 345.5 mg/l retained as an independent predictor for 6-month poor outcome with odds ratio of 4.922 (95% confidence interval = 1.552– 15.606; P = 0.017).
Conclusion: Elevated serum C1q levels are closely correlated with traumatic severity and independently predicted the risk of long-term poor prognosis after TBI.
Keywords: traumatic brain injury, C1q, severity, functional outcome, biomarkers
A Letter to the Editor has been published for this article.
Introduction
Traumatic brain injury (TBI) is one of the leading causes of death and disability globally.1 Inflammatory response is implicated in pathophysiological processes underlying secondary injury events after TBI.2 The complement system is an essential element in the inflammatory reaction, which is activated via three complement activation pathways, namely classical, alternative and lectin.3 The complement system contributes to neuronal cell death, brain edema, disruption of blood-brain barrier and infiltration of inflammatory cells, thus playing an important role in mechanisms involved in secondary brain injury post-TBI.4
Complement component 1q (C1q) is an important component of the classical complement pathway, which is involved in both adaptive and innate immunity via activating a cascade of other soluble or membrane bound proteins.5 C1q can be synthesized in microglia and neurons.6,7 Its elevated expression has been revealed in brain tissues of animals with acute brain injury and humans with TBI.8,9 In patients with acute ischemic stroke, serum C1q levels were significantly increased.10 A recent clinical investigation showed that serum C1q levels were positively associated with severity of neurological impairment and infarct size of patients with acute ischemic stroke.11 However, to the best of our knowledge, there is a paucity of data available regarding the relationship between serum C1q levels and the severity plus prognosis of TBI. The purpose of the current study was to determine serum C1q levels after TBI and further evaluate the reliability in regard to serum C1q for the prediction of long-term poor functional outcome among a cohort of TBI patients.
Materials and Methods
Design and Subjects
In this prospective and observational study, we consecutively recruited hospitalized patients with blunt TBI from July 2016 to February 2020. We further excluded those patients who had any one of the following criteria: (1) age less than eighteen years; (2) abbreviated injury scale score of 3 or greater in any non-cranial aspects; (3) admission time exceeding 12 h since trauma; (4) incomplete information; (5) loss to a 6-month follow-up post- trauma; (6) refusal to participation; (7) unavailable blood sampling and (8) other known severe diseases, eg, malignancy, uremia, liver cirrhosis and heart failure. Alternatively, a group of healthy volunteers were selected as controls. The study was performed in accordance with the tenets of the Declaration of Helsinki. The ethical committee at the Quzhou Affiliated Hospital of Wenzhou Medical University (Quzhou People’s Hospital) gave approval for the protocol of this study (opinion number: LW2021-004). Informed consent to participation was signed by participants themselves or their relatives if patients were unconscious.
Recorded Data
We collected some routine information with respect to demographic data (age and gender), adverse life habits (cigarette smoking and alcohol drinking), coexisting diseases (hypertension, diabetes mellitus and hyperlipidemia), time parameters (admission time and blood-collection time) and traumatic causes (automobile/motorcycle, fall/jump or others). Alcohol abuse was defined as moderate-to severe alcohol consumption in social history (> 168g/week).12 Those patients who smoked regularly at least one cigarette per day at the time of presentation were considered as current smokers.12 Systolic and diastolic arterial blood pressures were measured by use of a noninvasive technique. Positive radiological appearances included abnormal cisterns, midline shift, epidural hematoma, subdural hematoma, subarachnoid hemorrhage, intraventricular hemorrhage, intracerebral hematoma, brain contusion and pneumocephalus. Clinical severity was assessed using Glasgow coma scale (GCS) and radiological severity was evaluated utilizing Rotterdam computed tomography (CT) classification. Clinical outcome at post-traumatic 6 months was assessed using 8-grade Extended Glasgow Outcome Scale (GOSE). GOSE score of 1–4 was defined as a poor outcome and GOSE score of 5–8 was regarded as a good outcome.13
Detection of Serum C1q
Venous blood samples were acquired and then centrifuged. Serum was stored at –80 ° C until assayed. Serum C1q levels were in duplicate gauged using a commercially available enzyme-linked immunosorbent assay kit in accordance with the manufacturer’s instructions (Cloud‑Clone Corp., Wuhan, China). Measurements were done in batches by the same technician who was inaccessible to clinical information.
Statistical Analysis
All data were analyzed using MedCal version 17.9.7. (MedCalc Software, Mariakerke, Belgium) software or the SPSS version 20.0 (SPSS Inc., Chicago, Illinois, USA) statistical package. Variables were reported as mean ± standard deviation (SD) for normally distributed quantitative data, median (upper-lower quartiles) for non-normally distributed quantitative data and count (proportion) for qualitative data. The significances of mean and median comparisons between two groups were determined using the Student’s t-test and Mann–Whitney U-test respectively. Qualitative data were compared using the Pearson chi-square test or Fisher’s exact test as appropriate. Non-normally quantitative data were compared among multiple groups using the Kruskal‑Wallis test. Bivariate correlations were evaluated using Spearman correlation analysis. Simultaneously, the multivariate linear regression analysis was conducted. The multivariable logistic regression analysis was done to identify independent predictors of 6-month poor outcome after head trauma. The associations were reported as odds ratios (ORs) and the corresponding 95% confidence intervals (CIs). We constructed the receiver operating characteristic (ROC) curve to assess the 6-month poor outcome prediction ability of serum C1q levels. Area under ROC curve (AUC) and its 95% CI were subsequently generated. Using the maximum Youden J index, the optimal cut-off value of serum C1q levels was chosen, which yielded the corresponding sensitivity and specificity values for differentiating between patients with a poor outcome and those presenting with a good outcome at 6 months post-injury. P<0.05 was considered to indicate a statistically significant difference.
Results
Patient Selection and Characteristics
In the current study, we at first assessed 227 patients with blunt TBI admitted to our hospital. We further excluded 39 patients because of age less than eighteen years (4 cases), abbreviated injury scale score of 3 or greater in any non-cranial aspects (8 cases), admission time exceeding 12 h since trauma (9 cases), incomplete information (3 cases), loss to a 6-month follow-up post- trauma (2 cases), refusal to participation (1 case), unavailable blood sampling (2 cases) and other known severe diseases (10 cases). Ultimately, a total of 188 TBI patients were included in this study. Simultaneously, 188 healthy controls were recruited. There were no substantial differences in age and percentage of sex between controls and patients.
The eventually assessed TBI patients, of whom, 112 were males and 76 were females, were aged from 18 to 78 years (mean, 40.0 years; SD, 14.7 years). Current cigarette smoking and alcohol abuse were found in 48 (25.5%) and 42 (22.3%) patients respectively. In total, 31 (16.5%) patients were inflicted with hypertension, 16 (8.5%) coexisted with diabetes mellitus and 32 (17.0%) suffered from hyperlipidemia. Patients were admitted to hospital from 0.5 to 12.0 hours following trauma (median, 5.3 hours; lower-upper quartiles, 2.7–8.3 hours) and peripheral venous blood was obtained from 1.4 to 13.7 hours after trauma (median, 6.8 hours; percentiles 25th – 75th, 4.7–9.3 hours). GCS score ranged from 3 to 15 (median, 10; lower-upper quartiles, 7–10). In addition, there were 63 patients with severe TBI (GCS 3–8), 81 with moderate TBI (GCS 9–12) and 44 with mild TBI (GCS 13–15). As regards traumatic causes, almost half of patients had TBI engendered by automobile or motorcycle accidents (92 cases, 48.9%), other causes of TBI included fall and jump (77 cases, 41.0%), and a little portion of patients (19 cases, 10.1%) experienced a bicycle mishap, a physical assault, or a sudden collapse. Systolic, diastolic and mean arterial blood pressures ranged from 71 to 177 mmHg (mean, 121.1 mmHg; SD, 29.8 mmHg), from 43 to 115 mmHg (mean, 76.3 mmHg; SD, 20.3 mmHg) and from 52 to 132 mmHg (mean, 91.3 mmHg; SD, 22.6 mmHg) respectively. Rotterdam CT classification ranged from 1 to 6 (median, 3; lower-upper quartiles, 2–4). When Rotterdam CT classification was regarded as a categorical variable. There were 25 patients with score 1, 40 with score 2, 57 with score 3, 34 with score 4, 20 with 5 and 12 with 6. All patients had essentially cranial injuries, among whom there were 79 patients with abnormal cisterns, 75 showing midline shift above 5 mm, 87 displaying epidural hematoma, 111 exhibiting subdural hematoma, 132 suffering from subarachnoid hemorrhage, 12 presenting with intraventricular hemorrhage, 81 coexisting with intracerebral hematoma, 112 having brain contusion, 53 inflicted with pneumocephalus, 112 with presence of skull-cap fracture and 87 with existence of skull-base fracture. At 6 months after head trauma, GOSE score ranged from 1 to 8 (median, 6; percentiles 25th - 75th, 4–7). A total of 52 (27.7%) TBI patients had a poor outcome (GOSE 1–4).
Serum C1q Levels and Severity Plus Inflammation
In Figure 1, TBI patients had substantially higher serum C1q levels than controls (P<0.001). As regards relationship between serum C1q levels and trauma severity indicated by GCS score and Rotterdam CT classification among this group of TBI patients, we found that (1) serum C1q levels were significantly inversely correlated with GCS score, which was identified as a continuous variable (P<0.001) (Figure 2); (2) serum C1q levels were significantly higher in patients with severe TBI (GCS 3–8) than in those experiencing moderate TBI (GCS 9–12) (P<0.001) and in severe TBI patients than in those presenting with mild TBI (GCS 13–19) (P<0.001), while there was no marked difference in terms of serum C1q levels between patients with moderate TBI and those who presented with mild TBI (P>0.05) (Figure 3); (3) when Rotterdam CT classification was identified as a qualitative variable, there was a significant trend that serum C1q levels were substantially elevated, with increasing Rotterdam CT classification (P<0.001) (Figure 4). Alternatively, serum C-reactive protein levels were highly correlated with serum C1q levels after head trauma (P<0.001) (Figure 5). A multivariate linear regression model, which contained variables significantly correlated with serum C1q levels in Table 1 (namely, GCS score, Rotterdam CT classification, abnormal cisterns, midline shift above 5 mm, epidural hematoma, subdural hematoma, subarachnoid hemorrhage, intraventricular hemorrhage, intracerebral hematoma, serum C-reactive protein levels and blood glucose levels), showed that serum C1q levels were independently correlated with GCS score (t=−3.234, P=0.001), Rotterdam CT classification (t=2.937, P=0.004) and serum C-reactive protein levels (t=2.589, P=0.010).
 |
Table 1 Univariate Correlation Analysis Between Serum C1q Levels and Other Variables in 188 Patients with Traumatic Brain Injury |
 |
Figure 1 Differences in terms of serum C1q levels between healthy controls and patients with traumatic brain injury. Serum C1q levels were reported as median (upper-lower quartiles). Serum C1q levels were significantly higher in patients with traumatic brain injury than in healthy controls using the Mann–Whitney U-test. |
 |
Figure 2 Relationship between serum C1q levels and Glasgow coma scale score after traumatic brain injury. Serum C1q levels were tightly correlated with Glasgow coma scale score following head trauma using the Spearman correlation coefficient. Abbreviation: GCS, Glasgow coma scale. |
 |
Figure 3 Comparisons of serum C1q levels across severity grade among patients with traumatic brain injury. Significant differences of serum C1q levels existed after head trauma among multiple groups using the Kruskal‑Wallis test. Abbreviation: GCS, Glasgow coma scale. |
 |
Figure 4 Differences of serum C1q levels by Rotterdam computerized tomography classification after traumatic brain injury. There were substantial differences in terms of serum C1q levels after head trauma among multiple groups using the Kruskal‑Wallis test. Abbreviation: CT, computerized tomography. |
 |
Figure 5 Relation of serum C1q levels to serum C-reactive protein levels after traumatic brain injury. Serum C1q levels were closely correlated with serum C-reactive protein levels after head trauma using the Spearman correlation coefficient. Abbreviation: CRP, C-reactive protein. |
Serum C1q Levels and Prognosis
Figure 6 shows that serum C1q levels were closely and negatively correlated with GOSE score in this host of TBI patients (P<0.001). Moreover, patients with development of a poor outcome (GOSE 1–4) at 6 months following head trauma had statistically significantly elevated serum C1q levels, as compared with those with a good outcome (P<0.001) (Figure 7). Under ROC curve, serum C1q levels distinguished patients with a poor outcome from the other remaining ones with AUC at 0.793 (Table 2). Moreover, using maximum Youden index, an optimal value of serum C1q levels was selected, which was 345.5 mg/l, yielding the corresponding sensitivity and specificity values (Figure 8). In Table 2, the prognostic predictive ability of serum C1q levels was equivalent to those of GCS score and Rotterdam CT classification (both P>0.05). Furthermore, serum C1q levels significantly improved the AUCs of GCS score and Rotterdam CT classification (both P<0.05, Table 2).
 |
Table 2 Receiver Operating Characteristic Curve Analysis for Predicting 6-Month Poor Outcome After Traumatic Brain Injury |
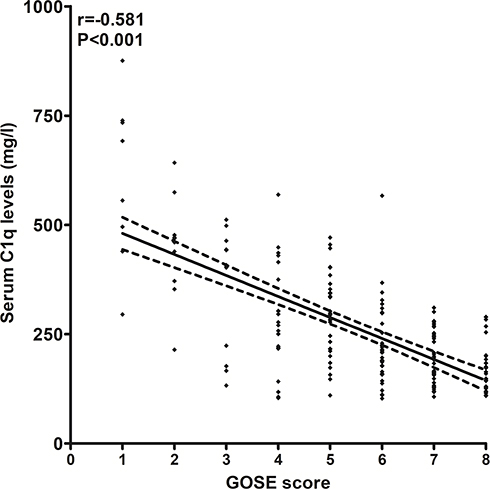 |
Figure 6 Association of serum C1q levels with extended Glasgow outcome scale score after head trauma. Serum C1q levels were highly correlated with extended Glasgow outcome scale score after head trauma using the Spearman correlation coefficient. Abbreviation: GOSE, Glasgow outcome scale score. |
 |
Figure 7 Differences of serum C1q levels between patients with extended Glasgow outcome scale score 1–4 and those with extended Glasgow outcome scale score 5–8 at 6 months after traumatic brain injury. Serum C1q levels were markedly raised in patients with extended Glasgow outcome scale score 1–4, as compared to those presenting with score 5–8 at 6 months after head trauma using the Mann–Whitney U-test. Abbreviation: GOSE, Glasgow outcome scale score. |
 |
Figure 8 Analysis regarding the predictive ability of serum C1q levels for 6-month poor outcome after traumatic brain injury. Poor outcome was defined as extended Glasgow outcome scale score 1–4. Discriminatory capability was assessed under receiver operating characteristic curve. Using maximum Youden index, an optimal value of serum C1q levels was selected. Arrow indicates the selected cutoff value of serum C1q levels, namely, 345.5 mg/l, which predicted 6-month poor outcome with 59.6% sensitivity and 92.6% specificity. |
In Table 3, using univariate analysis, the associated factors of 6-month poor outcome were as follows: GCS score, Rotterdam CT classification, abnormal cisterns, midline shift more than 5 mm, epidural hematoma, blood glucose levels, serum C-reactive protein levels and serum C1q levels > 345.5 mg/l. The aforementioned significant variables were entered into the multivariate model and as a consequence, the factors retaining independently associated with a poor outcome at post-traumatic 6 months were GCS score (odd ratio, 0.721; 95% CI, 0.591–0.881; P=0.001), Rotterdam CT classification (odd ratio, 1.849; 95% CI, 1.247–2.740; P=0.007) and serum C1q levels > 345.5 mg/l (odd ratio, 4.922; 95% CI, 1.552–15.606; P=0.017).
 |
Table 3 Differences in Baseline Characteristics by a Poor Outcome at 6 Months After Traumatic Brain Injury |
Discussion
Neuroinflammation happens after TBI. Excessive complement activation is implicated in neuroinflammation and can promote secondary brain injury after TBI.2,4 Complement C1q is identified as a component of the C1 complex and is involved in both adaptive and innate immunity via the classical complement pathway.3 C1q functional activity has been revealed to be raised markedly in cerebrospinal fluid of rats after transient global cerebral ischemia.8 In two previous studies of patients with ischemic stroke, serum C1q levels of patients were substantially elevated as compared to healthy controls or controls without stroke.10,11 Our study also displayed that serum C1q levels were statistically significantly enhanced in patients with TBI than in healthy controls. Moreover, C1q expressions were significantly increased in rat brain microglia following the ischemic insult.14 A dramatical up-regulation of C1q expression was confirmed in cortex, striatum, thalamus and hippocampus of mice exposed to controlled cortical impact, as well as it was localized in microglia and neurons.15 Interestingly, in patients with TBI, elevated levels of C1q were found in the penumbra of the injured area.9 Thus, it is presumed that C1q in serum of TBI patients might be at least partially derived from injured brain tissues.
C1q possesses various complement and non-complement functions.5 C1q may participate in synaptic pruning, thereby exerting a key role in shaping neuronal architecture during the development of the central nervous system.16,17 Also, C1q was demonstrated to enhance microglial clearance of apoptotic cells using primary rat microglia and neurons.18 In addition, in cultured microglial cells, extrinsic C1q markedly increased intracellular Ca2+ levels and the release of interleukin-6, tumor necrosis factor-alpha and nitric oxide.19 In another study, C1q suppressed the lipopolysaccharide -induced production of proinflammatory cytokines (such as interleukin-1 alpha, interleukin-1beta, interleukin-6 and tumor necrosis factor-alpha) from cultured microglial cells, while the presence of C1q enhanced levels of monocyte chemoattractant protein-1.18 In line with such data, our study found that serum C1q levels were strongly correlated with serum C-reactive protein levels after TBI. Receptor for advanced glycation end-product (RAGE) is related to the brain pro-inflammatory signaling pathways and is also a receptor for C1q.20 Thus, C1q/RAGE complexes may regulate neuroinflammation. The preceding evidence is supportive of the notion that C1q might regulate neuroinflammation responding to acute brain injury. In mice with middle cerebral artery occlusion, the complement inhibitor soluble complement receptor-1 significantly lessened cerebral infarct volume and improved neurologic outcome, presumably in large part through the blockade of the downstream effects of postischemic cerebral C1q expression.21 Another experiment showed that C1q-deficiency may be neuroprotective against hypoxic-ischemic brain injury in neonatal mice.22 Thus, C1q may emerge as a therapeutic target for preventing inflammatory injury after acute brain injury.
To the best of our knowledge, no data have existed regarding relationship between serum C1q levels and severity plus prognosis after TBI. However, there are two human studies demonstrating its close association with severity and prognosis after ischemic stroke.10,11 In a study of patients with acute ischemic stroke, serum C1q levels were substantially higher in patients than in healthy controls and its elevated levels were significantly positively correlated with infarction volumes.10 In another study, serum C1q levels were positively associated with severity of neurological impairment and infarct size of patients with acute ischemic stroke.11 Nevertheless, a long-term neurologic function assessment was not done in those two studies of humans with acute ischemic stroke.10,11 Our study not only found that elevated serum C1q levels, as compared to healthy controls, were markedly correlated with trauma severity indicated by GCS and Rotterdam CT classification, but also showed that serum C1q levels were independently associated with 6-month poor outcome. More intriguingly, serum C1q levels displayed similar prognostic capabilities, as compared to GCS scores and Rotterdam CT classification, as well as dramatically improved prognostic abilities of GCS scores and Rotterdam CT classification based on ROC curve. In summary, serum C1q may be a potential prognostic biomarker of TBI.
There is at least a limitation to mention in the current study. This study recruited two groups of subjects, namely, healthy controls and patients with traumatic brain injury. Although there were no significant intergroup differences in terms of age and percentage of sex, other confounding factors were not investigated. Thus, the change of serum C1q levels between healthy controls and patients with traumatic brain injury may need to be further validated.
Conclusions
To the best of our knowledge, our study, for the first time, found that elevated serum C1q levels, in close correlation with GCS score and Rotterdam CT classification, are independently associated with 6-month poor prognosis after TBI and significantly improve prognostic abilities of GCS score and Rotterdam CT classification among such a group of TBI patients, substantializing serum C1q as a useful prognostic predictor for brain trauma.
Abbreviations
GCS, Glasgow coma scale; TBI, traumatic brain injury; CT, computerized tomography; ROC, receiver operating characteristic; AUC, area under curve; GOSE, Extended Glasgow Outcome Scale; RAGE, advanced glycation end-product; OR, odds ratio; 95% CI, 95% confidence interval.
Acknowledgments
The authors thank all staffs in Department of Neurosurgery, The Quzhou Affiliated Hospital of Wenzhou Medical University, Quzhou People’s Hospital (Quzhou, China) for their technical support.
Disclosure
The authors declare that there were no conflicts of interest.
References
1. Khellaf A, Khan DZ, Helmy A. Recent advances in traumatic brain injury. J Neurol. 2019;266(11):2878–2889. doi:10.1007/s00415-019-09541-4
2. Killen MJ, Giorgi-Coll S, Helmy A, Hutchinson PJ, Carpenter KL. Metabolism and inflammation: implications for traumatic brain injury therapeutics. Expert Rev Neurother. 2019;19(3):227–242. doi:10.1080/14737175.2019.1582332
3. Dalakas MC, Alexopoulos H, Spaeth PJ. Complement in neurological disorders and emerging complement-targeted therapeutics. Nat Rev Neurol. 2020;16(11):601–617. doi:10.1038/s41582-020-0400-0
4. Roselli F, Karasu E, Volpe C, Huber-Lang M. Medusa’s head: the complement system in traumatic brain and spinal cord injury. J Neurotrauma. 2018;35(2):226–240. doi:10.1089/neu.2017.5168
5. Kishore U, Reid KB. C1q: structure, function, and receptors. Immunopharmacology. 2000;49(1–2):159–170. doi:10.1016/s0162-3109(00)80301-x
6. Fonseca MI, Chu SH, Hernandez MX, et al. Cell-specific deletion of C1qa identifies microglia as the dominant source of C1q in mouse brain. J Neuroinflammation. 2017;14(1):48. doi:10.1186/s12974-017-0814-9
7. Datta D, Leslie SN, Morozov YM, et al. Classical complement cascade initiating C1q protein within neurons in the aged rhesus macaque dorsolateral prefrontal cortex. J Neuroinflammation. 2020;17(1):8. doi:10.1186/s12974-019-1683-1
8. Schäfer MK, Schwaeble WJ, Post C, et al. Complement C1q is dramatically up-regulated in brain microglia in response to transient global cerebral ischemia. J Immunol. 2000;164(10):5446–5452. doi:10.4049/jimmunol.164.10.5446
9. Bellander BM, Singhrao SK, Ohlsson M, Mattsson P, Svensson M. Complement activation in the human brain after traumatic head injury. J Neurotrauma. 2001;18(12):1295–1311. doi:10.1089/08977150152725605
10. Zhao X, Wang C, Pang B, Zhu Y, Zhang Y. The value of serum complement C1q in the diagnosis of acute ischemic stroke. Clin Lab. 2017;63(5):915–920. doi:10.7754/Clin.Lab.2016.161033
11. Wang DD, Hou XH, Li HQ, et al. Association of serum complement C1q concentration with severity of neurological impairment and infarct size in patients with acute ischemic stroke. J Stroke Cerebrovasc Dis. 2020;29(12):105363. doi:10.1016/j.jstrokecerebrovasdis.2020.105363
12. Kim BS, Jung HS, Bang OY, Chung CS, Lee KH, Kim GM. Elevated serum lipoprotein(a) as a potential predictor for combined intracranial and extracranial artery stenosis in patients with ischemic stroke. Atherosclerosis. 2010;212(2):682–688. doi:10.1016/j.atherosclerosis.2010.07.007
13. Stein DM, Hu PF, Brenner M, et al. Brief episodes of intracranial hypertension and cerebral hypoperfusion are associated with poor functional outcome after severe traumatic brain injury. J Trauma. 2011;71(2):
14. Mack WJ, Sughrue ME, Ducruet AF, et al. Temporal pattern of C1q deposition after transient focal cerebral ischemia. J Neurosci Res. 2006;83(5):883–889. doi:10.1002/jnr.20775
15. Ciechanowska A, Ciapała K, Pawlik K, et al. Initiators of classical and lectin complement pathways are differently engaged after traumatic brain injury-time-dependent changes in the cortex, striatum, thalamus and hippocampus in a mouse model. Int J Mol Sci. 2020;22(1):45. doi:10.3390/ijms22010045
16. Stevens B, Allen NJ, Vazquez LE, et al. The classical complement cascade mediates CNS synapse elimination. Cell. 2007;131(6):1164–1178. doi:10.1016/j.cell.2007.10.036
17. Stephan AH, Barres BA, Stevens B. The complement system: an unexpected role in synaptic pruning during development and disease. Annu Rev Neurosci. 2012;35:369–389. doi:10.1146/annurev-neuro-061010-113810
18. Fraser DA, Pisalyaput K, Tenner AJ. C1q enhances microglial clearance of apoptotic neurons and neuronal blebs, and modulates subsequent inflammatory cytokine production. J Neurochem. 2010;112(3):733–743. doi:10.1111/j.1471-4159.2009.06494.x
19. Färber K, Cheung G, Mitchell D, et al. C1q, the recognition subcomponent of the classical pathway of complement, drives microglial activation. J Neurosci Res. 2009;87(3):644–652. doi:10.1002/jnr.21875
20. Ma W, Rai V, Hudson BI, Song F, Schmidt AM, Barile GR. RAGE binds C1q and enhances C1q-mediated phagocytosis. Cell Immunol. 2012;274(1–2):72–82. doi:10.1016/j.cellimm.2012.02.001S0008-8749(12)00022-6.
21. Huang J, Kim LJ, Mealey R, et al. Neuronal protection in stroke by an sLex-glycosylated complement inhibitory protein. Science. 1999;285(5427):595–599. doi:10.1126/science.285.5427.595
22. Ten VS, Sosunov SA, Mazer SP, et al. C1q-deficiency is neuroprotective against hypoxic-ischemic brain injury in neonatal mice. Stroke. 2005;36(10):2244–2250. doi:10.1161/01.STR.0000182237.20807.d0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.