Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Electronic Health Record Implementation Enhances Financial Performance in High Medicaid Nursing Homes
Authors Dayama N ![]() , Pradhan R
, Pradhan R ![]() , Davlyatov G, Weech-Maldonado R
, Davlyatov G, Weech-Maldonado R
Received 7 February 2024
Accepted for publication 23 April 2024
Published 23 May 2024 Volume 2024:17 Pages 2577—2589
DOI https://doi.org/10.2147/JMDH.S457420
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 9
Editor who approved publication: Dr Scott Fraser
Neeraj Dayama,1,* Rohit Pradhan,2,* Ganisher Davlyatov,3 Robert Weech-Maldonado4
1Department of Healthcare Management and Leadership, Texas Tech University Health Sciences Center, Lubbock, TX, USA; 2School of Health Administration, Texas State University, San Marcos, TX, USA; 3Department of Health Administration & Policy, University of Oklahoma Health Sciences Center, Oklahoma City, OK, USA; 4Department of Health Services Administration, University of Alabama at Birmingham, Birmingham, AL, USA
*These authors contributed equally to this work
Correspondence: Rohit Pradhan, School of Health Administration, Texas State University, University Dr, San Marcos, TX, 78666, USA, Tel +512-245-6529, Email [email protected]
Introduction: The nursing home (NH) industry operates within a two-tiered system, wherein high Medicaid NHs which disproportionately serve marginalized populations, exhibit poorer quality of care and financial performance. Utilizing the resource-based view of the firm, this study aimed to investigate the association between electronic health record (EHR) implementation and financial performance in high Medicaid NHs. A positive correlation could allow high Medicaid NHs to leverage technology to enhance efficiency and financial health, thereby establishing a business case for EHR investments.
Methods: Data from 2017 to 2018 were sourced from mail surveys sent to the Director of Nursing in high Medicaid NHs (defined as having 85% or more Medicaid census, excluding facilities with over 10% private pay or 8% Medicare), and secondary sources like LTCFocus.org and Centers for Medicare & Medicaid Services cost reports. From the initial sample of 1,050 NHs, a 37% response rate was achieved (391 surveys). Propensity score inverse probability weighting was used to account for potential non-response bias. The independent variable, EHR Implementation Score (EIS), was calculated as the sum of scores across five EHR functionalities—administrative, documentation, order entry, results viewing, and clinical tools—and reflected the extent of electronic implementation. The dependent variable, total margin, represented NH financial performance. A multivariable linear regression model was used, adjusting for organizational and market-level control variables that may independently affect NH financial performance.
Results: Approximately 76% of high Medicaid NHs had implemented EHR either fully or partially (n = 391). The multivariable regression model revealed that a one-unit increase in EIS was associated with a 0.12% increase in the total margin (p = 0.05, CI: − 0.00– 0.25).
Conclusion: The findings highlight a potential business case —long-term financial returns for the initial investments required for EHR implementation. Nonetheless, policy interventions including subsidies may still be necessary to stimulate EHR implementation, particularly in high Medicaid NHs.
Keywords: electronic health records, health information technology, financial performance, high-Medicaid nursing homes
A Letter to the Editor has been published for this article.
A Response to Letter by Mr Wijaya has been published for this article.
Introduction
Background
The nursing home industry is an important component of the United States (U.S.) healthcare system. According to the National Center for Health Statistics,1 there are approximately 15,600 nursing homes in the U.S., with 1.7 million licensed beds, and 1.3 million residents. In the past few decades, for-profit corporate chains have emerged as the dominant ownership form in the nursing home industry. For-profit chains operate 66% of nursing homes, with the largest ten chains owning over 10% of all beds.2 Nursing homes serve vulnerable individuals who are often physically and cognitively challenged, acting as a safety net for older adults and people with disabilities. The nursing home industry operates in a highly competitive and resource-constrained environment.
Medicaid is the largest purchaser of nursing home services.3 However, a recent government report has estimated that the median Medicaid base payment rate was 86% of reported facility costs. Furthermore, nursing homes that serve a high proportion of Medicaid-covered residents tend to receive lower reimbursement rates.4 To compensate, nursing homes cross-subsidize Medicaid residents by offsetting lower reimbursement rates with more lucrative payments from Medicare and private-pay residents. However, nursing homes with high Medicaid census face further constraints due to their heavy reliance on Medicaid for a significant portion of their funding. Yet, they operate under the same staffing and other regulatory requirements limiting their ability to cut costs.
Mor et al5 have argued that the lopsided payer mix mechanism prevalent in the nursing home industry results in a distinct two-tiered system, with Medicaid-dependent facilities falling into the lower-tier category. The high Medicaid nursing homes (defined as having a Medicaid census of 85% or more, private-pay census of 10% or less, and Medicare census of 8% of less), struggle with poor quality of care, as evident through increased health-related deficiencies and chronic nurse staffing shortages.6,7 The inadequately remunerative payer mix of high Medicaid nursing homes is also reflected in their relatively poor financial performance. Unaddressed financial difficulties can not only lead to a further decline in quality but also result in insolvency and closures, affecting the availability of institutional long-term care in rural and other underserved areas.8 As high Medicaid nursing homes disproportionately serve the poor and minorities; it is imperative to improve their performance if the goal of elevating nursing home quality is to be realized.
Electronic Health Records
The Centers for Medicare & Medicaid Services9 (CMS) defines an Electronic Health Record (EHR) as a
digital version of a patient’s paper medical chart that contains information about the patient’s medical history, diagnoses, medications, treatment plans, immunization dates, allergies, radiology images, and laboratory and test results.
There is a broad academic and policy consensus that nursing homes would benefit from EHR implementation.10 EHR can enhance the accessibility and sharing of resident information, reduce medical errors through applications such as alerts and reminders, and improve practice efficiency resulting in greater revenue capture and reduced costs.11–14 Nursing home researchers have also reported that implementing EHR can yield substantial resident quality of care benefits such as reduced medication errors, fewer urinary tract infections, improved adverse incidence reporting, and increased immunization rates.15–17
Prior literature has associated higher quality in nursing homes with improved financial performance; facilities that performed better on quality exhibited higher operating margins.18 Therefore, EHR implementation in high Medicaid nursing homes has the potential to concomitantly address the two critical challenges administrators face: quality and financial performance.
The Rationale for This Study
Despite its purported impact on performance, nursing homes lag in EHR implementation.19 Various factors have contributed to the relatively slow implementation of EHR systems within the nursing home industry such as financial challenges and policy choices, particularly exclusion from the meaningful use (MU) incentive program.17,19 The MU program, initiated as part of the Health Information Technology for Economic and Clinical Health (HITECH) Act, was designed to incentivize the adoption of EHRs to improve quality, safety, and efficiency of patient care. However, the program predominantly targeted acute care settings, omitting nursing homes from its provisions.15 An additional hurdle arises from the fact that most existing EHR systems are primarily designed for acute care settings. Given that NHs often have their own unique requirements, such as specific medication dosing protocols and distinct reporting and regulatory needs, this misalignment can deter NHs from implementing EHRs.20
Experts and regulatory agencies have explicitly acknowledged the need to increase EHR penetration in nursing homes.21,22 These calls for action highlight the importance of addressing the barriers to EHR implementation within the nursing home industry to improve resident care and the overall operational efficiency.
Financial concerns are one of the main obstacles impeding wider EHR implementation in nursing homes.15,23 Installing EHR systems is expensive as it involves investing in hardware, data migration, training, information technology (IT) support, and supporting ongoing maintenance costs.24
High Medicaid nursing homes with their lean financial resources may be particularly reluctant to invest in expensive EHR systems for two reasons: low Medicaid reimbursement and uncertainty about future revenues. Moreover, state budget-led constraints on Medicaid spending may further dampen the appetite for large capital investments, given the ambiguity surrounding the return on investment (ROI).25
Therefore, high Medicaid nursing homes face a conundrum: though they would potentially benefit the most from EHR implementation, financial limitations and fiscal challenges limit their willingness to invest in EHR systems. How do we encourage EHR implementation in high Medicaid nursing homes? Short of direct policy interventions, one approach could involve building a business case that showcases the positive impact of EHR on financial outcomes.
Although several studies have assessed the impact of EHR on hospital financial performance,24,26,27 the empirical evidence in the nursing home industry is scarce. Hitt and Tambe28 have reported that operating costs were 2.3% higher for nursing homes that implemented EHR. However, their study was limited to a single state, and the data may be outdated. The absence of recent research that has investigated the influence of EHR implementation on nursing home financial performance represents a significant knowledge gap. This study is motivated by the need to address this substantial void in the existing literature.
This study contributes to the literature in three specific ways. First, utilizing primary data, it offers a national-level examination of the impact of EHR implementation on nursing home financial performance. The primary data gathered are one of the strengths of this study, as the data on EHR implementation in administrative datasets are limited to a single dichotomous variable. Second, by focusing on high Medicaid nursing homes that serve a higher proportion of marginalized populations, the findings may significantly improve the health and well-being of some of the most vulnerable Americans. Finally, the conceptual model and the employment of a rigorous analytical design, including controlling for organizational and market factors that may independently influence nursing home financial performance, lend credibility and strength to the findings of this study.
Conceptual Framework
The resource-based view (RBV) of the firm was used to examine the relationship between EHR implementation and financial performance. RBV posits that differences in firm performance can be explained by variations in their internal resources, and these differences remain stable over time, allowing firms to pursue value-creating strategies that result in sustained competitive advantage.29
Adapting Bharadwaj’s30 taxonomy, nursing home EHR-based resources are classified as the following: a) tangible resources comprising the physical EHR infrastructure, b) the human EHR-based resources comprising the technical and managerial skills and c) intangible EHR-based resources such as knowledge assets and synergy.
The physical EHR resources encompass components such as scheduling systems and clinical decision support systems. While these resources are not unique in themselves, when customized and integrated to meet specific facility needs, they gain value and can provide a strategic competitive advantage.
Human EHR skills encompass technical proficiency in using EHR components and managerial capabilities like project management.30 RBV argues that while individual human resource (HR) practices can be replicated, the unique HR systems and routines that develop over time contribute to the creation of specific human capital skills, offering a distinct competitive edge.31
Furthermore, RBV explicitly recognizes the role of intangible organizational resources such as culture and reputation, which can be enhanced through EHR implementation and improved market responsiveness.30 For instance, nursing homes may exploit EHR as a reputational “signaling device” to indicate higher quality. This approach could increase their market share and prompt a shift in their payer mix towards more financially advantageous Medicare/private pay residents.
Based on the preceding discussion, nursing home EHR-based resources can be classified as valuable, inimitable, rare, and organization-wide supported resource serving as a fount of sustained competitive advantage,32 an avowed consequence of its attainment is superior economic performance.33
Improved financial performance may be derived from increased revenues and/or reduced costs. Hospitals may favor nursing homes with electronic patient information sharing, prioritizing these facilities for the more remunerative post-acute care patients (Medicare). Moreover, EHR systems can directly improve quality, resulting in higher ratings within the CMS nursing home five-star quality rating system. Research shows a consumer preference for facilities awarded a 5-star rating.34 Revenues may also increase due to comprehensive charge capture and resource utilization group optimization. Simultaneously, cost reductions may arise from improved workflow efficiency, reduced expenditures on paper and transcription costs, and an overall reduction in waste.35–37 In summary, EHR implementation can result in increased revenues as well as lower costs, translating into improved financial performance (Figure 1).
 |
Figure 1 Conceptual Framework (Resource-Based View of the Firm). |
Therefore, we hypothesize that:
Hypothesis: High Medicaid nursing homes with higher EHR implementation will experience better financial performance.
Materials and Methods
Data
The study was conducted by merging primary survey and secondary data sources for the year 2017–2018. EHR implementation data were collected via mail surveys sent to the Director of Nursing (DON) in high-Medicaid nursing homes in the U.S. To ensure a higher response rate, a modified approach to Dillman’s total design method was followed: three rounds of surveys with post-card reminders and follow-up phone calls from November 2017 through March 2018.38 All mailings included a link to the online survey. An incentive payment of $25 was provided to survey respondents.
The analytical sample was constructed by surveying the entire population of nursing homes meeting specific criteria: those with an 85% or higher Medicaid census and consistent with prior approaches, nursing homes with 10% or higher private pay and/or 8% or higher Medicare were excluded.5 The number of nursing homes that qualified under these criteria was 1,050, from which we received 391 completed surveys, resulting in a response rate of 37%.
The survey instrument used in this study was adapted from the one developed by Abramson et al which was originally used to investigate EHR adoption in New York nursing homes.39 The original survey comprised ten questions that evaluated various facets including the extent of EHR implementation and participation in health information exchange. Only minor modifications were made to enhance the clarity of the survey language.
The survey data were merged with the following secondary data sources: LTCFocus.org, Area Health Resource File (AHRF), and the CMS Medicare cost reports. The LTCFocus.org aggregates facility-level data drawn from different sources including Certification and Survey Provider Enhanced Reporting (OSCAR/CASPER) as well as the minimum data set (MDS).40 AHRF was utilized to obtain demographic and market data at the county level. Medicare cost reports provided data on nursing home financial performance. The primary and secondary data were merged using nursing home provider ID and year.
Variables
Dependent Variable
Total (profit) margin is a measure of overall financial performance and is defined as net income divided by total revenue. Net income is calculated as the difference between total revenue and total expenses of the nursing home.

Independent Variables
Mail surveys on EHR implementation assessed five functionalities: 1. administrative, 2. documentation, 3. order entry, 4. results viewing and 5. clinical tools. Administrative functions included processes and reporting such as scheduling systems and clinical task assignments. Documentation included health information and data such as resident demographics and medical history. Order entry had order management information including medication order entry. Results viewing had data on routing, managing, and presenting test results to clinical personnel for review. Clinical tool had decision support system and telemonitoring/telehealth data. Each item was assigned a score based on the response received: 0 = paper only, 1 = paper and electronic, 2 = fully electronic.
The independent variable, EHR implementation score (EIS), was the sum of scores received for each item across the five functionalities: administrative (6 items), documentation (9 items), order entry (2 items), results viewing (4 items), and clinical tools (2 items). For example, if the nursing home responded “fully electronic” for items across all assessed 23 functionalities, the EIS would total 46 points.
Control Variables
Control variables were identified based upon the organizational and market factors that may affect the financial performance of a nursing home.18,41 Organizational-level variables included ownership, chain affiliation, size, occupancy rate, presence of nurse practitioners/physician assistants (NPs/PAs), nurse staffing, acuity index, and proportion of racial/ethnic minorities. Ownership identified whether a nursing home was for-profit (0), not-for-profit (1) or government-owned (2). Chain affiliation reflected whether the nursing home was part of a chain (0 = freestanding; 1 = chain affiliated). Evidence suggests that for-profit chain affiliated nursing homes generally report better financial performance.42 Size captured the total number of beds within the nursing home. Larger nursing home would be expected to benefit financially from economies of scale and shared efficiencies. Occupancy rate was the percentage of occupied nursing home beds. It ranges from 0 to 100 where a higher number indicated more occupied beds in a facility. Higher occupancy rates often correlate with better financial performance due to increased revenue, allowing for better cost distribution across more residents. The presence of NPs/PAs reflected whether the nursing home utilized a NP/PA (0-no presence of NP/PA; 1 = presence of NP/PA). The presence of NPs/PAs in nursing homes can lead to better financial performance by optimizing patient care delivery and reducing hospital readmissions. Nurse staffing reflected three measures: registered nurse (RN) hours per resident day (PRD), licensed practical nurse (LPN) hours PRD, and certified nursing assistant (CNA) hours PRD. Nurse staffing is perhaps the most potent determinant of nursing home quality,43 and the literature has associated higher quality with better financial performance.44 The acuity index is a measure of care needed by residents in a nursing homes. It was calculated based on the number of residents requiring assistance with activities of daily living (ADL), such as bed mobility, transferring from bed to chair, as well as those needing special treatments like physical therapy or tube feeding. The acuity index ranged from 0 to 24, where the larger number indicated a resident requiring more specialized care.45 The proportion of racial/ethnic minorities was the proportion of nursing home residents who were Black, Hispanic, and other race/ethnicity. Evidence suggests that nursing homes with higher proportion of minority residents experience poorer financial performance.5
Market level variables included socio-economic factors that may affect the supply and demand for long-term care, and therefore the availability of environmental resources. Market factors were captured at the county level. Market variables included competition, Medicare Advantage (MA) market penetration, per capita income (U.S. dollars), unemployment rate, poverty level, education level, location (1 = urban, 0 = rural), and the proportion of population 65 and older.
Market competition was assessed through the Herfindahl-Hirschman Index (HHI), a metric that evaluates market concentration within an industry. It was calculated by summing the squared value of each nursing home’s market share based on inpatient days, with values ranging between 0 and 1. Higher values suggest greater market concentration, indicating more monopolistic markets, while lower values indicate higher competition. Nursing homes located in more competitive markets may experience inferior financial performance due to reduced pricing power. MA market penetration was calculated as the proportion of all Medicare beneficiaries in the county enrolled in an MA (managed care) plan. Research suggests that counties with higher MA penetration are more competitive.46 Per capita income is a measure of the average income of individuals in a county. Poverty level is the percentage of persons in the county in poverty. The unemployment rate refers to the percentage of individuals within a specific county’s labor force actively seeking employment but currently unemployed.47 Education level captured the percentage of population in the county that has greater than a high-school diploma. Counties with a higher per capita income, lower poverty level, lower unemployment rate, higher educational level, and urban location are expected to have greater environment munificence, resulting in better financial performance.42 Proportion of population 65 and older was calculated at the county level, with total county population as the denominator. A higher proportion is expected to correlate with increased demand for nursing home care.
Data Analysis
To adjust for potential non-response bias, we included propensity score weights in the regression analysis.48 The propensity score weights were calculated as the inverse of the propensity scores, using a logistic regression model where the outcome variable (respondent = 1, non-respondent = 0) was regressing on the following variables: occupancy, payer-mix, size (total beds), acuity index, chain affiliation, ownership status, resident racial/ethnicity mix, nurse staffing ratios, competition, Medicare Advantage penetration rate, unemployment rate, poverty level, education level, location, and the proportion of population 65 and older. Then, the inverse of the propensity score and the propensity score weight was calculated and included in the models. Respondents had higher occupancy rate and were more likely to be not-for-profit, compared to non-respondent nursing homes. On every other metric, both groups were similar.
As the dependent variable (total margin) was normally distributed, multivariable linear regression was used to model the relationship between EHR implementation (EIS) and financial performance (total margin), adjusting for both organizational and market-level variables. Stata 16 was utilized for data management and analysis, and statistical tests were evaluated at the 0.05 level of significance. The study was approved by the University of Alabama Institutional Review Board, and informed consent was taken from all the survey participants.
Results
Figure 2 illustrates the EHR implementation status in our sample. Approximately 44% of the nursing homes had fully implemented and operational EHR systems, while 32% had partially implemented and operational systems. Additionally, 11% were planning to implement EHR in the future, and 7% had no current implementation plans.In total, approximately 76% of the nursing homes in our study sample had either fully or partially implemented EHR systems. Figure 3 shows EHR implementation status among nursing homes in terms of the five functionalities. While 46% of nursing homes had fully implemented EHR for the more mundane administrative tasks, only 13% had implemented EHR for clinical tools.
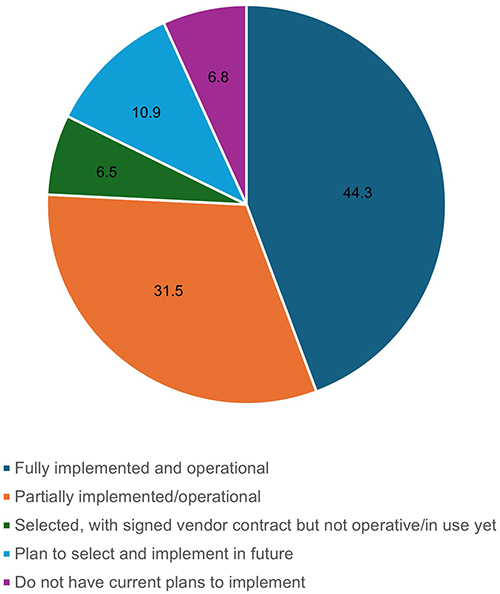 |
Figure 2 Status of Electronic Health Records Implementation in high Medicaid nursing homes (n = 391). Notes: About 44.3% nursing homes (blue) had a fully implemented and operational EHR. About 31.5% (green) nursing homes had a partially implemented and operational EHR. About 6.5% (red) nursing homes had selected a vendor and signed vendor contract but did not have an EHR in operation. About 10.9% (yellow) of nursing homes were planning to implement EHR in the future. about 6.8% (gray) nursing homes currently did not have a plan to implement EHR. |
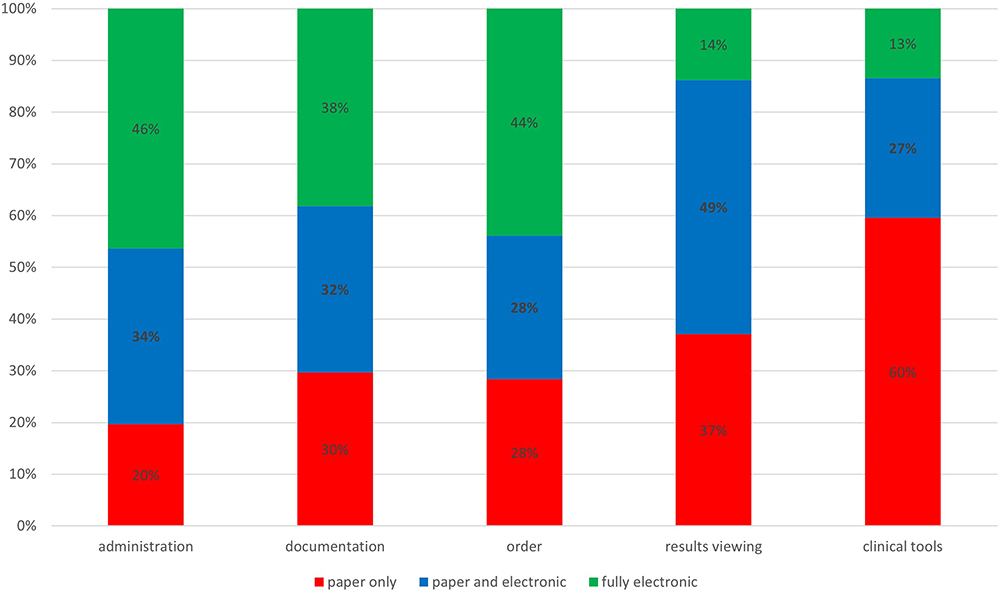 |
Figure 3 Electronic Health Records implementation in high Medicaid nursing homes by functionality (n = 391). Notes: EHR functionalities (administration, documentation, order, results viewing, and clinical tools), type of health record: red = paper only, blue = paper and electronic, and green = fully electronic. |
Table 1 presents the descriptive statistics for the sample. The mean total margin for our sample was 1.04%, while the average EIS score was 24.17. The average bed size was 103, while the occupancy rate was 85%. Most of the high Medicaid nursing homes were for-profit (68%), independent (58%), located in urban areas (94%) and in competitive markets (HHI = 0.22). With respect to race/ethnicity mix, 19% of residents were Black, 5% were Hispanic, and 14% were classified as “Other”.
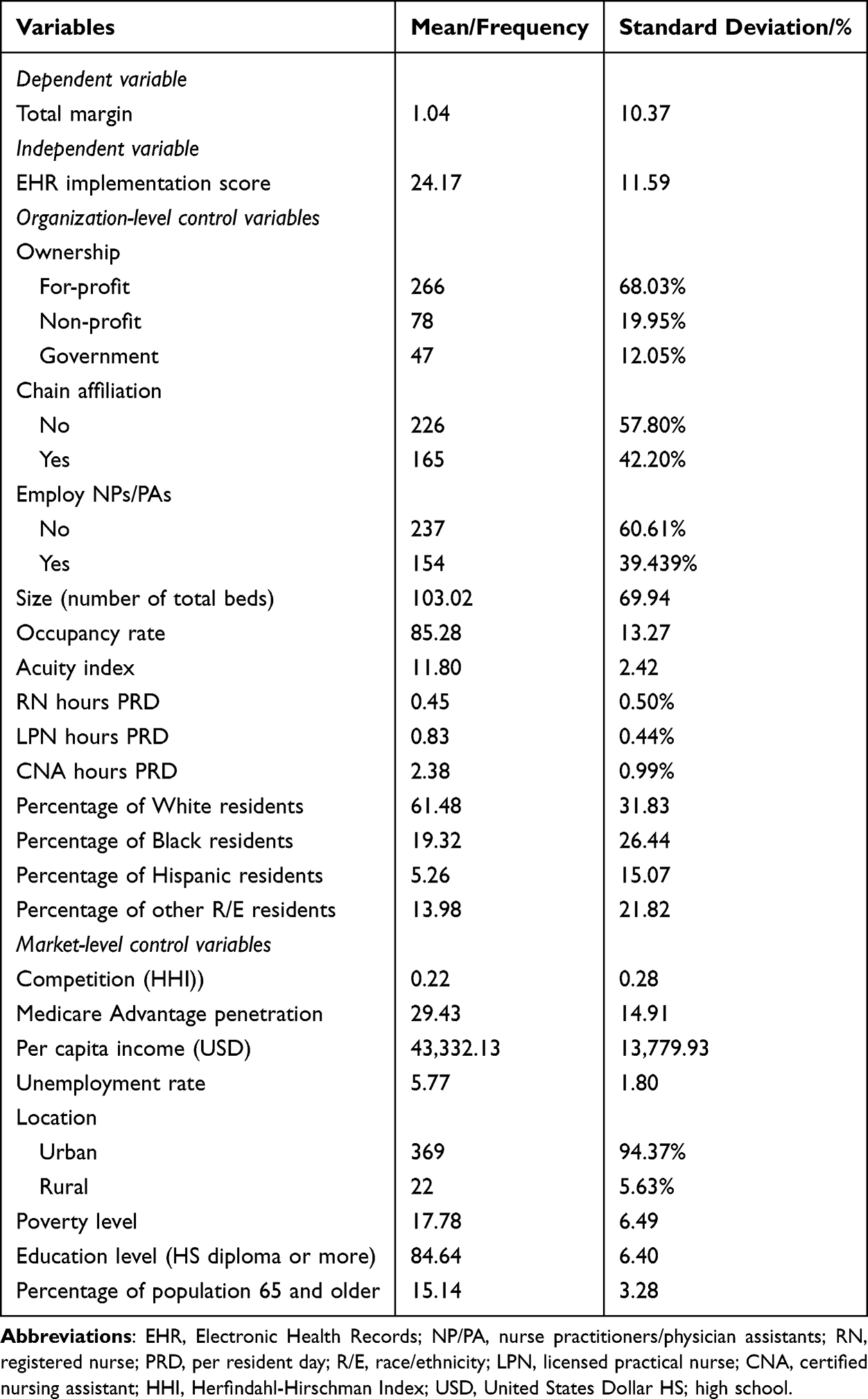 |
Table 1 Descriptive Statistics of the Sample (N = 391) |
Table 2 presents the results of the regression analysis. Each unit increase in EIS was associated with a 0.12% increase in total margin (p = 0.05). With respect to the control variables, total margin was 0.15% points higher for a unit increase in the occupancy rate (p < 0.001). All other results were statistically non-significant.
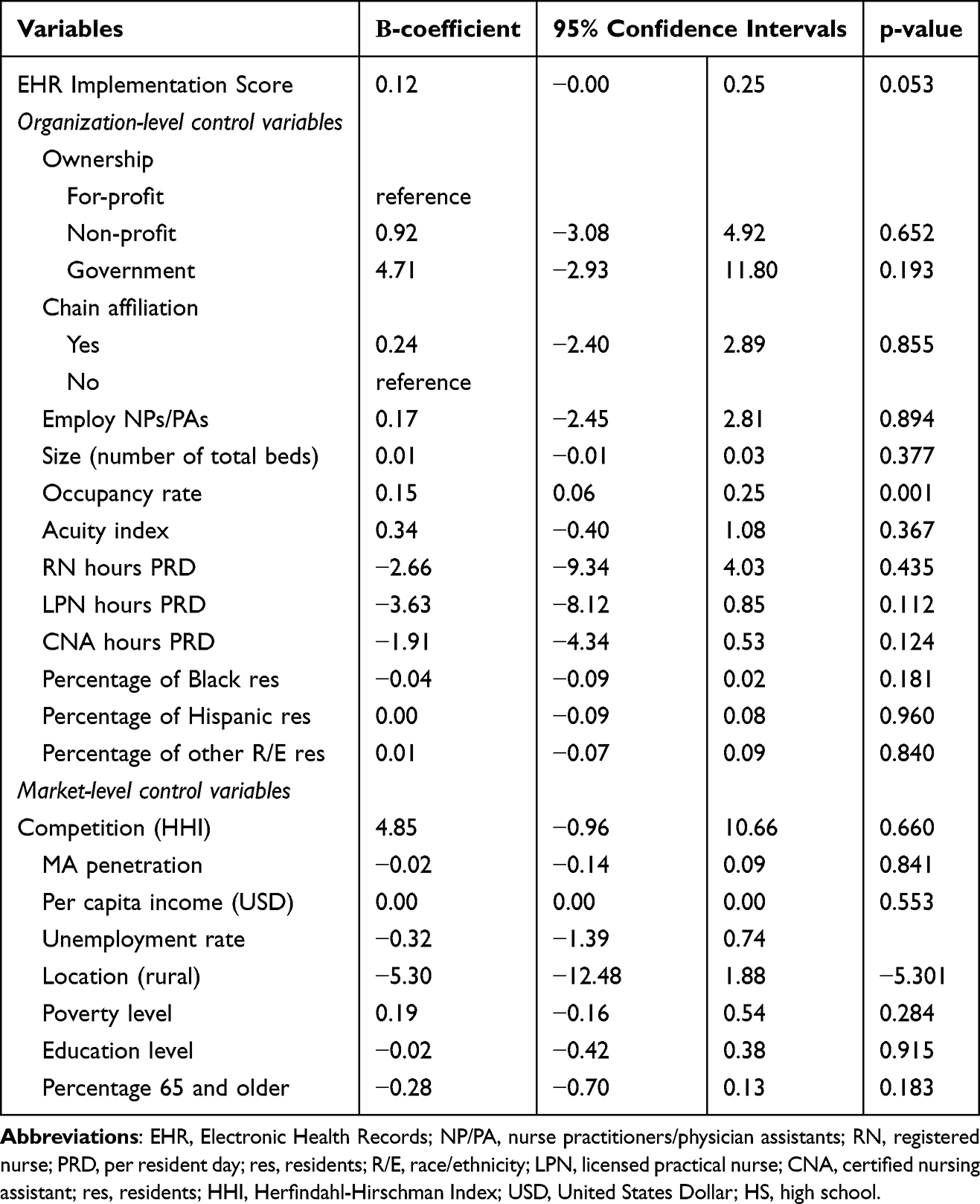 |
Table 2 Linear Multivariable Regression Model of Electronic Health Record Implementation on Total Margin (N = 391) |
Discussion
Drawing from the tenets of RBV, this study aimed to investigate the association between EHR implementation and financial performance within high Medicaid nursing homes. This research focused on high Medicaid facilities because they are classified as the “lower tier” among nursing homes, are under-resourced, and experience poor quality of care. These facilities often cater to marginalized populations, and improving their performance could address disparities within the nursing home industry. This study provides encouraging new evidence that these resource-constrained nursing homes may be able to improve their financial performance through EHR implementation.
Previous nursing home studies have reported sharply variable EHR implementation rates ranging from 18% to 84%,20,39,49 whereas the EHR implementation rates in hospitals and physician offices consistently exceed 90%.50,51 The results suggest that only 44% of high Medicaid nursing homes had a fully implemented and operational EHR. Although the samples are different and the definitions of EHR vary across studies, high Medicaid facilities appear to be trailing behind the average U.S. nursing home in EHR implementation.
As hypothesized, EHR implementation was associated with better financial performance (total margin). Nursing homes that implement EHR systems might experience increased revenue realization through improved coding efficiency, optimal utilization of available reimbursement methods, and accurate recording of comorbid illnesses.52 EHR-linked documentation management, medication safety, adverse event reporting, reduced time to access resident data, and claims management are some of the elements that may enhance efficiency and lower costs in nursing homes.17 Savings in operating expenses could also stem from a reduction in redundant tests, costs related to paper records, chart pulls, and transcription.35,53 Finally, nursing homes may be able to achieve a more lucrative patient profile by leveraging EHR implementation to signal superior quality, thereby enhancing their market power.
Managerial and Policy Implications
This study should provide cautious optimism to administrators of high Medicaid nursing homes wrestling with the decision to invest in an EHR system while still navigating a financially precarious environment. The findings suggest a positive correlation between EHR implementation and profitability, offering a compelling incentive for administrators to prioritize investments in EHR systems. However, the data also reveal a significant gap between EHR implementation for relatively mundane administrative tasks, and its application in more complex clinical operations, which require a higher level of employee training. Therefore, to realize the full potential of EHR systems, healthcare organizations must continue investing in both IT infrastructure and human resources.
Policymakers and regulators may not be overly concerned with nursing homes’ financial performance, but their viability and the ability to deliver a minimally adequate level of care are certainly important considerations. Poor financial performance can result in nursing home closures, significantly affecting access to long-term care, particularly in underserved communities.54 An important reason nursing homes lag hospitals and physician offices on EHR implementation is because they were excluded from the subsidies provided by the HITECH Act.19 Consequently, a financial incentive structure analogous to the HITECH Act may be required to stimulate EHR implementation in nursing homes, particularly those with high Medicaid populations.
Even if subsidies were extended to nursing homes, policymakers might have a legitimate concern: would facilities, especially those with high Medicaid census, have the financial wherewithal to make the ongoing investments required to fully leverage their EHR systems? Establishing a business case for EHR implementation outlines a potential scenario wherein subsidies stimulate the initial implementation, while the financial gains encourage facilities to perceive EHR systems as an asset rather than a regulatory burden. Furthermore, the importance of efficient and accurate health information exchange has been highlighted by the COVID-19 pandemic which disproportionately affected nursing homes.55 Thus, a business case for EHR implementation could ensure continued investments, making EHR systems sustainable and beneficial in the long term.
This study presents certain limitations. First, our study sample was limited to high Medicaid nursing homes. Therefore, our findings may not be generalizable to the larger nursing home population. To address this, future studies should investigate the financial impact of EHR implementation across a more diverse array of nursing home settings. Second, our criteria for defining high Medicaid nursing homes, although based on previous literature, may be deemed overly restrictive considering the significant changes that have occurred in the nursing home environment over the past two decades. Therefore, future research should examine potential revisions to these criteria to evaluate their relevance and accuracy. Third, a cross-sectional study contributes to the extant literature; however, it cannot evaluate longitudinal effects over time. Additionally, nursing homes with better financial performance may be more inclined to implement EHR. Future studies that collect longitudinal data may offer a more nuanced understanding of the evolving financial impact of EHR systems in nursing homes. Fourth, despite our best attempts to measure EHR implementation, there is a need to better operationalize the combined effects of individual EHR functionalities, as done in the case of hospitals.56 Future research should quantitatively assess the contribution of individual EHR functionalities to nursing home performance as that may lead to more precise and actionable findings. Furthermore, it is important to note that the data for our study were collected in 2017–2018, prior to the significant disruptions caused by the COVID-19 pandemic. The pandemic has profoundly altered the landscape of nursing home operations, making it imperative to utilize more recent data to assess the current state of EHR implementation in nursing homes and its impact on performance. Finally, we must acknowledge the possibility of survey response bias as nursing homes that have implemented or are planning to implement EHR have a higher likelihood of responding to surveys of this nature.
Conclusions
The purpose of this study was to examine the impact of EHR implementation on the financial performance of high Medicaid nursing homes. The results indicated a positive influence, demonstrating how EHR systems may financially benefit resource-constrained nursing homes that are responsible for the health and well-being of some of the most vulnerable Americans. The findings of this study offer a rationale for targeted policy efforts to ensure that U.S. nursing homes are no longer the laggards in EHR implementation. It is untenable to exclude nursing homes from incentives available to other sectors of the U.S. healthcare system. For nursing home administrators, the results highlight a potential business case for EHR implementation, with the long-term financial gains outweighing the initial burden of implementation.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request. Publicly available datasets used in this study can be found here: https://www.cms.gov/.
Ethics Statement
This study was performed in accordance with the Declaration of Helsinki ethical principles for medical research involving human subjects. It was reviewed and approved by the University of Alabama at Birmingham’s Institutional Review Board (IRB-140828005). Informed consent to participate was obtained from all survey participants.
Acknowledgments
The abstract of this paper was presented at the Gerontological Society of America’s Annual Scientific Meeting (2022) as an oral presentation with interim findings. The presentation’s abstract was published in “Innovations in Aging” 2 (1), 599–600.
The abstract of this paper was presented at the AcademyHealth’s Annual Research Meeting (2018) as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts”andisavailablehere: https://academyhealth.confex.com/academyhealth/2022arm/meetingapp.cgi/Paper/53787
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Agency for Healthcare Research and Quality (1R01HS023345-01).
Disclosure
The authors declare no competing interests in this work.
References
1. National Center for Health Statistics. Nursing Home Care; 2018. Available from: https://www.cdc.gov/nchs/fastats/nursing-home-care.htm.
2. Welch WP, Ruhter J, Bosworth A, Lew N, Sommers BD Changes of ownership of hospital and skilled nursing facilities: an analysis of newly-released CMS data; 2022. Available from: https://aspe.hhs.gov/reports/changes-ownership-hospital-skilled-nursing-facilities.
3. Singletary E, Roiland R, Harker M, Taylor D Value-based payment and skilled nursing facilities: supporting SNFs during COVID19 and beyond; 2021.
4. The Medicaid and CHIP Payment and Access Commission.Estimates of Medicaid nursing facility payments relative to costs; 2023. Available from: https://www.macpac.gov/publication/estimates-of-medicaid-nursing-facility-payments-relative-to-costs/.
5. Mor V, Zinn J, Angelelli J, Teno JM, Miller SC. Driven to tiers: socioeconomic and racial disparities in the quality of nursing home care. Milbank Q. 2004;82(2):227–256. doi:10.1111/j.0887-378X.2004.00309.x
6. Gandhi A, Yu H, Grabowski DC. High nursing staff turnover in nursing homes offers important quality information: study examines high turnover of nursing staff at us nursing homes. Health Affairs. 2021;40(3):384–391. doi:10.1377/hlthaff.2020.00957
7. Grabowski DC, Angelelli JJ, Mor V. Medicaid payment and risk-adjusted nursing home quality measures. Health Affairs. 2004;23(5):243–252. doi:10.1377/hlthaff.23.5.243
8. Bowblis JR. Ownership conversion and closure in the nursing home industry. Health Econ. 2011;20(6):631–644. doi:10.1002/hec.1618
9. Centers for Medicare & Medicaid Services. Electronic Health Records; 2023. Available from: https://www.cms.gov/priorities/key-initiatives/e-health/records.
10. Alexander GL, Travers J, Galambos C, Rantz M, Ferrell B, Stevenson D. Strategic recommendations for higher quality nursing home care in the United States: the NASEM report. Res Gerontol Nurs. 2022;15(6):266–269.
11. Adler-Milstein J, Jha AK. HITECH Act drove large gains in hospital electronic health record adoption. Health Affairs. 2017;36(8):1416–1422. doi:10.1377/hlthaff.2016.1651
12. Castaneda C, Nalley K, Mannion C, et al. Clinical decision support systems for improving diagnostic accuracy and achieving precision medicine. J Clin Bioinform. 2015;5(1):1–16. doi:10.1186/s13336-015-0019-3
13. Radley DC, Wasserman MR, Olsho LE, Shoemaker SJ, Spranca MD, Bradshaw B. Reduction in medication errors in hospitals due to adoption of computerized provider order entry systems. J Am Med Inf Assoc. 2013;20(3):470–476. doi:10.1136/amiajnl-2012-001241
14. Tanner C, Gans D, White J, Nath R, Pohl J. Electronic health records and patient safety. Appl Clin Inform. 2015;6(01):136–147. doi:10.4338/ACI-2014-11-RA-0099
15. Bjarnadottir RI, Herzig CT, Travers JL, Castle NG, Stone PW. Implementation of electronic health records in US nursing homes. Comput Inform Nurs. 2017;35(8):417. doi:10.1097/CIN.0000000000000344
16. Handler SM, Sharkey SS, Hudak S, Ouslander JG. Incorporating INTERACT II clinical decision support tools into nursing home health information technology. Ann Longterm Care. 2011;19(11):23–26.
17. Kruse CS, Mileski M, Vijaykumar AG, Viswanathan SV, Suskandla U, Chidambaram Y. Impact of electronic health records on long-term care facilities: systematic review. JMIR Med Inform. 2017;5(3):e7958. doi:10.2196/medinform.7958
18. Weech-Maldonado R, Pradhan R, Dayama N, Lord J, Gupta S. Nursing home quality and financial performance: is there a business case for quality? Inquiry. 2019;56:0046958018825191. doi:10.1177/0046958018825191
19. Alvarado CS, Zook K, Henry J. Electronic health record adoption and interoperability among US skilled nursing facilities in 2016. ONC Data Brief. 2017;39.
20. Wang T, Biedermann S. Adoption and utilization of electronic health record systems by long-term care facilities in Texas. Perspect Health Inf Manag. 2012;9(Spring).
21. Dougherty ML, Williams M, Millenson ML, Harvell J. EHR Payment Incentives for Providers Ineligible for Payment Incentives and Other Funding Study. Washington D.C: Office of Disability, Aging and Long-Term Care Policy, Department of Health and Human Services; 2013.
22. Federal register medicare and Medicaid program; patient protection and affordable care act; interoperability and patient access. Available from: https://www.federalregister.gov/documents/2020/05/01/2020-05050/medicare-and-medicaid-programs-patient-protection-and-affordable-care-act-interoperability-and.
23. Filipova AA. Electronic health records use and barriers and benefits to use in skilled nursing facilities. CIN. 2013;31(7):305–318. doi:10.1097/NXN.0b013e318295e40e
24. Fleming NS, Becker ER, Culler SD, et al. The impact of electronic health records on workflow and financial measures in primary care practices. Health Serv Res. 2014;49(1pt2):405–420. doi:10.1111/1475-6773.12133
25. Bowblis JR, Applebaum R. How does Medicaid reimbursement impact nursing home quality? The effects of small anticipatory changes. Health Serv Res. 2017;52(5):1729–1748. doi:10.1111/1475-6773.12553
26. Collum TH, Menachemi N, Sen B. Does electronic health record use improve hospital financial performance? Evidence from panel data. Health Serv Manag Rev. 2016;41(3):267–274. doi:10.1097/HMR.0000000000000068
27. Wang T, Wang Y, McLeod A. Do health information technology investments impact hospital financial performance and productivity? Int J Account Inf Syst. 2018;28:1–13. doi:10.1016/j.accinf.2017.12.002
28. Hitt LM, Tambe P. Health care information technology, work organization, and nursing home performance. ILR Rev. 2016;69(4):834–859. doi:10.1177/0019793916640493
29. Barney J. Firm resources and sustained competitive advantage. J Manage. 1991;17(1):99–120. doi:10.1177/014920639101700108
30. Bharadwaj AS. A resource-based perspective on information technology capability and firm performance: an empirical investigation. MIS Quarterly. 2000;24(1):169–196. doi:10.2307/3250983
31. Barney J, Wright M, Ketchen DJ. The resource-based view of the firm: ten years after 1991. J Manage. 2001;27(6):625–641. doi:10.1177/014920630102700601
32. Miller RH, West C, Brown TM, Sim I, Ganchoff C. The value of electronic health records in solo or small group practices. Health Affairs. 2005;24(5):1127–1137. doi:10.1377/hlthaff.24.5.1127
33. Wiggins RR, Ruefli TW. Sustained competitive advantage: temporal dynamics and the incidence and persistence of superior economic performance. Organ Sci. 2002;13(1):81–105. doi:10.1287/orsc.13.1.81.542
34. Werner RM, Konetzka RT, Polsky D. Changes in consumer demand following public reporting of summary quality ratings: an evaluation in nursing homes. Health Serv Res. 2016;51(S2):1291–1309. doi:10.1111/1475-6773.12459
35. Chen P, Tanasijevic MJ, Schoenenberger RA, Fiskio J, Kuperman GJ, Bates DW. A computer-based intervention for improving the appropriateness of antiepileptic drug level monitoring. Am J Clin Pathol. 2003;119(3):432–438. doi:10.1309/A96XU9YKU298HB2R
36. Levine DM, Healey MJ, Wright A, Bates DW, Linder JA, Samal L. Changes in the quality of care during progress from stage 1 to stage 2 of Meaningful Use. J Am Med Inf Assoc. 2017;24(2):394–397. doi:10.1093/jamia/ocw127
37. Menachemi N, Collum TH. Benefits and drawbacks of electronic health record systems. Risk Manag Healthc Policy. 2011;47–55. doi:10.2147/RMHP.S12985
38. Dillman DA. Mail and Telephone Surveys: The Total Design Method. Vol. 19. New York: Wiley; 1978.
39. Abramson EL, McGinnis S, Moore J, Kaushal R, Investigators H. A statewide assessment of electronic health record adoption and health information exchange among nursing homes. Health Serv Res. 2014;49(1pt2):361–372. doi:10.1111/1475-6773.12137
40. LTCFocus. Who are We; 2023. Avalable from: https://ltcfocus.org/about.
41. Pradhan R, Ghiasi A, Ganisher D, Orewa GN, Weech-Maldonado R. Beyond the balance sheet: investigating the association between NHA turnover and nursing home financial performance. Risk Manag Healthc Policy. 2024;17:249–260. doi:10.2147/RMHP.S421889
42. Weech-Maldonado R, Laberge A, Pradhan R, Johnson CE, Yang Z, Hyer K. Nursing home financial performance: the role of ownership and chain affiliation. Health Serv Manag Rev. 2012;37(3):235–245. doi:10.1097/HMR.0b013e31823dfe13
43. Abt Associates. Nursing home staffing study; 2023.
44. Weech-Maldonado R, Neff G, Mor V. Does quality of care lead to better financial performance?: the case of the nursing home industry. Health Serv Manag Rev. 2003;28(3):201–216. doi:10.1097/00004010-200307000-00002
45. Orewa GN, Davlyatov G, Pradhan R, Lord J, Weech-Maldonado R. High Medicaid nursing homes: contextual factors associated with the availability of specialized resources required to care for obese residents. J Aging Soc Policy. 2023;36(1):1–18.
46. Weech-Maldonado R, Lord J, Pradhan R, et al. High Medicaid nursing homes: organizational and market factors associated with financial performance. INQUIRY. 2019;56:0046958018825061. doi:10.1177/0046958018825061
47. U.S. Department of Agriculture. Economic research service: county-level data sets; 2022.
48. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399–424. doi:10.1080/00273171.2011.568786
49. Zhang N, Lu SF, Xu B, Wu B, Rodriguez-Monguio R, Gurwitz J. Health information technologies: which nursing homes adopted them? J Am Med Directors Assoc. 2016;17(5):441–447. doi:10.1016/j.jamda.2016.02.028
50. Charles D, Gabriel M, Searcy T. Adoption of electronic health record systems among US non-federal acute care hospitals: 2008–2014. ONC Data Brief. 2015;23(4).
51. Centers for Disease Control and Prevention. National electronic health records survey: 2015 state and national electronic health record adoption summary tables; 2015. Available from: https://www.cdc.gov/nchs/data/ahcd/nehrs/2015_nehrs_web_table.pdf.
52. Britton JR. Healthcare reimbursement and quality improvement: integration using the electronic medical record: comment on” fee-for-service payment-an evil practice that must be stamped out?”. Int J Health Policy Manag. 2015;4(8):549. doi:10.15171/ijhpm.2015.93
53. Bates DW, Kuperman GJ, Rittenberg E, et al. A randomized trial of a computer-based intervention to reduce utilization of redundant laboratory tests. Am j Med. 1999;106(2):144–150. doi:10.1016/S0002-9343(98)00410-0
54. Hughes K, Feng Z, Li Q, Segelman M, Oliveira I, Dey JG. Rates of nursing home closures were relatively stable over the past decade, but warrant continuous monitoring. Health Aff Sch. 2023;1(2):qxad025. doi:10.1093/haschl/qxad025
55. Chidambaram P Over 200,000 residents and staff in long-term care facilities have died from COVID-19; 2022. Available from: https://www.kff.org/policy-watch/over-200000-residents-and-staff-in-long-term-care-facilities-have-died-from-covid-19/.
56. Healthcare Information and Management Systems Society. HIMSS electronic medical records adoption model; 2018. Available from: https://www.himssanalytics.org/europe/electronic-medical-record-adoption-model.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.