Back to Journals » Journal of Pain Research » Volume 18
Electroacupuncture for the Subacute Stage of Lumbar Disc Herniation: A Randomized Controlled Trial Protocol with EEG
Authors Yu H, Zhang J, Zhang D, Zhao L, Wu S, Zhang L, Yang Y, Li G
Received 2 August 2025
Accepted for publication 6 November 2025
Published 26 November 2025 Volume 2025:18 Pages 6279—6295
DOI https://doi.org/10.2147/JPR.S557800
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Hanbo Yu,* Jie Zhang,* Dingchen Zhang, Lingyan Zhao, Sixian Wu, Luofan Zhang, Youlie Yang, Guiping Li
National Clinical Research Center for Chinese Medicine Acupuncture and Moxibustion, First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guiping Li, National Clinical Research Center for Chinese Medicine Acupuncture and Moxibustion, First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China, Email [email protected]
Purpose: This study aims to elucidate the central mechanisms of electroacupuncture (EA) for subacute lumbar disc herniation (LDH) using electroencephalography (EEG). To our knowledge, this is the first study to apply EEG to characterize the neurophysiological correlates of EA treatment in this specific clinical condition.
Patients and Methods: In this randomized controlled trial, a total of 66 patients with subacute lumbar disc herniation (LDH) will be enrolled from the Departments of Acupuncture and Orthopedics. Participants will be randomly allocated at a 1:1 ratio to either an EA group or a sham EA group, resulting in 33 participants per group. The primary outcomes are the clinical efficacy rate and the Japanese Orthopaedic Association (JOA) score. Secondary outcomes include the Oswestry Disability Index (ODI) and the Visual Analogue Scale (VAS) for pain. Clinical outcomes will be assessed at baseline, two weeks, four weeks (end of treatment), and at a three-month follow-up. The neuroimaging outcome is EEG. EEG data will be collected at baseline and at the four-week endpoint, with analyses focusing on core parameters such as power spectral density (PSD) analysis, time-frequency analysis, and microstate analysis.
Conclusion: This study will verify the clinical efficacy of electroacupuncture in treating subacute LDH and explore its core central mechanisms using EEG technology. We anticipate that the expected improvements in clinical outcomes (eg, JOA, ODI, and VAS scores) will significantly correlate with the normalization of aberrant neural oscillations—specifically, a reduction in theta power and restoration of alpha activity. Such findings would provide direct neuroimaging evidence for EA’s central neuromodulatory role, offering a mechanistic basis for its broader clinical application in the treatment of LDH.
Keywords: lumbar disc herniation, electroacupuncture, electroencephalography, protocol
Introduction
Lumbar disc herniation (LDH), a common degenerative condition of the spine, occurs when the nucleus pulposus extrudes through a tear in the annulus fibrosus. The resulting compression of neural structures, such as nerve roots or the cauda equina, culminates in a clinical syndrome of low back and leg pain, sensory deficits, and motor dysfunction.1 The clinical course of LDH can be classified into acute, subacute, and recovery stages. The subacute stage, defined by a Visual Analogue Scale (VAS) score of 4 to <7, is particularly critical as it represents a key therapeutic window that dictates long-term prognosis.2 Although patients in this phase experience partial symptomatic relief, they often suffer from persistent pain and limited physical endurance. With a lifetime prevalence approaching 30% and a 1–3% risk of symptomatic episodes,3 LDH poses a significant healthcare burden. The current standard of care encompasses both conservative and surgical strategies. Although non-steroidal anti-inflammatory drugs (NSAIDs) and physical therapy are considered first-line conservative treatments, their efficacy for sustained management is often limited. Furthermore, the clinical use of NSAIDs is constrained by their well-documented gastrointestinal and cardiovascular side effects.4,5 While surgical interventions like discectomy can offer expedited relief for severe, refractory cases,6 their long-term superiority is not definitively established. Notably, the landmark Spine Patient Outcomes Research Trial (SPORT) demonstrated a convergence of outcomes between surgical and non-surgical cohorts at 4- and 8-year follow-ups.7 Moreover, surgery is associated with inherent risks and a non-negligible recurrence rate, compelling up to 3.2% of patients to undergo reoperation for recurrent sciatica.8 Consequently, the pronounced limitations in both the long-term efficacy and safety of current paradigms create a compelling need for novel, mechanism-based therapies that can offer a more durable and safer solution for LDH.
The failure of conventional therapies to deliver sustained long-term relief can be attributed to a crucial paradigm shift in our understanding of chronic pain. It is now increasingly recognized that as LDH-associated acute pain becomes chronic, the condition transcends its origins as a local biomechanical problem to become a disorder of the central nervous system (CNS).9 The underlying mechanism is the induction of maladaptive neuroplasticity by persistent nociceptive signaling, with central sensitization as its clinical hallmark.10 Central sensitization fundamentally rewires pain processing circuits, resulting in lowered pain thresholds and an amplified pain experience. This central reorganization is substantiated by functional neuroimaging evidence, which reveals profound remodeling of brain networks in chronic pain patients. Notably, key networks integral to pain, emotion, and cognition, including the Salience Network (SN) and Default Mode Network (DMN), display significantly disrupted functional connectivity.11 Consequently, this evidence strongly suggests that a truly effective long-term therapeutic strategy must target and reverse these central pathological alterations, rather than solely addressing the peripheral source of pain.
Electroacupuncture (EA), a modern integration of traditional acupuncture with electrical stimulation, is emerging as a compelling therapeutic modality due to its capacity for multi-level neuromodulation. The mechanisms of EA extend far beyond the periphery and spinal cord, where it provides analgesia and anti-inflammatory relief by triggering the release of endogenous opioids, suppressing nociceptor activity, and downregulating pro-inflammatory cytokines like TNF-α and IL-6.12,13 Crucially, mounting evidence highlights the potent supraspinal effects of EA, demonstrating its ability to directly modulate brain activity. Preclinical studies have elucidated that EA mitigates central neuroinflammation and hyperalgesia by restraining microglial over-activation, steering microglial polarization towards an anti-inflammatory M2 phenotype, and modulating pivotal signaling cascades such as the CB2 receptor and NF-κB pathways.14 These preclinical findings are mirrored in clinical research, where EA as an adjunctive therapy significantly lowers VAS scores and systemic inflammatory markers in patients with LDH.15 Taken together, this body of evidence positions EA as a unique therapeutic strategy that can concurrently target the dual pathologies of peripheral inflammation and central sensitization.
Ascertaining the central effects of electroacupuncture necessitates an objective, real-time measure of brain function. While subjective pain scales such as the VAS and ODI remain the clinical gold standard, their inherent susceptibility to patient emotion, expectation, and recall bias limits their utility in precisely tracking therapy-induced neurofunctional changes. Resting-state functional magnetic resonance imaging (fMRI) is highly sensitive to changes in blood oxygen level-dependent (BOLD) signals and provides excellent spatial resolution, enabling the assessment of functional connectivity across different brain regions.16 However, it is limited by temporal resolution and faces challenges such as non-portability, high operational costs, and complex data interpretation.17 Near-infrared spectroscopy (NIRS) offers an innovative approach to studying brain function by monitoring changes in cortical blood oxygen saturation.18 Despite its novelty, NIRS is constrained by both spatial and temporal resolution limitations and is highly susceptible to motion artifacts that can significantly distort results. EEG provides an ideal “window” into the central mechanisms of pain, owing to its non-invasive nature and outstanding temporal resolution at the millisecond scale. A substantial body of research confirms that EEG can reliably detect characteristic alterations in neural oscillatory patterns linked to chronic pain.19–21 For example, elevated theta band power and suppressed or slowed alpha band activity during resting-state are well-documented features across numerous chronic pain conditions, including LDH.22 These specific rhythmic alterations are widely regarded as the core electrophysiological signatures of central sensitization. Yet, how electroacupuncture intervention modulates these aberrant neural oscillations in patients during the subacute stage of LDH remains a critical and unanswered question. Research has demonstrated that in patients with subacute peripheral pain, pain intensity is positively correlated with alpha wave activity in central brain regions during resting-state conditions.23 This change suggests that the brain may begin to overreact to persistent pain signals, signaling the onset of central sensitization. These findings provide evidence that pathological changes in the central nervous system may initiate during this phase. Thus, the subacute phase not only serves as a recovery period for peripheral injuries but also represents a critical juncture for functional changes in the central nervous system, thereby providing a theoretical basis for early intervention.
Despite preliminary evidence supporting the efficacy of EA for LDH,24 the current body of research suffers from critical limitations. There is a notable paucity of high-quality, rigorously designed RCTs employing an adequate sham-EA control. Moreover, there is a near-complete absence of studies elucidating the central mechanisms that may underline the long-term benefits of EA.
This study was designed to address these deficiencies with several key innovations. We are the first to: 1) specifically target the subacute LDH population, a critical window for the potential transition to chronic pain; 2) implement a rigorous, sham-controlled RCT design within this cohort; and 3) leverage multidimensional EEG analysis to systematically decode the electrophysiological underpinnings of EA’s therapeutic effects. Accordingly, we posit the primary hypothesis that verum EA will yield superior improvements in clinical outcomes (pain and function) over sham EA. Our secondary hypothesis is that these clinical improvements will be directly associated with the normalization of aberrant neural oscillations—specifically, a significant reduction in theta power and restoration of alpha activity—indicative of a reversal of central sensitization. The overarching aims of this study are therefore to furnish high-level evidence for the clinical utility of EA in subacute LDH and to provide the first objective, electrophysiological account of its central mechanisms.
Materials and Methods
Study Design
This single-center, randomized controlled trial (RCT) will be conducted at the First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, China. The study protocol was approved by the institutional Ethics Committee (Approval No.: TYLL2025[K]No.023) and prospectively registered with the International Traditional Medicine Clinical Trial Registration Platform (ITMCTR; Registration No.: ITMCTR2025000889). All procedures will be performed in accordance with the ethical standards of the Declaration of Helsinki.
We designed this trial protocol according to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT),25 with the corresponding checklist in Table 1. For the final report, we will adhere to the Consolidated Standards of Reporting Trials (CONSORT) and the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) guidelines,26(Supplementary Table S1).
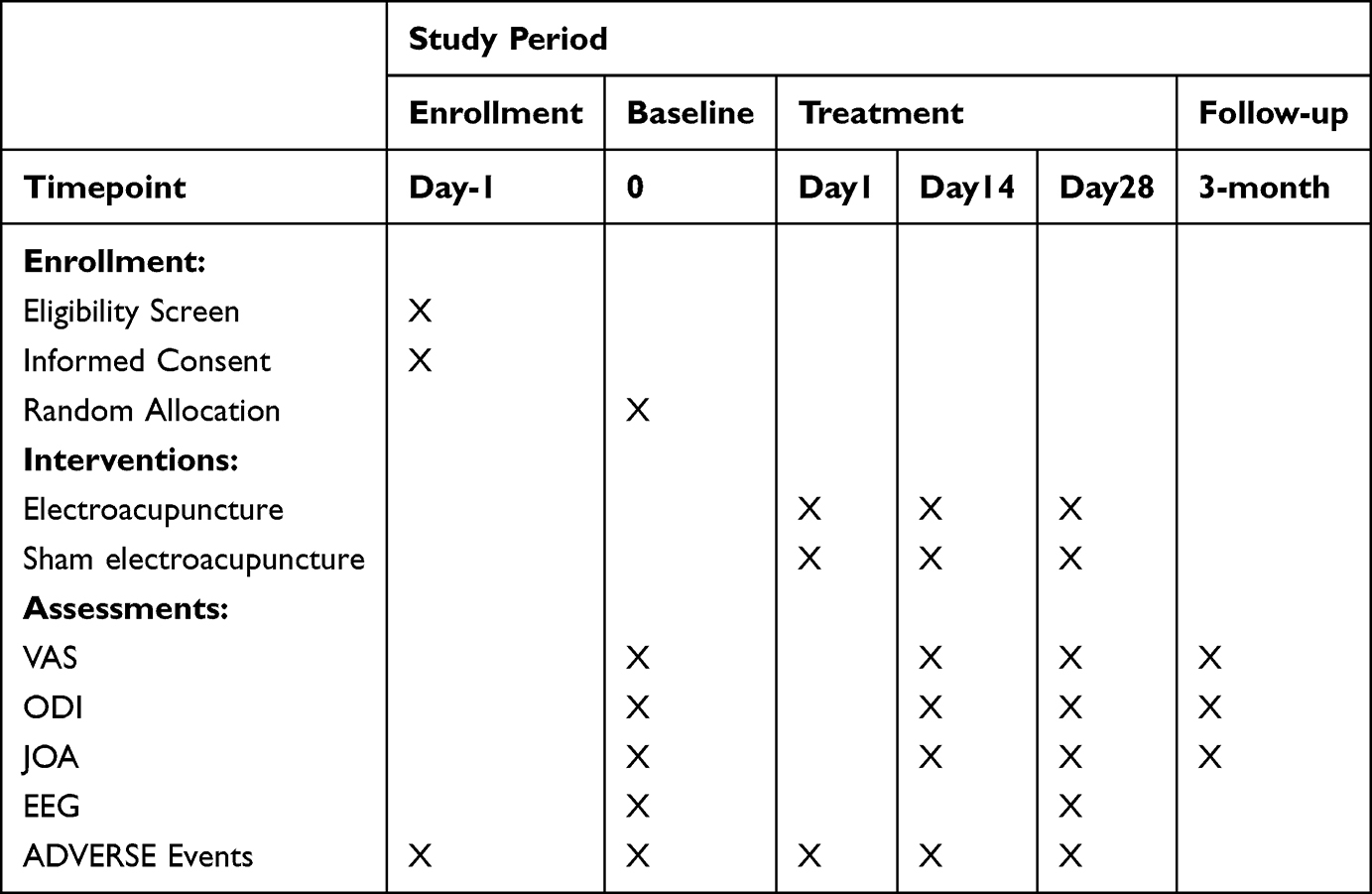 |
Table 1 Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) Schedule of the Trial |
Study Participants
This study aims to recruit 66 patients with subacute LDH. Eligibility for enrollment requires that all participants meet the specified inclusion criteria and provide written informed consent.
Inclusion Criteria
Individuals will be included in the study provided that they met all the following criteria:
- A clinical diagnosis of LDH that meets the established diagnostic criteria3 and is classified as being in the subacute stage.2
- Radiological evidence from Computed Tomography (CT) or Magnetic Resonance Imaging (MRI) confirming disc herniation at one or more levels between L3 and S1.
- Aged between 18 and 59 years, inclusive.
- Right-handed.
- Able to comprehend and cooperate with the study procedures, including the requirements for EEG data acquisition.
- Voluntarily agrees to participate and has provided written informed consent.
Exclusion Criteria
Individuals meeting any of the following criteria will be excluded from study enrollment:
- Clear indications for immediate lumbar surgery, such as cauda equina syndrome or progressive, severe neurological deficits.
- Pregnancy, lactation, or planning to become pregnant during the study period.
- Presence of severe or unstable concurrent diseases, including cardiovascular, cerebrovascular, hepatic, or renal conditions, as well as severe psychiatric or psychological disorders.
- Coexisting acute or chronic pain conditions that could confound the assessment of pain related to LDH.
- Any contraindications to acupuncture or electroacupuncture treatment (eg, severe needle phobia, localized skin infections at acupoints, or certain medical implants like cardiac pacemakers).
Intervention Measures
All participants, regardless of group allocation, will receive standardized health education. This includes instructions on maintaining healthy lifestyle habits, avoiding exposure to cold, adopting proper sitting and standing postures, and guidance on performing appropriate back exercises.
EA Group
Acupoint Selection
The following acupoints on the affected side will be selected: Shenshu (BL23), Dachangshu (BL25), Zhibian (BL54), and Weizhong (BL40). The location of all acupoints will adhere to the World Health Organization (WHO) Standard Acupuncture Locations.
Needling Procedure
After standard skin disinfection at the acupoint sites, sterile, single-use acupuncture needles (0.25 × 40 mm; Suzhou Medical Appliance Factory Co., Ltd., Suzhou, China) will be inserted perpendicularly to a depth of 1.0–1.5 cun. The needles will be manually manipulated until the De-qi sensation (characterized by soreness, numbness, distension, or heaviness) is achieved.
EA Parameters
The positive and negative electrodes of an SDZ-III electroacupuncture device (Hwato brand; Suzhou Medical Appliance Factory Co., Ltd., Suzhou, China; Registration No. Su Xie Zhu Zhun 20172270675) will be connected to the needles at BL23 and BL25 on the ipsilateral side. The stimulation will be delivered with a continuous wave at a frequency of 2 Hz and an intensity of 2 mA, or adjusted to the patient’s maximum tolerance without causing pain.
Treatment Regimen
To achieve the highest degree of procedural fidelity and to eliminate inter-operator variability, a critical source of potential bias, all treatments for all participants in both the verum EA and sham EA groups will be performed by a single, licensed acupuncturist with over 10 years of clinical experience. Prior to the trial’s commencement, this acupuncturist will conduct several practice runs of both the verum and sham protocols to ensure complete adherence to the standardized procedures outlined in this manuscript. The treatment will be administered twice a week for four consecutive weeks, for a total of eight sessions. The needle retention time for each session will be 30 minutes.
Sham EA Group
The sham EA group will receive a treatment involving shallow needling at non-acupoints, designed to be a credible placebo control and ensure patient blinding. This type of invasive sham control is well-established in the literature and has been shown to be effective in minimizing placebo effects while maintaining the integrity of participant blinding in numerous clinical trials.27,28 The procedure is designed to mimic the initial sensation and visual cues of the verum EA treatment without eliciting a true therapeutic response.
Sham Acupoint Selection and Localization
To ensure standardization and replicability, four non-acupoint locations will be used. These points are intentionally located away from major meridians and are defined by precise anatomical landmarks (see also Supplementary Figure S1):
Sham Point 1
At the level of the lower border of the spinous process of the second lumbar vertebra (L2), approximately 2.5 cun lateral to the posterior midline.
Sham Point 2
At the level of the lower border of the spinous process of the fourth lumbar vertebra (L4), approximately 2.5 cun lateral to the posterior midline.
Sham Point 3
At the level of the fourth posterior sacral foramen, approximately 4 cun lateral to the posterior midline.
Sham Point 4
At a point 2 cm superior and 2 cm lateral to the midpoint of the transverse popliteal crease.
Sham Procedure
After standard skin disinfection, the same type of needles will be used. The needles will be inserted superficially to a depth of only 2–3 mm at the non-acupoint locations, without any manual manipulation to avoid eliciting the De-qi sensation. On each side, the electrodes of the same EA device will be connected to the needles at Sham Point 1 and Sham Point 2. The device will be turned on to provide a brief sensation of stimulation for 30 seconds and then immediately turned off, while the device continues to appear operational (eg, flashing lights). This procedure is designed to mimic the initial sensation and visual cues of the verum EA treatment.
Treatment Regimen
The treatment frequency and duration will be identical to that of the verum EA group (twice a week for four weeks, 30-minute sessions).
Adherence Strategy
To promote participant adherence, our research staff will schedule treatment sessions at times convenient for the participants. Furthermore, appointment reminders will be provided via telephone call or text message 24 hours prior to each scheduled session. The importance of completing the full course of eight treatment sessions for the validity of the study results will be thoroughly explained during the informed consent process and reinforced by the treating acupuncturist throughout the study period.
Ethical Considerations for the Control Group
As stipulated in our institutional Ethics Committee-approved protocol, after the completion of the entire study, including the follow-up period, participants allocated to the sham EA group will be offered a full course of verum EA treatment, identical to that received by the intervention group, free of charge. This provision is a key ethical consideration to ensure fairness and that all participants have the opportunity to receive the potentially beneficial active intervention. During the trial, participants must refrain from all analgesic medications and other acupoint stimulation therapies. In instances of severe, unbearable pain, a designated rescue medication may be used, and its usage must be documented. Stable, ongoing treatments for other medical conditions are permitted. All deviations concerning concomitant treatments will be recorded but will not lead to participant withdrawal.
Outcome Measurement
At enrollment, baseline demographic and clinical characteristics of the participants will be recorded. These include age, gender, occupation, educational level, and the duration of disease.
Primary Outcome Measures
Clinical Efficacy Rate (Based on JOA Score)
The primary outcome is the clinical efficacy rate, calculated from the improvement in the JOA score. The efficacy rate will be calculated using the following formula:

Treatment Efficacy Will Be Categorized Based on the Rate
Cure (>75%), Markedly Effective (50% to ≤75%), Effective (25% to ≤50%), and Ineffective (<25%).
The JOA score assesses the functional status of the lumbar spine across several domains, including pain, lumbar function, gait, social function, and psychological well-being.29 The total score ranges from 0 to 29, with higher scores indicating better functional status.
Secondary Outcome Measures
Oswestry Disability Index (ODI)
The ODI will be used to evaluate the degree to which the patient’s functional ability is limited by their low back pain.30 This 10-item questionnaire assesses daily activities, yielding a total score ranging from 0 to 50, with higher scores indicating a greater level of disability.
Visual Analogue Scale (VAS)
The VAS will be used to measure the intensity of pain.31 The scale is a 10-cm horizontal line anchored by “no pain” (score of 0) and “the worst imaginable pain” (score of 10). Patients mark a point on the line that corresponds to their current pain level.
Neurophysiological Measures
EEG-derived metrics will serve as objective neurophysiological outcomes. Analyses will include, but are not limited to, power spectral density (PSD) analysis, time-frequency analysis, and microstate analysis.
Safety Assessment and Adverse Event Reporting
Participant safety is the highest priority and will be monitored throughout the trial. An Adverse Event (AE) is defined as any untoward medical occurrence in a participant administered the intervention, which does not necessarily have a causal relationship with the treatment. A Serious Adverse Event (SAE) is defined as any AE that results in death, is life-threatening, requires inpatient hospitalization or prolongation of existing hospitalization, or results in persistent or significant disability/incapacity.
AE Documentation, Grading, and Causality Assessment: All AEs, whether observed by the investigator or reported by the participant, will be documented in the Case Report Form (CRF). The documentation will include a description of the event, date of onset and resolution, severity, causality, and action taken.
Severity will be graded using a standard 3-point scale: Grade 1 (Mild), symptoms are easily tolerated; Grade 2 (Moderate), discomfort interferes with usual activities; Grade 3 (Severe), symptoms are incapacitating and prevent the performance of usual activities.
Causality in relation to the intervention will be assessed by the investigator as: Unrelated, Unlikely, Possible, Probable, or Definite.
Reporting Timelines
All AEs will be recorded in the CRF within 48 hours of the study team becoming aware of them. All SAEs, regardless of causality, must be reported by the site investigator to the Principal Investigator (PI) and the Institutional Ethics Committee (IEC) within 24 hours of awareness. The PI is responsible for reporting SAEs to the relevant regulatory authorities as required.
Finally, the incidence, severity, and causality of all AEs and SAEs will be summarized and compared between the treatment and sham groups at the end of the trial.
Data Collection and Quality Control
To ensure the reliability and validity of the clinical data, the following standardized procedures will be implemented:
Blinded Assessors
All clinical assessments will be administered by a trained third-party researcher who is blinded to the study hypotheses and group allocations.
Standardized Environment
Participants will complete the questionnaires independently in a neutral, quiet setting to minimize distractions.
Non-Directive Guidance
The administrator will only provide clarification on questionnaire items when explicitly asked and will refrain from guiding or influencing participant responses.
Blinded Data Handling
Completed questionnaires will be immediately collected by a separate, blinded data analyst for independent data entry and processing. All assessors will receive comprehensive training on the use of each scale before the trial commences.
Data Management and Confidentiality
A systematic data management plan will be implemented to ensure data integrity and protect participant confidentiality in accordance with the ethical principles of the Declaration of Helsinki.
Confidentiality and De-Identification
Upon enrollment, each participant will be assigned a unique, non-identifying alphanumeric code. All research data, including Case Report Forms (CRFs), questionnaires, and raw EEG files, will be labeled solely with this code. A master list linking these codes to participants’ personal identifying information (eg, name, contact details, informed consent forms) will be encrypted and stored separately from the research dataset on a secure server. Access to this linkage file will be restricted to the Principal Investigator and the designated trial coordinator.
Data Storage and Security
All physical documents containing personal information will be stored in locked filing cabinets within a secure, access-controlled office at the First Teaching Hospital of Tianjin University of Traditional Chinese Medicine. All digital data, including the de-identified research database and EEG files, will be stored on a password-protected, encrypted central server maintained by the hospital’s IT department. Access to the server is restricted to authorized research personnel via two-factor authentication.
Data Backup and Integrity
To prevent data loss, the central server will undergo automated daily incremental backups and full weekly backups. A copy of the weekly full backup will be securely transferred and stored on a separate, encrypted off-site server managed by the university. Regular data quality checks will be performed by the data manager to ensure the accuracy and completeness of the dataset.
Observation Time Points
All patients completed JOA, ODI, and VAS assessments before treatment, 14 days after treatment, 28 days after treatment, and at the 3-month follow-up. Fifteen patients were randomly selected from the treatment group and the control group for EEG data collection before and after treatment. The study flowchart is shown in Figure 1 and Table 1.
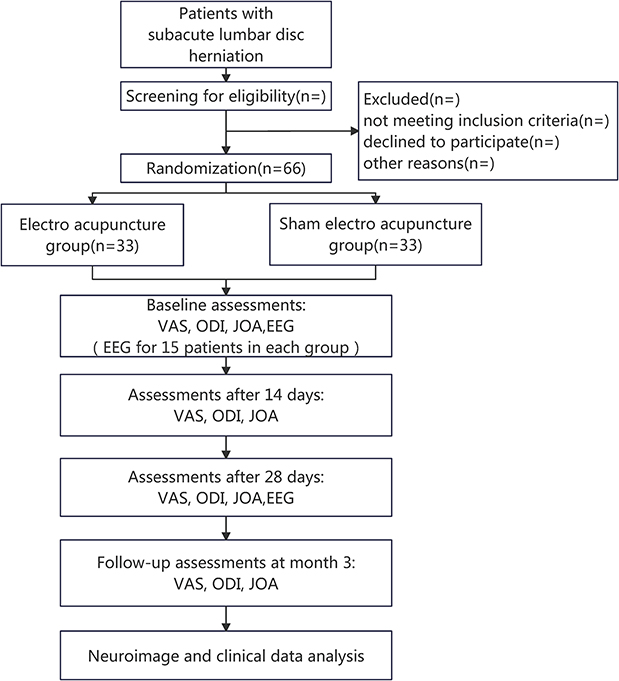 |
Figure 1 Flow chart of the trail. Abbreviations: VAS, Visual Analogue Scale; JOA, Japanese Orthopaedic Association score; ODI, Oswestry Disability Index. |
EEG Parameters
EEG data will be acquired at the First Teaching Hospital of Tianjin University of Traditional Chinese Medicine using a 64-channel EEG system (Neuracle Co., Ltd., Changzhou, China). Continuous EEG signals will be acquired using scalp electrodes arranged according to the international 10–20 system. The signals will be digitized at 1000 Hz and subjected to a hardware band-pass filter of 0.5–70 Hz. To ensure data quality, electrode impedances will be monitored and kept below 5 kΩ for the duration of the recording session.
Prior to the recording session, participants will be allowed to rest for 10 minutes to acclimate to the experimental environment. During the acquisition, participants will be instructed to lie in a comfortable, supine position in a quiet, dimly lit, and electromagnetically shielded room. They will be asked to keep their eyes closed, remain in a relaxed but wakeful state, and minimize any physical movements or swallowing. A continuous 10-minute segment of resting-state EEG data will be recorded for each participant.
Offline data processing and analysis will be performed using MATLAB (version R2025b; The MathWorks, Inc., Natick, MA, USA) with the EEGLAB toolbox (version 2025.0.0; Swartz Center for Computational Neuroscience, La Jolla, CA, USA). To promote transparency, data sharing, and reproducibility, all raw and derived data, along with their corresponding metadata, will be organized and structured according to the Brain Imaging Data Structure (BIDS) standard.
EEG Preprocessing
A standardized preprocessing pipeline will be applied to the raw EEG data as follows:
Initial Filtering
Data Import
Data organized according to the BIDS standard will be imported into EEGLAB using its BIDS import tools (eg, pop_importbids).
Band-Pass Filtering
A two-way, zero-phase-shift Finite Impulse Response (FIR) filter will be applied. To enhance filter stability, high-pass and low-pass filtering will be performed sequentially. A high-pass filter will be applied with a cutoff frequency of 0.5 Hz. A low-pass filter will be applied with a cutoff frequency of 45 Hz. The filter order will be automatically determined by EEGLAB’s pop_firws function, using a Hamming window, to achieve an optimal balance between effective artifact removal and the prevention of time-domain ringing artifacts.
Notch Filtering
A zero-phase FIR notch filter will be applied to remove the 50 Hz power-line noise (and its harmonics), with the rejection band precisely set to 49–51 Hz, as specified in the BIDS metadata.
Bad Data Identification and Correction
Bad Channel Detection and Interpolation
Channels will be identified as “bad” if they meet any of the following quantitative criteria: 1) Excessive Flatline: The signal remains flat for a duration exceeding 5 seconds. 2) Amplitude Abnormality: The robust z-score of the channel’s standard deviation is greater than 5. 3) Low Correlation: The maximum correlation with any other channel is less than 0.4 for more than 1% of the time windows. Identified bad channels will be repaired using spherical spline interpolation, as implemented in the eeg_interp.m function of EEGLAB.
Removal of Bad Data Segments
The Artifact Subspace Reconstruction (ASR) algorithm, implemented in the clean_rawdata plugin, will be used to identify and remove transient, high-amplitude artifacts from the continuous data.
Independent Component Analysis (ICA) for Artifact Removal
ICA Decomposition
The Adaptive Mixture Independent Component Analysis (AMICA) algorithm (or, if unavailable, the Extended Infomax algorithm via runica) will be run on the data. To improve decomposition, a temporary high-pass filter (eg, at 1.0 Hz) may be applied before running ICA. The resulting ICA weights will then be applied back to the original, more leniently filtered (0.5 Hz high-pass) dataset. The number of components will be equal to the rank of the data after bad channel removal.
Automated Component Classification
The ICLabel plugin will be used for objective and reproducible classification of the resulting independent components (ICs).
Artifactual Component Removal
An independent component (IC) will be automatically marked for rejection and subsequently removed if it meets the following quantitative, dual-threshold criteria based on the ICLabel classification: 1) The probability assigned by ICLabel to any single artifact category (Muscle, Eye, Heart, Line Noise, Channel Noise) is greater than 0.8 (80%), AND 2) the probability assigned to the “Brain” category is less than 0.1 (10%). This approach ensures that only high-confidence artifactual components are removed, minimizing the risk of rejecting components of neural origin. The number and types of components removed for each participant will be documented and reported.
Power Spectral Density (PSD) Analysis
We will estimate the Power Spectral Density (PSD) of the preprocessed EEG data by applying Welch’s periodogram method. The data will be segmented using a 2-second fixed sliding window with a 50% overlap, and a Hanning window (taper) will be applied to each segment to reduce spectral leakage. For each channel, absolute power will be calculated by integrating the PSD within five classical frequency bands: delta (δ: 0.5–4 Hz), theta (θ: 4–7 Hz), alpha (α: 8–13 Hz), beta (β: 14–28 Hz), and gamma (γ: 30–45 Hz). Relative power for each band was subsequently calculated by normalizing its absolute power to the total power across the entire 0.5–45 Hz spectrum. For statistical analysis, the relative power values will be log10-transformed to better approximate a normal distribution.
Time-Frequency Analysis
The Short-Time Fourier Transform (STFT) will be employed to analyze the time-varying spectral characteristics of the EEG signal. Using a 2-second fixed sliding window, the STFT will compute the spectral distribution within each time segment, yielding a time-frequency representation of the signal. Time-frequency features from specific frequency bands will be extracted to characterize dynamic brain activity and event-related spectral perturbations.
Microstate Analysis
Data Preparation and Microstate Segmentation
The preprocessed EEG data will first be band-pass filtered between 2 and 20 Hz and re-referenced to the whole-brain average reference. The Global Field Power (GFP) will be computed for the continuous data. Topographic maps corresponding to the peaks of the GFP curve, representing moments of maximal signal-to-noise ratio, will be extracted. These maps will then be submitted to a K-means clustering algorithm to identify a set of archetypal microstate templates at the group level. The optimal number of microstates will be determined using established criteria (eg, Cross-validation criterion, Krzanowski-Lai criterion).
Back-Fitting and Parameter Calculation
The optimal group-level microstate maps will be fitted back to the continuous EEG data of each individual participant. At each time point, the data will be labeled with the microstate map with which it shares the highest spatial correlation. From this resulting sequence of microstate labels, the following temporal parameters will be calculated for each microstate class and each participant: 1) Mean Duration: The average time a microstate remains stable before transitioning. 2) Occurrence per Second: The average number of times a microstate appears per second. 3) Coverage: The fraction of total recording time that a given microstate is active. 4) Transition Probabilities: A transition matrix will be computed for each participant, quantifying the probability of transitioning from any given microstate to any other.
Statistical Analysis
Differences in microstate temporal parameters (Duration, Occurrence, Coverage) and transition probabilities between clinical groups will be assessed using independent samples t-tests (for two-group comparisons) or one-way Analysis of Variance (ANOVA) (for comparisons of more than two groups), with “group” as the between-subject factor. Post-hoc tests will be corrected for multiple comparisons using the Bonferroni correction method, given the relatively small number of pre-defined comparisons.
Sample Size Estimation
The sample size calculation was performed for the primary clinical outcome. As there are no prior RCTs directly comparing verum EA with sham EA for the treatment of subacute LDH, our estimation is based on the efficacy rates reported in previous studies on LDH. These studies reported an efficacy rate of 90.62% for a verum EA group32 and 51.72% for a placebo control group.33 The sample size was calculated using the formula for comparing two proportions, with a two-sided significance level (α) of 0.05 and a statistical power (1-β) of 90%. The formula used is:

Based on this calculation, a minimum of 29 participants per group is required. Allowing for a potential attrition rate of 10%, a total of 66 participants (33 per group) will be recruited to ensure an adequate final sample size for analysis. For the EEG sub-study, there is currently no universally accepted method for a priori sample size calculation for neurophysiological outcomes. Therefore, guided by common practices in the field of clinical neuroscience, which suggest that sample sizes of 12–15 participants per group can yield stable and statistically meaningful results, we plan to recruit a subset of 15 participants from each group (for a total of 30) for EEG analysis.
Randomization and Allocation Concealment
A simple randomization sequence will be generated by an independent statistician who is not involved in patient recruitment or assessment. This sequence will be created using SPSS software (version 21.0) to ensure an overall 1:1 allocation ratio between the EA and sham EA groups.
To guarantee allocation concealment, the same independent statistician will oversee the preparation of allocation materials. The group assignments (“EA Group” or “Sham EA Group”) will be printed on cards. Each card will be folded and placed inside an opaque, sealed envelope along with an opaque piece of cardboard to prevent transillumination. The exterior of the envelopes will be sequentially numbered from 1 to 66. These prepared envelopes will be stored in a locked, secure cabinet in the office of the principal investigator, accessible only to the designated recruiting researcher at the time of allocation. After a participant provides written informed consent and is confirmed to meet all eligibility criteria, the recruiting researcher will retrieve the next consecutively numbered envelope in the sequence to determine the participant’s group assignment.
Blinding
Throughout the trial, participants, outcome assessors, and data statisticians will remain blinded to group allocation. Due to the nature of the intervention, the acupuncturist responsible for administering the treatments cannot be blinded. To minimize the risk of performance bias, the acupuncturist will be instructed to maintain a neutral attitude towards both interventions and will have no contact with the outcome assessors or be involved in any part of the data collection or analysis.
Although blinding the practitioner is not possible, the integrity of the trial is protected by using a robust randomization sequence, ensuring allocation concealment with sealed envelopes, and maintaining the blinding of all participants, assessors, and analysts. This design minimizes the risk of selection, detection, and performance bias, thereby ensuring the scientific rigor of the trial results.
Statistical Analysis
All statistical analyses will be performed using SPSS software (v. 26.0; IBM Corp., Armonk, NY, USA) following initial data management in Microsoft Excel. A two-sided p-value < 0.05 will be considered statistically significant for all tests. To minimize analytical bias, these analyses will be conducted by an independent statistician blinded to the group allocations.
Descriptive Statistics
Baseline demographic and clinical characteristics of the participants will be summarized using descriptive statistics. Continuous variables will be expressed as mean ± standard deviation (SD) or median (interquartile range, IQR), contingent upon the data distribution as determined by the Shapiro–Wilk test. Categorical variables will be reported as counts and percentages (%).
Analysis of Efficacy
The analysis of treatment efficacy will adhere to the principle of Intent-to-Treat (ITT). Both the Full Analysis Set (FAS), which includes all randomized participants who received at least one treatment session, and the Per-Protocol (PP) set, which includes participants who completed the trial without major protocol deviations, will be used for a comprehensive comparative analysis.
For continuous outcomes with repeated measurements (eg, JOA, ODI, VAS scores), we will employ linear mixed-effects models (LMM) or Generalized Estimating Equations (GEE) to analyze inter-group differences over time. These models will be used to assess the main effects of group and time, as well as the primary outcome of interest: the group-by-time interaction effect. GEE will be prioritized for its robustness in handling various correlation structures and missing data, while repeated measures ANOVA may be considered for complete datasets that satisfy its underlying assumptions (eg, sphericity).
For categorical outcomes, group differences will be assessed using the Pearson’s Chi-square (χ2) test, or Fisher’s exact test if any expected cell count is less than 5.
Comparisons of ordinal data or non-normally distributed continuous data between the two groups will be performed using the non-parametric Mann–Whitney U-test.
Correlation Analysis
To test the core hypothesis that clinical improvements are associated with central neuromodulation, we will investigate the relationship between the change from baseline to the 4-week endpoint in clinical outcomes and EEG parameters. Change scores will be calculated for all relevant variables.
The analysis will proceed in two stages. First, as an initial exploratory step, we will use bivariate correlations to assess the direct relationship between changes in clinical and EEG measures. Pearson’s correlation coefficient will be used for normally distributed data, while Spearman’s rank correlation will be used for non-normally distributed data.
Second, to conduct a more robust test of the relationship while accounting for potential confounding variables, our primary analysis will employ multiple linear regression models. For each model, the change in a primary clinical outcome will serve as the dependent variable, and the change in a key EEG metric will be the primary independent variable of interest. We will include age, disease duration, and the baseline score of the clinical outcome as covariates in the model. This approach will allow us to rigorously assess the unique contribution of neuromodulatory changes to therapeutic efficacy after controlling for these important factors.
Handling of Missing Data
Our statistical analysis will follow the Intent-to-Treat (ITT) principle, including all randomized participants in the final analysis. We have developed distinct strategies for handling missing data for our clinical and neurophysiological outcomes.
- For Clinical Outcomes (JOA, ODI, VAS): For the repeated measurements of clinical outcomes, our primary analytical method will be the use of Linear Mixed-Effects Models (LMM) or Generalized Estimating Equations (GEE). These modern statistical approaches are robust for handling data that are Missing At Random (MAR). They utilize all available data points from each participant over the multiple time points (baseline, 2 weeks, 4 weeks, and 3-month follow-up), which is superior to older methods like Last Observation Carried Forward (LOCF) that can introduce significant bias. This approach allows us to include participants who may have dropped out before the study’s completion in the analysis, thereby upholding the ITT principle.
- For EEG Outcomes: The EEG sub-study involves a pre-post comparison (baseline vs 4 weeks). Therefore, the primary analysis will necessarily be conducted on the set of participants who provide complete EEG data at both time points. To investigate potential attrition bias in this subset, we will perform the following steps:
- We will compare the baseline demographic and clinical characteristics (eg, age, gender, VAS, ODI, JOA scores) of participants who complete the EEG sub-study with those who drop out.
- Any significant differences between these groups will be noted, and the potential impact of this attrition bias on the interpretation of the EEG results will be thoroughly discussed in the final manuscript.
- If the rate of missing EEG data is substantial (eg, >10%), we will perform a sensitivity analysis using multiple imputation techniques to assess the robustness and stability of our findings.
Discussion
This study was designed as a randomized, sham-controlled trial to provide the first investigation into the central neuromodulatory mechanisms of EA for patients in the subacute stage of LDH, utilizing multidimensional EEG techniques. We anticipate that this research will not only furnish high-level, evidence-based support for the clinical application of EA but, more crucially, will uncover objective neurobiological markers underlying its therapeutic effects. Our core hypothesis is that the clinical improvements conferred by EA will be significantly correlated with the normalization of specific resting-state neural oscillatory patterns and the functional reorganization of large-scale brain networks, collectively reflecting an effective reversal of the central sensitization state associated with chronic pain. It is important to acknowledge that our central hypothesis—that EA will normalize aberrant neural oscillations in subacute LDH—is predicated on an extrapolation from findings in established chronic pain populations. Our framework assumes that the subacute stage represents a critical transitional period where the early electrophysiological signatures of central sensitization, such as the excess theta power characteristic of chronic pain, have already begun to manifest. This is a foundational, yet untested, assumption. Therefore, a key secondary objective of this trial is to test this premise directly through our baseline EEG analysis. Comparing the baseline oscillatory patterns of our subacute cohort against established normative data will be a crucial first step in contextualizing any treatment-induced neuroplastic changes. It is also critical to consider the interpretation of potential negative findings. If our primary hypothesis is not supported—that is, if significant clinical improvements in the verum EA group do not correlate with the hypothesized normalization of theta and alpha oscillations—several alternative hypotheses would warrant consideration. First, there may be a temporal mismatch; the four-week endpoint for the EEG assessment might be too early to capture the full extent of cortical reorganization, which may require a longer period of consolidation. A null finding would suggest that future studies should incorporate longer-term neuroimaging follow-ups. Second, our a priori focus on specific frequency bands, while theory-driven, may be incomplete. A lack of correlation could indicate that other neurophysiological parameters, such as activity in the gamma band (often linked to higher-order pain perception and cognition) or changes in cross-frequency coupling, are more sensitive markers of EA’s central effects. Finally, a null correlation at the cortical level would not negate the treatment’s efficacy but would suggest that the primary therapeutic mechanisms in the subacute stage may be more strongly rooted in peripheral or spinal-level modulation (eg, sustained anti-inflammatory effects or regulation of spinal glial cell activity) rather than large-scale cortical plasticity detectable by scalp EEG. Such a result would underscore the necessity for a multi-level mechanistic investigation in future research.
The primary innovation of this study is twofold. Clinically, we are the first to focus on the critical “subacute” phase, a transitional window from acute to chronic pain where effective intervention is paramount for preventing recurrence. Mechanistically, we are the first to employ high-temporal-resolution EEG to systematically elucidate the dynamic cerebral processes through which EA exerts its effects over a full course of treatment. Although a substantial body of literature has investigated the analgesic mechanisms of acupuncture, this research suffers from two notable limitations: a heavy reliance on functional magnetic resonance imaging (fMRI) and a primary focus on the acute effects of a single intervention. By implementing a rigorous sham-controlled design and observing effects over an extended treatment period, this study aims to fill a significant gap in our understanding of the central mechanisms driving the long-term efficacy of EA, thereby providing direct evidence to advance the scientific rigor and clinical precision of acupuncture research.
The subacute stage of LDH represents a long-neglected yet pivotal window for research. We posit that during this phase, the brain may exist in a “metastable” pathological state. Although the intense pain symptoms have subsided, the cortical excitation/inhibition imbalances and network connectivity abnormalities caused by the preceding nociceptive barrage likely persist. This latent dysregulation represents a state of neurobiological vulnerability and may constitute the neural foundation for pain recurrence and the eventual transition into intractable chronic pain. Indeed, a landmark study has demonstrated that the functional connectivity patterns between the cerebral cortex and the striatum can predict the chronification of acute back pain.34 Therefore, by intervening and observing during this specific period, our study aims to capture whether EA can clear these residual pathological signatures, thereby interrupting the chronification process at its root. This focus endows our research with a unique significance in the context of preventive medicine.
The processing of pain involves a complex brain network encompassing regions such as the thalamus, insula, somatosensory cortices (S1/S2), anterior cingulate cortex (ACC), and prefrontal cortex (PFC).35 With its excellent spatial resolution, fMRI has made immense contributions to localizing structural and functional abnormalities in these pain-related regions.36,37 For instance, studies have found altered network centrality in nodes like the inferior frontal gyrus and insula in LDH patients, changes that correlate with the clinical Oswestry Disability Index.38 However, fMRI relies on the blood-oxygen-level-dependent (BOLD) signal, which has a sluggish temporal response on the scale of seconds. This limits its ability to capture the brain’s rapid, transient activities. Pain perception and neuromodulation via EA are, in essence, dynamic processes that unfold on a millisecond scale. While fMRI excels at revealing the “static” spatial map of pain-related networks, it is limited in its capacity to delineate their “dynamic” activity. EEG, by directly measuring the synchronous firing of neuronal populations with millisecond temporal resolution, is the ideal tool for capturing these rapid state transitions. Our choice of EEG is therefore deliberate: to infuse the “spatial map” provided by fMRI with critical “temporal information”, viewed through the lens of neural oscillations and whole-brain network dynamics.
Chronic pain is increasingly understood as a state of cortical hyperexcitability or thalamocortical dysrhythmia. Previous research has clearly shown that, compared to healthy controls, chronic pain patients exhibit specific power spectrum abnormalities in frontal and parietal regions, particularly an excess of activity in the high theta (6–9 Hz) and low beta (12–16 Hz) frequency ranges.39,40 This overabundance of theta-band activity is considered a hallmark of thalamocortical dysrhythmia, reflecting persistent aberrant input from sensory pathways.41 We anticipate that after a full course of effective EA treatment, patients’ resting-state theta power will be significantly reduced, signifying a correction of this pathological cortical rhythm.
Alpha-band activity, conversely, is closely associated with cortical inhibition, functional calmness, and attentional disengagement.42 One prior study found that alpha power in LDH patients increased significantly during resting-state immediately following a single session of acupotomy, though its long-term effects remain unknown.43 We hypothesize that after a complete regimen of EA, alpha-band activity will be sustainably enhanced. This would not only reflect a reduction in pain intensity but could also represent the brain’s liberation from a state of sustained, obligatory attention to pain, thereby freeing up cognitive resources.
We further propose that the changes in specific frequency bands will manifest as a macroscopic reorganization of whole-brain network patterns. Microstate analysis is a powerful tool for capturing such global changes, and its distinct “topographic snapshots” have been shown to correlate strongly with resting-state networks (RSNs) identified by fMRI.44 Previous research has found that, compared to healthy individuals, chronic pain patients exhibit a significant reduction in the duration and coverage of Microstate D.45 As Microstate D is typically associated with the fronto-parietal attention and executive control networks, its diminished activity may reflect the persistent cognitive interference caused by chronic pain. We expect that after EA treatment, the parameters associated with Microstate D will normalize towards healthy levels.
More importantly, we speculate that Microstate C, which is functionally associated with the Salience Network, will play a pivotal role in this study. The Salience Network is responsible for detecting and processing salient internal and external stimuli and is thought to be persistently “hijacked” by nociceptive signals in chronic pain, leading to a state of hypervigilance.11,46 We hypothesize that pre-treatment, patients will exhibit abnormally elevated activity of Microstate C. A core central mechanism of EA, we propose, will be the downregulation of this Salience Network over-activation (ie, reducing the activity of Microstate C), thereby breaking the vicious cycle of pain.47,48 This network-level reorganization may be the fundamental reason why EA can provide long-lasting therapeutic benefits.
The primary strength of this study lies in its theory-driven, innovative design: it is the first to focus on the clinically critical “subacute” stage; it employs a rigorous randomized, sham-controlled methodology; and it applies a multidimensional EEG analysis strategy to systematically elucidate the central mechanisms of EA from multiple perspectives. If successful, our findings may provide objective, neuroimaging-based biomarkers to help identify patients in this critical subacute stage who are most likely to benefit from this intervention, thereby advancing the practice of “precision acupuncture”.
However, we also recognize its limitations. First, as an exploratory, single-center trial, the sample size may not be sufficiently powered to detect EEG changes with smaller effect sizes or to conduct meaningful subgroup analyses (eg, based on disease duration). Our results will require validation in larger, multicenter studies before they can be generalized. Second, perfect double-blinding is inherently challenging in acupuncture research. Nevertheless, the sham EA protocol we have adopted is a widely accepted control method designed to minimize placebo effects and maintain patient blinding to the greatest extent possible.
Future research should aim to validate the findings of this study in larger, multicenter trials. Furthermore, the simultaneous acquisition of EEG and fMRI data represents an ideal direction for future mechanistic studies, as it would synergistically combine the temporal resolution of EEG with the spatial precision of fMRI to map the spatiotemporal dynamics of pain modulation by EA with unparalleled detail.49 Finally, should this study successfully identify robust neurophysiological biomarkers, future work could explore their utility in predicting treatment response in LDH patients at different stages or with varying pain severities. This could pave the way for screening patients based on their baseline EEG characteristics to identify those most likely to benefit from EA, thus taking a firm step towards the realization of “precision acupuncture”.
Trial Status
Protocol: version 1.0, 15 January 2025.
Date opened to recruitment: 6 May 2025.
Recruitment closure: 31 December 2025.
Data Sharing Statement
Data collected during the study can be obtained from the corresponding author upon request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by Graduate Research Innovation Project of TUTCM (YJSKC-20240049) and Innovation team for Research on Dominant Diseases of Acupuncture and Moxibustion (No. 4042502034). The funding sources had no role in the study design; in the collection, analysis, and interpretation of data; or in the writing of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang AS, Xu A, Ansari K, et al. Lumbar disc herniation: diagnosis and management. Am J Med. 2023;136(7):645–651. doi:10.1016/j.amjmed.2023.03.024
2. Long G, Jing L, Wenru S, et al. Non-operative treatments for lumbar disc herniation: an evidence-based practice guideline. Chin J Evidence-Based Med. 2024;24(02):125–148.
3. Pojskic M, Bisson E, Oertel J, Takami T, Zygourakis C, Costa F. Lumbar disc herniation: epidemiology, clinical and radiologic diagnosis WFNS spine committee recommendations. World Neurosurg X. 2024;22:100279. doi:10.1016/j.wnsx.2024.100279
4. Bally M, Dendukuri N, Rich B, et al. Risk of acute myocardial infarction with NSAIDs in real world use: bayesian meta-analysis of individual patient data. BMJ. 2017;357:j1909. doi:10.1136/bmj.j1909
5. Trelle S, Reichenbach S, Wandel S, et al. Cardiovascular safety of non-steroidal anti-inflammatory drugs: network meta-analysis. BMJ. 2011;342:c7086. doi:10.1136/bmj.c7086
6. Jacobs WC, van Tulder M, Arts M, et al. Surgery versus conservative management of sciatica due to a lumbar herniated disc: a systematic review. Eur Spine J. 2011;20(4):513–522. doi:10.1007/s00586-010-1603-7
7. Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical versus nonoperative treatment for lumbar disc herniation: four-year results for the Spine Patient Outcomes Research Trial (SPORT). Spine. 2008;33(25):2789–2800. doi:10.1097/BRS.0b013e31818ed8f4
8. Peul WC, van Houwelingen HC, van den Hout WB, et al. Surgery versus prolonged conservative treatment for sciatica. N Engl J Med. 2007;356(22):2245–2256. doi:10.1056/NEJMoa064039
9. Apkarian AV, Baliki MN, Geha PY. Towards a theory of chronic pain. Prog Neurobiol. 2009;87(2):81–97. doi:10.1016/j.pneurobio.2008.09.018
10. Latremoliere A, Woolf CJ. Central sensitization: a generator of pain hypersensitivity by central neural plasticity. J Pain. 2009;10(9):895–926. doi:10.1016/j.jpain.2009.06.012
11. Kucyi A, Davis KD. The dynamic pain connectome. Trends Neurosci. 2015;38(2):86–95. doi:10.1016/j.tins.2014.11.006
12. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/aln.0000000000000101
13. Zhao ZQ. Neural mechanism underlying acupuncture analgesia. Prog Neurobiol. 2008;85(4):355–375. doi:10.1016/j.pneurobio.2008.05.004
14. Yang JX, Zhu J, Ni K, Yang HK, Zhang HL, Ma ZL. Electroacupuncture relieves chronic pain by promoting microglia M2 polarization in lumbar disc herniation rats. Neuroreport. 2023;34(12):638–648. doi:10.1097/wnr.0000000000001935
15. Hu R, Xu Z, Dang M, et al. Comprehensive electroacupuncture treatments reduce serum inflammatory factors and relieve pain symptoms in patients with lumbar disc herniation: a systematic review and network meta-analysis. Int J Surg. 2025;111(1):1526–1530. doi:10.1097/js9.0000000000001979
16. Fox MD, Raichle ME. Spontaneous fluctuations in brain activity observed with functional magnetic resonance imaging. Nat Rev Neurosci. 2007;8(9):700–711. doi:10.1038/nrn2201
17. Sorger B, Goebel R. Real-time fMRI for brain-computer interfacing. Handb Clin Neurol. 2020;168:289–302. doi:10.1016/b978-0-444-63934-9.00021-4
18. Barud M, Dabrowski W, Siwicka-Gieroba D, Robba C, Bielacz M, Badenes R. Usefulness of Cerebral Oximetry in TBI by NIRS. J Clin Med. 2021;10(13):2938. doi:10.3390/jcm10132938
19. Purdon PL, Sampson A, Pavone KJ, Brown EN. Clinical electroencephalography for anesthesiologists: Part I: background and basic signatures. Anesthesiology. 2015;123(4):937–960. doi:10.1097/aln.0000000000000841
20. Sun G, Wen Z, Ok D, Doan L, Wang J, Chen ZS. Detecting acute pain signals from human EEG. J Neurosci Methods. 2021;347:108964. doi:10.1016/j.jneumeth.2020.108964
21. Tracey I, Mantyh PW. The cerebral signature for pain perception and its modulation. Neuron. 2007;55(3):377–391. doi:10.1016/j.neuron.2007.07.012
22. Ploner M, Sorg C, Gross J. Brain rhythms of pain. Trends Cognit Sci. 2017;21(2):100–110. doi:10.1016/j.tics.2016.12.001
23. Hsu HH, Yang YR, Chou LW, Huang YC, Wang RY. The brain waves during reaching tasks in people with subacute low back pain: a cross-sectional study. IEEE Trans Neural Syst Rehabil Eng. 2024. doi:10.1109/tnsre.2024.3521286
24. Lv Y, Dai DC, Jiang HN, Shen XM, Lu JC. Effect of electroacupuncture on the multifidus muscle in patients with lumbar disc herniation. Zhongguo Zhen Jiu. 2022;42(10):1103–1107. doi:10.13703/j.0255-2930.20220215-k0006
25. Chan AW, Tetzlaff JM, Gøtzsche PC, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346:e7586. doi:10.1136/bmj.e7586
26. MacPherson H, Altman DG, Hammerschlag R, et al. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): extending the CONSORT statement. PLoS Med. 2010;7(6):e1000261. doi:10.1371/journal.pmed.1000261
27. Hershman DL, Unger JM, Greenlee H, et al. Effect of acupuncture vs sham acupuncture or waitlist control on joint pain related to aromatase inhibitors among women with early-stage breast cancer: a randomized clinical trial. JAMA. 2018;320(2):167–176. doi:10.1001/jama.2018.8907
28. Witt C, Brinkhaus B, Jena S, et al. Acupuncture in patients with osteoarthritis of the knee: a randomised trial. Lancet. 2005;366(9480):136–143.
29. Haro H, Ebata S, Inoue G, et al. Japanese Orthopaedic Association (JOA) clinical practice guidelines on the management of lumbar disc herniation, third edition - secondary publication. J Orthop Sci. 2022;27(1):31–78. doi:10.1016/j.jos.2021.07.028
30. Fairbank JC, Pynsent PB. The oswestry disability index. Spine. 2000;25(22):
31. Lee JS, Hobden E, Stiell IG, Wells GA. Clinically important change in the visual analog scale after adequate pain control. Acad Emerg Med. 2003;10(10):1128–1130. doi:10.1111/j.1553-2712.2003.tb00586.x
32. Zhen D, Shao P, He Y, et al. Repair of lumber interverbral disc herniation: the comparison between electro-acupuncture on Huatuo Jiaji points and slow-released diclofenac sodium tablets. Liaoning J Tradit Chin Med. 2009;36(09):1566–1569. doi:10.13192/j.ljtcm.2009.09.130.duzh.057
33. Lu L, Zhou J, Liu Y, et al. Clinical effects of crude herb moxibustion on treating low back pain of lumbar disc herniation. Chin Gen Pract. 2017;20(04):
34. Baliki MN, Petre B, Torbey S, et al. Corticostriatal functional connectivity predicts transition to chronic back pain. Nat Neurosci. 2012;15(8):1117–1119. doi:10.1038/nn.3153
35. Garcia-Larrea L, Peyron R. Pain matrices and neuropathic pain matrices: a review. Pain. 2013;154(Suppl 1):S29–s43. doi:10.1016/j.pain.2013.09.001
36. Morton DL, Sandhu JS, Jones AK. Brain imaging of pain: state of the art. J Pain Res. 2016;9:613–624. doi:10.2147/jpr.S60433
37. Apkarian AV, Bushnell MC, Treede RD, Zubieta JK. Human brain mechanisms of pain perception and regulation in health and disease. Eur J Pain. 2005;9(4):463–484. doi:10.1016/j.ejpain.2004.11.001
38. Zhang YP, Hong GH, Zhang CY. Brain network changes in lumbar disc herniation induced chronic nerve roots compression syndromes. Neural Plast. 2022;2022:7912410. doi:10.1155/2022/7912410
39. Pinheiro ES, de Queirós FC, Montoya P, et al. Electroencephalographic patterns in chronic pain: a systematic review of the literature. PLoS One. 2016;11(2):e0149085. doi:10.1371/journal.pone.0149085
40. Stern J, Jeanmonod D, Sarnthein J. Persistent EEG overactivation in the cortical pain matrix of neurogenic pain patients. Neuroimage. 2006;31(2):721–731. doi:10.1016/j.neuroimage.2005.12.042
41. Llinás RR, Ribary U, Jeanmonod D, Kronberg E, Mitra PP. Thalamocortical dysrhythmia: a neurological and neuropsychiatric syndrome characterized by magnetoencephalography. Proc Natl Acad Sci U S A. 1999;96(26):15222–15227. doi:10.1073/pnas.96.26.15222
42. Jensen O, Mazaheri A. Shaping functional architecture by oscillatory alpha activity: gating by inhibition. Front Hum Neurosci. 2010;4:186. doi:10.3389/fnhum.2010.00186
43. Li R, Shao W, Zhao S, et al. EEG alpha/beta features as a biomarker for quantifying pain in patients with lumbar disk herniation. Front Neurosci. 2025;19:1507245. doi:10.3389/fnins.2025.1507245
44. Michel CM, Koenig T. EEG microstates as a tool for studying the temporal dynamics of whole-brain neuronal networks: a review. Neuroimage. 2018;180(Pt B):577–593. doi:10.1016/j.neuroimage.2017.11.062
45. May ES, Gil Ávila C, Ta Dinh S, et al. Dynamics of brain function in patients with chronic pain assessed by microstate analysis of resting-state electroencephalography. Pain. 2021;162(12):2894–2908. doi:10.1097/j.pain.0000000000002281
46. Seeley WW, Menon V, Schatzberg AF, et al. Dissociable intrinsic connectivity networks for salience processing and executive control. J Neurosci. 2007;27(9):2349–2356. doi:10.1523/jneurosci.5587-06.2007
47. Li SS, Xing XX, Hua XY, et al. Alteration of brain functional networks induced by electroacupuncture stimulation in rats with ischemia-reperfusion: an independent component analysis. Front Neurosci. 2022;16:958804. doi:10.3389/fnins.2022.958804
48. Shen Z, Zhang H, Wu Z, et al. Electroacupuncture alleviates chronic pain-induced anxiety disorders by regulating the rACC-Thalamus circuitry. Front Neurosci. 2020;14:615395. doi:10.3389/fnins.2020.615395
49. Jorge J, van der Zwaag W, Figueiredo P. EEG-fMRI integration for the study of human brain function. Neuroimage. 2014;102(Pt 1):24–34. doi:10.1016/j.neuroimage.2013.05.114
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.