Back to Journals » Journal of Pain Research » Volume 15
Electro-Acupuncture for Bladder Pain Syndrome: A Protocol of a Randomized Controlled Trial and Study for Central Mechanism
Authors Xu Y ![]() , Chen Y
, Chen Y ![]() , Shi Y, Lu J, Wu Z, Liu Z, Chen Y
, Shi Y, Lu J, Wu Z, Liu Z, Chen Y ![]() , Ni W, Ding Q, Dai W, Wu X, Fang J, Wu Y
, Ni W, Ding Q, Dai W, Wu X, Fang J, Wu Y ![]()
Received 14 April 2022
Accepted for publication 29 June 2022
Published 13 July 2022 Volume 2022:15 Pages 1959—1970
DOI https://doi.org/10.2147/JPR.S370751
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Yunyun Xu,1,* Yangyun Chen,1,* Yan Shi,2 Jianhua Lu,3 Zonglin Wu,1 Zhe Liu,1 Yuerong Chen,1 Wenqin Ni,1 Qike Ding,4 Wei Dai,4 Xinyuan Wu,4 Jianqiao Fang,1 Yuanyuan Wu5
1The Third Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou City, Zhejiang Province, People’s Republic of China; 2Department of Acupuncture & Tuina, Hangzhou First People’s Hospital, Hang Zhou City, Zhejiang Province, People’s Republic of China; 3Department of Acupuncture & Moxibustion, Mishi Xiang Community Health Service Center, Hang Zhou City, Zhejiang Province, People’s Republic of China; 4The Second Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou City, Zhejiang Province, People’s Republic of China; 5Department of Acupuncture & Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hang Zhou City, Zhejiang Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuanyuan Wu, Email [email protected]
Objective: The efficacy of conventional treatments for treating bladder pain syndrome (BPS) remains unsatisfactory. Electro-acupuncture (EA) is one of the complementary treatments with great analgesic effect and minimal side effect, but evidence of the efficacy of EA on BPS is limited. Thus, this study aims to investigate the efficacy and safety of EA for treating BPS and study on central mechanism of patients with BPS.
Methods/Design: The study is a randomized controlled and assessor-blinded design trial. A total of 84 participants will be randomly assigned to medication group (n=21), EA group (n=42) and sham electro-acupuncture (SA) group (n=21) in a 1:2:1 allocation ratio. This trial will include baseline period, 4-week treatment period and 4-week follow-up period. Participants in medication group will undergo treatment of amitriptyline for a period of 4 weeks. Participants in EA and SA groups will receive a 30 min EA or SA treatment for a total of 12 sessions over 4 weeks. The primary outcome is the Visual Analog Scale (VAS). The secondary outcomes include the O’Leary-Sant questionnaire, 24-hour voiding diary, Hamilton Anxiety Scale (HAMA), Hamilton Depression Scale (HAMD) and functional magnetic resonance imaging (fMRI). The VAS will be collected at baseline, week 2, week 4, and week 8 after randomization. The O’Leary-Sant questionnaire, HAMA and HAMD will be assessed at baseline, week 4 and week 8 after randomization. The 24-hour voiding diary will be assessed every single day. The fMRI data will be collected at baseline and week 4.
Discussion: The results will provide evidence on the efficacy and safety of EA in the management of BPS and investigate the central mechanism of EA in treating patients with BPS.
Trial Registration: ClinicalTrials.gov identifier: NCT05279963. Registered on 15 March 2022.
Keywords: electro-acupuncture, bladder pain syndrome, randomized controlled trial, functional magnetic resonance imaging
Background
Bladder pain syndrome (BPS) is a chronic, nonbacterial cystitis characterized by persistent or recurrent pain, pressure or discomfort in the bladder region associated with lower urinary tract symptoms of more than 6 weeks duration.1 It usually occurs in middle-aged women and is characterized by fibrotic of the bladder wall accompanied by a reduction in bladder volume.2 The prevalence of BPS in previous reports ranges from 10 to 510 per 100,000.3–5 In addition, because of its delayed, refractory bladder or perineal pain, usually accompanied by frequency and urgency, BPS patients have significantly more pain, sleep dysfunction, anxiety, depression and stress.6 At present, although various treatments, such as amitriptyline, pentosan polysulfate sodium, hydroxyzine, cyclosporine A, hydroxyzine hydrochloride, tricyclic antidepressants, anticholinergics and intravesical therapy, have been used to relieve the symptoms, the efficacy of these therapies remains unsatisfactory because the therapies have either short-lived effect or long-term benefits accompanied by side effects leading to patient intolerance.5,7,8 Recently, there has been an increase in the use of complementary and alternative therapies, including electro-acupuncture (EA).9 Though multiple clinical trials have confirmed the efficacy of EA on a variety of pain conditions,10–13 studies on the use of EA for BPS are not yet widely conducted. Besides, the reliability within previous trials is still limited against methodological defects, such as small sample sizes.14,15 Meanwhile, few studies have been designed for the assessments of concomitant symptom improvement, such as psychological disorder. In general, there is no high quality evidence regarding the efficacy of EA for treating BPS. Therefore, the critical objective of this randomized controlled trial is to investigate, based on conventional treatment, the efficacy and safety of EA versus sham electro-acupuncture (SA) for treating BPS in terms of symptom management. Brain functional magnetic resonance imaging (fMRI) has revealed that the pain matrix consists mainly of the thalamus, amygdala, insular cortex, supplementary motor area, and periaqueductal gray.16–18 It also provides a new method to quantify how EA affects changes in the brain network. Thus, the another aim of this study is to investigate the central mechanism of EA in treating patients with BPS by measuring the changes in brain with fMRI.
Methods/Design
Study Design
This is a randomized controlled and assessor-blinded design trial to evaluate the efficacy and safety of EA. All eligible participants will be randomly assigned to medication group (n=21), EA group (n=42) and SA group (n=21) in a 1:2:1 allocation ratio, and receive 4-week treatments phase followed by 4-week follow-up phase. The reporting of this protocol will be reported based on the SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) reporting guidelines19 and STRICTA (Standards for Reporting Interventions in Clinical Trials of Acupuncture).20 Outcomes will be assessed at baseline, during the treatment and at the end of the follow-up. Outcome assessors, data managers and statisticians will be blinded to the group allocation, while acupuncturists and participants in medication group will not be blinded for obvious reasons. A flow diagram of the study process is shown in Figure 1 and the trial schedule of enrolment, treatments and assessments is showed in Table 1.
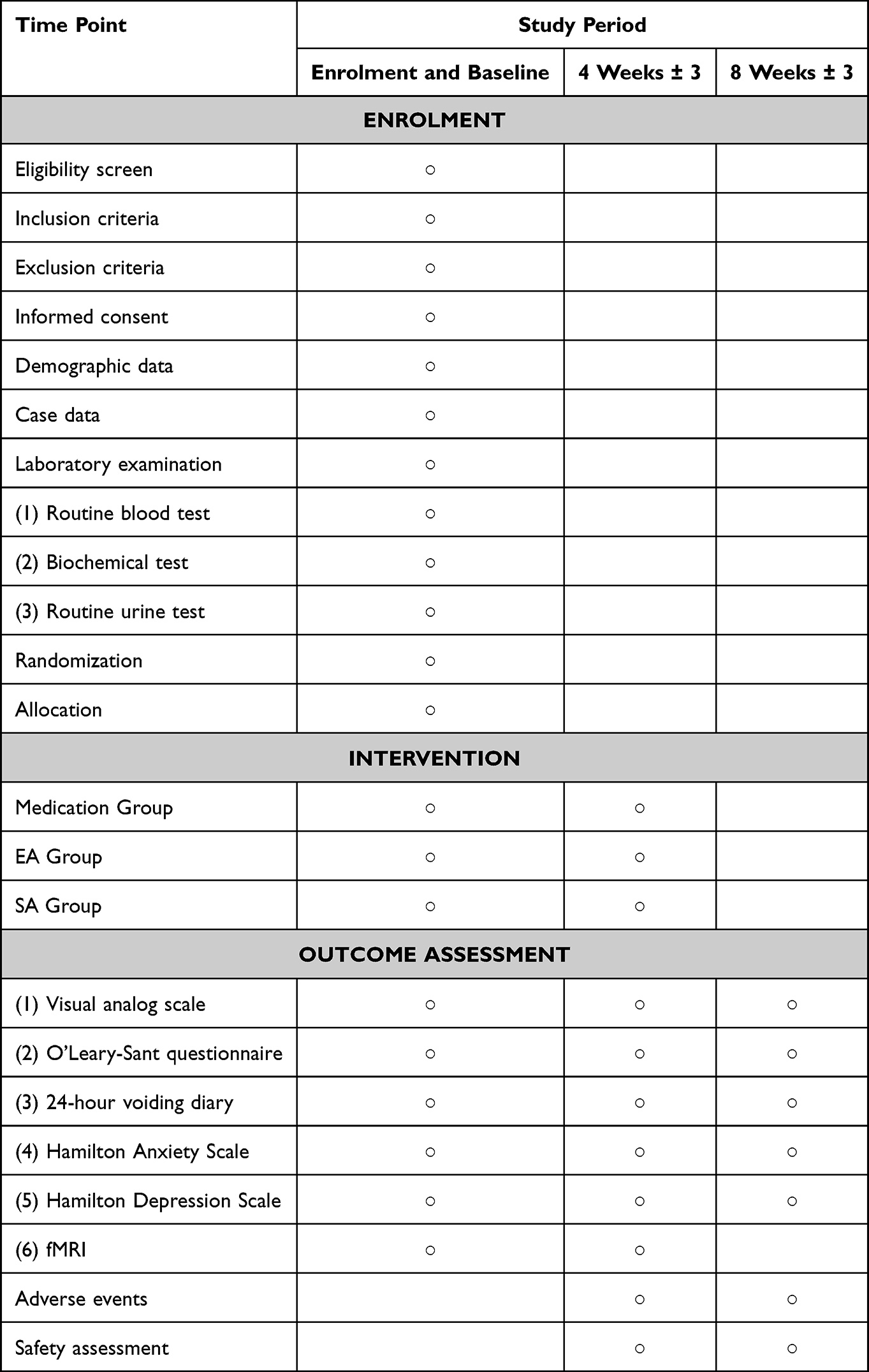 |
Table 1 The Schedule of Enrollment, Interventions, and Assessments |
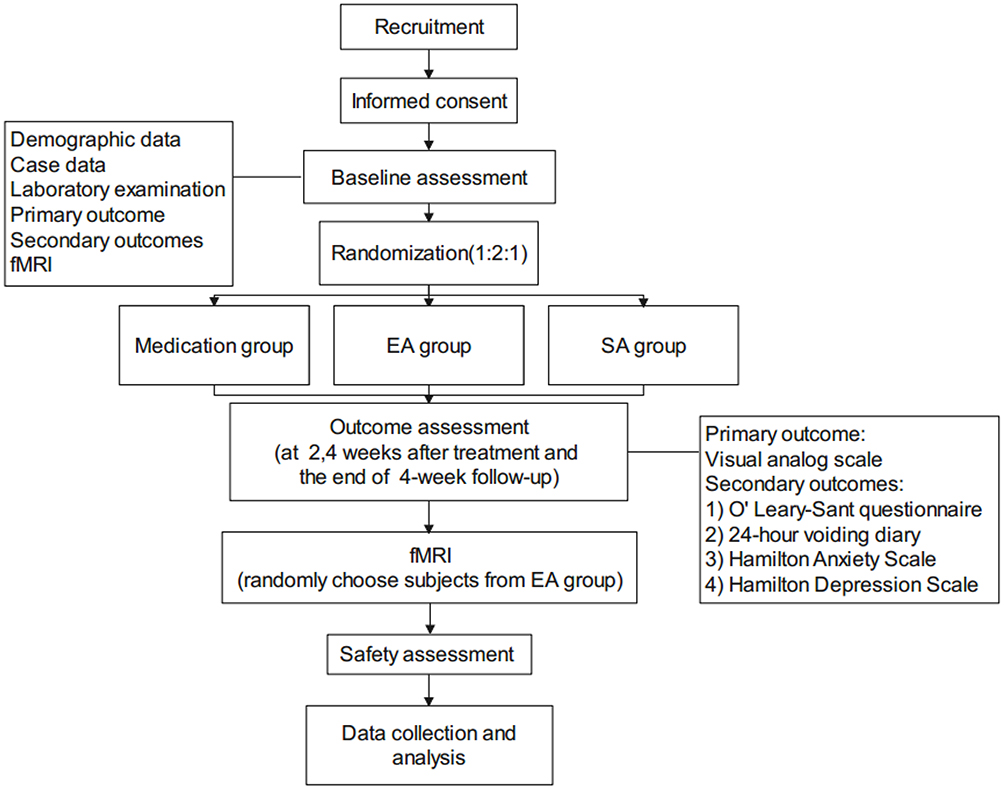 |
Figure 1 Flow chart of the study process. |
Recruitment
Participants will be primarily recruited from gynecology, urology and acupuncture departments during outpatient service in three hospitals, including The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou First People’s Hospital, Mishi Xiang Community Health Service Center from April 2022 to January 2025. The eligibility of individuals will be evaluated by the researchers on the basis of the criteria described in details. The Third Affiliated Hospital of Zhejiang Chinese Medical University will carry out interventions and be responsible for data management.
Ethical Consideration
This study protocol has been approved by the Ethics Committee of The Third Affiliated Hospital of Zhejiang Chinese Medical University (approval document NO. ZSLL-KY-2022-004-02) and registered at ClinicalTrials.gov on 15 March 2022 (NCT05279963). Prior to enrollment, researchers will explain the objective, research items, benefits and potential risks of the study to subjects in details. Before randomization, all eligible participants will be asked to sign an informed consent. All individuals will be entitled to full rights to decide whether they are willing to participate in this trial. Participant privacy will be strictly protected throughout the trials. All personal and disease information of participants will be kept confidential.
Eligibility Criteria
Diagnosis Criteria
Diagnostic criteria of BPS will be made according to guidelines the described by European Society for Interstitial Cystitis (ESSIC) and International Urinary Incontinence Advisory Committee (ICI).2,21
- The main symptoms are pain, discomfort or acid distension in regions of bladder, perineum, periurethral and pelvic, which relieved after urination, accompanied by frequent urination, urgent urination, nocturnal enuresis and other symptoms;
- Symptoms have been lasting for more than 6 months;
- Previous cystoscopy and water dilation therapy under anesthesia show characteristic bladder submucosal hemorrhagic spots or Hunner ulcer.
Inclusion Criteria
- Adults aged 18–70 years (include the age of 18 and 70; either sex);
- Must fulfill the first and the second diagnostic criteria;1,22
- 30 mm ≤ VAS score ≤ 80 mm;
- Participants fully understand the study protocol and a written informed consent is signed.
Exclusion Criteria
- Patients with previous bladder stones or other space-occupying lesions;
- Previous positive urine culture or significant abnormal urine routine;
- Significant organic lesions of genitourinary system and pelvic organs;
- Patients suffer from severe primary diseases such as cardiovascular, cerebrovascular, respiratory, liver and kidney, or patients cannot receive EA treatment due to any reasons;
- People with heart stents and other metallic substances in their bodies;
- Women who are pregnant, planning to become pregnant, breast-feeding or allergic to study drugs;
- Patients have participated in other clinical trials within the last 3 months.
Elimination Criteria
- Subjects suffer from obvious adverse reactions or complications during the treatment;
- Subjects fail to complete the prescribed treatment due to other accidents during treatment;
- Subjects do not meet the inclusion or exclusion criteria yet included in the trial by mistake;
- Subjects do not follow the prescribed treatment or have incomplete data that affects the evaluation;
Excluded cases will be explained and the original medical records will be retained for reference. The cases with at least one treatment record will merely be included for adverse event analysis rather than efficacy evaluation.
Randomization and Allocation Concealment
All patients will be randomly assigned to either medication group, EA group or SA group via random number table SAS 9.3 software will be adopted to generate random numbers. The independent clinical research assistant will be responsible for generating random numbers and making random allocation cards, each with its group allocation information and sealed into an opaque envelope, which will not be open until the first treatment. According to the order of enrollment, eligible participants will be randomly assigned into medication, EA or SA group at 1:2:1 ratio under the allocation in the envelope.
Blinding
Due to the characteristics of acupuncture, acupuncture manipulators and patients in medication group cannot be blinded. Nevertheless, to avoid the subjective bias of researchers and subjects, outcome assessment, data management and statistical analysis will be performed by different researchers blinded to the allocation information. Patients in EA and SA group are informed that they will receive one of two effective acupuncture interventions after enrollment, and during the treatment, patients in EA or SA groups will be in separate rooms to avoid communication.
Interventions
A total of 84 participants are randomly divided into medication group (n = 21), EA group (n = 42), and SA group (n = 21) at 1:2:1 ratio. Treatments will be performed by licensed acupuncturists who have at least 2 years of experience in acupuncture.
Medication Group
Participants in medication group will be merely treated with oral administration of amitriptyline capsule. The dosage of amitriptyline is 25mg twice a day, continue taking for 4 weeks in the treatment phase. Any changes in medications of participants will be recorded on diary cards.
EA Group
Acupoint Selection
The location of the acupoints will be determined based on the nomenclature and location of acupuncture points designated by the National Standard of the People’s Republic of China (GB/T 12346–2006). The prespecified acupoints applied here will include bilateral Sanyinjiao (SP6), Shenshu (BL23), Ciliao (BL32), Zhongliao (BL33), Zhibian (BL54) (Table 2 and Figure 2).
 |
Table 2 Location and Indication of Acupoints for Treating BPS |
 |
Figure 2 Locations of acupoints and non-acupoints in waist and lower limb region. The black nodes represent acupoints. The red nodes represent non-acupoints. The abbreviations and corresponding acupoints are connected by virtual lines. |
Manipulation
Acupuncture treatment will be performed by acupuncturists who have been well trained. Acupuncture will be performed with disposable and sterile needles in the specification of 0.25×40 mm (diameter: 0.25mm; Suzhou Medical Products Factory Co., Ltd, China). Patients are asked to lie in a prone position with whole body relaxed. Both the skin around the selected acupoint and the hand of acupuncturists are routinely disinfected, after insertion, manipulations of twirling, lifting and uniform reinforcing reducing manipulation will be performed on all needles to elicit “deqi”. The compositional sensation of “deqi” involves with numbness, soreness and heaviness, which are believed to be an essential component for acupuncture efficacy. EA procedures will be performed with electronic instruments (Hans-100A, Nanjing Jisheng Medical Technology Co., Ltd, China). Two paired of acupoints (ie, two Shenshu (BL23) and two Ciliao (BL32), respectively) are connected to the EA apparatus. Alternating-frequency mode is selected and the frequency is 2/100 Hz. EA intensity is determined in accordance with patients’ endurance. EA will last for 30 min for each treatment. Patients will receive a total number of 12 EA sessions, with the frequency of 3 sessions per week for 4 weeks.
SA Group
Acupoint Selection
Patients allocated to this group will receive acupuncture in non-meridian and non-acupoints regions. In the trunk region, the points are 5 cm away from respective acupoints. In the lower limb region, the point is 3cm away from Sanyinjiao (SP6). All points will only receive shallow insertion.
Manipulation
Acupuncture will be conducted by well-trained acupuncturists and performed with disposable and sterile needles in the specification of 0.25×40 mm (diameter: 0.25 mm; Suzhou Medical Products Factory Co., Ltd, China). Patients are asked to lie in a prone position with whole body relaxed. Both the skin around the selected acupoint and the hand of acupuncturists are routinely disinfected. The needles are subcutaneously inserted to non-meridian and non-acupoints regions. SA procedures will be performed with electronic instruments (Hans-100A, Nanjing Jisheng Medical Technology Co., Ltd, China). Two paired of points are connected to the electronic instruments. Alternating-frequency mode is selected and the frequency is 2/100 Hz. Different from EA group, the apparatus will run without electricity in SA group. The procedure will last for 30 min. Patients will receive a total number of 12 SA sessions, with the frequency of 3 sessions per week for 4 weeks.
Outcomes
Primary Outcome
Visual analog scale (VAS) score will be used as the primary outcome indicator from baseline to treatment completion in this study, since the BPS is characterized with pain. During the assessment, patients will quantify the pain intensity by marking the most relevant point on a 100mm horizontal line anchored by 2 descriptors: 100, representing “the most severe imaginable pain”, and 0, indicating “no pain.”23 The VAS will be collected at baseline, week 2, week 4, and week 8 after randomization.
Secondary Outcome Measures
Secondary outcome measures are as follows:
- O’Leary-Sant questionnaire: O’Leary-Sant questionnaire include interstitial cystitis Inflammation Index (ICSI) and interstitial Cystitis Problems Index (ICPI), which have been confirmed to be useful in the quantitative evaluation of therapies for BPS patients. It will be assessed at baseline, week 4 and week 8 after randomization. Both ICSI and ICPI contain 4 questions, which are respectively evaluated in four aspects: nocturia, frequency, urgency and pain or burning in bladder.24 ICSI mainly assesses the severity of symptoms and higher score indicates more severe symptoms. ICPI evaluates the degree of distress to the patient, and higher score represents the more serious the distress.25
- Hamilton Anxiety Scale (HAMA) will be used to assess emotional state at baseline, week 4 and week 8 after randomization. The HAMA has 14 symptom-defined elements that describe both somatic and psychological symptoms, of which scores range from 0 (no problem) to 4 (severe) with each item.26 A total HAMA score ranges from 0 to 56. Higher the score, severe the situation. In this scale, score 7–14 indicates mild severity, 15–21 represents mild to moderate severity, 22–28 represents moderate severity, and >28 indicates severe condition.
- Hamilton Depression Scale (HAMD) is identified as the “gold standard” of depression evaluations. It consists of 17 questions that serve as a point of reference for more recently developed scales.27 It will be assessed at baseline, week 4 and week 8 after randomization. According to recommendations, the total score is interpreted as follows: 0–7 = normal; 8–13 = mild depression; 14–18 = moderate depression; 19–22 = severe depression and ≥ 23 = very severe depression.28
- 24-hour voiding diary: The 24-hour voiding diary is a commonly used diagnostic tool to aid the clinician in treatment planning for patients with lower urinary tract symptoms. A standardized voiding diary will be given to patients. The frequency of urination and special feelings during the urination will be carefully recorded every day.
- Functional MRI: The fMRI data, including resting-state fMRI (rs-fMRI) and diffusion tensor imaging (DTI) data, will record changes in local brain activity and white matter integrity of patients with BPS after EA. In this study, twenty patients will be randomly selected from EA group and undergo two MRI scan sessions. The first session takes place at baseline period before the treatment starts while the second session takes place at week 4. The data will be obtained with a 1.5 Tesla MRI scanner (GE Medical Systems, LLC) in The Third Affiliated Hospital of Zhejiang Chinese Medical University. The rs-MRI and DTI will be acquired using echo-planar imaging (EPI) sequences and T1-weighted images are anticipated to be performed with a multi-echo magnetization-prepared rapid-acquisition gradient echo sequence.
Sample Size
According to the previous researches and the pilot experimental results from this study,14 the VAS scores was regarded as primary outcome, the VAS score of conventional treatment group was 4.89 ± 1.71, the VAS score of EA group was 3.14 ± 0.75, and the VAS score of SA group was 4.67 ± 1.13. This study was a prospective study with three groups and the sample size as 1:2:1. The sample size is calculated in software PASS 15.0, and we used One-Way Analysis of Covariance to calculate the sample size. The test level was set at α = 0.05, β = 0.1, and the test efficiency was set at 1 − β = 0.9. The results showed that the number of samples in each group was not less than 15. By considering the problem of missing samples or losing to follow-up, the sample size will be increased by 20. Thus, the total sample of the three groups will include cases not less than 84.
Statistical Analysis
All statistical analysis will be analyzed using SAS 9.3 for Windows by third-party statisticians based on the intention-to-treat principle (ITT) and per-protocol (PP) analysis. The categorical data will be displayed as counts and percentages, whereas the numeric data with normal distribution will be expressed as mean ± standard deviations. For data in normal distribution, repeated measures analysis of variance (ANOVA) will be used to perform between-group comparison by evaluating change in continuous variables before and after intervention. For data with skewed distribution, comparison will be assessed using non-parametric test. P values < 0.05 (two-sided) are considered statistically significant. For the fMRI data, pre-processing will be performed by DPARSFA and SPM8 software. Pre-processing will be completed on the data including realignment, co-registration, and spatial normalization into a standard space and smoothing. Statistical analysis of fMRI data will be based on Paired t-tests within participants in EA group, P values < 0.05 is used to indicate a significant difference.
Safety Assessment
The indicator of safety evaluation is the occurrence date, frequency, degree or duration of adverse events (AEs) arisen during the treatment course. For this trial, AEs related to acupuncture and EA mainly include unbearable pain, bleeding, haematoma, skin pigmentation, skin allergies, fainting during acupuncture, or other uncomfortable symptoms. AEs related to medication mainly include drug allergies, such as thirsty, drowsiness, constipation, blurred vision, dysuria, palpitations, arrhythmias, vertigo, dyskinesia, epileptic seizures, postural hypotension, liver injury or tardive dyskinesia. AEs that occur throughout the study will be assessed and recorded by investigators. At the occurrence of AEs, emergency management will be taken in a timely manner. For serious AEs, the researchers should report to the principal investigator and medical ethics committee immediately, who will determine whether the participant should be withdrawn from the study.
Quality Control, Data Management and Monitoring
Before the recruitment, in order to ensure the progress of the study, the research group will be required to complete a strict clinical training conference to conduct unified training on the protocol, Standard Operation Procedure (SOP) and scale evaluation, and each clinical researcher will be familiar with the research process and specific implementation rules, so as to improve internal observation consistency of researchers, which ensure the reliability of clinical research conclusions. The interventions will be performed by licensed acupuncturists with more than 2 years of experience in hospitals or clinics. Meanwhile, outcome assessors will attend standard training to record outcome assessments and fill in the case report forms uniformly. As for fMRI, routine quality control will be performed before each fMRI scan. All subjects will be tested under the same scanner and parameters, and all the scanning work will get performed by the same technician. At the same time, the environmental factors such as humidity and temperature are controlled. Overall, all outcomes and findings in clinical studies will be verified by the subjects and repeatedly confirmed to ensure the reliability and originality of the data. The data will be carefully collected and recorded on CRFs and checked twice by two independent investigators who are blinded to allocation. Data quality will be checked regularly by research assistants and supervised by monitors. The original CRFs and all other forms will be preserved securely at The Third Affiliated Hospital of Zhejiang Chinese Medical University.
Discussion
This is a study to investigate the efficacy of EA for treating BPS in contrast to medication and SA. The results might provide evidence for the application of acupuncture and exhibit the central mechanism on BPS.
The Effect of Acupuncture and EA for PHN
BPS is a chronic painful bladder condition characterized by pelvic pain and urinary symptoms without identified cause.29–31 Once the diagnosis is confirmed on the basis of symptoms, and other diseases are excluded, management should focus on symptom control, which include oral medications, intravesical instillations and cystoscopy with hydrodistension.32–34 However, therapies can only partially relieve the symptoms, and are often limited by unavoidable side effects.7 As a conservation treatment, acupuncture cannot only alleviate pain intensity, but also relieve co-exist conditions of BPS.35 At the same time, EA is also instrumental in simple operation, less associated risk and low medical cost. To date, several previous clinical observations have provided evidence on the efficacy and safety of acupuncture for BPS. For example, an RCT by Lv14 found that EA shows an early and long-term anti-hyperalgesic effect on BPS patients. Su15 claimed that 4 weeks of acupuncture may cause a greater improvement in pain of BPS.
Strengths of the Study
First, acupuncture, especially EA, is a common clinical treatment in Chinese medicine and already widely used in clinical practice. Previous studies have indicated that the use of EA at the beginning of pain can effectively increase pain threshold and prevent the occurrence of negative emotions.36,37 Besides, animal experiments have partially revealed the analgesia mechanism of EA for various diseases, including serotonin, opioids, and norepinephrine. Despite that the mechanism of EA for BPS is not clear yet, several studies have figured out some evidences to strengthen the assumption. One study conducted by Li38 found that EA can increase the mechanical pain threshold of the bladder in rats by reducing p-ERK1/2 and c-fos expression in the dorsal horn of the spinal cord. Additionally, with regard to EA parameters, 2/100 Hz is chosen in our trial given that previous studies reveal that EA with alternating-frequency mode plays an important role in analgesia by evoking the release of dynorphin and endorphin.39 However, to date, there is a lack of high-quality RCTs investigating the efficacy and safety of EA for treating BPS.
Second, acupoint prescription is carefully selected in our trial. Prescription include ten acupoints, namely, bilateral Sanyinjiao (SP6), Shenshu (BL23), Ciliao (BL32), Zhongliao (BL33), Zhibian (BL54). It has confirmed that Sanyinjiao acupoints could relieve nociception and emotion disorder in rats with painful emotions model.11 Other acupoints are located in lumber and sacrum region, ranging from the second lumbar vertebra to the fourth sacral foramen. Tissues of these acupoints area have widely distributed nerve endings, thus the application of these acupoints can eliminate inflammatory edema of nerves and fibers, and accelerate local blood circulation and tissue metabolism.
Third, superficial skin penetration at non-meridian and non-acupoints regions will be performed in the SA group, without needle manipulation for “deqi”. On the basis of various literature reviews, researchers have reported that superficial insertion at non-acupoints is the most commonly used method for administering sham treatments among acupuncture trials,40–42 and this strategy will most probably eliminate the placebo effect and confirm the specific physiological effect of needling because SA may be preferable, particularly for Chinese patients who are familiar with the general procedure of acupuncture.43,44
Fourth, twenty participants in EA group will be randomly selected to receive fMRI, which can investigate the structure and functional mechanism on the human brain.45 Despite numerous literatures of central regulatory network of pain emotion in animals, there are few breakthroughs in human beings.46 With the development of fMRI, it has been the best tool for gaining insights into brain function and eventually testable hypotheses.47
Limitations
Limitations also exist in the design of this trial. Given to the characteristic of EA procedure and the different therapies between the three groups, one important limitation of our study is that participants in medication group and acupuncture manipulators cannot be blinded, which probably lead to performance and detection bias. Besides, the primary outcome of VAS is subjective, which might reduce detection bias. However, the large bias is unlikely to be attached to the results since outcome assessors and statistical analysis will be blinded to group allocation. Additionally, in this study, the selection of acupoints is standardized and utilized for every participant without syndrome differentiation. Although dysfunction of the bladder is the main cause of BPS, acupoint selection base on subtype may optimize the effectiveness of EA. Further studies with more meticulous methodological quality and a larger sample size are imperatively warranted.
Conclusion
This protocol describes a randomized controlled, assessor-blinded trial that aims to evaluate the efficacy and safety of EA for treating BPS. The results will reveal whether EA can relieve the pain and emotional disorders in BPS patients. The findings will provide an evidence base for clinical practice to identify a complementary modality for treating BPS and investigate central mechanism of BPS.
Abbreviations
BPS, bladder pain syndrome; EA, electro-acupuncture; SA, Sham electro-acupuncture; VAS, Visual Analog Scale; HAMA, Hamilton Anxiety Scale; HAMD, Hamilton Depression Scale; fMRI, Functional magnetic resonance imaging; rs-fMRI, resting-state fMRI; DTI, diffusion tensor imaging; SPIRIT, Standard Protocol Items: Recommendations for Interventional Trials; STRICTA, Standards for Reporting Interventions in Clinical Trials of Acupuncture; SP6, The acupoint of Sanyinjiao; BL23, The acupoint of Shenshu; BL32, The acupoint of Ciliao; BL23, The acupoint of Zhongliao; BL54, The acupoint of Zhibian; ICSI, Interstitial cystitis Inflammation Index; ICPI, Interstitial Cystitis Problems Index.
Data Sharing Statement
It is a protocol of ongoing clinical trial and therefore there is no finding to report yet. After completion of this trial, data requested for public purposes will be provided.
Ethics and Dissemination
All procedures in the study will be conducted in accordance with the “Declaration of Helsinki”. The studies were reviewed and approved by the Ethics Committee of The Third Affiliated Hospital of Zhejiang Chinese Medical University (NO. ZSLL-KY-2022-004-02). The results of the study will be published in a peer-reviewed journal.
Consent
The participants provided their signed informed consent to participate in this trial after they received detailed information about the study procedures, possible risks, and their rights. Written informed consent was obtained from the individuals for the publication of any potentially identifiable images or data collected in this article.
Acknowledgments
The authors appreciate the support from all subjects who will participate in this study. The authors would like to express their appreciation to Wenqin Ni, Qike Ding, Wei Dai, Xinyuan Wu for their help on revising the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, or in all these areas; took part in drafting, revising or critically reviewing the article; and agree on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work. Yunyun Xu and Yangyun Chen contributed equally to this work.
Funding
The study was financially supported by Program of Sci-research Foundation of Zhejiang Provincial TCM Administration (2022ZB180), the National Natural Science Foundation of China (NSFC) (No. 82074541, 81873360, 81603691), Sci-research Foundation of Zhejiang Chinese Medical University (2021YKJ08, 2021YKJ09), Innovation and Entrepreneurship Training program for College students of Zhejiang Chinese Medicine University (202110344012), Science and Technology Innovation Activity plan and Xinmiao talent Plan for College students in Zhejiang province (2021R410017).
Disclosure
The authors declare that they have no competing interests.
References
1. Hanno PM, Erickson D, Moldwin R, Faraday MM; American Urological Association. Diagnosis and treatment of interstitial cystitis/bladder pain syndrome: AUA guideline amendment. J Urol. 2015;193(5):1545–1553. doi:10.1016/j.juro.2015.01.086
2. van de Merwe JP, Nordling J, Bouchelouche P, et al. Diagnostic criteria, classification, and nomenclature for painful bladder syndrome/interstitial cystitis: an ESSIC proposal. Eur Urol. 2008;53(1):60–67. doi:10.1016/j.eururo.2007.09.019
3. Hanno PM. Re-imagining interstitial cystitis. Urol Clin North Am. 2008;35(1):
4. Konkle KS, Berry SH, Elliott MN, et al. Comparison of an interstitial cystitis/bladder pain syndrome clinical cohort with symptomatic community women from the RAND interstitial cystitis epidemiology study. J Urol. 2012;187(2):508–512. doi:10.1016/j.juro.2011.10.040
5. Juliebø-Jones P, Hjelle KM, Mohn J, et al. Management of Bladder Pain Syndrome (BPS): a practical guide. Adv Urol. 2022;10(2022):7149467.
6. Nickel JC, Payne CK, Forrest J, Parsons CL, Wan GJ, Xiao X. The relationship among symptoms, sleep disturbances and quality of life in patients with interstitial cystitis. J Urol. 2009;181(6):2555–2561. doi:10.1016/j.juro.2009.02.030
7. Marcu I, Campian EC, Tu FF. Interstitial cystitis/bladder pain syndrome. Semin Reprod Med. 2018;36(2):123–135. doi:10.1055/s-0038-1676089
8. Chermansky CJ, Guirguis MO. Pharmacologic management of interstitial cystitis/bladder pain syndrome. Urol Clin North Am. 2022;49(2):273–282. doi:10.1016/j.ucl.2022.01.003
9. Ouyang H, Chen JD. Review article: therapeutic roles of acupuncture in functional gastrointestinal disorders. Aliment Pharmacol Ther. 2004;20(8):831–841. doi:10.1111/j.1365-2036.2004.02196.x
10. Qaseem A, Wilt TJ, McLean RM, et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline From the American College of Physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/M16-2367
11. Quinlan-Woodward J, Gode A, Dusek JA, Reinstein AS, Johnson JR, Sendelbach S. Assessing the Impact of Acupuncture on Pain, Nausea, Anxiety, and Coping in Women Undergoing a Mastectomy. Oncol Nurs Forum. 2016;43(6):725–732. doi:10.1188/16.ONF.725-732
12. Tsai SL, Fox LM, Murakami M, Tsung JW. Auricular acupuncture in emergency department treatment of acute pain. Ann Emerg Med. 2016;68(5):583–585. doi:10.1016/j.annemergmed.2016.05.006
13. Wu YY, Jiang YL, He XF, et al. Effects of electroacupuncture with dominant frequency at sp 6 and st 36 based on meridian theory on pain-depression dyad in rats. Evid Based Complement Alternat Med. 2015;2015:732845. doi:10.1155/2015/732845
14. Lv TT, Lv JW, Wang SY, Jiang C, Gu YJ, Liu HR. Efficacy of electroacupuncture nerve stimulation therapy for interstitial cystitis/bladder pain syndrome. Zhongguo Zhen Jiu. 2019;39(5):467–472. doi:10.13703/j.0255-2930.2019.05.003
15. Min-zhi SU, Xi-quan HU, Xue-lian CHEN, et al. Clinical observation of electroacupuncture combined with bladder irrigation for bladder pain syndrome. Shanghai J Acu-mox. 2020;39(2):4.
16. Chao-Gan Y, Yu-Feng Z. DPARSF: a MATLAB toolbox for “pipeline” data analysis of resting-state fMRI. Front Syst Neurosci. 2010;14(4):13.
17. He TW, Li F, Yang BF, et al. Neural mechanisms of acupuncture as revealed by fMRI studies. Auton Neurosci. 2015;190:1–9. doi:10.1016/j.autneu.2015.03.006
18. Legrain V, Iannetti GD, Plaghki L, Mouraux A. The pain matrix reloaded: a salience detection system for the body. Prog Neurobiol. 2011;93(1):111–124. doi:10.1016/j.pneurobio.2010.10.005
19. Chan AW, Tetzlaff JM, Altman DG, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;158(3):200–207. doi:10.7326/0003-4819-158-3-201302050-00583
20. Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Int J Surg. 2012;10(1):28–55. doi:10.1016/j.ijsu.2011.10.001
21. Hanno P, Lin A, Nordling J, et al. Bladder pain syndrome committee of the international consultation on incontinence. Neurourol Urodyn. 2010;29(1):191–198. doi:10.1002/nau.20847
22. Malde S, Palmisani S, Al-Kaisy A, Sahai A. Guideline of guidelines: bladder pain syndrome. BJU Int. 2018;122(5):729–743. doi:10.1111/bju.14399
23. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011;63(Suppl 11):S240–52.
24. El-Hefnawy AS, Soliman HMM, Abd-Elbary SOM, Shereif WI. Long-standing nonulcerative bladder pain syndrome: impact of Thiele massage on bladder and sexual domains. Low Urin Tract Symptoms. 2020;12(2):123–127. doi:10.1111/luts.12291
25. Huang MC, Hsieh CH, Chang WC, Chang ST, Lee MS. Assessment of treatment outcomes of interstitial cystitis with hydrodistention and bladder training by O’Leary-Sant interstitial cystitis symptom and problem indices. Taiwan J Obstet Gynecol. 2018;57(5):718–721. doi:10.1016/j.tjog.2018.08.019
26. Thompson E. Hamilton Rating Scale for Anxiety (HAM-A). Occup Med. 2015;65(7):601. doi:10.1093/occmed/kqv054
27. Carneiro AM, Fernandes F, Moreno RA. Hamilton depression rating scale and Montgomery-asberg depression rating scale in depressed and bipolar I patients: psychometric properties in a Brazilian sample. Health Qual Life Outcomes. 2015;2(13):42. doi:10.1186/s12955-015-0235-3
28. Melzer J, Rostock M, Brignoli R, Keck ME, Saller R. Preliminary data of a HAMD-17 validated symptom scale derived from the ICD-10 to diagnose depression in outpatients. Forsch Komplementmed. 2012;19(4):191–196. doi:10.1159/000342018
29. Suskind AM, Berry SH, Ewing BA, Elliott MN, Suttorp MJ, Clemens JQ. The prevalence and overlap of interstitial cystitis/bladder pain syndrome and chronic prostatitis/chronic pelvic pain syndrome in men: results of the RAND interstitial cystitis epidemiology male study. J Urol. 2013;189(1):141–145. doi:10.1016/j.juro.2012.08.088
30. McLennan MT. Interstitial cystitis: epidemiology, pathophysiology, and clinical presentation. Obstet Gynecol Clin North Am. 2014;41(3):385–395. doi:10.1016/j.ogc.2014.05.004
31. Jhang JF, Kuo HC. Pathomechanism of interstitial cystitis/bladder pain syndrome and mapping the heterogeneity of disease. Int Neurourol J. 2016;20(Suppl 2):S95–104. doi:10.5213/inj.1632712.356
32. Cox A. Management of interstitial cystitis/bladder pain syndrome. Can Urol Assoc J. 2018;12(6 Suppl 3):S157–S160. doi:10.5489/cuaj.5324
33. Beckett MK, Elliott MN, Clemens JQ, Ewing B, Berry SH. Consequences of interstitial cystitis/bladder pain symptoms on women’s work participation and income: results from a national household sample. J Urol. 2014;191(1):83–88. doi:10.1016/j.juro.2013.07.018
34. Huffman MM, Slack A, Hoke M. Bladder Pain Syndrome. Prim Care. 2019;46(2):213–221. doi:10.1016/j.pop.2019.02.002
35. Pingping T, Jianbing L, Yanzhi X, Chao B. Professor Wu Xu’s experience in the treatment of interstitial cystitis with tongdu wenyang acupuncture. J Nanjing Univ Tradit Chin Med. 2021;37(3):3.
36. Guo JD, O’Flaherty BM, Rainnie DG. Serotonin gating of cortical and thalamic glutamate inputs onto principal neurons of the basolateral amygdala. Neuropharmacology. 2017;126:224–232. doi:10.1016/j.neuropharm.2017.09.013
37. Liao HY, Lin YW. Electroacupuncture attenuates chronic inflammatory pain and depression comorbidity through transient receptor potential V1 in the brain. Am J Chin Med. 2021;49(6):1417–1435. doi:10.1142/S0192415X2150066X
38. Li W, Jin Z, Liu JD, et al. Effect of electroacupuncture on expression of p-ERK1/2 and c-fos in spinal dorsal horn in rats with interstitial cystitis. Zhen Ci Yan Jiu. 2021;46(5):375–379. doi:10.13702/j.1000-0607.200713
39. Zhao ZQ. Neural mechanism underlying acupuncture analgesia. Prog Neurobiol. 2008;85(4):355–375. doi:10.1016/j.pneurobio.2008.05.004
40. Tan JY, Suen LK, Wang T, Molassiotis A. Sham acupressure controls used in randomized controlled trials: a systematic review and critique. PLoS One. 2015;10(7):e0132989. doi:10.1371/journal.pone.0132989
41. Jinli K, Mingxue Z, Hongsai S, Hongxu L. Bibliometrics analysis of control study of sham acupuncture in journals with high impact factors in recent 10 years based on PubMed. J Pain Res. 2021;28(7):6.
42. Xu H, Fang JQ, Ma RJ, et al. Ethics review characteristics of clinical research of acupuncture and moxibustion. Zhong Guo Zhen Jiu. 2021;41(11):1273–1275.
43. Liu Z, Yan S, Wu J, et al. Acupuncture for chronic severe functional constipation: a randomized trial. Ann Intern Med. 2016;165(11):761–769. doi:10.7326/M15-3118
44. Manber R, Schnyer RN, Lyell D, et al. Acupuncture for depression during pregnancy: a randomized controlled trial. Obstet Gynecol. 2010;115(3):511–520. doi:10.1097/AOG.0b013e3181cc0816
45. Filippi M, Rocca MA. Present and future of fMRI in multiple sclerosis. Expert Rev Neurother. 2013;13(12 Suppl):27–31. doi:10.1586/14737175.2013.865871
46. Bair MJ, Robinson RL, Eckert GJ, Stang PE, Croghan TW, Kroenke K. Impact of pain on depression treatment response in primary care. Psychosom Med. 2004;66(1):17–22. doi:10.1097/01.PSY.0000106883.94059.C5
47. Logothetis NK. What we can do and what we cannot do with fMRI. Nature. 2008;453(7197):869–878. doi:10.1038/nature06976
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.