")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Elderly Individuals Residing in Nursing Homes in Western Romania Who Have Been Diagnosed with Hearing Loss are at a Higher Risk of Experiencing Cognitive Impairment
Authors Arnautu SF , Arnautu DA , Jianu DC, Tomescu MC , Blajovan MD, Banciu CD, Malita DC
Received 20 October 2023
Accepted for publication 21 February 2024
Published 29 February 2024 Volume 2024:17 Pages 881—888
DOI https://doi.org/10.2147/JMDH.S439282
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sergiu-Florin Arnautu,1,2 Diana-Aurora Arnautu,2 Dragos-Catalin Jianu,1,3 Mirela-Cleopatra Tomescu,2 Marc-Dan Blajovan,4 Christian-Dragos Banciu,2 Daniel-Claudiu Malita4
1Center for Cognitive Research in Neuropsychiatric Pathology (NeuroPsy-Cog), Department of Neurosciences, Victor Babes University of Medicine and Pharmacy, Timisoara, Romania; 2Department of Internal Medicine, Victor Babes University of Medicine and Pharmacy, Timisoara, Romania; 3Department of Neurology, Victor Babes University of Medicine and Pharmacy, Timisoara, Romania; 4Department XV-Orthopedics-Traumatology, Urology, Radiology and Medical Imagistics, Faculty of Medicine, Victor Babes University of Medicine and Pharmacy, Timisoara, Romania
Correspondence: Diana-Aurora Arnautu, Department of Internal Medicine, Victor Babes University of Medicine and Pharmacy, 2nd Eftimie Murgu Square, Timisoara, 340001, Romania, Tel +40 734600550, Email [email protected]
Purpose: The objective of this research was to determine if there is any correlation between the severity of neurocognitive disorder and hearing impairment in the elderly.
Patients and Methods: This is a population-based observational study that included subjects aged ≥ 65 years. They were evaluated for the existence of cardiovascular risk factors, diabetes, stroke, alcohol abuse, and smoking. Hearing impairment was diagnosed by an audiologist, using behavioral audiometric examination. These evaluations might have been performed in response to concerns about hearing loss, or they could have been a routine component of yearly comprehensive health screenings that included a Mini-Mental State Examination 2nd Edition (MMSE-2) test. According to the results of the MMSE-2 scale, we divided the individuals into two groups, Group I for those who had cognitive impairment and severe neurocognitive disorder, and Group II for those who did not have cognitive impairment.
Results: The study enrolled 203 patients with a mean age of 77 ± 7.5 years (range 65– 98), 99 (48%) were males. When comparing the two groups, group I patients presented more often cardiovascular risk factors, stroke, diabetes, and impaired hearing. The univariable logistic regression found that cognitive impairment was significantly more frequent in the elderly with cardiovascular disease, diabetes, and stroke (p< 0.0001). The multivariate regression analysis found that stroke (p< 0.0001) diabetes (p=0.0008), cardiovascular disease (p=0.0004), and impaired hearing (p=0.0011) were significantly linked to cognitive impairment. The occurrence of hearing impairment in the elderly was related to having an MMSE-2 score of 14 or below.
Conclusion: According to the findings of this research, the elderly who have trouble hearing in addition to other conditions might have an increased risk for severe neurocognitive disorder.
Keywords: elderly, impaired hearing, cognitive impairment, MMSE-2, nursing home
Introduction
The sensation of isolation and loneliness can have deleterious impacts on both mental and physical health, since it has been scientifically linked to an increased risk of developing severe health problems.1 Individuals with mental health disorders, hearing and visual impairments, and chronic
Recently, hearing loss has been recognized as a risk factor for severe neurocognitive disorder. However, this area has not received significant attention in the management of patients at risk for severe neurocognitive disorder.2 Recent studies have shown that hearing loss is an independent risk factor for severe neurocognitive disorder, even in individuals who are cognitively intact.3–8 The population attributable fraction (PAF) of hearing loss for severe neurocognitive disorder has been determined to be 23%, surpassing other individual modifiable risk factors such as diabetes, hypertension, smoking, depression, and social isolation.2 Age-related hearing loss (ARHL) is prevalent among the elderly, and it is often undertreated. Given its easy diagnosis and treatability, it is a promising target for preventive strategies for severe neurocognitive disorder. However, establishing a causal link between ARHL and severe neurocognitive disorder is crucial before making definitive recommendations involving ARHL as a threat for severe neurocognitive disorder.
Adult-onset hearing loss was often thought as a natural part of aging, but it is now understood to be a chronic condition with serious ramifications for people’s health. As well as increasing the patient’s risk of cognitive decline, depression, loneliness, and social isolation, impaired communication and attentiveness raise practical safety issues.9–13 In the last decade, research on the association between severe neurocognitive disorder and hearing loss has exploded, and hearing loss has been called the highest changeable risk factor for severe neurocognitive disorder.2,14 It’s important to recognize adult-onset hearing loss as a disease with serious consequences, particularly given the lack of information available to both healthcare providers and the general public.15 According to estimates, by 2050 almost 2.5 billion people around the world will experience some form of hearing loss. The prevalence of severe neurocognitive disorder in Romania, was estimated by the United Nation’s World Population to be 1.43 in 2018 and it estimates on future population projections an increase of prevalence of severe neurocognitive disorder up to 2.56% by 2050.16,17
As the biggest modifiable risk factor for severe neurocognitive disorder, hearing loss was identified by the Lancet Commission on the basis of just three research.5,8,17 There seems to be a correlation between the severity of hearing loss as determined by an automated testing device and an increased risk of severe neurocognitive disorder.4
The limited number of studies, in conjunction with a large variation in severe neurocognitive disorder and audiometric evaluations that may be seen across research, highlights the need of collecting further prospective longterm epidemiologic data. In the present research, we investigated hearing loss and its possible link to the development of mild cognitive impairment and severe neurocognitive disorder.
Materials and Methods
This research, conducted in nursing homes for the elderly in Timisoara, Romania, is population-based, observational, and cross-sectional. The participants had to be ≥ 65 years old, and they were given official behavioral audiometric examinations by an audiologist. The exclusion criteria included individuals with documented histories of depression, stroke, prior alcohol or drug misuse, previous traumatic brain injury and related neurosurgical interventions, as well as any other medical condition (including significant visual impairments that have not been sufficiently corrected).18
Patients have been examined and enrolled in April 2023. A number of 203 people with ages ≥65 years were included in the research and met the study’s eligibility requirements since they were either cognitively unimpaired or had cognitive impairment. A neurologist, an otolaryngologist and a psychologist made up the expert panel that assessed cognitive state for each patient.
At inclusion, subjects’ age, gender, ethnicity, education level (12 vs >12 years), smoking habits, alcohol use history, and the presence of co-morbidities like diabetes, stroke, and cardiovascular disease (defined as coronary artery disease, atrial fibrillation, hypertension, and congestive heart failure) were all registered. Participants’ demographic and clinical characteristics were gathered either by an in-person medical interview conducted at the time of enrollment or a retrospective assessment of their medical records.
To the question “is the subject’s hearing functionally normal?”, hearing loss and hearing aid is indicated by a score of 1, with normal hearing being 0. Clinician evaluations of these items were used to place people in either the “Normal Hearing” or “Impaired Hearing” groups.
At baseline of study all patients’ symptoms of depression were evaluated using the Geriatric Depression Scale (GDS).19 The GDS has 15 questions, all of which need a yes/no response, and scores range from 0 to 15. It has been established that a cutoff of ≥ 5 is fairly sensitive for the detection of severe depression.20
A thorough neuropsychological battery21 was administered after a history and physical examination, as well as evaluations of behavioral symptoms (Clinical Dementia Rating),22,23 Neuropsychiatric Inventory Questionnaire,24 and functional symptoms (Functional Assessment Questionnaire).25 A normal cognitive status, mild cognitive impairment, or severe neurocognitive disorder was assigned to each participant. The criteria established by the Alzheimer’s Disease Centres Clinical Task Force26 were used to diagnose mild cognitive impairment and severe neurocognitive disorder. Severe neurocognitive disorder is typically identified when a person’s cognitive abilities decline in a way that impedes their ability to live independently. It’s important to note that a previous diagnosis of mild cognitive impairment does not necessarily indicate that the person will develop severe neurocognitive disorder.
Clinical interviews and physical examinations were used to detect hearing loss at enrollment. The 203 subjects who were tested formally using audiometers often had concerns about their hearing or were tested as part of their yearly checkup.
Regarding the behavioral audiometric testing the study followed reporting standards and calculated air-conduction and bone-conduction pure-tone averages (PTAs) at frequencies of 0.5, 1, 2, and 3 kilohertz (kHz), with a preference for masked frequencies.27 In cases where the frequency 3 kHz was not accessible, the alternative approach was to utilize the average of 2 kHz and 4 kHz.28 For analysis, the lowest air-conduction pure tone average (PTA) from both the left and right ear, as well as the corresponding bone-conduction PTA from each ear, were chosen. The results of the air-conduction pure-tone audiometry (PTA) were classified into different categories based on the level of hearing loss. These categories include normal hearing (≤25 dB HL), mild hearing loss (26–39 dB HL), moderate hearing loss (40–69 dB HL), severe hearing loss (70–89 dB HL), and profound hearing loss (≥90 dB HL).29 The analysis focused on selecting the highest standard speech audiometry word recognition score (WRS) from both the left and right ear. This included Isophonemes,30 W-22,31 and NU-6.32 The audiometric tests were conducted without the use of hearing aids.
During the enrollment interview, the study partners (referred to as informants) were asked to assess any subjective hearing difficulties that may interfere with the participants’ daily activities. The informants were questioned about whether the participant experiences hearing difficulties that significantly impact their daily activities.
Based on how they did on the Mini-Mental State Examination 2nd Edition (MMSE-2), with utilized permission from Oana Mihaela Popescu in Romanian version, the patients with cognitive impairment were put into one of three categories: mild cognitive impairment (score of 21–23), moderate cognitive impairment (score of 10–20), or serious cognitive impairment (score ≤ 9).
The retrieval and analysis of data were preceded by permission from an institutional review board.
It was ensured that all participants gave their written informed consent before enrolling in the study. The research was carried out in compliance with the Helsinki Declaration’s guidelines and was authorized by the Ethics Committee of “Victor Babes” University of Medicine and Pharmacy Timisoara (nr.8/2023).
Statistical Analysis
The statistical analysis utilized version 20.211 of the MedCalc statistical software for Windows, developed by MedCalc Software Ltd in Ostend, Belgium. The software can be accessed at https://www.medcalc.org and the analysis was conducted in 2023. The study groups were compared using Chi-square tests for categorical data and Student’s t-tests for continuous variables. The covariates that were examined for their potential influence on severe neurocognitive disorder were chosen on the basis of previous studies and consisted in cardiovascular disease, diabetes, history of stroke, age, gender, history smoking, years of education, and diagnosed impaired hearing.1–11 Univariate and multivariate logistic regression models were utilized to evaluate the impact of each variable on the observed outcomes. Logistic regression models were used to assess the probability of an event happening. The odds ratio (OR) and its corresponding 95% confidence interval (CI) were analyzed to determine the likelihood of the event occurring. All variables associated with severe neurocognitive disorder in univariate analysis were subjected to a multivariate regression analysis with the backward stepwise method. The analyzed parameters’ sensitivity and specificity were computed using receiver-operating characteristic (ROC) curves. Area under the ROC curve (AUC) was used to calculate the discrimination ability of the analyzed parameters. Two-tailed p<0.05 was used as the statistical significance threshold.
Results
The study group included 203 patients with an average age of 77 ± 7.5 years (ranging from 65 to 98 years). Among these patients, 99 (48.7%) were male, 124 (61%) had more than 12 years of education, 16 (7.88%) had a Geriatric Depression Scale (GDS) score less than 5, 28 (13.7%) had cognitive impairment, and 122 (60%) had impaired hearing.
The subjects were divided into two groups based on the presence (group A) or absence (group B) of severe neurocognitive disorder. The comparison of demographic and clinical characteristics of the elderly patients with and without severe neurocognitive disorder is presented in Table 1.
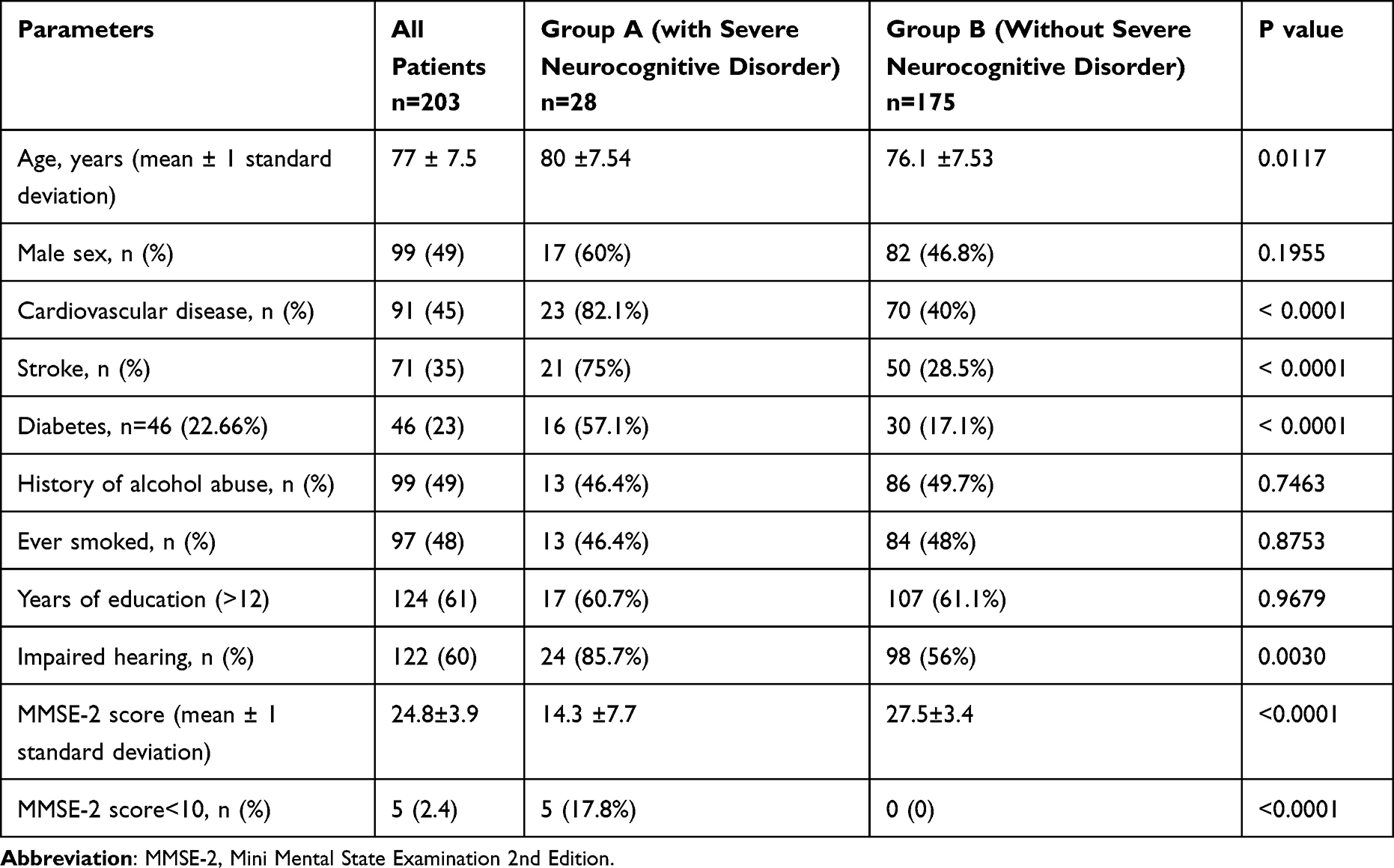 |
Table 1 Comparison of Demographic and Clinical Characteristics of the Elderly Patients |
Upon comparing the two groups, it was observed that individuals with severe neurocognitive disorder exhibited a higher prevalence of comorbidities and a greater percentage of impaired hearing.
In the analysis using univariate logistic regression (Table 2), a strong association was found between the presence of severe neurocognitive disorder in the elderly and several factors. Specifically, the presence of cardiovascular disease (p<0.0001), history of stroke (p<0.0001), diabetes mellitus (p<0.0001), and impaired hearing (p=0.0015) were all notably associated with severe neurocognitive disorder.
 |
Table 2 Predictors of Severe Cognitive Impairment |
In the investigation of prognostic factors for severe neurocognitive disorder, a multivariate analysis using logistic regression revealed a higher probability, with statistical significance, for several factors. These factors include cardiovascular disease (p=0.0004), diabetes mellitus (p=0.0008), stroke (p<0.0001), and impaired hearing (p=0.001), as shown in Table 2.
Upon analyzing the ROC curves, it was observed that the prevalence of impaired hearing rose when the MMSE-2 score was equal to or less than 14, as shown in Figure 1. The sensitivity of this occurrence was determined to be 84.21% with a 95% CI ranging from 60.4% to 96.6%. Additionally, the specificity was found to be 55% with a 95% CI ranging from 21.2% to 86.3%. The area under the curve (AUC) is 0.728, indicating the overall performance of the model. The p-value is 0.0317, suggesting that there is a statistically significant association between the variables.
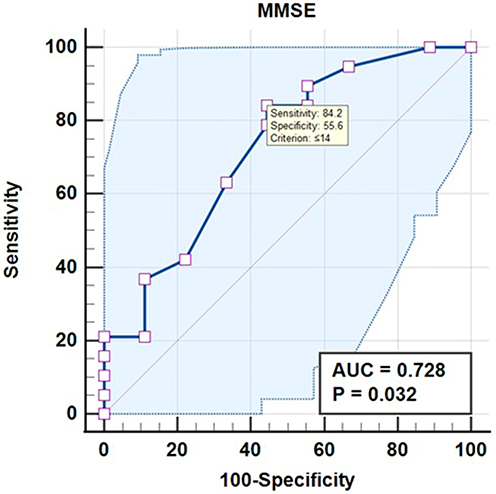 |
Figure 1 ROC curve analysis for impaired hearing as independent predictor of MMSE-2 score. Abbreviations: AUC, area under the curve; MMSE-2, Mini Mental State Examination 2nd Edition; ROC, receiver operating curve. |
Discussion
This is the first study to evaluate the link between cognitive decline and impaired hearing in Romania. Its findings indicate a notable association between hearing impairment and increased rates of cognitive decline. The study found that individuals with hearing impairment had an 85% increased likelihood of developing cognitive impairment.
While the primary clinical criteria for diagnosing moderate cognitive impairment do include cognitive symptoms such as memory issues, it is possible for older individuals to inaccurately assess their own cognitive ability. A higher level of awareness index, indicating a larger difference between objective and subjective performance, was found to be associated with poorer performance in various neuropsychological tests. One particularly noteworthy finding among the statistically significant negative connections is the reduced awareness of overall cognitive abilities, which appears to be associated with lower scores on the MMSE-2.18
There has been a lot of work put into explaining the connection between sensory impairment and cognitive function in the elderly, but very little data on the nature of this connection has emerged. Several theories have been proposed in order to explain the connection between sensory impairment and cognitive performance. The “cognitive load on perception” hypothesis is the first one, and it states that cognitive decline may lead to apparent losses in sensory performance due to the fact that cognitive decline reduces the cognitive resources that are accessible for sensory perception.33,34 Speech recognition becomes more difficult for those who have a hearing impairment, which may lead to greater perceptual load and cognitive burden in comparison to people who have normal hearing function. According to Pichora-Fuller et al’s framework for understanding effortful listening (FUEL), listening effort also relies on the desire of the listener to expend their mental effort to remain listening in any scenario.35 In other words, listening effort depends on how much the listener wants to put in the effort to listen. The “sensory deprivation” theory is the second one, and it states that cognitive decline may be caused by sensory loss in later life. This is because cognitive deterioration reflects the impact of decreasing sensory stimulation.34–38 The “common cause” theory is the third one, and it suggests that the correlations between sensory functioning and cognitive capacity may develop as a result of age-related characteristics that are common to both.34 Individuals who have sensory impairments may be at a disadvantage in their performance on psychometric tests as a direct consequence of problems in sensory perception.34,39 This is the fourth hypothesis. Individuals who have sensory impairments may be at a disadvantage in their performance on psychometric tests.
Analyzing and comprehending the patterns of cognitive decline and their connection to sensory impairment can provide valuable understanding of the progression of cognitive decline. This knowledge can help identify potential interventions that can optimize cognitive function and promote healthy longevity in older individuals.
Previous research on the relationship between sensory impairments and cognitive decline and severe neurocognitive disorder has been limited in both quantity and conclusive findings. A longitudinal study conducted by Deal et al investigated the link between cognitive function and hearing loss.40 The study included 253 individuals aged 45–64 years at the beginning of the study and followed them for a period of 20 years. The findings of the study indicated that hearing damage was associated with a faster decline in cognitive abilities over the course of the study. In a study conducted by Dupuis et al, the impact of single and dual sensory impairment on cognitive function was investigated.41 The researchers used the Montreal Cognitive Assessment (MoCA) to assess cognitive function. The findings revealed that individuals with normal hearing and visual functioning had a higher likelihood of passing the MoCA compared to those with sensory impairments. Hong et al conducted a study called the Blue Eye Mountain Study, which involved 3654 participants. They found that there was no connection between sensory impairments (specifically visual, hearing, and dual impairments) and cognitive decline.42 In a study conducted by van Hooren et al, the researchers examined the influence of hearing aids on cognitive performance in older individuals with mild-to-moderate hearing impairment. The study included a group of 56 participants who were equipped with hearing aids, with a mean age of 72.5, and a control group of 46 individuals with hearing impairment but without hearing aids, with a mean age of 74.5. The results of the study indicated that there was no observed improvement in cognitive performance after a period of 12 months for either group.43 This finding supports the notion that hearing aids may not have a significant impact on cognitive abilities in older individuals with mild-to-moderate hearing impairment. The study found a strong link between sensory impairment and the risk of severe neurocognitive disorder, which is consistent with previous research and reviews.5,6,8,44,45 The Health, Ageing and Body Composition (Health ABC) study conducted by Deal et al discovered a significant association between moderate/severe audiometric hearing impairment and a 55% higher risk of incident severe neurocognitive disorder over a period of 9 years.44
Limitations
The study’s sample size is relatively small, which could potentially limit its ability to accurately detect significant effects due to insufficient statistical power. The findings may lack representativeness in relation to the wider population.
The sample is not randomly selected or does not accurately represent the larger population, the findings may lack generalizability beyond the participants involved in the study.
It may be difficult to demonstrate causality between independent (risk factors) and dependent (hearing aid usage in the progression of cognitive impairment) variables in the absence of a control group.
A research with such a limited time frame may not be capable to identify subtle or gradual changes over time.
Conclusion
According to the findings of this research, those who have trouble hearing in addition to other conditions may represent a clinical feature that is at increased risk for severe neurocognitive disorder. Hearing loss that is associated with aging as well as severe neurocognitive disorder are responsible for enormous costs to public health, including a significant amount of disability, morbidity, and death. It is possible that a deeper understanding of the mechanisms that link the disorders of later life could make it easier to identify and disseminate interventions (such as hearing rehabilitation and control of risk factors) that are capable of preserving brain health throughout the aging process and altering the clinical courses of individuals who are at risk.
Furthermore, in situations of diminished self-awareness, it is crucial to notify family members/caregivers and recommend that patients follow appropriate intervention programs that employ strategies to enhance self-awareness and enhance important capabilities.
Acknowledgments
Our acknowledgments to the audiologists who performed the audiometric testing and to the psychologist Oana Mihaele Popescu who performed the MMSE-2 testing for the elderly institutionalized in nursing homes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tragantzopoulou P, Giannouli V. Social isolation and loneliness in old age: exploring their role in mental and physical health. Psychiatrike. 2021;32(1):59–66. doi:10.22365/jpsych.2021.009
2. Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care. Lancet. 2017;390(10113):2673–2734. doi:10.1016/s0140-6736(17)31363-6
3. Quaranta N, Coppola F, Casulli M, et al. The prevalence of peripheral and central hearing impairment and its relation to cognition in older adults. Audiol Neurotol. 2014;19(Suppl. 1):10–14. doi:10.1159/000371597
4. Gallacher J, Ilubaera V, Ben-Shlomo Y, et al. Auditory threshold, phonologic demand, and incident dementia. Neurology. 2012;79(15):1583–1590. doi:10.1212/wnl.0b013e31826e263d
5. Lin FR, Metter EJ, O’Brien RJ, Resnick SM, Zonderman AB, Ferrucci L. Hearing loss and incident dementia. Arch Neurol. 2011;68(2). doi:10.1001/archneurol.2010.362
6. Gurgel RK, Ward PD, Schwartz S, Norton MC, Foster NL, Tschanz JT. Relationship of hearing loss and dementia. Otol Neurotol. 2014;35(5):775–781. doi:10.1097/mao.0000000000000313
7. Golub JS, Luchsinger JA, Manly JJ, Stern Y, Mayeux R, Schupf N. Observed hearing loss and incident dementia in a multiethnic cohort. J Am Geriatr Soc. 2017;65(8):1691–1697. doi:10.1111/jgs.14848
8. Deal JA, Betz J, Yaffe K, et al. Hearing impairment and incident dementia and cognitive decline in older adults: the health ABC study. GERONA. 2016:glw069. doi:10.1093/gerona/glw069
9. Anstey K, Wood J, Lord S, Walker J. Cognitive, sensory and physical factors enabling driving safety in older adults. Clinic Psychol Rev. 2005;25(1):45–65. doi:10.1016/j.cpr.2004.07.008
10. Shukla A, Harper M, Pedersen E, et al. Hearing loss, loneliness, and social isolation: a systematic review. Otolaryngol-Head Neck Surg. 2020;162(5):622–633. doi:10.1177/0194599820910377
11. Lawrence BJ, Jayakody DMP, Bennett RJ, Eikelboom RH, Gasson N, Friedland PL. Hearing loss and depression in older adults: a systematic review and meta-analysis. Gerontologist. 2019;60(3):e137–e154. doi:10.1093/geront/gnz009
12. Jianu DC, Barsan C. Vascular Cognitive Impairment. Ro J Neurol. 2019;18(1):8–15. doi:10.37897/rjn.2019.1.2
13. Powell DS, Oh ES, Reed NS, Lin FR, Deal JA. Hearing loss and cognition: what we know and where we need to go. Front Aging Neurosci. 2022;13. doi:10.3389/fnagi.2021.769405
14. Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396(10248):413–446. doi:10.1016/s0140-6736(20)30367-6
15. Chadha S, Kamenov K, Cieza A. The world report on hearing, 2021. Bull World Health Organ. 2021;99(4):242–242A. doi:10.2471/blt.21.285643
16. Carlson ML, Nassiri AM, Marinelli JP, Lohse CM, Sydlowski SA. Awareness, perceptions, and literacy surrounding hearing loss and hearing rehabilitation among the adult population in the United States. Otol Neurotol. 2022;43(3):e323–e330. doi:10.1097/mao.0000000000003473
17. Sydlowski SA, Marinelli JP, Lohse CM, Carlson ML. Hearing health perceptions and literacy among primary healthcare providers in the United States: a National Cross-Sectional Survey. Otol Neurotol. 2022;43(8):894–899. doi:10.1097/mao.0000000000003616
18. Giannouli V, Tsolaki M. Self-awareness of cognitive efficiency, cognitive status, insight, and financial capacity in patients with Mild AD, aMCI, and healthy controls: an intriguing liaison with clinical implications? Neurol Int. 2022;14:628–637. doi:10.3390/neurolint14030051
19. Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982;17(1):37–49. doi:10.1016/0022-3956(82)90033-4
20. Brown PJ, Woods CM, Storandt M. Model stability of the 15-item Geriatric Depression Scale across cognitive impairment and severe depression. Psychol Aging. 2007;22(2):372–379. doi:10.1037/0882-7974.22.2.372
21. Weintraub S, Salmon D, Mercaldo N, et al. The Alzheimer’s Disease Centers’ Uniform Data Set (UDS). Alzheimer Dis Associated Disord. 2009;23(2):91–101. doi:10.1097/wad.0b013e318191c7dd
22. Morris JC. The Clinical Dementia Rating (CDR). Neurology. 1993;43(11):2412.2–2412–A. doi:10.1212/wnl.43.11.2412-A
23. Korsnes MS. Performance on the mini-mental state exam and the Montreal cognitive assessment in a sample of old age psychiatric patients. SAGE Open Med. 2020;8:2050312120957895. doi:10.1177/2050312120957895
24. Kaufer DI, Cummings JL, Ketchel P, et al. Validation of the NPI-Q, a brief clinical form of the neuropsychiatric inventory. JNP. 2000;12(2):233–239. doi:10.1176/jnp.12.2.233
25. Pfeffer RI, Kurosaki TT, Harrah CH, Chance JM, Filos S. Measurement of functional activities in older adults in the community. J Gerontol. 1982;37(3):323–329. doi:10.1093/geronj/37.3.323
26. Beekly DL, Ramos EM, Lee WW, et al. The National Alzheimer’s Coordinating Center (NACC) database: the uniform data set. Alzheimer Dis Associated Disord. 2007;21(3):249–258. doi:10.1097/wad.0b013e318142774e
27. Gurgel RK, Jackler RK, Dobie RA, Popelka GR. A new standardized format for reporting hearing outcome in clinical trials. Otolaryngol Head Neck Surg. 2012;147(5):803–807. doi:10.1177/0194599812458401
28. Gurgel RK, Popelka GR, Oghalai JS, Blevins NH, Chang KW, Jackler RK. Is it valid to calculate the 3‐kilohertz threshold by averaging 2 and 4 Kilohertz? Otolaryngol Head Neck Surg. 2012;147(1):102–104. doi:10.1177/0194599812437156
29. Clark JG. Uses and abuses of hearing loss classification. ASHA. 1981;23(7):493–500.
30. Olsen WO, Van Tasell DJ, Speaks CE. Phoneme and word recognition for words in isolation and in sentences. Ear Hear. 1997;18(3):175–188. doi:10.1097/00003446-199706000-00001
31. Hirsh I, Davis H, Silverman S, Reynolds E, Eldert E, Benson R. Development of materials for speech audiometry. J Speech Hear Disord. 1952;17(3):321–337. doi:10.1044/jshd.1703.321
32. Tillman TW, Carhart R. An expanded test for speech discrimination utilizing CNC monosyllabic words. Northwestern University Auditory Test No. 6. SAM-TR-66-55. Tech Rep SAM-TR. 1966;1–12. doi:10.21236/ad0639638
33. Humes LE, Busey TA, Craig J, Kewley-Port D. Are age-related changes in cognitive function driven by age-related changes in sensory processing? Atten Percept Psychophys. 2012;75(3):508–524. doi:10.3758/s13414-012-0406-9
34. Lindenberger U, Baltes PB. Sensory functioning and intelligence in old age: a strong connection. Psychol Aging. 1994;9(3):339–355. doi:10.1037/0882-7974.9.3.339
35. Blajovan M-D, Arnăutu D-A, Malița D-C, Tomescu M-C, Faur C, Arnăutu S-F. Fall risk in elderly with insomnia in Western Romania—a retrospective cross-sectional study. Medicina. 2023;59(4):718. doi:10.3390/medicina59040718
36. Pichora-Fuller MK, Kramer SE, Eckert MA, et al. Hearing impairment and cognitive energy: the Framework for Understanding Effortful Listening (FUEL). Ear Hear. 2016;37(1):5S–27S. doi:10.1097/aud.0000000000000312
37. Lin FR, Ferrucci L, An Y, et al. Association of hearing impairment with brain volume changes in older adults. NeuroImage. 2014;90:84–92. doi:10.1016/j.neuroimage.2013.12.059
38. Whillans J, Nazroo J, Matthews K. Trajectories of vision in older people: the role of age and social position. Eur J Ageing. 2016;13(2):171–184. doi:10.1007/s10433-015-0360-1
39. van Boxtel MPJ, ten Tusscher MPM, Metsemakers JFM, Willems B, Jolles J. Visual determinants of reduced performance on the stroop color-word test in normal aging individuals. J Clin Exper Neuropsychol. 2001;23(5):620–627. doi:10.1076/jcen.23.5.620.1245
40. Deal JA, Sharrett AR, Albert MS, et al. Hearing impairment and cognitive decline: a pilot study conducted within the atherosclerosis risk in Communities Neurocognitive Study. Am jo epidemiol. 2015;181(9):680–690. doi:10.1093/aje/kwu333
41. Dupuis K, Pichora-Fuller MK, Chasteen AL, Marchuk V, Singh G, Smith SL. Effects of hearing and vision impairments on the Montreal Cognitive Assessment. Aging Neuropsychol Cognit. 2014;22(4):413–437. doi:10.1080/13825585.2014.968084
42. Hong T, Mitchell P, Burlutsky G, Liew G, Wang JJ. Visual impairment, hearing loss and cognitive function in an older population: longitudinal findings from the blue mountains eye study. PLoS One. 2016;11(1):e0147646. doi:10.1371/journal.pone.0147646
43. van Hooren SAH, Anteunis LJC, Valentijn SAM, et al. Does cognitive function in older adults with hearing impairment improve by hearing aid use? Int J Audiol. 2005;44(5):265–271. doi:10.1080/14992020500060370
44. Albers MW, Gilmore GC, Kaye J, et al. At the interface of sensory and motor dysfunctions and Alzheimer’s disease. Alzheimer’s Dementia. 2014;11(1):70–98. doi:10.1016/j.jalz.2014.04.514
45. Thomson RS, Auduong P, Miller AT, Gurgel RK. Hearing loss as a risk factor for dementia: a systematic review. Laryngoscope Invest Otolaryngol. 2017;2(2):69–79. doi:10.1002/lio2.65
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.