Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
eHealth for people with COPD in the Netherlands: a scoping review
Authors Hallensleben C ![]() , van Luenen S
, van Luenen S ![]() , Rolink E, Ossebaard HC
, Rolink E, Ossebaard HC ![]() , Chavannes NH
, Chavannes NH ![]()
Received 1 March 2019
Accepted for publication 17 May 2019
Published 26 July 2019 Volume 2019:14 Pages 1681—1690
DOI https://doi.org/10.2147/COPD.S207187
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Cynthia Hallensleben,1,* Sanne van Luenen,1,* Emiel Rolink,2 Hans C Ossebaard,3,4 Niels H Chavannes1
1Department of Public Health and Primary Care, Leiden University Medical Center, Leiden, the Netherlands; 2Lung Alliance Netherlands, Amersfoort, the Netherlands; 3National Health Care Institute, Diemen, the Netherlands; 4Department of Medical Informatics, Amsterdam UMC, Amsterdam, the Netherlands
*These authors contributed equally to this work
Background: In the Netherlands, almost 600,000 people had chronic obstructive pulmonary disease (COPD) in 2017. This decreases quality of life for many and each year, COPD leads to approximately 6,800 deaths and about one billion health care expenditures. It is expected that eHealth may improve access to care and reduce costs. However, there is no conclusive scientific evidence available of the added value of eHealth in COPD care. We conducted a scoping review into the use of eHealth in Dutch COPD care. The aim of the research was to provide an overview of all eHealth applications used in Dutch COPD care and to assess these applications on a number of relevant criteria.
Methods: In order to make an overview of all eHealth applications aimed at COPD patients in the Netherlands, literature was searched in the electronic databases PubMed and Google Scholar. In addition, Dutch health care websites were searched for applications that have been evaluated for effectiveness and reliability. The identified eHealth applications were assessed according to five relevant quality criteria, eg, whether research has been conducted on the effectiveness.
Results: Thirteen health care programs and patient platforms in COPD care have been found that use eHealth. In addition, 13 self-care and informative websites and 15 mobile apps were found that are available to citizens and patients. Five of 13 care programs and patient platforms were found to be effective in improving quality of life or reducing hospital admissions in small pilot studies. The effectiveness of these and the other eHealth applications should be established in larger studies in the future.
Discussion: More research into the effectiveness of eHealth applications for COPD patients is needed. We recommend to develop a nationwide open source platform where well-evaluated eHealth applications can be showcased for patients and health care providers to improve COPD care.
Keywords: COPD, eHealth, care programs, scoping review
Introduction
In 2017, almost 600.000 people had chronic obstructive pulmonary disease (COPD) in the Netherlands.1 Having COPD may reduce the quality of life and the burden of disease is high.2,3 In addition, health care costs related to COPD were estimated to be around €1 billion in the Netherlands in 2015.1
Self-management may be important to improve well-being and quality of life of COPD patients, for example, by reducing exacerbations.4 eHealth may be promising to improve self-management and health outcomes in people with somatic diseases, including COPD.5,6 eHealth can be defined as the use of new information and communication technologies, in particular Internet technology, to support or improve health and health care.7 Using eHealth applications in the care for patients with COPD is attractive because the number of patients is growing and this puts pressure on the quality, accessibility, and affordability of (COPD) care.8 eHealth may reduce this pressure by making health care accessible from home or other places, affordable by decreasing costs, while the quality remains high when the effectiveness is established in research.
Meta-analyses and reviews have been conducted to investigate the effectiveness of eHealth interventions in COPD care outside the Netherlands. Most studies were conducted into telehealth, in which telecommunications and virtual technology are used to provide health care outside health care institutions.9 A meta-review by Hanlon et al (2017)10 summarized the evidence of eight previous reviews on the effectiveness of telehealth interventions for people with COPD. They concluded that no effect of telehealth was found on mortality and improved health outcomes. Sul et al (2018)11 found similar results in their meta-analysis on telemonitoring. The results of another meta-analysis indicated that physical activity improved after telehealth, but no effect on dyspnea was found.12 A meta-analysis of 10 studies into telecare for COPD13 showed a decrease in the number of emergency room visits and hospital admissions, compared with control groups receiving regular care. However, no effect was found of telecare on quality of life. In recent reviews, also no effect on quality of life was found,14 nor are there any negative effects of the use of telecare programs.10 More research into this topic is needed, as results are not consistent and mostly telehealth was investigated in these studies.
Previous studies also examined for which COPD patients eHealth may be most effective. A recent review of the effect of telemedicine for COPD15 shows that the programs with the most effective outcomes target elderly patients with severe COPD. Patients with frequent exacerbations and comorbidity may also benefit more. Furthermore, larger effects of telemedicine are found when patients live further away from regular care or have a limited social network and therefore have limited access to care. Although most studies have been conducted in the group of older patients with COPD, there is also evidence that COPD patients who are younger than 60 years may be the most cost-effective group.16
Many eHealth applications for COPD patients have been developed in the Netherlands. However, an overview of these applications and their scientific validation are, as far as we know, lacking. This study provides an overview of all eHealth applications used in Dutch COPD care. In addition, the applications were assessed on a number of quality criteria, such as available scientific evidence of the effectiveness on quality of life.
Methods
Search strategy and selection of eHealth applications
Several strategies have been used to search for eHealth applications. First, the electronic databases PubMed and Google Scholar have been searched. We used the search terms COPD, eHealth, digital care, digital care program, telemedicine, telecare, telemonitoring, and teleconsultation. Second, the references of “Playbook The future of care requires action” (Playbook De Toekomst van de zorg vraagt om actie)17 and the digital care guide COPD (digitale zorggids COPD)18 were searched for eHealth applications. Third, the websites of Trimbos institute19 (quit smoking) and GGD Appstore20 (quit smoking, adherence to therapy and informative apps) were used for the selection of informative apps. These two organizations recommend apps that were proven to be effective and reliable by the organizations. Last, we used the snowball method to find eHealth applications, in which the references in one article are the source for finding other relevant articles. We searched for articles and eHealth applications in March and April 2018.
An inclusion criterion for an eHealth application for the review was that it should be a digital application for COPD patients within Dutch health care. eHealth applications that were included were health care programs, patient platforms, (self-) care websites, informative websites, and mobile apps. Teleconsultation and telemonitoring were included (eg, teleconsultation was often a part of health care programs), but telerehabilitation was not included. We will use the term eHealth applications as an umbrella term. If no information was provided by the owners of an application, the application was not included in the study. No restrictions regarding publication year were applied and articles in Dutch or English were included in the review.
Assessment criteria
The included eHealth applications have been evaluated according to the criteria described below. Health care programs and patient platforms were assessed on all criteria. Most websites and apps were available for everyone, so not specifically for COPD patients. Therefore, the websites and apps could not be evaluated on all criteria. For example, it was not possible to evaluate the availability in primary and secondary health care for most websites and apps. Websites and apps that did not specifically target COPD patients may provide accessible and useful information that can support self-management. Therefore, they are included in this scoping review. In Table 1, the criteria and scoring are described in more detail.
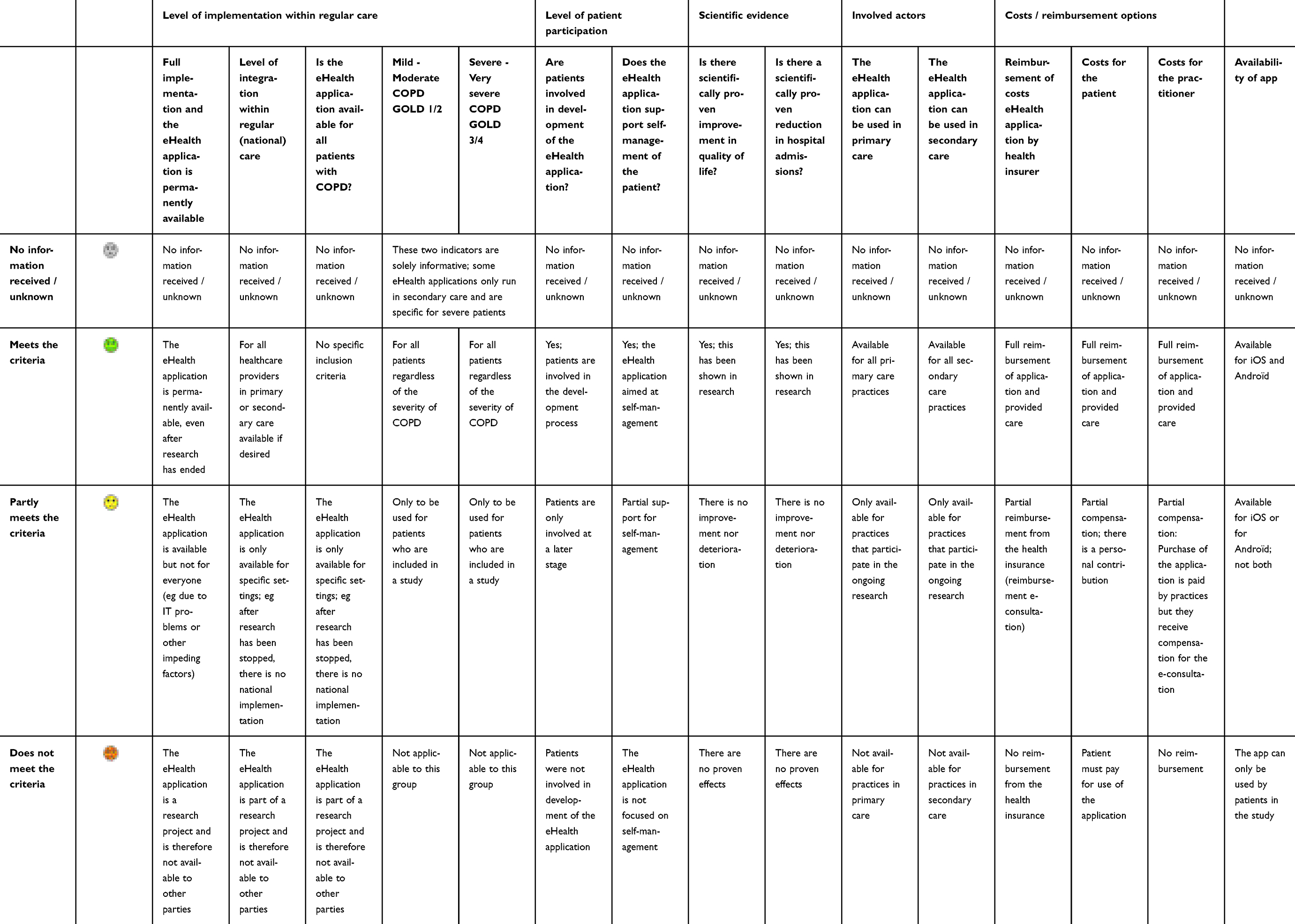 |
Table 1 Overview of assessment criteria and scoring |
Integration into routine (national) care
This criterion involves the availability of the eHealth application for all COPD patients or for a specific group of patients. An application can only be available during a research period or it can be permanently implemented and thus accessible to a large group of patients. In the former case, this is usually for a limited group of patients and there is a chance that the application will no longer be used after the study has ended.
Involvement of patients in the development of the eHealth application
This criterion concerns the extent to which patients were involved in the development of the eHealth application. When this so-called co-creation is applied, the wishes and needs of users are taken into account in the development. Implementation of eHealth applications could then be more successful.21
Effectiveness on improving quality of life and reducing hospital admissions
It has been examined whether research has been conducted that shows that the eHealth application improves the quality of life of patients or that a reduction in the number of hospital admissions was found.
Availability in primary and secondary health care
In this criterion, the extent to which the eHealth application is available for all general practitioners and pulmonologists/hospitals was examined. Some applications are only available for some health care professionals in primary or secondary health care, eg, because of an investigation. Other applications are only available for either primary or secondary health care, making cooperation between both difficult.
Costs of the eHealth application
We assessed whether the patient and care provider had to pay for using the eHealth application. It was also investigated whether the use of the application is covered by the health care package or otherwise reimbursed by the health insurer.
Procedure
One author searched for articles and eHealth applications and screened them on eligibility. All owners of the identified eHealth applications were approached by e-mail with the request to participate in the study. Questions were asked regarding the assessment criteria (eg, integration into routine care and costs of the application). When parties did not respond to the first email, reminders were sent. The information received (mostly in writing, sometimes by telephone when owners requested this) were collected in an Excel database. Subsequently, each eHealth application in the database was assessed on each criterion with a green, yellow, red, or gray smiley. A green smiley means that the application met the criterion, a yellow smiley means that the criterion was partially met, a red smiley means that the criterion was not met, and a gray smiley means that there was not enough information to assess this criterion. In the end, there was an overall assessment for each eHealth application based on the number of green, yellow, red, and gray smileys. For example, when most criteria of an eHealth application received a green smiley, the overall assessment was also a green smiley.
The assessment was carried out independently by two assessors. In case of disagreement, the assessment was discussed. All disagreements could be solved this way, no third assessor was needed. No verification of the received information was conducted. We did not assign weighting to the different assessment criteria because of the nature of this scoping review.
Results
Included applications
A total of 47 eHealth applications were found that met the inclusion criteria. The owners of two care programs and four informative applications have not provided data. One of them stated no information could be provided because of the ongoing scientific research into their application. The other five parties did not respond to repeated requests for information. The 41 resulting eHealth applications were divided into 13 care programs22–28 and patient platforms,29–34 13 informative eHealth applications,22,35–46 and 15 apps,35,37,42,46–57 which were assessed. The results of the assessment procedure will be described below and are included in Table 2.
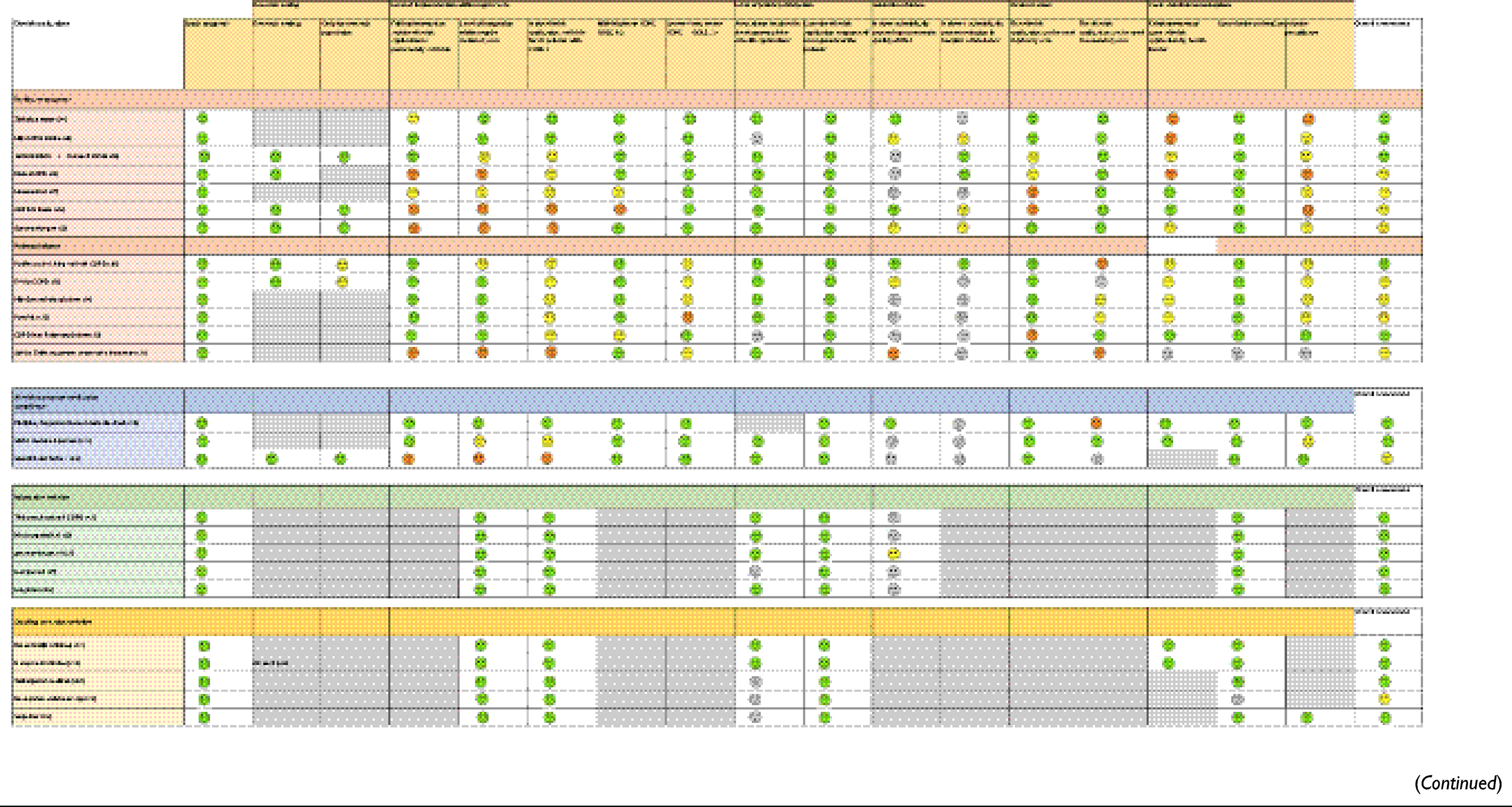 |
Table 2 Overview of eHealth applications and results of the assessment procedure |
Assessment of care programs and patient platforms
Five23–26,30 of 13 included care programs and patient platforms showed positive results in terms of improving quality of life or reducing hospital admissions based on small pilot studies. For most of the other programs and platforms, no information was available about the effectiveness (yet). In addition, the long-term effectiveness of the programs and platforms was not studied up to now.
The number of users of the different programs and platforms ranges from 2033 to 2000.41 Costs of the programs and platforms are usually not for the patient (12 out of 13 programs, 1 unclear31), but often for the care provider (11 out of 13, 1 unclear,31 1 without costs for the care provider32). This mainly concerns the development costs of a program or platform or the purchase thereof.
Care programs
All care programs except one24 are still part of ongoing research, mainly situated in secondary health care. This implies that especially patients with severe COPD which are treated by the pulmonologist are eligible for these eHealth care programs. Only three22,24,28 of the seven care programs could be used in both primary care and secondary care. In the future, care programs may become more and more accessible to patients with a milder disease course and the cost-effectiveness compared to usual care may be more likely then. One program was found to be effective in improving quality of life and perceived quality of care compared to usual care in a randomized controlled trial (RCT), and it is used in both primary and secondary health care.24
Patient platforms
The patient platforms focus mainly on implementation in primary care. The platforms that are linked to or are part of the chain information systems seem to have a greater scope than the platforms that are used alongside GP information systems.
Assessment of self-care and informative websites
The self-care and informative websites that (partially) focus on patients with COPD are divided into three websites to promote medication adherence,35,40,41 five informative websites,22,36,37,39,42 and five websites focused on smoking cessation.38,43–46 For the majority of the various self-care and informative websites, there is no link with existing programs and no treatment relation between the patient and the care provider is necessary. The scientific evidence for the effectiveness of these applications is limited or completely absent. The uptake depends on the accessibility, advertising, and recommendation by individual care providers.
Two informative sites, although not integrated in care or chain programs, have an increasing uptake in primary care based on scientific effectiveness on quality of life22 and health care usage.42 However, one of these sites42 is not only focused on COPD but on other diseases as well. The study does not show the effectiveness of the website specifically for people with COPD. Only one informative site22 is publicly accessible, but also linked to one of the care programs. This program is part of a study and there are no results about the effectiveness of the program yet.
Two informative websites/self-care applications for smoking cessation44,45 have been found where research into the effectiveness has been conducted. However, the effectiveness of the applications has been established for the general public or for specific groups; there is no evidence of the applications specifically for COPD patients.58,59 There are usually no costs for the patient for using self-care and informative websites.
Assessment of eHealth apps
Fifteen apps were found that focused on COPD care, medication adherence, smoking cessation, and information about COPD-related topics. The results of the assessment of apps are almost similar to the results of the assessment of self-care and informative websites. Six apps were found to be effective,42,46,47,51,52,56 and most apps are available for all COPD patients and can be accessed via iOS and Android and are free for patients.
Discussion
This study provides an overview of eHealth applications used in COPD care in the Netherlands. Thirteen health care programs and patient platforms have been found. In addition, 13 self-care and informative websites and 15 mobile apps were found that are available to citizens and patients. Five of the 13 care programs and patient platforms were scientifically investigated in small pilot studies, and positive effects were found on improving quality of life or reducing hospital admissions for COPD patients. No evidence is available about the effectiveness of the other care programs and patient platforms yet, but research is ongoing for most of them. As self-care and informative websites and eHealth apps are available to everyone, the effectiveness of these applications specifically for COPD patients was not established yet. There are usually no costs for using the applications for patients. However, often care providers have to pay the development or purchase of a care program or patient platform.
As far as we know, this was the first review that summarized eHealth applications for COPD patients in the Netherlands. In previous research outside the Netherlands, mostly telehealth was studied and the results regarding the effectiveness were mixed.10–14 This review adds other eHealth applications than telehealth and applications that are used and studied in the Netherlands. The effectiveness of many eHealth applications included in this review was not investigated yet. Therefore, more research in primary and secondary care is needed to draw any conclusions about the effectiveness of eHealth applications for COPD care in the Netherlands.
Despite the limited evidence of the effectiveness for eHealth in primary COPD care, it appears that a large proportion of general practitioners in the Netherlands offer or intend to offer eHealth services.60 The patient platforms we found focus primarily on implementation in primary care and thus meet a demand from the field. The programs that are linked to or are part of the chain information systems seem to have a greater scope than the programs that have to be used separately in addition to the general practice information system. Therefore, we recommend to implement promising eHealth applications for COPD patients in primary care while studying their effectiveness.
Some limitations of this review should be mentioned. First, the study is a scoping review, which is by definition less comprehensive than a systematic review. Second, the search was conducted by one person (author CH), instead of two independent persons. Third, the owners of six eHealth applications did not provide data and therefore could not be included in the review. Fourth, most of the self-care and informative websites and eHealth apps are not specifically for COPD patients. Therefore, they could not be assessed on all criteria. Fifth, the included eHealth applications were quite diverse in terms of both purpose and form. Therefore, it was difficult to compare them on the assessment criteria.
For future research, we recommend to investigate the long-term effects of eHealth applications for COPD patients, in addition to the short-term effects. Furthermore, the effectiveness of different eHealth applications may be studied in the future to find out which applications are the most effective. Thereafter, the implementation of the most effective applications may be facilitated in Dutch COPD care. We also recommend to improve collaboration between primary and secondary care. Most care programs are used in secondary care and most patient platforms are used in primary care. It would be valuable when this could be more integrated in order to improve care for COPD patients. Additionally, it may be relevant to conduct the current review also in other countries to enable international comparison. It may also be relevant to investigate which COPD patients use eHealth applications and which patients do not use it and why. Lastly, it is necessary to develop a nationwide open source platform for effective eHealth applications. This platform could possibly be modularly arranged to make links with other diseases. Well-evaluated eHealth applications can be displayed and found in this way by patients and health care providers.
Conclusions
We can conclude that there are 47 eHealth applications used in Dutch COPD care. Five of the 13 care programs and patient platforms were found to be effective in improving quality of life or reducing hospital admissions in small pilot studies. More research into the effectiveness of eHealth applications is needed. Furthermore, usually patients do not have to pay for the use of these eHealth applications. However, the costs for care providers to develop or purchase care programs or patient platforms may be considerable, which is a barrier for implementation.
Abbreviations list
COPD, Chronic Obstructive Pulmonary Disease; GGD, Gemeentelijke Gezondheidsdienst (municipal health service); GP, general practitioner; RCT, randomized controlled trial.
Acknowledgments
The study was funded by the National Health Care Institute (Zorginstituut Nederland). The sponsor contributed to the design of the study and the drafting of the paper.
Disclosure
The authors work in research or practice with some of the included eHealth applications (E-Vita COPD, SARA, ziektelastmeter, Thuisarts, mijn luchtpunt 2, MonitAir). The present study was commissioned and funded by the National Health Care Institute, an independent government body. It's outcomes will be used for collaborative, multistakeholder efforts to improve lung care in the Netherlands. Dr Hans C Ossebaard is an employee of the National Health Care Institute. Miss Sanne van Luenen conducts a study (mijnluchtpunt.nl) with Boehringer Ingelheim outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. RIVM. COPD. 2017. Available from: https://www.volksgezondheidenzorg.info/onderwerp/copd. Accessed April 1, 2019.
2. Halpin DM, Miravitlles M. Chronic obstructive pulmonary disease: the disease and its burden to society. Proc Am Thorac Soc. 2006;3(7):619–623. doi:10.1513/pats.200603-093SS
3. Joshi M, Joshi A, Bartter T. Symptom burden in chronic obstructive pulmonary disease and cancer. Curr Opin Pulm Med. 2012;18(2):97–103. doi:10.1097/MCP.0b013e32834fa84c
4. Bentsen SB, Langeland E, Holm AL. Evaluation of self‐management interventions for chronic obstructive pulmonary disease. J Nurs Manag. 2012;20(6):802–813. doi:10.1111/j.1365-2834.2012.01469.x
5. Elbert NJ, van Os-Medendorp H, van Renselaar W, et al. Effectiveness and cost-effectiveness of ehealth interventions in somatic diseases: a systematic review of systematic reviews and meta-analyses. J Med Internet Res. 2014;16(4). doi:10.2196/jmir.2790
6. Lorig KR, Ritter PL, Laurent DD, Plant K. Internet-based chronic disease self-management: a randomized trial. Med Care. 2006;44:964–971.
7. Eng TR. The eHealth Landscape: A Terrain Map of Emerging Information and Communication Technologies in Health and Health Care. Princeton, NJ: The Robert Wood Johnson Foundation; 2001.
8. Minsterie Volksgezondheid Welzijn en Sport (Ministry of Health Welfare and Sport). Kamerbrief over voortgang e-health en zorgvernieuwing (Letter to Parliament about the progress of e-health and care innovation). 2018. Avaialble from: https://www.rijksoverheid.nl/documenten/kamerstukken/2018/05/18/kamerbrief-over-voortgang-e-health-en-zorgvernieuwing. Accessed April 1, 2019.
9. WHO. Telehealth. Available from: https://www.who.int/sustainable-development/health-sector/strategies/telehealth/en/. Accessed April 1, 2019.
10. Hanlon P, Daines L, Campbell C, McKinstry B, Weller D, Pinnock H. Telehealth interventions to support self-management of long-term conditions: a systematic metareview of diabetes, heart failure, asthma, chronic obstructive pulmonary disease, and cancer. J Med Internet Res. 2017;19(5):e172. doi:10.2196/jmir.6688
11. Sul A-R, Lyu D-H, Park D-A. Effectiveness of telemonitoring versus usual care for chronic obstructive pulmonary disease: a systematic review and meta-analysis. J Telemed Telecare. Epub 2018 Dec 12.
12. Lundell S, Holmner Å, Rehn B, Nyberg A, Wadell K. Telehealthcare in COPD: a systematic review and meta-analysis on physical outcomes and dyspnea. Respir Med. 2015;109(1):11–26. doi:10.1016/j.rmed.2014.10.008
13. McLean S, Nurmatov U, Liu JL, Pagliari C, Car J, Sheikh A. Telehealthcare for chronic obstructive pulmonary disease: Cochrane Review and meta-analysis. Br J Gen Pract. 2012;62(604):e739–e749. doi:10.3399/bjgp12X658269
14. Gregersen TL, Green A, Frausing E, Ringbæk T, Brøndum E, Ulrik CS. Do telemedical interventions improve quality of life in patients with COPD? A systematic review. Int J Chron Obstruct Pulmon Dis. 2016;11:809.
15. Vitacca M, Montini A, Comini L. How will telemedicine change clinical practice in chronic obstructive pulmonary disease? Ther Adv Respir Dis. 2018;12:1753465818754778. doi:10.1177/1753465818754778
16. Udsen FW, Lilholt PH, Hejlesen OK, Ehlers LH. Subgroup analysis of telehealthcare for patients with chronic obstructive pulmonary disease: the cluster-randomized Danish Telecare North Trial. ClinicoEcon Outcomes Res. 2017;9:391. doi:10.2147/CEOR.S139064
17. Breteler M, de Neef R, Dohmen D. Playbook De Toekomst van de zorg vraagt om actie [The Future of Care Requires Action]. Driebergen: Menzis en Focus Cura; 2018.
18. Patiëntenfederatie Nederland. COPD apps en websites. 2019. Available from: https://www.digitalezorggids.nl/aandoeningen/copd. Accessed April 1, 2019.
19. Trimbos Institute. Trimbos Institute. 2019. Available from: www.trimbos.org. Accessed April 1, 2019.
20. GGD. GGD appstore. 2019. Available from: www.GGDAppstore.nl. Accessed April 1, 2019.
21. van Limburg M, Wentzel J, Sanderman R, van Gemert-Pijnen L. Business modeling to implement an eHealth portal for infection control: a reflection on co-creation with stakeholders. JMIR Res Protoc. 2015;4(3):e104. doi:10.2196/resprot.4519
22. Gezonde longen. Available from: https://www.gezonde-longen.nl/.
23. Medicine Men. Emma COPD. Available from: https://www.medicinemen.eu/nl/emmacopd/.
24. Slok AH, Kotz D, van Breukelen G, et al. Effectiveness of the Assessment of Burden of COPD (ABC) tool on health-related quality of life in patients with COPD: a cluster randomised controlled trial in primary and hospital care. BMJ Open. 2016;6(7):e011519. doi:10.1136/bmjopen-2016-011519
25. Trappenburg JC, Niesink A, de Weert-van Oene GH, et al. Effects of telemonitoring in patients with chronic obstructive pulmonary disease. Telemed e-Health. 2008;14(2):138–146. doi:10.1089/tmj.2007.0037
26. van der Burg J, Aziz NA, Kaptein M, et al. Long-Term Effects of Telemonitoring on Healthcare Usage in Patients with Heart Failure or COPD (Preprint). 2018.
27. van't Hul AJ, Frouws S, van den Akker E, et al. Decreased physical activity in adults with bronchial asthma. Respir Med. 2016;114:72-77. doi:10.1016/j.rmed.2016.03.016
28. Van Noort E, Kasteleyn M, Mennema B, Chavannes N. Selfmanagement by eHealth in Asthma and COPD Patients: With or without the Professional. European Respiratory Journal. 2017;50:suppl 61. doi:10.1183/1393003.congress-2017.PA1606.
29. Portavita. Portavita. Available from: https://nl.portavita.com/.
30. Bischoff EW, Akkermans R, Bourbeau J, van Weel C, Vercoulen JH, Schermer TR. Comprehensive self management and routine monitoring in chronic obstructive pulmonary disease patients in general practice: randomised controlled trial. BMJ. 2012;345:e7642. doi:10.1136/bmj.e7642
31. Eikelenboom N, van Lieshout J, Jacobs A, et al. Effectiveness of personalised support for self-management in primary care: a cluster randomised controlled trial. Br J Gen Pract. 2016;66(646):e354–e361. doi:10.3399/bjgp16X684985
32. Radboud UMC. COPD Net/Patientenplatform. Available from: https://www.picassozorgoptimalisatie.nl/kennis-delen/nieuws/2014/12/09/copd-net-échte-integrale-benadering-van-de-patiënt/.
33. Talboom-Kamp EP, Verdijk NA, Kasteleyn MJ, et al. The effect of integration of self-management web platforms on health status in chronic obstructive pulmonary disease management in primary care (e-vita study): interrupted time series design. J Med Internet Res. 2017;19(8):e291. doi:10.2196/jmir.8262
34. Zorgverzekeraar CZ. Mijn Gezondheidsplatform. Available from: http://www.mijngezondheidsplatform.info/media/74e9a8ab-cbb4-446c-8130-12a6b93f0542/VrWGQQ/PDF/NRC120324_8.pdf.
35. Smartinhaler Turbu+. Available from: nice.org.uk/guidance/mib90.
36. Longforum. Available from: https://www.longforum.nl/categories/copd-algemeen.
37. Boehringer Ingelheim. Luchtpunt.nl. Available from: https://www.luchtpunt.nl/copd/.
38. Jellinek. Zelfhulptabak (Jellinek). Available from: https://www.jellinek.nl/informatie-over-alcohol-drugs/tabak/.
39. Long Alliantie Nederland. Inhalatorgebruik.nl. Available from: https://inhalatorgebruik.nl/nl/home.
40. Pluriplus. Pluriplus, Zorgstraat/Nexus Medicatie check. Available from: https://www.pluriplus.nl/nexus-medicatie-check/.
41. Service Apotheek. SARA (Service Apotheek). Available from: http://www.de-eerstelijns.nl/wp-content/uploads/2018/09/DEL-nr6_2018_Service-Apotheken-SARA_LR.pdf.
42. Spoelman WA, Bonten TN, de Waal MW, et al. Effect of an evidence-based website on healthcare usage: an interrupted time-series study. BMJ Open. 2016;6(11):e013166. doi:10.1136/bmjopen-2016-013166
43. STIVORO, Stichting Stop Bewust. De stopsite/website en app. Available from: https://www.destopsite.nl/.
44. Trimbos Institute. Roken infolijn (trimbos). Available from: https://www.rokeninfo.nl/publiek/contactinformatie.
45. Trimbos Institute. ik stop nu.nl (trimbos). Available from: https://www.ikstopnu.nl/.
46. Trimbos Institute. Stoptober. Available from: https://www.rokeninfo.nl/professionals/stoptober.
47. Medapp. Available from: https://medapp.nu/professionals.
48. Quit smoking Buddy. Available from: https://play.google.com/store/apps/details?id=nl.hqmedia.quitsmokingbuddyfree&hl=nl.
49. Rookvrij pro. Available from: https://itunes.apple.com/nl/app/rookvrij-pro/id409605521?mt=8
50. Boer LM, van der Heijden M, van Kuijk NM, et al. Validation of ACCESS: an automated tool to support self-management of COPD exacerbations. Int J Chron Obstruct Pulmon Dis. 2018;13:3255. doi:10.2147/COPD.S167272
51. GGZ Friesland. Medalert. Available from: https://play.google.com/store/apps/details?id=nl.freed.medalert&hl=nl.
52. Koninklijke Nederlandse Maatschappij ter bevordering der Pharmacie (KNMP). Apotheek.nl. Available from: https://www.apotheek.nl/medicijnen.
53. Medisafe. Medisafe medicatieherinnering. Available from: https://play.google.com/store/apps/details?id=com.medisafe.android.client.
54. Novartis. Volari. Available from: https://www.novartis.nl/news/media-releases/nieuwe-gebruiksvriendelijke-volari-app-voor-en-door-mensen-met-copd.
55. RIVM. Ik heb nu last. Available from: https://magazines.rivm.nl/2015/10/rivm-magazine/app-ik-heb-nu-last-creatief-maatwerk-voor-luchtweg-pati%C3%ABnten.
56. RIVM, Rijnmond DM, Amsterdam G, Limburg OM-eWBeP, Milieu MvI. mijnluchtkwaliteit. Available from: https://www.rivm.nl/nieuws/nieuwe-app-mijn-luchtkwaliteit-gelanceerd.
57. Trimbos Institute. Quitnow! Available from: https://www.rokeninfo.nl/professionals/stoppen-met-roken1/gevolgen-vanstoppen.
58. Mujcic A, Blankers M, Boon B, Engels R, van Laar M. Internet-based self-help smoking cessation and alcohol moderation interventions for cancer survivors: a study protocol of two RCTs. BMC Cancer. 2018;18(1):364. doi:10.1186/s12885-018-4242-8
59. Scheffers-van Schayck T, Otten R, Engels R, Kleinjan M. Evaluation and implementation of a proactive telephone smoking cessation counseling for parents: A study protocol of an effectiveness implementation hybrid design. Int J Environ Res Public Health. 2018;15(1):97. doi:10.3390/ijerph15061188
60. Peeters JM, Krijgsman JW, Brabers AE, De Jong JD, Friele RD. Use and uptake of eHealth in general practice: a cross-sectional survey and focus group study among health care users and general practitioners. JMIR Med Inform. 2016;4(2). doi:10.2196/medinform.5853
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.