")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Egyptian Society of Liver Cancer Recommendation Guidelines for the Management of Hepatocellular Carcinoma
Authors Omar A, Kaseb A, Elbaz T, El-Kassas M , El Fouly A, Hanno AF, El Dorry A, Hosni A, Helmy A, Saad AS, Alolayan A, Eysa BE, Hamada E, Azim H, Khattab H, Elghazaly H, Tawfik H, Ayoub H, Khaled H , Saadeldin I, Waked I , Barakat EMF , El Meteini M, Hamed Shaaban M, EzzElarab M, Fathy M, Shaker M, Sobhi M, Shaker MK , ElGharib M, Abdullah M, Mokhtar M, Elshazli M, Heikal OMK, Hetta O, ElWakil RM, Abdel Wahab S, Eid SS, Rostom Y
Received 26 March 2023
Accepted for publication 1 September 2023
Published 18 September 2023 Volume 2023:10 Pages 1547—1571
DOI https://doi.org/10.2147/JHC.S404424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Gerber
Ashraf Omar,1 Ahmed Kaseb,2 Tamer Elbaz,1 Mohamed El-Kassas,3 Amr El Fouly,3 Abdel Fatah Hanno,4 Ahmed El Dorry,5 Ahmed Hosni,6 Amr Helmy,7 Amr S Saad,8 Ashwaq Alolayan,9 Basem Elsayed Eysa,10 Emad Hamada,11 Hamdy Azim,11 Hany Khattab,12 Hesham Elghazaly,8 Hesham Tawfik,13 Hisham Ayoub,14 Hussein Khaled,11 Ibtessam Saadeldin,11 Imam Waked,15 Eman MF Barakat,16 Mahmoud El Meteini,17 Mohamed Hamed Shaaban,6 Mohamed EzzElarab,10 Mohamed Fathy,17 Mohamed Shaker,5 Mohamed Sobhi,5 Mohamed Kamal Shaker,16 Mohamed ElGharib,5 Mohammed Abdullah,11 Mohesn Mokhtar,11 Mostafa Elshazli,18 Omar Mohamed Khaleil Heikal,14 Osama Hetta,5 Reda Mahmoud ElWakil,16 Sameh Abdel Wahab,5 Samir Shehata Eid,19 Yousri Rostom20 On behalf of the Egyptian Liver Cancer Committee Study Group
1Department of Gastroenterology, Faculty of Medicine, Cairo University, Cairo, Egypt; 2Department of Gastrointestinal Medical Oncology, the University of Texas MD Anderson Cancer Center, Houston, TX, USA; 3Department of Endemic Medicine, Faculty of Medicine, Helwan University, Cairo, Egypt; 4Department of Gastroenterology, Faculty of Medicine, Alexandria University, Alexandria, Egypt; 5Department of Interventional Radiology, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 6Department of Interventional Radiology, Faculty of Medicine, Cairo University, Cairo, Egypt; 7Department of Surgery, National Liver Institute Menoufia University, Menoufia, Egypt; 8Department of Oncology, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 9Department of Oncology, National Guard Hospital, Riyadh, Saudi Arabia; 10Department of Gastroenterology, National Hepatology and Tropical Medicine Research Institute, Cairo, Egypt; 11Department of Oncology, Faculty of Medicine, Cairo University, Cairo, Egypt; 12Department of Pathology, Faculty of Medicine, Cairo University, Cairo, Egypt; 13Department of Oncology, Faculty of Medicine, Tanta University, Tanta Egypt; 14Department of Gastroenterology, Military Medical Academy, Cairo, Egypt; 15Department of Gastroenterology, Menoufia Liver Institute, Menoufia, Egypt; 16Department of Gastroenterology, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 17Department of Surgery, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 18Department of Surgery, Faculty of Medicine, Cairo University, Cairo, Egypt; 19Department of Oncology, Faculty of Medicine, Assiut University, Assiut, Egypt; 20Department of Oncology, Faculty of Medicine, Alexandria University, Alexandria, Egypt
Correspondence: Ashraf Omar, Department of Gastroenterology, Faculty of Medicine, Cairo University, Cairo, Egypt, Email [email protected]
Abstract: Globally, hepatocellular carcinoma (HCC) is the fourth most common cause of death from cancer. The prevalence of this pathology, which has been on the rise in the last 30 years, has been predicted to continue increasing. HCC is the most common cause of cancer-related morbidity and mortality in Egypt and is also the most common cancer in males. Chronic liver diseases, including chronic hepatitis C, which is a primary health concern in Egypt, are considered major risk factors for HCC. However, HCC surveillance is recommended for patients with chronic hepatitis B virus (HBV) and liver cirrhosis; those above 40 with HBV but without cirrhosis; individuals with hepatitis D co-infection or a family history of HCC; and Nonalcoholic fatty liver disease (NAFLD) patients exhibiting significant fibrosis or cirrhosis. Several international guidelines aid physicians in the management of HCC. However, the availability and cost of diagnostic modalities and treatment options vary from one country to another. Therefore, the current guidelines aim to standardize the management of HCC in Egypt. The recommendations presented in this report represent the current management strategy at HCC treatment centers in Egypt. Recommendations were developed by an expert panel consisting of hepatologists, oncologists, gastroenterologists, surgeons, pathologists, and radiologists working under the umbrella of the Egyptian Society of Liver Cancer. The recommendations, which are based on the currently available local diagnostic aids and treatments in the country, include recommendations for future prospects.
Keywords: hepatocellular carcinoma, clinical recommendations, Egyptian society of liver cancer, hepatitis c virus, Egypt, guidelines
Corrigendum for this paper has been published.
Introduction
Globally, the prevalence of hepatocellular carcinoma (HCC), which is the fourth most common cause of cancer-related death, has been increasing over the last 30 years.1 In 2018, the number of deaths caused by HCC worldwide was reported to be 781,631, which is higher than the 746,000 deaths reported in 2012.2 Furthermore, in 2020, HCC was reported to be the most common cancer type in Egypt and the leading cause of mortality among all cancers, causing more than 26,000 deaths.3 The incidence of HCC is on the rise due to the increase in the number of screening programs and the prolonged survival rate of patients with liver cirrhosis and nonalcoholic steatohepatitis (NASH).4 Chronic liver diseases, which are a primary health concern in Egypt, are associated with high economic costs, a high disease burden, and poor prognoses, including HCC development.1 In 2008, the estimated seroprevalence of the hepatitis C virus (HCV) in people aged 15–59 years was 14.7%, and this value was reduced to approximately 10% in 2015.5,6 In 2019, the estimated HCV seroprevalence dropped to 4.6% among people aged above 18 years.1 This significant decrease in the seroprevalence of HCV resulted from the immense efforts of the Egyptian government in screening almost 60 million Egyptians and treating more than 2 million patients infected with the virus. In 2020, the “100 Million Healthy Lives” campaign attained its objectives, making Egypt the first country in the world to reach the World Health Organization (WHO) HCV elimination target of reducing the HCV-related mortality rate by 65% and the incidence of the infection by 90%.7 This success story is believed to be an essential strategy in decreasing the incidence of HCC in Egypt as a secondary preventive approach.7
Regarding hepatitis B virus (HBV), A meta-analysis spanning from 1983 to 2002, which incorporated 13 Egyptian studies, suggested a 6.7% HBV prevalence in healthy individuals and 25.9% among those with HCC.8 The 2015 Egyptian Health Issues Survey (EHIS) demonstrated that the estimated prevalence of HBV was 1% based on HBsAg seroprevalence from a sample of 26,047 healthy individuals aged 1–59 years and 1.56% in a subgroup of 16,003 participants aged 15–59 years.9 The most recent meta-analysis reported a consolidated national prevalence of 3.67%. Notably, children below 20 years, who were vaccinated against HBV in their infancy, exhibited the lowest prevalence at 0.69%. Specific groups showed varied prevalence: pregnant women at 2.95%, blood donors at 1.8%, and healthcare workers at 1.1%. Furthermore, when assessing gender differences, HBV prevalence was higher in males (3.75%) compared to females (2.2%). Overall, the trend indicates a decreasing prevalence of HBV in Egypt over the years.10
In 2015, an observational study involving 154 physicians from Egypt reported that 93% of physicians aged >45 years and 75% of physicians aged <45 years depended on guidelines when managing patients with HCC.11 The study also demonstrated that 71% of physicians in the Ministry of Health (MOH) were not aware of the existence of any guidelines (local or international) due to a lack of awareness or limited interest, as per the authors.11,12 The current diagnosis and treatment of HCC in the country are in line with the existing international guidelines such as those of the European Association for the Study of Liver (EASL), the American Association for the Study of Liver Diseases (AASLD), and the Japan Society of Hepatology (JSH). However, the treatment options, in terms of availability, cost, and variation of the patient population, are limited in Egypt. There is also a paucity of available data on HCC in Egypt compared to other countries available worldwide, the high prevalence of the disease notwithstanding.
This document aims to provide recommendations to standardize the management of patients with HCC in Egypt based on the currently available evidence. The recommendations are developed under the umbrella of the Egyptian Society of Liver Cancer (ESLC). The guidelines define the use of surveillance, diagnosis, and therapeutic strategies recommended for these patients. Users of these guidelines should be aware that the recommendations are intended to guide clinical practice in situations where all the required resources and therapies are available.
Methodology
The guidelines development team consisted of a group of Egyptian experts in different specialties working in the field of HCC, including 16 hepatologists, 12 Oncologists, 8 interventional radiologists, one pathologist, and 4 liver and transplant surgeons from 11 different centers. All panelists have more than 20 years of experience in HCC management in their relevant fields. Experts with different HCC management experience levels were selected equally to minimize the bias toward interventional-dominated opinions. Each panelist is either an active board member of an academic society working in HCC, a member of the HCC multidisciplinary team in a recognized institution, someone who contributed to guidelines development on this subject, or someone who published scientific manuscripts on HCC management. Even though all panelists are of academic background, they fairly represent Egypt’s governmental and private healthcare sectors. The panel identified, prioritized, and selected relevant topics on which a comprehensive literature search was performed. A literature search was conducted on Medline via PubMed from January 2015 to October 2021 to collect relevant information. The following search terms were used in combinations: ((carcinoma, hepatocellular [MeSH Terms]) OR (liver neoplasms [MeSH Terms])) AND ((population surveillance [MeSH Terms])) OR (diagnosis [MeSH Terms])) OR (neoplasm staging [MeSH Terms])) AND (disease management [MeSH Terms])) AND ((Egypt [MeSH Terms])) AND ((guideline [MeSH Terms]) OR (practice guideline [MeSH Terms])). Initially, the titles and abstracts of the retrieved records were screened, followed by full texts of the publications that addressed the guideline objectives. A manual search of the references of retrieved publications was also conducted. Besides, the last version of HCC management guidelines of major international societies, including the AASLD, EASL, JSH, and Asia Pacific Association for the Study of Liver (APASL), were referred to for additional statements.
The clinical practice guidelines methodology was used to agree on the recommendations. All experts voted on the recommendations in two consensus meetings held in December 2021. The level of evidence (LOE) of the retrieved statements was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach (Table 1).13 The statements were primarily extracted from studies with high-quality evidence. Additional statements were retrieved from studies with lower-quality evidence whenever deemed necessary by the committee. Forty-one statements were developed, clustered, and distributed according to the defined working groups, including surveillance and epidemiology, diagnosis and risk assessment, early and advanced disease management, and follow-up. Statements with a voting percentage of 75% or more were considered “consensus reached”, which was observed to be 95% (39/41). Additionally, areas of future research were identified to guide future prospective clinical trials. All the consented recommendations are presented in Table 2.
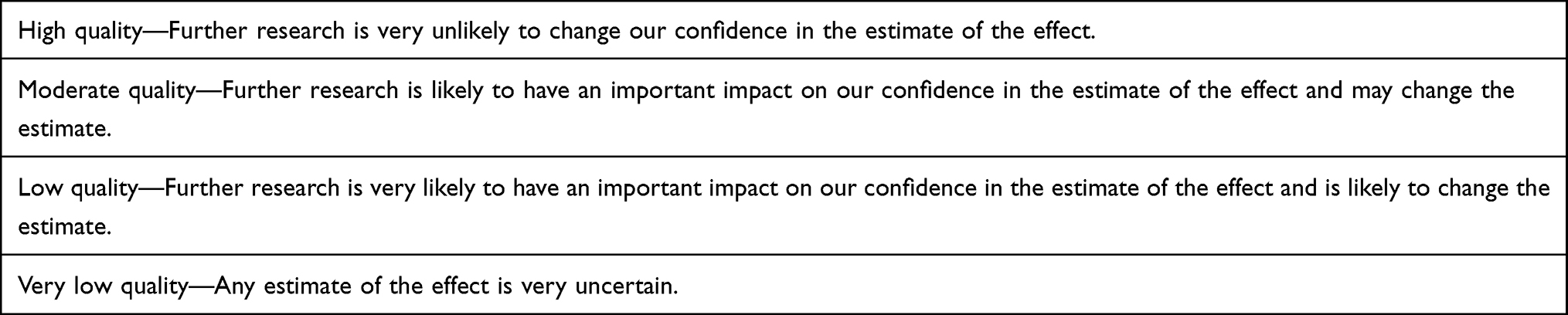 |
Table 1 Quality of Evidence and Definitions |
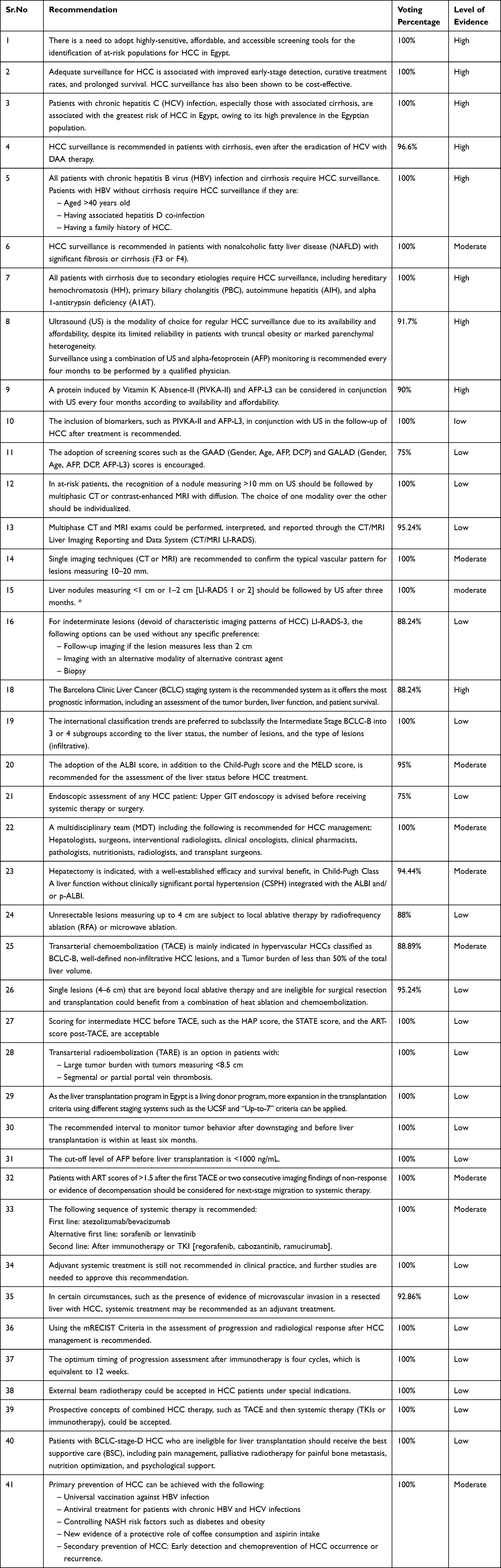 |
Table 2 Consensus on HCC Management in Egypt |
Discussion
Screening and Surveillance for HCC
Significance of HCC Surveillance in Egypt
Consensus Statements
The panel unanimously agreed (100%) on the need to adopt highly-sensitive, affordable, and accessible screening tools to identify populations predisposed to HCC in Egypt. The experts highlighted the change in HCC epidemiology worldwide and emphasized the significance of HCC screening and the selection of the right patients for screening. A meta-analysis and several local studies support the need for surveillance, proving that HCC surveillance is associated with a better prognosis and significant improvement in early tumor detection, receipt of curative therapies, and overall survival.9,11 Early diagnosis can provide curative treatment options such as transplantation, surgical resection, and percutaneous ablation, which are not possible if the disease is detected at an advanced stage.14,15 HCC surveillance with either AFP and US or multiphasic multidetector CT is economical, with a cost-effectiveness ratio of less than 50,000 USD quality-adjusted life year compared to no surveillance.15 Accordingly, all panel experts (100%) agreed that HCC surveillance is cost-effective and associated with improved early-stage detection, high curative treatment rates, and prolonged survival.
The experts unanimously (100%) agreed that patients with chronic hepatitis C (HCV) infection, especially those with associated liver cirrhosis, are more predisposed to HCC than anyone else in Egypt, owing to its high prevalence in the Egyptian population. The panel members highlighted the fact that patients approaching the age at which they are at risk of developing HCC could be the reason for the increase in the proportion of HCC patients with HCV in Egypt, even after appropriate treatment is administered. However, some panelists believed that the rising incidence rate was expected to reduce in two or three decades. Previous studies reported that the incidence rates of HCV in Egypt were constantly rising, with an estimated increase of 14% in the general population.12 HCV infection promotes liver fibrosis and cirrhosis, indirectly leading to the development of HCC. HCV also induces liver cell proliferation through viral gene products resulting in hepatic carcinogenesis.16 The AASLD guidelines highlighted the fact that patients with HCV-associated liver cirrhosis have a 3.5% annual rate of HCC development.17 The risk of HCC in patients with chronic HCV infection is 15–20 times higher than that in patients without HCV infection.15
In 2018, the Egyptian MOH initiated a national screening campaign to contain the high HCV incidence in the country by 2020, following which a direct-acting antiviral (DAA) sofosbuvir-based regimen was provided to all the screened individuals with confirmed HCV infection.18 Many studies showed conflicting results regarding the outcome of DAA treatment and HCC recurrence exit.19,20 Given the previous prevalence of HCV and HCC in Egypt, the national HCV treatment program proved the impact of screening and the efficiency of DAA agents in HCV treatment.1 A majority of the panel members (96.6%) recommended HCC surveillance in patients with cirrhosis post-DAA therapy, even after HCV eradication. The experts highlighted the importance of screening for HCC at follow-up in patients who have received DAA therapy. Previous studies showed that DAAs are well-tolerated by HCV patients with advanced liver disease and could provide SVR rates >95%.15 However, some studies revealed that the incidence of de novo HCC in patients with HCV cirrhosis increased with the use of the DAA regimen, which may be attributed to the increasing age, severity of liver disease, and waitlist mortality in liver transplant patients.15,21 Most guidelines recommended close surveillance in patients with HCV-associated cirrhosis even after DAA therapy and an evaluation of the benefit of viral cure against the recurrence risk.15,22 The panel members suggested that Egyptian patients with cirrhosis treated with DAA are advised to be followed up every four months. The mandatory screening of patients prior to the initiation of treatment with DAA was suggested. The panelists also stressed the need to raise awareness among patients with cirrhosis to be regularly followed up after receiving DAA therapy.
The panel unanimously recommended that all patients with chronic hepatitis B virus (HBV) infection and liver cirrhosis require HCC surveillance. However, patients with HBV without cirrhosis require HCC surveillance only if they are above 40 years of age, have the hepatitis D co-infection, or have a family history of HCC. All HCC experts recommended surveillance in patients with nonalcoholic fatty liver disease (NAFLD) with significant fibrosis or cirrhosis (F3 or F4). The panel recognized the impact of HBV on HCC development, considering that HBV was associated with 88% of histologic cirrhosis worldwide, most of which developed into HCC.23 The literature demonstrates the direct impact of HBV on the pathogenesis of HCC and its integration into the host’s DNA.24,25 Although the prevalence of HBV infection is declining in Egypt due to the universal hepatitis B vaccination program, this infection is considered a higher risk for HCC than HCV.25 A single-center Egyptian study found that HBsAg positivity was an independent risk factor for HCC owing to a two-fold increase in HCC development.26 Another study found a shift in the risk factor influence between HCV and HBV over a decade; however, the risk of HCC development associated with HBV infection remained higher than that associated with HCV infection during the study period.25 In Egypt, the seroprevalence of the hepatitis D virus (HDV) was estimated to be 3.4% in the Nile Delta region.27 However, the prevalence of HCC among people co-infected with HBV and HDV was comparable, ranging from 8.8% to 13.6%.27,28 International and local studies suggest that a family history of liver cancer is a significant risk factor for HCC development.29,30 A study by Velazquez reported that the risk of developing HCC in cirrhotic patients above 54 years of age is four times higher than that in younger patients.31 An Egyptian single-center study demonstrated that cirrhotic patients aged 40–59 years are 3.7 times more likely to develop HCC than others.25
The panel members (100%) stated that HCC surveillance is essential in patients with secondary etiologies of cirrhosis, including hereditary hemochromatosis (HH), primary biliary cholangitis (PBC), autoimmune hepatitis (AIH), and alpha 1-antitrypsin deficiency (A1AT). This statement was supported by the AASLD guidelines that recommended HCC surveillance in patients with HH and PBC.32 In Egypt, several studies have reported the association of HCC in HCV patients carrying hemochromatosis gene (HFE) mutant alleles, such as the A allele at position 346 of the ghrelin gene or the D allele of the H63D mutation.33,34 However, other studies failed to prove the impact of HFE mutations on the risk of HCC in cirrhotic patients.35 A study conducted in Sweden reported that patients with HH have a 20 times higher risk for HCC without an increased risk for non-hepatic malignancies.36 According to the current literature, cirrhosis secondary to PBC increases the risk of HCC occurrence at a level similar to that observed in patients with HCV infection.37 Although AIH is associated with a significantly lower risk of HCC development compared to other chronic liver diseases,38 patients with cirrhosis secondary to AIH showed an annual incidence rate of >1.5%, resulting in the need to include such patients in routine HCC surveillance programs.39 Another study added that HCC occurs in 7% of patients with AIH and cirrhosis of at least a five-year duration, with an incidence rate of 1 per 350 patients-years.40 Further, a retrospective study revealed that patients with cirrhosis secondary to A1AT deficiency show a 0.88% annual incidence of HCC,41 which justifies the need for surveillance in such patients. The prevalence of A1AT deficiency in the Egyptian population is not well defined; however, a previous Egyptian study on 100 HCC patients did not prove a significant association between the A1AT mutation and the incidence of HCC.33
Modes of HCC Surveillance
Consensus Statements
The majority of the panel members (92%) recommended US imaging as the modality of choice for regular HCC surveillance due to its availability and affordability, in spite of its limited reliability in patients with either truncal obesity or marked parenchymal heterogeneity. They recommended surveillance using US and alpha-fetoprotein (AFP) monitoring every four months (to be performed by a qualified physician). Several studies and existing international guidelines supported and recommended US as one of the primary, most effective, non-invasive, sensitive, and affordable imaging modalities for HCC surveillance.22,42–44 A meta-analysis of 32 studies showed that US had an overall sensitivity of 84% for detecting HCC at any stage and a sensitivity of 47% for the early detection of HCC.21,45 Another systematic review of 14 studies showed that the pooled estimate of the sensitivity of the US for HCC detection was 60%, and the specificity was 97%.21 Real-world data from a multicenter study of 374 patients revealed that 42% of the patients with HCC were diagnosed during screening, and the use of US for screening was associated with a higher rate of early tumor detection, a higher rate of curative treatment, and improved survival compared with HCC detected via techniques other than screening.46 An observational study conducted in Egypt reported that 74% of physicians from university hospitals and 46% of physicians from the MOH considered US the most important HCC screening test.11 The panelists advocate for the use of AFP, as the current literature proved it is one of the most widely used serological markers in HCC due to its affordability and availability. A plasma concentration of 20 ng/mL as a pathological threshold for diagnosis shows elevated levels of AFP in 60%–80% of hepatic cancers.21 US alone has a lower sensitivity for any-stage and early-stage HCC than when combined with AFP. AFP alone was reported to have low specificity, as elevated levels could be recorded in liver cirrhosis, chronic hepatitis, neurodegenerative diseases, and non-seminomatous testicular cancer. Therefore, a combination of both diagnostic tools was recommended.21 Previous studies in Egypt also supported the combined use of ultrasonography and AFP (≥ 200 ng/mL) monitoring for the diagnosis of HCC.25 A study conducted in Egypt on 514 patients with chronic HCV infection proved that the combination of AFP monitoring and ultrasonography could improve HCC surveillance.30 The study highly recommended a national surveillance program for the detection of HCC in cirrhotic HCV Egyptian patients by combining AFP monitoring and ultrasonography.30
The panelists stressed the use of quality equipment and qualified physicians to perform ultrasound imaging. This recommendation was based on the current literature demonstrating that multiple factors, such as the screening frequency, the physician’s experience, and the patient’s disease status, are known to determine the effectiveness of ultrasonography.45 A study in the USA revealed that US sensitivity ranged between 35% and 84% depending on the equipment used and the operator’s expertise.21 A study conducted in Egypt reported that the accuracy of US is highly dependent on the operator’s ability to discriminate HCC from non-neoplastic lesions (regenerative nodules),30 therefore, the panelists emphasized the importance of using trained personnel to perform ultrasonography and obtain accurate results. International societies, including the AASLD, EASL, and APASL, recommended surveillance for adults with cirrhosis and high-risk patients without cirrhosis using US with or without AFP at six-month intervals. The surveillance interval is decided according to the patient’s clinical status, available resources, and affordability.14,15 Studies have shown that performing surveillance every six months increases the sensitivity for detecting early-stage HCC to 70%.14 Considering the increasing prevalence of HCC and its associated risk factors in Egypt, the panelists recommended a surveillance interval of four months.45
Diagnosis, Staging, and Risk Assessment
Laboratory Diagnosis
Consensus Statements
There was a 90% agreement among the panel members that proteins induced by Vitamin K Absence-II (PIVKA-II) and AFP-L3 can be considered in conjunction with US every four months, depending on the availability and affordability. Some experts suggested that PIVKA-II and AFP-L3 are more sensitive yet expensive than AFP; however, some panelists referred to them as cost-effective. Most experts stated that their use would depend on their availability in the country. The literature supports the statement stating that AFP, the AFP-L3 fraction, and PIVKA-II/DCP are the three primary tumor markers for HCC with recommended cut-off values of 10 ng/mL, 10%, and 40 mAU/mL, respectively.45 A study conducted among patients with Child-Pugh classes A and B revealed that a combination of AFP monitoring and ultrasonography increased the sensitivity in detecting early-stage HCC from 32% to 65%.14
The AASLD and EASL guidelines do not recommend AFP alone as a screening test due to its relatively inadequate sensitivity and specificity for surveillance, low positive predictive value, and inadequate accuracy for early-stage HCC.12,22 However, the KLCA-NCC and APASL surveillance recommendations support AFP use with US.47 Thus, AFP and US may play complementary roles once combined. The efficiency of the surveillance method varies as per the onset and incidence of HCC in the region.47 A previous study recommended an AFP threshold of 400 ng/mL as a suitable cut-off level for detecting HCC, regardless of its combination with ultrasonography. However, there was no correlation between elevated serum AFP levels and the tumor size or number in the previous study conducted in Egypt.30
All (100%) panelists agreed on the inclusion of biomarkers such as PIVKA-II and AFP-L3 in conjunction with US in the follow-up of HCC after treatment considering the fact that currently, AFP-L3 is approved by the FDA for liver cancer assessment as part of the GALAD score (a tool to address the heterogeneity in biology among the etiologies of cirrhosis).14,21 According to the experts, the biomarkers (PIVKA-II and AFP-L3) are prognostic tools. AFP is known to have low specificity and can be elevated in non-HCC conditions. As mentioned earlier, AFP-L3 (the lens culinaris agglutinin-reactive fraction of AFP) demonstrated superior diagnostic efficacy in HCC.48,49 A previous study reported that elevated AFP-L3 levels could predict early HCC even in the absence of elevated AFP.50 A study carried out on 80 Egyptian patients evaluating the role of AFP-L3 as a biomarker revealed that AFP-L3 had a higher sensitivity than AFP and could serve as a diagnostic biomarker for detecting early-stage HCC.51
PIVKA-II has been an accepted biomarker for HCC surveillance and is currently included in evidence-based Japanese and APASL clinical guidelines.45 In a study conducted in Egypt on 83 patients, PIVKA-II was highly sensitive, specific, and superior to AFP monitoring in the early detection of HCC patients. It also demonstrated the ability to differentiate between the histopathological grades of HCC, evaluate the thrombosis of the portal vein, and categorize the early and late stages of HCC.52 A pilot study conducted in Europe concluded that the PIVKA-II could be added to the routine panel of HCC tumor markers as it achieved better sensitivity than AFP.53 Another study conducted in Egypt on 441 HCC patients at a hospital concluded that with abnormal AFP levels (≥ 400 ng/mL), the serum AFP level remains useful, whereas AFP-L3 is more specific than AFP in the diagnosis of HCC using AFP levels (<400 ng/mL).54
Some panelists (75%) encouraged the adoption of screening scores such as GAAD (Gender, Age, AFP, DCP) and GALAD (Gender, Age, AFP, DCP, AFP-L3). However, some (17.39%) experts did not agree and highlighted the need for additional studies to identify the optimum score and validate the tools to be used in the early detection of HCC. This recommendation was based on the results of several international studies demonstrating that a combination of biomarkers is possibly the best tool for HCC detection. Multiple studies support the use of the GALAD score, which the FDA approved for the early detection of HCC in March 2020.55,56 A study conducted in Europe demonstrated that the GALAD score outperforms the biomarkers AFP, DCP, and AFP-L3 used alone for the early-stage detection of HCC in Caucasian patients with chronic hepatitis B or C. The score displayed a robust performance in identifying HCC patients independent of the tumor burden, the extent of the liver disease, and the viral load.57 A study conducted in the United States demonstrated the superiority of the GALAD score compared to US and recommended its use in patients with advanced-stage hepatic dysfunction or obesity who are at risk of false-negative US findings.58 No specific studies on the use of these scores in the Egyptian population have been reported so far. The panelists recommended that additional prospective and observational studies on the validity of these scores to use in the early detection of HCC are essential.
Radiological Diagnosis
Consensus Statements
* Except for Hemangioma
Imaging techniques are crucial in managing patients with detected nodular hepatic lesions. All panelists (100%) recommended that in at-risk patients, the recognition of a nodule measuring >10 mm using US should be followed by multiphasic CT or contrast-enhanced MRI with diffusion as currently, all existing international guidelines recommended multiphase CT or MRI with extracellular contrast agents or hepatobiliary contrast agent (HBA)-enhanced MRI as first-line diagnostic imaging modalities for at-risk patients.47 Studies have shown that multiphase CT is suitable for HCC diagnosis because of its lower cost, faster imaging times, and lower technical complexity.59,60 The experts suggested using multiphasic CT and dynamic MRI with diffusion and strongly insisted that MRI is superior to CT when performed appropriately. Dynamic studies are essential to visualize the hemodynamic and histopathological characteristics of HCC and differentiate typical hypervascular HCC from other hypervascular benign lesions or false positives.47 The choice of imaging modality should be made after considering the clinical scenario, technical advantages, limitations, and local practices. So, the experts suggested that the choice of one technique over the other should be individualized.
Most experts (95.24%) recommended that multiphase CT and MRI exams could be performed, interpreted, and reported through the CT/MRI Liver Imaging Reporting and Data System (CT/MRI LI-RADS), as some studies demonstrated that CT/MRI LI-RADS for the diagnosis of HCC could be applied to multiphasic CT or MRI performed in patients with cirrhosis.29,61 Lesions are divided into eight distinctive LI-RADS categories reflecting the chances of HCC according to the presence or absence of primary features (non-rim APHE, non-peripheral portal venous or delayed-phase washout, enhanced capsule appearance, a size of at least 1 cm, threshold growth of more than 50% in less than six months), and additional factors.62
As diagnostic tools, MRI and CT have high sensitivity and specificity for HCC diagnosis.63–66 The current literature shows that MRI has sensitivity and specificity of over 90% each for lesions >2 cm, and for all-size lesions, its per-patient sensitivity and specificity are 88% and 94%, respectively.59,67 Studies have shown that CT/MRI images are attained for the differential diagnosis of US-detected lesions. The LR-1 and LR-2 category of LI-RADS includes simple cysts to distinctive nodules (<2cm) without any malignant features.62 The LI-RADS detection score designations help regulate the need for more frequent surveillance or additional imaging. For lesions measuring 10–20 mm, expert radiologists suggested the use of either CT or MRI; however, other panelists recommended using both techniques. Thus, all experts (100%) recommended the use of a single imaging technique (CT or MRI) to confirm the typical vascular pattern for lesions measuring 10–20 mm based on the available evidence and recommended approach of the LI-RADS for CT and MRI.62
The LI-RADS recommends US-based surveillance in LR-1 observations and CT-scan or MRI for lesions in the category of LR-2 as they are simple cysts with no major features favoring malignancy.62 All (100%) panelists recommended that liver nodules measuring either <1 cm or 1–2 cm (LI-RADS criteria 1 or 2) should be followed by US after three months. The LI-RADS 3 category includes lesions with an intermediate probability of HCC (38% HCC; 40% malignancy).62,64 The recommendation for managing such lesions is as per the multidisciplinary discussion. Most of the experts (88.24%) agreed that for such lesions, the approach to management would include follow-up imaging (if the lesion measures <2 cm), imaging with an alternative modality (of alternative contrast agent), and biopsy. There was no preference for any specific technique, as the clinical practice and tailored approach were the deciding factors. The LI-RADS can categorize and characterize abnormal liver lesions and enable the radiological diagnosis of HCC in patients with cirrhosis. However, liver biopsy is still recommended for diagnosis in patients without cirrhosis.62 Percutaneous liver biopsy can be considered when the diagnostic imaging results are unclear, including in patients with cirrhosis and nodules of hypovascular nature, as the AASLD and EASL guidelines support liver biopsy in the diagnosis of HCC.17,22,68
Staging and Assessment of HCC
Most panelists (88.24%) recommended using the Barcelona Clinic Liver Cancer (BCLC) staging system as it offers the most prognostic information, including an assessment of the tumor burden, liver function, and patient survival. It is widely and officially accepted by the EASL, AASLD, and other international societies69 and is reported to have the best correlation with patient outcomes.70 It includes four elements: tumor extension, liver functional reserve, physical status, and cancer-related symptoms. Its algorithm classifies HCC into five stages depending on the disease status, Child-Pugh score, and ECOG PS.68,69 Each stage in this system is allocated a treatment recommendation from the currently available options, distinguishing this staging system from the others. Various studies conducted in Egypt use the BCLC staging system for performing clinical studies.30,52 A study conducted in Egypt on 2000 patients revealed that BCLC was the best at discriminating the survival of patients in distinct stages and had the greatest homogeneity of survival among patients within the same stage, confirming that it is a good prognostic system.71 Several studies conducted in Italy and China revealed that the BCLC classification is the best predictive model for HCC patients receiving radical therapy, including percutaneous ablation or surgical resection.72–75 A trial conducted on 3892 HCC patients in Taiwan revealed that the treatment regimens determined by the BCLC classification are beneficial and reasonable for survival.76 The BCLC staging system also proved to be of significant prognostic value in HCC patients with early- to advanced-stage tumors treated with multiple modalities as per the investigations from Egypt, South Korea, Spain, Italy, and the USA.69 All studies show that the predictive accuracy of the BCLC classification is highly established and independent of the tumor stage, treatment modality, underlying liver disorder, and environmental differences.77
All panelists recommended sub-classifying the Intermediate Stage BCLC-B into three or four subgroups according to the liver status, the number of lesions, and the type of lesions (infiltrative) to facilitate treatment decisions associated with the heterogeneity of patients in this stage. Studies revealed that the subclassification of stage B into Stages B1–B4 was proposed by Bolondi (2013)78 in association with multiple first-line and alternative treatment options. The subclassification was also validated externally in a cohort of HCC patients in South Korea and Taiwan.79,80 In 2016, another subclassification of the BCLC-stage B into three sub-classes, as per the Child-Pugh score plus Milan and up-to-7 criteria, known as the “Kinki Criteria”, was reported.81
A majority of the panelists (95%) recommended the adoption of the ALBI score, the Child-Pugh score, and the MELD score for the assessment of liver status before HCC treatment. They emphasized the need to raise awareness of the use of the albumin/bilirubin (ALBI) score among the medical community. Some experts advocated that many clinical trials use only the Child-Pugh score to evaluate the liver status before treatment. The BCLC model of classification used the Child-Pugh score, and the MELD is an independent predictor of mortality in patients with HCC.81 The suggestion to use the ALBI score was based on the evidence from the literature confirming that the ALBI score is one of the standard measures to assess liver function in patients with HCC. It uses only objective parameters (albumin and total bilirubin) that assist in its superior evaluation, regardless of its complex calculation, which may limit its applicability.82 The ALBI score is calculated from the archived laboratory work-up using the following equation: ALBI score = (log10 bilirubin × 0.66) + (albumin × −0.085).83,84 The prognostic performance of the Child-Pugh-based BCLC is used to assess the hepatic reserve function along with the BCLC and ALBI grade is similar. A previous study revealed that the ALBI score is suitable for BCLC-B (intermediate-stage disease) cases to overcome survival heterogeneity.85 The modified intermediate liver cancer criteria (MICAN), a sub-grading for the BCLC-B using the ALBI score, has shown good ability over the other systems in the prognosis of BCLC-B patients, including those treated with transarterial chemoembolization (TACE).85
Most of the panelists (75%) recommended upper GIT endoscopy before systemic therapy or surgery for any HCC patient. Some physicians disagreed with the need for an endoscopic assessment prior to HCC therapy. Furthermore, some experts suggested endoscopic assessment only in patients who have not had a recent endoscopy prior to treatment. The panelists advocating endoscopic assessment before systemic therapy or surgery in HCC patients stated that endoscopy and the measurement of the portal vein tension are essential for treatment stratification. Previous studies reported gastrointestinal bleeding as an adverse effect of systemic therapies.86–89 Studies supporting endoscopic assessments prior to HCC treatment included case reports demonstrating the use of endoscopy in treating hard-to-reach HCC lesions.90,91 Hsu et al recommended upper endoscopy before systemic therapy in patients with cirrhosis (with or without portal hypertension) to assess the risk of variceal and non-variceal bleeding.92 Further research on the utility of endoscopy in the management of HCC is recommended.
Management of HCC
Multidisciplinary Teams in HCC
Consensus Statements
All (100%) panelists agreed that a multidisciplinary team (MDT) is essential for the management of HCC. HCC has diverse presentations that are compounded by the liver disease status, and multiple treatment options are available. An MDT composed of all specialists delivering different therapies can help improve patient outcomes. A balanced, individualized, and unbiased treatment selection is ensured when specialists from many different fields discuss the benefits and risks of the available treatment.93 Studies have shown that in HCC patients, the diagnosis, staging, and treatment selection are challenging and influenced by the increased prevalence, genetic heterogeneity, multiple etiologies, and concomitant chronic liver diseases.94 An MDT approach ensures that the disease is staged correctly and that the treatment recommendations are patient-centered, evidence-based, and arrived at by consensus. Several studies reveal that the multidisciplinary management of HCC patients improves survival and reduces disease-related mortality. A retrospective cohort study of newly diagnosed HCC patients revealed that the 5-year survival rate was significantly higher in patients managed by an MDT compared to those not managed by a team.94 A hospital-based prospective study conducted in Egypt demonstrated improved management of HCC through an MDT decision.95 According to the literature, an MDT should include hepatologists, medical and surgical oncologists, transplant surgeons, diagnostic and interventional radiologists, pathologists, radiation oncologists, nurses, supportive care specialists, and palliative physicians.96 All members play an essential and active role as their expertise is required to provide optimum care for HCC patients.
Resection and Ablation in HCC Treatment
The majority (94.44%) of the panelists recommended surgical resection in HCC patients with Child-Pugh Class A liver function without clinically significant portal hypertension integrated with ALBI and/or p-ALBI. Multiple studies and literature reviews indicate that in patients with adequate liver functional reserves, potentially curative hepatectomy is an optimal treatment option for HCC.68 Patients with a preserved liver function and HCC confined to the liver with no evidence of portal hypertension and the invasion of hepatic vasculature are ideal for surgical resection. Also, patients with Child-Pugh Class A cirrhosis, with normal bilirubin levels and well-preserved hepatic functions, can safely undergo hepatectomy. In selective HCC patients, relapse-free long-term survival rates (40%) and improved five-year survival rates (up to 90%) were reported.97 A study conducted in two Egyptian centers reported improved three-year survival rates with hepatectomy and concluded that it is an effective therapeutic tool in Child-A score HCC patients with well-compensated livers.98 The practice of resection in patients with significant portal hypertension is controversial, with portal hypertension in cirrhotic patients being considered a contraindication to surgical resection by some authors.99,100 The ALBI score could predict the risk of post-hepatectomy liver failure more accurately than the Child-Pugh scores in HCC patients after liver resection.101,102 The panelists advocated its integration into clinical practice. Several existing guidelines also recommend liver resection in well-compensated patients.22,32
The majority of panelists (88%) recommended that unresectable lesions measuring up to 4 cm be subjected to local ablative therapy by radiofrequency ablation (RFA) or microwave ablation (MWA), as several studies demonstrate the safety and efficacy of RFA and MWA in treating unresectable colorectal liver metastases near large vessels or major bile ducts. The safety and efficacy of RFA in unresectable hepatic lesions measuring less than 6 cm have been depicted by several studies, some of them reporting that the best outcomes are achieved in single tumors measuring <4 cm.93,103,104 RFA is considered a suitable treatment approach for unresectable lesions because of its efficacy, reproducibility, low complication rates, and availability. A cohort study and three independent meta-analyses, including five RCTs, advocate improved results, especially in patients with tumors measuring 2–5 cm in terms of local tumor control and survival benefits with RFA.105–108 Studies support the use of MWA as its benefits include an improved convection profile, higher constant intra-tumoral temperatures, faster ablation times, and the ability to use multiple probes for the simultaneous treatment of multiple lesions.103 MWA is generally preferred when the tumor measures ≥ 3 cm or if the nodule is closer to large vessels, independent of its size.103 Previous studies supported the use of MWA to treat unresectable HCC.109 A meta-analysis of seven RCTs concluded that both RFA and MWA have similar mortality, safety, and efficacy outcomes in treating HCC.110 However, a significant advantage of MWA over RFA is that the treatment outcome with MWA is not influenced by the tumor site.68,111 An RCT conducted in Egypt revealed no significant difference between outcomes obtained from RFA and MWA in HCC patients, except for the shorter time required for ablation.112
Trans-Arterial Chemo-Embolization (TACE) and Its Associated Combinations in HCC Treatment
TACE is recommended by a majority of the panelists (88.89%) in hypervascular HCCs classified as BCLC-B: well-defined non-infiltrative HCC lesions with a tumor burden of less than 50% of the total liver volume as several existing international guidelines, including the AASLD, ESMO, EASL, SAUDI, and INASL, recommend the use of TACE as the primary treatment option for BCLC-stage B HCC.15 The BCLC classification also recommends TACE for intermediate-stage HCC.113 Two randomized controlled trials114,115 and meta-analyses115,116 demonstrated the survival benefits of TACE in comparison to the best supportive care in patients with multinodular and/or large HCC, no cancer-related symptoms, and no evidence of vascular invasion or extrahepatic spread. Several studies and literature reviews conducted in Egypt also reported the use of TACE as the primary treatment in stage B patients, increasing the median survival of such patients to 20 months.93,117,118 A single-center study conducted on 221 patients with locally-advanced HCC treated with TACE in Egypt showed a median OS of 16 months and a median PFS of 6 months, demonstrating that TACE has good survival rates in such patients with noticeable toxicities. The study emphasized the appropriate selection of patients to improve outcomes with TACE.119
A majority (95.24%) of the panelists recommended that single lesions measuring 4–6 cm, beyond the local ablative therapy and unfit for surgical resection and transplant, could benefit from combined heat ablation with chemoembolization. Some studies revealed that in patients with HCC, a combination of TACE and RFA is associated with a significantly higher OS and recurrence-free survival than RFA monotherapy, especially in lesions measuring >3 cm.22 The literature also recommended that thermal ablation and TACE could be combined if the tumor size exceeds 5 cm, allowing for ablations of up to 6 cm with good response rates.113 A retrospective study conducted in Egypt on 22 patients ablated using TACE-RFA and 45 patients ablated with TACE-MWA, all with unresectable HCC lesions <5 cm and Child-Pugh Class A-B, demonstrated that the combination techniques are more effective with TACE-MWA showing a higher response rate than TACE-RFA in lesions measuring 3–5 cm. There was no significant difference in the survival rates between the two groups.120 Some experts suggested the addition of lesions measuring up to 8 cm; however, other panelists disagreed as there is insufficient evidence to support the use of the combination for such big lesions. The panelists agreed that in a combination treatment approach, chemoembolization needs to be done prior to ablation to reduce the size of the lesion. However, a combination of the two techniques may appear to be demanding in terms of resources.
The different scoring systems provide additional support in deciding if a patient is eligible for TACE and deciding the further course of treatment during TACE. The STATE (Selection for TrAnsarterial chemoembolization TrEatment) score and the HAP (Hepatoma Arterial-embolization Prognostic) score, with its modifications (mHAP-II and mHAP-III), have been specially devised to assist in deciding if treatment with TACE is suitable for a patient.113
The STATE score, which consists of serum albumin, tumor burden (up-to-7 criteria), and the CRP level, states that patients with lower scores have a significantly impaired median OS (5.3 months vs 19.5 months) and are not recommended to be treated with TACE.121 The HAP score includes AFP levels, tumor size, and serum levels of albumin and bilirubin. It categorizes patients into four subgroups, and the values of the individual factors help decide if the patient is eligible for treatment with TACE.122 The external validation of these two scores by some studies shows that they have a moderate ability to predict individual patients’ prognoses.123 A multicenter study concluded that the HAP score is best suited for screening patients prior to initial TACE.124 All panelists (100%) suggested using the STATE score and HAP score for stratification before TACE based on the relevant literature; however, they did not recommend basing clinical decisions on the scores alone.
A multivariate analysis125 investigated TACE repeated for a second or third time and identified three prognostic factors, which are an increase in the aspartate aminotransferase level by >25%, an increase in the Child-Pugh score, and the absence of tumor response. These factors were imbibed into an “ART” score, and patients with an ART score of 0–1.5 points were noted to be the ones who benefited most from a second TACE. Patients with a higher score of ≥ 2.5 showed significantly impaired survival and were associated with more adverse events after the second TACE treatment.125,126 A multicenter study concluded that the ART score is a validated prognostic score in patients with intermediate-stage HCC undergoing TACE and improves the early detection of chemoembolization failure.124 All panelists (100%) suggested using the ART score post-TACE based on the relevant literature.
Trans-Arterial Radio-Embolization (TARE) in HCC Treatment
TARE demonstrates a good safety profile and promising efficacy in disease control and involves using the selective intra-arterial administration of microspheres loaded with a radioactive compound such as yttrium-90.127 The ESMO defined TARE as a promising and suitable therapeutic option for patients with diffuse intrahepatic tumor spread or a “bridging” therapy.128 The NCCN recommends TARE for patients with liver-confined HCC who are not eligible for transplantation or resection.129 Studies involving selective patients with intermediate-stage HCC reveal that tumor shrinkage performed to reduce the disease burden and allow for resection or transplantation was better with TARE than with TACE.130,131 The current literature supports the downsizing of tumors in selected patients with a large disease and moderate residual liver volumes using TARE.127 Accordingly, all panelists (100%) recommended using TARE in patients with a large tumor burden beyond TACE procedures.
Previous studies demonstrated that treatment with TARE achieved an OS of up to 23.2 months in patients with portal vein thrombosis involving segmental or lobar branches, BCLC-stage C HCC.132,133 All panelists (100%) recommended the use of TARE in patients with segmental or partial portal vein thrombosis. Most experts agree that TARE is a cost-effective treatment and must be reserved for patients who are ineligible for TACE. A study conducted in Egypt was performed for ten months in two University Hospitals on 86 HCC patients using the conventional TACE with either doxorubicin or TARE Y-90 using glass microspheres. It revealed that in intermediate-stage HCC patients, both treatments resulted in similar survival probabilities despite more advanced disease in the TARE-Y 90 group of patients. The study concluded that patients in the TARE Y-90 group were associated with shorter hospitalization periods and fewer treatment sessions, and the treatment was well-tolerated.134
Liver Transplantation in HCC Treatment
Liver transplantation (LT) is the best treatment option for patients with decompensated cirrhosis. In HCC, LT allows for the removal of the primary tumor and treats hepatic insufficiency.135 Living donor transplantation is one of the strategies used to overcome the organ shortage in LT. More than 300 liver transplants have been performed annually from living donors in Egypt. The transplants from deceased donors are rare in the country despite the approval for the same by the Egyptian Parliament in 2010.136 LT is recommended as the first-line treatment option for HCC within the Milan criteria, which is a benchmark for selecting HCC patients eligible for LT. Patients with T2 stage criteria are considered eligible for LT, while those beyond this stage are considered only after a successful downstaging into the Milan criteria. The literature demonstrates that the UCSF criteria (single nodule ≤ 6.5 cm or 2–3 nodules ≤ 4.5 cm and a total diameter ≤ 8 cm),137,138 Up-to-7 criteria (Lesions with number 7 as the sum of the size (cm) of the largest tumor and the number of tumors)139 have non-significant differences compared to the Milan criteria in terms of post-LT-survival and have been externally validated.22 A review stated that it was ethically acceptable for LDLT to be offered to patients with tumors exceeding the Milan criteria.140 The evidence supports the recommendation by all the panelists (100%) that the expansion in transplantation criteria using different staging systems such as the UCSF and the “up-to-7” criteria can be applied to LT in Egypt.
In neoadjuvant treatments, downstaging is defined as the treatment applied to bring patients with a tumor burden outside the accepted criteria for transplantation within the acceptable criteria.141 Several studies accepted patients as LT candidates when their HCC was successfully down-staged to within the Milan criteria.142–144 The panelists suggested that the recommended interval to monitor tumor behavior after downstaging into the acceptance criteria is between 6–18 months. All panelists recommended a six-month monitoring interval after downstaging and before the LT, as 18 months was alleged to be a long time. Studies depict several AFP cut-off levels in the transplant criteria; however, there has been no common consensus in any existing guidelines on how to combine them with the structural characteristics of HCC. All panelists (100%) suggested an AFP cut-off level of <1000 ng/mL before transplantation based on their clinical practice. Some literature reviews and studies also supported using a cut-off level of <1000 ng/mL; however, more data are required.142,145 The experts also highlighted the need to study the impact of systemic therapy after downstaging and before LT to reduce the recurrence of the disease.
TACE Failure in HCC Treatment
The literature stated that the repeated application of TACE results in the emergence of new lesions, a consistent increase in the levels of tumor markers, and a gradual decrease in liver function with reduced tumor necrosis. Molecularly targeted therapies are now available, and the repetition of TACE can be avoided after TACE failure, which makes it essential to define it. The JSH first published the criteria for TACE failure in 2011 and 2014 and defined it as a failure to control the tumor in the target lesion or the appearance of new lesions after ≥ 2 consecutive TACE sessions.45 Other criteria defining TACE refractoriness include the Taiwan criteria and the International Expert Panel (EPOI HCC) Criteria (A. L. Cheng et al, 2014), which state that patients who need two or more TACE sessions within 6–12 months should be regarded as TACE failure and switched to molecularly targeted agents. The criteria proposed by Raoul (2014) also recommended switching to the next systemic treatment if there is no response after two TACE sessions.146 The definition of TACE failure is known to differ from one country to another. According to several studies, existing guidelines, and the current literature, intermediate-stage patients showing disease progression or poor tolerance after the first or second TACE should be migrated to systemic therapy, preferably Sorafenib,93,147,148 as it preserves the liver function and reduces the incidence of extrahepatic or vascular invasion.149–151 Based on the available evidence on the importance of recognizing TACE failure and considering the next available treatment in patients with TACE refractoriness, and the earlier recommendation of using the ART score post-TACE to determine whether or not the patient can benefit from a subsequent TACE, all panelists (100%) recommended that patients with an ART score of >1.5 after the first TACE or two consecutive imaging findings of non-response or evidence of decompensation should be considered for next-stage migration to systemic therapy.
Systemic Therapy in HCC Treatment
All panelists (100%) recommended the following sequence of systemic therapy for HCC: First-line treatment with atezolizumab/bevacizumab or sorafenib or lenvatinib; second-line treatment after immunotherapy or with TKIs such as regorafenib, cabozantinib, and ramucirumab.
The Phase 3 IMbrave-150 trial showed that patients with unresectable HCC had better OS and PFS with atezolizumab/bevacizumab than with sorafenib. The one-year OS was 67.2% (95% CI, 61.3–73.1) with atezolizumab/bevacizumab compared to 54.6% (95% CI, 45.2–64.0) with sorafenib. The median PFS values were 6.8 months (95% CI, 5.7–8.3) and 4.3 months (95% CI, 4.0–5.6), respectively. The JSH guidelines recommended a combination of atezolizumab plus bevacizumab as first-line treatment for unresectable advanced HCCs that cannot undergo surgical resection, loco-regional therapy, LT, or TACE in patients with Child-Pugh A (good PS and liver function) based on positive results from the IMbrave-150 trial.152 The ESMO guidelines state that atezolizumab plus bevacizumab showed superiority to sorafenib in terms of efficacy in patients with advanced HCC. It was recommended as the standard of care in the first-line therapy of patients with advanced HCC and approved by the EMA in 2020.153
Another LOE was available for sorafenib (a multi-tyrosine kinase inhibitor, TKI) as an alternative first-line treatment for advanced-stage HCC, being the first drug to be approved in 2007.22,45,68,154 The highly acclaimed SHARP study (OS 10.7 months with sorafenib vs 7.9 months with placebo) and the Asia Pacific study (OS 6.5 months with sorafenib vs 4.2 months with placebo) led to the approval of sorafenib as the first-line treatment of patients with Childs A cirrhosis and unresectable or metastatic HCC.155–157 The EASL guidelines recommended sorafenib for advanced tumors, BCLC-stage C, or tumors progressing despite loco-regional therapies. It recommended maintaining sorafenib therapy until radiographic progression is observed and, later, second-line treatment with regorafenib.22 Previous studies also demonstrated that sorafenib is of greater benefit in HCC patients with underlying HCV infection compared to HBV infection.158
The REFLECT trial comparing lenvatinib (a multi-tyrosine kinase inhibitor) to sorafenib in the first-line therapy of unresectable HCC showed that lenvatinib was non-inferior to sorafenib in terms of OS.159 The results demonstrate that lenvatinib provides clinically significant benefits to patients with a well-preserved liver function (Child-Pugh A class), good performance status, advanced tumors, BCLC-C without main portal vein invasion, or biliary ducts invasion or >50% liver occupation by tumors or tumors unsuitable for or progressing despite loco-regional therapies.159 Several existing guidelines recommend using lenvatinib in the first-line treatment setting.22,153 However, the JSH clinical practice guidelines for HCC 2017160 recommended sorafenib or lenvatinib as second-line therapy for Child-Pugh Class A patients who fail treatment with first-line therapy due to intolerable side effects or radiographic progression.45
Regorafenib was reported to be effective as a second-line agent for prolonging survival in patients with HCC who tolerated sorafenib by the RESORCE trial.161 Ramucirumab was approved in June 2019 to treat HCC in patients with an AFP level of ≥ 400 ng/mL based on results from the REACH-2 study.162 According to the study of Llovet et al, who conducted a pooled analysis of the REACH II study, ramucirumab survival benefit in patients with very aggressive HCC (AFP ≥ 400 ng/mL) was (HR: 0.64; 95% CI: 0.49–0.84) and in nonviral advanced HCC, it was (HR: 0.56; 95% CI: 0.40–0.79).
Cabozantinib was approved based on the results of the CELESTIAL trial. It has been evaluated in the second and third-line treatment after intolerance to or progression under sorafenib treatment. The efficacy and safety of cabozantinib depend on the duration of sorafenib pretreatment.163 All panelists recommended the first-line and second-line therapies based on the existing guidelines and studies proving the efficacy of the molecularly targeted agents in the treatment of HCC.
A single, high priming dose of tremelimumab (anti-cytotoxic T lymphocyte-associated antigen 4) plus durvalumab (anti-programmed cell death ligand-1) showed encouraging clinical activity and safety in Phase 2 and 3 trials of advanced HCC.164,165 Moreover, the combination of tremelimumab and durvalumab has been reported to be superior to sorafenib, adding another first-line treatment option. According to BCLC 2022, tremelimumab with durvalumab can be administrated as first-line systemic therapy in patients with advanced HCC with an expected survival of >2 years.166 If atezolizumab-bevacizumab or tremelimumab with durvalumab are not feasible, sorafenib, lenvatinib, or durvalumab can be administered as a first-line therapy.167 Lenvatinib and single-agent durvalumab are non-inferior to sorafenib, but it is essential to mention that there is a significant need to evaluate whether the current second-line alternatives maintain their efficacy in patients initially receiving any of these options. Sorafenib, lenvatinib, or durvalumab may be beneficial following atezolizumab-bevacizumab or tremelimumab/durvalumab, but it is important to determine whether they should be regarded “de facto” second-line alternatives or if their efficacy may be altered in this setting.167,168
Adjuvant therapy aims to decrease the incidence of HCC recurrence in patients who undergo surgical resection. The use of adjuvant systemic therapy following resection, transplantation, or loco-regional ablation drew the attention of oncologists and hepatologists treating patients with HCC. A majority (92.86%) of the panelists recommended that systemic treatment can be used as an adjuvant treatment in certain circumstances, such as the presence of evidence of microvascular invasion in a resected liver with HCC. A large Phase III trial (the STORM trial) was conducted to assess the use of Sorafenib as an adjuvant treatment in patients with resected HCC. It revealed no difference in the RFS between the two groups after 12.5 months, showing that sorafenib treatment was associated with increased adverse events, including four deaths.169 A network meta-analysis revealed that the addition of adjuvant therapy lowers the risk of recurrence and provides survival benefits after surgical resection indicated for HCC.170 Based on the poor evidence supporting adjuvant treatment in routine clinical practice, all (100%) panelists do not recommend adjuvant therapy in HCC and suggest further studies to prove its benefit to be included in routine practice. The panelists recommended that all the proposed studies should be carried out in Egypt.
Treatment Assessment in HCC
According to previous oncology trials, tumor response is generally measured as per the RECIST (Response Evaluation Criteria in Solid Tumors) criteria. The EASL and AASLD guidelines adopted a modified version of the RECIST criteria. The treatment response accounted for the induction of intra-tumoral necrotic areas in estimating the decrease in the tumor load and not just the reduction in the overall tumor size.100,171 Several clinical studies have demonstrated that the objective response measured by mRECIST predicts survival in patients receiving loco-regional therapies.172 A meta-analysis identified seven clinical trials using mRECIST response to assess the survival outcomes after loco-regional treatments.173 Only two clinical trials have evaluated the objective response in systemic therapies by mRECIST,174,175 and more research in this area is essential. A trial conducted on 30 HCC patients in Egypt used the mRECIST criteria to assess the radiological response.176 The EASL guidelines recommended evaluating the response to locoregional therapy with mRECIST and systemic therapy with both RECIST and mRECIST criteria.22 Based on the evidence from the literature, existing guidelines, and clinical trials, all (100%) panelists recommended using the mRECIST Criteria to assess the progression and radiological response after HCC management. Although no existing guideline or literature describes the optimum time to assess the disease progression after immunotherapy, all (100%) panelists recommended a time of 12 weeks or four cycles of immunotherapy to assess the disease progression based on their clinical practice.
Some trials and series have reported the efficacy and tolerability of different external beam radiotherapy techniques in distinct stages of HCC treatment.177 A meta-analysis of trials of TACE alone versus TACE plus external beam radiotherapy demonstrated significant benefits with the combination therapy for the post-treatment OS and local tumor control.178 Additional data on the efficacy of TARE and external beam radiotherapy is known to be emerging. Despite the signs of efficacy and safety, there exists a need for large prospective studies to assess the role of radiotherapy in HCC. The available evidence supporting this therapeutic approach in HCC management is low. Based on the available literature, all (100%) panelists suggest using external beam radiotherapy in HCC treatment only under special indications, where local thermal ablative techniques are contraindicated, or in HCC recurrence following RFA or TACE.
Combination Therapy in HCC Treatment
Several prospective controlled studies evaluated the efficacy of combination treatment, including sorafenib plus TACE, for intermediate and advanced-stage HCC treatment, and the overall results appeared promising.93 According to previous studies, the combination of sorafenib and TACE has an acceptable safety profile; however, there were no conclusive data on the efficacy of the combination.179–181 TARE, in combination with systemic therapy, is under investigation.22 A single-center retrospective study of 104 HCC patients with BCLC-stage B/C reported that TACE plus Sorafenib improved the OS compared to Sorafenib alone.182 Prolonged PFS and OS, and a significantly increased tumor response rate depicting potential efficacy, were noted in the study comparing and evaluating the benefits between the two groups–sorafenib alone and sorafenib plus TACE.182 A multicenter retrospective real-world study conducted in China demonstrated that regorafenib combined with TACE was beneficial and tolerable in patients with unresectable HCC.183 Based on the currently available evidence, all panelists (100%) supported the use of combination therapy in HCC management.
Palliative Care in HCC Treatment
All panelists recommended that patients with BCLC-stage-D HCC who are not eligible for liver transplantation should receive the best supportive care (BSC), including pain management, palliative radiotherapy for painful bone metastasis, nutrition optimization, and psychological support. The recommendation was based on evidence from all international hepatology societies suggesting the use of palliative support, including pain management, nutrition, and psychological support in HCC patients with BCLC-stage D or Child-Pugh Class C who are not eligible for LT.22,45,68 The life expectancy of such patients is about 3–4 months, and the disease management is only symptomatic.184 An ideal palliative care team includes liver and palliative care physicians and nurses, allied healthcare practitioners (physiotherapists, pharmacists, and dieticians), counselors, and other staff.2 The best supportive care is selected for patients whose disease is not responsive to active treatment or who are too sick to receive such therapy. The EASL guidelines recommended the use of paracetamol (up to 3 g/day) or opioids (avoiding NSAIDs); palliative radiotherapy for painful bone metastases; active enhancement of the nutritional status; psychological support (non-pharmacological); QOL for both the patient and their family, and the importance of engaging an appropriately trained palliative care team to provide optimum management in this terminal stage.22
Prevention of HCC
According to the current literature, the prevention of HCC depends on the early prevention of risk factors (primary prevention), the treatment of risk factors at an early stage (secondary prevention), and the prevention or decrease in the rate of HCC relapse after successful curative treatment (tertiary prevention).185,186 Primary prevention of HCC is the only sustainable and practical method to decrease the associated disease burden. Vaccination against hepatitis B reduces the risk of HCC and is recommended for all newborns (within 24 hours) and high-risk groups by the WHO.187 The panelists mentioned that HBV vaccination is mandatory in Egypt and suggested a universal vaccination against HBV infection as one of the strategies to prevent HCC. In Egypt, the HBV vaccination program and HCV eradication through the national campaign are the two approaches adopted to prevent HCC. The EASL guidelines recommended antiviral treatment for patients with chronic HBV and HCV infections.22 Direct-acting antivirals were introduced in Egypt through the efforts of the government and the National Committee for the Control of Viral Hepatitis. The 100 “Million Healthy Lives” initiative treated millions of patients with HCV with a cure rate of over 90%.1 The speed, scale, and quality of the Egyptian initiative were praised by the WHO representatives. More than 60 million Egyptians were screened, and 4 million HCV patients were treated between 2014 and 2020.7 Therefore, all panelists (100%) also recommended the same for the prevention of HCC.
HCC surveillance is a secondary prevention strategy to decrease the burden of HCC through early tumor detection and management of the disease. It needs to be complemented by primary prevention and development and utilization of chemo-preventive strategies. A national follow-up program was established for patients with cirrhosis to encourage the early detection of HCC.7 All panelists (100%) advocate secondary prevention strategies for the prevention of HCC.
The burden of HCC associated with NAFLD and NASH is increasing in many countries. Metabolic diseases such as diabetes and obesity are also associated with an increased risk for HCC.188 The current literature supports the recommendation of all (100%) experts who control lifestyle-related modifiable factors such as changing dietary patterns, increased physical activity, reduced alcohol consumption, and avoiding certain food items can help prevent HCC related to NAFLD and NASH.188 The panelists advocated that patients with diabetes, obesity, and cardiovascular disorders may benefit from chemoprevention along with lifestyle modification based on a pooled analysis of two prospective studies showed that the regular use of aspirin (650 mg) per week was associated with a 50% reduction in risk of HCC.189 New evidence on the association between the regular consumption of coffee and a decreased risk of fibrosis development in NAFLD190 was also noted and suggested as a prevention strategy for HCC.191
Conclusion
The recommendations presented in this report represent measures taken at the highest-level HCC treatment centers in Egypt and were developed by an expert panel consisting of hepatologists, oncologists, gastroenterologists, surgeons, pathologists, and radiologists, under the umbrella of the ESLC. The recommendations were based on the country’s currently available local diagnostic aids and treatment methods and suggested future prospects. The recommendations serve as guidance to all stakeholders involved in HCC management in Egypt, the Middle East, and the African region. Areas of future research were identified, including several potential collaborations to support and improve clinical practice at different Egyptian institutes. The panel suggested a routine follow-up and update of the guidelines.
Acknowledgments
The Egyptian Liver Cancer Committee would like to thank the faculty and experts who provided critical reviews of these consensus statements.
CTI Clinical Trial and Consulting Services provided medical writing and editing support in the preparation of these statements.
Funding
CTI’s support was funded by Roche (Egypt) and Bayer (Egypt).
Disclosure
Dr Hamdy Azim reports grants, personal fees from Roche, grants from Astra Zenca, personal fees from Bayer, during the conduct of the study; grants, personal fees from Novartis, grants, personal fees from Pfizer, grants, personal fees from MSD, personal fees from BMS, personal fees from GSK, outside the submitted work. Prof. Dr. Imam Waked reports personal fees, Investigator Advisory Board Member from Astra Zeneca, personal fees from Hoffman La Roche, personal fees from Bayer, during the conduct of the study; Investigator from Abbvie, personal fees, Advisory Board from Eva Pharma, Investigator from Pfizer, other from Investigator, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Waked I, Esmat G, Elsharkawy A, et al. Screening and treatment program to eliminate hepatitis C in Egypt. N Eng J Med. 2020;382(12):1166–1174. doi:10.1056/NEJMsr1912628
2. Laube R, Sabih A, Strasser SI, Lim L, Cigolini M, Liu K. Palliative care in hepatocellular carcinoma. J Gastroenterol Hepatol. 2021;36(3):618–628. doi:10.1111/jgh.15169
3. World Health Organization (WHO). Global Health Estimates 2020: estimated number of deaths in 2020, Egypt, both sexes, all ages (excl. NMSC). WHO; 2020. Available from: https://gco.iarc.fr/today/online-analysis-table?v=2020&mode=cancer&mode_population=countries&population=900&populations=818&key=asr&sex=0&cancer=39&type=1&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&group_cancer=1&include_nmsc=0&include_nmsc_other=1.
4. Liu Z, Jiang Y, Yuan H, et al. The trends in incidence of primary liver cancer caused by specific etiologies: results from the Global Burden of Disease Study 2016 and implications for liver cancer prevention. J Hepatol. 2019;70(4):674–683. doi:10.1016/j.jhep.2018.12.001
5. El-Zanaty F, Way A. Egypt Demographic and Health Survey, 2008 Cairo, Egypt: Ministry of Health and Population, 2009. Demographic and Health Survey (EDHS); 2009.
6. El-Zanaty and Associates. Egypt Health Issues Survey 2015. Rockville, MD: Ministry of Health and Population, ICF International; 2015.
7. Hassanin A, Kamel S, Waked I, Fort M. Egypt’s Ambitious Strategy to Eliminate Hepatitis C Virus: a Case Study. Glob Health Sci Pract. 2021;9(1):187–200. doi:10.9745/GHSP-D-20-00234
8. Lehman EM, Wilson ML. Epidemiology of hepatitis viruses among hepatocellular carcinoma cases and healthy people in Egypt: a systematic review and meta-analysis. Int J Cancer. 2009;124(3):690–697. doi:10.1002/ijc.23937
9. Ministry of Health Egypt, El-Zanaty and Associates, ICF International. The 2015 Egypt Health Issues Survey (EHIS); 2015. Available from: https://dhsprogram.com/pubs/pdf/FR313/FR313.pdf.
10. Azzam A, Khaled H, Elbohy OA, et al. Seroprevalence of hepatitis B virus surface antigen (HBsAg) in Egypt (2000–2022): a systematic review with meta-analysis. BMC Infect Dis. 2023;23(1):151. doi:10.1186/s12879-023-08110-5
11. Hassany SM. Screening for hepatocellular carcinoma by Egyptian physicians. World J Gastrointest Oncol. 2015;7(9):161. doi:10.4251/wjgo.v7.i9.161
12. Singal AG, Pillai A, Tiro J. Early Detection, Curative Treatment, and Survival Rates for Hepatocellular Carcinoma Surveillance in Patients with Cirrhosis: a Meta-analysis. PLoS Med. 2014;11(4). doi:10.1371/journal.pmed.1001624
13. Guyatt GH, Oxman AD, Vist GE, et al. GRADE Working Group. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–6. doi:10.1136/bmj.39489.470347
14. Harris PS, Hansen RM, Gray ME, Massoud OI, McGuire BM, Shoreibah MG. Hepatocellular carcinoma surveillance: an evidence-based approach. World J Gastroenterol. 2019;25(13):1550–1559. doi:10.3748/wjg.v25.i13.1550
15. Song P, Cai Y, Tang H, Li C, Huang J. The clinical management of hepatocellular carcinoma worldwide: a concise review and comparison of current guidelines from 2001 to 2017. Biosci Trends. 2017;11(4):389–398. doi:10.5582/bst.2017.01202
16. McGivern DR, Lemon SM. Virus-specific mechanisms of carcinogenesis in hepatitis C virus associated liver cancer. Oncogene. 2011;30(17):1969–1983. doi:10.1038/onc.2010.594
17. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
18. Esmat G, El-Sayed MH, Hassany M, Doss W, Waked I. One step closer to elimination of hepatitis C in Egypt. Lancet Gastroenterol Hepatol. 2018;3(10):665. doi:10.1016/S2468-1253(18)30268-1
19. El Kassas M, Funk AL, Salaheldin M, et al. Increased recurrence rates of hepatocellular carcinoma after DAA therapy in a hepatitis C-infected Egyptian cohort: a comparative analysis. J Viral Hepat. 2018;25(6):623–630. doi:10.1111/jvh.12854
20. Guarino M, Sessa A, Cossiga V, Morando F, Caporaso N, Morisco F. Direct-acting antivirals and hepatocellular carcinoma in chronic hepatitis C: a few lights and many shadows. World J Gastroenterol. 2018;24(24):2582–2595. doi:10.3748/wjg.v24.i24.2582
21. Adeniji N, Dhanasekaran R. Current and Emerging Tools for Hepatocellular Carcinoma Surveillance. Hepatol Commun. 2021;5(12):1972–1986. doi:10.1002/hep4.1823
22. Galle PR, Forner A, Llovet JM, et al. EASL Clinical Practice Guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
23. Yang JD, Kim WR, Coelho R, et al. Cirrhosis Is Present in Most Patients With Hepatitis B and Hepatocellular Carcinoma. Clin Gastroenterol Hepatol. 2011;9(1):64–70. doi:10.1016/j.cgh.2010.08.019
24. Prenner SB, VanWagner LB, Flamm SL, Salem R, Lewandowski RJ, Kulik L. Hepatocellular carcinoma decreases the chance of successful hepatitis C virus therapy with direct-acting antivirals. J Hepatol. 2017;66(6):1173–1181. doi:10.1016/j.jhep.2017.01.020
25. El-Zayadi AR, Badran HM, Barakat EM, et al. Hepatocellular carcinoma in Egypt: a single center study over a decade. World J Gastroenterol. 2005;11(33):5193–5198.
26. El-Zayadi R. Prevalence and epidemiological features of hepatocellular carcinoma in Egypt—a single center experience. Hepatol Res. 2001;19(2):170–179. doi:10.1016/S1386-6346(00)00105-4
27. Makhlouf NA, Morsy KH, Mahmoud AA. Hepatitis D virus infection among hepatitis B virus surface antigen positive individuals in Upper Egypt: prevalence and clinical features. J Infect Public Health. 2018;12(3):350–356. doi:10.1016/j.jiph.2018.12.001
28. Elzefzafy W, Soliman R, Saleh L, et al. Seroprevalence and epidemiological characteristics of HDV infection among HBV patients in the Nile Delta, Egypt. J Viral Hepat. 2022;29(1):87–90. doi:10.1111/jvh.13621
29. Tang A, Hallouch O, Chernyak V, Kamaya A, Sirlin CB. Epidemiology of hepatocellular carcinoma: target population for surveillance and diagnosis. Abdominal Radiol. 2018;43(1):13–25. doi:10.1007/s00261-017-1209-1
30. Ziada DH, El Sadany S, Soliman H, et al. Prevalence of hepatocellular carcinoma in chronic hepatitis C patients in Mid Delta, Egypt: a single center study. J Egypt Natl Canc Inst. 2016;28(4):257–262. doi:10.1016/j.jnci.2016.06.001
31. Velázquez R. Prospective analysis of risk factors for hepatocellular carcinoma in patients with liver cirrhosis. Hepatology. 2003;37(3):520–527. doi:10.1053/jhep.2003.50093
32. Heimbach JK, Kulik LM, Finn RS, et al. AASLD Guidelines for the Treatment of Hepatocellular Carcinoma. OncoTargets Therap. 2017:5575. doi:10.1002/hep.29086/suppinfo
33. Gharib AF, Karam RA, Pasha HF, Radwan MI, Elsawy WH. Polymorphisms of hemochromatosis, and alpha-1 antitrypsin genes in Egyptian HCV patients with and without hepatocellular carcinoma. Gene. 2011;489(2):98–102. doi:10.1016/j.gene.2011.08.010
34. Motawi TK, Shaker OG, Ismail MF, Sayed NH. Genetic variants associated with the progression of hepatocellular carcinoma in hepatitis C Egyptian patients. Gene. 2013;527(2):516–520. doi:10.1016/j.gene.2013.06.053
35. Dawood R, Abd El Meguid M, Elrobe W, et al. Significance of Hereditary Hemochromatosis Gene (HFE) Mutations in Chronic Hepatitis C and Hepatocellular Carcinoma Patients in Egypt: a Pilot Study. Asian Pacific J Cancer Prevention. 2021;22(9):2837–2845. doi:10.31557/APJCP.2021.22.9.2837
36. Elmberg M, Hultcrantz R, Ekbom A, et al. Cancer risk in patients with hereditary hemochromatosis and in their first-degree relatives. Gastroenterology. 2003;125(6):1733–1741. doi:10.1053/j.gastro.2003.09.035
37. Liang Y, Yang Z, Zhong R. Primary biliary cirrhosis and cancer risk: a systematic review and meta-analysis. Hepatology. 2012;56(4):1409–1417. doi:10.1002/hep.25788
38. Hamed MA, Ali SA. Non-viral factors contributing to hepatocellular carcinoma. World J Hepatol. 2013;5(6):311. doi:10.4254/wjh.v5.i6.311
39. Tansel A, Katz LH, El-Serag HB, et al. Incidence and Determinants of Hepatocellular Carcinoma in Autoimmune Hepatitis: a Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2017;15(8):1207–1217.e4. doi:10.1016/j.cgh.2017.02.006
40. Meza-Junco J, Montaño-Loza AJ, Martínez-Benitez B, Kimura-Hayama E. Hepatocellular carcinoma in patients with autoimmune liver diseases: two case reports and literature review. Ann Hepatol. 2019;6(2):122–126.
41. Antoury C, Lopez R, Zein N, Stoller JK, Alkhouri N. Alpha-1 antitrypsin deficiency and the risk of hepatocellular carcinoma in end-stage liver disease. World J Hepatol. 2015;7(10):1427–1432. doi:10.4254/wjh.v7.i10.1427
42. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68(2):723–750. doi:10.1002/hep.29913
43. Omata M, Cheng AL, Kokudo N, et al. Asia–Pacific clinical practice guidelines on the management of hepatocellular carcinoma: a 2017 update. Hepatol Int. 2017;11(4):317–370. doi:10.1007/s12072-017-9799-9
44. Colli A, Fraquelli M, Casazza G, et al. Accuracy of Ultrasonography, Spiral CT, Magnetic Resonance, and Alpha-Fetoprotein in Diagnosing Hepatocellular Carcinoma: a Systematic Review. CME. Am J Gastroenterol. 2006;101(3):513–523. doi:10.1111/j.1572-0241.2006.00467.x
45. Kudo M, Kawamura Y, Hasegawa K, et al. Management of hepatocellular carcinoma in Japan: JSH consensus statements and recommendations 2021 update. Liver Cancer. 2021;10(3):181–223. doi:10.1159/000514174
46. Singal AG, Mittal S, Yerokun OA, et al. Hepatocellular Carcinoma Screening Associated with Early Tumor Detection and Improved Survival Among Patients with Cirrhosis in the US. Am J Med. 2017;130(9):1099–1106.e1. doi:10.1016/j.amjmed.2017.01.021
47. Kim TH, Kim SY, Tang A, Lee JM. Comparison of international guidelines for noninvasive diagnosis of hepatocellular carcinoma: 2018 update. Clin Mol Hepatol. 2019;25(3):245–263. doi:10.3350/cmh.2018.0090
48. Choi J, Kim G, Han S, Lee W, Chun S, Lim Y. Longitudinal Assessment of Three Serum Biomarkers to Detect Very Early‐Stage Hepatocellular Carcinoma. Hepatology. 2019;69(5):1983–1994. doi:10.1002/hep.30233
49. Caviglia GP, Abate ML, Petrini E, Gaia S, Rizzetto M. Highly sensitive alpha-fetoprotein, Lens culinaris agglutinin-reactive fraction of alpha-fetoprotein and des-gamma-carboxyprothrombin for hepatocellular carcinoma detection. Hepatol Res. 2016;46(3):E130–E135. doi:10.1111/hepr.12544
50. Kumada T, Toyoda H, Tada T, et al. High-sensitivity Lens culinaris agglutinin-reactive alpha-fetoprotein assay predicts early detection of hepatocellular carcinoma. J Gastroenterol. 2014;49(3):555–563. doi:10.1007/s00535-013-0883-1
51. Ibrahim HM, Elghannam MZ, Elkhawaga OAY, El-Sokkary AMA. Evaluation of serum alpha fetoprotein-L3 as an accuracy novel biomarker for the early diagnosis of hepatocellular carcinoma in Egyptian patients. Saudi J Biol Sci. 2021;28(10):5760–5764. doi:10.1016/j.sjbs.2021.06.020
52. Zakhary NI, Khodeer SM, Shafik HE, Abdel Malak CA. Impact of PIVKA-II in diagnosis of hepatocellular carcinoma. J Adv Res. 2013;4(6):539–546. doi:10.1016/j.jare.2012.10.004
53. Svobodova S, Karlikova M, Topolcan O, et al. PIVKA-II as a Potential New Biomarker for Hepatocellular Carcinoma – a Pilot Study. Vivo. 2018;32(6):1551–1554. doi:10.21873/invivo.11413
54. Morad WS, Basuni AA, Fouad T, et al. The value of PIVKA-II and AFP-L3% in the diagnosis of hepatocellular carcinoma with normal and abnormal AFP levels. Egyptian Liver J. 2013;3(1):1–5. doi:10.1097/01.ELX.0000424246.18235.c5
55. Johnson PJ, Pirrie SJ, Cox TF, et al. The Detection of Hepatocellular Carcinoma Using a Prospectively Developed and Validated Model Based on Serological Biomarkers. Cancer Epidemiol Bio Prevention. 2014;23(1):144–153. doi:10.1158/1055-9965.EPI-13-0870
56. Best J, Bilgi H, Heider D, et al. The GALAD scoring algorithm based on AFP, AFP-L3, and DCP significantly improves detection of BCLC early stage hepatocellular carcinoma. Z Gastroenterol. 2016;54(12):1296–1305. doi:10.1055/s-0042-119529
57. Schotten C, Ostertag B, Sowa JP, et al. Galad score detects early-stage hepatocellular carcinoma in a european cohort of chronic hepatitis b and c patients. Pharmaceuticals. 2021;14(8). doi:10.3390/ph14080735
58. Yang JD, Addissie BD, Mara KC, et al. GALAD Score for Hepatocellular Carcinoma Detection in Comparison with Liver Ultrasound and Proposal of GALADUS Score. Cancer Epidemiol Bio Prevention. 2019;28(3):531–538. doi:10.1158/1055-9965.EPI-18-0281
59. Lee YJ, Lee JM, Lee JS, et al. Hepatocellular Carcinoma: diagnostic Performance of Multidetector CT and MR Imaging—A Systematic Review and Meta-Analysis. Radiology. 2015;275(1):97–109. doi:10.1148/radiol.14140690
60. Roberts LR, Sirlin CB, Zaiem F, et al. Imaging for the diagnosis of hepatocellular carcinoma: a systematic review and meta-analysis. Hepatology. 2018;67(1):401–421. doi:10.1002/hep.29487
61. Chernyak V, Fowler KJ, Kamaya A, et al. Liver Imaging Reporting and Data System (LI-RADS) Version 2018: imaging of Hepatocellular Carcinoma in At-Risk Patients. Radiology. 2018;289(3):816–830. doi:10.1148/radiol.2018181494
62. Lee YT, Wang JJ, Zhu Y, Agopian VG, Tseng HR, Yang JD. An Official Learning Resource of AASLD Review Diagnostic Criteria and Li-RaDs for Hepatocellular Carcinoma. J Hepatocell Carcinoma. 2021;17.
63. Liang Y, Xu F, Guo Y, et al. Diagnostic performance of LI-RADS for MRI and CT detection of HCC: a systematic review and diagnostic meta-analysis. Eur J Radiol. 2021;134:109404. doi:10.1016/j.ejrad.2020.109404
64. van der Pol CB, Lim CS, Sirlin CB, et al. Accuracy of the Liver Imaging Reporting and Data System in Computed Tomography and Magnetic Resonance Image Analysis of Hepatocellular Carcinoma or Overall Malignancy—A Systematic Review. Gastroenterology. 2019;156(4):976–986. doi:10.1053/j.gastro.2018.11.020
65. Lee S, Kim S, Roh YH, Choi J, Park M, Kim M. Diagnostic Performance of CT/MRI Liver Imaging Reporting and Data System v2017 for Hepatocellular Carcinoma: a Systematic Review and Meta‐Analysis. Liver Int. 2020;40(6):1488–1497. doi:10.1111/liv.14424
66. Hanna RF, Miloushev VZ, Tang A, et al. Comparative 13-year meta-analysis of the sensitivity and positive predictive value of ultrasound, CT, and MRI for detecting hepatocellular carcinoma. Abdominal Radiol. 2016;41(1):71–90. doi:10.1007/s00261-015-0592-8
67. Becker-Weidman DJS, Kalb B, Sharma P, et al. Hepatocellular Carcinoma Lesion Characterization: single-Institution Clinical Performance Review of Multiphase Gadolinium-enhanced MR Imaging—Comparison to Prior Same-Center Results after MR Systems Improvements. Radiology. 2011;261(3):824–833. doi:10.1148/radiol.11110157
68. Attwa MH, El-Etreby SA. Guide for diagnosis and treatment of hepatocellular carcinoma. World J Hepatol. 2015;7(12):1632–1651. doi:10.4254/wjh.v7.i12.1632
69. Kinoshita A, Onoda H, Fushiya N, Koike K, Nishino H, Tajiri H. Staging systems for hepatocellular carcinoma: current status and future perspectives. World J Hepatol. 2015;7(3):406–424. doi:10.4254/wjh.v7.i3.406
70. Marrero JA, Fontana RJ, Barrat A, et al. Prognosis of hepatocellular carcinoma: comparison of 7 staging systems in an American cohort. Hepatology. 2005;41(4):707–715. doi:10.1002/hep.20636
71. Gomaa AI, Hashim MS, Waked I. Comparing Staging Systems for Predicting Prognosis and Survival in Patients with Hepatocellular Carcinoma in Egypt. PLoS One. 2014;9(3):e90929. doi:10.1371/journal.pone.0090929
72. Cillo U, Bassanello M, Vitale A, et al. The critical issue of hepatocellular carcinoma prognostic classification: which is the best tool available? J Hepatol. 2004;40(1):124–131. doi:10.1016/j.jhep.2003.09.027
73. Cillo U, Vitale A, Grigoletto F, et al. Prospective validation of the Barcelona Clinic Liver Cancer staging system. J Hepatol. 2006;44(4):723–731. doi:10.1016/j.jhep.2005.12.015
74. Guglielmi A, Ruzzenente A, Pachera S, et al. Comparison of Seven Staging Systems in Cirrhotic Patients With Hepatocellular Carcinoma in a Cohort of Patients Who Underwent Radiofrequency Ablation With Complete Response. Am J Gastroenterol. 2008;103(3):597–604. doi:10.1111/j.1572-0241.2007.01604.x
75. Vitale A, Saracino E, Boccagni P, et al. Validation of the BCLC Prognostic System in Surgical Hepatocellular Cancer Patients. Transplant Proc. 2009;41(4):1260–1263. doi:10.1016/j.transproceed.2009.03.054
76. Wang JH, Changchien CS, Hu TH, et al. The efficacy of treatment schedules according to Barcelona Clinic Liver Cancer staging for hepatocellular carcinoma – survival analysis of 3892 patients. Eur J Cancer. 2008;44(7):1000–1006. doi:10.1016/j.ejca.2008.02.018
77. Abdelaziz AO, Elbaz TM, Shousha HI, et al. Survival and prognostic factors for hepatocellular carcinoma: an Egyptian multidisciplinary clinic experience. Asian Pacific J Cancer Prevention. 2014;15(9):3915–3920. doi:10.7314/APJCP.2014.15.9.3915
78. Bolondi L, Burroughs A, Dufour JF, et al. Heterogeneity of Patients with Intermediate (BCLC B) Hepatocellular Carcinoma: proposal for a Subclassification to Facilitate Treatment Decisions. Semin Liver Dis. 2013;32(04):348–359. doi:10.1055/s-0032-1329906
79. Ha Y, Shim JH, Kim SO, Kim KM, Lim YS, Lee HC. Clinical appraisal of the recently proposed Barcelona Clinic Liver Cancer stage B subclassification by survival analysis. J Gastroenterol Hepatol. 2014;29(4):787–793. doi:10.1111/jgh.12452
80. Wang JH, Kee KM, Lin CY, et al. Validation and modification of a proposed substaging system for patients with intermediate hepatocellular carcinoma. J Gastroenterol Hepatol. 2015;30(2):358–363. doi:10.1111/jgh.12686
81. Kudo M, Arizumi T, Ueshima K, Sakurai T, Kitano M, Nishida N. Subclassification of BCLC B Stage Hepatocellular Carcinoma and Treatment Strategies: proposal of Modified Bolondi’s Subclassification (Kinki Criteria). Digestive Dis. 2015;33(6):751–758. doi:10.1159/000439290
82. Kariyama K, Nouso K, Hiraoka A, et al. EZ-ALBI Score for Predicting Hepatocellular Carcinoma Prognosis. Liver Cancer. 2020;9(6):734–743. doi:10.1159/000508971
83. Božin T, Mustapić S, Bokun T, et al. Albi score as a predictor of survival in patients with compensated cirrhosis resected for hepatocellular carcinoma: exploratory evaluation in relationship to palbi and meld liver function scores. Acta Clin Croat. 2018;57(2):292–300. doi:10.20471/acc.2018.57.02.09
84. Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of Liver Function in Patients With Hepatocellular Carcinoma: a New Evidence-Based Approach—The ALBI Grade. J Clin Oncol. 2015;33(6):550–558. doi:10.1200/JCO.2014.57.9151
85. Hiraoka A, Kumada T, Michitaka K, Kudo M. Newly Proposed ALBI Grade and ALBI-T Score as Tools for Assessment of Hepatic Function and Prognosis in Hepatocellular Carcinoma Patients. Liver Cancer. 2019;8(5):312–325. doi:10.1159/000494844
86. Faivre S, Raymond E, Boucher E, et al. Safety and efficacy of sunitinib in patients with advanced hepatocellular carcinoma: an open-label, multicentre, Phase II study. Lancet Oncol. 2009;10(8):794–800. doi:10.1016/S1470-2045(09)70171-8
87. Zhu AX, Sahani DV, Duda DG, et al. Efficacy, safety, and potential biomarkers of sunitinib monotherapy in advanced hepatocellular carcinoma: a phase II study. J Clin Oncol. 2009;27(18):3027–3035. doi:10.1200/JCO.2008.20.9908
88. Fang P. Efficacy and safety of bevacizumab for the treatment of advanced hepatocellular carcinoma: a systematic review of phase II trials. PLoS One. 2012;7(12):e49717–e49717. doi:10.1371/journal.pone.0049717
89. Ranpura V, Hapani S, Wu S. Treatment-Related Mortality With Bevacizumab in Cancer Patients: a Meta-analysis. JAMA. 2011;305(5):487–494. doi:10.1001/jama.2011.51
90. Girotra M, Soota K, Dhaliwal AS, Abraham RR, Garcia-Saenz-de-Sicilia M, Tharian B. Utility of endoscopic ultrasound and endoscopy in diagnosis and management of hepatocellular carcinoma and its complications: what does endoscopic ultrasonography offer above and beyond conventional cross-sectional imaging? World J Gastrointest Endosc. 2018;10(2):56–68. doi:10.4253/wjge.v10.i2.56
91. Bhutani M, Koduru P, Suzuki R, Lakhtakia S, Ramchandani M, Makmun D. Role of endoscopic ultrasound in diagnosis and management of hepatocellular carcinoma. J Hepatocell Carcinoma. 2015;143. doi:10.2147/JHC.S60868
92. Hsu C, Rimassa L, Sun HC, Vogel A, Kaseb AO. Immunotherapy in hepatocellular carcinoma: evaluation and management of adverse events associated with atezolizumab plus bevacizumab. Ther Adv Med Oncol. 2021;13:17588359211031140. doi:10.1177/17588359211031141
93. Gomaa AI. Recent advances in multidisciplinary management of hepatocellular carcinoma. World J Hepatol. 2015;7(4):673. doi:10.4254/wjh.v7.i4.673
94. Sinn DH, Choi GS, Park HC, et al. Multidisciplinary approach is associated with improved survival of hepatocellular carcinoma patients. PLoS One. 2019;14(1). doi:10.1371/journal.pone.0210730
95. Zaky S. Multidisciplinary decision making in the management of hepatocellular carcinoma: a hospital-based study. Turkish J Gastroenterol. 2015;26(6):498–505. doi:10.5152/tjg.2015.0158
96. Barone C, Koeberle D, Metselaar H, Parisi G, Sansonno D, Spinzi G. Multidisciplinary approach for HCC patients: hepatology for the oncologists. Ann Oncol. 2013;24:15–23. doi:10.1093/annonc/mdt053
97. Dodd GD, Miller WJ, Baron RL, Skolnick ML, Campbell WL. Detection of malignant tumors in end-stage cirrhotic livers: efficacy of sonography as a screening technique. Am J Roentgenol. 1992;159(4):727–733. doi:10.2214/ajr.159.4.1326883
98. Senbel A, Elmahdy Y, Roshdy S, et al. Role of Hepatic Resection for HCC in the era of Transplantation; an Experience of Two Tertiary Egyptian Centers. Indian J Surg Oncol. 2017;8(4):514–518. doi:10.1007/s13193-017-0679-5
99. Bruix J, Castells A, Bosch J, et al. Surgical resection of hepatocellular carcinoma in cirrhotic patients: prognostic value of preoperative portal pressure. Gastroenterology. 1996;111(4):1018–1022. doi:10.1016/S0016-5085(96)70070-7
100. Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53(3):1020–1022. doi:10.1002/hep.24199
101. Allaire M, Goumard C, Lim C, le Cleach A, Wagner M, Scatton O. New Frontiers in Liver Resection for Hepatocellular Carcinoma. JHEP Reports. 2020:100134.
102. Mai RY, Wang YY, Bai T, et al. Combination of ALBI and APRI to predict posthepatectomy liver failure after liver resection for HBV-related HCC patients. Cancer Manag Res. 2019;11:8799–8806. doi:10.2147/CMAR.S213432
103. Izzo F, Granata V, Grassi R, et al. Radiofrequency Ablation and Microwave Ablation in Liver Tumors: an Update. Oncologist. 2019;24(10):e990–e1005. doi:10.1634/theoncologist.2018-0337
104. Khan A, Mostowy M, Owusu M, et al. Microwave ablation determines similar survival outcomes as compared to radiofrequency ablation for the treatment of hepatocellular carcinoma. Expert Rev Gastroenterol Hepatol. 2021;15(7):829–833. doi:10.1080/17474124.2021.1869939
105. Orlando A, Leandro G, Olivo M, Andriulli A, Cottone M. Radiofrequency Thermal Ablation vs. Percutaneous Ethanol Injection for Small Hepatocellular Carcinoma in Cirrhosis: meta-Analysis of Randomized Controlled Trials. Am J Gastroenterol. 2009;104(2):514–524. doi:10.1038/ajg.2008.80
106. Cho YK, Kim JK, Kim MY, Rhim H, Han JK. Systematic review of randomized trials for hepatocellular carcinoma treated with percutaneous ablation therapies. Hepatology. 2009;49(2):453–459. doi:10.1002/hep.22648
107. Shen A, Zhang H, Tang C, et al. A systematic review of radiofrequency ablation versus percutaneous ethanol injection for small hepatocellular carcinoma up to 3 cm. J Gastroenterol Hepatol. 2013;28(5):793–800. doi:10.1111/jgh.12162
108. Livraghi T, Meloni F, Di Stasi M, et al. Sustained complete response and complications rates after radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: is resection still the treatment of choice? Hepatology. 2008;47(1):82–89. doi:10.1002/hep.21933
109. Zanus G, Boetto R, Gringeri E, et al. Microwave Thermal Ablation for Hepatocarcinoma: six Liver Transplantation Cases. Transplant Proc. 2011;43(4):1091–1094. doi:10.1016/j.transproceed.2011.02.044
110. Facciorusso A, Abd El Aziz MA, Tartaglia N, et al. Microwave Ablation Versus Radiofrequency Ablation for Treatment of Hepatocellular Carcinoma: a Meta-Analysis of Randomized Controlled Trials. Cancers. 2020;12(12):3796. doi:10.3390/cancers12123796
111. Lencioni R, Crocetti L, De Simone P, Filipponi F. Loco-regional interventional treatment of hepatocellular carcinoma: techniques, outcomes, and future prospects. Transplant Int. 2010;23(7):698–703. doi:10.1111/j.1432-2277.2010.01109.x
112. Kamal A, Elmoety AAA, Rostom YAM, Shater MS, Lashen SA. Percutaneous radiofrequency versus microwave ablation for management of hepatocellular carcinoma: a randomized controlled trial. J Gastrointest Oncol. 2019;10(3):562–571. doi:10.21037/jgo.2019.01.34
113. Müller L, Stoehr F, Mähringer-Kunz A, Hahn F, Weinmann A, Kloeckner R. Current Strategies to Identify Patients That Will Benefit from TACE Treatment and Future Directions a Practical Step-by-Step Guide. J Hepatocell Carcinoma. 2021;8:403–419. doi:10.2147/jhc.s285735
114. Lo CM, Ngan H, Tso WK, et al. Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology. 2002;35(5):1164–1171. doi:10.1053/jhep.2002.33156
115. Llovet J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology. 2003;37(2):429–442. doi:10.1053/jhep.2003.50047
116. Cammà C, Schepis F, Orlando A, et al. Transarterial Chemoembolization for Unresectable Hepatocellular Carcinoma: meta-Analysis of Randomized Controlled Trials. Radiology. 2002;224(1):47–54. doi:10.1148/radiol.2241011262
117. Elshaarawy O, Gomaa A, Omar H, Rewisha E, Waked I. Intermediate stage hepatocellular carcinoma: a summary review. J Hepatocell Carcinoma. 2019;6:105–117. doi:10.2147/JHC.S168682
118. Bessar AA, Farag A, Abdel Monem SM, et al. Transarterial chemoembolisation in patients with hepatocellular carcinoma: low-dose doxorubicin reduces post-embolisation syndrome without affecting survival—prospective interventional study. Eur Radiol Exp. 2021;5(1):10. doi:10.1186/s41747-021-00204-6
119. Zeeneldin AA, Salem SE, Tabashy RH, Ibrahim AA, Alieldin NH. Transarterial chemoembolization for the treatment of hepatocellular carcinoma: a single center experience including 221 patients. J Egypt Natl Canc Inst. 2013;25(3):143–150. doi:10.1016/j.jnci.2013.05.003
120. Abdelaziz AO, Abdelmaksoud AH, Nabeel MM, et al. Transarterial Chemoembolization Combined with Either Radiofrequency or Microwave Ablation in Management of Hepatocellular Carcinoma. Asian Pac J Cancer Prev. 2017;18(1):189–194. doi:10.22034/APJCP.2017.18.1.189
121. Hucke F, Pinter M, Graziadei I, et al. How to STATE suitability and START transarterial chemoembolization in patients with intermediate stage hepatocellular carcinoma. J Hepatol. 2014;61(6):1287–1296. doi:10.1016/j.jhep.2014.07.002
122. Kadalayil L, Benini R, Pallan L, et al. A simple prognostic scoring system for patients receiving transarterial embolisation for hepatocellular cancer. Ann Oncol. 2013;24(10):2565–2570. doi:10.1093/annonc/mdt247
123. Kloeckner R, Pitton MB, Dueber C, et al. Validation of Clinical Scoring Systems ART and ABCR after Transarterial Chemoembolization of Hepatocellular Carcinoma. J Vascular Int Radiol. 2017;28(1):94–102. doi:10.1016/j.jvir.2016.06.012
124. Pinato DJ, Arizumi T, Jang JW, et al. Combined sequential use of HAP and ART scores to predict survival outcome and treatment failure following chemoembolization in hepatocellular carcinoma: a multi-center comparative study. Oncotarget. 2016;7(28):44705–44718. doi:10.18632/oncotarget.9604
125. Sieghart W, Hucke F, Pinter M, et al. The ART of decision making: retreatment with transarterial chemoembolization in patients with hepatocellular carcinoma. Hepatology. 2013;57(6):2261–2273. doi:10.1002/hep.26256
126. Hucke F, Sieghart W, Pinter M, et al. The ART-strategy: sequential assessment of the ART score predicts outcome of patients with hepatocellular carcinoma re-treated with TACE. J Hepatol. 2014;60(1):118–126. doi:10.1016/j.jhep.2013.08.022
127. Sacco R, Conte C, Tumino E, et al. Transarterial radioembolization for hepatocellular carcinoma: a review. J Hepatocell Carcinoma. 2016;3:25–29. doi:10.2147/jhc.s50359
128. Jelic S, Sotiropoulos GC. Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21:v59–v64. doi:10.1093/annonc/mdq166
129. Thomas MB, Jaffe D, Choti MM, et al. Hepatocellular carcinoma: consensus recommendations of the National Cancer Institute Clinical Trials Planning Meeting. J Clin Oncol. 2010;28(25):3994–4005. doi:10.1200/JCO.2010.28.7805
130. Iñarrairaegui M, Pardo F, Bilbao JI, et al. Response to radioembolization with yttrium-90 resin microspheres may allow surgical treatment with curative intent and prolonged survival in previously unresectable hepatocellular carcinoma. Eur J Surgical Oncol. 2012;38(7):594–601. doi:10.1016/j.ejso.2012.02.189
131. de la Torre MA, Buades-Mateu J, de la Rosa PA, et al. A comparison of survival in patients with hepatocellular carcinoma and portal vein invasion treated by radioembolization or sorafenib. Liver Int. 2016;36(8):1206–1212. doi:10.1111/liv.13098
132. Mazzaferro V, Sposito C, Bhoori S, et al. Yttrium-90 radioembolization for intermediate-advanced hepatocellular carcinoma: a phase 2 study. Hepatology. 2013;57(5):1826–1837. doi:10.1002/hep.26014
133. Garin E, Lenoir L, Edeline J, et al. Boosted selective internal radiation therapy with 90Y-loaded glass microspheres (B-SIRT) for hepatocellular carcinoma patients: a new personalized promising concept. Eur J Nucl Med Mol Imaging. 2013;40(7):1057–1068. doi:10.1007/s00259-013-2395-x
134. El Fouly A, Ertle J, El Dorry A, et al. In intermediate stage hepatocellular carcinoma: radioembolization with yttrium 90 or chemoembolization? Liver Int. 2015;35(2):627–635. doi:10.1111/liv.12637
135. Mazzaferro V, Chun YS, Poon RTP, et al. Liver Transplantation for Hepatocellular Carcinoma. Ann Surg Oncol. 2008;15(4):1001–1007. doi:10.1245/s10434-007-9559-5
136. Lankarani KB, Hosseini SAM. The Status of Liver Transplantation in the Middle East. Clin Liver Dis. 2019;14(6):215–218. doi:10.1002/cld.889
137. Yao F. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001;33(6):1394–1403. doi:10.1053/jhep.2001.24563
138. Yao FY, Xiao L, Bass NM, Kerlan R, Ascher NL, Roberts JP. Liver Transplantation for Hepatocellular Carcinoma: validation of the UCSF-Expanded Criteria Based on Preoperative Imaging. Am J Transplantation. 2007;7(11):2587–2596. doi:10.1111/j.1600-6143.2007.01965.x
139. Mazzaferro V, Llovet JM, Miceli R, et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: a retrospective, exploratory analysis. Lancet Oncol. 2009;10(1):35–43. doi:10.1016/S1470-2045(08)70284-5
140. Azzam AZ. Liver transplantation as a management of hepatocellular carcinoma. World J Hepatol. 2015;7(10):1347. doi:10.4254/wjh.v7.i10.1347
141. Clavien PA, Lesurtel M, Bossuyt PM, Gores GJ, Langer B, Perrier A. Recommendations for liver transplantation for hepatocellular carcinoma: an international consensus conference report. Lancet Oncol. 2012;13(1):e11–e22. doi:10.1016/S1470-2045(11)70175-9
142. Yao FY, Mehta N, Flemming J, et al. Downstaging of hepatocellular cancer before liver transplant: long-term outcome compared to tumors within Milan criteria. Hepatology. 2015;61(6):1968–1977. doi:10.1002/hep.27752
143. Lei J, Wang W, Yan L. Downstaging Advanced Hepatocellular Carcinoma to the Milan Criteria May Provide a Comparable Outcome to Conventional Milan Criteria. J Gastrointestinal Surgery. 2013;17(8):1440–1446. doi:10.1007/s11605-013-2229-y
144. Bova V, Miraglia R, Maruzzelli L, Vizzini GB, Luca A. Predictive Factors of Downstaging of Hepatocellular Carcinoma Beyond the Milan Criteria Treated with Intra-arterial Therapies. Cardiovasc Intervent Radiol. 2013;36(2):433–439. doi:10.1007/s00270-012-0458-1
145. Berry K, Ioannou GN. Serum alpha-fetoprotein level independently predicts posttransplant survival in patients with hepatocellular carcinoma. Liver Transplantation. 2013;19(6):634–645. doi:10.1002/lt.23652
146. Raoul JL, Gilabert M, Piana G. How to Define Transarterial Chemoembolization Failure or Refractoriness: a European Perspective. Liver Cancer. 2014;3(2):119–124. doi:10.1159/000343867
147. Raoul JL, Sangro B, Forner A, et al. Evolving strategies for the management of intermediate-stage hepatocellular carcinoma: available evidence and expert opinion on the use of transarterial chemoembolization. Cancer Treat Rev. 2011;37(3):212–220. doi:10.1016/j.ctrv.2010.07.006
148. Piscaglia F, Bolondi L. The intermediate hepatocellular carcinoma stage: should treatment be expanded? Digestive Liver Dis. 2010;42:S258–S263. doi:10.1016/S1590-8658(10)60514-2
149. Ogasawara S, Chiba T, Ooka Y, et al. Efficacy of sorafenib in intermediate-stage hepatocellular carcinoma patients refractory to transarterial chemoembolization. Oncology. 2014;87(6):330–341. doi:10.1159/000365993
150. Arizumi T, Ueshima K, Chishina H, et al. Validation of the Criteria of Transcatheter Arterial Chemoembolization Failure or Refractoriness in Patients with Advanced Hepatocellular Carcinoma Proposed by the LCSGJ. Oncology. 2014;87(s1):32–36. doi:10.1159/000368143
151. Arizumi T, Ueshima K, Minami T, et al. Effectiveness of Sorafenib in Patients with Transcatheter Arterial Chemoembolization (TACE) Refractory and Intermediate-Stage Hepatocellular Carcinoma. Liver Cancer. 2015;4(4):253–262. doi:10.1159/000367743
152. Hack SP, Spahn J, Chen M, et al. IMbrave 050: a Phase III trial of atezolizumab plus bevacizumab in high-risk hepatocellular carcinoma after curative resection or ablation. Future Oncol. 2020;16(15):975–989. doi:10.2217/fon-2020-0162
153. Vogel A, Martinelli E, Cervantes A, et al. Updated treatment recommendations for hepatocellular carcinoma (HCC) from the ESMO Clinical Practice Guidelines. Ann Oncol. 2021;32(6):801–805. doi:10.1016/j.annonc.2021.02.014
154. Abdel-Rahman O. Systemic therapy for hepatocellular carcinoma (HCC): from bench to bedside. J Egypt Natl Canc Inst. 2013;25(4):165–171. doi:10.1016/j.jnci.2013.08.002
155. Akateh C, Black SM, Conteh L, et al. Neoadjuvant and adjuvant treatment strategies for hepatocellular carcinoma. World J Gastroenterol. 2019;25(28):3704–3721. doi:10.3748/wjg.v25.i28.3704
156. Cheng AL, Kang YK, Chen Z, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10(1):25–34. doi:10.1016/S1470-2045(08)70285-7
157. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in Advanced Hepatocellular Carcinoma. N Eng J Med. 2008;359(4):378–390. doi:10.1056/NEJMoa0708857
158. Abdel-Rahman O, Cheung WY. The expanding role of systemic therapy in the management of hepatocellular carcinoma. Can J Gastroenterol Hepatol. 2018;2018:1–4. doi:10.1155/2018/4763832
159. Yamashita T, Kudo M, Ikeda K, et al. REFLECT-a phase 3 trial comparing efficacy and safety of lenvatinib to sorafenib for the treatment of unresectable hepatocellular carcinoma: an analysis of Japanese subset. J Gastroenterol. 2020;55(1):113–122. doi:10.1007/s00535-019-01642-1
160. Kokudo N, Takemura N, Hasegawa K, et al. Clinical practice guidelines for hepatocellular carcinoma: the Japan Society of Hepatology 2017 (4th JSH‐HCC guidelines) 2019 update. Hepatol Res. 2019;49(10):1109–1113. doi:10.1111/hepr.13411
161. Bruix J, Qin S, Merle P, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;389(10064):56–66. doi:10.1016/S0140-6736(16)32453-9
162. Zhu AX, Kang YK, Yen CJ, et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(2):282–296. doi:10.1016/S1470-2045(18)30937-9
163. Abou-Alfa GK, Meyer T, Cheng AL, et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N Eng J Med. 2018;379(1):54–63. doi:10.1056/NEJMoa1717002
164. Kelley RK, Sangro B, Harris W, et al. Safety, Efficacy, and Pharmacodynamics of Tremelimumab Plus Durvalumab for Patients With Unresectable Hepatocellular Carcinoma: randomized Expansion of a Phase I/II Study. J Clin Oncol. 2021;39(27):2991–3001. doi:10.1200/JCO.20.03555
165. K AAG, George L, Masatoshi K, et al. Tremelimumab plus Durvalumab in Unresectable Hepatocellular Carcinoma. NEJM Evidence. 2022;1(8):EVIDoa2100070. doi:10.1056/EVIDoa2100070
166. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
167. Bruix J, Chan SL, Galle PR, Rimassa L, Sangro B. Systemic treatment of hepatocellular carcinoma: an EASL position paper. J Hepatol. 2021;75(4):960–974. doi:10.1016/j.jhep.2021.07.004
168. Bruix J. Endpoints in clinical trials for liver cancer and their value in evidence-based clinical decision making: an unresolved Gordian knot. J Hepatol. 2021;74(6):1483–1488. doi:10.1016/j.jhep.2021.01.033
169. Bruix J, Takayama T, Mazzaferro V, et al. Adjuvant sorafenib for hepatocellular carcinoma after resection or ablation (STORM): a phase 3, randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2015;16(13):1344–1354. doi:10.1016/S1470-2045(15)00198-9
170. Liu Y, Wang Y, Guo X, et al. Comparative Effectiveness of adjuvant treatment for resected hepatocellular carcinoma: a systematic review and network meta-analysis. Front Oncol. 2021:11. doi:10.3389/fonc.2021.709278
171. Bruix J, Sherman M, Llovet JM, et al. Clinical Management of Hepatocellular Carcinoma. Conclusions of the Barcelona-2000 EASL Conference. J Hepatol. 2001;35(3):421–430. doi:10.1016/S0168-8278(01)00130-1
172. Lencioni R. New Data Supporting Modified RECIST (mRECIST) for Hepatocellular Carcinoma. Clin Cancer Res. 2013;19(6):1312–1314. doi:10.1158/1078-0432.CCR-12-3796
173. Vincenzi B, Di Maio M, Silletta M, et al. Prognostic Relevance of Objective Response According to EASL Criteria and mRECIST Criteria in Hepatocellular Carcinoma Patients Treated with Loco-Regional Therapies: a Literature-Based Meta-Analysis. PLoS One. 2015;10(7):e0133488. doi:10.1371/journal.pone.0133488
174. Lencioni R, Montal R, Torres F, et al. Objective response by mRECIST as a predictor and potential surrogate end-point of overall survival in advanced HCC. J Hepatol. 2017;66(6):1166–1172. doi:10.1016/j.jhep.2017.01.012
175. Meyer T, Palmer DH, Cheng AL, Hocke J, Loembé AB, Yen CJ. mRECIST to predict survival in advanced hepatocellular carcinoma: analysis of two randomised phase II trials comparing nintedanib vs sorafenib. Liver Int. 2017;37(7):1047–1055. doi:10.1111/liv.13359
176. Abdella H, Shaker MK, Montasser IF, et al. Outcome of transarterial chemoembolization in Egyptian patients with hepatocellular carcinoma and branch portal vein thrombosis. Indian J Gastroenterol. 2018;37(2):127–132. doi:10.1007/s12664-018-0830-4
177. Nabavizadeh N, Mitin T, Dawson LA, Hong TS, Thomas CR. Stereotactic body radiotherapy for patients with hepatocellular carcinoma and intermediate grade cirrhosis. Lancet Oncol. 2017;18(4):e192. doi:10.1016/S1470-2045(17)30162-6
178. Huo YR, Eslick GD. Transcatheter Arterial Chemoembolization Plus Radiotherapy Compared With Chemoembolization Alone for Hepatocellular Carcinoma. JAMA Oncol. 2015;1(6):756. doi:10.1001/jamaoncol.2015.2189
179. Lencioni R, Llovet JM, Han G, et al. Sorafenib or placebo plus TACE with doxorubicin-eluting beads for intermediate stage HCC: the SPACE trial. J Hepatol. 2016;64(5):1090–1098. doi:10.1016/j.jhep.2016.01.012
180. Meyer T, Fox R, Ma YT, et al. Sorafenib in combination with transarterial chemoembolisation in patients with unresectable hepatocellular carcinoma (TACE 2): a randomised placebo-controlled, double-blind, phase 3 trial. Lancet Gastroenterol Hepatol. 2017;2(8):565–575. doi:10.1016/S2468-1253(17)30156-5
181. Chao Y, Chung YH, Han G, et al. The combination of transcatheter arterial chemoembolization and sorafenib is well tolerated and effective in Asian patients with hepatocellular carcinoma: final results of the START trial. Int J Cancer. 2015;136(6):1458–1467. doi:10.1002/ijc.29126
182. Zou X, Fan W, Xue M, Li J. Evaluation of the Benefits of TACE Combined with Sorafenib for Hepatocellular Carcinoma Based on Untreatable TACE (unTACEable) Progression. Cancer Manag Res. 2021;13:4013–4029. doi:10.2147/CMAR.S304591
183. Han Y, Cao G, Sun B, et al. Regorafenib combined with transarterial chemoembolization for unresectable hepatocellular carcinoma: a real-world study. BMC Gastroenterol. 2021;21(1):393. doi:10.1186/s12876-021-01967-3
184. Kumar M, Panda D. Role of supportive care for terminal stage hepatocellular carcinoma. J Clin Exp Hepatol. 2014;4:S130–S139. doi:10.1016/j.jceh.2014.03.049
185. Schütte K, Balbisi F, Malfertheiner P. Prevention of Hepatocellular Carcinoma. Gastrointest Tumors. 2016;3(1):37–43. doi:10.1159/000446680
186. Singal AG, El-Serag HB. Hepatocellular carcinoma from epidemiology to prevention: translating knowledge into practice. Clin Gastroenterol Hepatol. 2015;13(12):2140–2151. doi:10.1016/j.cgh.2015.08.014
187. World Health Organization. Hepatitis B. Available from: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b.
188. Lange NF, Radu P, Dufour JF. Prevention of NAFLD-associated HCC: role of lifestyle and chemoprevention. J Hepatol. 2021;75(5):1217–1227. doi:10.1016/j.jhep.2021.07.025
189. Simon TG, Ma Y, Ludvigsson JF, et al. Association between aspirin use and risk of hepatocellular carcinoma. JAMA Oncol. 2018;4(12):1683. doi:10.1001/jamaoncol.2018.4154
190. Hayat U, Siddiqui AA, Okut H, Afroz S, Tasleem S, Haris A. The effect of coffee consumption on the non-alcoholic fatty liver disease and liver fibrosis: a meta-analysis of 11 epidemiological studies. Ann Hepatol. 2021;20:100254. doi:10.1016/j.aohep.2020.08.071
191. Cheng AL, Amarapurkar D, Chao Y, et al. Re-evaluating transarterial chemoembolization for the treatment of Hepatocellular Carcinoma: consensus recommendations and review by an International Expert Panel. Liver Int. 2014;34(2):174–183. doi:10.1111/liv.12314
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.