Back to Journals » International Journal of Nanomedicine » Volume 15
Egyptian Propolis-Loaded Nanoparticles as a Root Canal Nanosealer: Sealing Ability and in vivo Biocompatibility
Authors Abdel Raheem IA ![]() , Abdul Razek A, Elgendy AA
, Abdul Razek A, Elgendy AA ![]() , Labah DA, Saleh NM
, Labah DA, Saleh NM ![]()
Received 19 April 2020
Accepted for publication 8 July 2020
Published 27 July 2020 Volume 2020:15 Pages 5265—5277
DOI https://doi.org/10.2147/IJN.S258888
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Anderson Oliveira Lobo
Islam Ali Abdel Raheem,1 Amro Abdul Razek,1 Abeer Abdelaziz Elgendy,1 Doaa Ahmed Labah,2 Noha Mohamed Saleh3
1Endodontics Department, Faculty of Dentistry, Mansoura University, Mansoura, Egypt; 2Oral Biology and Dental Medicine Department, Faculty of Dentistry, Zagazig University, Zagazig, Egypt; 3Pharmaceutics Department, Faculty of Pharmacy, Mansoura University, Mansoura, Egypt
Correspondence: Noha Mohamed Saleh Email [email protected]
Background: Successful endodontic therapy is mainly governed by the satisfactory sealing ability of the applied root canal sealer. Also, tolerability of root canal structure to accommodate the presence of a sealer participates in the efficiency of the treatment. Hence, this study was aimed to extrapolate our previous one that was concerned with the preparation and evaluation of novel nature-based root canal sealers. Our current work is focused on the evaluation of sealing ability and in vivo biocompatibility.
Materials and Methods: Egyptian propolis was extracted (ProE) and encapsulated in polymeric nanoparticles (ProE-loaded NPs). Two root sealers, PE sealer and PE nanosealer, were fabricated by incorporating ProE and ProE-loaded NPs, respectively. The sealing ability of the developed sealers was tested by a dye extraction method. An in vivo biocompatibility study was conducted using a subcutaneous implantation method for two and four weeks. At the same time, a model sealer (AH Plus®) was subjected to the same procedures to enable accurate and equitable results.
Results: The teeth treated with PE sealer exhibited weak sealing ability which did not differ from that of unfilled teeth. PE nanosealer enhanced the sealing ability similarly to the model sealer with minimal apical microleakage. Studying in vivo biocompatibility indicated the capability of the three tested sealers to induce cell proliferation and tissue healing. However, PE nanosealer had superior biocompatibility, with higher potential for cell regeneration and tissue proliferation.
Conclusion: PE nanosealer can be presented as an innovative root canal sealer, with enhanced sealing ability as well as in vivo biocompatibility. It can be applied as a substitute for the currently available sealers that demonstrate hazardous effects.
Keywords: propolis, nanoparticles, root sealer, sealing ability, dye extraction, biocompatibility, subcutaneous implantation
Introduction
Root filling is the final step of the classic triad of endodontics that includes instrumentation, disinfection, and obturation. Effective endodontic treatment is mainly served by complete debridement of the root canal system, eradication of pathogenic microorganisms, and comprehensive filling of the canal space.1 Filling or obturation of the canal space is of paramount significance to prevent the entrance of bacteria from the oral environment, preclude coronal leakage, and avoid fluid accumulation.1,2 Hence, filling materials should accomplish a whole sealing, adaptation, and adhesion to the root canal wall. The association of a core filling material with a root canal sealer is considered as a typical procedure in endodontic obturation because the core material cannot directly attach to the dentin surface.3 The principal role of the core material is to passively fill the instrumented space and to serve as a piston for pressing the sealer one peripherally. Although many materials have been proposed as core fillings, gutta-percha has remained the material of choice for over a century and it is currently the standard of reference.1,4
Gutta-percha points consist of about 80% zinc oxide and some 20% beta-phase gutta-percha with a minute amount of coloring and softening agents.1 One important aspect that might severely compromise a proper seal is the shrinkage of backfill gutta-percha, with subsequent formation of irregularities and voids. Hence, a worthy sealer should be able to infiltrate deep into the dentinal tubules, fill formed irregularities, prevent percolation of fluids between gutta-percha and dentinal walls, and resist exterior microleakage of filling materials.1,5,6 The ability of a sealer to resist apical microleakage through the entire thickness is called “sealing ability.”7 Contact between gutta-percha and a sealer or between sealer and dentin cause contamination of root canals by oral bacteria, which can survive, propagate, and re-infect the surrounding tissues.7,8 For efficient root canal sealers, their leachable and biodegradable fractions should not exert an irritating effect on the peri-radicular tissues of the root canal system.9 Therefore, the pattern of tissue reaction and the inflammatory response towards an employed sealer are crucial to evaluate expected complications.10,11 The term “biocompatibility” is currently used to describe the tissue response to a sealing material. A biocompatible sealer is one that is able to exhibit an appropriate host response within a specific application.9 To sum up, there is a pressing need to evaluate the sealing ability and biocompatibility of a developed root sealer to assess its potential effectiveness in the clinical arena.
Due to leaching of their paraformaldehyde content, some of the currently used synthetic root canal sealers have induced irritation, toxicity, inflammatory modulation, and apical tissue degeneration.12 Propolis has been suggested to meet the necessities of a satisfactory sealer such as antimicrobial, anti-inflammatory, antioxidant, analgesic, and immuno-stimulating activities, as well as its success in enhancing regeneration of soft tissue.13,14 Moreover, Kuropatnicki et al reported the ability of propolis to induce hard tissue formation and promote bone regeneration.15 Thus, Egyptian propolis (honey glue) was extracted in our studies to obtain a remarkable bioactive resinous mixture (ProE) as a nature-based sealer.16
Due to the ability of bacteria to infiltrate, penetrate, and infect dentinal tubules, classical carriers of antimicrobial agents cannot get access to eradicate such deep infection.8,17 The penetration capability of an endodontic material to dentinal tubules is controlled by the size of the tubules, the number of the tubules, particle size, and setting reaction of the material.18 At the pulpal wall, the diameter of dentinal tubules ranges from 2.0 to 3.2 μm with the smallest ones being about 500 nm.19,20 The number of tubules varies according to their location; the average density of tubules is greatest in cervical dentin while these in radicular dentin display a significant reduction in number. Only materials with particle size smaller than the tubules’ diameter can penetrate.18
Nanotechnology, which deals with objects of nanometer size, has different applications in clinical dentistry. Nanoparticle applications have been presented as medication, as additives within sealers/restorative materials, or in irrigation solutions.21 Other applications of nanoparticles, such as antibacterial activity,22 reinforcement of composites,23 anti-biofilm properties,24 and biomimetic purposes,25 were studied. In endodontics, the application of nanoparticles has been primarily dedicated to the amalgamation of nanocomposites with different endodontic sealers. Silver nanoparticles have been studied for their use as an endodontic irrigator due to their high antimicrobial activity.26 Heid et al had reported the incorporation of nanometric bioactive glasses into a commercially available epoxy-resin root canal sealer.27 In a similar manner, other conventional endodontic sealers were combined with silver and chitosan nanoparticles to study their antimicrobial effectiveness.28 The effectiveness of calcium- and zinc-doped NPs in facilitating remineralization and reducing the permeability of dentin after endodontic treatment was evaluated.29
Nanotechnology was applied in our aforementioned study to enhance the physicochemical properties of ProE, improve its penetration ability, and optimize its manipulation. Polymeric PLGA-based nanoparticles (NPs) were loaded with ProE to serve as nanocarrier (ProE-loaded NPs). Nanoparticles by virtue of their size can penetrate into complex anatomies and there they can deliver entrapped active agents.17 Therefore, the inherent value of ProE-based sealer and ProE-loaded NPs as nanosealer was primarily highlighted as potential endodontic materials. The previously obtained outcomes of our developed sealers, such as prolonged release and accepted in vitro cytocompatibility as well as antimicrobial activity, encouraged us to extend their evaluation to the current appraisal study.
Hence, the aim of the present work was to extrapolate the examination of the developed ProE-based sealer (PE sealer) and nanosealer (PE nanosealer) to involve sealing ability and in vivo biocompatibility. To determine the appropriateness of the developed sealers in the clinical arena, the potential benefits should be balanced against the complications. For more accurate, realistic, and unbiased judgment, the benchmark standard was used and the currently approved sealer was used as the model sealer for comparing results.
Methodology
Materials
The following chemicals were used: Egyptian propolis (Mansoura, Province of Dakhahlia, Delta, Egypt), PDLGA®5010 (DL-lactide/glycolide 50/50, 153 KDa, Corbion, Amsterdam, the Netherlands), trehalose dihydrate (Sisco Research Laboratories Pvt Ltd, Mumbai, India), polyvinyl alcohol (PVA, 14 kDa, BDH, USA), hydroxypropyl methylcellulose (HPMC), Carbopol 940 (Colorcon Ltd, Orpington, UK), methylene blue (MB) (Sigma-Aldrich, St Louis, Missouri, USA), AH Plus® as a model of approved root canal sealers (Dentsply De Trey GmbH, Konstanz, Germany), nitric acid 69% extra pure, and thymol (Alpha Chemika, Mumbai, India), and anti-PCNA primary antibody (PC10) (Santa Cruz Biotechnology, Inc., Santa Cruz, California, USA). All other solvents and chemicals were of analytical grades.
Preparation of Root Canal Sealers
Samples of Egyptian propolis were collected from Dakhahlia province (Delta, Egypt) in April. The samples were extracted in the form of dried ethanolic extract (ProE). Then, ProE-loaded NPs were prepared using the nanoprecipitation method. Concisely, ProE (0.5%) and PDLGA (0.6%) were dissolved in 10 mL acetone to form an organic phase, that then was added dropwise to 40 mL of a stabilizer aqueous phase (2% PVA). After that, the obtained dispersion was subjected to sonication followed by solvent evaporation and centrifugation. NPs pellets were collected and lyophilized at −80°C using trehalose (5% w/v) to serve as a cryoprotectant. NPs-based root canal sealer (PE nanosealer) was prepared by incorporating ProE-loaded NPs in a gelling system of Carbopol 940 and HPMC K4M (0.6%:0.4% w/w). On the other hand, PE sealer was composed of ProE without extra treatment. For the model sealer, it is known as a past-paste system that delivered in two tubes. Paste A or epoxide paste contains di-epoxide, while 1-adamantane amine, N,N’-dibenzyl-5-oxa-nonandiamine-1,9, and TCD-diamine are the ingredients of amine paste (paste B). Both pastes were mixed according to the manufacturer’s instructions to prepare the model sealer. Sealers were freshly prepared under aseptic conditions just prior to application. Full details of propolis extraction, preparation of ProE-loaded NPs, and fabrication of sealers were extensively described in our aforementioned study.16
Evaluation of Sealing Ability
Sample Collection and Preparation
Sealing ability was evaluated using a modified method of Sinhal et al.30 Ethical approval (Code No. M13120219) of the study was obtained from the Research and Ethics Committee at the Faculty of Dentistry, Mansoura University. Forty-eight freshly extracted human single-rooted teeth (maxillary anterior teeth) were collected from fully informed patients. All patients provided informed consent for their extracted teeth to be used for research. To preclude the effect of dentinal sclerosis that changes with age and disease, the inclusion criteria of patients were male type I-diabetic subjects from 45 to 50 years old.31,32 Teeth with fractures, cracks, and caries, and previously restored, immature apices/root resorption, multiple canals, curvatures, and calcified canals were excluded. Soft tissues and calculus were removed by the aid of 5.25% sodium hypochlorite (NaOCl) and ultrasonic scaler (Varios 550, NSK, Nakanishi, Japan), respectively. Solutions of NaOCl were dilutions prepared from commercial preparations of Clorox bleach (Clorox Co., Oakland, CA, USA). After that, teeth were kept in 0.1% thymol solution at room temperature until use. Teeth were decoronated with a diamond disk (NTI® Interflex, Kerr, USA) to a fixed root length of 16 mm (digital Vernier caliper, Mitutoyo, model 500–144B, Tokyo, Japan), and the pulp tissues were removed with a barbed broach. To ensure patency, a size 10 K type file (MANI, Tokyo, Japan) was introduced into each root canal using a small back-and-forth motion. At that point, roots were instrumented with Revo-S™ (Micro-Mega, Besançon, France) in the following sequence; SC1, SC2, SU, AS30, AS35, and AS40 taper 0.06. The specimens were irrigated with NaOCl (2.6%) after each file followed by rinsing with EDTA (17%) and sterile water. Finally, the root canals were dried with a paper point.
Samples Grouping
The total sample size of forty-eight teeth (12 in each group) with an effect size of 0.5 was sufficient to acquire a power of 0.8 and a significance level of 0.05. The sample size was calculated using open source software (Gpower software 3.1, Universidad Düsseldorf, Düsseldorf, Germany). The prepared specimens were divided randomly into four groups; three treated groups and one control group. The teeth of the control group (Control) were enlarged, but not root-filled. The prepared root canals of the treated groups; Group I, Group II, and Group III were filled with PE sealer, PE nanosealer and the model sealer, respectively. Cold lateral condensation by size 40, 0.06 tapered (DiaDent, Seoul, Korea), and size 20, 0.02 tapered gutta-percha (Meta Biomed, Chungcheongbuk-do, Korea) was used as the root filling technique. After placement and condensation, the excess of gutta-percha was removed to the level of canal orifice by application of heat. All specimens were prepared and filled by the same operator. Also, the same number of secondary gutta-percha cones were used in the cold lateral condensation.
Apical Microleakage Evaluation by Dye Extraction Method
To allow setting of the sealer, the specimens were stored at 37°C and 100% humidity in an incubator for 24 hours.33 Then, the specimens with the exception of the first apical millimeter were coated with a layer of transparent nail varnish (RUNWAY, Egypt). The teeth were dipped in a preformulated aqueous solution of methylene blue (MB) at a concentration of 2% w/v. In a vacuum chamber (Heraeus, Liederkerke, Belgium), the teeth were kept under reduced pressure for 15 min to allow penetration of MB to unsealed voids and gapes. The specimens were then thoroughly rinsed with phosphate buffer saline pH 7.4 (PBS) to remove excess dye. Each tooth was transferred into a screw-capped glass tube containing 65% nitric acid and left for three days to allow complete dissolution. After that, the tubes were centrifuged at 10,000 rpm for 30 min to separate teeth debris from the extracted dye.34 The absorbance of the extracted dye in the supernatant was analyzed spectrophotometrically at 550 nm using concentrated nitric acid as a blank. Higher absorbance values mean more unsealed tubules, pores, and cavities were present in the root canal, which could be interpreted as lower sealing ability of the tested material and vice versa.
In vivo Biocompatibility Study
Our study protocol was reviewed and approved by the Research and Ethics Committee at the Faculty of Dentistry, Mansoura University that approved the protocols regarding animal experiments in accordance with “the Principles of Laboratory Animal Care” (NIH publication, 1985 revision). Twenty adult male Wistar albino rats with an average body weight of 180–200 g were used in this study. The sample size calculation was based on a previous study reported by Meneses et al.35 For each sealer, five animals were required per time point to provide reliable results with a statistical power of 80% and a significance level of 5% (Gpower software 3.1). Rats were housed in cages, labeled numerically, and kept in a well-ventilated animal house. Room temperature and humidity were maintained at 23°C and 60%, respectively, with normal photoperiod (12 h dark and 12 h light). The animals were fed with dry rat pellets and allowed drinking water ad libitum throughout the study period. Forty sterile clear polyethylene tubes (Well Lead Medical Co. Ltd, China) with 1.3 mm inner diameter and 10 mm length were divided into four groups (ten tubes/group). Each group was filled with a particular sealer to represent it. The first three tens were filled with PE sealer, PE nanosealer and the model sealer to designate Group I, Group II, and Group III, respectively. The last set of tubes was left empty to serve as a control (Control Group).
Surgical Procedures
Surgical procedures according to the method reported by Minotti et al were followed.36 After a one-week acclimatization period to the new laboratory environment, the animals were divided randomly into two equal sets. Animals were anesthetized by an intramuscular (IM) injection of 0.08 mL/kg ketamine and 0.04 mL/kg xylazine chloride (2%). The dorsum of each animal was shaved and rubbed with gauze soaked in 3% alcohol-iodine (Natural Herba Kings, Heckmondwike, England). In a head-to-tail orientation, a # 15 scalpel blade (Swann-Morton, Sheffield, England) was used to make two incisions (2 cm/each) with a separating distance of 1.6 cm. Subcutaneous tissue under each incision was dissected laterally with a blunt-end scissor to generate a pocket. One polyethylene tube was inserted as an implant in each pocket using surgical forceps, so that each animal received two implants of different sealers. The tubes of Group I and Group III were implanted in the first set of animals and the other set received the tubes of Group II and Control Group. This assignment of groups was followed to allow more facilitation and to standardize the number of sacrificed animals per time period. The incisions were sutured using mononylon stitch (0–4). To diminish the risk of infection, IM injection of penicillin (40,000 IU/mL, 1 mL/kg) was continued for 3 days postoperatively.36,37 Animals were clinically observed daily for any signs of infection and were maintained on their regular diets.
Specimens Collection and Tissues Preparation
Two and four weeks postoperatively, ten animals were sacrificed with an overdose of anesthetics, and their death was confirmed by cervical dislocation. Hair was shaved and incisions with a safety margin of 1 cm were made to remove the tubes with the surrounding tissues. Immediately, the specimens were fixed in a 10% buffered formaldehyde for 48 hours. After that, formalin-fixed specimens were dehydrated in ascending concentrations of ethyl alcohol, cleared in xylene, and then embedded in paraffin. Each block was sectioned using a microtome (Leica RM 2025, Nussloch, Baden-Wurttemberg, Germany) and five serial sections (5μm thick) were obtained.
Histologic and Immunohistochemical (IHC) Studies
For conventional histological assessment, one set of sections was picked up on slides, deparaffinized, and stained with hematoxylin and eosin (H&E).38 Other representative sections were prepared for IHC studies to assess the expression of proliferating cell nuclear antigen (PCNA) using the avidin-biotin complex (ABC) detecting method. The sections of IHC were deparaffinized by xylene and dehydrated through a descending series of ethanol concentrations. Then, the sections were washed with Tris-buffered saline (TBS; pH 7.4) and incubated in 0.3% H2O2 at room temperature for 30 min to block the activity of endogenous peroxidase. Antigen retrieval was performed according to the manufacture instructions. Slides were placed in 100 µL blocking solution (Abcam) for 30 minutes at room temperature. The sections were incubated with primary monoclonal antibodies at dilution 1:300 at 4ºC overnight. They were washed in PBS and incubated with secondary biotinylated antibody (anti-mouse) in blocking buffer for 1 hour at room temperature in a humidified chamber. To perform peroxidase visualization, the sections were incubated in ABC solution for 1 hour at room temperature. Color reaction was then developed by adding DAB solution (0.5 mg/mL DAB and 0.1% H2O) onto the sections. When the color reaction was satisfactory, it was stopped by rinsing with water for 5–10 minutes and the sections were counterstained with hematoxylin for 2 minutes. After that, the sections were gradually dehydrated and mounted with coverslips.
The slides were inspected and images were captured with a digital color CCD camera (Olympus, DP73, Tokyo, Japan) mounted on a light microscope (Olympus BX53, Tokyo, Japan). For IHC, the presence of brown-colored reaction localized in the nucleus was considered as positive PCNA reaction. The intensity of the immunostaining was classified as negative, weak, moderate, or strong from three fields in a blinded analysis performed by two experienced research associates. Immunostained images were further analyzed by ImageJ analysis (NIH, Bethesda, MD, USA) to quantitatively determine levels of PCNA expression in different groups.
Statistical Analysis
All measurement data were presented as mean ± standard deviation (SD). GraphPad Prism 6 software (San Diego, USA) was used for the statistical analysis. Gaussian assumption was checked via pretesting the normality of the data using the Shapiro–Wilk normality test. One-way analysis of variance (ANOVA) with Tukey–Kramer multiple comparison tests at a significance level of P < 0.05 were used to reveal statistical difference among groups.
Results and Discussion
Evaluation of Sealing Ability
Complete sealing of root canal is essential to obtain a fluid-tight seal which in turn results in the success of endodontic therapy. Endodontic failure is caused mainly by apical leakage which is affected by many factors such as physical and chemical properties of root canal sealer in addition to the applied filling technique.39 Moreover, shrinkage, overfilling, or stripping of gutta-percha from the carrier can result in negative impacts on the endodontic treatment.6,40 In recent decades, new materials have been introduced as root canal sealers. However, the different outcomes have demonstrated that so far no ideal sealing material has been achieved. Accepted sealers should provide optimal sealing ability, easy manipulation, biocompatibility, and ability of osteogenesis induction. Hence, apical leakage or sealing ability of a root sealer should be evaluated to assess its potential effectiveness if it is designed to be applied clinically.41
Different in vitro sealing ability tests have been reported in the literature. Methods such as bacterial penetration, isotopes, and electromechanical means could serve as the qualitative assessment of sealing ability. For more representative and quantitative measurement of microleakage, dye-penetration, dye-extraction, and fluid-infiltration techniques have been used.42 Due to the smaller size of dye molecules than the size of bacteria, the dye-penetration technique is not able to assess the exact volume of dye absorbed by a sample tooth. Instead, the dye-penetration technique merely measures the deepest point reached by the dye. In the fluid-infiltration technique, the filtration values have a habit to lessen over time as water penetrates all the irregularities till a plateau is gotten. In the dye-extraction-based technique, the whole tooth is dissolved in a concentrated acid. Complete dissolution of teeth guarantees release and extraction of all dye including that penetrating unsealed irregularities, the deepest and smallest dentinal tubules.30,33,41,42 The dye-extraction method is found to be a reliable, simple, widely used passive technique for volumetric determination of sealing ability.42,43 The capillarity principle is of great significance in the dye-extraction method for assessing apical leakage. Hence, the dye-extraction method was selected to be used in the present study. MB is a phenothiazinium compound that has been approved by the US Food and Drug Authority for broad applications. It is a cationic water-soluble, simple, available, and convenient dye with a molecular size of 0.84 nm.44 As a tooth is immersed in MB aqueous solution, dye molecules can freely penetrate through the smallest dentinal tubules to fill all spaces between the dentinal walls and root canal sealer.30,42
Figure 1 shows the absorbance values of the dye extracted from the control and treated groups. It was understandable that Control Group exhibited the lowest value of sealing ability (absorbance of 0.6703 ± 0.18 at 550 nm) due to the lack of sealer application. The root-filled groups showed absorbance values of 0.6588 ± 0.37, 0.3391 ± 0.15, and 0.2048 ± 0.1 for Group I, Group II, and Group III, respectively. Statistical analysis of the abovementioned results showed that Group II and Group III had comparable sealing abilities accompanied by a minimal degree of microleakage (P > 0.05). As the model sealer is considered as a benchmark “Gold Standard,”45 such analogous sealing ability of our developed PE nanosealer has indicated a noteworthy potential role of it in the field of endodontics. It is significant for a proper sealer to reach the smallest dentinal tubules that ranged from 500 nm to 1 μm.19 PE nanosealer could meet this condition due to its nanosized particles of about 200 nm (data shown in our previous study).16 Such nanosize might permit efficient penetration of PE nanosealer to fill the lateral microcanals over the dentinal walls. Moreover, hydrophobicity and slow degradability of PDLGA could afford more resistance of PE nanosealer to dissolve or leak after application. However, the sealing ability of the model sealer could be attributed to its ability to mechanically interlock the root dentin and its penetration into the micro-irregularities in dentinal walls of the root canal.33 On the other hand, the PE sealer exhibited significantly lower sealing ability than those of the PE nanosealer (P < 0.01) and the model sealer (P < 0.001), as shown in Figure 1. At the same time, the PE sealer exhibited a comparable sealing ability to that of Control (P > 0.05). The sealing ability of Control Group was significantly lower than the corresponding values of Group II (P < 0.01) and Group III (P < 0.001). Weak sealing ability of PE sealer could be attributed to the fact that its application was relatively constrained by the sticky nature of ProE (honey glue). Hence, a special applicator with programmed temperature is suggested to be designed to facilitate its application in the future. During the experiment, some sort of PE sealer macroleakage associated with marked teeth staining was actually noticed after the incubation step. Such findings might be responsible for its trivial sealing ability. Superior qualities, rapid and clean mixing associated with good handling capabilities of PE nanosealer over PE sealer have indicated the outstanding profits of nanotechnology. Hence, the PE nanosealer deserves to undergo further assessment and could, later on, be a potential novel nature-based root canal nanosealer.
 |
Figure 1 Absorbance values of MB extracted from Control Group (non-root-filled teeth), Group I (PE sealer), Group II (PE nanosealer) and Group III (the model sealer). Notes: **Means significant difference at P < 0.01; ***means significant difference at P < 0.001; ns means non-significant difference at P > 0.05.Abbreviation: MB, methylene blue. |
In vivo Biocompatibility Study
To perform satisfactorily during years of service, root sealers must not produce abnormal responses in periapical tissues and should not induce toxic or carcinogenic properties, either locally or systemically. One of the most reliable in vivo methods to evaluate the biocompatibility of root canal sealers is the subcutaneous surgical implantation of the sealer material in animals.46,47 Albino rats of Wistar strain were used in the present study because of their availability, easy handling, less sensitivity to infection after surgery, being economically viable, and presenting an acceptable model for determining biocompatibility of materials.48 To ensure standardization and similarity to the clinical situation, polyethylene tubes were used in this study. These tubes are known to be neutral and efficiently put the examined materials in contact with the surrounding tissues. Hence, this technique allowed us to simulate the responses that occur in the periapical region after the obturation of root canals.37,47 Rats of the current study were found to be healthy throughout the experimental periods and seemed to tolerate the anesthesia and surgical procedure. Examination of the wound site on the dorsal surface of all rats revealed that Group II, Group III, and Control Group showed satisfactory wound healing and lacked obvious signs of infection at the site of the wound throughout the two experimental periods. However, in Group I there was an apparent edematous area at the site of wound healing four weeks postoperatively.
Histological Findings
Figure 2 illustrates H&E stained sections two weeks postoperatively of Group I (A), Group II (B), Group III (C), and Control Group (D). Histological sections of the tubes and the surrounding tissues from different groups revealed variable degrees of healing and formation of a fibrocellular capsule juxtaposed to the polyethylene tubes. In Group I, the formed capsule was relatively thin and contained some collagen fibers and fibroblasts along with several interstitial spaces (Figure 2A). For Group II, there was dense fibrous connective tissue rich in fibroblasts and collagen fibers which appeared thicker and more organized than in Group I (Figure 2B). These results denoted that the PE nanosealer promoted more advanced healing degree than the PE sealer. This outcome could be explained by the ability of ProE-loaded NPs to deliver ProE at the wound site and to target the complexity of the normal wound healing process more efficiently than their original counterpart (ProE).49 Both Group I and Group II disclosed a few inflammatory cells close to the tubes. This mild inflammatory reaction probably originated from the surgical trauma.50 On the other hand, Group III displayed fibrous connective tissue formation with thick collagen fibers and few fibroblasts. Macrophage/multinucleated giant cells were more evident adjacent to Group III tubes than other groups (Figure 2C). These results are comparable with that of Batista et al51 and Grecca et al37 who stated that the model sealer was more aggressive during the initial periods of contact with connective tissues than the other tested materials and this aggression might be reduced over time. In Control Group, a thin connective tissue capsule formed of thin collagen fibers, few fibroblasts, and many interstitial spaces was obvious nearby the empty tube (Figure 2D). The perceived inflammatory reaction adjacent to an empty polyethylene tube could indicate its suitability as a control.52
 |
Figure 2 Histologic evaluation of in vivo biocompatibility after two weeks of subcutaneous implantation in rats. Notes: (A) Group I, (B) Group II, (C) Group III, and (D) Control. Black arrows point to multinucleated giant cells. Blue arrows point to collagen fibers. Green arrows point to inflammatory cells. PT points to the area of polyethylene tube implant. Yellow arrows point to fibroblasts. H&E, 400×.Abbreviation: H&E, hematoxylin and eosin. |
Figure 3 illustrates H&E stained sections four weeks postoperatively of Group I (A), Group II (B), Group III (C), and Control Group (D). Group I showed a network of loosely arranged collagen fiber and several fibroblasts. Severe inflammatory cell infiltration and vascular congestion were evident adjacent to Group I tubes (Figure 3A). These histological findings could explain the noticeable edematous area of Group I at the site of the wound. This could indicate that the tissues became no longer able to tolerate the PE sealer. Similar outcomes were reported by Jolly et al.53 On the other hand, some scholars pointed out that propolis could lead to normal tissue reorganization without increased vascular or cellular events.54,55 Also, Ramous et al verified low periapical tissue responses towards propolis paste.56 The influence of geographical position, bee species, harvesting season, and botanical origin on the composition of propolis could be responsible for the variation of bioactivity and biocompatibility.57,58
 |
Figure 3 Histologic evaluation of in vivo biocompatibility after four weeks of subcutaneous implantation in rats. Notes: (A) Group I, (B) Group II, (C) Group III, and (D) Control. Asterisk points to vascular congestion. Green arrows point to inflammatory cells. PT points to the area of polyethylene tube implant. Red arrows point to blood capillaries. H&E, 400×.Abbreviation: H&E, hematoxylin and eosin. |
Interestingly, Group II revealed properly organized thick fibrous vascularized connective tissue with denser bundles of collagen fibers and several elongated fibroblasts. There was a mild inflammatory reaction and a minimal amount of inflammatory cells appeared in close proximity to PE nanosealer tubes (Figure 3B). This observation was considered as a proof of acceptable tissue tolerance towards this material. These findings are in the agreement with Elgendy and Fayyad who proved that milling-induced propolis nanoparticles were less cytotoxic and induced less apoptotic changes than propolis in its original untreated form.59 On the other hand, Group III showed an apparent disorganized collagen fiber network with fibroblasts, moderate inflammatory cell infiltration, and discrete angiogenesis (Figure 3C). It indicated that the model sealer had extended its early noticed aggressive effect to the second time period. Control Group showed fibrous connective tissue with organized collagen fibers and fibroblasts of various sizes and some interstitial spaces were still noticeable. The fibrous connective tissue deposition in Control Group appeared to have a slower rate than those of other groups (Figure 3D).
PCNA IHC
PCNA is a ubiquitous cell cycle marker protein that plays an essential role in DNA replication, DNA repair, cell cycle progression, and cell proliferation.60 Different patterns of PCNA staining are believed to correlate with phases of the cell cycles. Therefore, the intensity of positive signals generated by PCNA IHC can be related to the degree of cell proliferation.61,62 Figures 4 and 5 illustrate, respectively, the IHC stained sections of Group I (A), Group II (B), Group III (C), and Control Group (D) two and four weeks postoperatively. PCNA immunoreactivity two weeks postoperatively revealed weak nuclear expression in Control Group, weak to moderate expression in Group I, moderate expression in Group III whereas stronger expression was evident in Group II (Figure 4A–D). Four weeks postoperatively displayed moderate PCNA nuclear expression in both Control group and Group I while Group II and Group III showed strong expression (Figure 5A–D).
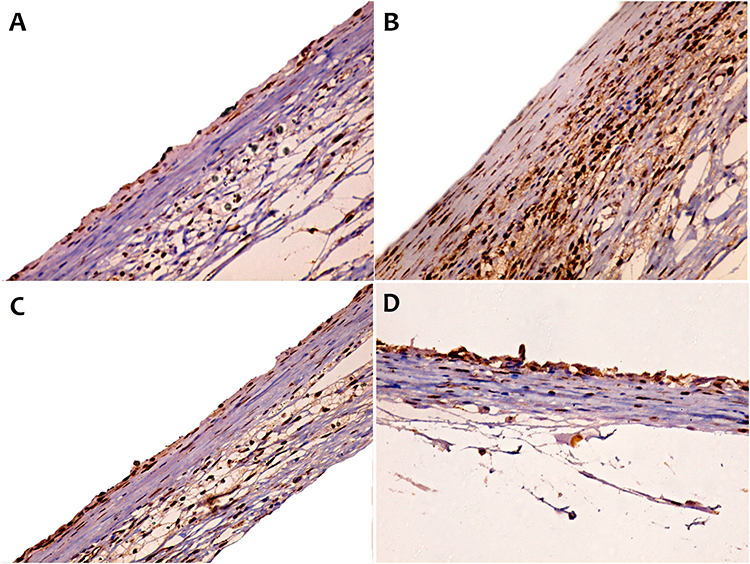 |
Figure 4 IHC estimation of PCNA expression in rats after two weeks of subcutaneous implantation. |
 |
Figure 5 IHC estimation of PCNA expression in rats after four weeks of subcutaneous implantation. |
Table 1 documents the quantitative representation of PCNA expression and its statistical analysis two and four weeks postoperatively. The values of PCNA expression were 46 ± 6.06, 179 ± 11.46, 70.25 ± 6.55, and 29.75 ± 4.57 for Group I, Group II, Group III, and Control Group, respectively, after two weeks. It was evident that Group II demonstrated a significant increase of PCNA expression in comparison to those of Group I, Group III, and Control Group (P < 0.001). Moreover, Group III showed a significant increase in its PCNA expression compared to both Group I and Control Group (P < 0.001). Also, Group I exhibited significant increased PCNA expression compared to Control Group (P < 0.05).
 |
Table 1 Expression Levels of PCNA Two and Four Weeks Postoperatively in Different Groups |
Four weeks postoperatively, Group I, Group II, Group III, and Control depicted PCNA expression levels of 328 ± 70.14, 461 ± 55.59, 474.5 ± 53.97, and 325.25 ± 56.75, respectively. The statistical analysis documented that PCNA expression of Group II and Group III was comparable (P > 0.05). Also, it was found that Group II and Group III displayed significantly higher expression levels in comparison to those of Group I and Control Group (P < 0.01). PCNA expression of Group I and Control Group showed a non-significant difference (P > 0.05). In addition, statistical analysis demonstrated a marked significant increase of PCNA expressions in all groups four weeks postoperatively in comparison with their corresponding values after two weeks (P < 0.001).
Although results of in vivo biocompatibility indicated the capability of the three tested sealers to induce cell proliferation and tissue healing, the PE nanosealer had the superior tissue proliferation potential. The biodegradable nature of PDLGA by enzymatic pathways into physiological tolerant products, lactic acids and glycolic acids, might exhibit very limited toxicity to the surrounding tissues.63 Actually, PDLGA can provide a wide range of degradation rates from months to years and it is the most frequently applied polymer in tissue engineering.64,65 Moreover, it was found that ProE-loaded NPs had respectable antimicrobial activity as reported in our previous study.16 Hence, smart ProE-loaded NPs could release the loaded ProE with a prudent and prolonged pattern without interfering with tissue healing. We must keep in our mind that the model sealer is a resin-based type in which bisphenol A diglycidyl ether has a mutagenic effect.66,67 As well, formaldehyde, amine, and other epoxy resins were reported to leach from this sealer to the neighboring tissues.67–69 Such evidence might be the cause of the noticed aggressive effect of the model sealer towards adjacent tissues.
In the case of PE sealer, it was thought that tissues were subjected to a large amount of naked ProE at once and they were not able to tolerate it. In vitro release of ProE from its unprocessed form was found to continue as one phase, with a faster rate than that of ProE-loaded NPs (our previous study).16 This could result in negative influences on cell proliferation and tissue regeneration during the first time period (two weeks). Depletion of PE sealer might occur after four weeks of implantation but the apparent edema in Group I indicated further tissue reaction and clear intolerance to this sealer. To sum up, it can be concluded that the nanotechnology-induced changes of the physicochemical properties of ProE were accompanied by positive aspects of its biological activity. Taking all results together, we report new evidence in favor of the use of the PE nanosealer as a nature-based root nanosealer and it deserves further investigation including clinical trials.
Conclusion
Nature grants us with a wide range of biologically active materials. Modulating the properties of these materials enables their use as therapeutics. Propolis has antimicrobial, anti-inflammatory, antioxidant, analgesic, and tissue regeneration activities. Nanotechnology could be used to enhance the physicochemical properties of propolis, improve its penetration, and optimize its manipulation. In our studies, propolis-based nanoparticles were used to prepare an efficient root canal sealer (PE nanosealer). The attractive and reasonable outcomes of the PE nanosealer via its extensive evaluation in our previous and current studies were proven with in vitro and in vivo studies. Eventually, the PE nanosealer deserves to be produced on a large scale and to undergo further assessment via clinical trials. Currently, further studies investigating its clinical convenience are in progress.
Abbreviations
ABC, avidin–biotin complex; ANOVA, one-way analysis of variance; DAB, 1,4-dideoxy-1,4-imino-d-arabinitol; H&E, hematoxylin and eosin; HPMC, hydroxypropyl methylcellulose; IHC, immunohistochemical studies; MB, methylene blue; NaOCl, sodium hypochlorite; NPs, nanoparticles; PBS, phosphate buffer saline pH 7.4; PCNA, proliferating cell nuclear antigen; PDLGA, DL-lactide/glycolide copolymer; ProE, ethanolic extract of Egyptian propolis; PT, polyethylene tube; PVA, polyvinyl alcohol; TBS, Tris-buffered saline pH 7.4.
Disclosure
The authors report that they have no competing interests in this work.
References
1. Ørstavik D. Obturation of root canals. In: Chugal N, Lin LM editors. Endodontic Prognosis: Clinical Guide for Optimal Treatment Outcome. Springer International Publishing; 2017:141–159. doi:10.1007/978-3-319-42412-5_9.
2. Adl AR, Sobhnamayan F, Shojaee NS, Azizi S. A comparison of push-out bond strength of two endodontic sealers to root canal dentin: an in vitro study. J Dent Biomater. 2016;3(1):199–204.
3. Plotino G, Venturi M, Grande NM. Complications due to root canal filling procedures. In: Jain P editor. Common Complications in Endodontics: Prevention and Management. Springer International Publishing; 2018:101–146. doi:10.1007/978-3-319-60997-3_6.
4. Bodrumlu E, Tunga U. Coronal sealing ability of a new root canal filling material. JCDA. 2007;73(7):623–623c.
5. Timpawat S, Amornchat C, Trisuwan W. Bacterial coronal leakage after obturation with three root canal sealers. J Endod. 2001;27(1):36–39. doi:10.1097/00004770-200101000-00011
6. Lottanti S, Tauböck TT, Zehnder M. Shrinkage of backfill gutta-percha upon cooling. J Endod. 2014;40(5):721–724. doi:10.1016/j.joen.2013.09.043
7. Nabeel M, Tawfik HM, Abu-Seida AMA, Elgendy AA. Sealing ability of Biodentine versus ProRoot mineral trioxide aggregate as root-end filling materials. Saudi Dent J. 2019;31(1):16–22. doi:10.1016/j.sdentj.2018.08.001
8. Fan W, Wu D, Tay FR, Ma T, Wu Y, Fan B. Effects of adsorbed and templated nanosilver in mesoporous calcium-silicate nanoparticles on inhibition of bacteria colonization of dentin. Int J Nanomedicine. 2014;9:5217–5230. doi:10.2147/IJN.S73144
9. Ghanaati S, Willershausen I, Barbeck M, et al. Tissue reaction to sealing materials: different view at biocompatibility. Eur J Med Res. 2010;15(11):483. doi:10.1186/2047-783X-15-11-483
10. Mohammadi Z, Karim Soltani M, Shalavi S, Yazdizadeh M, Jafarzadeh M. Calcium hydroxide-based root canal sealers: an updated literature review. Compend Contin Educ Dent Jamesburg NJ. 2014;35(5):334–339.
11. Royer K, Liu XJ, Zhu Q, Malmstrom H, Ren Y-F. Apical and root canal space sealing abilities of resin and glass ionomer-based root canal obturation systems. Chin J Dent Res off J Sci Sect Chin Stomatol Assoc CSA. 2013;16(1):47–53.
12. Silva EJNL, Accorsi-Mendonça T, Almeida JFA, Ferraz CCR, Gomes BPFA, Zaia AA. Evaluation of cytotoxicity and up-regulation of gelatinases in human fibroblast cells by four root canal sealers: sealers cytotoxic and up-regulation of gelatinases. Int Endod J. 2012;45(1):49–56. doi:10.1111/j.1365-2591.2011.01946.x
13. Bruschi ML, Jones DS, Panzeri H, Gremião MPD, de Freitas O, Lara EHG. Semisolid systems containing propolis for the treatment of periodontal disease: in vitro release kinetics, syringeability, rheological, textural, and mucoadhesive properties. J Pharm Sci. 2007;96(8):2074–2089. doi:10.1002/jps.20843
14. Bruschi ML, Rosseto HC, de Francisco LMB, et al. Nanostructured propolis as therapeutic systems with antimicrobial activity. In: Grumezescu AM editor. Nano- and Microscale Drug Delivery Systems. Elsevier; 2017:377–391. doi:10.1016/B978-0-323-52727-9.00020-0.
15. Kuropatnicki AK, Szliszka E, Kłósek M, Król W. The beginnings of modern research on propolis in Poland. Evid Based Complement Alternat Med. 2013;2013:1–6. doi:10.1155/2013/983974
16. Abdel Raheem IA, Abdul Razek A, Elgendy AA, Saleh NM, Shaaban MI, Abd El-Hady FK. Design, evaluation and antimicrobial activity of egyptian propolis-loaded nanoparticles: intrinsic role as a novel and naturally based root canal nanosealer. Int J Nanomedicine. 2019;14:8379–8398. doi:10.2147/IJN.S219577
17. Shrestha A, Fong S-W, Khoo B-C, Kishen A. Delivery of antibacterial nanoparticles into dentinal tubules using high-intensity focused ultrasound. J Endod. 2009;35(7):1028–1033. doi:10.1016/j.joen.2009.04.015
18. Bird DC, Komabayashi T, Guo L, Opperman LA, Spears R. In vitro evaluation of dentinal tubule penetration and biomineralization ability of a new root-end filling material. J Endod. 2012;38(8):1093–1096. doi:10.1016/j.joen.2012.04.017
19. Komabayashi T, Nonomura G, Watanabe LG, Marshall Jr GW, Marshall SJ. Dentin tubule numerical density variations below the CEJ. J Dent. 2008;36(11):953–958. doi:10.1016/j.jdent.2008.08.002
20. Seyedkavoosi S, Sevostianov I. Multiscale micromechanical modeling of the elastic properties of dentin. J Mech Behav Biomed Mater. 2019;100:103397. doi:10.1016/j.jmbbm.2019.103397
21. Ibrahim AIO, Moodley DS, Petrik L, Patel N. Use of antibacterial nanoparticles in Endodontics. SADJ. 2017;72(3):105–112.
22. Cheng L, Weir MD, Xu HHK, et al. Antibacterial amorphous calcium phosphate nanocomposites with a quaternary ammonium dimethacrylate and silver nanoparticles. Dent Mater. 2012;28(5):561–572. doi:10.1016/j.dental.2012.01.005
23. Scribante A, Massironi S, Pieraccini G, et al. Effects of nanofillers on mechanical properties of fiber-reinforced composites polymerized with light-curing and additional postcuring. J Appl Biomater Funct Mater. 2015;13(3):296–299. doi:10.5301/jabfm.5000226
24. Cheng L, Zhang K, Melo MAS, Weir MD, Zhou X, Xu HHK. Anti-biofilm dentin primer with quaternary ammonium and silver nanoparticles. J Dent Res. 2012;91(6):598–604. doi:10.1177/0022034512444128
25. Scribante A, Dermenaki Farahani MR, Marino G, et al. Biomimetic effect of nano-hydroxyapatite in demineralized enamel before orthodontic bonding of brackets and attachments: visual, adhesion strength, and hardness in in vitro tests. Biomed Res Int. 2020;2020:1–9. doi:10.1155/2020/6747498
26. Salas-Orozco M, Niño-Martínez N, Martínez-Castañón G-A, Méndez FT, Jasso MEC, Ruiz F. Mechanisms of resistance to silver nanoparticles in endodontic bacteria: a literature review. J Nanomater. 2019;2019:1–11. doi:10.1155/2019/7630316
27. Heid S, Stoessel PR, Tauböck TT, Stark WJ, Zehnder M, Mohn D. Incorporation of particulate bioactive glasses into a dental root canal sealer. Biomed Glas. 2016;2:29–37. doi:10.1515/bglass-2016-0004
28. Loyola-Rodríguez JP, Torres-Méndez F, Espinosa-Cristobal LF, et al. Antimicrobial activity of endodontic sealers and medications containing chitosan and silver nanoparticles against Enterococcus faecalis. J Appl Biomater Funct Mater. 2019;17(3):1–9. doi:10.1177/2280800019851771
29. Toledano M, Osorio E, Aguilera FS, et al. Polymeric nanoparticles for endodontic therapy. J Mech Behav Biomed Mater. 2020;103:1–51. doi:10.1016/j.jmbbm.2019.103606
30. Sinhal TM, Shah RRP, Jais PS, et al. An in vitro comparison and evaluation of sealing ability of newly introduced C-point system, cold lateral condensation, and thermoplasticized gutta-percha obturating technique: a dye extraction study. Contemp Clin Dent. 2018;9(2):164–169. doi:10.4103/ccd.ccd_722_17
31. Kakoli P, Nandakumar R, Romberg E, Arola D, Fouad AF. The effect of age on bacterial penetration of radicular dentin. J Endod. 2009;35(1):78–81. doi:10.1016/j.joen.2008.10.004
32. Atar M, Körperich EJ. Systemic disorders and their influence on the development of dental hard tissues: a literature review. J Dent. 2010;38(4):296–306. doi:10.1016/j.jdent.2009.12.001
33. Kataia EM, Kataia MM. Dye extraction method evaluation of the sealing ability of three types of endodontic sealers. Egypt Dent J. 2016;62:251–256. doi:10.21608/edj.2016.92668
34. Tandan M, Hegde MN, Hegde P. Effect of four different intracanal medicaments on the apical seal of the root canal system: a dye extraction study. Indian J Dent Res. 2014;25(5):607–612. doi:10.4103/0970-9290.147104
35. Meneses IHC, De, Sampaio GA, de M, et al. In vivo biocompatibility, mechanical, and antibacterial properties of cements modified with propolis in different concentrations. Eur J Dent. 2020;14(01):77–84. doi:10.1055/s-0040-1702255
36. Minotti PG, Ordinola-Zapata R, Midena RZ, et al. Rat subcutaneous tissue response to calcium silicate containing different arsenic concentrations. J Appl Oral Sci. 2015;23(1):42–48. doi:10.1590/1678-775720130523
37. Grecca FS, Kopper PMP, Santos Dos RB, et al. Biocompatibility of RealSeal, its primer and AH plus implanted in subcutaneous connective tissue of rats. J Appl Oral Sci. 2011;19(1):52–56. doi:10.1590/S1678-77572011000100011
38. Bancroft JD, ed. Theory and Practice of Histological Techniques. Elsevier Health Sciences; 2008.
39. Salem AS, Saleh ARM, Elmasmari HAA. In vitro assessment of apical leakage of bioceramic endodontic sealer with two obturation techniques. Open Dent J. 2018;12(1):1162–1168. doi:10.2174/1874210601812011162
40. Raghuwanshi S, Jain P, Patni PM, Pandey SH, Hiremath H, Baghel S. Dentinal adaptation of warm thermoplastic obturating material and cold thermoplastic obturating material: an in vitro study. Contemp Clin Dent. 2019;10(1):64–68. doi:10.4103/ccd.ccd_312_18
41. Reddy NV, Srujana P, Daneswari V, Konyala HR, Mareddy AR, Mohammad N. Sealing ability of MTA vs Portland cement in the repair of furcal perforations of primary molars: a dye extraction leakage model—an in vitro study. Int J Clin Pediatr Dent. 2019;12(2):83–87. doi:10.5005/jp-journals-10005-1597
42. Uysal İ. Comparison of apical microleakage of dual-curing resin cements with fluid-filtration and dye extraction techniques. Med Sci Monit. 2015;21:937–944. doi:10.12659/MSM.892741
43. Camps J, Pashley D. Reliability of the dye penetration studies. J Endod. 2003;29(9):592–594. doi:10.1097/00004770-200309000-00012
44. Guarín JR, Moreno-Pirajan JC, Giraldo L. Kinetic study of the bioadsorption of methylene blue on the surface of the biomass obtained from the algae D. Antarctica J Chem. 2018;2018:1–12. doi:10.1155/2018/2124845
45. Azar NG, Heidari M, Bahrami ZS, Shokri F. In vitro cytotoxicity of a new epoxy resin root canal sealer. J Endod. 2000;26(8):462–465. doi:10.1097/00004770-200008000-00008
46. Christian Gomes Moura C, Cristina Cunha T, Oliveira Crema V, Dechichi P, Carlos Gabrielli Biffi J. A study on biocompatibility of three endodontic sealers: intensity and duration of tissue irritation. Iran Endod J. 2014;9(2):137–143.
47. Silva‐Herzog D, Ramírez T, Mora J, et al. Preliminary study of the inflammatory response to subcutaneous implantation of three root canal sealers. Int Endod J. 2011;44(5):440–446. doi:10.1111/j.1365-2591.2011.01849.x
48. Farhad AR, Hasheminia S, Razavi S, Feizi M. Histopathologic evaluation of subcutaneous tissue response to three endodontic sealers in rats. J Oral Sci. 2011;53(1):15–21. doi:10.2334/josnusd.53.15
49. Chakrabarti S, Chattopadhyay P, Islam J, Ray S, Raju PS, Mazumder B. Aspects of nanomaterials in wound healing. Curr Drug Deliv. 2019;16(1):26–41. doi:10.2174/1567201815666180918110134
50. Sönmez NS, Sönmez E, Akçaboy C. Evaluation of biocompatibility of targis dentin and artglass by using subcutaneous implantation test. Indian J Dent Res. 2010;21(4):537–543. doi:10.4103/0970-9290.74211
51. Batista RFC, Hidalgo MM, Hernandes L, et al. Microscopic analysis of subcutaneous reactions to endodontic sealer implants in rats. J Biomed Mater Res A. 2007;81A(1):171–177. doi:10.1002/jbm.a.30918
52. Silveira CMM, Pinto SCS, Zedebski R, de AM, Santos FA, Pilatti GL. Biocompatibility of four root canal sealers: a histopathological evaluation in rat subcutaneous connective tissue. Braz Dent J. 2011;22(1):21–27. doi:10.1590/S0103-64402011000100003
53. Jolly M, Singh N, Rathore M, Tandon S, Sharma S. Propolis and commonly used intracanal irrigants. comparative evaluation of inflammatory potential. J Clin Pediatr Dent. 2013;37(4):373–376. doi:10.17796/jcpd.37.4.l4t31237p5723784
54. Al-Shaher A, Wallace J, Agarwal S, Bretz W, Baugh D. Effect of propolis on human fibroblasts from the pulp and periodontal ligament. J Endod. 2004;30(5):359–361. doi:10.1097/00004770-200405000-00012
55. da Silva FB, de Almeida JM, de Sousa SMG. Natural medicaments in endodontics: a comparative study of the anti-inflammatory action. Braz Oral Res. 2004;18(2):174–179. doi:10.1590/S1806-83242004000200015
56. Ramos IF, de AS, Biz MT, et al. Histopathological analysis of corticosteroid-antibiotic preparation and propolis paste formulation as intracanal medication after pulpectomy: an in vivo study. J Appl Oral Sci. 2012;20(1):50–56. doi:10.1590/S1678-77572012000100010
57. Silici S, Kutluca S. Chemical composition and antibacterial activity of propolis collected by three different races of honeybees in the same region. J Ethnopharmacol. 2005;99(1):69–73. doi:10.1016/j.jep.2005.01.046
58. Toreti VC, Sato HH, Pastore GM, Park YK. Recent progress of propolis for its biological and chemical compositions and its botanical origin. Evid Based Complement Alternat Med. 2013;2013:1–13. doi:10.1155/2013/697390
59. Elgendy A, Fayyad D. Cell viability and apoptotic changes of dental pulp stem cells treated with propolis, chitosan, and their nano counterparts. Tanta Dent J. 2017;14(4):198–207. doi:10.4103/tdj.tdj_27_17
60. Naryzhny SN. Proliferating cell nuclear antigen: a proteomics view. Cell Mol Life Sci. 2008;65(23):3789–3808. doi:10.1007/s00018-008-8305-x
61. Strzalka W, Ziemienowicz A. Proliferating cell nuclear antigen (PCNA): a key factor in DNA replication and cell cycle regulation. Ann Bot. 2011;107(7):1127–1140. doi:10.1093/aob/mcq243
62. Adan A, Kiraz Y, Baran Y. Cell proliferation and cytotoxicity assays. Curr Pharm Biotechnol. 2016;17(14):1213–1221. doi:10.2174/1389201017666160808160513
63. Salama HA, Ghorab M, Mahmoud AA, Abdel Hady M. PLGA nanoparticles as subconjunctival injection for management of glaucoma. AAPS PharmSciTech. 2017;18(7):2517–2528. doi:10.1208/s12249-017-0710-8
64. Cao Y, Mitchell G, Messina A, et al. The influence of architecture on degradation and tissue ingrowth into three-dimensional poly(lactic-co-glycolic acid) scaffolds in vitro and in vivo. Biomaterials. 2006;27(14):2854–2864. doi:10.1016/j.biomaterials.2005.12.015
65. Mainardes RM, Gremião MPD, Evangelista RC. Thermoanalytical study of praziquantel-loaded PLGA nanoparticles. Rev Bras Ciênc Farm. 2006;42(4):523–530. doi:10.1590/S1516-93322006000400007
66. Colak KM, Keles A, Bayrak OF, Koseoglu M, Sahin F. Study of cytotoxicity of six root canal sealing dental materials. Mater Res Innov. 2009;13(4):415–420. doi:10.1179/143289109X12494867167161
67. Jung S, Sielker S, Hanisch MR, Libricht V, Schäfer E, Dammaschke T. Cytotoxic effects of four different root canal sealers on human osteoblasts. PLoS One. 2018;13(3):e0194467. doi:10.1371/journal.pone.0194467
68. Eldeniz AU, Mustafa K, Ørstavik D, Dahl JE. Cytotoxicity of new resin-, calcium hydroxide- and silicone-based root canal sealers on fibroblasts derived from human gingiva and L929 cell lines. Int Endod J. 2007;40(5):329–337. doi:10.1111/j.1365-2591.2007.01211.x
69. Anumula L, Kumar S, Kumar VS, et al. An assessment of antibacterial activity of four endodontic sealers on Enterococcus faecalis by a direct contact test: an in vitro study. ISRN Dent. 2012;2012:1–5. doi:10.5402/2012/989781
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.