Back to Journals » International Journal of Nanomedicine » Volume 21
EGCG-Building Nanocarriers for Multitasking Drug Delivery: Design Principles, Therapeutic Opportunities, and Translational Challenges
Authors Yongvongsoontorn N ![]() , Kurisawa M
, Kurisawa M ![]() , Chung JE
, Chung JE ![]()
Received 25 March 2026
Accepted for publication 1 June 2026
Published 30 June 2026 Volume 2026:21 558394
DOI https://doi.org/10.2147/IJN.S558394
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Lijie Grace Zhang
Yongvongsoontorn N, Kurisawa M, Chung JE
Graduate School of Advanced Science and Technology, Japan Advanced Institute of Science and Technology, Nomi, Ishikawa, 923-1292, Japan
Correspondence: Motoichi Kurisawa, Email [email protected]
Joo Eun Chung, Email [email protected]
Recent advances in nanotechnology for drug delivery have enabled improved pharmacokinetics, controlled drug release, and enhanced tissue targeting. However, the clinical impact of many nanocarrier systems remains limited because most carriers exhibit typically low drug loading, resulting in modest therapeutic benefit and concerns related to excipient burden. Conventional nanocarriers are often composed predominantly of pharmacologically inert materials, requiring large carrier doses that may contribute to immune-related effects, undesired tissue accumulation, and manufacturing complexity. Moreover, the traditional drug loading–stability trade-off has long constrained nanocarrier design. These limitations have stimulated increasing interest in therapeutically active carriers, in which the carrier itself contributes to therapeutic efficacy. (–)-Epigallocatechin-3-gallate (EGCG), the major catechin found in green tea, has emerged as a promising molecular building block for such systems. EGCG possesses intrinsic biological activities such as antioxidant, anti-inflammatory, anticancer, and drug resistance-modulating effects. In addition, the polyphenolic structure of EGCG enables diverse molecular interactions, including hydrophobic interaction, π–π stacking, hydrogen bonding, metal coordination, and dynamic boronate–catechol bonding, allowing EGCG to associate with a wide range of therapeutic agents and promote nanoscale assembly in aqueous environments. Through these combined physicochemical and pharmacological properties, EGCG-building nanocarriers integrate structural and therapeutic functions within a single platform. Such systems can achieve relatively high drug loading, reduce reliance on inert excipients, and promote combinational therapeutic effects between carrier and payload, including the modulation of drug resistance pathways. EGCG-building nanocarriers can be constructed either through direct assembly with therapeutic agents or through chemical modification that programs EGCG into hierarchically organized nanostructures. This review provides an up-to-date overview of EGCG-building nanocarriers, highlighting their design principles, nanocarrier architectures, functional advantages, predominantly preclinical and cancer-focused applications, and key challenges for clinical translation.
Keywords:
EGCG, nanocarriers, drug delivery, pharmacoactive nanocarriers, polyphenols, synergistic therapy
Introduction
Nanocarrier-based drug delivery systems (DDS) have become a central strategy in modern pharmaceutical development, offering opportunities to improve pharmacokinetics, tissue targeting, and therapeutic indices for a wide range of therapeutic modalities. Liposomes, polymeric micelles, polymeric nanoparticles (NPs), inorganic nanomaterials, and hybrid systems have been extensively investigated and, in several cases, successfully translated into clinical products.1–3 These platforms can enhance drug solubility, prolong systemic circulation, modulate release kinetics, and reduce off-target toxicity. Nevertheless, despite decades of progress in nanotechnology and materials engineering, the clinical advantages of many nanoformulations over free drugs remain modest and often insufficient to produce transformative therapeutic outcomes.4,5
One of the most persistent formulation challenges in DDS is the drug loading dilemma. In many conventional nanocarrier systems, the drug loading is typically around 10% (w/w), meaning that a substantial proportion of the administered dose consists of pharmacologically inactive carrier materials.6 These materials may induce immune-related effects, including complement activation and accelerated blood clearance (ABC phenomenon), as well as accumulation in reticuloendothelial organs such as the liver and spleen under repeated administration.7,8 In addition, a high excipient burden complicates manufacturing scalability and regulatory evaluation. Despite extensive efforts, achieving high drug loading while maintaining robust colloidal stability and controlled release remains a major design challenge because of the traditional drug loading–stability trade-off that limits nanocarrier development. Accordingly, there is growing interest in streamlined carrier systems that minimize inert carrier components while preserving structural stability and therapeutic efficacy.9
In this context, pharmacoactive carrier systems have attracted increasing attention. In these systems, structural components of the nanocarrier contribute pharmacological activity rather than serving solely as pharmacologically inert excipients, thereby integrating structural and pharmacological functions within a single platform.9 This design strategy can reduce excipient burden and may also promote synergistic effects between the carrier and the payload. Importantly, because the carrier itself contributes pharmacological activity, efficacy does not rely solely on maximizing drug loading, in contrast to conventional nanomedicines that primarily depend on high drug content. As a result, pharmacoactive carrier systems offer the possibility of simultaneously achieving structural stability, reduced inert carrier burden, and improved therapeutic outcomes (Figure 1).
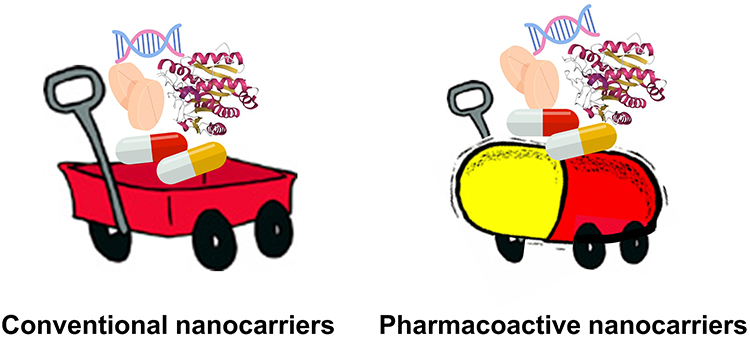 |
Figure 1 Conventional nanocarriers and pharmacoactive nanocarriers. Conventional nanocarriers are generally composed of pharmacologically inert carrier components and may be limited by low drug loading, high excipient burden, carrier-associated toxicity or immunogenicity, and a drug loading–stability trade-off. In contrast, pharmacoactive nanocarriers contain carrier components with intrinsic therapeutic activity, which can contribute to enhanced efficacy through drug–carrier synergy, reduced inert excipient burden, and less dependence on high drug loading or strict drug-to-carrier ratio optimization. |
Bioactive molecules capable of forming multiple noncovalent interactions with therapeutic agents, such as polyphenols (eg, tannic acid (TA) and curcumin) and other aromatic bioactive compounds, have attracted attention as promising building blocks for pharmacoactive nanocarriers. Among them, (–)-epigallocatechin-3-gallate (EGCG), the predominant catechin in green tea, has emerged as a particularly attractive candidate. EGCG possesses a polyphenolic structure containing multiple catechol and galloyl moieties that confer versatile intermolecular interaction capabilities, including hydrogen bonding, π–π stacking, hydrophobic interactions, metal coordination, and dynamic boronate–catechol bondinghas.10 These interactions enable EGCG to bind diverse therapeutic agents, including hydrophobic small molecule drugs, proteins, peptides, and nucleic acids and promote spontaneous nanoscale assembly in aqueous environments.11,12 From a formulation perspective, several reported EGCG-based assemblies exhibit relatively high drug loading, often exceeding 30% (w/w) and in some cases reaching markedly higher levels depending on the strength of interactions between EGCG and the drug, as well as the assembly strategy. These values are generally higher than those typically reported for conventional liposomal or polymeric nanocarriers.
TA, curcumin, and other aromatic polyphenols can participate in supramolecular assembly through hydrogen bonding, hydrophobic interactions, π–π stacking, and metal coordination, and some carrier-free or drug-rich systems can achieve high drug loading by minimizing inactive carrier components.13 However, these platforms differ substantially in their molecular properties and formulation behavior. Curcumin-based systems benefit from intrinsic anticancer and anti-inflammatory activity but are often limited by poor aqueous solubility, crystallization tendency, and formulation-dependent dose-related toxicity concerns.14 TA provides strong multivalent binding and metal–phenolic network formation, but its high molecular weight and broad binding capacity can lead to nonspecific interactions.15 EGCG is distinguished by its relatively small molecular size, water compatibility, catechol/galloyl-rich structure, and ability to combine drug binding with antioxidant, anti-inflammatory, anticancer, and resistance-modulating activities. These features provide a rationale for considering EGCG as a versatile pharmacoactive building block for nanocarrier construction.
Beyond its formulation utility, EGCG has been extensively investigated as a bioactive molecule for diverse pathological conditions, including cancer, inflammatory diseases, metabolic disorders, cardiovascular injury, neurodegenerative diseases, and tissue damage associated with oxidative stress.16–19 Its therapeutic activities are associated with modulation of oxidative stress, inflammatory signaling, apoptosis, angiogenesis, and epithelial–mesenchymal transition (EMT) through scavenging of reactive oxygen species (ROS) and binding to biological molecules. EGCG has also been reported to modulate drug resistance mechanisms, increase intracellular drug accumulation in resistant cells, and mitigate drug-induced toxicity through bioactive pathways of EGCG when co-administered with drugs.20 These pleiotropic biological effects make EGCG attractive as a therapeutic agent.
However, the direct therapeutic application of free EGCG remains limited by poor chemical stability, rapid oxidation, extensive metabolism, limited systemic bioavailability, and possible dose-dependent toxicity at high systemic exposure.21,22 In addition, nonspecific interactions of EGCG with proteins, nucleic acids, transporters, and drug molecules may alter pharmacokinetics or reduce therapeutic activity when EGCG is simply co-administered with drugs. These limitations provide a strong rationale for engineering EGCG into nanocarrier architectures, where its interaction capacity can be directed toward drug binding, structural stabilization, and controlled release. Moreover, when incorporated as a pharmacoactive carrier component, EGCG can cooperate with encapsulated therapeutic agents through its inherent biological activities, promoting therapeutic synergy, thereby enabling it to serve dual roles as both a structural binder and a pharmacologically active component. Collectively, these properties distinguish EGCG-building nanocarriers from conventional inert-carrier systems and highlight their potential as pharmacoactive nanocarrier platforms.
A growing number of studies have incorporated EGCG into drug delivery platforms; however, the functional roles of EGCG in these systems are often heterogeneous and conceptually underdefined. In some formulations, EGCG acts merely as a co-delivered therapeutic molecule, whereas in others it functions as a structural component that directly drives NP formation through multivalent intermolecular interactions. Distinguishing these roles is important from a formulation science perspective because the interaction chemistry of EGCG can strongly influence drug loading capacity, assembly stability, and release behavior.23–25
Based on these physicochemical interaction mechanisms and functional characteristics, EGCG-building nanocarriers can generally be classified into two principal design strategies. The first involves carrier-free or metal-bridged EGCG–drug nanocomplexes, in which unmodified EGCG interacts with drugs through noncovalent interactions or metal coordination to form nanoscale assemblies. In such systems, EGCG acts primarily as a molecular binder and structural crosslinker. The second strategy comprises chemically modified EGCG architectures, where EGCG is conjugated to polymers, targeting ligands, or other functional groups to construct hierarchically organized nanostructures with improved stability and tunable pharmacokinetic behavior. Representative interaction modes and nanocarrier architectures enabled by EGCG chemistry are illustrated in Figure 2.
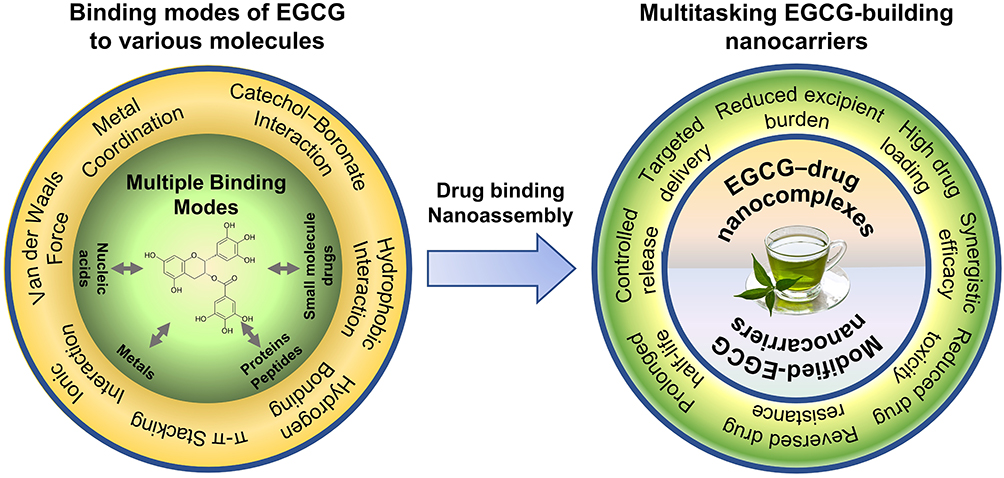 |
Figure 2 Conceptual framework of (–)-epigallocatechin-3-gallate (EGCG)-building nanocarriers as multitasking pharmacoactive nanocarriers. |
Nevertheless, the chemical fragility of EGCG may still influence the reproducibility and scalability of EGCG-building nanocarriers during manufacturing. In addition, the physicochemical complexity of interaction-driven assemblies introduces further challenges related to large-scale production, batch-to-batch consistency, and regulatory classification. A systematic and formulation-oriented understanding of their design strategies, interaction mechanisms, and formulation characteristics is therefore timely and important for guiding further advancement as next-generation drug delivery platforms.
At the current stage, EGCG-building nanocarrier research is rapidly expanding yet remains largely preclinical, with no formulation having yet progressed to clinical trials. Accordingly, this review focuses on formulation design principles, preclinical therapeutic performance, and key physicochemical and translational challenges that must be addressed to support future clinical development.
This review provides a formulation-focused overview of EGCG-building nanocarriers within the framework of drug delivery science and technology. The literature considered in this review is drawn from peer-reviewed studies describing nanocarrier systems in which EGCG functions as an integral structural component. Systems that merely deliver EGCG itself or involve simple EGCG–drug co-delivery without structural integration are outside the scope of this article. Unlike previous reviews that primarily emphasize the pharmacological activities of EGCG or its co-administration with therapeutic agents, this review specifically examines EGCG as a molecular building block for nanocarrier construction. Particular attention is given to the intermolecular interaction chemistry of EGCG and how these interactions facilitate the formation of carrier-efficient DDS architectures characterized by high drug loading, reduced reliance on inert excipients, and integrated therapeutic functionality. Representative EGCG-building nanocarrier formulations developed for diverse classes of therapeutic agents are discussed, with emphasis on their formulation design principles and key physicochemical and functional characteristics, including drug loading capacity, assembly stability, and therapeutic performance. Through this perspective, the review aims to clarify the potential advantages and remaining challenges associated with EGCG-building nanocarriers. Emerging formulation strategies and design considerations derived from these systems are also highlighted to support the continued development of pharmacoactive nanocarrier platforms for advanced drug delivery applications. Relevant literature was identified through searches of PubMed, Web of Science, Scopus, and Google Scholar. Search terms included “epigallocatechin gallate nanoparticle”, “EGCG nanocarrier”, “EGCG drug delivery”, “EGCG drug interaction”, “EGCG drug binding”, “polyphenol nanocarrier”, “polyphenol-mediated assembly”, “metal–polyphenol network”, “boronate catechol drug delivery”, and “pharmacoactive nanocarrier.” Additional relevant studies were identified by screening the reference lists of selected articles. The final selection of studies was guided by the scope and conceptual framework of this review, as outlined above.
EGCG–Drug Interactions in Combination Relevant to Nanocarrier Design
Because EGCG exhibits diverse biological and pharmacological activities, it has attracted increasing attention as a synergistic agent in combination therapies. Numerous studies have reported that EGCG can enhance therapeutic efficacy, reduce drug-associated toxicity, and modulate resistance mechanisms when administered together with various therapeutic agents, particularly in oncology. Collectively, these studies suggest that the pharmacological outcomes of EGCG combinations with drugs are strongly influenced by the interactions between EGCG and co-administered drugs.20,26–29 Understanding these interactions is therefore important not only for interpreting the therapeutic behavior of EGCG-containing combination therapies but also for informing the rational design of EGCG-building drug delivery systems.
In the following sections, representative examples of combination therapies of EGCG and drug are summarized according to their effects on therapeutic outcomes, toxicity reduction, drug resistance-modulation, and pharmacokinetic behavior, providing insights relevant to the design of EGCG-building nanocarriers.
Enhanced Efficacy
A substantial body of evidence demonstrates that EGCG can enhance the therapeutic efficacy of anticancer drugs when used in combination, functioning as a chemosensitizer or adjuvant. These enhanced effects have been observed across multiple cancer types and drug classes, including anthracyclines, platinum agents, kinase inhibitors, and antimetabolites, in both in vitro and in vivo studies, indicating that combinations of EGCG and anticancer drugs can achieve stronger antitumor activity than monotherapy.20
One well-characterized example is the combination of EGCG and doxorubicin (DOX). In bladder cancer models, EGCG markedly potentiated DOX-induced apoptosis and tumor suppression both in vitro and in xenografted mice by suppressing NF-κB and MDM2 signaling while restoring p53 activity, resulting in significantly greater tumor growth inhibition compared with DOX alone.26 Platinum-based chemotherapy has likewise been widely investigated in combination with EGCG. In ovarian cancer models, EGCG enhanced cisplatin sensitivity by upregulating the copper transporter CTR1, increasing intracellular cisplatin accumulation and DNA–platinum adduct formation, and inhibiting nucleic acid repair enzymes such as ERCC1/XPF, thereby improving tumor suppression in vivo relative to cisplatin monotherapy.27
Enhanced efficacy has also been observed with targeted therapies. EGCG combined with the epidermal growth factor receptor (EGFR) inhibitor, erlotinib significantly increased apoptosis in head and neck squamous cell carcinoma through post-transcriptional regulation of Bim and Bcl-2.30 In addition, EGCG has been shown to augment the antitumor activity of kinase inhibitors such as apatinib and sorafenib by suppressing vascular endothelial growth factor (VEGF)-regulated metabolic pathways and promoting apoptotic signaling.31,32 Similar cooperative effects have been reported with antimetabolite drugs. EGCG increased the chemosensitivity of colorectal cancer cells to 5-fluorouracil (5-FU), including in chemoresistant and cancer stem-like cell populations, through enhanced apoptosis, cell-cycle arrest, and suppression of stemness-related signaling pathways.33 In pancreatic cancer models, EGCG combined with gemcitabine significantly reduced tumor proliferation, migration, and invasion and suppressed tumor growth in xenograft models by modulating glycolytic metabolism and EMT signaling.34
Reduced Drug Toxicity
Non-specific toxicity of anticancer drugs represents one of the major limitations of chemotherapy and frequently leads to dose reduction or discontinuation of treatment. Combination strategies incorporating EGCG have been proposed to mitigate such toxicity through two complementary mechanisms: (i) enabling dose reduction of cytotoxic drugs via synergistically enhanced therapeutic efficacy, and (ii) directly counteracting drug-induced toxic mechanisms, including oxidative stress and inflammation.
One of the most extensively studied examples is cisplatin-induced nephrotoxicity, a clinically significant complication that limits cumulative dosing and long-term treatment. Cisplatin-associated renal injury is closely linked to oxidative stress, mitochondrial dysfunction, inflammation, and tubular cell apoptosis. Experimental studies have shown that EGCG protects against cisplatin-induced nephrotoxicity through antioxidant and anti-apoptotic mechanisms, reducing tubular apoptosis and inflammatory responses while preserving renal histological integrity.35 EGCG has also been reported to attenuate mitochondrial ROS production and apoptotic cell death in cisplatin-treated human renal tubular cells, accompanied by increased activities of antioxidant enzymes such as manganese superoxide dismutase and glutathione peroxidase.36 Furthermore, EGCG exhibited neuroprotective effects against cisplatin-induced neurotoxicity also by activating the Nrf2/HO-1 antioxidant pathway while inhibiting NF-κB-mediated inflammation.37 EGCG has also been reported to mitigate other cisplatin-associated toxicities, including ototoxicity and salivary gland damage, through suppression of oxidative and inflammatory injury pathways.38
Cardiotoxicity associated with anthracycline chemotherapy, particularly DOX, represents another major dose-limiting adverse effect. DOX-induced cardiac injury is largely driven by excessive ROS generation, mitochondrial dysfunction, and activation of apoptotic signaling pathways in cardiomyocytes. Several studies have shown that EGCG can attenuate these pathological processes without compromising the anticancer activity of DOX. For instance, EGCG reduced DOX-induced cardiotoxicity in tumor-bearing mice by decreasing oxidative stress, stabilizing mitochondrial function, and suppressing apoptosis in cardiac tissue.39 Additional studies demonstrated that EGCG pretreatment ameliorated DOX-induced oxidative stress and inflammatory responses in the heart while improving antioxidant defense systems.40 Mechanistic investigations further revealed that EGCG can protect against DOX-induced cardiotoxicity by activating AMPK-dependent autophagy and suppressing ferroptotic cell death, thereby preserving mitochondrial integrity and reducing lipid peroxidation.41 A synthetic EGCG derivative, Y6 showed strong cardioprotective and antitumor effects of daunorubicin by suppressing CBR1 expression through PI3K/AKT and MEK/ERK signaling pathways.42
EGCG has also demonstrated protective effects against toxicities associated with other anticancer agents. In experimental models of bleomycin-induced pulmonary fibrosis, EGCG administration restored antioxidant capacity, reduced extracellular matrix accumulation, and suppressed inflammatory cytokine production, thereby attenuating lung injury.43
Reversal of Drug Resistance
Drug resistance represents a major obstacle to successful chemotherapy and is a key factor contributing to treatment failure and poor clinical outcomes. Increasing evidence suggests that EGCG can restore the sensitivity of resistant cancer cells to various anticancer agents by modulating multiple resistance-associated mechanisms. One of the most widely reported mechanisms involves inhibition of drug efflux transporters. EGCG has been shown to suppress the activity of P-glycoprotein (P-gp), an ATP-binding cassette transporter responsible for the efflux of numerous chemotherapeutic drugs. Inhibition of P-gp by EGCG enhances intracellular drug accumulation, thereby restoring chemosensitivity in multidrug-resistant tumor cells.20
For example, in colorectal cancer cells, EGCG significantly enhanced the cytotoxicity of 5-FU by suppressing the GRP78/NF-κB/miR-155-5p signaling pathway, leading to downregulation of the MDR-1/P-gp efflux transporter, increased intracellular drug retention, and enhanced apoptotic cell death.44 Similar chemosensitizing effects have been reported in gastric cancer, where EGCG restored sensitivity to 5-FU through suppression of the TFAP2A/VEGF signaling axis and reduced expression of MDR-1 and P-gp.45 EGCG has also been shown to enhance the efficacy of anthracyclines. In DOX-treated cancer cells, EGCG increased intracellular drug accumulation, promoted apoptotic signaling through activation of the p53 pathway, and significantly improved antitumor activity both in vitro and in vivo.26,39
Beyond modulation of drug efflux, EGCG can influence resistance through epigenetic and signaling pathway regulation. In estrogen receptor-negative breast cancer cells, EGCG sensitized tumors to tamoxifen by epigenetically reactivating ERα expression via histone modification and DNA methylation changes, thereby restoring estrogen-responsive growth inhibition.46 EGCG has also been reported to suppress proliferation and survival signaling in trastuzumab-resistant breast cancer cells by inhibiting AKT activity and promoting nuclear accumulation of FOXO3a and p27Kip1.47 Furthermore, EGCG resensitized non-small cell lung cancer cells to cisplatin through demethylation of genes associated with cell death pathways,48 and exhibited antitumor activity in platinum-resistant ovarian cancer by downregulating S100A4 and NF-κB while restoring p53 signaling.49
Molecular Binding and Pharmacokinetic Interactions
Although numerous studies have reported beneficial pharmacological effects of EGCG and drugs in combinations, unfavorable interactions can also occur depending on the physicochemical and pharmacokinetic characteristics of the co-administered agents. EGCG has been shown to influence the pharmacokinetics and pharmacodynamics of various therapeutic drugs by altering their absorption, metabolism, transport, or chemical stability.28,29,50–52 Consequently, co-administration of EGCG does not always lead to improved therapeutic outcomes and may, in certain cases, reduce drug efficacy or alter systemic exposure.
Several studies have reported antagonistic interactions between EGCG and anticancer agents. For example, Golden et al demonstrated that EGCG markedly abolished the antitumor activity of bortezomib (BTZ), a boronate-based proteasome inhibitor widely used for the treatment of multiple myeloma and mantle cell lymphoma.28 This antagonism results from the formation of a cyclic boronate complex between EGCG and BTZ, which chemically inactivates the drug. Another representative example involves the multikinase inhibitor sunitinib (SU). While delayed administration of EGCG after SU treatment enhanced antitumor efficacy in some studies,53 other investigations reported that the simultaneous administration of EGCG significantly reduced plasma concentrations of SU by forming poorly soluble complexes in the gastrointestinal tract, thereby impairing drug absorption.29
EGCG can also influence drug disposition by modulating membrane transporters and metabolic enzymes. Inhibition of P-gp by EGCG may enhance intracellular drug accumulation and reverse multidrug resistance, but it can also alter the pharmacokinetics of P-gp substrate drugs such as verapamil, diltiazem, digoxin, tamoxifen, and doxorubicin.51,54–57 Because P-gp contributes to biliary drug elimination,51 its inhibition may increase systemic drug exposure and potentially elevate toxicity risk. For instance, EGCG administration significantly increased plasma concentrations and half-life of irinotecan and its active metabolite SN-38.52,58 EGCG has also been shown to enhance the bioavailability of 5-FU by inhibiting dihydropyrimidine dehydrogenase, the key enzyme responsible for 5-FU metabolism.59 In contrast, co-administration of green tea catechins has been reported to decrease systemic exposure of certain drugs, including digoxin, highlighting the complexity of EGCG–drug pharmacokinetic interactions.51 In addition to transporter-mediated effects, EGCG may influence drug disposition through inhibition of organic anion transporting polypeptides (OATP)60 and interference with CYP3A4-dependent metabolic pathways.61 Clinical studies have also shown that green tea consumption can reduce the oral bioavailability of several drugs, including folic acid and warfarin.62 These observations emphasize the need for caution when EGCG is co-administered with drugs that possess narrow therapeutic indices or limited solubility.63
Implications of EGCG–Drug Interactions for Nanocarrier Design
EGCG–drug interactions exert multifaceted effects on therapeutic efficacy, toxicity, resistance, and drug disposition, providing a mechanistic foundation for EGCG-building nanocarrier design. The same interactions that enhance apoptosis, suppress survival signaling, and modulate cellular metabolism can be leveraged to reinforce cooperative therapeutic effects through carrier–payload co-localization (Table 1). In addition, the intrinsic antioxidant and cytoprotective properties of EGCG offer opportunities to mitigate treatment-related toxicity and improve the therapeutic index. EGCG-mediated modulation of drug resistance pathways, including efflux transport and survival signaling, may further enhance intracellular drug retention in resistant tumors.
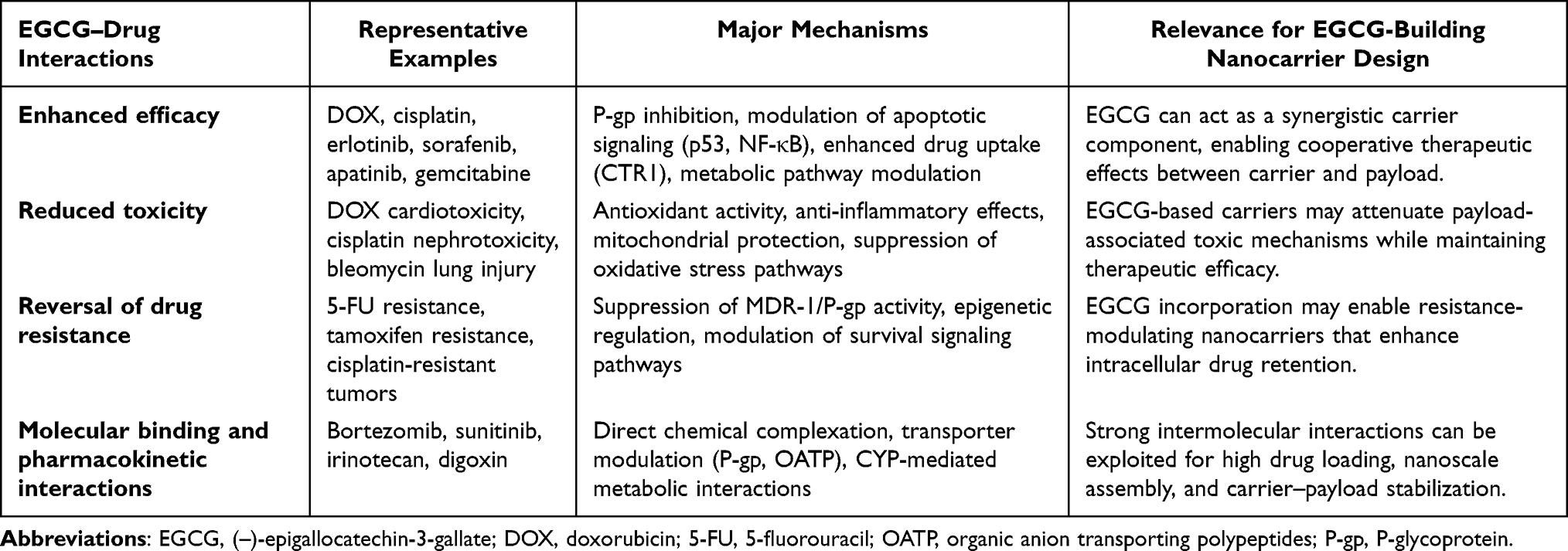 |
Table 1 Therapeutic Implications of EGCG–Drug Interactions Relevant to the Design of EGCG-Building Nanocarriers |
Notably, intermolecular interactions responsible for unfavorable pharmacokinetic effects can be repurposed as a design principle in nanodelivery systems. In EGCG-building nanocarriers, such interactions promote nanoscale assembly and stabilize carrier–payload complexes. Therefore, rational design requires careful consideration of compatibility between EGCG and the payload to achieve balanced interaction strength, enabling stable assembly, controlled drug retention, responsive release, and favorable therapeutic synergy. These insights provide a conceptual framework for the EGCG-building nanocarrier systems discussed in the following sections.
Unmodified EGCG as a Molecular Binder for Nanocomplex Formation
Versatile Binding Properties of EGCG
EGCG exhibits versatile binding properties toward various biomolecules, including peptides, proteins, and nucleic acids, through multiple covalent and noncovalent interactions such as hydrophobic interactions, hydrogen bonding, π–π stacking, and electrostatic.11 The diverse therapeutic properties of EGCG have been attributed, at least in part, to its ability to interact with biological molecules and thereby modulate a variety of signal transduction pathways.17,64 For instance, EGCG binds to a variety of proteins mainly through hydrophobic interactions,65 while its polyphenolic rings can interact with aromatic and proline residues of proteins through π–π stacking.66 These interactions can contribute to the regulation of multiple signaling pathways.17,64 In addition, the oxidized ortho-quinone form of EGCG can react with nucleophilic thiol groups in proteins.67 The hydroxyl groups of EGCG also serve as hydrogen-bond donors, allowing strong interactions with proteins and nucleic acids.68 EGCG has been reported to enter the nucleus and bind to DNA and RNA in CpG-rich regions,69 suggesting that EGCG–nucleic acid interactions may contribute to the regulation of gene-related functions.
EGCG can also coordinate with various metal cations, including Cu2⁺, Zn2⁺, Fe2⁺, Fe3⁺, and Al3⁺, through its polyphenolic moieties, thereby forming metal–polyphenol complexes and nanostructures.70 Coordination interactions between phenolic moieties and metal ions are fundamental to natural phenomena such as plant pigmentation and nutrient cycling, with the stoichiometry of the resulting complexes, including mono-, bis-, or tris-coordinated forms, governed by pH, metal ion valence, and metal-to-phenolic group ratios.10 EGCG–metal complexes have attracted broad interest for biomedical applications because of their facile one-step formation, biocompatibility, and stability in systemic circulation.11
Furthermore, the pyrogallol and galloyl moieties of EGCG can form dynamic covalent linkages with boronate groups through boronate–catechol complexation.71 The structural similarity between EGCG and many multiring aromatic small molecule drugs also favors EGCG–drug association through π–π stacking, which can be reinforced by hydrogen bonding, hydrophobic interactions, and/or electrostatic interactions.72 These binding properties may also underlie antagonistic or pharmacokinetic interactions observed when EGCG is co-administered with certain drugs, particularly in the gastrointestinal (GI) tract or systemic circulation. Several studies have reported that EGCG can alter the pharmacokinetics and pharmacodynamics of therapeutic agents through direct or indirect mechanisms, thereby affecting their absorption, bioavailability, or activity.73 Nevertheless, these same interaction mechanisms can be advantageously exploited in nanocarrier design. EGCG-mediated binding can promote efficient loading of active pharmaceutical ingredients (APIs) into nanoscale assemblies, stabilize payloads within confined nanostructures, protect them during exposure to the GI tract or systemic circulation, and ultimately improve pharmacokinetic performance.
Noncovalent EGCG–Drug Nanocomplexes Driven by Molecular Binding
Noncovalent EGCG–drug nanocomplexes represent the most direct strategy for constructing EGCG-building nanocarriers. In these systems, unmodified EGCG participates in nanocarrier formation through reversible molecular interactions, including hydrogen bonding, π–π stacking, hydrophobic interactions, electrostatic interactions, and metal–phenolic coordination. These interaction-driven assemblies can incorporate structurally diverse payloads under mild aqueous conditions, thereby reducing the need for large amounts of inert carrier materials. At the same time, their performance depends strongly on the balance between complex stability and stimulus-responsive dissociation, which determines drug retention during circulation and release at the target site. The following examples illustrate how noncovalent EGCG-mediated binding has been used to construct nanocomplexes for small molecule drugs, metal-coordinated systems, and nucleic acid delivery.
Shan et al developed a self-assembled NP in which DOX was loaded through EGCG/Fe3⁺ coordination, and the resulting complex was further encapsulated with high molecular weight polyphenol-conjugated poly(ethylene glycol) (PEG) for evaluation in glioma xenograft mice (Figure 3A).74 The NP formulation exhibited prolonged systemic circulation, increased tumor accumulation, and significant suppression of tumor growth in a uppsala 87 malignant glioma (U87MG) xenograft model. In addition, the NPs mitigated DOX-induced cardiotoxicity and hematological toxicity by EGCG-mediated inhibition of CBR1 expression, thereby reducing the formation of doxorubicinol, a key DOX metabolite implicated in drug resistance and cardiotoxicity.74 A similar strategy was used to construct hybrid phenolic complexes composed of EGCG, a 5-hydroxydopamine-modified platinum(IV) prodrug (Pt-OH), Fe3+, and a polyphenol-modified block copolymer (PEG-b-PPOH) (Figure 3B).75 Incorporation of gadolinium ions (Gd3+) endowed the NPs with magnetic resonance imaging (MRI) contrast for noninvasive in vivo tracking, creating a bifunctional nanomedicine for both drug delivery and imaging. Wang et al developed an oral delivery system in which EGCG and 5-FU, a first-line chemotherapeutic agent for colon cancer, were complexed with gelatin and chitosan to form NPs.76 The NPs loaded with 5-FU and EGCG exhibited controlled drug release, improved cellular internalization, and prolonged systemic circulation, which collectively resulted in enhanced antitumor and pro-apoptotic effects in vivo compared with free drug formulations. Zhou et al prepared EGCG/ruthenium (Ru) NPs loaded with luminescent Ru complexes [Ru(2,2’-bipyridine)2(4-B)] (ClO4)2·2H2O (RuBB) for liver cancer treatment (Figure 3C).77 RuBB-loaded EGCG/Ru NPs showed monodisperse, homogeneous and spherical morphology, improved stability, and selective accumulation in 67LR-overexpressed liver cancer cells (SMMC-7721) due to the targeting ability of EGCG. The NPs were nontoxic in normal cells (L-02) and showed direct ROS-dependent cytotoxic, pro-apoptotic, and anti-invasive effects in SMMC-7721 cells. Also, the NPs demonstrated high antitumor efficacy in tumor-bearing nude mice. Wang et al developed DOX-loaded EGCG/Fe NPs using zeolitic imidazolate framework-8 (ZIF-8) particles as sacrificial templates (Figure 3D).78 DOX was initially incorporated into ZIF-8 via a coprecipitation process, followed by deposition of EGCG/Fe layers onto the particle surface. Subsequent removal of the ZIF-8 core with EDTA yielded hollow EGCG/Fe NPs encapsulating DOX. These NPs exhibited strong ROS scavenging capability and underwent structural disassembly upon oxidation of EGCG during ROS neutralization, thereby triggering DOX release. Elevated endogenous ROS levels in tumor cells further accelerated NP degradation and intracellular drug release, resulting in superior tumor growth inhibition compared with free DOX, while showing minimal acute toxicity to normal tissues. Chen et al developed a multifunctional nanocomplex composed of EGCG, Fe3⁺, and DOX through metal–phenolic coordination, enabling combined tumor therapy, imaging, and metastasis suppression.79 The nanocomplex preferentially accumulated in tumor tissue via the enhanced permeability and retention (EPR) effect and released DOX within tumor cell endosomes as the coordination network destabilized under mildly acidic conditions. Following dissociation, EGCG functioned as a therapeutic adjuvant by inhibiting EMT and reducing matrix metalloproteinase expression, thereby suppressing metastatic progression. Meanwhile, Fe3⁺ served as an effective magnetic resonance imaging contrast agent, allowing noninvasive visualization of nanocomplex distribution. Both in vitro and in vivo studies confirmed enhanced antitumor efficacy, reduced metastasis, and concurrent diagnostic capability. Building on this strategy, Zhang et al developed a self-assembled nanomedicine by coordinating Fe2⁺ with EGCG and encapsulating the ferroptosis inducer RSL3, resulting in Fe-EGCG@RSL3 NP (Figure 3E).80 EGCG served multiple roles including chelating iron, stabilizing the NP architecture, and contributing antioxidant effects. In subcutaneous and orthotopic bladder cancer mouse models, the NP accumulated in tumors and significantly inhibited tumor growth compared with RSL3 or EGCG alone after intravesical administration. Fe-EGCG@RSL3 integrated ferroptosis induction with immunomodulation, supporting its potential as a multifunctional nanomedicine.
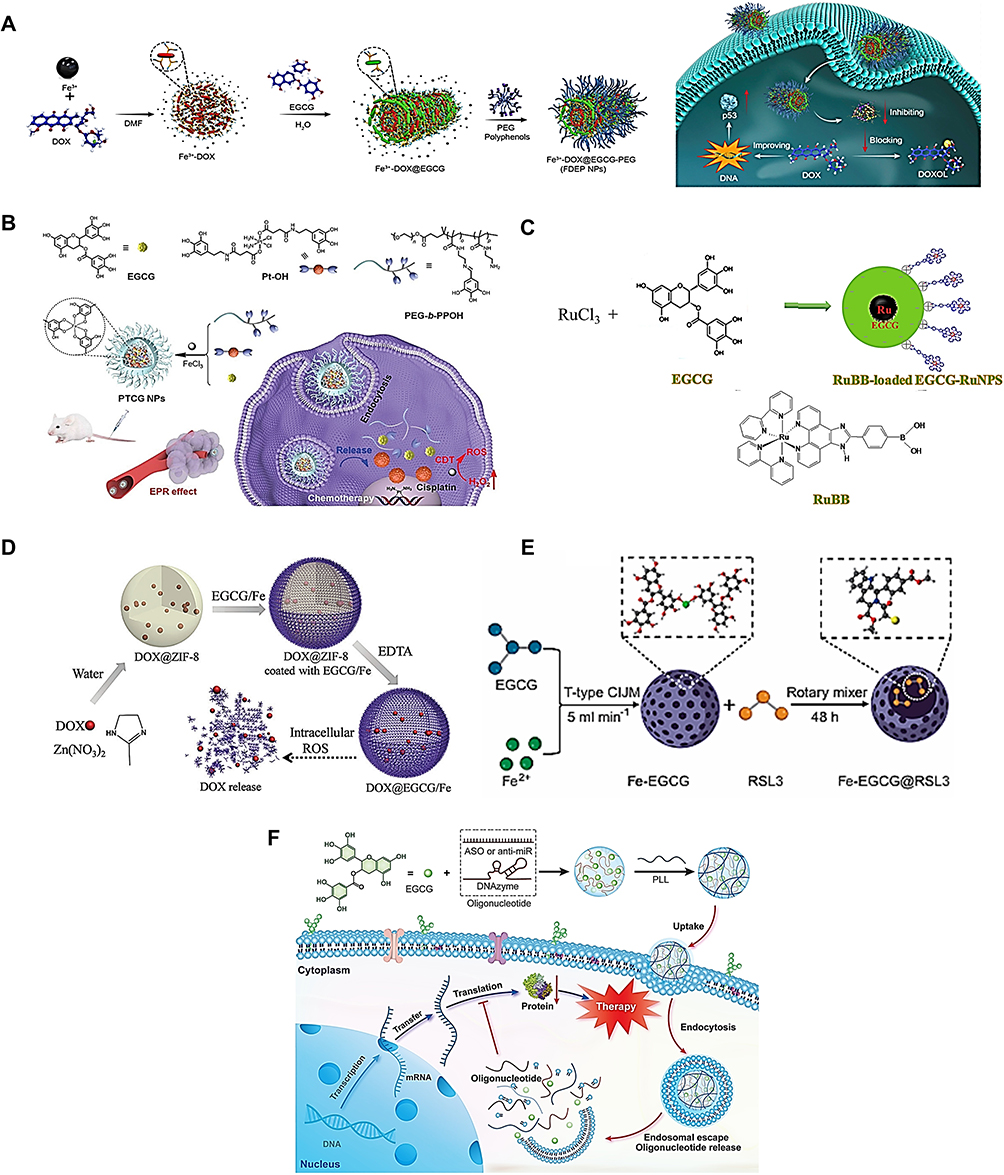 |
Figure 3 Drug–EGCG nanocomplexes via noncovalent bonding. (A) DOX-loaded EGCG/Fe3+/PEG NP and its intracellular mechanism.74 (B) Pt(IV) prodrug-loaded EGCG/Fe3+/PEG-b-PPOH NP.75 (C) RuBB-loaded EGCG/Ru NP.77 (D) DOX-loaded EGCG/Fe NP by ZIF-8 template.78 (E) RSL3-loaded Fe/EGCG NP.80 (F) Oligonucleotide-loaded EGCG/ε-poly-L-lysine NP.81 Reproduced with permission. Abbreviations: DOX, doxorubicin; EGCG, (–)-epigallocatechin-3-gallate; NP, nanoparticle; PEG, poly(ethylene glycol); PEG-b-PPOH, polyphenol modified PEG block copolymer; PLL, ε-poly-L-lysine; Pt, platinum; ZIF-8, zeolitic imidazolate framework-8. |
Nanocomplexes of EGCG and biomolecules such as nucleic acids and proteins have also been developed. Ding et al reported NPs co-loaded with small interfering RNA (siRNA) and protamine via complexation with EGCG, and then encapsulated by HA and tumor-homing cell-penetrating peptides grafted on the surface for triple-negative breast cancer treatment.82 The NPs have demonstrated superior selectivity and tumor growth inhibition compared with EGCG alone in MDA-MB-231 tumor-bearing xenograft mice. Beyond cancer therapy, Shen et al have reported core-shell NPs prepared by complexation of siRNA with EGCG, followed by coating low molecular weight polymers to form the shell for inflammatory bowel disease treatment.83 The NPs achieved selective inhibition of target gene expression in vitro and in vivo and effectively mitigated chronic intestinal inflammation in an experimental model of inflammatory bowel disease. EGCG facilitated siRNA condensation into NPs, reducing reliance on highly cationic polymers whose toxicity often increases with transfection efficiency. Using the same technique, EGCG formed complexes with several types of single-strand oligonucleotides, including antisense oligonucleotides, anti-miRNA, and DNAzyme, which were further coated with the low molecular weight cationic polymer ε-poly-L-lysine to enhance cellular internalization (Figure 3F).81 The resulting core-shell structured NPs showed improved cargo stability and achieved efficient intracellular delivery in vitro. In another approach, a noncationic NP for mRNA delivery was developed by the sequential mixing of PEG, mRNA, and EGCG to form agglomerates, followed by introduction of metal ions to stabilize the NP through metal/EGCG complexation.84 Among various polyphenols examined, EGCG produced the highest transfection of HEK 293T cells, likely attributed to its high loading capacity. Intravenous administration of the NP enabled predominant protein expression and gene editing in the brain, liver, and kidney, while organ tropism could be tuned by varying NP composition.
Boronate–Catechol Dynamic Conjugation for EGCG-Mediated Nanocomplex Formation
Boronate–catechol dynamic conjugation provides a more chemically defined and stimuli-responsive mode of EGCG-mediated nanocomplex formation. Because the catechol or galloyl groups of EGCG can form reversible boronate ester linkages with boronic acid-containing drugs or polymers, this strategy enables stable complexation under selected conditions and dissociation in response to environmental changes such as pH. Importantly, interactions that are unfavorable in simple co-administration, such as EGCG-mediated inactivation of boronate-containing drugs, can be repurposed for controlled nanocarrier assembly and tumor-responsive release. The representative systems described below demonstrate how boronate–catechol chemistry can be used to improve drug retention, trigger intracellular release, and integrate EGCG-derived bioactivity with payload function.
Wang et al used metal coordination interaction and boronate‒catechol interaction with four types of polyphenols (catechin, EGCG, TA, and procyanidin) to form BTZ-loaded NPs for cancer therapy (Figure 4A).85 EGCG can form a cyclic boronate–catechol diester bond with BTZ, an interaction that inactivates BTZ during simple co-administration. In this nanocarrier design, however, the same interaction was deliberately exploited to construct a pH-responsive supramolecular nanomedicine. Ferric ions were incorporated into the NPs through metal–phenolic coordination to improve structural stability and introduce bioimaging capability. The fabricated NPs exhibited pH-responsive release behavior, minimizing premature BTZ leakage under physiological conditions while enabling rapid drug liberation under acidic tumor conditions. This system effectively triggered apoptosis in cancer cells and significantly inhibited tumor growth in both subcutaneous and bone tumor models, with minimal systemic toxicity. This example illustrates how an EGCG–drug interaction that is generally considered detrimental can be repurposed to achieve controlled drug delivery and improved therapeutic efficacy. A polyion complex (PIC) micelle encapsulating DOX and EGCG was prepared via a combination of electrostatic interactions and phenylboronic acid–catechol binding between poly(ethylene glycol)-block-poly(lysine-co-lysine-phenylboronic acid) (PEG-PLys/PBA) and EGCG, while DOX was incorporated into the micellar core via π–π stacking interactions with EGCG (Figure 4B).86 The PIC micelles remained stable under physiological conditions through phenylboronic acid–catechol complexation, whereas the acid-labile nature of this interaction enabled pH-triggered dissociation in the micellar core, resulting in coordinated release of EGCG and DOX and enhanced synergistic effects. In addition, the combination of EGCG and DOX protected cardiomyocytes from DOX-mediated cardiotoxicity through the ROS scavenging activity of EGCG and overcame multidrug resistance by suppressing P-gp activity. Collectively, this system demonstrates the potential of boronate–catechol-stabilized EGCG-based micelles to improve DOX delivery while reducing cardiotoxicity and multidrug resistance. Lui et al developed polyphenol-based NPs for cytosolic protein delivery using EGCG, (+)-catechin, ellagic acid, or procyanidin (Figure 4C).87 These polyphenols formed nanocomplexes with proteins such as bovine serum albumin (BSA), R-phycoerythrin and ribonuclease A via hydrogen bonding and hydrophobic interactions. EGCG–BSA complexation was reported to be exothermic, and the EGCG/BSA complex retained the secondary structure of the protein. The pyrogallol groups on the nanocomplex surface were further decorated with boronate-containing polymers, such as boronic acid-conjugated dendrimers and boronic acid-modified polylysine. Under acidic conditions, pH-responsive cleavage of boronate–catechol bonds promoted protein release from the nanocomplexes and facilitated endosomal/lysosomal escape, thereby enhancing intracellular protein delivery. Sun et al reported a phenolic-based, tumor-permeable nanoframework (EGPt-NF) constructed through pH-reversible borate ester linkages mediated by EGCG, which crosslinked phenylboronic acid-modified platinum NPs (PBA-Pt) with dextran grafted with phenylboronic acid (Dex-g-PBA) (Figure 4D).88 The resulting EGPt-NF effectively enhanced dendritic cell maturation while suppressing PD-L1 expression in tumor cells. In addition, the nanoframework alleviated tumor hypoxia, thereby promoting cytotoxic T-lymphocyte infiltration and increasing interferon-γ secretion. The enhanced tumor immunogenicity was attributed to the synergistic interplay between PBA-Pt as an inducer of immunogenic cell death and EGCG as a PD-L1 inhibitory component.
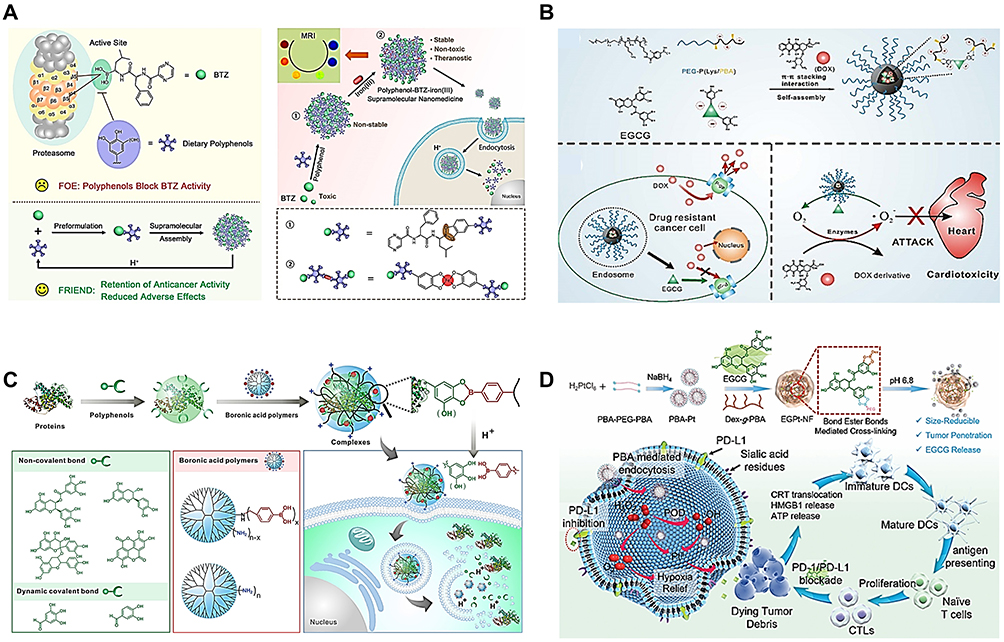 |
Figure 4 Drug-EGCG nanocomplexes via boronic acid–catechol dynamic conjugation. (A) BTZ-loaded EGCG/Fe3+ NP.85 (B) Formation and proposed mechanism by which DOX-loaded EGCG/PEG-P(Lys/PBA) NPs overcome multidrug resistance and reduce cardiotoxicity.86 (C) Protein-loaded polyphenol/boronate polymer NP.87 (D) PBA-Pt/EGCG/Dex-g-PBA nano-framework (EGPt-NF) for immunogenic cell death induction together with PD-L1 checkpoint blockade immunotherapy.88 Reproduced with permission. Abbreviations: BTZ, bortezomib; Dex, dextran; DOX, doxorubicin; EGCG, (–)-epigallocatechin-3-gallate; NP, nanoparticle; PBA, phenylboronic acid; PEG, poly(ethylene glycol). |
Representative unmodified EGCG-mediated nanocomplexes based on noncovalent binding, metal coordination, and boronate–catechol dynamic conjugation are summarized in Table 2, highlighting their payloads, binding mechanisms, reported loading values, and major functional advantages.
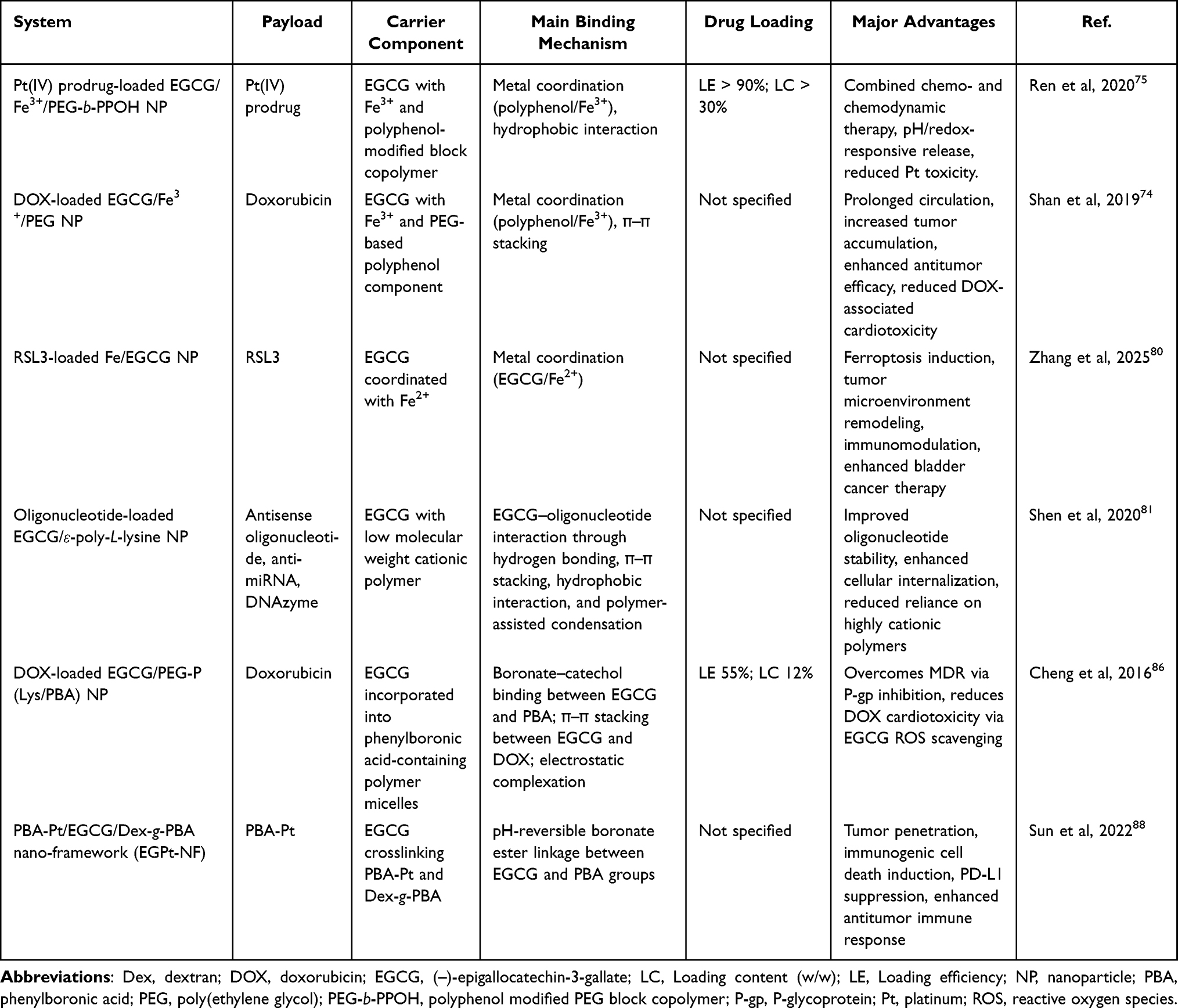 |
Table 2 Representative Unmodified EGCG-Mediated nanocomplexes |
Chemically Modified EGCG Derivatives as Building Blocks for Hierarchically Organized Nanocarriers
Although unmodified EGCG-mediated nanocomplexes offer a simple and efficient strategy for payload association, their assembly generally relies on reversible equilibrium-driven interactions. As a result, these systems may undergo partial dissociation or structural rearrangement under physiological pH, ionic strength, dilution, or serum-rich conditions. Such assemblies can enhance drug binding and reduce excipient use, but they may provide limited control over higher-order organization such as well-defined core–shell or multilayered architectures. Because of their dynamic nature, these formulations may exhibit structural heterogeneity and batch-to-batch variability, which can complicate manufacturing consistency, shelf-life stability, and reproducible therapeutic performance. NPs with exposed EGCG or drug-rich surfaces may also be prone to protein adsorption in plasma, leading to protein corona formation, particle destabilization, aggregation, and accelerated recognition and clearance by the mononuclear phagocyte system. These effects may shorten systemic circulation and reduce therapeutic efficacy.
To improve thermodynamic and kinetic stability, chemically modified EGCG derivatives have been developed to enable programmed assembly with therapeutic payloads into more ordered nanostructures. Chemical modification of EGCG introduces molecular directionality and amphiphilic balance, enabling controlled hierarchical self-assembly into organized core–shell, micellar, or multilayered architectures with improved stability and tunable functionality. This approach can improve EGCG resistance to oxidation, enhance drug loading and release tunability, and support thermodynamic and pharmacokinetic robustness, which are important for reproducibility and therapeutic precision. This section reviews chemically modified EGCG-building nanocarriers in which engineered EGCG derivatives function as designed building blocks for hierarchical assembly, transforming EGCG from a transient molecular binder into a structural and functional component of multitasking nanocarriers. Several studies, including those from our group, have demonstrated therapeutically active nanocarriers based on modified EGCG derivatives that enable efficient and stable loading of diverse payloads and promote synergistically enhanced efficacy.72,89–96 More recently, various engineered EGCG derivatives have been investigated to construct effective, safe, and versatile nanocarrier systems that exploit both the broad binding capacity and intrinsic therapeutic activity of EGCG.
Chemically Modified EGCG-Based Nanocarriers for Protein and Peptide Delivery
Compared with small molecule pharmaceuticals, peptide and protein drugs are expanding rapidly and are expected to represent an increasingly important segment of the global drug market.97 This growth reflects their advantages, including high target specificity, potent biological activity, and, in some cases, reduced off-target toxicity compared with conventional small molecule drugs.98 However, effective delivery of protein and peptide therapeutics remains challenging because these biomacromolecules are highly susceptible to denaturation, enzymatic degradation, and loss of bioactivity during formulation, storage, and administration. Intracellular delivery is particularly difficult, as proteins and peptides must overcome cellular membrane barriers, avoid lysosomal degradation, and escape from endosomal compartments.99 Accordingly, conventional protein delivery approaches, including PEGylation, emulsion-based formulations, covalent modification, and encapsulation in polymeric or lipid carriers, can suffer from low loading efficiency, reduced biological activity, complex formulation processes, or limited yield.
The pyrogallol and galloyl groups of EGCG can readily interact with proteins and peptides through noncovalent interactions, enabling self-assembled nanocomplexes to form under mild aqueous conditions. Chemically modified EGCG carriers are therefore particularly attractive for protein and peptide delivery because they allow reversible complexation while avoiding extensive covalent modification of fragile biomacromolecules. Compared with conventional protein delivery approaches that may compromise protein activity or formulation yield, EGCG-derived carriers can provide a gentle complexation strategy for encapsulating and stabilizing fragile proteins and peptides. By combining multivalent EGCG–protein interactions with protective polymer or polysaccharide shells, these systems can improve loading, preserve bioactivity, and enhance systemic or intracellular delivery. The following examples highlight how EGCG-derived carriers have been engineered to stabilize protein and peptide therapeutics and promote carrier–payload synergy.
In a pioneering study performed by Chung et al, a micellar nanocomplex (MNC) carrier comprising two EGCG derivatives has been developed to encapsulate proteins in a spatially ordered nanostructure for cancer therapy (Figure 5A).89 One component was oligomerized EGCG (OEGCG), which was designed to possess greater oxidative stability than native EGCG and to form a stable core complex with proteins through strengthened multidentate binding. The other component was PEG-conjugated EGCG (PEG-EGCG), which was designed to anchor onto the preformed protein/OEGCG core complex through EGCG moieties and form an inert hydrophilic PEG shell. This shell protects the core from biological environments and prolongs the blood half-life of the nanocomplex. The MNC loaded Herceptin, a trastuzumab antibody against HER2/neu (erbB2), mainly through hydrophobic interactions between EGCG moieties and the protein, yielding monodisperse nanocomplexes of approximately 90 nm with high loading efficiency (~100%) and loading content (64% (w/w)). Herceptin-loaded MNCs exhibited excellent stability under physiologically relevant conditions, including incubation at 37°C in PBS with serum for 15 days, extreme dilution up to 1000-fold, and exposure to enzymatic proteolysis. They also showed greater growth-inhibitory effects against HER2-overexpressing human cancer cell lines (BT-474, SK-BR3, and SKOV3) than free Herceptin, attributable to synergistic effects between the antibody and the carrier, as indicated by a combination index (CI) < 1. No inhibitory effects were observed in normal breast cell lines (MCF-10A and HMEC). In vivo, Herceptin-loaded and interferon α-2a (IFN-α-2a)-loaded MNCs achieved superior antitumor efficacy, inducing pronounced tumor regression in BT-474 and HAK-1B-xenograft models, respectively, compared with free drug, carrier alone, or their sequential administration. The MNCs also exhibited markedly increased tumor accumulation, reduced distribution to off-target organs such as the liver, kidney, and lung, and a ~29-fold prolonged blood half-life relative to free protein drugs. Collectively, these results demonstrate that MNCs can improve protein delivery and therapeutic outcomes through carrier–drug synergy. Wang et al prepared an a matrix metalloproteinase protein 2 (MMP-2)-responsive nanocomplex loaded with anti-PD-L1 antibody and the photosensitizer indocyanine green (ICG) (Figure 5B).100 In this system, anti-PD-L1 and ICG were complexed with EGCG dimers (dEGCG) and a PEG-EGCG conjugate containing MMP-2-cleavable peptide linkers. The nanocomplex was designed to accumulate at tumor sites and release both anti-PD-L1 and ICG in response to overexpressed MMP-2, thereby amplifying intratumoral ROS production under near-infrared (NIR) laser irradiation. This strategy promoted intratumoral infiltration of cytotoxic T cells and sensitized tumors to anti-PD-L1 blockade therapy. Treatment with the nanocomplex combined with NIR laser irradiation markedly inhibited tumor progression and reduced metastatic spread to the lungs and lymph nodes in murine models.
 |
Figure 5 Chemically modified EGCG-based nanocarriers for protein and peptide delivery. (A) Herceptin-loaded OEGCG/PEG-EGCG MNC and its enhanced antitumor efficacy and tumor-selective biodistribution.89 (B) Anti-PD-L1/ICG-loaded dEGCG/PEG-EGCG NP.100 (C) GzmB-loaded HA-EGCG/PEI nanogel.91 (D) TEM images and anti-tumor efficacy of MPI-loaded FEGCG NP (scale bar = 100 nm).101 Reproduced with permission. *p<0.05, **p<0.01, ***p<0.0001 by one-way ANOVA. Abbreviations: EGCG, (–)-epigallocatechin-3-gallate; FEGCG, fluorinated EGCG; GzmB, Granzyme B; HA-EGCG, hyaluronic acid-conjugated EGCG; ICG, indocyanine green; MNC, micellar nanocomplex; MPI, melittin; NP, nanoparticle; OEGCG, oligomerized EGCG; PEG-EGCG, poly(ethylene glycol)-conjugated EGCG; PEI, poly(ethylenimine). |
Cytosolic delivery is particularly important for intracellularly active proteins such as granzyme B (GzmB), but achieving efficient cytosolic access remains challenging because proteins must cross cellular membranes, avoid lysosomal degradation, and escape from endosomes.99 Liang et al developed a hyaluronic acid-EGCG conjugate (HA-EGCG)-based nanocarrier for cytosolic delivery of GzmB, a cytotoxic effector protein released by cytotoxic T lymphocytes and natural killer cells to eliminate pathogen-infected, premalignant, and malignant cells (Figure 5C).91 GzmB-loaded nanogels were formulated through noncovalent interactions between HA-EGCG and GzmB with the assistance of poly(ethylenimine) (PEI). The nanogels delivered GzmB into the cytosol of the cluster of determination 44 (CD44)-overexpressing cancer cells and induced CD44-targeted cancer cell killing. The observed cytotoxicity was attributed to GzmB-mediated apoptosis, indicating successful cytosolic delivery of functional GzmB. Sun et al developed melittin-loaded fluorinated EGCG NPs for cancer immunotherapy (Figure 5D).101 Melittin (MPI) is a 26-amino-acid cytolytic peptide derived from bee venom that exhibits antitumor and immunomodulatory activities;102 however, its clinical translation is hindered by pronounced hemolytic activity and systemic toxicity. To address these limitations, EGCG was modified with fluorinated linkers to generate fluorinated EGCG (FEGCG), thereby enhancing hydrophobic and lipophobic interactions. Through hydrophobic interactions and hydrogen bonding, FEGCG and MPI self-assembled into NPs (FEGCG@MPI NPs). In hepatoma models, these NPs modulated PD-L1 signaling via IRF and STAT1/pSTAT1 pathways and triggered apoptosis through regulation of Bcl-2 and Bax expression, reflecting synergistic actions of EGCG and MPI. Importantly, FEGCG@MPI NPs significantly reduced MPI-induced hemolysis, highlighting their potential as a safer and effective platform for antitumor immunotherapy.
Chemically Modified EGCG-Based Nanocarriers for Small Molecule Drug Delivery
Small molecule drug delivery using chemically modified EGCG carriers mainly takes advantage of the molecular compatibility between EGCG and aromatic or hydrophobic drugs. Through π–π stacking, hydrophobic interactions, hydrogen bonding, and coordination interactions, EGCG derivatives can promote drug association and organized nanocarrier formation in aqueous media. These features make chemically modified EGCG carriers particularly suitable for improving the loading, dispersion, and therapeutic performance of poorly soluble small molecule drugs. With this design principle, EGCG derivatives can self-assemble with various small molecule drugs to form spatially organized nanoarchitectures. In particular, small molecule drugs possessing multiring aromatic structures can form stable nanocomplexes with high drug loading efficiency when combined with EGCG-building carriers, owing to their structural similarity to EGCG.
Liang et al developed highly stable MNCs with exceptionally high drug loading based on the self-assembly of DOX and PEG-EGCG conjugates (Figure 6A).72 The MNC consisting of DOX/EGCG core surrounded by a PEG corona was constructed through favorable noncovalent interactions between EGCG and DOX, driven primarily by π–π stacking of aromatic rings. This design enabled an exceptionally high drug loading content of up to 88% (w/w) and imparted strong thermodynamic and kinetic stability. The DOX-MNC achieved a 25-fold increase in intratumoral DOX accumulation at 24 h relative to free DOX, along with a 16-fold extension in blood half-life and a 27-fold increase in area under the concentration–time curve. The formulation produced pronounced tumor growth suppression in a human liver cancer (HAK-1B) xenograft model with minimal systemic toxicity, whereas free DOX and the clinically approved liposomal formulation DOXIL failed to show efficacy at their lethal doses of 10 mg/kg. Collectively, these results highlight the potential of PEG-EGCG-based MNCs as a safe and effective platform for DOX delivery in cancer therapy. As described above, SU strongly interacts with EGCG, and co-administration of EGCG can markedly impair SU bioavailability, raising caution regarding EGCG intake during SU treatment.29 However, Yongvongsoontorn et al deliberately employed this EGCG–SU intermolecular interaction to construct an EGCG-building nanocarrier for SU delivery.93 The SU-loaded MNC (SU-MNC) was developed through self-assembly of SU and PEG-EGCG (Figure 6B). SU-MNC effectively inhibited VEGF-stimulated proliferation of human umbilical vein endothelial cells (HUVECs) and suppressed tumor growth in human renal cell carcinoma (HRCC) xenograft models through carrier–drug synergy while exhibiting minimal systemic toxicity. Compared with free SU, SU-MNC prolonged blood half-life and increased intratumoral SU accumulation by 2.2-fold and 5.1-fold in wild-type and SU-resistant HRCC tumors, respectively, while reducing accumulation in normal tissues. SU-MNC reduced the minimum effective dose by 50-fold compared with free SU and exhibited no apparent adverse effects even at doses higher than the maximum tolerated dose of free SU. By contrast, SU-loaded PEG-b-poly(lactic acid) polymeric micelles, used as a conventional nanocarrier control, reduced toxicity but failed to enhance antitumor efficacy despite showing drug loading capacity and tumor-targeting performance comparable to SU-MNC. This study demonstrated that EGCG-building nanocarriers can expand the therapeutic window of small molecule anticancer drugs beyond the safety improvements conferred by tumor-targeted delivery alone. Moreover, SU-MNC significantly inhibited the growth of SU-resistant A498 renal cell carcinoma xenografts at a 28-fold lower dose than conventional free SU treatment, indicating its potential to overcome SU resistance. Chuan et al synthesized folic acid-conjugated PEG-EGCG (FA-PEG-EGCG) and formulated DOX-loaded NPs (DOX/FA-PEG-EGCG NPs) through self-assembly of DOX and FA-PEG-EGCG for targeted delivery to ovarian cancer (Figure 6C).103 FA can bind specifically to folate receptors, enabling FA-modified NPs to enter tumor cells through receptor-mediated endocytosis. DOX/FA-PEG-EGCG NPs showed increased cellular uptake and anticancer efficacy in human ovarian cancer cells (SKOV3) and SKOV3 xenografts compared with NPs without FA modification. Liu et al enhanced the lipophilicity of EGCG by introducing 9-fluorenylmethoxycarbonyl (Fmoc) groups onto its phenolic hydroxyl moieties, enabling self-assembly with paclitaxel.104 This carrier system significantly improved cellular uptake and tumor-site delivery of paclitaxel, leading to pronounced tumor growth suppression, increased apoptotic responses, and reduced metastatic progression. Chen et al constructed self-assembled photodynamic nanocarriers (EGP-Ce6 NPs) by assembling PEG-EGCG with chlorin e6 (Ce6), a photosensitizer, for carrier-enhanced photodynamic cancer therapy (PDT) (Figure 6D).105 PEG-EGCG enabled efficient encapsulation of Ce6 into stable nanoplatforms through π–π stacking and hydrogen bonding interactions. Compared with free Ce6, EGP-Ce6 NPs exhibited enhanced cellular internalization, increased ROS generation, and elevated apoptosis in cancer cells, leading to effective suppression of cell proliferation through photodynamic action. Three-dimensional multicellular spheroid studies further demonstrated deep NP penetration into the spheroid core and efficient destruction of tumor cells after light irradiation. The PEG-EGCG segment acted as a bioactive antioxidant carrier that improved Ce6 solubility and stability, reduced aggregation-caused quenching, enhanced cellular uptake, and thereby amplified PDT efficiency.
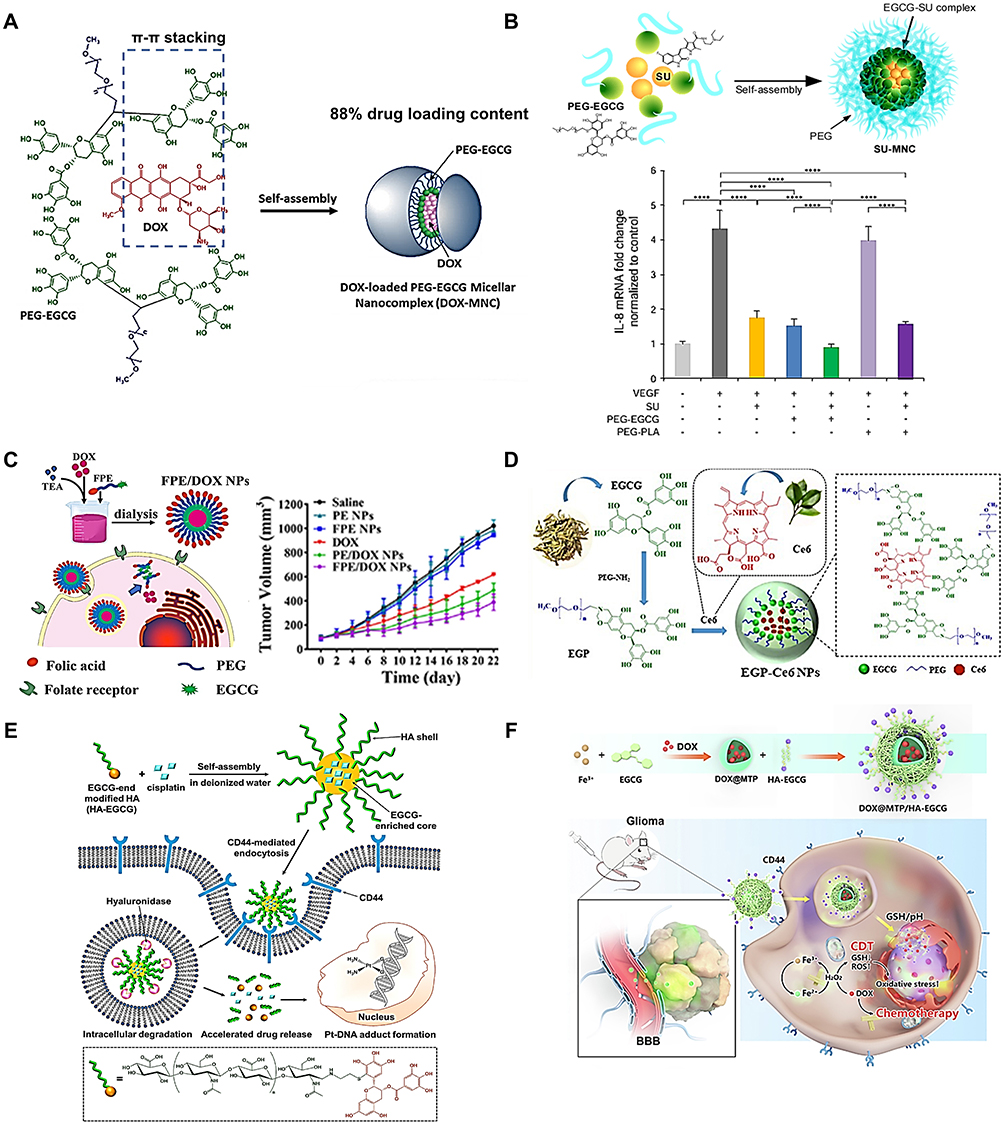 |
Figure 6 Chemically modified EGCG-based nanocarriers for small molecule drug delivery. (A) DOX-loaded PEG-EGCG MNC.72 (B) SU-loaded PEG-EGCG MNC and its synergistic inhibitory effects on IL-8 mRNA expression.93 (C) DOX-loaded FA-PEG-EGCG NP and its antitumor efficacy.103 (D) Ce6-loaded PEG-EGCG NP.105 (E) Cisplatin-loaded HA-EGCG MNC.92 (F) DOX-loaded Fe3+/EGCG/HA-EGCG NP.106, Reproduced with permission. Abbreviations: CD44, cluster of determination 44; Ce6, chlorin e6; DOX, doxorubicin; EGCG, (–)-epigallocatechin-3-gallate; FA, folic acid; HA-EGCG, hyaluronic acid-conjugated EGCG; MNC, micellar nanocomplex; MTP, metal-tea polyphenol network; NP, nanoparticle; PEG-EGCG, poly(ethylene glycol)-conjugated EGCG; SU, sunitinib. |
In recent years, safety concerns associated with exogenous synthetic materials have encouraged increasing attention to carrier designs based on endogenous or biodegradable materials. Although EGCG-building nanocarriers can reduce excipient burden by replacing inactive synthetic materials with pharmacoactive EGCG-building blocks that contribute to drug binding and structural stabilization, many formulations still use synthetic polymers such as PEG to achieve efficient drug delivery. PEG has long been regarded as a gold-standard material for increasing drug stability and circulation half-life; however, the emergence of PEG immunogenicity, as evidenced by anti-PEG serum antibodies, has raised concerns regarding reduced efficacy and severe adverse reactions in some PEGylated drugs.107 In pursuit of improved biocompatibility, emerging designs have employed EGCG derivatives coupled to bio-sourced materials to construct inherently safer nanocarriers.
Hyaluronic acid (HA) is an endogenous polysaccharide with favorable biocompatibility and biodegradability, supporting its use in drug delivery applications.108,109 HA can also bind to CD44, which is overexpressed on various cancer cells and tumor-associated angiogenic vascular cells, enabling receptor-mediated tumor targeting.109 This active targeting mechanism may enhance tumor and tumor-vasculature specificity in addition to passive tumor accumulation. For example, Bae et al developed CD44-targeted MNCs constructed by self-assembly of HA-EGCG and cisplatin for ovarian cancer treatment (Figure 6E).92 HA presented on the NP surface facilitated targeted cisplatin delivery to CD44-overexpressing cancer cells through receptor-mediated endocytosis, followed by enzyme-responsive drug release triggered by endosomal hyaluronidase. EGCG moieties contributed to favorable cisplatin loading and provided antioxidant protection against cisplatin-induced ROS-mediated toxicity. Pharmacokinetic and biodistribution studies revealed prolonged blood circulation and preferential tumor accumulation of the MNC compared with HA/cisplatin complexes and free cisplatin. The MNC exhibited superior antitumor efficacy over free cisplatin in both subcutaneous xenograft and peritoneal metastatic models of human ovarian cancer while showing no apparent systemic toxicity. Using the same HA-EGCG nanocarrier, sorafenib, daunorubicin (DNR), and gilteritinib were separately loaded into MNCs through self-assembly with HA-EGCG conjugates for acute myeloid leukemia (AML) treatment. Sorafenib-loaded MNCs significantly enhanced the antileukemic activity of sorafenib by selectively interfering with pro-survival mTOR signaling pathways.94 Biodistribution analyses revealed that the MNC achieved approximately 11-fold higher accumulation in bone marrow compared with free sorafenib. In an AML patient-derived xenograft model, treatment with the MNC effectively eliminated leukemic blasts within the bone marrow and markedly prolonged survival while exhibiting minimal off-target toxicity. A DNR-loaded MNC was engineered to release DNR, an anthracycline used as first-line therapy for AML, under mildly acidic conditions (pH 5.5) resembling the endosomal environment.95 Compared with free DNR, this MNC exhibited markedly enhanced cytotoxicity against multidrug-resistant leukemia cells, with median-effect analysis confirming strong synergistic activity. The chemosensitizing effect was attributed to increased nuclear accumulation of DNR, elevated intracellular ROS, and activation of caspase-dependent apoptosis. In a related system, gilteritinib, an FMS-like tyrosine kinase 3 (FLT3) inhibitor with limited stand-alone efficacy, was incorporated into an MNC and efficiently internalized by FLT3-mutant leukemia cells via CD44 receptor-mediated uptake.96 Combination index analysis demonstrated pronounced synergism arising from the combination of HA-EGCG and gilteritinib, resulting in enhanced antileukemic efficacy compared with free drug. This improvement was associated with augmented ROS production and increased caspase-3/7 activation. Furthermore, Mu et al developed a nanodelivery platform based on HA-EGCG containing reducible disulfide linkages for chemodynamic therapy of glioblastoma (Figure 6F).106 DOX-loaded metal–polyphenol networks (MTPs) were first formed through coordination between EGCG and Fe3⁺, followed by introduction of HA-EGCG via self-assembly to generate DOX@MTP/HA-EGCG. The system was designed so that MTPs dissociate in the acidic, glutathione (GSH)-rich intracellular environment, releasing DOX, EGCG, and Fe3⁺. EGCG subsequently reduces Fe3⁺ to Fe2⁺, enabling continuous Fenton conversion of H2O2 into hydroxyl radicals (•OH), thereby enhancing the chemotherapeutic effect of DOX. In addition, disulfide linkages within the HA-EGCG carrier depleted abnormally high intracellular GSH levels in tumor cells, further intensifying oxidative stress. The nanocomplexes selectively accumulated in glioblastoma tissue through CD44 receptor-mediated targeting and were retained in tumors for extended durations. Consequently, DOX@MTP/HA-EGCG significantly suppressed tumor progression and extended survival in tumor-bearing mice by integrating chemodynamic therapy with enhanced chemotherapy.
Yi et al developed NPs composed of covalently assembled catechins (EGCG ≥80% (w/w)) and hair keratin in the presence of formaldehyde as a biocompatible, colloidally stable, and stimuli-responsive nanocarrier for DOX delivery.110 The DOX-loaded NPs showed GSH-responsive drug release due to cleavage of disulfide bonds in keratin under reducing conditions and achieved enhanced anticancer efficacy with negligible systemic toxicity compared with free DOX in an HT-29 human colon cancer xenograft mouse model.
To improve the extremely low oral bioavailability of lycopene, a natural antioxidant, Li et al employed OEGCG as a carrier for oral lycopene delivery.111 OEGCG NPs containing lycopene were fabricated using a nanoprecipitation technique and subsequently coated with chitosan to generate an outer shell. The chitosan-coated OEGCG/lycopene NP system displayed pH-responsive release, with sustained lycopene release in acidic gastric media and accelerated release in simulated intestinal fluid. In vivo pharmacokinetic evaluation in mice demonstrated improved lycopene absorption with OEGCG/chitosan NPs compared with PLGA/chitosan-based systems, supporting their suitability for oral delivery applications.
Chemically Modified EGCG-Based Nanocarriers for Nucleic Acid Delivery
Although gene therapy has emerged as a powerful therapeutic approach for diverse diseases by modulating pathogenic pathways at the genetic level, its clinical application remains limited by the lack of efficient and safe nucleic acid delivery systems. Conventional polymeric carriers typically compact DNA or RNA through electrostatic interactions, which often require polymers with high molecular weights or dense cationic charge.112 However, such strongly cationic materials can induce cytotoxicity, membrane disruption, inflammatory responses, and limited biocompatibility.
EGCG-based carriers provide an alternative strategy for nucleic acid delivery by exploiting the intrinsic binding affinity of EGCG toward DNA and RNA. EGCG can interact with nucleic acids through hydrogen bonding, π–π stacking, hydrophobic interactions, and other noncovalent forces, enabling nanocomplex formation while potentially reducing reliance on highly cationic polymers. In particular, chemically modified EGCG architectures can further improve complex stability, serum resistance, and targeting capability. These features may support safer and more efficient delivery of plasmid DNA, siRNA, and other nucleic acid therapeutics. The following examples illustrate how EGCG-building nanocarriers have been engineered to overcome key barriers in nucleic acid delivery.
For example, HA-EGCG was used to stabilize preformed plasmid DNA (pDNA)/PEI complexes through the strong affinity of EGCG for nucleic acids, forming a ternary nanocomplex for targeted gene delivery (Figure 7A).90 The pDNA/PEI/HA-EGCG nanocomplex showed enhanced resistance to nuclease attack, partly due to the enzyme-inhibitory effect of EGCG, and promoted successful endosomal escape, demonstrating its ability to overcome major barriers in gene therapy. The nanocomplex also facilitated delivery into CD44-overexpressing colon cancer cells (HCT-116), which are typically difficult to transfect, even in serum-containing media. Compared with pDNA/PEI/HA nanocomplexes, the HA-EGCG-containing nanocomplex showed enhanced stability, CD44-targeting capability, and higher transfection efficiency both in vitro and in vivo. Wu et al developed PD-L1 siRNA-loaded FEGCG/Zn/erythrocyte NPs for cancer immunotherapy (Figure 7B).113 Fluorinated, zinc-coordinated EGCG NPs (FEGCG/Zn) were generated by incorporating fluorine moieties and Zn2+ ions into EGCG, enabling the assembly of nanostructures capable of carrying diverse cargos, including small molecule chemotherapeutics such as sorafenib, gemcitabine, and DOX, as well as nucleic acids, peptides, and proteins. These NPs were subsequently anchored onto erythrocytes to extend systemic circulation. Erythrocyte hitchhiking enhanced intratumoral accumulation of PD-L1 siRNA, while co-delivery with FEGCG/Zn potentiated T cell-mediated cancer cell killing, likely through blockade of the PD-1/PD-L1 inhibitory axis that suppresses infiltrating CD8+ T cell activity. Collectively, these findings indicate that FEGCG/Zn can function both as a PD-L1 inhibitory component and as a versatile carrier for immune biomolecule delivery via cell-based transport.
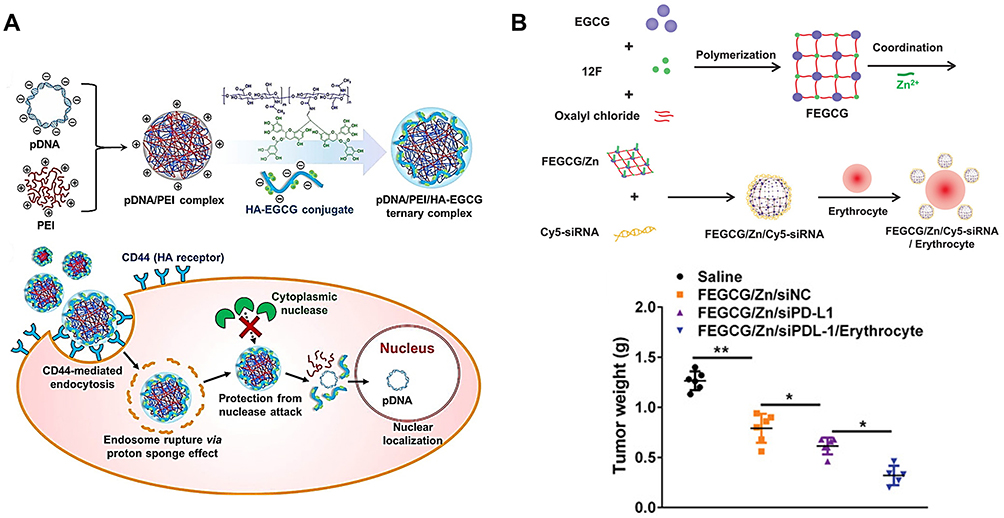 |
Figure 7 Chemically modified EGCG-based nanocarriers for nucleic acid delivery. (A) pDNA-loaded PEI/HA-EGCG nanocomplex.90 (B) PD-L1 siRNA-loaded FEGCG/Zn/erythrocyte NP.113 Reproduced with permission. *p < 0.05, **p < 0.01 by one-way ANOVA analysis. Abbreviations: CD44, cluster of determination 44; EGCG, (–)-epigallocatechin-3-gallate; FEGCG, fluorinated EGCG; HA-EGCG, hyaluronic acid-conjugated EGCG; NP, nanoparticle; pDNA, plasmid DNA; PEI, poly(ethylenimine); siRNA, small interfering RNA. |
Representative chemically modified EGCG-based nanocarriers for protein, small molecule, and nucleic acid delivery are summarized in Table 3, highlighting how EGCG modification enables more organized nanocarrier architectures with improved loading, stability, targeting, and therapeutic performance.
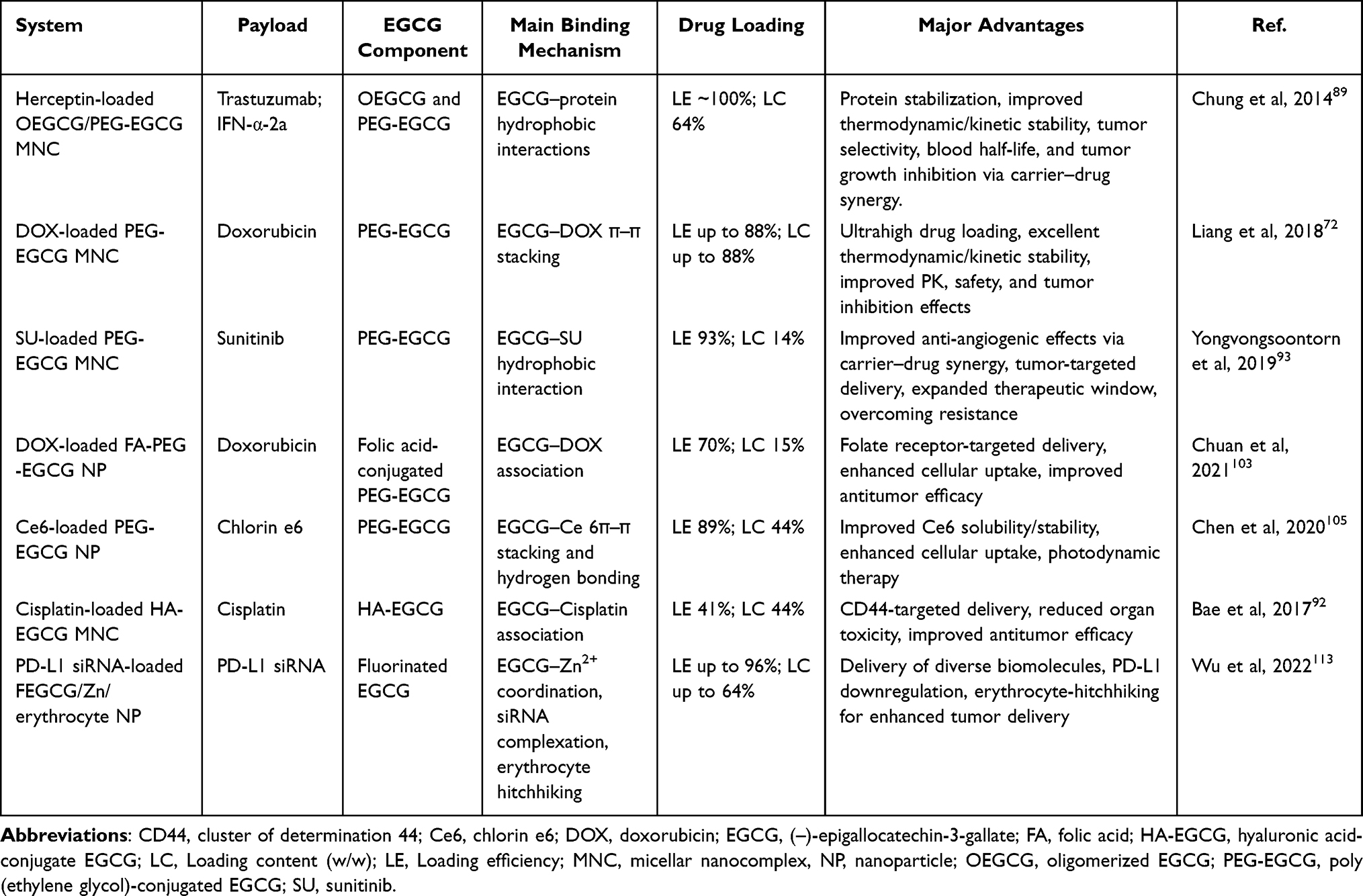 |
Table 3 Representative Chemically Modified EGCG-Based Nanocarriers |
EGCG-Building Nanocarriers versus Conventional Encapsulation Strategies
The examples discussed above demonstrate that EGCG-building nanocarriers are conceptually distinct from conventional encapsulation-based delivery systems. Conventional nanocarriers have contributed substantially to drug delivery by improving drug solubility, pharmacokinetics, biodistribution, and controlled release. Although these systems vary widely in formulation design and include several clinically established platforms, their therapeutic contribution is mainly derived from the loaded drug, whereas the carrier itself primarily serves delivery functions.
A key formulation constraint in conventional nanocarriers is the drug loading dilemma. In many systems, the API constitutes only a small fraction of the total NP mass, meaning that most of the administered NP dose consists of pharmacologically inert carrier materials rather than active ingredients.6 Although such materials, including lipids, synthetic polymers such as PEG, and inorganic components, are generally considered biocompatible, their cumulative exposure may contribute to carrier-associated toxicity, immunogenicity, or undesired tissue accumulation.7,8
To address the low-loading limitation of conventional carriers, minimal-carrier and carrier-free nanomedicines, including prodrug assemblies, drug–drug conjugates, and drug-rich self-assembled systems, have also been explored.114,115 These strategies can substantially increase drug content by reducing inactive excipients, in some cases to 15–95% (w/w); however, they may also introduce new challenges, including colloidal instability, premature drug release, complex synthesis, and limited batch-to-batch reproducibility.
In contrast, EGCG-building nanocarriers use EGCG as a carrier-forming and pharmacoactive component. Through multivalent interactions, including π–π stacking, hydrogen bonding, hydrophobic interactions, metal coordination, and dynamic covalent bonding, EGCG can support the incorporation of structurally diverse payloads and contribute to nanocarrier assembly. This interaction-driven design may reduce reliance on inert carrier materials while enabling the carrier component to participate not only in drug loading and stabilization but also in therapeutic activity. In addition, the antioxidant, anti-inflammatory, anticancer, chemosensitizing, and resistance-modulating activities of EGCG may cooperate with the payload, distinguishing EGCG from auxiliary excipients or simply co-loaded therapeutic agents.
Another important distinction is payload adaptability. In conventional nanocarriers, carrier composition and formulation parameters often need to be optimized for each payload because drug loading depends strongly on drug-specific physicochemical properties and compatibility with the carrier matrix. By contrast, the multivalent interaction capacity of EGCG can enable adaptable loading of structurally diverse payloads through multiple favorable interactions.
A concise comparison of conventional encapsulation strategies and EGCG-building nanocarriers is provided in Table 4. As summarized, EGCG-building nanocarriers represent an emerging pharmacoactive nanocarrier platform with potential to serve as an alternative to inert carrier-based DDS by integrating delivery and therapeutic functions. The physicochemical and translational issues that must be addressed to realize this potential are discussed in the following section.
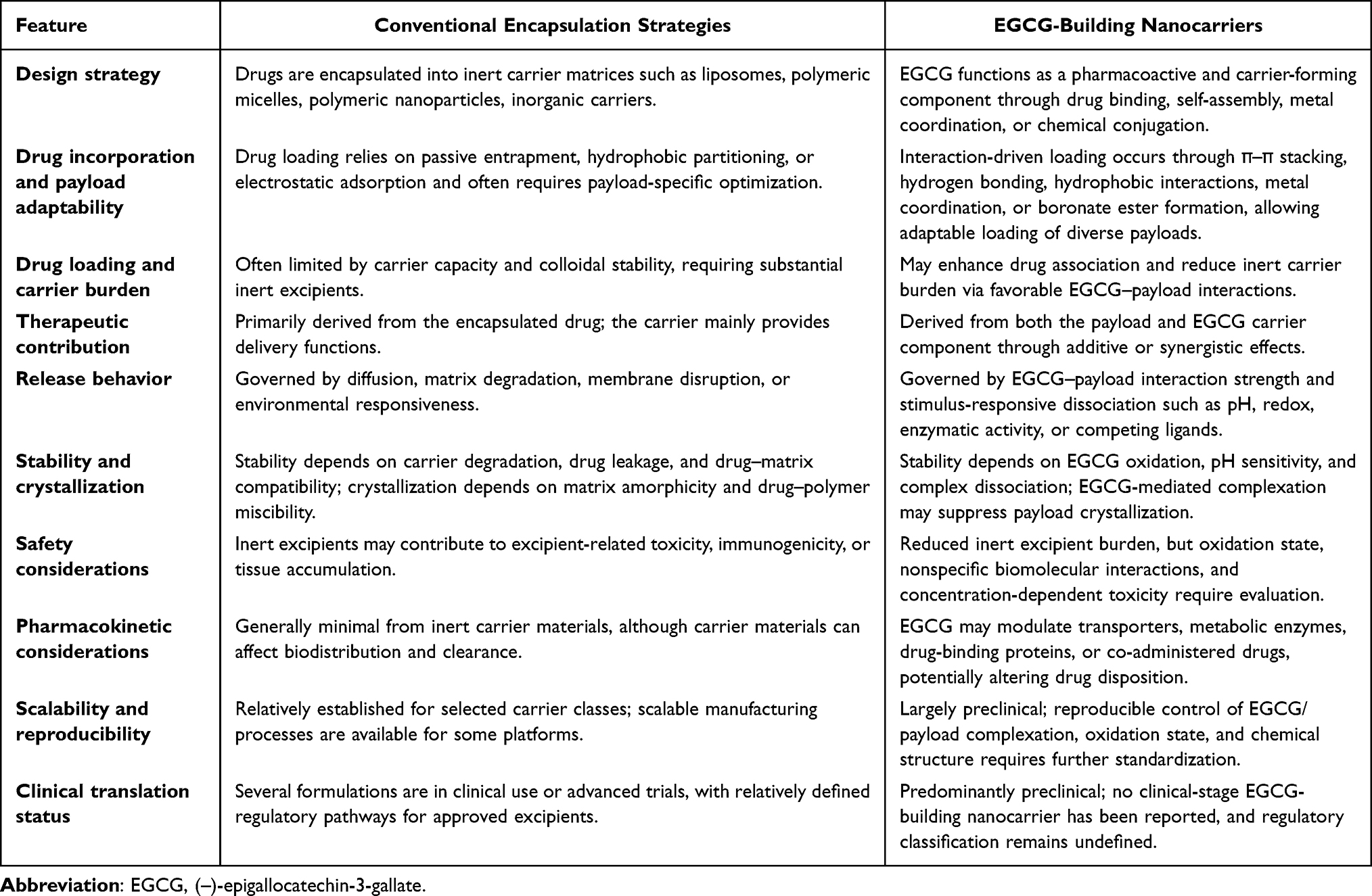 |
Table 4 Comparison of EGCG-Building Nanocarriers and Conventional Encapsulation Strategies |
Physicochemical Consideration, Translational Challenges, and Future Perspectives
EGCG-building nanocarriers represent a promising pharmacoactive delivery platform because EGCG can function simultaneously as a drug-binding element, structural carrier component, and therapeutic contributor. By integrating these roles, EGCG-building systems can improve drug loading, stabilize payloads within nanoscale assemblies, reduce reliance on pharmacologically inert excipients, and promote cooperative therapeutic effects between the carrier and payload. Chemically modified EGCG derivatives further enable more organized nanostructures with improved stability, tunable release behavior, and enhanced pharmacokinetic performance. This shift in carrier function, from serving merely as an inert excipient to acting as a therapeutic contributor, represents a significant conceptual advancement in nanomedicine design and may help address long-standing constraints such as low drug loading and modest therapeutic benefit. Nevertheless, these advantages remain largely preclinical, and several physicochemical, biological, and translational challenges must be addressed before clinical application.
Besides EGCG, other polyphenol-based nanocarriers have also been studied, and their formulation properties differ substantially depending on the molecular characteristics of the polyphenol used. For instance, curcumin is a representative pharmacoactive polyphenol that has been widely investigated for nanomedicine applications because of its anticancer, anti-inflammatory, and antioxidant activities.14 However, curcumin is highly hydrophobic and poorly water-soluble, and its crystallization or aggregation can limit formulation stability and bioavailability. By comparison, EGCG is relatively more water-compatible and contains catechol and galloyl groups that enable diverse interactions with therapeutic payloads. A defining advantage of EGCG-building nanocarriers is that structurally diverse drugs can be complexed or assembled into nanostructures in aqueous media through favorable EGCG–drug interactions. These interaction-driven assemblies can facilitate efficient drug loading without requiring large amounts of synthetic polymers or organic solvents, thereby supporting a simpler and potentially less excipient-intensive formulation strategy. Nevertheless, EGCG is more susceptible to oxidation and pH-dependent degradation in aqueous and physiological environments. Thus, the key formulation challenges differ among polyphenol-based systems: curcumin-based systems often require strategies to improve solubilization and suppress crystallization, whereas EGCG-building systems require precise control of oxidation, interaction dynamics, and biological fluid-induced complex dissociation.
In this context, solubility, crystallization, and aggregation behavior also require systematic evaluation. Free EGCG is relatively water-soluble compared with highly hydrophobic polyphenols such as curcumin, but many therapeutic payloads incorporated into EGCG-building nanocarriers are poorly water-soluble aromatic drugs. EGCG-mediated complexation can improve apparent aqueous dispersibility by promoting nanoscale assembly through aromatic stacking, hydrogen bonding, hydrophobic interactions, or coordination bonds. In some systems, EGCG-based carriers may also suppress drug crystallization by maintaining payloads in an amorphous, molecularly associated, or nanoscale dispersed state within the nanostructure.116 However, this benefit is formulation-dependent. Insufficiently controlled EGCG–payload interactions may result in partial crystallization, aggregation, or precipitation during storage, dilution, or exposure to biological fluids, thereby altering drug loading, release kinetics, biodistribution, and toxicity. Therefore, future characterization should include not only particle size and drug loading but also payload crystallinity, amorphous stability, aggregation behavior, colloidal stability, and physical stability under storage and physiologically relevant conditions.
A central challenge is the intrinsic chemical instability of EGCG. As a polyphenolic compound, EGCG can undergo autoxidation and react with oxygen or metal ions, and it may degrade upon exposure to light, elevated temperature, pH variations, or enzymatic activity.22 This instability can complicate manufacturing because oxidation may occur during conjugation or NP formation, producing heterogeneous reaction by-products and leading to variable molecular structures, inconsistent drug-to-carrier ratios, and batch-to-batch variability. For example, oxidation-driven self-assembly strategies, often involving metal ions or oxidative enzymes, have been widely explored because they enable facile NP formation, but the precise chemical identities of oxidized intermediates are often poorly defined, and structural heterogeneity remains insufficiently characterized.117 Given that the antioxidant, anticancer, and anti-inflammatory activities of EGCG are structure-dependent, controlling its oxidation state is essential for reproducible therapeutic performance. In vivo, EGCG is also vulnerable to oxidation after administration, producing quinones or other reactive intermediates that may form unwanted adducts with biomolecules, potentially leading to off-target effects or premature loss of activity.118 While EGCG’s redox behavior can be therapeutically advantageous, for example by participating in redox cycling or enhancing ROS levels in tumors, it may simultaneously cause unintended biological outcomes. Importantly, conjugation of EGCG to polymers or assembly into hierarchically organized structures has been shown to markedly improve oxidation resistance compared with free EGCG.22,119 In organized structures, EGCG may be physically shielded within hydrophobic domains or sterically protected by polymer shells, limiting exposure to oxidative triggers. These observations are promising, yet systematic studies examining oxidation kinetics, degradation pathways, and in vivo chemical stability of EGCG within nanostructures remain limited. Therefore, validation of EGCG structural integrity under storage, physiological, and disease-specific conditions will be important for further development.
EGCG–payload interaction dynamics are another important determinant of nanocarrier performance. The multimodal interactions of EGCG enable efficient loading of diverse payloads, ranging from hydrophobic small molecule drugs to hydrophilic biomacromolecules such as proteins and nucleic acids. These interactions can enable high drug loading and reversible association with fragile biomolecules, helping to preserve their structure and activity, which is often challenging for conventional polymeric or lipid carriers. However, the same interaction-driven design requires careful control. Although strong EGCG–drug binding promotes drug encapsulation and prevents premature leakage during circulation, excessively strong binding may hinder payload release at the disease site. Conversely, weak or unstable interactions may lead to premature dissociation during dilution or exposure to biological fluids. To balance robust drug loading with responsive release, careful selection of drugs with well-defined interaction modes, together with rational carrier design, is required.
The broad binding capacity of EGCG may also influence biological interactions after administration. EGCG does not exclusively bind therapeutic payloads; it can also interact with endogenous proteins, nucleic acids, lipophilic molecules, transporters, and metabolic enzymes. When EGCG moieties are exposed on nanoparticle surfaces, interactions with circulating proteins may contribute to protein corona formation, altered biodistribution, immunological recognition, or unintended biological activity. Hydrophilic shells such as PEG or polysaccharides are therefore commonly used to shield EGCG–payload complexes and reduce nonspecific interactions. However, some unshielded or minimally shielded EGCG-based assemblies formed through oxidative or metal-coordination crosslinking have shown efficient delivery and antitumor efficacy without apparent acute toxicity, suggesting that the biological consequences of surface-exposed EGCG remain system-dependent and incompletely understood. Further studies on nanoparticle morphology, surface chemistry, protein corona formation, and in vivo fate are needed to support predictable biological performance.
The synergistic therapeutic effect enabled by EGCG-building nanocarriers represents one of their most transformative advantages. Besides enabling drug loading and delivery, EGCG directly participates in therapy by modulating signaling pathways, altering redox balance, inhibiting multidrug resistance transporters, and protecting normal tissues from drug-induced toxicity. These actions may enable enhanced therapeutic outcomes at lower drug doses and expand therapeutic windows for otherwise toxic drugs. Although numerous studies have reported improved efficacy in vitro and in vivo using EGCG-building nanocarriers, only a limited number have quantitatively and mechanistically evaluated synergy through combination index analysis, pathway elucidation, or computational assessment. Because synergy underpins the rationale for EGCG-building nanocarriers in addressing the limited efficacy of traditional low-loading formulations, robust and mechanistically grounded evidence of such synergy is indispensable for advancing these systems toward clinical translation and regulatory approval.
In addition, EGCG-containing carriers may influence drug disposition, particularly when they produce high local or systemic EGCG exposure. Because EGCG can modulate drug transporters and metabolic enzymes and can directly bind certain therapeutic agents,50 EGCG-building nanocarriers should be evaluated not only as delivery systems but also as potential modifiers of pharmacokinetics and biodistribution. This consideration is particularly important for drugs with narrow therapeutic windows, limited solubility, transporter-dependent absorption or clearance, or known sensitivity to catechol/boronate interactions. Comparative pharmacokinetic studies using free drug, free EGCG plus drug, blank EGCG-building carrier, drug-loaded EGCG-building nanocarrier, and, where relevant, co-administered drugs would help distinguish nanocarrier-mediated delivery effects from EGCG-mediated pharmacokinetic interactions.
Safety considerations are also polyphenol-specific and dose-dependent. Although polyphenols are often perceived as biocompatible natural compounds, their biological activities can change at pharmacological concentrations. Curcumin and other polyphenols have been reported to show formulation- and dose-dependent cytotoxic or pro-oxidant effects under certain conditions.120 Similarly, EGCG can exert antioxidant or pro-oxidant effects depending on concentration, redox environment, metal ion availability, and cellular context, and high systemic exposure has been associated with hepatotoxicity concerns.21 Therefore, EGCG-building nanocarriers should be evaluated based on EGCG-equivalent dose, release kinetics, oxidation state, tissue exposure, and repeated dose safety, rather than assuming safety solely from the dietary origin of EGCG. Such evaluation should also consider whether high EGCG-equivalent exposure from the carrier alters the disposition or toxicity of the loaded drug or concomitantly administered medications.
Long-term safety and manufacturability remain major translational considerations. Repeated administration may raise concerns about accumulation of non-degradable or slowly eliminated components, particularly in formulations containing inorganic materials used for coordination, imaging, catalysis, or chemodynamic therapy.121 Although many NPs containing inorganic materials have demonstrated useful potential for catalysis, bioimaging, and targeting, safety remains a well-recognized barrier to their clinical translation.122 Immunogenic carrier segments, including certain polymers, peptides, or targeting ligands, may also induce immune activation, reduce therapeutic efficacy, or cause immediate or delayed adverse reactions after repeated exposure. Although many short-term preclinical studies have shown acceptable safety, comprehensive evaluation of pharmacokinetics, metabolism, biodegradation, immunogenicity, organ accumulation, and chronic toxicity will be necessary. From a manufacturing perspective, chemically modified EGCG systems require rigorous control of chemical structure, substitution degree, purity, oxidation state, batch-to-batch consistency, and scalable synthesis, in addition to the EGCG stability issues discussed above.
Finally, the route of administration will strongly affect clinical feasibility. Most EGCG-building nanocarriers have been evaluated by parenteral injection, whereas non-invasive routes may be desirable for chronic diseases because they can improve patient convenience and adherence. Oral delivery is particularly challenging because nanocarriers must maintain structural integrity in the gastrointestinal tract, withstand acidic and enzymatic environments, and cross the intestinal epithelium. These requirements are especially demanding for protein and peptide payloads. Only a limited number of EGCG-building nanocarriers have demonstrated improved oral bioavailability of small molecule drugs. Further development of oral or other non-invasive systems will require protection of both EGCG moieties and payloads from degradation, together with nanostructure engineering strategies such as mucoadhesive design, surface charge optimization, and absorption enhancement.
Taken together, the clinical translation of EGCG-building nanocarriers will require coordinated advances in EGCG molecular engineering, mechanistic understanding of EGCG–payload and EGCG–biomolecule interactions, standardized physicochemical characterization, scalable manufacturing, and rigorous pharmacokinetic and safety evaluation. With continued progress in these areas, EGCG-building systems have strong potential to advance from promising preclinical platforms to clinically meaningful pharmacoactive nanocarriers.
Conclusions
EGCG-building nanocarriers represent an emerging class of pharmacoactive delivery systems that integrate structural and therapeutic functions within a single platform. By exploiting the multivalent binding capacity and intrinsic bioactivity of EGCG, these systems can promote efficient payload association, reduce reliance on pharmacologically inert carrier materials, and enable cooperative therapeutic effects between the carrier and payload. Unlike many conventional nanocarriers, in which therapeutic performance is primarily determined by the loaded drug, EGCG-building architectures allow the carrier component itself to contribute to drug stabilization, controlled release, resistance-modulation, toxicity reduction, and therapeutic efficacy.
Current evidence remains largely preclinical, with many studies focused on cancer therapy, but the concept may be extendable to other disease areas when EGCG–payload interactions, carrier stability, and biological behavior are appropriately controlled. Several challenges may explain the current translational gap. In relatively simple EGCG–drug nanocomplexes or metal–phenolic assemblies, oxidation sensitivity, dynamic EGCG–payload interactions, and biological fluid-induced dissociation may affect formulation reproducibility, stability, and release behavior. Chemically modified EGCG systems may partially address these limitations through more controlled molecular design and hierarchical assembly, but they require rigorous characterization of chemical structure, substitution degree, purity, oxidation state, batch-to-batch consistency, scalability, and degradation behavior.
Future development will require precise control of EGCG chemistry, standardized characterization of drug loading, release profiles, surface properties, colloidal stability, oxidation state, and degradation behavior, together with rigorous pharmacokinetic, biodistribution, immunogenicity, and toxicity evaluation. Particular attention should also be given to the potential influence of EGCG-containing carriers on the disposition and safety of loaded drugs and concomitantly administered medications. With these advances, EGCG-building systems may progress from promising preclinical platforms to clinically meaningful pharmacoactive nanocarriers capable of improving therapeutic efficacy while reducing inert carrier burden.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. John J. Advancements in nano-based drug delivery systems for therapeutics: a comprehensive review. RSC Pharmaceutics. 2026;3(1):43–30. doi:10.1039/D5PM00179J
2. Zeinali R, Zaeifi D, Zolfaghari-Moghaddam SY, Paul MK, Biazar E. Current advances in nanocarriers for cancer therapy. Int J Nanomed. 2025;20:12217–12262. doi:10.2147/IJN.S548088
3. Jacob S, Varkey NR, Boddu SHS, Gorain B, Rao R, Nair AB. Advances in lipid-polymer hybrid nanoparticles: design strategies, functionalization, oncological and non-oncological clinical prospects. Pharmaceuticals. 2025;18(12):1–41. doi:10.3390/ph18121772
4. Kim M, Shin M, Zhao Y, Ghosh M, Son Y-O. Transformative impact of nanocarrier-mediated drug delivery: overcoming biological barriers and expanding therapeutic horizons. Small Sci. 2024;4(11):2400280. doi:10.1002/smsc.202400280
5. Wang G, Wang N, Xia X, Ismail M, Shi B. Clinical translation of nanomedicines for brain diseases: current challenges and future directions. J Control Release off J Control Release Soc. 2026;389:114426. doi:10.1016/j.jconrel.2025.114426
6. Liu Y, Yang G, Jin S, Xu L, Zhao C-X. Development of high-drug-loading nanoparticles. ChemPlusChem. 2020;85(9):2143–2157. doi:10.1002/cplu.202000496
7. Cheng H, Liao J, Ma Y, Sarwar MT, Yang H. Advances in targeted therapy for tumor with nanocarriers: a review. Mater Today Bio. 2025;31:101583. doi:10.1016/j.mtbio.2025.101583
8. Jan N, Shah H, Shi G. Biomimetic approaches against accelerated blood clearance (ABC) phenomenon of nanoparticulate drug delivery systems. Int J Pharm. 2025;680:125753. doi:10.1016/j.ijpharm.2025.125753
9. Etter EL, Mei K-C, Nguyen J. Delivering more for less: nanosized, minimal-carrier and pharmacoactive drug delivery systems. Adv Drug Deliv Rev. 2021;179:113994. doi:10.1016/j.addr.2021.113994
10. Xue S, Tan W, Mao S, et al. Polyphenol-based functional materials: structural insights, composite strategies, and biomedical applications. Adv Sci. 2025;12(39):e08924. doi:10.1002/advs.202508924
11. Zhou J, Lin Z, Ju Y, Rahim MA, Richardson JJ, Caruso F. Polyphenol-mediated assembly for particle engineering. Acc Chem Res. 2020;53(7):1269–1278. doi:10.1021/acs.accounts.0c00150
12. Jiang X, Zhang J, Lo PK, Mao Z. Polyphenol-based assembly nanosystems as multifunctional biopharmaceutical platform. Adv NanoBiomed Res. 2023;3(6):2200168. doi:10.1002/anbr.202200168
13. Liang H, Zhou B, Wu D, Li J, Li B. Supramolecular design and applications of polyphenol-based architecture: a review. Adv Colloid Interface Sci. 2019;272:102019. doi:10.1016/j.cis.2019.102019
14. Magini A, Datti A. Curcumin between pleiotropic potential and translational constraints. Int J Mol Sci. 2026;27(5):2212. doi:10.3390/ijms27052212
15. Neisiany RE, Enayati M, Das O. Tannic acid-based platforms for biomedical applications. Mater Chem Horizons. 2024. https://api.semanticscholar.org/CorpusID:274123566.
16. Alam M, Gulzar M, Akhtar MS, et al. Epigallocatechin-3-gallate therapeutic potential in human diseases: molecular mechanisms and clinical studies. Mol Biomed. 2024;5(1):73. doi:10.1186/s43556-024-00240-9
17. Mokra D, Joskova M, Mokry J. Therapeutic effects of green tea polyphenol (‒)-Epigallocatechin-3-Gallate (EGCG) in relation to molecular pathways controlling inflammation, oxidative stress, and apoptosis. Int J Mol Sci. 2022;24(1):340. doi:10.3390/ijms24010340
18. Radeva-Ilieva M, Stoeva S, Hvarchanova N, Georgiev KD. Green tea: current knowledge and issues. Foods. 2025;14(5). doi:10.3390/foods14050745
19. Rovaldi E, Di Donato V, Paolino G, et al. Epigallocatechin-Gallate (EGCG): an essential molecule for human health and well-being. Int J Mol Sci. 2025;26(18):1–20. doi:10.3390/ijms26189253
20. Wang L, Li P, Feng K. EGCG adjuvant chemotherapy: current status and future perspectives. Eur J Med Chem. 2023;250(February):115197. doi:10.1016/j.ejmech.2023.115197
21. Acosta L, Byham-Gray L, Kurzer M, Samavat H. Hepatotoxicity with high-dose green tea extract: effect of Catechol-O-methyltransferase and uridine 5’-diphospho-glucuronosyltransferase 1A4 genotypes. J Diet Suppl. 2023;20(6):850–869. doi:10.1080/19390211.2022.2128501
22. Yongvongsoontorn N, Kihara M, Inada M, Chung JE, Kurisawa M. Suppressed autoxidation, enhanced antioxidant activity, and improved cytocompatibility of epigallocatechin gallate via alginate site-specific conjugation with tunable substitution degree. Int J Mol Sci. 2025;26(17):8725. doi:10.3390/ijms26178725
23. Liu Q, He Y, Fang Y, et al. Emerging self-assembled nanoparticles constructed from natural polyphenols for intestinal diseases. Adv NanoBiomed Res. 2023;3(11):2300046. doi:10.1002/anbr.202300046
24. Guo Y, Sun Q, Wu F-G, Dai Y, Chen X. Polyphenol-containing nanoparticles: synthesis, properties, and therapeutic delivery. Adv Mater. 2021;33(22):2007356. doi:10.1002/adma.202007356
25. Feng J, Wei X, Huang Q, et al. Polyphenol functional self-assembled drug delivery systems: mechanism, application, and future intelligent precision assembly mode. Nano Res. 2024;18(6):94907608. doi:10.26599/NR.2025.94907608
26. Luo K-W, Zhu X-H, Zhao T, et al. EGCG enhanced the anti-tumor effect of doxorubicine in bladder cancer via NF-κB/MDM2/p53 pathway. Front Cell Develop Biol. 2020;8:606123. doi:10.3389/fcell.2020.606123
27. Wang X, Jiang P, Wang P, Yang CS, Wang X, Feng Q. EGCG enhances Cisplatin sensitivity by regulating expression of the copper and cisplatin influx transporter CTR1 in ovary cancer. PLoS One. 2015;10(4):1–16. doi:10.1371/journal.pone.0125402
28. Golden EB, Lam PY, Kardosh A, et al. Green tea polyphenols block the anticancer effects of bortezomib and other boronic acid–based proteasome inhibitors. Blood. 2009;113(23):5927–5937. doi:10.1182/blood-2008-07-171389
29. Ge J, Tan B-X, Chen Y, et al. Interaction of green tea polyphenol epigallocatechin-3-gallate with sunitinib: potential risk of diminished sunitinib bioavailability. J Mol Med. 2011;89(6):595–602. doi:10.1007/s00109-011-0737-3
30. Haque A, Rahman MA, Chen ZG, et al. Combination of erlotinib and EGCG induces apoptosis of head and neck cancers through posttranscriptional regulation of Bim and Bcl-2. Apoptosis. 2015;20(7):986–995. doi:10.1007/s10495-015-1126-0
31. Zhou Y, Qin L, Li C, Zhu D, Liu B. EGCG enhances antitumor effect of apatinib in nonsmall cell lung cancer by targeting VEGF signaling to inhibit glycolysis. Drug Dev Res. 2024;85(7):e22239. doi:10.1002/ddr.22239
32. Yang L, Fang Y, He Y, Zhang J. (−)-Epigallocatechin-3-Gallate and quercetin inhibit quiescin sulfhydryl oxidase 1 secretion from hepatocellular carcinoma cells. Antioxidants. 2025;14(1):106. doi:10.3390/antiox14010106
33. Moracci L, Sensi F, Biccari A, et al. An investigation on [5 fluorouracil and epigallocatechin-3-gallate] complex activity on HT-29 cell death and its stability in gastrointestinal fluid. Oncotarget. 2022;13(1):476–489. doi:10.18632/oncotarget.28207
34. Wei R, Hackman RM, Wang Y, Mackenzie GG. Targeting Glycolysis with Epigallocatechin-3-Gallate enhances the efficacy of chemotherapeutics in pancreatic cancer cells and xenografts. Cancers. 2019;11(10):1496. doi:10.3390/cancers11101496
35. Chen B, Liu G, Zou P, et al. Epigallocatechin-3-gallate protects against cisplatin-induced nephrotoxicity by inhibiting endoplasmic reticulum stress-induced apoptosis. Exp Biol Med. 2015;240(11):1513–1519. doi:10.1177/1535370215573394
36. Pan H, Chen J, Shen K, et al. Mitochondrial Modulation by Epigallocatechin 3-Gallate Ameliorates Cisplatin Induced Renal Injury through Decreasing Oxidative/Nitrative Stress, Inflammation and NF-kB in Mice. PLoS One. 2015;10(4):e0124775. doi:10.1371/journal.pone.0124775
37. Arafa MH, Atteia HH. Protective role of Epigallocatechin Gallate in a rat model of cisplatin-induced cerebral inflammation and oxidative damage: impact of modulating NF-κB and Nrf2. Neurotox Res. 2020;37(2):380–396. doi:10.1007/s12640-019-00095-x
38. Borse V, Al Aameri RFH, Sheehan K, et al. Epigallocatechin-3-gallate, a prototypic chemopreventative agent for protection against cisplatin-based ototoxicity. Cell Death Dis. 2017;8(7):e2921. doi:10.1038/cddis.2017.314
39. Zhang T, Li N, Wang R, et al. Enhanced therapeutic efficacy of doxorubicin against multidrug-resistant breast cancer with reduced cardiotoxicity. Drug Deliv. 2023;30(1):2189118. doi:10.1080/10717544.2023.2189118
40. Saeed NM, El-Naga RN, El-Bakly WM, Abdel-Rahman HM, Salah ElDin RA, El-Demerdash E. Epigallocatechin-3-gallate pretreatment attenuates doxorubicin-induced cardiotoxicity in rats: a mechanistic study. Biochem Pharmacol. 2015;95(3):145–155. doi:10.1016/j.bcp.2015.02.006
41. He H, Wang L, Qiao Y, et al. Epigallocatechin-3-gallate pretreatment alleviates doxorubicin-induced ferroptosis and cardiotoxicity by upregulating AMPK α adaptive autophagy. Redox Biology. 2021;48:102185. doi:10.1016/j.redox.2021.102185
42. Zhou H, Fu L-X, Li L, et al. The epigallocatechin gallate derivative Y6 reduces the cardiotoxicity and enhances the efficacy of daunorubicin against human hepatocellular carcinoma by inhibiting carbonyl reductase 1 expression. J Ethnopharmacol. 2020;261:113118. doi:10.1016/j.jep.2020.113118
43. Tsai MJ, Chang WA, Liao SH, Chang KF, Sheu CC, Kuo PL. The effects of Epigallocatechin Gallate (EGCG) on pulmonary fibroblasts of Idiopathic Pulmonary Fibrosis (IPF)-A next-generation sequencing and bioinformatic approach. Int J Mol Sci. 2019;20(8):1958. doi:10.3390/ijms20081958
44. La X, Zhang L, Li Z, Li H, Yang Y. (−)-Epigallocatechin Gallate (EGCG) enhances the sensitivity of colorectal cancer cells to 5-FU by inhibiting GRP78/NF-κB/miR-155-5p/MDR1 pathway. J Agric Food Chem. 2019;67(9):2510–2518. doi:10.1021/acs.jafc.8b06665
45. Tang H, Zeng L, Wang J, et al. Reversal of 5-fluorouracil resistance by EGCG is mediate by inactivation of TFAP2A/VEGF signaling pathway and down-regulation of MDR-1 and P-gp expression in gastric cancer. Oncotarget. 2017;8(47):82842–82853. doi:10.18632/oncotarget.20666
46. Li Y, Meeran SM, Tollefsbol TO. Combinatorial bioactive botanicals re-sensitize tamoxifen treatment in ER-negative breast cancer via epigenetic reactivation of ERα expression. Sci Rep. 2017;7(1):9345. doi:10.1038/s41598-017-09764-3
47. Eddy SF, Kane SE, Sonenshein GE. Trastuzumab-resistant HER2-driven breast cancer cells are sensitive to epigallocatechin-3 gallate. Cancer Res. 2007;67(19):9018–9023. doi:10.1158/0008-5472.CAN-07-1691
48. Zhang Y, Wang X, Han L, Zhou Y, Sun S. Green tea polyphenol EGCG reverse cisplatin resistance of A549/DDP cell line through candidate genes demethylation. Biomed Pharmacother. 2015;69:285–290. doi:10.1016/j.biopha.2014.12.016
49. Li X, Hou Y, Han G, et al. S100A4/NF-κB axis mediates the anticancer effect of epigallocatechin-3-gallate in platinum-resistant ovarian cancer. iScience. 2024;27(2):108885. doi:10.1016/j.isci.2024.108885
50. Kyriacou NM, Gross AS, McLachlan AJ. Green tea catechins as perpetrators of drug pharmacokinetic interactions. Clin Pharmacol Ther. 2025;118(1):45–61. doi:10.1002/cpt.3547
51. Kim T-E, Shin K-H, Park J-E, et al. Effect of green tea catechins on the pharmacokinetics of digoxin in humans. Drug Des Devel Ther. 2018;12:2139–2147. doi:10.2147/DDDT.S148257
52. Lin L-C, Wang M-N, Tsai T-H. Food–drug interaction of (−)-epigallocatechin-3-gallate on the pharmacokinetics of irinotecan and the metabolite SN-38. Chem Biol Interact. 2008;174(3):177–182. doi:10.1016/j.cbi.2008.05.033
53. Zhou Y, Tang J, Du Y, Ding J, Liu J-Y. The green tea polyphenol EGCG potentiates the antiproliferative activity of sunitinib in human cancer cells. Tumour Biol J Int Soc Oncodevelopmental Biol Med. 2016;37(7):8555–8566. doi:10.1007/s13277-015-4719-x
54. Chung J-H, Choi D-H, Choi J-S. Effects of oral epigallocatechin gallate on the oral pharmacokinetics of verapamil in rats. Biopharm Drug Dispos. 2009;30(2):90–93. doi:10.1002/bdd.644
55. Li C, Li C, Choi JS. Effects of epigallocatechin gallate on the bioavailability and pharmacokinetics of diltiazem in rats. Die Pharmazie. 2008;63(11):815–818. doi:10.31083/ph.2008.8645
56. Shin S-C, Choi J-S. Effects of epigallocatechin gallate on the oral bioavailability and pharmacokinetics of tamoxifen and its main metabolite, 4-hydroxytamoxifen, in rats. Anticancer Drugs. 2009;20(7):584–588. doi:10.1097/CAD.0b013e32832d6834
57. Liang G, Tang A, Lin X, et al. Green tea catechins augment the antitumor activity of doxorubicin in an in vivo mouse model for chemoresistant liver cancer. Int J Oncol. 2010;37(1):111–123. doi:10.3892/ijo_00000659
58. Mohamed M-EF, Tseng T, Frye RF. Inhibitory effects of commonly used herbal extracts on UGT1A1 enzyme activity. Xenobiotica. 2010;40(10):663–669. doi:10.3109/00498254.2010.505669
59. Qiao J, Gu C, Shang W, et al. Effect of green tea on pharmacokinetics of 5-fluorouracil in rats and pharmacodynamics in human cell lines in vitro. Food Chem Toxicol. 2011;49(6):1410–1415. doi:10.1016/j.fct.2011.03.033
60. Granja A, Frias I, Neves AR, Pinheiro M, Reis S. Therapeutic potential of epigallocatechin gallate nanodelivery systems. Biomed Res Int. 2017;2017:5813793. doi:10.1155/2017/5813793
61. Zeng W, Lao S, Guo Y, et al. The Influence of EGCG on the pharmacokinetics and pharmacodynamics of bisoprolol and a new method for simultaneous determination of EGCG and bisoprolol in rat plasma Front Nutr. 2022;9(May):1–10. doi:10.3389/fnut.2022.907986
62. Surana AR, Agrawal SP, Kumbhare MR, Gaikwad SB. Current perspectives in herbal and conventional drug interactions based on clinical manifestations. Futur J Pharm Sci. 2021;7(1). doi:10.1186/s43094-021-00256-w
63. Cerbin-Koczorowska M, Waszyk-Nowaczyk M, Bakun P, Goslinski T, Koczorowski T. Current view on green tea catechins formulations, their interactions with selected drugs, and prospective applications for various health conditions. Appl Sci. 2021;11(11):4905. doi:10.3390/app11114905
64. Sharifi-Rad M, Pezzani R, Redaelli M, et al. Preclinical pharmacological activities of epigallocatechin-3-gallate in signaling pathways: an update on cancer. Molecules. 2020;25(3):467. doi:10.3390/molecules25030467
65. Chen J, Liang X, Kong B, et al. Underlying mechanisms and effects of EGCG on the interfacial composition and protein-lipid co-oxidation of whey protein isolate-stabilised O/W emulsions. LWT. 2023;184:115055. doi:10.1016/j.lwt.2023.115055
66. Huynh HD, Thi THT, Thi TXT, et al. Recent insights into protein-polyphenol complexes: molecular mechanisms, processing technologies, synergistic bioactivities, and food applications. Molecules. 2026;31(2):287. doi:10.3390/molecules31020287
67. Dong Y, Chen X, Lv Y, et al. Binding mechanisms of quinone-modified EGCG (QEGCG) with plant proteins: enhanced foaming-emulsifying properties and improved hypoglycemic activity. Food Chem. 2026;512:148914. doi:10.1016/j.foodchem.2026.148914
68. Yang J, Chen W, Chen J, Xie D, Wang Y, Zhou J. Tea polyphenol epigallocatechin gallate and the gut–health axis: unraveling structural characteristics, metabolic pathways, and systemic benefits. Adv Nutr. 2025;16(12):100545. doi:10.1016/j.advnut.2025.100545
69. Andreeva TV, Maluchenko NV, Efremenko AV, et al. Epigallocatechin Gallate affects the structure of chromatosomes, nucleosomes and their complexes with PARP1. Int J Mol Sci. 2023;24(18):14187. doi:10.3390/ijms241814187
70. Ma C, Xu Q, Ding L, et al. Metal–polyphenol network-based multifunctional materials for tumor therapy: intrinsic properties, advances, and applications. Acta Pharm Sin B. 2026;16(3):1421–1448. doi:10.1016/j.apsb.2025.11.038
71. Zhu F, Sun Z, Li Y, Chen C, Cheng Y. Polycatechols: promising materials for biomedical applications. Prog Polym Sci. 2024;155:101857. doi:10.1016/j.progpolymsci.2024.101857
72. Liang K, Chung JE, Gao SJ, Yongvongsoontorn N, Kurisawa M. Highly augmented drug loading and stability of micellar nanocomplexes composed of doxorubicin and poly(Ethylene Glycol)–green tea catechin conjugate for cancer therapy. Adv Mater. 2018;30(14). doi:10.1002/adma.201706963
73. Siew-Keah L, Jie TH, Ang-Lim C, Bin LK, Yik-Ling C. An update on impacts of Epigallocatechin Gallate Co-administration in modulating pharmacokinetics of statins, calcium channel blockers, and beta-blockers. Planta Med. 2023;89(13):1229–1235. doi:10.1055/a-2111-7319
74. Shan L, Gao G, Wang W, et al. Self-assembled green tea polyphenol-based coordination nanomaterials to improve chemotherapy efficacy by inhibition of carbonyl reductase 1. Biomaterials. 2019;210:62–69. doi:10.1016/j.biomaterials.2019.04.032
75. Ren Z, Sun S, Sun R, et al. A metal–polyphenol-coordinated nanomedicine for synergistic cascade cancer chemotherapy and chemodynamic therapy. Adv Mater. 2020;32(6):e1906024. doi:10.1002/adma.201906024
76. Wang R, Huang J, Chen J, et al. Enhanced anti-colon cancer efficacy of 5-fluorouracil by epigallocatechin-3-gallate co-loaded in wheat germ agglutinin-conjugated nanoparticles. Nanomed Nanotechnol Biol Med. 2019;21:102068. doi:10.1016/j.nano.2019.102068
77. Zhou Y, Yu Q, Qin X, et al. Improving the anticancer efficacy of laminin receptor-specific therapeutic ruthenium nanoparticles (RuBB-Loaded EGCG-RuNPs) via ROS-dependent apoptosis in SMMC-7721 cells. ACS Appl Mater Interfaces. 2016;8(24):15000–15012. doi:10.1021/acsami.5b02261
78. Wang X, Li X, Liang X, et al. ROS-responsive capsules engineered from green tea polyphenol–metal networks for anticancer drug delivery. J Mater Chem B. 2018;6(7):1000–1010. doi:10.1039/C7TB02688A
79. Chen S, Fan J-X, Zheng D-W, et al. A multi-functional drug delivery system based on polyphenols for efficient tumor inhibition and metastasis prevention. Biomater Sci. 2020;8(2):702–711. doi:10.1039/C9BM01646E
80. Zhang C, Liu S, Zhang J, et al. A multifunctional Fe-EGCG@RSL3 nanomedicine synergizes ferroptosis induction and tumor microenvironment remodeling for enhanced bladder cancer immunotherapy. Res (Washington, DC). 2025;8:735. doi:10.34133/research.0735
81. Shen W, Wang R, Fan Q, Li, Y, Chen Y. Natural polyphenol assisted delivery of single-strand oligonucleotides by cationic polymers. Gene Ther. 2020;27(7–8):383–391. doi:10.1038/s41434-020-0151-y
82. Ding J, Liang T, Min Q, Jiang L, Zhu J-J. “Stealth and fully-laden” drug carriers: self-assembled nanogels encapsulated with epigallocatechin gallate and siRNA for drug-resistant breast cancer therapy. ACS Appl Mater Interfaces. 2018;10(12):9938–9948. doi:10.1021/acsami.7b19577
83. Shen W, Wang Q, Shen Y, et al. Green tea catechin dramatically promotes RNAi mediated by low-molecular-weight polymers. ACS Cent Sci. 2018;4(10):1326–1333. doi:10.1021/acscentsci.8b00363
84. Gu Y, Chen J, Wang Z, et al. mRNA delivery enabled by metal–organic nanoparticles. Nat Commun. 2024;15(1):9664. doi:10.1038/s41467-024-53969-w
85. Wang C, Sang H, Wang Y, et al. Foe to friend: supramolecular nanomedicines consisting of natural polyphenols and bortezomib. Nano Lett. 2018;18(11):7045–7051. doi:10.1021/acs.nanolett.8b03015
86. Cheng T, Liu J, Ren J, et al. Green tea catechin-based complex micelles combined with doxorubicin to overcome cardiotoxicity and multidrug resistance. Theranostics. 2016;6(9):1277–1292. doi:10.7150/thno.15133
87. Liu C, Shen W, Li B, Li T, Chang H, Cheng Y. Natural polyphenols augment cytosolic protein delivery by a functional polymer. Chem Mater. 2019;31(6):1956–1965. doi:10.1021/acs.chemmater.8b04672
88. Sun X, Zhang J, Xiu J, et al. A phenolic based tumor-permeated nano-framework for immunogenic cell death induction combined with PD-L1 immune checkpoint blockade. Biomater Sci. 2022;10(14):3808–3822. doi:10.1039/d2bm00455k
89. Chung JE, Tan S, Gao SJ, et al. Self-assembled micellar nanocomplexes comprising green tea catechin derivatives and protein drugs for cancer therapy. Nat Nanotechnol. 2014;9(11):907–912. doi:10.1038/nnano.2014.208
90. Liang K, Bae KH, Lee F, et al. Self-assembled ternary complexes stabilized with hyaluronic acid-green tea catechin conjugates for targeted gene delivery. J Control Release. 2016:226. doi:10.1016/j.jconrel.2016.02.004
91. Liang K, Ng S, Lee F, et al. Targeted intracellular protein delivery based on hyaluronic acid-green tea catechin nanogels. Acta Biomater. 2016;33:142–152. doi:10.1016/j.actbio.2016.01.011
92. Bae KH, Tan S, Yamashita A, et al. Hyaluronic acid-green tea catechin micellar nanocomplexes: fail-safe cisplatin nanomedicine for the treatment of ovarian cancer without off-target toxicity. Biomaterials. 2017:148. doi:10.1016/j.biomaterials.2017.09.027
93. Yongvongsoontorn N, Chung JE, Gao SJ, et al. Carrier-enhanced anticancer efficacy of sunitinib-loaded green tea-based micellar nanocomplex beyond tumor-targeted delivery. ACS Nano. 2019;13(7):7591–7602. doi:10.1021/acsnano.9b00467
94. Bae KH, Lai F, Mong J, et al. Bone marrow-targetable green tea catechin-based micellar nanocomplex for synergistic therapy of acute myeloid leukemia. J Nanobiotechnol. 2022;20(1):481. doi:10.1186/s12951-022-01683-4
95. Bae KH, Lai F, Oruc B, Osato M, Chen Q, Kurisawa M. Self-assembled daunorubicin/epigallocatechin gallate nanocomplex for synergistic reversal of chemoresistance in leukemia. Int J Mol Sci. 2022;24(1):381. doi:10.3390/ijms24010381
96. Bae KH, Lai F, Chen Q, Kurisawa M. Potentiating gilteritinib efficacy using nanocomplexation with a hyaluronic acid–Epigallocatechin Gallate conjugate. Polymers. 2024;16(2):225. doi:10.3390/polym16020225
97. Mehrotra S, Kalyan Bg P, Nayak PG, Joseph A, Manikkath J. Recent progress in the oral delivery of therapeutic peptides and proteins: overview of pharmaceutical strategies to overcome absorption hurdles. Adv Pharm Bull. 2024;14(1):11–33. doi:10.34172/apb.2024.009
98. Cao S-J, Lv Z-Q, Guo S, Jiang G-P, Liu H-L. An update - Prolonging the action of protein and peptide drugs. J Drug Deliv Sci Technol. 2021;61:102124. doi:10.1016/j.jddst.2020.102124
99. Liu M, Svirskis D, Proft T, et al. Progress in peptide and protein therapeutics: challenges and strategies. Acta Pharm Sin B. 2025;15(12):6342–6381. doi:10.1016/j.apsb.2025.10.026
100. Wang D, Wang T, Yu H, et al. Engineering nanoparticles to locally activate T cells in the tumor microenvironment. Sci Immunol. 2019;4(37). doi:10.1126/sciimmunol.aau6584
101. Sun M, Wu Y, Zhou Z, Liu S, Mao S, Li G. Co-delivery of EGCG and melittin with self-assembled fluoro-nanoparticles for enhanced cancer therapy. Aging. 2023;15(11):4875–4888. doi:10.18632/aging.204769
102. Rady I, Siddiqui IA, Rady M, Mukhtar H. Melittin, a major peptide component of bee venom, and its conjugates in cancer therapy. Cancer Lett. 2017;402:16–31. doi:10.1016/j.canlet.2017.05.010
103. Chuan D, Mu M, Hou H, et al. Folic acid-functionalized tea polyphenol as a tumor-targeting nano-drug delivery system. Mater Des. 2021;206:109805. doi:10.1016/J.MATDES.2021.109805
104. Liu C, Wu H, Duan H, et al. An EGCG-mediated self-assembled micellar complex acts as a bioactive drug carrier. Food Chem. 2023;418:135939. doi:10.1016/j.foodchem.2023.135939
105. Chen X, Yi Z, Chen G, et al. Carrier-enhanced photodynamic cancer therapy of self-assembled green tea polyphenol-based nanoformulations. ACS Sustain Chem Eng. 2020;8(43):16372–16384. doi:10.1021/acssuschemeng.0c06645
106. Mu M, Chen H, Fan R et al. A tumor-specific ferric-coordinated Epigallocatechin-3-gallate cascade nanoreactor for glioblastoma therapy. J Adv Res. 2021;34: 29–41. doi:10.1016/j.jare.2021.07.010
107. d’Avanzo N, Celia C, Barone A, et al. Immunogenicity of polyethylene glycol based nanomedicines: mechanisms, clinical implications and systematic approach. Adv Ther. 2020;3(3):1900170. doi:10.1002/adtp.201900170
108. Chrostek L, Cylwik B. Hyaluronic acid in immune response. Biomolecules. 2025;15(7):29–41. doi:10.3390/biom15071008
109. Buckley C, Murphy EJ, Montgomery TR, Major I. Hyaluronic acid: a review of the drug delivery capabilities of this naturally occurring polysaccharide. Polymers. 2022;14(17):3442. doi:10.3390/polym14173442
110. Yi Z, Sun Z, Chen G, et al. Size-controlled, colloidally stable and functional nanoparticles based on the molecular assembly of green tea polyphenols and keratins for cancer therapy. J Mater Chem B. 2018;6(9):1373–1386. doi:10.1039/C7TB03293E
111. Li W, Yalcin M, Lin Q, Ardawi M-SM, Mousa SA. Self-assembly of green tea catechin derivatives in nanoparticles for oral lycopene delivery. J Control Release. 2017;248:117–124. doi:10.1016/j.jconrel.2017.01.009
112. Cai X, Dou R, Guo C, et al. Cationic polymers as transfection reagents for nucleic acid delivery. Pharmaceutics. 2023;15(5):1502. doi:10.3390/pharmaceutics15051502
113. Wu P, Zhang H, Yin Y, et al. Engineered EGCG-containing biomimetic nanoassemblies as effective delivery platform for enhanced cancer therapy. Adv Sci. 2022;9(15):e2105894. doi:10.1002/advs.202105894
114. Liu LH, Zhang XZ. Carrier-free nanomedicines for cancer treatment. Prog Mater Sci. 2022;125:100919. doi:10.1016/j.pmatsci.2021.100919
115. Dong X, Liu H, Liu H, Zhang X, Deng X. Carrier-free nanomedicines: mechanisms of formation and biomedical applications. Giant. 2024;18:100256. doi:10.1016/j.giant.2024.100256
116. Zhang G, Zhang J. Enhanced oral bioavailability of EGCG using pH-sensitive polymeric nanoparticles: characterization and in vivo investigation on nephrotic syndrome rats. Drug Des Devel Ther. 2018;12:2509–2518. doi:10.2147/DDDT.S172919
117. Pal J, Sharma M, Tiwari A, et al. Oxidative coupling and self-assembly of polyphenols for the development of novel biomaterials. ACS omega. 2024;9(18):19741–19755. doi:10.1021/acsomega.3c08528
118. Krupkova O, Ferguson SJ, Wuertz-Kozak K. Stability of (−)-epigallocatechin gallate and its activity in liquid formulations and delivery systems. J Nutr Biochem. 2016;37:1–12. doi:10.1016/j.jnutbio.2016.01.002
119. Bae KH, Chan KH, Kurisawa M. Autoxidation-resistant, ROS-scavenging, and anti-inflammatory micellar nanoparticles self-assembled from poly(acrylic acid)–green tea catechin conjugates. ACS Macro Lett. 2022;11(7):835–840. doi:10.1021/acsmacrolett.2c00239
120. Desai N, Finosh GT, Panicker NG, Ramachandran R, Varghese A. Cytotoxic Effects of Curcumin At Various Concentrations and Role of Curcumin on Lipid Peroxidation and Activities of Antioxidant Enzymes of the Rat Peripheral Blood Lymphocytes. Blood. 2011;118(21):4933. doi:10.1182/blood.V118.21.4933.4933
121. Menon D, Chakraborty S. How safe are nanoscale metal-organic frameworks? Front Toxicol. 2023;5:1233854. doi:10.3389/ftox.2023.1233854
122. Huang H, Feng W, Chen Y, Shi J. Inorganic nanoparticles in clinical trials and translations. Nano Today. 2020;35:100972. doi:10.1016/j.nantod.2020.100972
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Update on Novel Ocular Nanosystems with Possible Benefits in the Treatment of Corneal Neovascularization

Zhang C, Yin Y, Zhao J, Li Y, Wang Y, Zhang Z, Niu L, Zheng Y
International Journal of Nanomedicine 2022, 17:4911-4931
Published Date: 19 October 2022
Targeting Multiple Pathophysiological Axes in COPD: Nanomaterial Advances
Zhang Q, Xu S, Yang C, Wang X, Liu T, Zhang X, Qu C, Wu J, Yang J, Xing X
International Journal of Nanomedicine 2025, 20:11989-12007
Published Date: 1 October 2025
Nanotechnology-Driven Cancer Therapies for Precision Oncology: Advances and Clinical Outlook
Gupta V, Kumar D, Gupta S, Tanwar R, Jaiswal NK, Islam MM, Singh S, Choudhary N, Gowri S, Webster TJ, Faiyazuddin M
International Journal of Nanomedicine 2026, 21:568254
Published Date: 23 January 2026
Recent Advances in Novel Drug Delivery Systems for the Management of Cutaneous Squamous Cell Carcinoma
Fu X, Zhang Z, Dong Q, Li S, Wang X, Zhang H, Bai J, Han H, Shi L, Zheng K, Liang L
International Journal of Nanomedicine 2026, 21:592605
Published Date: 29 April 2026
Nanocarrier-Mediated Delivery Systems of Phytochemicals to Enhance and Accelerate Diabetic Wound Healing Processes
Wahyuningsih ES, Muhaimin M, Chaerunisaa AY, Khairinisa MA
Drug Design, Development and Therapy 2026, 20:607020
Published Date: 18 June 2026