Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Efficiency of the Guide Extension Catheter-Facilitated Tip-in Technique in the Recanalization of Coronary Chronic Total Occlusion
Authors Zhou Y ![]() , Deng L, Wang Z, Hu Y, Chen Z, Lu H, Qian J, Ge J
, Deng L, Wang Z, Hu Y, Chen Z, Lu H, Qian J, Ge J
Received 12 June 2023
Accepted for publication 17 August 2023
Published 25 August 2023 Volume 2023:16 Pages 2463—2470
DOI https://doi.org/10.2147/JMDH.S425489
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
You Zhou,* Lixiang Deng,* Zhe Wang,* Yiqing Hu, Zhangwei Chen, Hao Lu, Juying Qian, Junbo Ge
Department of Cardiology, Shanghai Institute of Cardiovascular Diseases, Zhongshan Hospital, Fudan University; National Clinical Research Center for Interventional Medicine; Shanghai Clinical Research Center for Interventional Medicine, Shanghai, 200032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hao Lu, Department of Cardiology, Shanghai Institute of Cardiovascular Diseases, Zhongshan Hospital, Fudan University; National Clinical Research Center for Interventional Medicine; Shanghai Clinical Research Center for Interventional Medicine, 180 Fenglin Road, Shanghai, 200032, People’s Republic of China, Tel +86-21-64041990, Email [email protected] Juying Qian, Department of Cardiology, Shanghai Institute of Cardiovascular Diseases, Zhongshan Hospital, Fudan University; National Clinical Research Center for Interventional Medicine; Shanghai Clinical Research Center for Interventional Medicine, 1609 Xietu Road, Shanghai, 200032, People’s Republic of China, Tel +86-21-64041990 ext 2728, Email [email protected]
Background: The tip-in technique, which involves advancing an antegrade microcatheter cross the lesion over a retrograde guidewire, is an elaborated maneuver in the recanalization of coronary chronic total occlusion (CTO). We seek to assess the efficiency of a guide extension catheter-facilitated tip-in technique in comparison to the traditional retrograde approach, which is accomplished by an externalization wire.
Methods: Thirty-three CTO patients successfully revascularized using guide extension catheter-facilitated “tip-in” were included and matched with another 33 patients by J-CTO score and operators, whose CTO was recanalized using an externalized wire. The manipulation time from the first retrograde wire entering the antegrade guide to the first antegrade balloon inflation in the occlusion was calculated.
Results: Compared with the wire-externalization group, the manipulation time in the tip-in group was significantly shortened [389s; interquartile range (IQR), 272– 478 vs 706s; IQR, 560– 914; p < 0.001]. There was a trend in decreasing total operation time and radiation dose, but it did not reach statistical significance.
Conclusion: Guide extension catheter-facilitated tip-in is an efficient method to achieve the recanalization of CTO in a retrograde way, which would be pivotal when the retrograde microcatheter could not be advanced into the antegrade guide catheter.
Keywords: chronic total occlusion, extension guide catheter, tip-in, retrograde
Introduction
With the innovation of equipment and techniques, the success rate of recanalization of coronary chronic total occlusion (CTO) via percutaneous coronary intervention (PCI) has been improved dramatically over the years.1 The retrograde approach played an indispensable role in crossing the occlusion, which could be accomplished by wire externalization, tip-in and rendezvous.2,3 Both wire externalization and rendezvous require retrograde crossing of a microcatheter, which could be impossible in tortuous and severely calcified lesions. Under such circumstances, tip-in would be the most suitable way to accomplish the procedure.
The tip-in technique involves inserting a retrograde wire into an antegrade microcatheter, most commonly in the distal curve of the antegrade guide catheter.4 Tip-in could avoid retrograde advancement of microcatheters cross the lesion and hold unique values in CTO PCI. However, we noticed that the maneuver to intubate the retrograde wire could be challenging in some cases, such as non-coaxial alignment of the guide catheter and coronary ostium. Hence, we adopted a guide extension catheter-facilitated tip-in technique, in which the antegrade extension catheter was added and could be used for three purposes: (1) “pick up” the retrograde wire within the coronary artery to assist the entry into the guide catheter; (2) Narrowing the lumen to facilitate the convergence of the retrograde wire and antegrade microcatheter; (3) Increase coaxial alignment and antegrade support if necessary.
We enrolled 33 CTO patients successfully revascularized by guide extension catheter-facilitated tip-in, who were matched 1:1 with another 33 CTO patients treated by wire externalization during the same period. This study aimed to assess the efficiency of this guide extension catheter-facilitated tip-in technique and assist in its application in clinical practice.
Methods
Population and Data Collection
Between March 2021 and October 2022, 33 consecutive patients with CTO lesions successfully recanalized using guide extension catheter-facilitated tip-in were included in Zhongshan hospital, Fudan University. Another 33 CTO patients, who were treated by externalized wire during the same time interval, were 1:1 matched by J-CTO score and operators. Of note, none of the patients in the externalization group have tip-in attempted. Demographic and procedural data were prospectively collected through electronic medical record system and analyzed retrospectively. This study was approved by the Ethics Committee of Zhongshan Hospital, Fudan University (No.: B2021-726R) and conducted in accordance with the guidelines of the Declaration of Helsinki. All participants were given written informed consent at the time of index hospitalization.
Study Definitions
CTO was defined as 100% occlusion with Thrombolysis in Myocardial Infarction (TIMI) 0 flow for a presumed or documented duration of ≥3 months.5 Occlusion duration was determined based on prior angiogram, the onset of ischemic symptoms, prior history of myocardial infarction, or typical angiographic features (such as no thrombus, no staining at the proximal cap, and presence of mature collaterals).
Angiographic assessment of a collateral connection (CC) was based on Werner’s classification: CC0, no continuous connection between the donor and recipient artery; CC1, thread-like continuous connection (<0.4 mm); and CC2, continuous branch-like connection (≥0.4 mm).5 The perfusion of the occluded artery segment was assessed using the Rentrop classification: 0, none; 1, filling of side branches of the occluded artery without visualization of the epicardial segment; 2, partial filling of the epicardial segment via collateral channels; 3, complete filling of the epicardial segment of the artery.6
The J-CTO (Multicenter CTO Registry in Japan) score was calculated by assigning 1 point to each of the following factors: blunt proximal cap, presence of calcification, bend >45°, occlusion length ≥20 mm, and previously failed attempt.7
Tip-in is achieved by intubating the retrograde wire with an antegrade microcatheter, usually in the distal curve of the antegrade guide catheter. In this study, this technique was adapted by adding an antegrade extension catheter, which was used to facilitate the retrograde wire to enter the antegrade guide catheter as well as the microcatheter (Figure 1). Wire externalization used a dedicated externalization wire (RG3, Asahi Intecc), which entered the retrograde microcatheter and ran through the occlusion into the antegrade guide catheter to allow the conversion to an antegrade approach.
 |
Figure 1 Depiction of guide extension catheter-facilitated tip-in technique. (A) The guide extension catheter could advance into the coronary artery to “pick up” the retrograde wire. (B) The guide extension catheter narrowed the lumen which facilitated the entry of retrograde wire into the antegrade microcatheter. |
Statistical Analysis
The continuous and categorical variables were summarized as median (interquartile range [IQR]) and n (%), respectively. Comparison between categorical groups was conducted by χ²-test or Fisher’s exact test, as applicable. Student’s t-test and the Mann–Whitney U-test were used to assess differences between groups in normally and nonnormally distributed continuous variables, respectively. A two-sided p value of less than 0.05 was considered statistically significant. Analysis was performed with SPSS for Windows, release 25.0 (IBM SPSS, Inc., Chicago, IL, USA).
Results
Baseline characteristics are summarized in Table 1. The median age of the population was 56 years old [interquartile range (IQR), 47–66]. About 90.9% of the patients were male. Forty-six patients (69.7%) had hypertension and 23 (34.8%) had diabetes. Eighteen patients had previously failed attempts to recanalize the target CTO. There was no significant difference in clinical features between the tip-in and wire externalization group (Table 1).
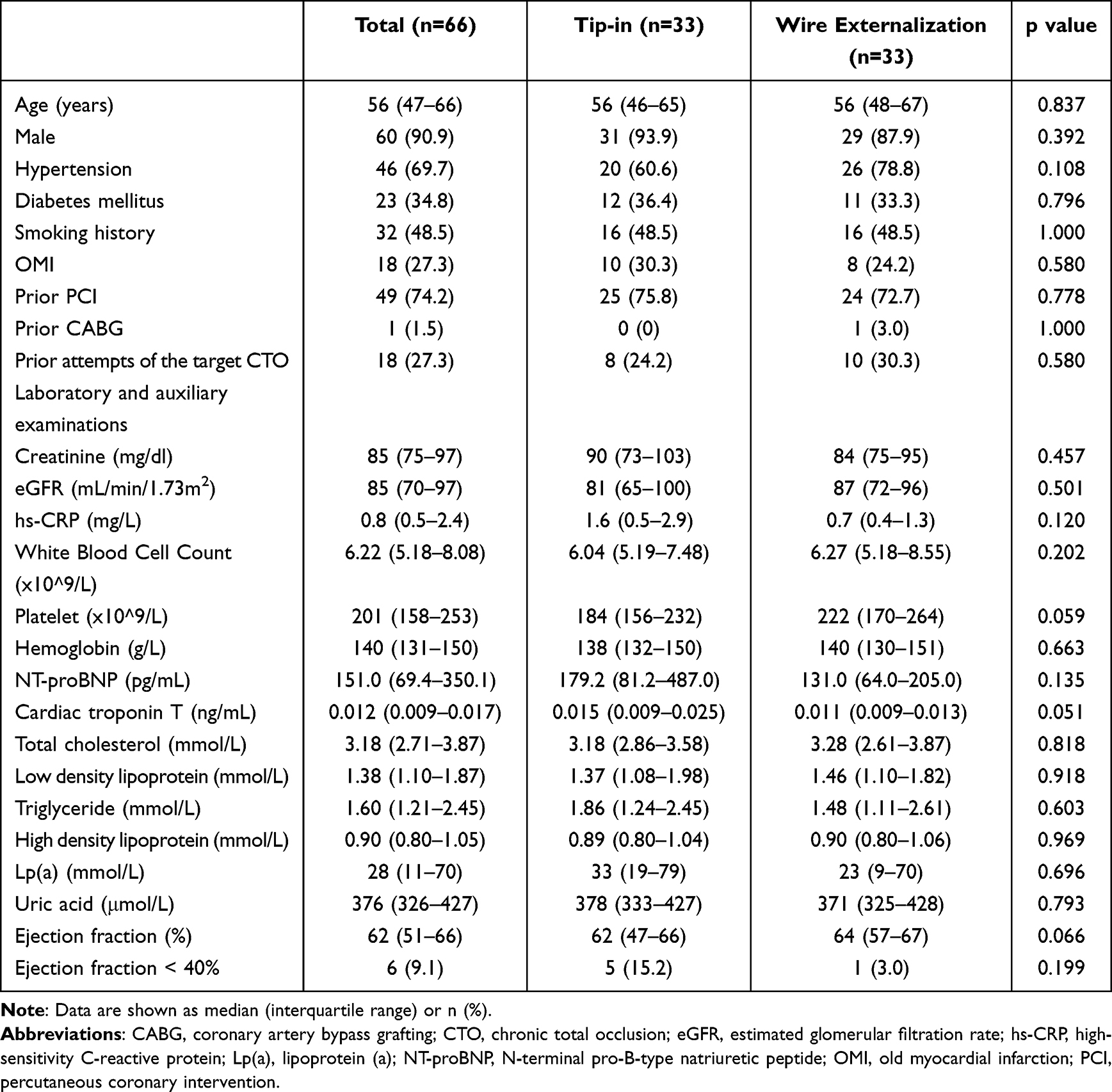 |
Table 1 Demographic and Clinical Characteristics |
Procedural details are displayed in Table 2. There was no significant difference in Syntax score, J-CTO score and the condition of collateral vessels (Rentrop classification and Werner’s classification), which we believed could infer that the complexity of the procedure was comparable between two groups. The targeted vessel with total occlusion was similar between the tip-in group and the wire externalization group. The operators most often chose the septal artery as the retrograde route (86.4%). Of note, most operators used Instantpass (APT) as the antegrade microcatheter in the tip-in group. It was probably due to the fact that the relatively larger size of the tip (1.9F) of this microcatheter would be easier to intubate the retrograde guidewire. Besides, the top two wires used to enter the antegrade microcatheter were Ultimate Bro 3 (Asahi) and Gaia 3rd (Asahi) (76.8% and 6.1%, respectively. Data not shown).
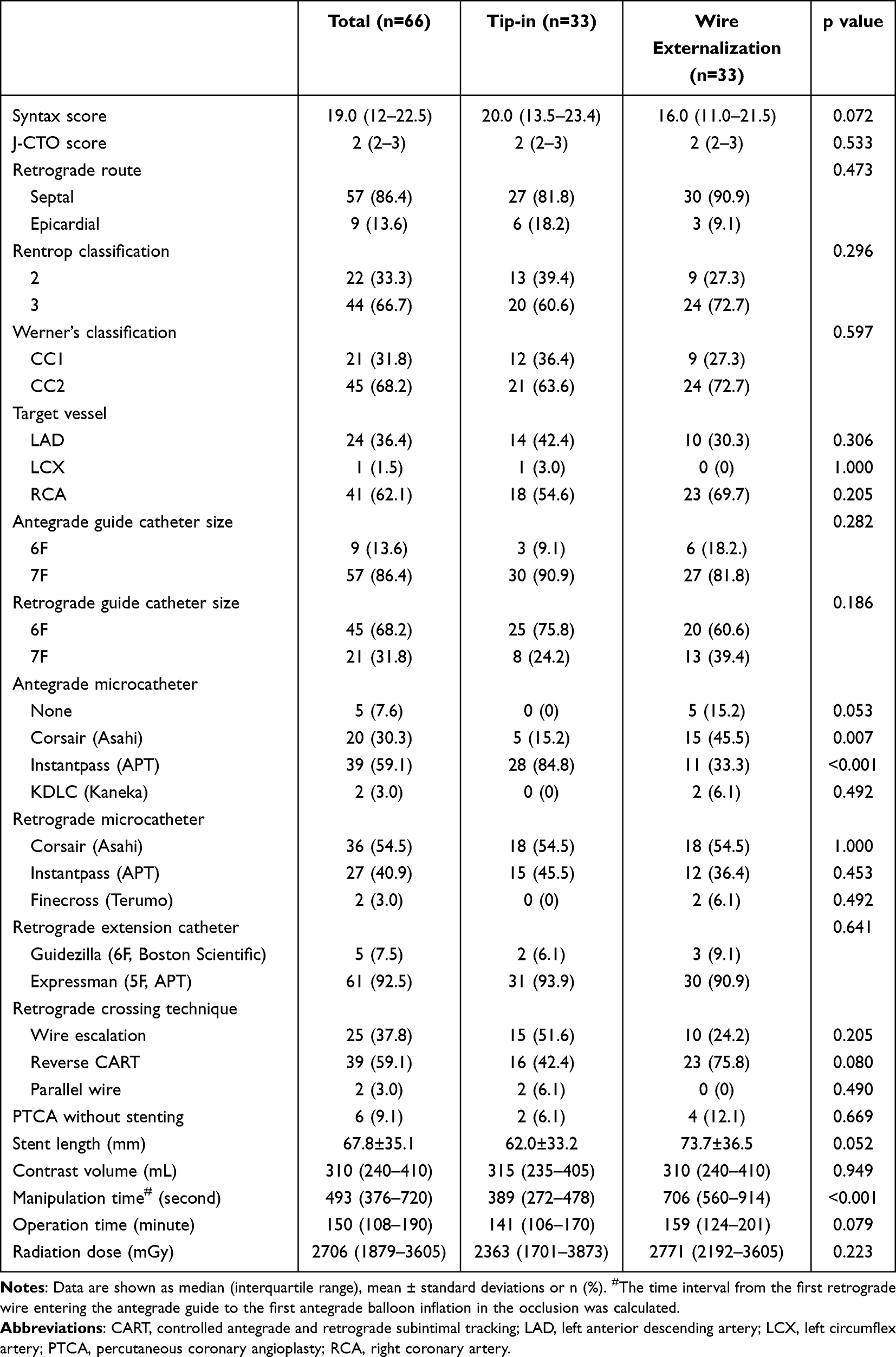 |
Table 2 Lesion and Procedural Features |
Compared with wire externalization, tip-in saved the time to advance the retrograde microcatheter and convert to a dedicated externalization wire. The critical step of tip-in was the convergence of the antegrade microcatheter and the retrograde wire, which could be time-consuming in some cases, for example, when large antegrade guide catheter (≥7F) was used. The antegrade extension catheter with narrowed lumen (mostly 5/6F) was used to further fasten this process (Figure 1). In order to assess the efficiency of guide extension catheter-facilitated tip-in technique, we calculated the manipulation time from the retrograde wire first entering the antegrade guide catheter to the first inflation of an antegrade balloon in the occlusion. The manipulation time was significantly shortened in the tip-in group (389s; IQR, 272–478 vs 706s; IQR, 560–914; p < 0.001). Besides, we noticed the trend in shorter total operation time (141min; IQR, 106–170 vs 159min; IQR 124–201; p = 0.079) and less radiation exposure (2363mGy; IQR 1701–3873 vs 2771mGy; IQR, 2192–3605; p = 0.307) in the tip-in group, which had not reached statistical significance yet.
Discussion
In this study, we evaluated the efficiency of guide extension catheter-facilitated tip-in technique. Compared with the conventional wire externalization method, the modified tip-in could significantly decrease the time to convert to an antegrade approach after retrograde wire entering the antegrade guide catheter.
With the constant improvement of techniques and equipment, CTO PCI could be currently achieved with a high success rate of 80–90%.8,9 The frequency of use of the retrograde approach was 30–40%, which would be even higher in complex CTO.9,10 In order to convert to an antegrade approach after retrograde lesion crossing, several candidate strategies can be considered contemporarily, such as wire externalization, rendezvous, tip-in and antegrade microcatheter probing.11
Among these techniques, a retrograde crossing of the microcatheter was mandatory except tip-in. A dedicated wire >300cm was also required in wire externalization. However, advancing a retrograde microcatheter into the intended location may not always be possible, especially when the lesion was calcified, torturous or within a stent.12 Besides, the microcatheter could impair the blood flow from collateral channels and the perfusion of the occluded territory. Long time deposition of the microcatheter in the collaterals may be intolerable for patients with profound heart failure. In such cases, tip-in would be the most appropriate strategy to accomplish the revascularization. Compared with other techniques, tip-in could maximally reduce the manipulation of the retrograde microcatheter.
The key step of tip-in was to advance the retrograde wire into the antegrade microcatheter, which could be occasionally time-consuming. Firstly, inserting the wire into the antegrade guide catheter could be challenging if the guide could not coaxially engage with the coronary ostium or the proximal segment of the artery was tortuous. Second, operators tended to use larger antegrade guiding catheters to increase the support and facilitate equipment delivery. As shown in Table, 7F antegrade guide catheters were most often used in our study. Meanwhile, in other reports, 8F catheters maybe the primary choice.13 This increased the difficulty to insert the wire into the microcatheter. Therefore, we adapted the traditional tip-in technique by adding an antegrade extension catheter. The extension catheter could improve the efficiency of tip-in from three aspects. (1) It could be advanced into the coronary artery to pick up the retrograde wire, which we called “active greeting technique” (AGT). (2) The extension catheter reduced the lumen to 5/6F, which facilitated the convergence of the wire and microcatheter. As mentioned above, the extension catheter-facilitated tip-in significantly decreased the manipulation time after the retrograde wire entered the antegrade guide catheter. (3) The extension catheter could also increase the antegrade support to assist in microcatheter advancement and equipment delivery if needed.
Even though 33 patients in the tip-in group were all successfully recanalized, there were 3 patients excluded in whom tip-in failed during the recruitment phase of this study. In order to increase the success rate of extension catheter-facilitated tip-in, certain tips are as follows. First, adequately dilate and modify of the lesion if reverse controlled antegrade and retrograde subintimal tracking (CART) is used. A balloon over 2.0mm in diameter is recommended if possible. Second, if resistant CTO is anticipated, choose a coiled type of microcatheter with tapered tip. Third, insert the retrograde wire into the antegrade microcatheter as far as possible or insert the back end of an extra-guidewire into the antegrade MC, as introduced by Giuseppe Venuti etc.14
In this study, the overall procedural time and radiation dose showed a trend to decrease in the tip-in group but it had not reached statistical significance yet. Even though the wire externalization process costs more time, externalized wire provides substantial support that may facilitate and expedite other parts of the procedure. With our experience, the manipulation time to convert to an antegrade approach after retrograde wire engagement could be further reduced if full preparation was made and proper equipment chosen (as we mentioned above). Moreover, in some cases, extra non-CTO lesions were treated in the meantime, so it was not feasible to concisely define the time spent on CTO. This could influence the final results concerning the total operation time and radiation dose. In addition, even the use of an externalization wire still, we believe guide extension catheter-facilitated tip-in is an efficient and promising retrograde approach to revascularize CTO in experienced hands.
This study had several limitations. This was a single-centered retrospective study. Although patients in the two groups were 1:1 matched and showed no significant difference in baseline characteristics, there may be bias due to unrealized factors. Besides, the strategies of PCI were chosen at the discretion of the operators and there was no universally standardized protocol. Third, the sample size was relatively small and as mentioned above, non-CTO lesions may be treated in the same operation. Fourth, the effect of failed tip-in technique on the manipulation or procedural time was not assessed due to limited cases. These limitations will be taken into account in our further clinical researches and prospective studies.
Conclusion
The guide extension catheter-facilitated tip-in is an efficient technique in retrograde CTO PCI with unique advantages. Further multicenter prospective randomized trials are needed to confirm our findings.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approvement
This study was approved by the Ethics Committee of Zhongshan Hospital, Fudan University (No.: B2021-726R) and conducted in accordance with the guidelines of the Declaration of Helsinki. All participants provided written informed consent at the time of index hospitalization.
Author Contributions
Hao Lu and Juying Qian are corresponding authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
There are no conflicts of interest pertaining to this submission.
References
1. Brilakis ES, Mashayekhi K, Tsuchikane E, et al. Guiding principles for chronic total occlusion percutaneous coronary intervention. Circulation. 2019;140(5):420–433. doi:10.1161/CIRCULATIONAHA.119.039797
2. Leibundgut G, Quagliana A, Riede F, et al. Simple techniques for antegrade guiding catheter engagement after retrograde CTO crossing. J Interv Cardiol. 2020;2020:7432831. doi:10.1155/2020/7432831
3. Megaly M, Ali A, Saad M, et al. Outcomes with retrograde versus antegrade chronic total occlusion revascularization. Catheter Cardiovasc Interv. 2020;96(5):1037–1043. doi:10.1002/ccd.28616
4. Vo MN, Ravandi A, Brilakis ES. ”Tip-in” technique for retrograde chronic total occlusion revascularization. J Invasive Cardiol. 2015;27(5):E62–E64.
5. Ybarra LF, Rinfret S, Brilakis ES, et al. Definitions and clinical trial design principles for coronary artery chronic total occlusion therapies: CTO-ARC consensus recommendations. Circulation. 2021;143(5):479–500. doi:10.1161/CIRCULATIONAHA.120.046754
6. Rentrop KP, Cohen M, Blanke H, et al. Changes in collateral channel filling immediately after controlled coronary artery occlusion by an angioplasty balloon in human subjects. J Am Coll Cardiol. 1985;5(3):587–592. doi:10.1016/S0735-1097(85)80380-6
7. Morino Y, Abe M, Morimoto T, et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. 2011;4(2):213–221. doi:10.1016/j.jcin.2010.09.024
8. Tajti P, Karmpaliotis D, Alaswad K, et al. The hybrid approach to chronic total occlusion percutaneous coronary intervention: update from the PROGRESS CTO registry. JACC Cardiovasc Interv. 2018;11(14):1325–1335. doi:10.1016/j.jcin.2018.02.036
9. Wu EB, Tsuchikane E, Ge L, et al. Retrograde versus antegrade approach for coronary chronic total occlusion in an algorithm-driven contemporary Asia-Pacific Multicentre Registry: comparison of outcomes. Heart Lung Circ. 2020;29(6):894–903. doi:10.1016/j.hlc.2019.05.188
10. Patel VG, Brayton KM, Tamayo A, et al. Angiographic success and procedural complications in patients undergoing percutaneous coronary chronic total occlusion interventions: a weighted meta-analysis of 18,061 patients from 65 studies. JACC Cardiovasc Interv. 2013;6(2):128–136. doi:10.1016/j.jcin.2012.10.011
11. Christ G, Glogar D. Successful recanalization of a chronic occluded left anterior descending coronary artery with a modification of the retrograde proximal true lumen puncture technique: the antegrade microcatheter probing technique. Catheter Cardiovasc Interv. 2009;73(2):272–275. doi:10.1002/ccd.21755
12. Suzuki Y, Muto M, Yamane M, et al. Independent predictors of retrograde failure in CTO-PCI after successful collateral channel crossing. Catheter Cardiovasc Interv. 2017;90(1):E11–E18. doi:10.1002/ccd.26785
13. Fairley SL, Lucking AJ, Mcentegart M, et al. Routine use of fluoroscopic-guided femoral arterial puncture to minimise vascular complication rates in CTO intervention: multi-centre UK experience. Heart Lung Circ. 2016;25(12):1203–1209. doi:10.1016/j.hlc.2016.04.006
14. Venuti G, D’Agosta G, Tamburino C, et al. When antegrade microcatheter does not follow: the “facilitated tip-in technique”. Catheter Cardiovasc Interv. 2020;96(4):E458–E461. doi:10.1002/ccd.28803
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Transradial and Transfemoral Access for Retrograde Chronic Total Occlusion Percutaneous Coronary Interventions: A Comparison of the Clinical Features and Prognostic Implications
Wu X, Li Q, Wu M, Huang H, Liu Z, Huang H, Wang L
International Journal of General Medicine 2024, 17:3689-3698
Published Date: 26 August 2024