Back to Journals » Journal of Pain Research » Volume 19
Efficacy Of Transforaminal Epidural Steroid Injections in Lumbar Radicular Pain
Authors Bilir EE ![]() , Ata AM, Özlemiş B
, Ata AM, Özlemiş B ![]() , Adıgüzel E
, Adıgüzel E
Received 23 April 2026
Accepted for publication 24 June 2026
Published 30 June 2026 Volume 2026:19 618013
DOI https://doi.org/10.2147/JPR.S618013
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Emine Esra Bilir,1 Ayşe Merve Ata,1 Bilge Özlemiş,2 Emre Adıgüzel2
1Physical Therapy and Rehabilitation Department, Ankara City Hospital, Physical Therapy and Rehabilitation Hospital, Ankara, Turkey; 2Physical Therapy and Rehabilitation Department, University of Health and Science Gülhane Faculty of Medicine, Ankara, Turkey
Correspondence: Emine Esra Bilir, Email [email protected]
Background: We aimed to investigate the efficacy of lumbar transforaminal epidural steroid injection therapy in patients with radicular low back pain that had not been alleviated by conservative management strategies.
Methods: This study included 252 patients with radiculopathy due to lumbar disc herniation who failed conservative treatment. This is a retrospective cohort study. Participants (aged 18– 90) underwent C-arm fluoroscopy-guided transforaminal epidural steroid injections (TFESI) using a subpedicular approach. Pain severity and functional status were evaluated at baseline, 2 weeks, and 3 months post-procedure using the Visual Analog Scale (VAS) and the Oswestry Disability Index (ODI). Statistical analysis focused on sociodemographic characteristics and longitudinal changes in VAS and ODI scores.
Results: Out of 252 patients, 221 completed the full 3-month follow-up (mean age 54.5 ± 14.1 years; 57.5% female). The median symptom duration was 5 months, and the most frequent injection levels were L4-5 (51.1%) and L5-S1 (48.4%). Significant improvements were observed in both pain (VAS) and functional status (ODI) at the 2-week and 3-month months (p < 0.001). At the 3-month follow-up, treatment success (defined as > 50%improvement) was achieved in 64.3% of patients for pain at rest, 57.5% for pain during movement, and 74.2% for nocturnal pain. Additionally, 55.7% of patients demonstrated a significant reduction in disability according to ODI scores.
Conclusion: TFESI is an effective non-operative treatment intervention that provides significant mid-term pain reduction and functional improvement in a substantial proportion of patients with lumbar radiculopathy. The low rate of surgical conversion suggests its value as a key alternative to surgery.
Clinical Trials Number: NCT07538765.
Keywords: lumbar radicular pain, transforaminal epidural steroid injection, interventional pain management
A Letter to the Editor has been published for this article.
A Response to Letter by Miss Zhang has been published for this article.
Introduction
Low back pain (LBP) is a common condition in the general population and represents a major cause of workforce loss. Its lifetime prevalence reaches up to 80%, and the annual hospital admission rate among adults is reported to be around 15%.1,2 Among those suffering from chronic LBP, approximately 40% of cases are believed to be related to the intervertebral discs, often described as discogenic pain.3,4 Lumbar disc herniation is characterized by herniation of the nucleus pulposus, typically presenting with progressive LBP followed by the sudden onset of hip and leg pain. Compression of the nerve root can trigger intense inflammatory responses, leading to significant radicular pain.5 Although conservative management yields positive outcomes for most individuals, a fraction of patients suffer from chronic pain and restricted mobility, necessitating interventional alternatives.6
The administration of a steroid injection creates a neural block that interrupts or changes the way the nervous system processes pain. This includes altering the nociceptive input, disrupting the afferent fiber reflex mechanism, silencing the self-sustaining neuronal activity, and modifying central neuronal patterns.7 Fluoroscopically guided epidural corticosteroid injections (ESIs) have been served as a non-surgical therapeutic modality in controlling of spinal and radicular pain attributed to intervertebral disc pathology in recent years.8 ESIs can be performed with three different methods: transforaminal, interlaminar or caudal. Transforaminal epidural steroid injection (TFESI) is a safe, minimally invasive, and target-specific intervention commonly used to treat radicular pain. This technique delivers corticosteroids directly into the epidural space adjacent to the affected nerve root. Administering the ESI via the transforaminal route allows a larger concentration of the corticosteroid to be delivered closer to the source of pain in the ventral epidural space.9
Various systematic reviews and randomized trials have proven the efficacy of TFESI for chronic radicular back pain.10–12
The present study was aimed to investigate the efficacy of lumbar TFESI therapy in patients whose lumbar pain and radicular symptoms had not been alleviated by conservative management strategies.
Materials and Methods
The study represents a retrospective analysis of a prospectively maintained clinical data at a physical therapy and rehabilitation outpatient clinic. Study population were all patients who had undergone lumbar TFESIs at the interventional pain center within Ankara Bilkent City Hospital between 2024–2025. The study protocol was approved by the Ankara City Hospital Medical Research Scientific and Ethical Review Board (TABED 1–25-1862) (19/11/2025) and conducted in accordance with the principles of the Declaration of Helsinki. All patients were informed about the study, and a written informed consent was obtained. We included 252 patients admitted to unilateral or bilateral radiating pain in the lower extremity associated with LBP. These individuals had failed to improve with conservative treatments and were subsequently diagnosed with radiculopathy due to lumbar disc herniation. Diagnosis was established using clinical presentation, physical examination, and lumbar magnetic resonance imaging (MRI).
Inclusion Criteria: (1) Age between 18 and 90 years, (2) presence of LBP with unilateral or bilateral pain radiating to the lower extremity, (3) unresponsive to conservative management, and (4) evidence of lumbar intervertebral disc herniation confirmed by MRI within the last six months. Exclusion criteria: (1) prior lumbar ESI within 3 months, (2) history of polyneuropathy or entrapment neuropathy, (3) presence of bleeding diathesis, systemic or local infections, and (4) having systemic and rheumatic diseases associated with peripheral nerve involvement.
Sociodemographic characteristics of the patients including age, sex, and education status and duration of pain were recorded. The pain severity was evaluated using the Visual analog scale (VAS: 0–10), for functional status the Oswestry Disability Index (ODI) was used, and evaluations were performed at the baseline, the 2nd weeks, and the 3rd months after the procedure.
Functional ability was quantified using the ODI, a self-administered measure of “back-specific function.” This tool uses a 10-item scale (covering areas like pain, sitting, standing, and lifting) where each item is scored 0–5. The cumulative score is standardized to a 0–100 range (higher scores mean worse disability), which is then categorized to indicate the degree of impairment, from Minimal Disability (0–20) up to Bed-Bound/Exaggerating Symptoms (81–100).
All patient evaluations-including demographic registration, pain assessment, outcomes measurement, and both pre- and post-procedural follow-up-were completed by one physiatrist. TFESI were carried out by physicians, who had over 5 years of experience with C arm fluoroscopy-guided injections.
TFESI Technique
All patients were monitored for vital signs before the procedure. Patients were placed in prone position on a C-arm compatible operating table with supporting a pillow under the abdomen to reduce lumbar lordosis. TFESI procedure was performed under sterile conditions, and the injection area was sterilized with povidone-iodine and a sterile drape was laid. To visualize the foramen, the fluoroscopy unit was rotated cranially and obliquely at an angle between 5 and 20 degrees, and 1% lidocaine was injected subcutaneously as a local anesthetic. A Quincke 90mm 22-gauge spinal needle was inserted under the intermittent guidance of fluoroscopy. The needle was advanced into the subpedicular space, proceeding along the path corresponding to the 6 o’clock position. Needle placement was confirmed with a lateral fluoroscopic image. Then, fluoroscopy turned to anteroposterior (AP) position. Subsequently, 1 to 2 mL of contrast was injected, and its satisfactory spread within the epidural space was finally documented using AP view (Figure 1). Following the administration of the contrast agent, the area was checked for vascular uptake. Subsequently, 1 mL of 2% lidocaine was injected, followed by 2 mL (8 mg) of dexamethasone. All patients were monitored for a 30-minute period. The post-procedural complications were evaluated at the end of this period.
 |
Figure 1 Fluoroscopic antero-posterior view of right L4-L5 transforaminal epidural injection contrast distribution pattern. |
Statistical Analysis
The statistical analysis was conducted using SPSS version 25.0 (SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov test was employed to assess the normal distribution. Descriptive analyses for categorical variables were presented as the number of cases (n) and percentage (%), whereas normally distributed variables were defined by the mean and standard deviation, and ordinal and non-normally distributed variables were presented by the median and interquartile range (IQR). Because parametric test assumptions were not met, intra-group comparisons of VAS and ODI were conducted using the Friedman test. When the difference existed and the results were significant, pairwise comparisons with Bonferroni corrections were employed. Statistical significance was established at p < 0.05.
Results
A total of 252 patients underwent TFESI. Out of the 252 patients, 10 declined to attend the 2-week follow-up, and 31 patients, including 8 patients who underwent surgery, did not complete the 3-month follow-up. A total of 221 patients with complete all assessments from the third month were included in the analysis. Ten patients underwent a second injection. The analysis included data from these patients following the second injection. The patients had a mean age of 54.5 ± 14.1 years; 57.5% were female. The demographic data of patients are presented in Table 1. The median duration of symptoms was 5 (2–12) months. All patients received medical therapy prior to the injection. The most common pharmacological treatment was NSAIDs (83.7%). Among the patients, 52% had participated in physical therapy, 19% had undergone prior interventional treatments, 5.9% had received complementary therapy, and 5% had undergone surgery. In 48.4% of patients, the symptomatic side was the left, while 36.2% were on the right. The predominant injection levels were L4-5 (51.1%) and L5-S1 (48.4%) (Table 2). Patients experienced improvements in pain and functionality in both 2nd weeks and 3rd months following the injection (p< 0.001) (Table 3). Treatment success, defined as a greater than 50% reduction in VAS and ODI scores, was achieved in 64.3%, 57.5%, and 74.2% of patients for pain (VAS) at rest, movement, and night, respectively, in the 3rd month.
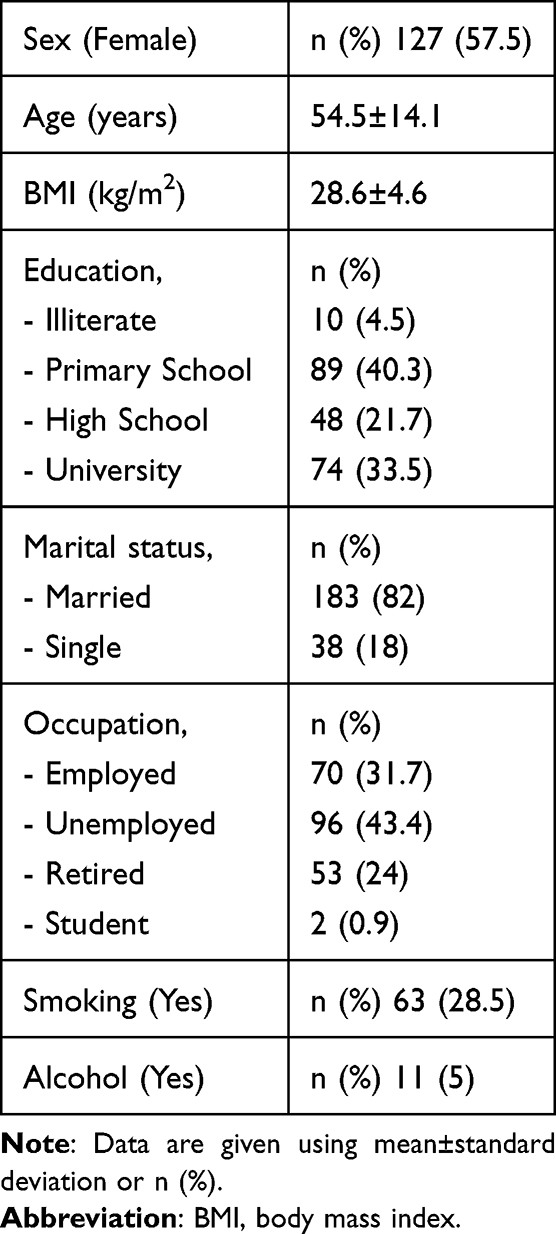 |
Table 1 Socio-Demographic Characteristics of Patients N=221 |
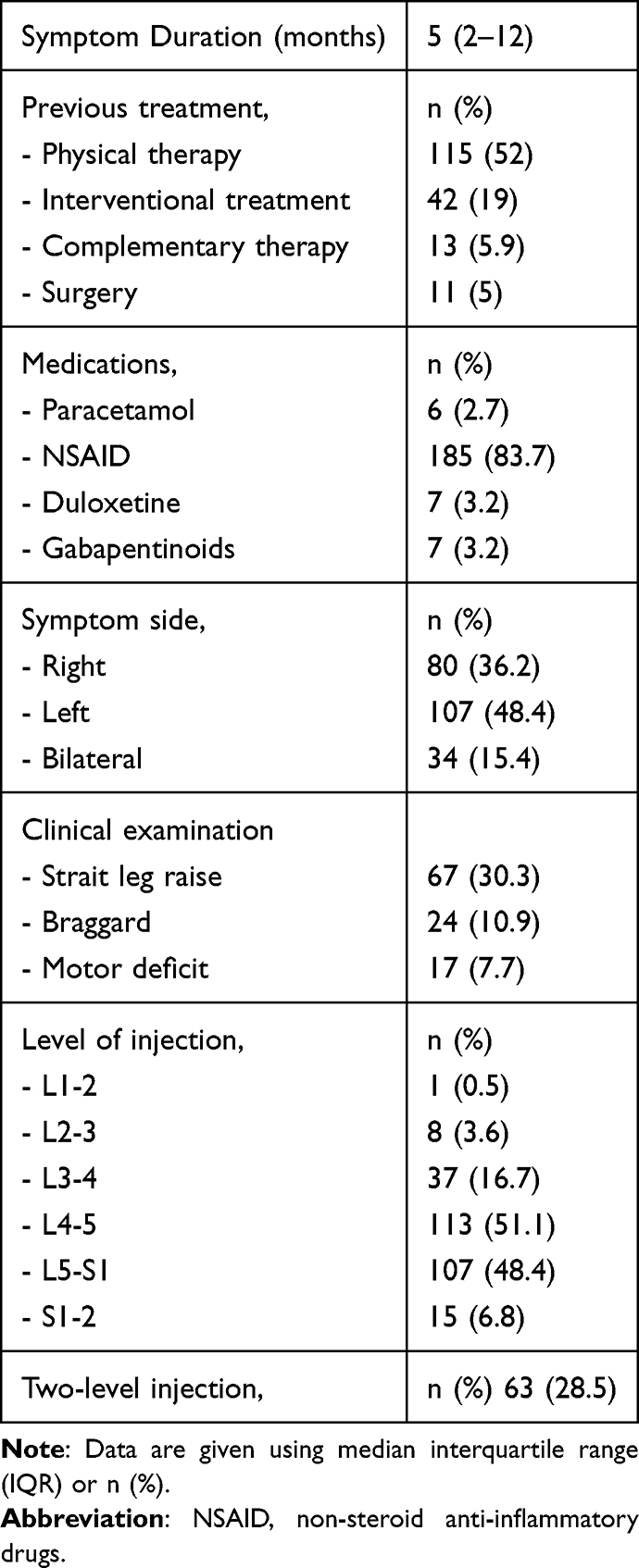 |
Table 2 Clinical Characteristics of Patients N=221 |
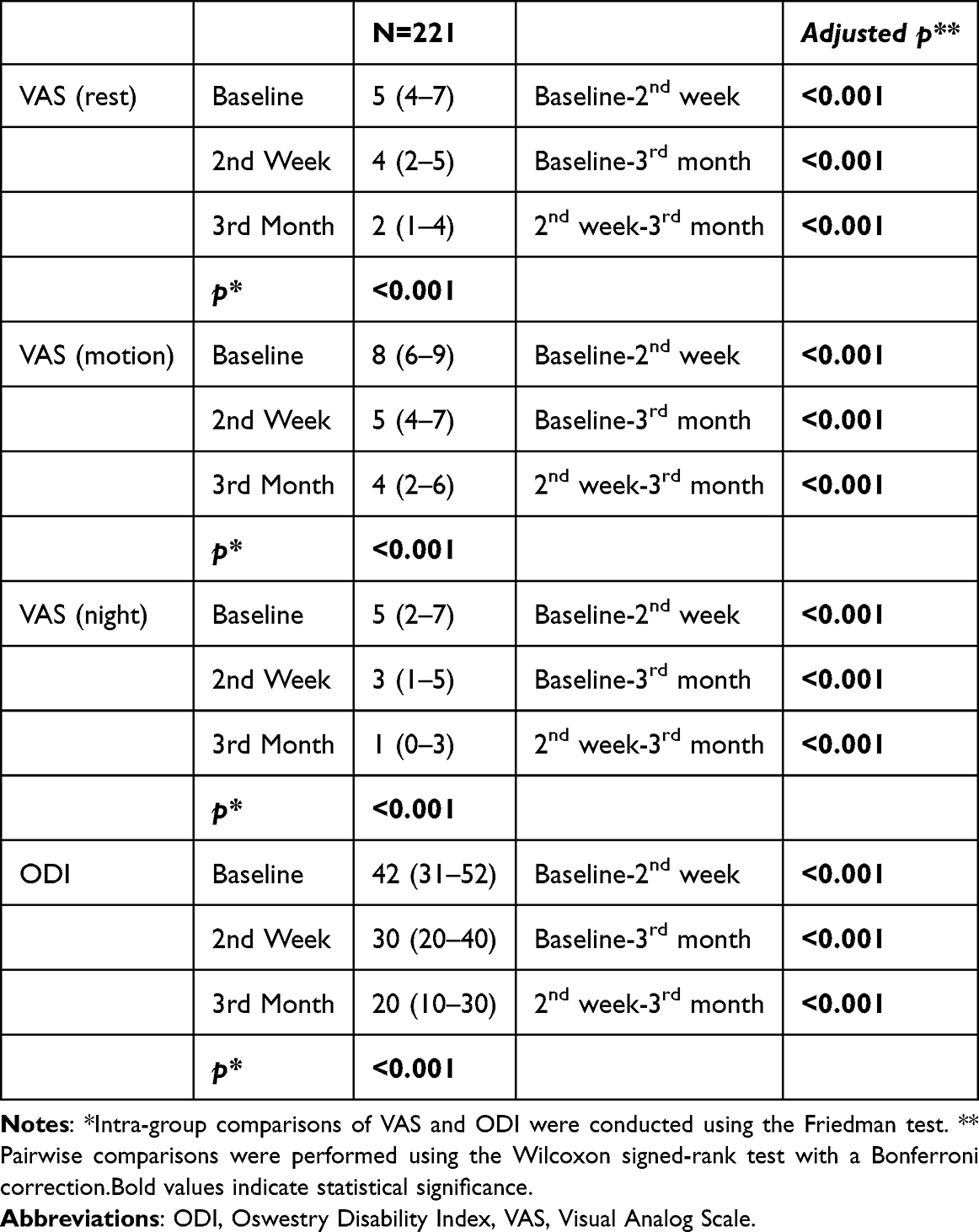 |
Table 3 The Change of Pain and Disability Levels Following the Injection |
Additionally, 55.7% of patients experienced a reduction in disability (ODI) in the 3rd month (Table 4).
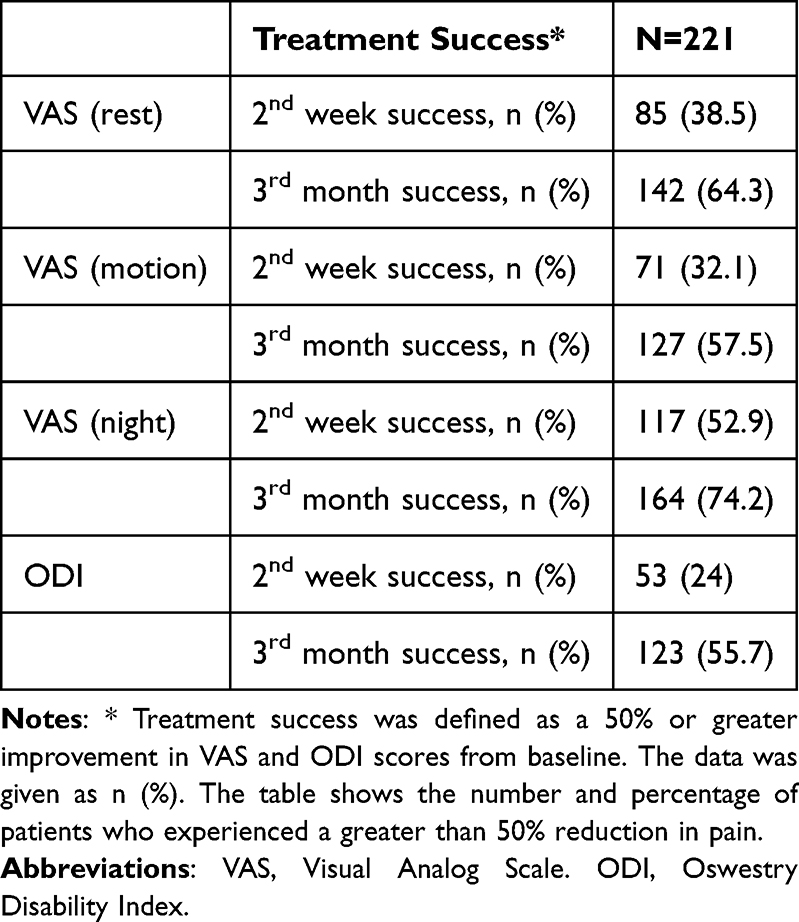 |
Table 4 The Treatment Success |
Discussion
The results of the present study demonstrate that the lumbar TFESIs led to significant and sustained clinical improvements in both pain intensity and functional capacity in patients with radicular pain due to lumbar intervertebral disc herniation. Notably, the substantial reductions in VAS and ODI scores as early as the second week post-injection were maintained through the three-month follow-up period, indicating a rapid onset of action and favorable short-term durability.
Our findings are broadly consistent with the systematic review and meta-analysis conducted by Helm et al which evaluated the efficacy and safety of TFESI for lumbar radicular pain.10 The authors reported Level I evidence supporting the use of TFESI for radicular pain secondary to lumbar disc herniation and demonstrated significant improvements in both pain and functional outcomes at 3 and 6 months. Similar to our results, the review found that a substantial proportion of patients achieved clinically meaningful reductions in pain and disability following treatment.
In a prospective study, Sencan et al demonstrated that TFESI significantly improves radicular pain and neuropathic components in patients with lumbar radiculopathy, supporting our short- and mid-term clinical efficacy.13 Similar to their outcomes, our patients experienced a substantial reduction in pain intensity and associated disability as early as the second week, which was maintained up to the third month.
Furthermore, Sariyildiz investigated the multifaceted effects of TFESI in patients with lumbar disc herniation and reported significant improvements not only in radicular pain and functionality but also in psychological status and sleep quality.14 This aligns with our findings, where the majority of patients achieved treatment success in night pain at the third month. Given that night pain is a major disruptor of sleep architecture and overall quality of life, the high treatment success rate regarding nocturnal symptoms in our cohort underscores the comprehensive benefit of TFESI, matching the holistic improvements observed by Sariyildiz.
While our study focused on a 3-month follow-up period, the sustainability of these clinical outcomes is well-documented in long-term literature. Taskaynatan et al evaluated the long-term effectiveness of TFESI due to lumbar disc herniation and reported that clinical benefits could extend up to two years post-treatment.15 Although our current analysis presents mid-term outcomes up to the third month, the robust initial response and the substantial rate of functional recovery observed in our cohort at 2 weeks and 3 months represent a critical therapeutic window that may predict favorable long-term trajectories, as suggested by Taskaynatan et al.
In a systematic review by Manchikanti et al, the effectiveness of epidural injections in the management of lumbar radiculopathy was confirmed for localized nerve root pathology.16 The outcome measures were pain relief and functional status improvement. Significant improvement was defined as 50% or greater pain relief and functional status improvement. This review states that improvements observed in months 1 and 3 have Level 1 (strong) evidence. Consistent with the Level 1 (strong) evidence reported in recent literature for 1- and 3-month outcomes, our findings revealed statistically significant improvements in both pain and functionality at the 2-week and 3-month follow-ups.
Knezevic et al in a systematic review and meta-analysis, including dual-arm and single-arm analysis, with inclusion of 15 publications, showed Level II, or moderate evidence for similar improvements in both short-and long-term relief of pain and improvement in function with the epidural administration of lidocaine alone or in combination with steroids17 The present study also demonstrated the effects of lidocaine with in combination steroid application on pain and functional improvement in the short and medium term.
In a multicentre study, Wilby et al reported comparable improvements in disability and pain between the two treatment groups at 18 weeks, suggesting that TFESI may represent an effective first-line invasive treatment before surgery in appropriately selected patients.18 Similarly, in our cohort, significant improvements in both pain and disability were observed at 3 months, while only a small proportion of patients subsequently required surgical intervention. These findings suggest that although not all patients respond to injection therapy, TFESI may represent an effective first-line invasive treatment before considering surgery.
Notably, in the present study, only 3.1% of the patients proceeded to surgery during the follow-up period, a finding that underscores the surgery-sparing potential of TFESI. This is consistent with the landmark study by Riew et al,19 which demonstrated that a significant proportion of patients scheduled for operative intervention could avoid surgery following selective nerve root injections.
An important finding of the present study is the considerable variability in individual treatment response. Although statistically significant improvements were observed at the group level, nearly one-third of patients did not achieve clinically meaningful pain relief and almost half failed to demonstrate a ≥50% improvement in disability scores. This discrepancy between group-level improvements and individual treatment success highlights an important limitation of relying solely on mean outcome measures. The heterogeneous response observed in our cohort is consistent with previous evidence suggesting that lumbar radiculopathy represents a clinically diverse condition with multiple biological and psychosocial determinants of outcome.20 Consequently, the beneficial effects of TFESI should not be interpreted as universal, and future research should focus on identifying reliable predictors of treatment response to facilitate more individualized patient selection and expectation management.
Several factors may contribute to this heterogeneity. Although the median symptom duration in our cohort was relatively short, radiological severity, degree of nerve root compression, psychosocial characteristics, and pain chronicity were not evaluated and may have influenced treatment outcomes.
Limitations
Despite its strengths, this study has several limitations. First, the single-center design may restrict the generalizability of our results. Second, the follow-up duration was limited to three months, which precludes conclusions regarding long-term outcomes. In addition, the specific anatomical levels of lumbar disc herniation and their morphological classifications (such as bulging, protrusion, or extrusion) were not specified, and their potential correlations with clinical healing rates were not analyzed. Although the lack of these radiological evaluations stands as a limitation, we specifically included patients with clinically confirmed nerve root compression. Furthermore, we did not strictly control concomitant medication use during the post-procedural period, which may have influenced the reported VAS and ODI scores. Lastly, the absence of a control group makes it challenging to rule out the placebo effect or the natural resolution of symptoms over time.
Conclusion
The present study contributes to the growing body of evidence supporting the clinical utility of TFESI by providing robust, prospective observational data from a large patient population. In particular, the data underscores a notable therapeutic impact on nocturnal pain and a significant recovery of functional autonomy, reflecting the treatment’s true clinical utility. Furthermore, the low rate of surgical conversion observed in the study. This may support TFESI as a key non-operative option in the management of radicular low back pain. Nevertheless, further randomized controlled studies with larger sample sizes are warranted to confirm these findings, particularly with respect to long-term outcomes.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study protocol was approved by the Ankara City Hospital Medical Research Scientific and Ethical Review Board (TABED 1-25-1862) (19/11/2025).
Consent for Publication
All patients were informed about the study, and a written informed consent was obtained.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding source.
Disclosure
The authors declare that they have no competing interests.
References
1. Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64:2028–9. doi:10.1002/art.34347
2. Ferreira ML, de Luca K, Haile LM. GBD. 2021 Low Back Pain Collaborators. Global, regional, and national burden of low back pain, 1990-2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(6):e316–e329. doi:10.1016/S2665-9913(23)00098-X
3. DePalma MJ, Slipman CW. Evidence-informed management of chronic low back pain with epidural steroid injections. Spine J. 2008;8(1):45–55. doi:10.1016/j.spinee.2007.09.009
4. Zhang YG, Guo TM, Guo X, Wu SX. Clinical diagnosis for discogenic low back pain. Int J Biol Sci. 2009;5(7):647–658. doi:10.7150/ijbs.5.647
5. van Os WKM, Alvarez-Jimenez R, Cohen SP, et al. 14. discogenic low back pain. Pain Pract. 2025;25(7):e70062.PMID: 40717265; PMCID: PMC12301617. doi:10.1111/papr.70062
6. Kaye AD, Manchikanti L, Abdi S, et al. Efficacy of epidural injections in managing chronic spinal pain: a best evidence synthesis. Pain Physician. 2015;18(6):E939–1004. [PMID: 26606031]. doi:10.36076/ppj.2015/18/E939
7. Quraishi NA. Transforaminal injection of corticosteroids for lumbar radiculopathy: systematic review and meta-analysis. Eur Spine J. 2012;21(2):214–219. doi:10.1007/s00586-011-2008-y
8. Pountos I, Panteli M, Walters G, Bush D, Giannoudis PV. Safety of epidural corticosteroid injections. Drugs R&D. 2016;16(1):19–34. doi:10.1007/s40268-015-0119-3
9. Lee JH, Shin KH, Park SJ, et al. Comparison of clinical efficacy between transforaminal and interlaminar epidural injections in lumbosacral disc herniation: a systematic review and meta-analysis. Pain Physician. 2018;21:433–448. doi:10.36076/ppj.2018.5.433
10. S HI, Harmon PC, Noe C, et al. Transforaminal epidural steroid injections: a systematic review and meta-analysis of efficacy and safety. Pain Physician. 2021;24(S1):S209–S232. PMID: 33492919.
11. Smith CC, McCormick ZL, Mattie R, et al. The effectiveness of lumbar transforaminal injection of steroid for the treatment of radicular pain: a comprehensive review of the published data. Pain Med. 2020;21:472–487. doi:10.1093/pm/pnz160
12. Manchikanti L, Knezevic E, Knezevic NN, et al. Epidural injections for lumbar radiculopathy or sciatica: a comparative systematic review and meta-analysis of cochrane review. Pain Physician. 2021;24(5):E539–E554. PMID: 34323441.
13. Sencan S, Celenlioglu AE, Yazici G, Gunduz OH. Transforaminal epidural steroid injection improves neuropathic pain in lumbar radiculopathy: a prospective, clinical study. Neurol India. 2021;69(4):910–915. doi:10.4103/0028-3886.323894
14. Sariyildiz MA, Batmaz I, Hattapoğlu S. Predictors of successful treatment after transforaminal epidural steroid injections in patients with lumbar disc herniation. J Back Musculoskelet Rehabil. 2024;37(2):327–335.PMID: 37840482. doi:10.3233/BMR-230051
15. Taskaynatan MA, Tezel K, Yavuz F, Tan AK. The effectiveness of transforaminal epidural steroid injection in patients with radicular low back pain due to lumbar disc herniation two years after treatment. J Back Musculoskelet Rehabil. 2015;28(3):447–451. doi:10.3233/BMR-140539
16. Manchikanti L, Knezevic E, Latchaw RE, et al. Comparative systematic review and meta-analysis of cochrane review of epidural injections for lumbar radiculopathy or sciatica. Pain Physician. 2022;25(7):E889–E916.
17. Knezevic N, Manchikanti L, Urits I, et al. Lack of superiority of epidural injections with lidocaine with steroids compared to without steroids in spinal pain: a systematic review and meta-analysis. Pain Physician. 2020;23:S239–70.
18. Wilby MJ, Best A, Wood E, et al. Surgical microdiscectomy versus transforaminal epidural steroid injection in patients with sciatica secondary to herniated lumbar disc (NERVES): a Phase 3, multicentre, open-label, randomised controlled trial and economic evaluation. Lancet Rheumatol. 2021;3(5):e347–e356. doi:10.1016/S2665-9913(21)00036-9
19. Riew KD, Yin Y, Gilula L, et al. The effect of nerve-root injections on the need for operative treatment of lumbar radicular pain. A prospective, randomized, controlled, double-blind study. J Bone Joint Surg Am. 2000;82(11):1589–1593.PMID: 11097449. doi:10.2106/00004623-200011000-00012
20. Cyteval C, Fescquet N, Thomas E, Decoux E, Blotman F, Taourel P. Predictive factors of efficacy of periradicular corticosteroid injections for lumbar radiculopathy. AJNR Am J Neuroradiol. 2006;27(5):978–982.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.