Back to Journals » Clinical Ophthalmology » Volume 19
Efficacy of Spectacle Correction Using Defocus Incorporated Multiple Segments in the Myopic Population
Authors Zakova M ![]() , Fus M
, Fus M ![]() , Tejkl L
, Tejkl L
Received 18 May 2025
Accepted for publication 7 August 2025
Published 4 September 2025 Volume 2025:19 Pages 3191—3199
DOI https://doi.org/10.2147/OPTH.S541232
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Marketa Zakova, Martin Fus, Leos Tejkl
Faculty of Biomedical Engineering, Czech Technical University in Prague, Kladno, Czech Republic
Correspondence: Marketa Zakova, FBME Czech Technical University in Prague, Sitna Sq. 3105, Kladno, 27201, Czech Republic, Email [email protected]
Aim: The objective of this study was to evaluate the efficacy of DIMS (Defocus Incorporated Multiple Segments) in comparison to control group (CTRL) in a wide age group of European progressive myopes (6– 26 years).
Methods: In this prospective, non-randomised observational study, 78 myopes with progression myopia to − 0.25 to − 8.5 D and astigmatism to − 0.25 to − 2.25 D chose DIMS (n=54) or single vision lenses (SV) (n=24). Baseline measurements included spherical equivalent refraction (SER) and axial length (AL), evaluated at regular intervals.
Results: In participants younger than 15 years of age, slower progression of myopia (SER) (SER − 0.25± 0.35 D) and reduced axial elongation (0.09 ± 0.16 mm) was observed in Group 1 (DIMS) compared to Group 2 (CTRL) (SER − 0.73 ± 0.57 D, AL 0.30 ± 0.20 mm), both significantly at p-value < 0.05. In participants over 15 years of age, Group 3 (DIMS) exhibited minimal myopia progression (SER − 0.24 ± 0.29D) and negligible axial elongation (0.00 ± 0.07 mm), Group 4 (CTRL) demonstrated more pronounced axial elongation (SER − 0.20 ± 0.53D, AL 0.01 ± 0.06 mm).
Conclusion: It can be stated that the DIMS variant is 68.7% more effective in the category of subjects younger than 15 years of age in the effect on AL and 65.6% more effective in the effect on SER compared to the SV lenses. This deceleration in myopia progression is statistically significant in the under 15 age group. A statistically significant difference in the effect on SER in this age group was observed for DIMS.
Keywords: myopia, myopia control, DIMS
Introduction
Myopia, otherwise known as shortsightedness, is a refractive error that affects up to 30% of the population in the Czech Republic and is expected to threaten up to half of the world’s population by 2050.1,2 In addition to reduced uncorrected visual acuity, the severity of high-grade myopia lies mainly in associated pathological complications, the consequences of which can lead to a fatal threat to the vision process itself.3,4 The primary factors contributing to the development of myopia are genetic predisposition and environmental influences.5,6 The most significant progression of myopia is observed in children aged between 7 and 14 years, continues to develop during secondary school and university studies.7,8 A COMET study (2023) found that 23% of 18-year-olds did not have stable myopia.6 A further study, also from 2023, found that approximately 10% of nearsighted individuals aged between 14 and 29 years were diagnosed with a progression of at least −0.50 D within a period of 12 to 26 months.9 It has been demonstrated that 7–20% of myopic individuals exhibit statistically significant myopia progression in adulthood (<-0.25 D/year) and an additional 2–7% progress at an even more rapid rate (<-0.50 D/year).10
We selected spectacle lenses equipped with DIMS technology and high efficacy to slow the progression of myopia for our study.
Spectacle lenses with DIMS (Defocus Incorporated Multiple Segments) technology are individually manufactured polycarbonate lenses for the control of the progression of myopia. These lenses are produced by Hoya and have been available on the global market since 2018 under the brand name Miyosmart. The DIMS lens is characterised by a ring design, comprising a central and functional zone. The central zone, measuring 9.4 mm in diameter, the peripheral zone, spanning 33 mm, is dedicated to myopia management. Myopic blurring is attributed to the presence of small segments (each +3.50 D) within the honeycomb structure, characterised by their high density (see Figure 1).11–13
 |
Figure 1 Spectacle lens with DIMS technology.13 |
These findings have led to the initiation of a three-year research project, the primary objective of which is to assess the efficacy of myopia progression control through the utilisation of integrated segment blur (DIMS) technology in spectacle lenses, with a focus on paediatric and adolescent patients. The objective of this study was to evaluate the efficacy of DIMS in comparison to control group (CTRL) in a wide age group of European progressive myopes (6–26 years).
Materials and Methods
Participants and Study Design
The study is conducted as a project (SGS23/195/OHK4/3T/17) of the Faculty of Biomedical Engineering of the Czech Technical University in Prague. Participants were recruited from across the Czech Republic with no ocular pathologies, no binocular disorders, a myopia range from −0.25 to −8.5 D, an age between 6 and 26 years, and an astigmatism range up to −2.25 D. All participants (78, European ethnicity) were instructed on the course of the study by informed consent form (number: B8/2023, FBME CTU). Subjects were categorised based on their preferences into two distinct groups: conventional single vision correction plastic antireflex spectacle lenses (index of 1.6) – control groups, and the other DIMS correction. The assignment of the form of treatment was made on the basis of subject preference, which could not be masked/blinded due to the visual obviousness of the difference in corrective lens design. All patients used spectacle lenses according to the manufacturer’s recommendations, to which all patients committed in their informed consent.
SER follow-up controls by autorefractometer in cycloplegia were performed on an annual basis, with axial length of the eye (AL) using swept-source interferometry (Lenstar 900) at three-month, six-month and 12-month intervals.
Learning and Data Practices
The primary and secondary outcomes were changes in SER (D) and AL (mm). SER was measured by autorefractometry in cycloplegia (cyclopentolate). Other measurements such as distance and near visual acuity (VA), as well as a comprehensive check of refractive, accommodative and binocular balance at distance and near, were performed in correction without cycloplegia.
Statistical Analysis
The Matlab R2024b statistical analysis software (MathWorks, Inc., USA) was utilised for the analysis of the data. Unless stated otherwise, the mean values and standard deviations (SD) of all continuous variables are given. The progression of myopia over a 12-month period in each group was calculated as the difference between SER at 12 months and the baseline value. Cumulative myopia progression and axial elongation at 3, 6, and 12 months for 1 year were calculated. The trend of changes in SER and AL was plotted against time. Changes in SER and AL were then compared between the four groups, with the results evaluated using a paired T-test.
Results
Participants
The one-year follow-up was completed by 78 participants (156 eyes). Two main groups on DIMS (n=54) or SV (n=24) were further divided into four subgroups according to age categories: up to 15 years, average age of participants 11.74 years (Group 1: DIMS, n = 36; Group 2: control group, n = 10) and over 15 years, average age of participants 19.33 years (Group 3: DIMS, n = 18; Group 4: control group, n = 14).
Changes in SER
A comprehensive analysis of changes in SER over a one-year period is evaluated in the entire study population (Table 1) and by treatment age group (Table 2 and Figure 2). Group 1 (DIMS, up to 15 years) exhibited an average change in SER of −0.25 ± 0.35 D, while Group 2 (CTRL, up to 15 years) demonstrated a change of −0.73 ± 0.57 D. In older participants (over 15 years), the change in SER was −0.24 ± 0.29 D in Group 3 (DIMS) and −0.20 ± 0.53 D in Group 4 (CTRL). The statistical significance was determined to be p<0.001 for Groups 1, 2 and 3 (statistically significant). In contrast, for Group 4, the statistical significance was determined to be p=0.525, (not statistically significant).
 |
Table 1 SER Changes in Overall DIMS and CTRL Across the Whole Population Over 1 Year |
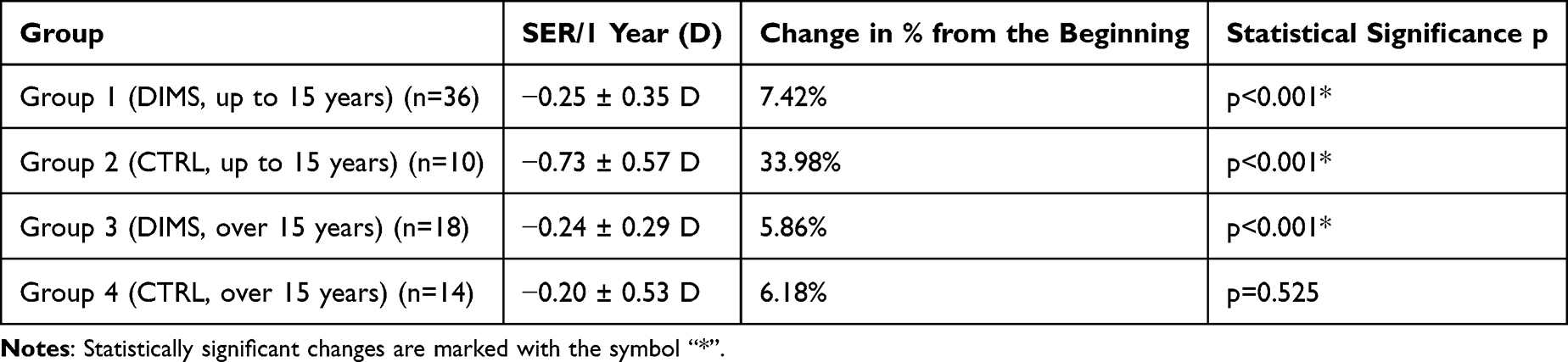 |
Table 2 Changes in SER by Age and Treatment Groups at 1 Year |
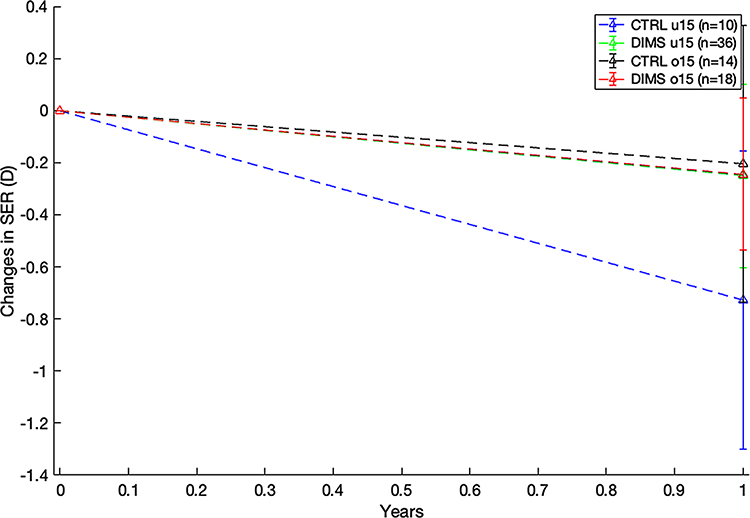 |
Figure 2 Changes in SER per year in monitored groups 1–4. |
Changes in AL
Table 3 and Figure 3 provides axial eye length changes (AL) over a one-year period in four distinct subgroups. Group 1 (DIMS, up to 15 years) exhibited an average axial elongation of 0.09 ± 0.16 mm, while Group 2 (CTRL, up to 15 years) demonstrated an elongation of 0.30 ± 0.21 mm. In young adults, participants over 15 years of age, the AL change in Group 3 (DIMS) was 0.00 ± 0.07 mm and in Group 4 (CTRL) 0.01 ± 0.06 mm. The statistical significance of these changes was determined to be p<0.001 for Groups 1 and 2 (statistically significant). In contrast, the changes observed in Groups 3 and 4 were not statistically significant (p=0.9814 and p=0.2734, respectively).
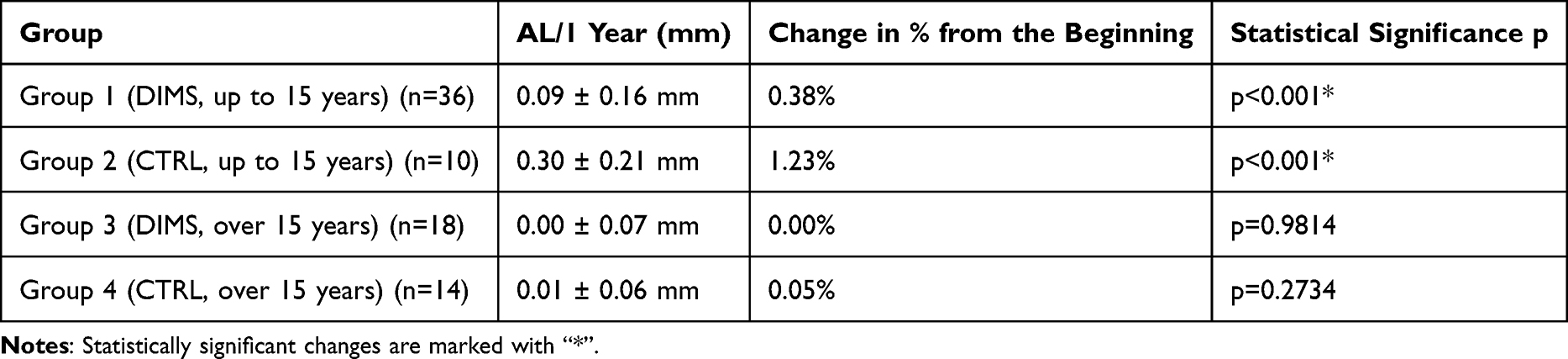 |
Table 3 Changes in the Axial Length of the Eye |
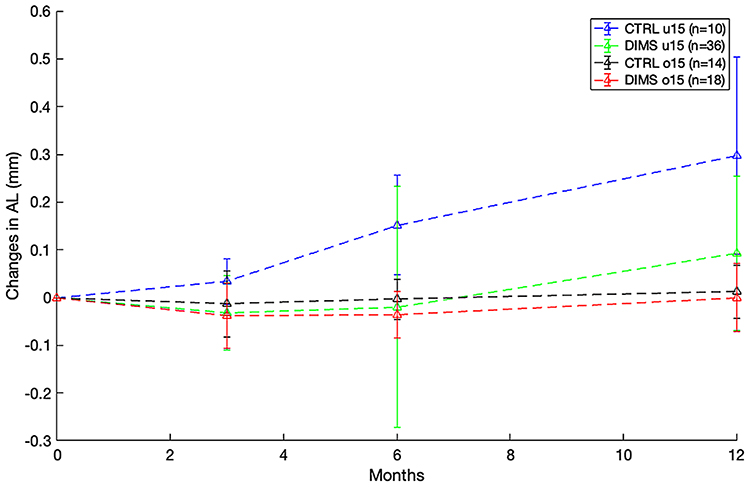 |
Figure 3 Changes in AL after 3, 6 and 12 months in monitored groups 1–4. |
Discussion
This study summarises the results of a 12-month follow-up period of myopia progression in the age range 6–26 years in European ethnicity, including an evaluation of the effect of DIMS on slowing myopia progression.
Influence of Ethnicity
The majority of studies on myopia are conducted on groups of Asian children.2 The mean rate of myopia progression in Hong Kong children aged 5 to 16 years was −0.63 D/year.14 A study on European children (DREAM, 2022) estimated the annual progression of myopia at −0.50 D at the age of up to 10 years and −0.38 D at the age of 10 to 12 years.15 In our study, conducted at a similar age range of 6–15 years, the mean progression rate per year was −0.73 ± 0.57 D. In a separate study on Asian children aged 8–11 years, the progression rate of the AL parameter was reported to be 0.37 mm/year.16 In contrast, the progression of AL in our control group (age 6–15 years) was found to be 0.30 ± 0.21 mm. In contrast to our study, previous research on Asian children has documented a lower SER/year parameter. The influence of ethnicity on the progression of both AL and SER has been demonstrated as questionable.
Effect of Age on Myopia Progression
Myopia typically manifests initially between the ages of 6 and 10, and continues to progress. For instance, the COMET study observed a decline in the rate of myopia progression with age in a cohort of 15.6 ± 4.2 years, with a mean refractive error of −4.87 ± 2.01 D. Approximately half (48%) of the COMET cohort demonstrated stability at the age of 15. The proportion of those whose myopia stabilised increased to 77% (330 out of 426) at age 18 and 90% (384 out of 426) at age 21, and almost all stabilised at age 24. These findings indicate that more than 50% of children still progress at age 15, almost 25% at age 18, and 10% at age 21.8 The Australian study follows a group of 20-year-old participants and measures their SER over an eight-year period. The study found that the spherical equivalent of the eyesight of the participants progressed by an average of −0.04 D per year.7
In contrast, the present study focuses on young adults, extending up to the age of 26. The study confirms that the progression of myopia in the SER and AL parameters decreases with age. In the control group, which was monitored from 15 to 26 years of age (mean age 20.28 years), the spherical equivalent (SER) was −0.20 ± 0.53 D and the axial length (AL) 0.01 ± 0.06 mm per year (not statistically significant). The higher change in SER in our group is explained by the inclusion of university students only.
Influence of Family Myopic History and Environment on the Development of Myopia
Genetics have a significant impact on eye growth. The presence of two short-sighted parents generally poses a greater risk than the presence of one.17,18
The present study’s findings reveal that 53% of participants had both parents with myopia, 18% had myopia in only their mother, 14% had myopia in only their father, and 15% had no family history of myopia. More than half of our participants, specifically 57%, reported a manifestation of myopia in their siblings. The influence of environmental factors, such as the child’s growth environment, outdoor activity levels, and the presence of digital devices, is frequently identified as a contributing element.19–21 The results of our participants spent between one and two hours outdoors daily, six hours working at close range, and between one and four hours using digital devices, the average sleep duration was eight to nine hours.
A comparative analysis of the efficacy of DIMS in relation to other methods of myopia treatment is presented in the following studies:
Orthokeratology has been demonstrated to be an effective method of slowing down the growth of AL, as confirmed by a five-year study.22 AL was 0.20 mm/year. A study on soft multifocal contact lenses (ADD+2.5) in children (mean age 10.3) wearing these contact lenses was 0.20 D/year (SER) and 0.16 mm/year (AL).23 The combination of DIMS and atropine at a concentration of 0.01% demonstrated an efficacy rate of 70% of SER/year and 77% AL compared to the CTRL group in European children aged 9.81 years.24 In a study of MiSight soft contact lenses on children aged 8–12 years SER was −0.18 D vs −0.58 D/year, AL 0.24 mm/year (CTRL group) versus 0.09 mm in the MiSight group.25
Efficacy of DIMS Compared to Other DIMS Studies for the Myopia Treatment
In a Chinese study of children aged 8–13 years, the effectiveness of DIMS was 52% greater for SER and 62% greater for AL compared to the control group over two years of research.13 In a separate European study, the effectiveness of DIMS in the age group 6–18 years was 57% of SER and 57% of AL compared to the control group.24 The findings of this study demonstrate that the treatment of myopia with DIMS is 68.7% more effective in the younger than 15 years group in the effect on AL and 65.6% more effective in the effect on SER compared to the control variant. This slowing of myopia progression is statistically significant in the under-15 category. In the category of subjects under 15 years of age, a statistically significant slowdown in progression is confirmed in the parameters of SER and AL. In the category of subjects over 15 years of age, a greater effect of DIMS on AL than SER compared to the control group was found, but unfortunately these results were not statistically significant. The absence of further studies in this age group hinders the ability to draw definitive conclusions regarding the effects of DIMS treatment on individuals over 18 years of age.
In their review of the results of several myopia control trials, Bullimore et al26 and Lam et al27–29 suggested that the benefit of any myopia control treatment appears to be the same regardless of the race of the children. This finding is corroborated by the present study.
A Comparative Analysis of the Efficacy of DIMS in Relation to Other Spectacle Lenses of Myopia Treatment
In a year-long study, the effect of spectacle lenses with different asphericity – highly aspherical lenslet (HAL) or slightly aspherical lenslet (SAL) on AL and SER was compared to that of SV spectacle lenses in Chinese children aged 8–13 years. After 1 year, the mean changes in the SER (±SE) and AL (±SE) in the SVL group were −0.81±0.06 D and 0.36±0.02 mm. Compared with SV, the myopia control efficacy measured using SER was 67% (difference of 0.53 D) for HAL and 41% (difference of 0.33 D) for SAL, and the efficacy measured using AL was 64% (difference of 0.23 mm) for HAL and 31% (difference of 0.11 mm) for SAL (all p<0.01).30,31 SightGlass Vision DOT 0.2 lenses have been investigated in a randomized clinical trial of children aged 6 to less than 10 years, with interim 12-month data recently published. The results showed that children wearing the test lens had 0.15mm axial length growth in a year, compared to 0.30mm in the control group, representing a 50% reduction. For children aged 6–7 years, refractive progression was −0.19D in a year in the test lens compared to −0.75D in the control group.32,33
In a 1-year randomized trial, 118 Chinese children (aged 8 to 12) with myopia and astigmatism were assigned either cylindrical annular refractive element (CARE) lenses (61 children) or single-vision lenses (CTRL, 57 children). Results show CARE lenses slowed myopia progression by 0.14D (21% reduction) compared to CTRL group. Axial length progression was also 0.09mm less with CARE lenses (a 23% reduction).34
In the present study, Group 1 (DIMS, up to 15 years) demonstrated an average axial elongation of 0.09 ± 0.16 mm, while Group 2 (CTRL, up to 15 years) exhibited an elongation of 0.30 ± 0.21 mm. Group 1 (DIMS, up to 15 years) exhibited an average change in SER of −0.25 ± 0.35 D, while Group 2 (CTRL, up to 15 years) demonstrated a change of −0.73 ± 0.57 D. This study’s results are as follows: the treatment of myopia with DIMS is 68.7% more effective in subjects under the age of 15 years on AL than CTRL variant, and 65.6% more effective in terms of its effect on SER. Comparison summary is presented in the Table 4.
 |
Table 4 Changes in AL and SER - Comparing Studies of Spectacle Lenses Used to Treat Myopia25 |
Conclusion
The use of the DIMS lens technology significantly slowed down the progression of myopia and axial elongation in myopic children under the age of 15. In the group of young adults, DIMS positively affected the axial length of the eyes compared to conventional lenses and no worsening of SER. The differences were not statistically significant in individuals over 15 years of age, with the exception of SER. A comparison of the annual results (SER, AL) obtained from the present study with the results of available studies aimed at decelerating the progression of myopia reveals that DIMS treatment is beneficial irrespective of the ethnicity of the probands. The results are limited by the sample size and one-year follow-up. However, these findings motivate us and ophthalmologists to use technologies that slow the progression of myopia and to continue our research. A follow-up study will monitor a larger sample of patients and allow for a longer follow-up period, which may confirm these results and the long-term stability of myopia.
Ethical Statement
This study complies with the Declaration of Helsinki when it adheres to ethical principles for medical research involving human subjects, ensuring scientific rigor, transparency, and participant well-being. Data are available on personal request by corresponding author. Consent form approved 8. 6. 2023 by the commission named: Faculty of Biomedical Engineering Czech Technical University Ethics Committee: no. B8/2023. Informed consent was always signed by a legal representative.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study is supported by SGS grant competition of Czech Technical University in Prague number: SGS23/195/OHK4/3T/17. Trail registration number: NCT05943912.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Belikova J. Vyvoj myopie. Ceska Ocní Optika. 2012;4.
2. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;5:123.
3. Fricke TR, Holden BA, Wilson DA. Global cost of correcting vision impairment from uncorrected refractive error. Bulletin of the World Health Organisation. 2012;(10):90.
4. IAPB: WHO - Global initiative for the elimination of blindness; 2020. Available from: https://www.iapb.org/resources/who-global-initiative-for-the-elimination-of-blindness/.
5. Tedja MS, Haarman AEG, Meester-Smoor MA, et al. IMI – myopia genetics report. Invest Ophthalmol Vis Sci. 2019;60(3):M89–M105. doi:10.1167/iovs.18-25965
6. COMET Group. Myopia stabilization and associated factors among participants in the Correction of Myopia Evaluation Trial (COMET). Invest Ophthalmol Vis Sci. 2013;54(13):7871–7884. PMID: 24159085; PMCID: PMC3850666. doi:10.1167/iovs.13-12403
7. Ip JM, Huynh SC, Robaei D, et al. Ethnic differences in the impact of parental myopia: findings from a population-based study of 12-year-old Australian children. Investigative Opthalmology & Visual Science. 2007;48:2520–2528. doi:10.1167/iovs.06-0716
8. Verkicharla PK, Kammari P, Das AV. Myopia progression varies with age and severity of myopia. PLoS One. 2020;15(11):e0241759. doi:10.1371/journal.pone.0241759
9. Ducloux A, Marillet S, Ingrand P, et al. Progression of myopia in teenagers and adults: a nationwide longitudinal study of a prevalent cohort. British Journal of Ophthalmology. 2023;107:644–649. doi:10.1136/bjophthalmol-2021-319568
10. Moore M, Lingham G, Flitcroft DI, Loughman J. Patterns of myopia progression in European adults. Ophthalmology Science. 2025;5:100713. doi:10.1016/j.xops.2025.100713
11. HOYA. MiYOSMART Available from: www.hoyavision.com/uk/vision-products/miyosmart/.
12. Kaymak H, Graff B, Neller K, et al. Myopietherapie und Prophylaxe mit “Defocus incorporated multiple segments”-Brillengläsern. Ophthalmologe. 2021;118:1280–1286. doi:10.1007/s00347-021-01452-y
13. Lam CSY, Tang WC, Tse DY, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. British Journal of Ophthalmology. 2020;104:363–368. doi:10.1136/bjophthalmol-2018-313739
14. Fan DS, Lam DSC, Lam RF, et al. Prevalence, incidence, and progression of myopia of school children in Hong Kong. Invest. Ophthalmol. Vis. Sci. 2004;45:1071–1075. doi:10.1167/iovs.03-1151
15. Polling JR, Klaver C, Tideman JW. Myopia progression from wearing first glasses to adult age: the DREAM study. Br. J. Ophthalmol. 2022;106:820–824. doi:10.1136/bjophthalmol-2020-316234
16. Cheng X, Xu J, Chehab K, Exford J, Brennan N. Soft contact lenses with positive spherical aberration for myopia control. Optom Vis Sci. 2016;93(4):353–366. PMID: 26704144. doi:10.1097/OPX.0000000000000773
17. Morgan I, Rose K. How genetic is school myopia? Prog Retin Eye Res. 2005;24(1):1–38. PMID: 15555525. doi:10.1016/j.preteyeres.2004.06.004
18. Cai XB, Shen SR, Chen DF, et al. An overview of myopia genetics. Experimental Eye Research. 2019;188:107778. doi:10.1016/j.exer.2019.107778
19. Morgan IG, French AN, Ashby RS, et al. The epidemics of myopia: aetiology and prevention. Prog Retin Eye Res. 2018;62:134–149. PMID: 28951126. doi:10.1016/j.preteyeres.2017.09.004
20. Biswas S, El Kareh A, Qureshi M, et al. The influence of the environment and lifestyle on myopia. J Physiol Anthropol. 2024;43(1):7. PMID: 38297353; PMCID: PMC10829372. doi:10.1186/s40101-024-00354-7
21. Jonas JB, Ang M, Cho PG, et al. IMI prevention of myopia and its progression. Invest. Ophthalmol. Vis. Sci. 2021;62(5):6. doi:10.1167/iovs.62.5.6
22. Hiraoka T, Kakita T, Okamoto F, et al. Long-term effect of overnight orthokeratology on axial length elongation in childhood myopia: a 5-year follow-up study. Invest. Ophthalmol. Vis. Sci. 2012;53:3913–3919. doi:10.1167/iovs.11-8453
23. Walline JJ, Walker MK, Mutti DO, et al. Effect of high add power, medium add power, or single-vision contact lenses on Myopia progression in children: the BLINK randomized clinical trial. JAMA. 2020;24:571–580. doi:10.1001/jama.2020.10834
24. Nucci P, Lembo A, Schiavetti I, Shah R, Edgar DF, Evans BJW. A comparison of myopia control in European children and adolescents with defocus incorporated multiple segments (DIMS) spectacles, atropine, and combined DIMS/atropine. PLoS One. 2023;18(2):e0281816. PMID: 36795775; PMCID: PMC9934319. doi:10.1371/journal.pone.0281816
25. Chamberlain P, Peixoto-de-matos SC, Logan NS, et al. A 3-year randomized clinical trial of MiSight lenses for myopia control. Optom. Vis. Sci. 2019;96:556–567. doi:10.1097/OPX.0000000000001410
26. Bullimore MA, Brennan NA. Efficacy in myopia control: does race matter? Optom. Vis. Sci. 2023;100:5–8. doi:10.1097/OPX.0000000000001977
27. Lam CSY, Tang WC, Zhang HY, et al. Long-term myopia control effect and safety in children wearing DIMS spectacle lenses for 6 years. Sci Rep. 2023;13(1):5475. PMID: 37015996; PMCID: PMC10073092. doi:10.1038/s41598-023-32700-7
28. Lam CS, Tang WC, Lee PH, et al. Myopia control effect of defocus incorporated multiple segments (DIMS) spectacle lens in Chinese children: results of a 3-year follow-up study. Br J Ophthalmol. 2022;106(8):1110–1114. PMID: 33731364; PMCID: PMC9340033. doi:10.1136/bjophthalmol-2020-317664
29. Lee SS, Lingham G, Sanfilippo PG, et al. Incidence and progression of myopia in early adulthood. JAMA Ophthalmol. 2022;140(2):162–169. PMID: 34989764; PMCID: PMC8739830. doi:10.1001/jamaophthalmol.2021.5067
30. Bao J, Yang A, Huang Y, et al. One-year myopia control efficacy of spectacle lenses with aspherical lenslets. Br J Ophthalmol. 2022;106(8):1171–1176. PMID: 33811039; PMCID: PMC9340037. doi:10.1136/bjophthalmol-2020-318367
31. Bao J, Huang Y, Li X, et al. Spectacle lenses with aspherical lenslets for myopia control vs single-vision spectacle lenses: a randomized clinical trial. JAMA Ophthalmol. 2022;140(5):472–478. PMID: 35357402; PMCID: PMC8972151. doi:10.1001/jamaophthalmol.2022.0401
32. Rappon J, Chung C, Young G, et al. Control of myopia using diffusion optics spectacle lenses: 12-month results of a randomised controlled, efficacy and safety study (CYPRESS). Br J Ophthalmol. 2023;107(11):1709–1715. PMID: 36126105; PMCID: PMC10646852. doi:10.1136/bjo-2021-321005
33. Neitz J, Neitz M. Diffusion Optics Technology (DOT): a myopia control spectacle lens based on contrast theory. Transl Vis Sci Technol. 2024;13(10):42. PMID: 39476085; PMCID: PMC11534017. doi:10.1167/tvst.13.10.42
34. Liu X, Wang P, Xie Z, et al. One-year myopia control efficacy of cylindrical annular refractive element spectacle lenses. Acta Ophthalmol. 2023;101(6):651–657. PMID: 36779428. doi:10.1111/aos.15649
35. Myopia Profile. Supporting eye care practitioners in myopia management. Available from: www.myopiaprofile.com.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Awareness of Myopia Associated Complications and Perspectives on Myopia Management Among Parents of Children with Myopia in France and the UK

Hafizi R, Deferne N, Paudel N, Angerer A, Hsieh HT
Patient Related Outcome Measures 2025, 16:147-161
Published Date: 13 November 2025
Ocular Dimensional Changes After 12 Months of Orthokeratology and Single-Vision Spectacle Use: A Three-Dimensional Magnetic Resonance Imaging Study
Low YC, Mohd-Ali B, Shahimin MM, Mohidin N, Wan Abdul Halim WH, Mokri SS, Abdul-Hamid H
Clinical Optometry 2026, 18:611080
Published Date: 14 July 2026