")
Back to Journals » International Journal of Nanomedicine » Volume 12
Efficacy of silk fibroin–nano silver against Staphylococcus aureus biofilms in a rabbit model of sinusitis
Authors Jia M , Chen Z, Guo Y, Chen X, Zhao X
Received 13 December 2016
Accepted for publication 20 March 2017
Published 10 April 2017 Volume 2017:12 Pages 2933—2939
DOI https://doi.org/10.2147/IJN.S130160
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Lei Yang
Minghui Jia,1,2 Zhongchun Chen,2 Yongwei Guo,2 Xin Chen,3 Xia Zhao2
1Department of Otolaryngology-Head and Neck Surgery, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, 2Department of Otolaryngology-Head and Neck Surgery, Huashan Hospital, Fudan University, 3State Key Laboratory of Molecular Engineering of Polymers, Department of Macromolecular Science, Laboratory of Advanced Materials, Fudan University, Shanghai, China
Background: Staphylococcus aureus biofilms contribute significantly to the recalcitrant nature of chronic rhinosinusitis. In previous studies, it has been shown that silk fibroin–nano silver solution can eliminate S. aureus biofilms in vitro, which suggests a potential role of this novel agent in the treatment of biofilm-associated diseases, such as sinusitis.
Objective: The aim of this study was to investigate the efficacy of silk fibroin–nano silver solution as a topical anti-biofilm agent in a rabbit model of sinusitis.
Methods: Biofilm-associated sinusitis models were established in 24 New Zealand White rabbits by gelatin sponge placement and S. aureus inoculation through a hole drilled into the anterolateral wall of the right maxillary sinus. After 4 weeks, indwelling catheters were placed into the maxillary sinus. Different concentrations of silk fibroin–nano silver solution or normal saline were irrigated slowly into the maxillary sinus via the indwelling catheters. After 7 days of irrigation, the rabbits were sacrificed. The sinus mucosa was harvested and examined for biofilm biomass as well as morphological integrity of the epithelium by scanning electron microscopy.
Results: Silk fibroin–nano silver solution was found to be most effective in reducing the biomass of the S. aureus biofilms at a concentration of 384 mg/L, followed by the concentration of 153.6 mg/L, when compared with saline. After treatment with 384 mg/L silk fibroin–nano silver solution, the biofilms were completely eliminated and the injured epithelium was almost restored with regenerated cilia on the surface.
Conclusion: Silk fibroin–nano silver solution was found to be an effective topical agent against S. aureus biofilms in the rabbit model of sinusitis, and its effect was concentration-dependent.
Keywords: chronic rhinosinusitis, nasal irrigation, maxillary sinus, biomass, scanning electron microscopy, animal
Introduction
Bacterial biofilm refers to aggregates of microorganisms embedded in a self-made protective matrix of exopolymers. The bacteria within the biofilms are resistant to antibiotics; in some cases, the resistance may increase a thousand fold.1 Therefore, conventional antibiotic therapy is frequently ineffective in eradicating bacteria in the biofilm. It is generally believed that biofilm is a common cause of persistent infections and chronic inflammatory diseases that are difficult to be cured.2,3
In recent years, biofilms have been consistently detected on the nasal mucosa of patients with chronic rhinosinusitis (CRS).4–11 These are typically associated with more severe disease and with poor outcomes of endoscopic sinus surgery.12,13 Staphylococcus aureus biofilm is increasingly implicated in the pathogenesis of CRS.11,14–16 Evaluation of therapeutic interventions that specifically target S. aureus biofilms in patients with CRS is a key imperative.17,18
Given that the mucosa of the sinus cavities is accessible to topical therapy, it is intuitive to evaluate the effect of topical antibiotics for treatment of biofilm infections. Earlier, the efficacy of silk fibroin–nano silver (SF-NS) solution in disrupting S. aureus biofilms has been demonstrated in vitro.19 This study tested the use of topical SF-NS solution in a rabbit model of S. aureus biofilm-associated sinusitis. The stable existence of S. aureus biofilms on the maxillary sinus mucosa was verified after 4 weeks of bacterial inoculation,20 which gave an opportunity to test this novel therapeutic agent against biofilm under in vivo conditions.
Materials and methods
Animals
Twenty-four New Zealand White rabbits (weight: 2.5–3.5 kg) were obtained from the Laboratory Animal Center at the Fudan University (Shanghai, China). All the experimental protocols were approved by the Animal Care and Use Committee of Fudan University, and the animal study was carried out in accordance with the Ethical Guidelines for Animal Experiments established by Fudan University.
SF-NS solution
The SF-NS solution used in this study was supplied by the State Key Laboratory of Molecular Engineering of Polymers and was made by in situ reduction reaction between natural polymer Bombyx mori silk fibroin and silver nitrate under light. The principles of synthesis of SF-NS and its key characteristics are shown in Figure 1; a more detailed description is available in a previous study.19 The average size of the silver nanoparticle was 12.0±2.1 nm. The minimum bactericidal concentration (MBC) for S. aureus strain (clinical isolate Sa006) was 76.8 mg/L, which was determined according to the Clinical & Laboratory Standards Institute (CLSI, 2011) guidelines for macrodilution in broth.19
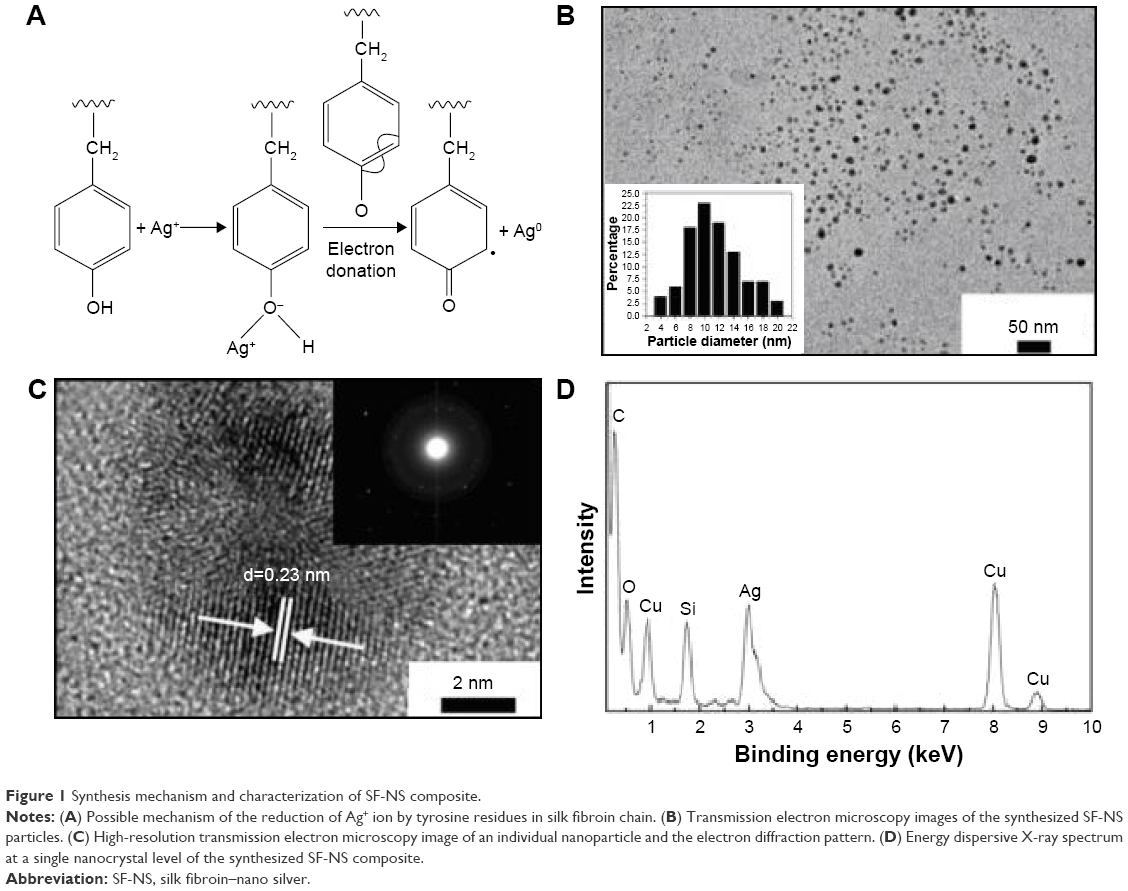 | Figure 1 Synthesis mechanism and characterization of SF-NS composite. |
Bacterial preparation
The biofilm-forming Sa006, determined by the traditional crystal violet biofilm assay,21,22 was chosen owing to its relatively strong biofilm formation capacity. The night before the modeling surgery, a single colony of Sa006 was inoculated in tryptic soy broth supplemented with 0.5% glucose (TSBg) and incubated overnight at 37°C with shaking. Then the bacterial suspension was diluted 200-fold with TSBg to achieve a concentration of ~1×106 Colony-Forming Units (CFU)/mL and kept on ice for further use.
Modeling surgery
A rabbit model of S. aureus biofilm-associated sinusitis was established surgically as previously described by our group.20 Briefly, under adequate anesthesia, the skin was incised vertically along the median line of the dorsum. A laterally based flap of periosteum was elevated from the midline to the right side, and then a small hole (diameter: 1.5 mm) was drilled to enter the right maxillary sinus. A piece of compressed absorbable gelatin sponge was inserted into the maxillary sinus, and subsequently inoculated with 0.5 mL of bacterial suspension through the hole. Then, the periosteal and skin incisions were closed with interrupted suture, and the rabbits were caged individually in an air-conditioned room with 12-hour dark–light cycles and free access to water and food.
Indwelling irrigation catheter
Four weeks after modeling surgery, indwelling maxillary sinus irrigation catheters were placed into the right maxillary sinus as described by Chiu et al23 with some modification. Briefly, a plastic catheter connected with an end-enlarged stainless steel needle was used as the irrigating catheter and tunneled under the skin from the vertex to the dorsum incision (Figure 2A). The hub of the metal needle was exposed outside the vertex and secured to the skin with a purse string suture, to avoid its displacement by the animals. The enlarged end of the metal needle under the skin was fixed between the skin and periosteum with interrupted suture to secure the catheter (Figure 2B). Approximately 4 mm of the plastic end was inserted into the maxillary sinus through the hole made in the modeling process (Figure 2C).
 | Figure 2 Methodology for implantation of indwelling catheter and sinus irrigation. |
Topical irrigation
The rabbits were randomly divided into four groups (six animals in each group): a blank control group (animal models without irrigation), a negative control group (treated with saline), and two experimental groups (treated with 153.6 and 384 mg/L of SF-NS solution [2× MBC and 5× MBC, respectively]l). The right maxillary sinus was irrigated at a slow pace with test solution, SF-NS solution or normal saline via the indwelling catheter (2 mL twice a day; flow rate: 0.2 mL/s), starting at 1 day after implantation of the indwelling catheter.
Tissue harvest
After 7 days of irrigation, the rabbits were anesthetized with intraperitoneal administration of 10% chloral hydrate (350 mg/kg) and sacrificed with air injection through ear vein. The maxillary sinuses were resected and opened with a pair of scissors. The sinus mucosa was carefully removed, washed thoroughly with saline, and placed in 2.5% glutaraldehyde for scanning electron microscopy (SEM) specimen preparation.
SEM specimen preparation and analysis
The specimens were initially fixed for 24 hours in 2.5% glutaraldehyde at 4°C, then rinsed three times with 1× phosphate-buffered saline (PBS) and fixed with 1% osmium tetroxide for 2 hours. They were then rinsed again three times with PBS, and dehydrated through a graded ethanol series (50%, 70%, 90%, 100%, 15 minutes each). The specimens were then immersed in a mixture of 100% ethanol and isoamyl acetate (2:1), and then in pure isoamyl acetate, for 15 minutes each solution. All specimens were dried in carbon dioxide critical point dryer, sputter coated with gold, and examined with an SU8010 SEM (Hitachi, Tokyo, Japan) at an accelerating voltage of 10 kV. The images were obtained at 2,000× to 5,000× magnification. Structures characterized by water channels, 3D structure, and matrix-embedded spherical bodies were evaluated for evidence of bacterial biofilms.9
For quantitative analysis of biofilm formation on the sinus mucosa in each rabbit, three fields of vision were randomly selected for each specimen. Each field of view (2,000×) was equally divided into nine regions and graded according to the number of biofilm affected regions (average of the three visual fields): lack of involvement of any region was recorded as 0, involvement of 1–3 regions as 1, involvement of 4–6 regions as 2, and involvement of 7–9 regions as 3. Statistical analysis was performed using Kruskal–Wallis rank sum test, and P-value <0.05 was considered as statistically significant.
Results
Overall, the animals tolerated the surgical procedures and catheter implantation well. The irrigation solutions were dripping out of the right nares of all rabbits (Figure 2D). Two of the 24 animals died prematurely during the period of nasal irrigation (one each in the saline group and the 5× MBC group) of pneumonia with empyema, presumably caused by aspiration of the test solutions into the lower respiratory tract. None of the other animals showed signs of systemic illness during the course of the experiment.
The sinuses of the model rabbits in the blank control group were filled with thick mucopurulent secretions, and the mucosa was friable and swollen. The sinuses in the negative control and 153.6 mg/L SF-NS experimental group showed mild to moderate edema of the mucosal linings with mild pus formation. The mucosa in 384 mg/L SF-NS experimental group was very thin and smooth, with no pus in the sinuses.
On SEM, significant differences were observed between specimens from the different groups. For the rabbits without topical irrigation, SEM showed destruction of cilia of the sinus mucosa and clusters of organisms attached to the mucosa with morphological features of biofilms, such as water channels, 3D structure, and matrix-embedded spherical bodies (Figure 3A1 and A2). This phenomenon was observed in all six rabbits in the group. Saline irrigation in the negative control group reduced the bacterial biofilms of the sinus mucosa to a certain extent. However, severe injury of the epithelial layer showed no sign of ciliary regeneration. A considerable portion of the biofilm still existed between the epithelial cells (Figure 3B1 and B2). For the experimental group treated with 153.6 mg/L SF-NS solution, the epithelium was found to have partially repaired with some ciliary buds and short cilia. The biofilms were almost impossible to detect at low magnification (Figure 3C1). However, the cell damage was still visible and a small portion of biofilms still existed; some damaged epithelial cells were observable at high magnification (Figure 3C2). In the experimental group treated with 384 mg/L SF-NS solution, the integrity of the epithelium was almost completely restored with relatively normal cilia; however, some naked epithelial cells were still present, and there was no evidence of bacterial biofilm on the mucosal surface (Figure 3D1 and D2), which was significantly lower than that in the negative control group or 153.6 mg/L of SF-NS-treated experimental group.
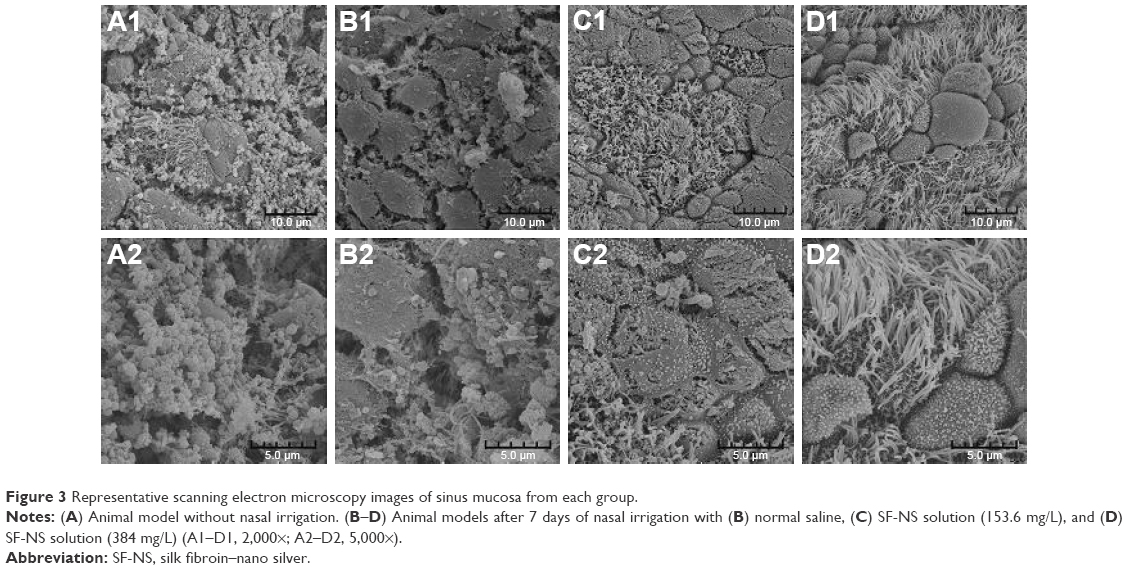 | Figure 3 Representative scanning electron microscopy images of sinus mucosa from each group. |
Quantitative analysis of bacterial biofilm revealed statistically significant between-group differences (Table 1). Although the bacterial biofilms on the sinus mucosa of the negative control group were reduced to a certain extent, statistical analysis showed that there was no significant difference in the range of biofilm involvement when compared with that in the blank control group. Although the bacterial biofilm involvement in the 153.6 mg/L SF-NS experimental group was significantly lower than that in blank control group, no significant difference was observed when compared with the saline group. However, the 384 mg/L SF-NS group showed the least biofilm involvement; the between-group difference with each of the other three groups was statistically significant.
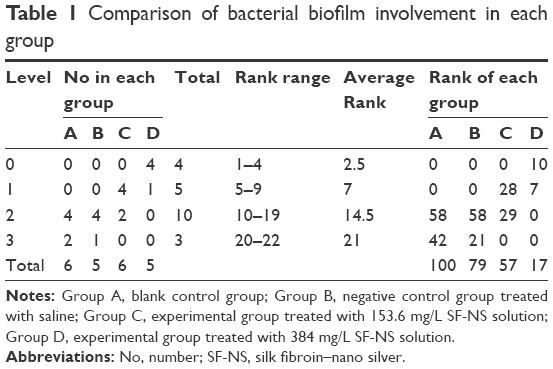 | Table 1 Comparison of bacterial biofilm involvement in each group |
Discussion
Topical nasal irrigation has been used for thousands of years for nasal health. The obvious advantage of topical administration is the higher local concentration of the therapeutic agent with minimal systemic side effects. In recent years, management of biofilm-associated CRS has largely been confined to topical administration of antimicrobials.24–27 This study evaluated the efficacy of SF-NS solution as a topical anti-biofilm agent in a rabbit model of sinusitis. The results showed that topical nasal irrigation, even with saline, has certain benefits in decreasing the biomass of the S. aureus biofilm in the sinuses of the rabbits.
However, although the saline irrigation is beneficial in reducing the microorganisms attached to the mucosal surface, yet a significant portion of the biofilms still persisted between the epithelial cells along with severe epithelial injury. This suggests that the saline might just remove the superficial and loose structure of the biofilms. This could be attributed to the lack of nutrients in the superficial layers of the biofilm, which results in fall off of the dead or dormant microorganisms. However, the viable biofilms located in deep sites or between the epithelial cells, which directly damaged the epithelium, were not eliminated by saline irrigation alone.
In vitro experiments found that SF-NS solution at 2× MBC level destroyed S. aureus biofilms partially, and when the concentration increased to 5× MBC, the biofilms were totally destroyed.19 Although in vitro and in vivo conditions are not the same, yet the purpose is the same, which is to observe biofilm-disrupting properties of SF-NS after direct contact with the biofilms. Hence, SF-NS solution was used at the concentrations of 153.6 and 384 mg/L (2× MBC and 5× MBC, respectively) as anti-biofilm agents in this study. Results showed that SF-NS solution at 2× MBC level is more effective in reducing the biofilm biomass when compared with saline. Although a small amount of biofilm still existed in some damaged epithelial cells, the injured epithelium exhibited signs of restoration, which indicated that it was the SF-NS component of the solution which acted against the biofilm and that the biofilm was not removed solely by the flushing action. This suggested that better results may be achieved if the duration of treatment is further extended.
Topical application of SF-NS solution at the 5× MBC level eliminated S. aureus biofilms in the sinuses of the rabbits after irrigation for 7 days. Furthermore, the integrity of epithelium had been recovered and most of the epithelial cells were normal with regeneration of cilia, which indicates that the repair of the epithelial cells had been in progress for some time.
The association of ciliary beat defect with CRS is well acknowledged. As noted in the experiment, a marked destruction of the sinonasal epithelium was observed with a complete absence of cilia, when the sinonasal mucosa was colonized by bacterial biofilms. Thus, as stated by Galli et al, biofilm formation represents the later phase of the inflammatory process that leads to complete epithelial destruction.28 The results of the present study clearly showed restoration of epithelium and cilia after treatment with SF-NS solutions. This can easily be considered as the consequence of biofilm removal by silver nanoparticles. Thus, although the mechanism of nasal epithelial restoration is still poorly understood, treatment of bacterial biofilms may be a key factor for ciliary recovery in biofilm-affected nasal mucosa. Although studies have found that silk fibroin has a role in promoting reepithelialization,29,30 the role of silk fibroin in epithelial restoration in this severe inflammatory condition needs to be studied further.
The antibacterial property of silver nanoparticles against a broad spectrum of bacteria has been increasingly used in various fields.31 Nonetheless, individual silver nanoparticles are easily oxidized and/or aggregated in air, which hampers their practical application.32 This study used green product SF-NS synthesized by the reaction of silk fibroin and silver nitrate, detailed information on which can be found in our previously published literature.19 The silk fibroin acted as a soluble template for biomineralization and the tyrosine residues in the silk fibroin backbone were thought to be responsible for the reduction of Ag+ into silver nanoparticles in situ. Silk fibroin is a natural nonionic surfactant that enhances the stability of silver nanoparticles in aqueous dispersion.33 Therefore, silk fibroin acts simultaneously as a reducing, dispersing, and stabilizing agent of the synthesized silver nanoparticles. In a previous study,19 it was found that synthesized SF-NS retained the antimicrobial properties of silver nanoparticles and could dissolve in water without aggregation, which makes it suitable for use as a solution for treatment. This study demonstrated that SF-NS solution is effective against mature biofilms formed by S. aureus in vivo in a concentration-dependent manner. Although 2× MBC and 5× MBC levels of SF-NS solutions showed no negative impact on the morphology of epithelial cells and cilia, for clinical use the other characteristics of silver nanoparticles still need to be considered, such as whether they can be easily taken up in the cells, and their potential toxic effects. Further studies will be carried out in the future to establish these facts.
Conclusion
SF-NS solution at concentrations of 153.6 and 384 mg/L was found to be an effective topical nasal antimicrobial agent, which reduced the biomass of S. aureus biofilms in the rabbit model of sinusitis. The clinical utility of SF-NS solution for patients with biofilm-associated CRS is yet to be determined. However, the anti-biofilm properties of SF-NS solution provide another option for future therapeutic interventions for biofilm-associated sinusitis.
Acknowledgments
The authors thank Huayong Liu, Institute of Medical Microbiology and Institutes of Biomedical Sciences, Shanghai Medical College, Fudan University for helping in bacteriological experiments, and Hongyang Gao, Electron Microscopy Center, Shanghai Medical College, Fudan University for helping in specimen preparation and photography.
This research was supported by National Natural Science Foundation of China (Grant No 81271094), Zhejiang Provincial Natural Science Foundation of China (Grant No LY17H130002), Wenzhou Public Welfare Science and Technology Project (Grant No Y20150270).
Disclosure
The authors report no conflicts of interest in this work.
References
Stewart PS, William Costerton J. Antibiotic resistance of bacteria in biofilms. Lancet. 2001;358(9276):135–138. | ||
Costerton JW, Stewart PS, Greenberg EP. Bacterial biofilms: a common cause of persistent infections. Science. 1999;284(5418):1318–1322. | ||
Chicurel M. Bacterial biofilms and infections. Slimebusters. Nature. 2000;408(6810):284–286. | ||
Perloff JR, Palmer JN. Evidence of bacterial biofilms on frontal recess stents in patients with chronic rhinosinusitis. Am J Rhinol. 2004;18(6):377–380. | ||
Ferguson BJ, Stolz DB. Demonstration of biofilm in human bacterial chronic rhinosinusitis. Am J Rhinol. 2005;19(5):452–457. | ||
Sanclement JA, Webster P, Thomas J, Ramadan HH. Bacterial biofilms in surgical specimens of patients with chronic rhinosinusitis. Laryngoscope. 2005;115(4):578–582. | ||
Psaltis AJ, Ha KR, Beule AG, Tan LW, Wormald PJ. Confocal scanning laser microscopy evidence of biofilms in patients with chronic rhinosinusitis. Laryngoscope. 2007;117(7):1302–1306. | ||
Oncel S, Pinar E, Sener G, Calli C, Karagoz U. Evaluation of bacterial biofilms in chronic rhinosinusitis. J Otolaryngol Head Neck Surg. 2010;39(1):52–55. | ||
Chen HH, Liu X, Ni C, et al. Bacterial biofilms in chronic rhinosinusitis and their relationship with inflammation severity. Auris Nasus Larynx. 2012;39(2):169–174. | ||
Tan NC, Tran HB, Foreman A, Jardeleza C, Vreugde S, Wormald PJ. Identifying intracellular Staphylococcus aureus in chronic rhinosinusitis: a direct comparison of techniques. Am J Rhinol Allergy. 2012;26(6):444–449. | ||
Wood AJ, Fraser JD, Swift S, Patterson-Emanuelson EA, Amirapu S, Douglas RG. Intramucosal bacterial microcolonies exist in chronic rhinosinusitis without inducing a local immune response. Am J Rhinol Allergy. 2012;26(4):265–270. | ||
Bendouah Z, Barbeau J, Hamad WA, Desrosiers M. Biofilm formation by Staphylococcus aureus and Pseudomonas aeruginosa is associated with an unfavorable evolution after surgery for chronic sinusitis and nasal polyposis. Otolaryngol Head Neck Surg. 2006;134(6):991–996. | ||
Psaltis AJ, Weitzel EK, Ha KR, Wormald PJ. The effect of bacterial biofilms on post-sinus surgical outcomes. Am J Rhinol. 2008;22(1):1–6. | ||
Foreman A, Psaltis AJ, Tan LW, Wormald PJ. Characterization of bacterial and fungal biofilms in chronic rhinosinusitis. Am J Rhinol Allergy. 2009;23(6):556–561. | ||
Foreman A, Wormald PJ. Different biofilms, different disease? A clinical outcomes study. Laryngoscope. 2010;120(8):1701–1706. | ||
Madeo J, Frieri M. Bacterial biofilms and chronic rhinosinusitis. Allergy Asthma Proc. 2013;34(4):335–341. | ||
Jervis-Bardy J, Foreman A, Bray S, Tan L, Wormald PJ. Methylglyoxal-infused honey mimics the anti-Staphylococcus aureus biofilm activity of manuka honey: potential implication in chronic rhinosinusitis. Laryngoscope. 2011;121(5):1104–1107. | ||
Singhal D, Foreman A, Jervis-Bardy J, Wormald PJ. Staphylococcus aureus biofilms: nemesis of endoscopic sinus surgery. Laryngoscope. 2011;121(7):1578–1583. | ||
Fei X, Jia M, Du X, et al. Green synthesis of silk fibroin-silver nanoparticle composites with effective antibacterial and biofilm-disrupting properties. Biomacromolecules. 2013;14(12):4483–4488. | ||
Jia M, Chen Z, Du X, Guo Y, Sun T, Zhao X. A simple animal model of Staphylococcus aureus biofilm in sinusitis. Am J Rhinol Allergy. 2014;28(2):e115–e119. | ||
Flemming K, Klingenberg C, Cavanagh JP, et al. High in vitro antimicrobial activity of synthetic antimicrobial peptidomimetics against staphylococcal biofilms. J Antimicrob Chemother. 2009;63(1):136–145. | ||
Kim Y, Wang X, Ma Q, Zhang XS, Wood TK. Toxin-antitoxin systems in Escherichia coli influence biofilm formation through YjgK (TabA) and fimbriae. J Bacteriol. 2009;191(4):1258–1267. | ||
Chiu AG, Antunes MB, Feldman M, Cohen NA. An animal model for the study of topical medications in sinusitis. Am J Rhinol. 2007;21(1):5–9. | ||
Desrosiers M, Myntti M, James G. Methods for removing bacterial biofilms: in vitro study using clinical chronic rhinosinusitis specimens. Am J Rhinol. 2007;21(5):527–532. | ||
Chiu AG, Palmer JN, Woodworth BA, et al. Baby shampoo nasal irrigations for the symptomatic post-functional endoscopic sinus surgery patient. Am J Rhinol. 2008;22(1):34–37. | ||
Le T, Psaltis A, Tan LW, Wormald PJ. The efficacy of topical antibiofilm agents in a sheep model of rhinosinusitis. Am J Rhinol. 2008;22(6):560–567. | ||
Singhal D, Jekle A, Debabov D, et al. Efficacy of NVC-422 against Staphylococcus aureus biofilms in a sheep biofilm model of sinusitis. Int Forum Allergy Rhinol. 2012;2(4):309–315. | ||
Galli J, Calo L, Ardito F, et al. Damage to ciliated epithelium in chronic rhinosinusitis: what is the role of bacterial biofilms? Ann Otol Rhinol Laryngol. 2008;117(12):902–908. | ||
Inouye K, Kurokawa M, Nishikawa S, Tsukada M. Use of Bombyx mori silk fibroin as a substratum for cultivation of animal cells. J Biochem Biophys Methods. 1998;37(3):159–164. | ||
Ni YS, Zhao X, Zhou L, et al. [Role of titanium mesh coated with silk fibroin in rabbit tracheal reconstruction]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2005;40(12):887–892. Chinese. | ||
Benn TM, Westerhoff P. Nanoparticle silver released into water from commercially available sock fabrics. Environ Sci Technol. 2008;42(11):4133–4139. | ||
Lok CN, Ho CM, Chen R, et al. Silver nanoparticles: partial oxidation and antibacterial activities. J Biol Inorg Chem. 2007;12(4):527–534. | ||
Kvitek L, Panáček A, Soukupova J, et al. Effect of surfactants and polymers on stability and antibacterial activity of silver nanoparticles (NPs). J Phys Chem C. 2008;112(15):5825–5834. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.