Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Efficacy of Psychosocial and Psychological Interventions in Addition to Drug Therapy to Improve Global Functioning of Inpatients with Schizophrenia Spectrum and Mood Disorders: A Real-World Observational Study
Authors Chiappini S ![]() , Di Carlo F, Mosca A, d'Andrea G, Di Paolo M, Lorenzini C, Lupica MG, Sampogna G, Pettorruso M, Fiorillo A, Martinotti G
, Di Carlo F, Mosca A, d'Andrea G, Di Paolo M, Lorenzini C, Lupica MG, Sampogna G, Pettorruso M, Fiorillo A, Martinotti G
Received 24 April 2023
Accepted for publication 21 July 2023
Published 30 August 2023 Volume 2023:19 Pages 1887—1897
DOI https://doi.org/10.2147/NDT.S418627
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Stefania Chiappini,1,2 Francesco Di Carlo,1 Alessio Mosca,1 Giacomo d’Andrea,1 Mariapia Di Paolo,1 Chiara Lorenzini,1 Maria Grazia Lupica,1 Gaia Sampogna,3 Mauro Pettorruso,1 Andrea Fiorillo,3 Giovanni Martinotti1,2
1Department of Neurosciences, Imaging and Clinical Sciences, ‘G. D’Annunzio’ University, Chieti, Italy; 2Psychopharmacology, Drug Misuse and Novel Psychoactive Substances Research Unit, School of Life and Medical Sciences, University of Hertfordshire, Hatfield, UK; 3Department of Psychiatry, University of Campania “L. Vanvitelli”, Naples, Italy
Correspondence: Stefania Chiappini, Department of Neurosciences, Imaging and Clinical Sciences, ‘G. D’Annunzio’ University, via dei Vestini, 31, Chieti (CH), 66100, Italy, Tel +393331698033, Email [email protected]
Introduction and Aim: Psychotic and mood disorders are associated with significant functional impairment, premature mortality, physical morbidity, and great social and economic burden. The aim of this study is to evaluate the effectiveness of psychosocial, psychological, and rehabilitative interventions implemented in an Italian psychiatric inpatient facility, with a focus on patients with schizophrenia spectrum versus those with mood disorders.
Methods: A retrospective observational study was conducted in the psychiatric hospital Villa Maria Pia in Rome, Italy, during 2022. Patients with an established diagnosis of schizophrenia spectrum and mood disorder (ICD-9-CM) were assessed on admission (T0) and at the end of treatment (T1), using the Brief Psychiatric Rating Scale (BPRS) and the Global Assessment of Functioning (GAF). Interventions involved a multidisciplinary team and included individual and group activities. The t-test for independent samples was used to compare continuous variables between groups and Spearman correlation coefficient to calculate correlations between variables.
Results: The study sample consisted of 141 patients, the majority of them being adults (51.3 years ± 12.4) men (F/M= 68/73). Among them, 85 patients (60.3%) actively engaged in psychosocial and rehabilitative interventions and, compared to non-participating individuals, they showed lower functioning and symptoms at discharge (delta GAF was significantly higher among patients who had taken part in the psychosocial activities, t = − 2.095; p = 0.038). Considering the index computed (n of interventions/days of hospitalization), the number of psychosocial activities was positively correlated with the improvement in patients’ functioning in the sample taking part in activities (r = 0.272, p = 0.012), especially with psychotherapy and support groups (r = 0.202, p = 0.017 and r = 0.188, p = 0.025, respectively). Splitting the total sample into schizophrenia-spectrum disorder (N = 37) and mood disorder (N = 48) groups, the positive correlations between GAF improvement and participation in psychosocial activities were confirmed only in the schizophrenia-spectrum group. These correlations were not significant for symptomatology (BPRS) either in the total or the individual group.
Conclusion: Evidence from our study suggests that inpatient rehabilitation can be effective and useful for people with severe mental disorders. Further investigations are needed to better understand its effectiveness on improving quality of life and social functioning in the long term.
Keywords: psychosis, schizophrenia, psychiatric rehabilitation, psychosocial intervention, mental health rehabilitation
Introduction
Mental disorders involve significant disturbances in thinking, emotional regulation, or behaviour and are usually associated with distress, impairment in important areas of functioning and risk of self-harm, contributing globally to disability, disproportionate health-care costs, and unemployment. A recent review estimates that the overall burden of mental illness accounts for 32.4% of the years lived with disability (YLD) and 13.0% of the disability-adjusted life years (DALYs), placing mental illness at the top of the global burden of disease in terms of YLDs and at the level of cardiovascular and circulatory diseases in terms of DALYs.1 Globally, major depressive disorder was among the five leading causes of YLDs in 2016.2
Among mental disorders, schizophrenia - and in general psychotic disorders – represent a major cause of disability worldwide. Estimates of the incidence of psychotic disorders vary according to demographic, geographical, and social characteristics;1 in fact, the World Health Survey (WHS) showed considerable heterogeneity among countries in the lifetime prevalence of schizophrenia (0.07%–5.7%).3 Prevalence estimates of psychosis obtained from studies with original data published between 1990 and 2015 found a median point prevalence of psychotic disorders of 3.89 per 1000 people among non-institutionalized persons.3 A recent systematic review and meta-analysis reported 21.7 per 100,000 person-years as the international incidence of psychotic disorders.4 The Global Burden of Disease Study estimated that globally 21 million people are living with schizophrenia, and this figure is set to continue to rise as the population ages and grows, particularly in middle-income countries.5 The early onset of the disorder, low remission rates, and high disability contribute to the excessive burden associated with this disorder.6 Psychotic disorders are associated with significant functional impairment, substantial premature mortality, physical morbidity such as heart disease, liver disease, and diabetes, and a large social and financial burden related to direct health-care expenditures and indirect costs such as lost productivity and caregiver burden.6–10 Psychosocial disability and withdrawal from relations are frequent prodromal signs of psychosis, exposing patients to long-term social exclusion, economic disadvantages, and reducing the effectiveness of available treatments.11 The effectiveness of pharmacological treatment strategies in schizophrenic patients might not be satisfactory to meet clinicians’ expectations due to persistent symptoms. They require pharmacological changes or modifications of the pharmacological strategy, such as the introduction of long-acting therapies or clozapine, to provide favorable improvement.12,13 Social and relational dysfunction is definitely a crucial aspect of schizophrenia, which, because of an approach to treatment mostly focused on positive symptoms than negative ones, may often be limitedly taken into account by clinicians.14
Similarly, mood disorders can impair normal functioning and adversely affect quality of life. In addition, patients with major depressive disorder and bipolar disorder show increased risk of developing obesity, metabolic syndrome, and cardiovascular disease, and in general higher morbidity and mortality, significantly worsening the therapeutic management and prognosis of affective disorders, due to greater treatment resistance, lower recovery rates, and worse course of illness.15 Assessing prevalence and burden estimates from the Global Burden of Disease study 2019, mental disorders accounted for 654.8 million estimated cases (95% UI 603.6–708.1) in 1990 and 970.1 million cases (900.9–1044.4) in 2019, corresponding to an increase of 48.1% between 1990 and 2019.16
The term “rehabilitation” has been used in mental health to describe a range of different approaches and interventions aimed at providing a recovery-orientated approach helping patients to progress from more intensive support to greater independence, to improve in functioning and quality of life through rehabilitation. The recent National Institute for Health and Care Excellence (NICE) guidelines recommend that rehabilitation services include community rehabilitation teams (residential care, supported housing and mobile care) in addition to rehabilitation pathway reserved for inpatients, such as high-dependency rehabilitation units and/or community rehabilitation units.17 Similarly, the American Psychiatric Association (APA) recommends that patients with schizophrenia be treated in a coordinated specialty care program in the context of a person-centered treatment plan, including evidence-based pharmacological and nonpharmacological treatments, the latter focusing on psychoeducation, psychosocial interventions, family interventions, social skills training, supportive psychotherapy, and assertive community treatments, especially if there is a history of poor engagement with services leading to frequent relapse or social disruption (eg, homelessness; legal difficulties, including imprisonment).18 Several psychosocial treatments have demonstrated efficacy during the acute and stable phase of schizophrenia. These include family intervention, supported employment, assertive treatment in the community, skills training, and cognitive-behavioral oriented psychotherapy.19 Similar to psychopharmacological management, the selection of psychosocial treatments must be individually tailored to the patient’s needs and preferences, to reduce hospitalizations and emergency room visits and enable a greater recovery. Thus, the selection of appropriate psychosocial treatments is guided by the circumstances of the individual patient’s needs and social context. For example, people with schizophrenia who present with residual psychotic symptoms while receiving appropriate pharmacotherapy may receive cognitive-behavioral oriented psychotherapy; interventions that educate family members about schizophrenia are needed to provide support and offer training in problem solving and effective communication, reduce symptom relapse, and help improve patient functioning and family well-being. Social skills training can be helpful in addressing functional problems related to social skills or activities of daily living. Group psychotherapeutic treatments can improve negative symptoms and social functioning deficits in the treatment of schizophrenia,20 eg, recovery-focused cognitive-behavioral interventions seem to be a promising treatment approach as they target disability from a broader perspective including activity and participation domains;21 group psychoeducation decreased the level of self-stigma and reduced perception of discrimination, assisting in recovery from schizophrenia.22
Treatment goals for patients with a psychiatric illness who also have a substance use disorder (SUD) are the same as those for the treatment of patients without comorbidities, but with the addition of goals for the treatment of SUD, eg, harm reduction, abstinence, relapse prevention, and rehabilitation. This form of treatment involves assertive outreach, case management, family interventions, housing, rehabilitation, and pharmacotherapy. It also includes behavioral interventions for those seeking to achieve or maintain abstinence and a staged motivational approach for patients who do not recognize the need for treatment.19
In this context, psychosocial interventions are supported by substantial evidence of efficacy in many outcome measures, and thus they should be considered as an evidence-based practice and need to become a part of the standard treatment of schizophrenia. Examining the recent literature on recovery in schizophrenia, Vita and Barlati23 argue that an integrated and multifaceted approach involving psychosocial interventions is effective and improves the treatment outcomes of disease. On this regard, the changes in the legislation on mental health care that took place in Italy through Law 180/1978, known as the Basaglia Law,24 which imposed the closure of asylums and regulated compulsory health treatment, establishing public Mental Health Services, with the intention of favoring therapies that were not detrimental to the dignity and quality of life of patients, have assumed an important role in the evolution of the morals and common sense of civil society in the country.
Information on the effects and effectiveness of non-pharmacological interventions, such as psychological, social, and family interventions, is currently limited in Italy. Existing literature on psychiatric rehabilitation is scarce and, to our knowledge, no specific evaluation has been carried out on psychosocial interventions and rehabilitation activities and techniques currently offered in Italian mental health settings. A previous survey limited to Northern Italy aimed to assess the type of activities implemented in Italy.25 Current psychosocial rehabilitation practices are highly variable in terms of methodology and content, with significant differences from one region to another, and even within the same region, depending on the specific orientation and tradition that characterizes regionally each Mental Health Department in Italy.
Therefore, the aim of this study is to evaluate the usefulness and effectiveness of psychosocial, psychological, and rehabilitative interventions implemented within a residential facility hosting psychiatric patients in Rome, with particular focus on patients with schizophrenia spectrum versus a mood disorder diagnosis.
Materials and Methods
Study Design
Data were collected in a retrospective observational study held in the inpatient psychiatric center of Villa Maria Pia in Rome, Italy, during the year 2022. The study focused on a total of 141 patients with an established diagnosis of schizophrenia spectrum or mood disorder according to the International Classification of Diseases (ICD-9-CM), which collects diagnoses and all diagnostic and therapeutic interventions by means of alphanumeric codes internationally recognised.26 Inclusion criteria were age between 18 and 65 years; a primary diagnosis of psychosis according to the ICD-9-CM (“schizophrenia and other functional psychoses”) or of a mood disorder, which was previously established; informed consent to participate in the study. Patients were enrolled while hospitalized. Patients recorded as comorbidly burdened with an alcohol use disorder (AUD)/SUD were also included.
Exclusion criteria were as follows: i) severe suicidal thoughts; ii) significant medical comorbidities, eg, acute respiratory/heart disease, cancer, severe infectious diseases, stroke, (cardio/cerebro) vascular diseases; iii) organic psychosis; iv) state of alcohol and substance intoxication and substance-induced psychosis; v) pregnancy; vi) a diagnosis of dementia or severe intellective disability.
Treatment Information
The clinical center is an intensive psychiatric treatment facility dedicated to post-acute patients, providing hospitalisation for 30 days, renewable up to a maximum of 60 days. Post-acute patients are patients with high care needs who require specific interventions aimed at stabilizing the clinical picture, following an acute episode of illness, for example, upon discharge from the hospital psychiatric diagnostic and treatment service (or in less severe cases than those admitted to the hospital, but who still require inpatient care); monitoring of drug treatment; setting of a medium- to long-term therapeutic program.
Apart from drug treatment, the non-pharmacological therapeutic interventions were chosen on the basis of a personalised treatment plan shared with patients, who could come from the psychiatric ward of the hospital for a post-acute period, or from community mental health centres. Interventions included both individual (eg, psychiatric interviews and psychotherapy) and group activities. In the present study, we focused on group activities addressed to patients, according to the Italian Informative System for Mental Health (Sistema Informativo per la Salute Mentale/SISM) classification.27 They included i) basic interpersonal individual/group skills training; ii) group expressive skills training; iii) motorial interventions; iv) practical-craft interventions; v) group psychotherapy and psychoeducation; and, if needed, vi) support groups for the rehabilitation of patients with a comorbid diagnosis of AUD/SUD. Two to four activities, lasting up to 2h each, were available for patients each day of treatment. They were organized on the basis of a specific schedule, known to patients from week to week. Three major groups of activities were here identified: i) Rehabilitation activities included basic interpersonal individual/group skills training; group expressive skills training; motorial interventions; and practical-craft interventions; ii) Psychotherapy activities included group psychotherapy and psychoeducation. Finally, iii) SUD activities included support groups for the rehabilitation of patients with a diagnosis of AUD/SUD.
Study Protocol
Demographic information including sex, age, marital status, psychiatric and organic diagnoses, pharmacological treatment, and eventual concomitant diagnoses, including SUD/behavioural addiction were recorded. Patients were evaluated at admission (T0) and at the end of hospitalization (T1), using the Brief Psychiatric Rating Scale (BPRS) and the Global Assessment of Functioning (GAF).
The interventions involved a multidisciplinary team (a psychiatrist, a psychologist, psychiatric rehabilitation technicians, and educators), adopting a biopsychosocial and person-centered approach that aimed to enable the person to gain skills for independent living and community integration.
Statistical Analysis
Descriptive statistics were expressed using mean ± standard deviation (SD) and median (range) for continuous variables, as appropriate, and n (%) for dichotomous and categorical variables. The t-test for independent samples was used to compare continuous variables between groups. Spearman correlation coefficient was used to calculate correlations between variables. Indexes were obtained by dividing the number of sessions of the different activities (eg, psychotherapeutic sessions, rehabilitation activities, and group activities) for the period of treatment (days). All statistical analyses were performed using SPSS Version 25 (SPSS Inc., Chicago, Illinois, USA). A two-sided p-value <0.05 was considered statistically significant.
Ethics
All eligible patients were asked to provide written informed consent to be evaluated following a detailed explanation of the nature, scope, and possible consequences of the study, and were informed of the possibility of withdrawing consent at any time. The study was conducted in accordance with the ethical principles stated in the Declaration of Helsinki and approved by the Ethic Committee of the Department of Neuroscience, Imaging, and Clinical Sciences of the University “G. d’Annunzio” of Chieti-Pescara. All personal data were anonymously extracted and identified using individual codes. Finally, both direct and indirect identifiers were removed.
Results
A total of 141 patients were included. The study sample consisted of a majority of adults (51.3 years ± 12.4), men (F/M= 68/73), diagnosed with a schizophrenia-spectrum disorder (n = 76, 53.9%) or a mood disorder (n = 65, 46.1%). A number of 39 subjects (27.7%) had a concomitant diagnosis, including a personality disorder (n = 18), a previous SUD (n = 16, including 7 related to cocaine, 4 related to cannabinoids, 2 related to opioids, 1 related to sedatives/hypnotics, and 2 related to other unclassified substances) or an AUD (n = 9), cognitive impairment (n = 3), adjustment disorder with mixed features (n = 1), and epilepsy (n = 1). Other sample characteristics are reported in Table 1.
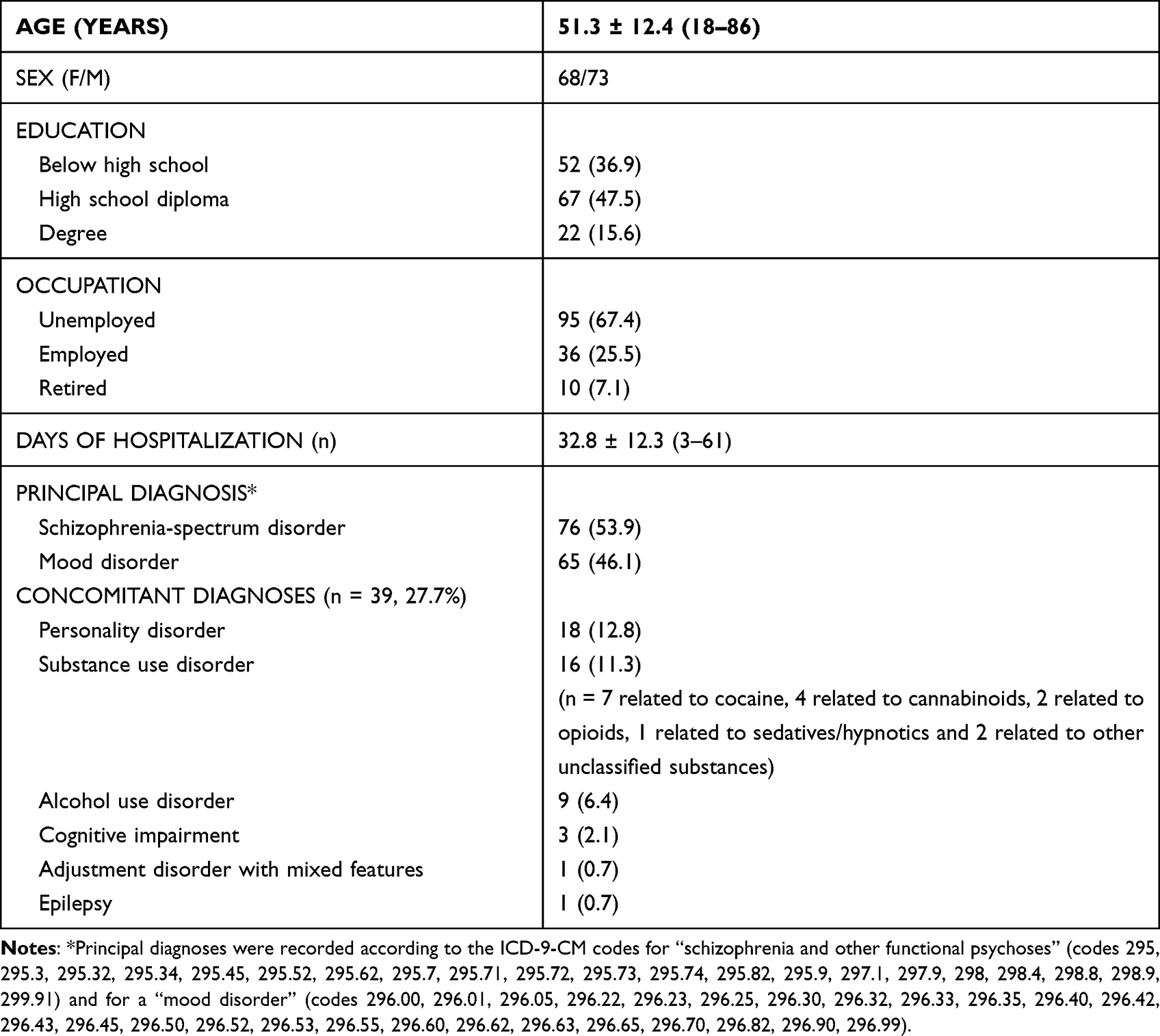 |
Table 1 Main Characteristics of the Sample (N = 141) |
In line with the objective of the study, the participants were divided into two groups, the first consisting of patients who attended at least one session of psychotherapy and one session of rehabilitative activity among those available, as well as those who attended at least two sessions of support group for AUD/SUD (Rehabilitative Activity Group), the second consisting of the remaining patients, excluded from the first group in view of low participation in activities. Thus, 85 patients (60.3%) actively engaged in psychosocial and rehabilitative interventions and were compared to non-participating individuals. Both functioning and symptoms at discharge were lower in the activity-participating group. Furthermore, the delta GAF between admission and discharge was significantly higher among patients who had taken part in the psychosocial activities (t = −2.095; p = 0.038) (see Table 2).
 |
Table 2 Differences in Functioning and Symptoms Among Patients Participating and Not in a Psychosocial Rehabilitation Program During Hospitalization |
Considering the index computed (n of interventions/days of hospitalisation), the emerging finding was that the number of psychosocial activities was positively correlated with the improvement in patients’ functioning (measured by the GAF) in the sample taking part in activities (r = 0.272, p = 0.012; Table 3). Considering the type of activities, both psychotherapy and support groups had a positive correlation with functional improvement (r = 0.202, p = 0.017 and r = 0.188, p = 0.025, respectively). Splitting the total sample into schizophrenia-spectrum disorder (n = 37) and mood disorder (n = 48) groups, the positive correlations between GAF improvement and participation in psychosocial activities were confirmed only in the schizophrenia-spectrum group (Table 3; Figure 1). These correlations were not significant for symptomatology (BPRS) either in the total or the individual groups (Table 2).
 |
Table 3 Index Computation in the Total Sample Participating in Rehabilitation and in the Two Groups of Patients with a Schizophrenia-Spectrum Disorder (N = 37) and a Mood Disorder (N = 48) |
 |
Figure 1 Correlation between index of psychosocial activities and change in functioning in patients participating in psychosocial rehabilitation interventions (N = 85). Index = n interventions/days of hospitalisation. Abbreviations: GAF, Global Assessment of Functioning; Index DELTA_GAF, difference between GAF score at discharge and at admission/days of hospitalisation. |
Patients diagnosed with schizophrenia spectrum disorder exhibited a lower rate of engagement in psychosocial activities compared to individuals with mood disorders (48.7% vs 73.8%). However, among the subset of patients who actively participated in psychosocial rehabilitation, no significant differences were observed, except for a younger age in the schizophrenic group (p = 0.001) (see Table 4). Group had lower functioning at discharge in comparison with patients diagnosed with mood disorder (GAF out 52.8 ± 8.0 versus 56.5 ± 9.0, t = −2.586, p = 0.011; Table 3). They also showed a lower participation in psychotherapy sessions and total number of psychosocial activities (t = −4.140, p < 0.001 and t = −2.905, p = 0.004, respectively).
 |
Table 4 Differences in Functioning and Symptoms Among Patients Diagnosed with a Schizophrenia Spectrum Disorder and a Mood Disorder at the Beginning and End of Hospitalisation (In/Out) |
Discussion
This is the first Italian study on a sample of inpatients with severe mental illness showing the effectiveness and usefulness of psychotherapy and rehabilitation interventions on the outcome of the disease in terms of functioning and symptomatology.
With regard to the sample, our findings showed consistency with previous Italian studies, where patients with severe mental illness were associated with unemployment, low educational level, and adult age (>45 years).28 Moreover, a high prevalence of comorbid AUD/SUD among schizophrenic and psychotic patients, with a rate of comorbidity assessed between 40% and 70%, is internationally recognized worldwide.29,30 Specifically, the recorded prevalence of SUD is 25.1% in patients with schizophrenia and 20.1% in those with bipolar disorder,31 confirming recent trends and socio-cultural changes, and evidence from the recent pandemic period. In Italy there are no recent and systematic epidemiological data regarding the rate of co-occurring disorders among people with SUD patients; a recent Italian study conducted in a rural area of Liguria Region has shown that patients with a psychiatric diagnosis and a SUD/AUD in drug abuse services are 24%.32 Data on the Italian population showed that in 2019 patients with SUD in treatment at drug services for comorbidity with a psychiatric disorder were 5.9%, of which 14.3% suffered from schizophrenia and related conditions, 0.9% from mania and bipolar disorders, and 3.1% from depression, and so on.33 Analyzing the frequency of comorbidities in the Veneto Region during 2019, in community mental health services the most prevalent SUDs were those related to the use of alcohol, polydrugs and cannabinoids, while in drug addiction services the most frequent SUDs were those related to the use of alcohol, opioids, and cocaine. Despite these differences, the most prevalent psychiatric disorders were equally represented by personality disorders, schizophrenia, and mood disorders in both cases.34
Based on our findings, rehabilitation activities, including groups for the treatment of SUD/AUD, showed efficacy in improving functioning in patients with schizophrenia-spectrum and mood disorder. Functioning (measured through GAF) and symptomatology (evaluated by BPRS) showed different results, as GAF improved in a significant way the more patients took part in activities. This finding appeared stronger when comparing the group of patients diagnosed with a schizophrenia spectrum disorder and the group with a mood disorder, the first one showing significant correlations between psychosocial activities and functional improvement despite having lower absolute GAF values at T1. However, symptomatology improvements did not appear to be related to psychosocial activities in the same way. Apparently, functioning and symptoms moved on different tracks with regard to the effectiveness of non-pharmacological activities, such as psychotherapeutic and rehabilitation groups, hypothetically showing that functioning improved, whereas the same did not happen with symptoms, which hypothetically respond predominantly to pharmacological treatment. Improved functioning in mood disorders, on the other hand, did not appear to be related to the number of psychosocial activities participated by the patients. This result could be related to contextual factors, eg, the severity of the illness in the two patient groups and the more severe course of schizophrenia spectrum disorders compared to mood disorders, resulting in a decline in personal functioning and individual resources. In this regard, the use of cognitive tests in the initial assessment of patients could be helpful. Likewise, tests that measure functioning and quality of life more specifically, but also as a self-assessment by the patients themselves, could be useful in the continuation of treatment and its monitoring.35
Based on our results, we do believe that rehabilitation activities and psychosocial interventions should be implemented and expanded from residential facilities to the community, developing a range of community-based mental health services involving both patients and family members.36 Indeed, clinical guidelines recommend an early and integrated approach, based on psychosocial and personalized interventions.14 The goals of long-term mental illnesses treatment are not only symptomatic and functional remission, but also a satisfying quality of life. In this regard, several unmet needs include difficulties at several clinical, psychosocial, relational, economic, and occupational levels.37 Health-care systems have not yet adequately responded to the needs of people with mental disorders and are significantly under-resourced.38 The gap between the need for care and its provision is wide throughout the world and the quality of care is often poor. For example, only 29% of people with psychosis and only one-third of people with depression receive formal mental health care.39 Psychosocial rehabilitation interventions might be an efficient tool to stimulate resocialization, interpersonal skills, functioning, and autonomy in a patient’s everyday life, bearing in mind that, regardless of their clinical severity, a patient’s areas of functioning can always be improved by therapeutic and rehabilitation work.40,41 Although psychiatric rehabilitation is sometimes considered a second-line treatment, intended as a generic and rough practice, consisting of extemporary actions and aimless entertainments designed to fill “the time passing”,42 activities and psychoeducation seem to be essential to support the patients both at the onset and at the chronic stage of the disease, promoting mental health.
Current challenges of mental health in Italy involve the implementation of services delivering integrated interventions in a person-centered treatment approach, which is not always available in real-world practice.42,43
Limitations
Limitations of the research methods include the observational nature of the study, the limited sample size, the length of the observation period that cannot consider the entire rehabilitation pathway needed, and the heterogeneity of the sample, which presented comorbidities with alcohol and substance abuse/personality disorders. Moreover, a further limitation might be the absence of self-evaluation by the patients themselves in terms of quality of life and treatment benefits, which could be taken into account in future studies. A final point to consider is the limited number of activities allowed in our center due to the CoronaVirus pandemic, which placed several restrictions regarding the possibility of group activities, to the entry of visitors or the exit of patients to external rehabilitation centers, to activities for family members (family counselling, psychoeducation, and others).
Conclusion
From our study, there is reasonable evidence to suggest that inpatient rehabilitation can be effective and useful for people with more complex mental health problems, enabling them to achieve a better outcome in terms of functioning. In severe conditions, such as mood disorders and schizophrenia, psychosocial and rehabilitation interventions should therefore be provided to them. In this regard, the field of research on mental health rehabilitation is heterogeneous and still lacking. Further investigations are needed to better understand the effectiveness and improvement of long-term quality of life and functioning.
Acknowledgments
We would like to thank the entire team (doctors, psychologists, rehabilitation technicians, social workers, and educators) at the inpatient psychiatric center Villa Maria Pia in Rome for the enormous work they carry out every day.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
Giovanni Martinotti has been a consultant and/or a speaker and/or has received research grants from Angelini, Doc Generici, Janssen-Cilag, Lundbeck, Otsuka, Pfizer, Servier, and Recordati. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationship that could be construed as a potential conflict of interest.
References
1. Vigo D, Thornicroft G, Atun R. Estimating the true global burden of mental illness. Lancet Psychiatry. 2016;3(2):171–178. doi:10.1016/S2215-0366(15)00505-2
2. GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016, Lancet. 2017;390(10100):1211–1259. Erratum in: Lancet. 2017 Oct 28;390(10106):e38. doi:10.1016/S0140-6736(17)32154-2
3. Nuevo R, Chatterji S, Verdes E, Naidoo N, Arango C, Ayuso-Mateos JL. The continuum of psychotic symptoms in the general population: a cross-national study. Schizophr Bull. 2012;38(3):475–485. doi:10.1093/schbul/sbq099
4. Moreno-Küstner B, Martín C, Pastor L. Prevalence of psychotic disorders and its association with methodological issues. A systematic review and meta-analyses. PLoS One. 2018;13(4):e0195687. doi:10.1371/journal.pone.0195687
5. Jongsma HE, Turner C, Kirkbride JB, Jones PB. International incidence of psychotic disorders, 2002–17: a systematic review and meta-analysis. Lancet Public Health. 2019;4(5):e229–e244. doi:10.1016/S2468-2667(19)30056-8
6. Charlson FJ, Ferrari AJ, Santomauro DF, et al. Global epidemiology and burden of schizophrenia: findings from the global burden of disease study 2016. Schizophr Bull. 2018;44(6):1195–1203. doi:10.1093/schbul/sby058
7. Hjorthøj C, Stürup AE, McGrath JJ, Nordentoft M. Years of potential life lost and life expectancy in schizophrenia: a systematic review and meta-analysis. Lancet Psychiatry. 2017;4(4):295–301. doi:10.1016/S2215-0366(17)30078-0
8. Hayes JF, Marston L, Walters K, King MB, Osborn DP. Mortality gap for people with bipolar disorder and schizophrenia: UK-based cohort study 2000–2014. Br J Psychiatry. 2017;211(3):175–181. doi:10.1192/bjp.bp.117.202606
9. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–1858. doi:10.1016/S0140-6736(18)32279-7
10. Jääskeläinen E, Juola P, Hirvonen N, et al. A systematic review and meta-analysis of recovery in schizophrenia. Schizophr Bull. 2013;39(6):1296–1306. doi:10.1093/schbul/sbs130
11. Fiorillo A. The complexity of vulnerability to psychosis. Epidemiol Psychiatr Sci. 2019;28(2):138–139. doi:10.1017/S2045796018000690
12. Kokurcan A, Güriz SO, Karadağ H, Erdi F, Örsel S. Treatment strategies in management of schizophrenia patients with persistent symptoms in daily practice: a retrospective study. Int J Psychiatry Clin Pract. 2021;25(3):238–244. doi:10.1080/13651501.2021.1879157
13. Kokurcan A. Comparison of clinical characteristics between the patients with schizophrenia on clozapine treatment with those taking combination of long-acting injectable and oral antipsychotics. Noro Psikiyatr Ars. 2019;56(3):219–223. doi:10.29399/npa.23548
14. Pompili M, Giordano G, Luciano M, et al. Unmet needs in Schizophrenia. CNS Neurol Disord Drug Targets. 2017;16(8):870–884. doi:10.2174/1871527316666170803143927
15. Colomer L, Anmella G, Vieta E, Grande I. Physical health in affective disorders: a narrative review of the literature. Braz J Psychiatry. 2021;43(6):621–630. doi:10.1590/1516-4446-2020-1246
16. GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry. 2022;9(2):137–150. doi:10.1016/S2215-0366(21)00395-3
17. NICE rehabilitation for adults with complex psychosis; 2020. Available from: https://www.nice.org.uk/guidance/ng181.
18. Keepers GA, Fochtmann LJ, Anzia JM, et al. The American Psychiatric Association practice guideline for the treatment of patients with schizophrenia. Am J Psychiatry. 2020;177(9):868–872. doi:10.1176/appi.ajp.2020.177901
19. Lehman AF, Lieberman JA, Dixon LB, et al.; American Psychiatric Association; Steering Committee on Practice Guidelines. Practice guideline for the treatment of patients with schizophrenia, second edition. Am J Psychiatry. 2004;161(2 Suppl):1–56. PMID: 15000267.
20. Orfanos S, Banks C, Priebe S. Are group psychotherapeutic treatments effective for patients with schizophrenia? A systematic review and meta-analysis. Psychother Psychosom. 2015;84(4):241–249. doi:10.1159/000377705
21. Nowak I, Sabariego C, Świtaj P, Anczewska M. Disability and recovery in schizophrenia: a systematic review of cognitive behavioral therapy interventions. BMC Psychiatry. 2016;16(1):228. doi:10.1186/s12888-016-0912-8
22. Vita A, Barlati S. Recovery from schizophrenia: is it possible? Curr Opin Psychiatry. 2018;31(3):246–255. doi:10.1097/YCO.0000000000000407
23. Basaglia F. La distruzione dell’ospedale psichiatrico come luogo di istituzionalizzazione [The destruction of the mental hospital as a place of institutionalisation]. Ann Neurol Psichiat. 1965;1:72.
24. Viganò C, Borghetti S, Casamenti R, et al. Indagine sulle attività riabilitative in Lombardia. Un progetto della Società Italiana di Riabilitazione Psicosociale, sezione regionale SIRP-Lo [Psychiatric rehabilitation patterns in Italy: Results from the Italian Society of Psychosocial Rehabilitation (SIRP) survey]. Errepiesse. 2012;2:3–17.
25. World Health Organization. Ministero del Lavoro, della Salute e delle Politiche Sociali. Classificazione Delle Malattie, Dei Traumatismi, Degli Interventi Chirurgici e Delle Procedure Diagnostiche e Terapeutiche- Versione Italiana Della ICD-9-CM “International Classification of Diseases - 9th revision - Clinical Modification” [International classification of diseases : [9th] ninth revision, basic tabulation list with alphabetic index; 1978]; 2007. Available from: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2251_allegato.pdf.
26. Ministero della Salute. Rapporto salute mentale. Analisi dei dati del Sistema Informativo per la Salute Mentale (SISM) anno 2016 [Italian Ministry of Health. Annuale report on mental health. Analysis of data from the Informative System for Mental Health (SISM); 2016]; 2016. Available from: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2731_allegato.pdf.
27. Altamura C, Fagiolini A, Galderisi S, Rocca P, Rossi A. Schizophrenia today: epidemiology, diagnosis, course and models of care. Ital J Psychopathol. 2014;20(3):223–243.
28. Hunt GE, Large MM, Cleary M, Lai HMX, Saunders JB. Prevalence of comorbid substance use in schizophrenia spectrum disorders in community and clinical settings, 1990–2017: systematic review and meta-analysis. Drug Alcohol Depend. 2018;191:234–258. doi:10.1016/j.drugalcdep.2018.07.011
29. Murthy P, Mahadevan J, Chand PK. Treatment of substance use disorders with co-occurring severe mental health disorders. Curr Opin Psychiatry. 2019;32(4):293–299. doi:10.1097/YCO.0000000000000510
30. Nesvag R, Knudsen GP, Bakken IJ, et al. Substance use disorders in schizophrenia, bipolar disorder, and depressive illness: a registry-based study. Soc Psychiatry Psychiatr Epidemiol. 2015;50(8):1267–1276. doi:10.1007/s00127-015-1025-2
31. Milano G, Vergani HM, Cattedra S, et al. Co-occurring psychiatric and substance use disorders: clinical survey among a rural cohort of Italian patients. Neuropsychiatr Dis Treat. 2019;15:3453–3459. doi:10.2147/NDT.S222567
32. Relazione annuale al Parlamento sul fenomeno delle tossicodipendenze in Italia anno 2021 (dati 2020) [Department for Anti-Drug Policies. Annual report drug abuse and addiction in Italy; 2021]; 2021. Available from: www.politicheantidroga.gov.it/media/3076/rap2021pdf.pdf.
33. Nava FA, Bassetti G, Bianco M, et al. Substance use disorders and psychiatric co-morbidity in the public healthcare services of Veneto Region. State of art and epidemiological data. MIS [Internet]; July 29, 2022. Available from: https://journals.francoangeli.it/index.php/mission-oa/article/view/12976.
34. Jaeschke K, Hanna F, Ali S, Chowdhary N, Dua T, Charlson F. Global estimates of service coverage for severe mental disorders: findings from the WHO Mental Health Atlas 2017. Glob Ment Health (Camb). 2021;8:e27. Erratum in: Glob Ment Health (Camb). 2021 Aug 03;8:e28. doi:10.1017/gmh.2021.19
35. Ercan Doğu S, Kokurcan A, Örsel S. An occupation-based healthy nutrition and wellness program for individuals with schizophrenia. OTJR (Thorofare N J). 2023;15394492231153113. doi:10.1177/15394492231153113
36. Fiorillo A, Luciano M, Del Vecchio V, Sampogna G, Obradors-Tarragó C, Maj M; ROAMER Consortium. Priorities for mental health research in Europe: a survey among national stakeholders’ associations within the ROAMER project. World Psychiatry. 2013;12(2):165–170. doi:10.1002/wps.20052
37. Mental health atlas 2020. Geneva: World Health Organization; 2021.
38. Moitra M, Santomauro D, Collins PY, et al. The global gap in treatment coverage for major depressive disorder in 84 countries from 2000–2019: a systematic review and Bayesian meta-regression analysis. PLoS Med. 2022;19(2):e1003901. doi:10.1371/journal.pmed.1003901
39. Franck N. Psychiatric rehabilitation in schizophrenia. Rev Prat. 2021;71(1):52–57.
40. Sociali A, Borgi M, Pettorruso M, et al. What role for cognitive remediation in the treatment of depressive symptoms? A superiority and noninferiority meta-analysis for clinicians. Depress Anxiety. 2022;39(7):586–606. doi:10.1002/da.23263
41. Viganò C, Ariu C, Barbieri D, et al.; SIRP Survey Group. Psychiatric rehabilitation patterns in Italy: results from the Italian Society of Psychosocial Rehabilitation (SIRP) survey. Front Psychiatry. 2023;14:1130811. doi:10.3389/fpsyt.2023.1130811
42. Vita A, Barlati S. The implementation of evidence-based psychiatric rehabilitation: challenges and opportunities for mental health services. Front Psychiatry. 2019;10:147. doi:10.3389/fpsyt.2019.00147
43. Galderisi S, Riva MA, Girardi P, et al. Schizophrenia and “unmet needs”: from diagnosis to care in Italy. Eur Psychiatry. 2020;63(1):e26. doi:10.1192/j.eurpsy.2019.8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.