Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Efficacy of Opportunistic Screening with Chest CT in Identifying Osteoporosis and Osteopenia in Patients with T2DM
Authors Xue C, Lu X, Sun G, Wang N, He G, Xu W, Xi Z, Xie L
Received 18 March 2024
Accepted for publication 8 May 2024
Published 27 May 2024 Volume 2024:17 Pages 2155—2163
DOI https://doi.org/10.2147/DMSO.S462065
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Antonio Brunetti
Congyang Xue,1 Xiaopei Lu,2 Guangda Sun,1 Nan Wang,1 Gansheng He,1 Wenqiang Xu,1 Zhipeng Xi,1 Lin Xie1
1Department of Spine Surgery, Affiliated Hospital of Integrated Traditional Chinese and Western Medicine, Nanjing University of Chinese Medicine, Nanjing, People’s Republic of China; 2Department of Traditional Chinese Medicine Surgery, Nanjing Hospital of Traditional Chinese Medicine, Nanjing University of Chinese Medicine, Nanjing, People’s Republic of China
Correspondence: Lin Xie, Department of Spine Surgery, Affiliated Hospital of Integrated Traditional Chinese and Western Medicine, Nanjing University of Chinese Medicine, 100th. Shizi Street, Nanjing, Jiangsu Province, 210028, People’s Republic of China, Email [email protected]
Purpose: To explore the validity of the thoracic spine Hounsfield Unit (HU) measured by chest computed tomography (CT) for opportunistic screening of diabetic osteoporosis. The current study attempted to establish a diagnostic threshold for thoracic spine HU in a type 2 diabetes mellitus (T2DM) population with osteoporosis.
Patients and Methods: The current study retrospectively included 334 patients with T2DM. They underwent chest CT and Dual-energy X-ray (DXA) between August 2021 and January 2022 in our hospital. HU values were measured on the resulting chest CT images at thoracic spine 11 and 12 to construct regions of interest. All patients were grouped according to the lowest T-value of DXA examination: osteoporosis, osteopenia and normal bone density. HU values were compared with T-values in each group of patients, and receiver operating characteristics curves were plotted to calculate diagnostic thresholds as well as sensitivity and specificity.
Results: There was a strong correlation between the HU values of chest CT and the T-values of DXA (p < 0.01). The sensitivity for osteoporosis was 88.7% for T11 attenuation≤ 98 HU and the specificity for osteoporosis was 87.5% for T12 attenuation ≤ 117HU; the specificity for normal BMD was 85.4% for T11 attenuation ≥ 147 HU and 82% for T12 attenuation ≥ 146 HU.
Conclusion: Chest CT can be used to screen patients with T2DM for opportunistic osteoporosis and help determine if they need DXA screening. The current study suggests that when the HU threshold of T11 ≤ 98/T12 ≤ 117, patients may need further osteoporosis screening.
Keywords: osteoporosis, T2DM, HU, thoracic vertebra, chest CT
Introduction
With the change of lifestyle, diabetes mellitus has become one of the most important diseases affecting people’s lives.1 Studies have shown that type 2 diabetes mellitus (T2DM) accounts for 90–95% of all diabetes mellitus.2 The number of persons with T2DM are far higher in China than in any other country. The age-standardized prevalence of diabetes mellitus was 9.6 per 1000 person-years for men and 9.2 per 1000 person-years for women.3 Osteoporosis is a chronic disease that is often overlooked and neglected.4,5 Patients frequently discover they have osteoporosis only after experiencing a fracture, which can lead to substantial financial losses. T2DM has been found to be one of the highest risks for the occurrence of fractures.6 T2DM predisposes 21.1% of cases to diabetic osteoporosis.7 However, the mechanism of its occurrence is complex and may be related to abnormal bone metabolism, deterioration of bone tissue microstructure, increased bone fragility, and the level of blood glucose control.8–11 Osteoporotic fractures have become one of the major complications of T2DM. Hence, early screening and prevention of diabetic osteoporosis are crucial.
Dual-energy X-ray (DXA) is now the gold standard in diagnosing osteoporosis.12 However, the values measured by DXA are high due to the effects of calcification of the vessel wall, hyperplasia of the articular eminence and degenerative bone spurs, resulting in false negatives.13 At the same time, T2DM patients have a larger BMI, which corresponds to a high area BMD, causing errors in DXA testing.14 Due to the numerous complications associated with T2DM, patients require a significant number of annual health screenings. However, the rate of regular DXA screening in T2DM patients is currently low. Therefore, finding a suitable method of opportunistic screening for T2DM can help physicians determine whether a patient should undergo further necessary osteoporosis investigations.
Chest CT is a widely used and extensively performed test in the clinic, and it is mostly used for screening of lung cancer and other lung diseases.15 Whereas vertebral HU values provided by CT images are valuable in the diagnosis of osteoporosis.16 Most of the previous studies on the correlation between HU values and osteoporosis have been conducted in non-diabetic patients, while mostly focusing on the L1 vertebrae, with few studies involving T2DM. The aim of this study was to discuss the relationship between HU values in the thoracic spine (T11, T12) and osteoporosis in T2DM and to derive the optimal HU thresholds for differentiating osteoporosis in T2DM.
Materials and Methods
Patients’ Population
Between August 2021 and January 2022, we recruited 411 cases of T2DM among individuals admitted to our Orthopedic and Endocrine Departments. The diagnosis of type 2 diabetes is determined based on the diagnostic criteria set by the American Diabetes Association.17 Inclusion criteria: (1) Age ≥18 years and type 2 diabetes mellitus; (2) Chest CT and DXA performed at our hospital. Exclusion criteria: (1) Patients with acute diabetic complications, inflammation or tumors; (2) Patients with severe heart failure, liver or renal impairment; (3) Patients with diseases affecting bone metabolism, such as hyperthyroidism, hypothyroidism, hyperparathyroidism, hypercortisolism, connective tissue disorders, and multiple myeloma. (4) Patients taking medications that affect bone metabolism, such as the use of glucocorticoids. (5) Lack of necessary data. A total of 344 patients (average age:59.3±12.5; male/female ratio: 1.9:1) were eventually included in the study (Figure 1).
 |
Figure 1 Patient inclusion/exclusion flow chart. Between August 2021 and January 2022, we recruited 411 cases of T2DM among individuals admitted to our Orthopedic and Endocrine Departments. The diagnosis of type 2 diabetes is determined based on the diagnostic criteria set by the American Diabetes Association. Inclusion criteria: (1) Age ≥18 years and type 2 diabetes mellitus; (2) Chest CT and DXA performed at our hospital. Exclusion criteria: (1) Patients with acute diabetic complications, inflammation or tumors; (2) Patients with severe heart failure, liver or renal impairment; (3) Patients with diseases affecting bone metabolism, such as hyperthyroidism, hypothyroidism, hyperparathyroidism, hypercortisolism, connective tissue disorders, and multiple myeloma. (4) Patients taking medications that affect bone metabolism, such as the use of glucocorticoids. (5) Lack of necessary data. A total of 344 patients were eventually included in the study. |
Ethical Considerations
The design of this study was approved by the Review Board of the Affiliated Hospital of Integrative Medicine of Nanjing University of Traditional Chinese Medicine (IRB No. 2022-LWKY-020). The Institutional Review Board waived the requirement for written informed consent from participants. Because the medical records used in this study were obtained from previous clinical consultations. Meanwhile, in order to protect the patients’ personal privacy, identity-sensitive information such as the name, address, and phone number of the subjects were not collected for this research study. We have maintained the confidentiality of patient information as required by law.
DXA & CT Data Acquisition
Dual-Energy X-Ray Absorptiometry
All patients underwent DXA at the lumbar spine (L1-L4) and hip. DXA measurements were performed at GE Medical Systems-LUNAR (Madison, WI, USA). Since both lumbar and hip DXA results were included, osteoporosis was diagnosed by the lower T-score on either lumbar or hip DXA. According to the criteria of the World Health Organization,18 osteoporosis was defined as T-score ≤ –2.5, osteopenia was defined as –2.5 < T-score ≤ –1.0, and normal BMD as T-score > –1.0.
CT Testing
Chest CT examinations were mainly done on the following two machines: GE 64-row 64-layer (Lightspeed VCT) CT or Neu soft Medical Systems Co. 64-row 128-layer (Neu Viz 128 Precision CT) CT. The patient was headfirst, and a CT scan of the chest was performed. The CT scanning parameters are as follows: Tube voltage, 120 kV; automatic milliampere-second technique tube current; collimation, 64×0.625 mm; pitch, 0.9 to 1; rotation time, 0.5 s; field of view, 500 mm. The CT scan data were transferred to the workstation and reconstructed with standard algorithms with a reconstruction layer thickness of 1.25 (GE VCT) and 1 mm (Neu Viz 128 CT), displaying a field of view of 380 mm. All chest CT examinations were performed without venography. The scanner is calibrated daily to ensure accurate vertebral CT attenuation numbers.19
HU values for the thoracic spine were measured from CT images.20 First, the sagittal position of the CT image was selected to determine the measurement position. Second, a region of interest (ROI) was drawn on the axial position of the corresponding vertebral body trabeculae to make it as large as possible, but excluding the vertebral cortical bone, surrounding venous plexus and trophoblastic foramen. Finally, the HU values of the near upper endplate, the middle, and the near lower endplate were measured separately and then averaged (Figure 2). All measurements were performed by a physician who was unaware of the DXA results. Another author randomized 20 patients for comparison of measurements.
 |
Figure 2 Schematic diagram of the measurement of HU values in the thoracic spine. Statistical analyses. HU values for the thoracic spine were measured from CT images. First, the sagittal position of the CT image was selected to determine the measurement position. Second, a region of interest (ROI) was drawn on the axial position of the corresponding vertebral body trabeculae to make it as large as possible, but excluding the vertebral cortical bone, surrounding venous plexus and trophoblastic foramen. Finally, the HU values of the near upper endplate, the middle, and the near lower endplate were measured separately and then averaged. |
Statistical analyses were performed using GraphPad prism 8.0 (GraphPad Software, USA). Continuous variables related to patients’ basic characteristics were described using mean and standard deviation; t-tests were used to compare whether there were differences between the basic characteristics and average HU values of osteoporotic and non-osteoporotic patients; The correlation between HU values and T values was analyzed using Pearson correlation.21 The area under the curve was calculated separately for each group using ROC curves, as well as sensitivity and specificity; The maximum value of the Jordon’s index was used to determine the optimal HU threshold. p ≤ 0.05 was statistically significant.
Results
A total of 344 patients with T2DM were enrolled in this study, and the basic information of all patients was listed in Table 1. Osteoporotic patients differed from non-osteoporotic patients in age, gender, BMI, T-score and HU values (p < 0.01). Classifying diabetic patients according to the lowest T-value, the prevalence of osteoporosis was found to be significantly higher in female (10.8%) than in male. Age and BMI were generally higher in female patients than in males, whereas T-scores and thoracic HUs were lower than in males.
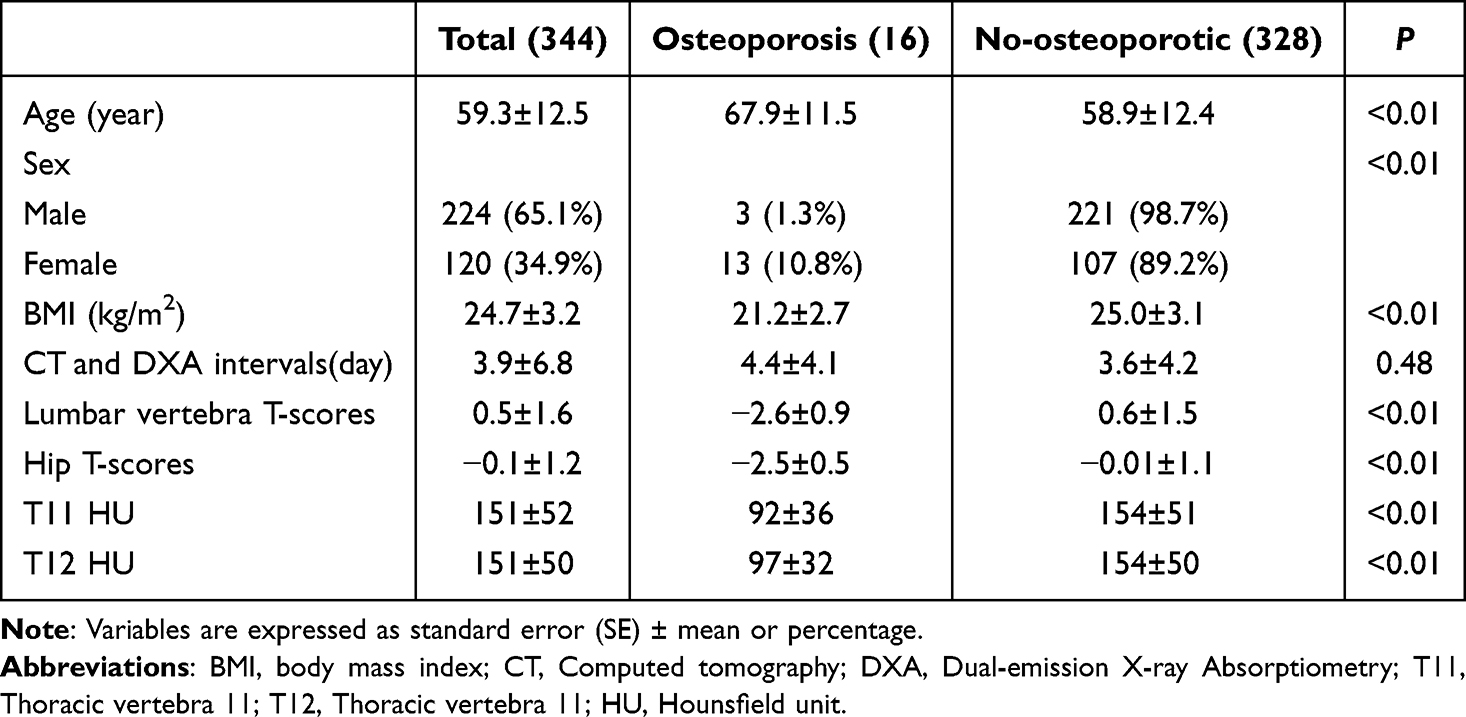 |
Table 1 Baseline Characteristics of the Study Population |
Thoracic Spine HU Values and DXA T-Score
Patients’ HU values were analyzed for person’s correlation with T values. The correlation between HU and T-values was found to be larger in the hip than in the lumbar spine; Meanwhile, the correlation between T11 attenuation and T-scores was greater than that of T12 attenuation (Table 2). The patients were grouped according to the lowest T-value in the osteoporosis, osteopenia and normal bone density. The scatter plot of their distribution is shown in Figure 3.
 |
Table 2 T-Scores and HU-Value Person Correlation Analysis |
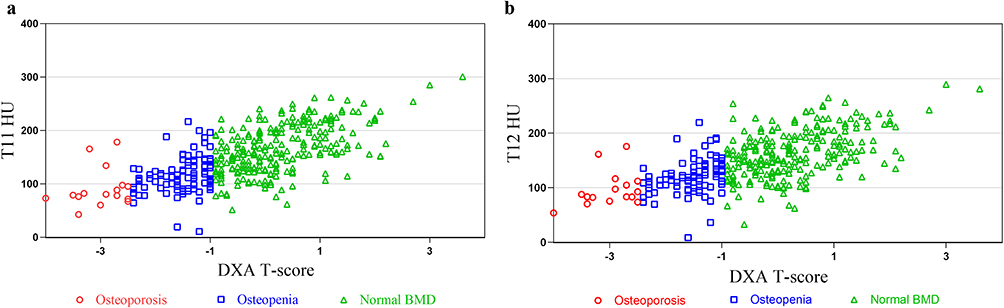 |
Figure 3 Scatter plot of the distribution of thoracic vertebra HU values and DXA T values. The patients were grouped according to the lowest T-value in the osteoporosis, osteopenia and normal bone density. (a) is a scatter plot of the distribution of T11 HU values and DXA T values; (b) is a scatter plot of the distribution of T12 HU values and DXA T values. |
Sensitivity and Specificity
We calculated HU values for T11 and T12 separately for the diagnostic threshold of osteoporosis (see Figures 4 and 5). Of these, the threshold of T11 attenuation values for distinguishing osteoporosis from non-osteoporosis was 98 (sensitivity 88.72%, specificity 81.25%, positive predictive values 25.5% and negative predictive values 99.0%). Threshold for distinguishing osteopenia from normal BMD is 147 (sensitivity 66.53%, specificity 85.39%, positive predictive values 92.5% and negative predictive values 69.6%). When HU scores of T11 was <98, 13 patients with osteoporosis were found in 50 patients; when HU scores of T11 was >147, 158 of 173 patients had normal BMD.
 |
Figure 4 ROC curves for T11 HU values; the area under the curve (AUC) of the ROC line for T11 distinguishing osteoporosis from non-osteoporosis was 0.86 (95% CI 0.752–0.968), with a HU value of 98; the AUC of the ROC line for T11 distinguishing reduced versus normal bone was 0.815 (95% CI 0.766–0.865), with a HU value was 147. The threshold of T11HU values for distinguishing osteoporosis from non-osteoporosis was 98 (sensitivity 88.72%, specificity 81.25%). Threshold for distinguishing osteopenia from normal BMD is 147 (sensitivity 66.53%, specificity 85.39%). When T11HU scores was <98, 13 patients with osteoporosis were found in 50 patients; when T11HU scores was >147, 158 of 173 patients had normal BMD. |
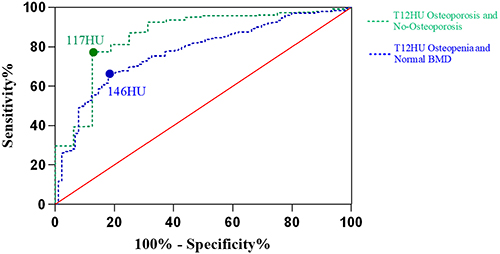 |
Figure 5 T12 HU value ROC curve; the AUC of the ROC line distinguishing osteoporosis from non-osteoporosis at T12 was 0.857 (95% CI 0.755–0.958), with a HU value of 117; the AUC of the ROC line distinguishing osteopenia from normal bone mass at T12 was 0.774 (95% CI 0.719–0.828), with a HU value was 146. The threshold for distinguishing osteoporosis from non-osteoporosis by T12 HU scores was 117 (sensitivity 77.44%, specificity 87.5%). The threshold for distinguishing osteopenia from normal BMD was 146 (sensitivity 60.32%, specificity 82.02%); When T12 HU <117, 14 patients with osteoporosis were found in 88 patients; when T12 HU >146, 157 of 175 patients had normal BMD. |
The threshold for distinguishing osteoporosis from non-osteoporosis by HU scores of T12 was 117 (sensitivity 77.44%, specificity 87.5%, positive predictive values 15.9% and negative predictive values 99.2%). The threshold for distinguishing osteopenia from normal BMD was 146 (sensitivity 60.32%, specificity 82.02%, positive predictive values 91.6% and negative predictive values 47.7%); When HU scores of T12 <117, 14 patients with osteoporosis were found in 88 patients; when HU scores of T12 >146, 157 of 175 patients had normal BMD.
Comparison with the HU thresholds obtained by Pickhardt (see Table 3). revealed that the HU values of the thoracic vertebrae were significantly more specific than the L1 in distinguishing osteoporosis from osteopenia, but slightly less sensitive; In contrast, T11 and T12 had better sensitivity and specificity than L1 in distinguishing HU values obtained from osteoporosis and non-osteoporosis.
 |
Table 3 The Study is Compared with Pickhardt’s Study |
Discussion
Our study found that opportunistic screening for osteoporosis occurrence in T2DM patients using chest CT is an effective method. At the same time, we established HU thresholds that are more suitable for the T2DM population, which is beneficial to help patients and physicians make decisions about whether to undergo further screening for DXA. Current studies find abdominal CT can be used as opportunistic screening for osteoporosis.13,22 However, few researchers have focused on chest CT. Simultaneously, researchers have mostly targeted their studies to the general population, with few studies focusing on diabetic patients.23 Nevertheless, the prevalence of T2DM in the population is increasing year by year,24 and the prevalence of diabetic osteoporosis is also increasing gradually.25 Meanwhile, the early stages of bone density loss in diabetic patients are asymptomatic. Whereas the diagnosis of osteoporosis is mostly established due to the first fracture.2 Therefore, early identification of the risk of osteoporosis in patients with T2DM is beneficial in reducing the probability of fracture in patients.
The prevalence of osteoporosis is significantly higher in women than in men, and the age of osteoporotic patients is significantly older than that of non-osteoporotic patients. We also found that male diabetic patients had significantly higher T-values and thoracic HUs than female patients. This may be related to the fact that menopause affects bone metabolism in women.26 The mean value of BMI for all patients is 24.7 kg/m2 which is overweight. Whereas the BMI of osteoporotic patients are significantly smaller than that of non-osteoporotic patients, which is within the normal range, and non-osteoporotic patients are overweight. This is consistent with previous studies suggesting that low body mass index is considered a risk factor for osteoporosis.27 The mean values of T11 and T12 HU were the same for the overall patients, which is different from previous studies that suggested a difference of 5 HU values between neighboring vertebrae.28 In contrast, the difference between T11 and T12 HU values in osteoporotic patients is 5 HU. It may be due to sample size differences.
Our study demonstrated a positive correlation between the HU values of the thoracic spine and the T-values of the DXA, indicating that the higher the HU value of the patient’s vertebrae, the better their bone condition. Although the study found greater correlation between thoracic spine HU and hip T-values, this study used the lowest T-values in the lumbar spine or hip to differentiate patients with osteoporosis and to reduce the study’s margin of error. The correlation between both T11 HU and T values was less than that of T12, which was considered to be due to the fact that T12 is located in the thoracolumbar segment of the thoracic spine, which experiences distinct forces compared to T11.
Our work proved that HU of T11 and T12 can excellently differentiate between osteoporotic and non-osteoporotic patients. It was found that HU values of CT may be more sensitive to increased bone fragility compared to DXA.29 Using the ROC curves, we derived HU values of 98 for T11 and 117 for T12 that distinguish osteoporosis from non-osteoporosis. The sensitivity of T11 HU (88.7%) was much higher than that of T12 HU (77.4%); Nonetheless, the specificity of T11 (81.3%) was lower than that of T12 (87.5%), which shows that the HU thresholds of T11 and T12 are each advantageous in the prediction of osteoporosis and non-osteoporosis. Buckens30 investigators collected data from 302 Dutch patients and obtained an optimal threshold of 104 for T12 to differentiate osteoporosis from osteopenia, with an AUC area of 0.74, a sensitivity of 62%, and a specificity of 79%, which is much smaller than the results we obtained. Considering that the study was collected from general patients while we collected from T2DM patients. Therefore, T2DM patients should have their own separate HU thresholds compared to the general population.
Jain29 collected 313 diabetic patients and found that the L1HU threshold was 135, which is significantly greater than the HU thresholds of T11 and T12 obtained in our study, which is the same as the L1 thresholds were greater than T11 and T12 in previous studies. In contrast, its AUC area was 0.73, and its specificity and sensitivity were 71% and 60%, which were much lower than our findings. Considering the thoracic spine HU values in diabetic patients may be superior to the lumbar spine for the diagnostic performance of osteoporosis.
For T2DM patients with reduced bone mass and normal bone density, our study obtained similar diagnostic thresholds for T11 and T12, 146 and 147 respectively. When the threshold for T11 was adjusted to 147, the sensitivity was reduced to 66.1% and the specificity was unchanged. The sensitivity of the diagnostic thresholds for T11 and T12 is less than the L1 threshold calculated by researchers such as Pickhardt31 and others. The diagnostic sensitivity of the thoracolumbar segment of the thoracic spine was poorer than that of the lumbar spine, but the diagnostic specificity of T11 and T12 was significantly better than the HU threshold of L1 Also, the AUC area of T11 (0.82) was greater than that of T12 (0.77) and L1 (0.8), considering that the higher the vertebrae the better its diagnostic performance may be.
There are limitations to this study. This is a retrospective study, we only analyzed T2DM patients in hospital with mostly poorly controlled blood glucose levels, therefore there is an effect of differences in blood glucose levels on osteoporosis and HU values, which needs to be studied prospectively; Secondly, this study excluded patients with fractures while including them, which may have reduced the prevalence of osteoporosis in the diabetic population while affecting the calculations. There are also some strengths in our research: The average time between CT and DXA examinations was 4 days, with the maximum interval not exceeding 14 days. It effectively reduces differences in test results due to health changes caused by time differences. Opportunistic screening for osteoporosis is facilitated by the widespread use of chest CT.
Conclusion
We established a correlation between thoracic spine HU values and T-values for DXA in patients with T2DM. We also established a thoracic spine HU threshold that can opportunistically predict osteoporosis in type 2 diabetic patients. It is recommended that radiologists include the results of HU values in chest CT reports so that clinicians can opportunistically screen patients for osteoporosis, leading to early detection, early treatment, and active prevention of fractures and related complications.
Ethics Approval
Approval for this study was obtained from the Affiliated Hospital of Integrated Traditional Chinese and Western Medicine, Nanjing University of Chinese Medicine (IRB number:2022-LWKY-020).
Acknowledgments
We would like to thank all the involved clinicians and technicians for their contribution to the study. We are grateful to all the participants for their dedication in data collection and laboratory measurements.
Funding
This study was funded by the Basic Research Program of Jiangsu Province (Natural Science Foundation) (NO. JD0335) and the Jiangsu Provincial Cadre Health Research Project (NO. BJ23020).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kaptoge S, Seshasai S, Sun L, et al. Life expectancy associated with different ages at diagnosis of type 2 diabetes in high-income countries: 23 million person-years of observation. Lancet Diabetes Endocrinol. 2023;11(10):731–742. doi:10.1016/S2213-8587(23)00223-1
2. Ye T, Lu L, Guo L, Liang M. Association between hemoglobin levels and osteoporosis in Chinese Patients with Type 2 diabetes mellitus: a cross-sectional study. Diabetes Metab Syndr Obes. 2022;15:2803–2811. doi:10.2147/DMSO.S382480
3. Zhang WL, Meng HZ, Yang RF, et al. Melatonin suppresses autophagy in type 2 diabetic osteoporosis. Oncotarget. 2016;7(32):52179–52194. doi:10.18632/oncotarget.10538
4. Abbouchie H, Raju N, Lamanna A, Chiang C, Kutaiba N. Screening for osteoporosis using L1 vertebral density on abdominal CT in an Australian population. Clin Radiol. 2022;77(7):e540–e548. doi:10.1016/j.crad.2022.04.002
5. Mazziotta C, Badiale G, Cervellera CF, Tognon M, Martini F, Rotondo JC. Regulatory mechanisms of circular RNAs during human mesenchymal stem cell osteogenic differentiation. Theranostics. 2024;14(1):143–158. doi:10.7150/thno.89066
6. Kurra S, Fink DA, Siris ES. Osteoporosis-associated fracture and diabetes. Endocrinol Metab Clin North Am. 2014;43(1):233–243. doi:10.1016/j.ecl.2013.09.004
7. Notarnicola A, Maccagnano G, Tafuri S, Moretti L, Laviola L, Moretti B. Epidemiology of diabetes mellitus in the fragility fracture population of a region of Southern Italy. J Biol Regul Homeost Agents. 2016;30(1):297–302.
8. Hao-hao S, Qing-wei J, Xin-huan Z, Yan W. Diagnostic value of dual energy X-ray absorptiometry and quantitative CT for osteoporosis in type 2 diabetes mellitus. Orthop J China. 2021;29(17):1579–1581.
9. Zhivodernikov IV, Kirichenko TV, Markina YV, Postnov AY, Markin AM. Molecular and cellular mechanisms of osteoporosis. Int J Mol Sci. 2023;24(21):15772. doi:10.3390/ijms242115772
10. Kim B, Cho YJ, Lim W. Osteoporosis therapies and their mechanisms of action (Review). Exp Ther Med. 2021;22(6):1379. doi:10.3892/etm.2021.10815
11. Li H, Xiao Z, Quarles LD, Li W. Osteoporosis: mechanism, molecular target and current status on drug development. Curr Med Chem. 2021;28(8):1489–1507. doi:10.2174/0929867327666200330142432
12. Gu Y, Otake Y, Uemura K, et al. Bone mineral density estimation from a plain X-ray image by learning decomposition into projections of bone-segmented computed tomography. Med Image Anal. 2023;90:102970. doi:10.1016/j.media.2023.102970
13. Huang CB, Hu JS, Tan K, Zhang W, Xu TH, Yang L. Application of machine learning model to predict osteoporosis based on abdominal computed tomography images of the psoas muscle: a retrospective study. BMC Geriatr. 2022;22(1):796.
14. Register TC, Lenchik L, Hsu FC, et al. Type 2 diabetes is not independently associated with spinal trabecular volumetric bone mineral density measured by QCT in the Diabetes Heart Study. Bone. 2006;39(3):628–633. doi:10.1016/j.bone.2006.03.003
15. Adams SJ, Stone E, Baldwin DR, Vliegenthart R, Lee P, Fintelmann FJ. Lung cancer screening. Lancet. 2023;401(10374):390–408. doi:10.1016/S0140-6736(22)01694-4
16. Sebro R, De la Garza-Ramos C. Opportunistic screening for osteoporosis and osteopenia from CT scans of the abdomen and pelvis using machine learning. Eur Radiol. 2023;33(3):1812–1823. doi:10.1007/s00330-022-09136-0
17. Chamberlain JJ, Rhinehart AS, Shaefer CJ, Neuman A. Diagnosis and management of diabetes: synopsis of the 2016 American diabetes association standards of medical care in diabetes. Ann Intern Med. 2016;164(8):542–552. doi:10.7326/M15-3016
18. Pai MV. Prevention and management of osteoporosis. World Health Organ Tech Rep Ser. 2003;921:1–164.
19. Park SY, Ha HI, Lee I, Lim HK. Comparison of HU histogram analysis and BMD for proximal femoral fragility fracture assessment: a retrospective single-center case-control study. Eur Radiol. 2022;32(3):1448–1455. doi:10.1007/s00330-021-08281-2
20. Kim YW, Kim JH, Yoon SH, et al. Vertebral bone attenuation on low-dose chest CT: quantitative volumetric analysis for bone fragility assessment. Osteoporos Int. 2017;28(1):329–338. doi:10.1007/s00198-016-3724-2
21. Mazziotta C, Pellielo G, Tognon M, Martini F, Rotondo JC. Significantly low levels of igg antibodies against oncogenic merkel cell polyomavirus in sera from females affected by spontaneous abortion. Front Microbiol. 2021;12:789991. doi:10.3389/fmicb.2021.789991
22. McNabb-Baltar J, Manickavasagan HR, Conwell DL, et al. A pilot study to assess opportunistic use of CT-scan for osteoporosis screening in chronic pancreatitis. Front Physiol. 2022;13:866945. doi:10.3389/fphys.2022.866945
23. Pinto EM, Neves JR, Teixeira A, et al. Efficacy of hounsfield units measured by lumbar computer tomography on bone density assessment: a systematic review. Spine. 2022;47(9):702–710. doi:10.1097/BRS.0000000000004211
24. Faizan M, Sarkar A, Singh MP. Type 2 diabetes mellitus augments Parkinson’s disease risk or the other way around: facts, challenges and future possibilities. Ageing Res Rev. 2022;81:101727. doi:10.1016/j.arr.2022.101727
25. Schwartz AV, Backlund JC, de Boer IH, et al. Risk factors for lower bone mineral density in older adults with type 1 diabetes: a cross-sectional study. Lancet Diabetes Endocrinol. 2022;10(7):509–518. doi:10.1016/S2213-8587(22)00103-6
26. Foessl I, Dimai HP, Obermayer-Pietsch B. Long-term and sequential treatment for osteoporosis. Nat Rev Endocrinol. 2023;19(9):520–533. doi:10.1038/s41574-023-00866-9
27. Zhang L, Luo X, Liu H, et al. Prevalence and risk factors of osteoporosis and osteopenia among residents in Hubei province, China. Arch Osteoporos. 2023;18(1):49. doi:10.1007/s11657-023-01245-7
28. Kobes T, Sweet A, Verstegen S, et al. Computed Tomography-Based L1 bone mineral density in 624 Dutch trauma patients-are north American reference values valid in Europe? J Pers Med. 2022;12(3):472. doi:10.3390/jpm12030472
29. Jain RK, Lee E, Mathai C, et al. Using opportunistic screening with abdominal CT to identify osteoporosis and osteopenia in patients with diabetes. Osteoporos Int. 2020;31(11):2189–2196. doi:10.1007/s00198-020-05521-x
30. Buckens CF, Dijkhuis G, de Keizer B, Verhaar HJ, de Jong PA. Opportunistic screening for osteoporosis on routine computed tomography? An external validation study. Eur Radiol. 2015;25(7):2074–2079. doi:10.1007/s00330-014-3584-0
31. Pickhardt PJ, Pooler BD, Lauder T, Del RA, Bruce RJ, Binkley N. Opportunistic screening for osteoporosis using abdominal computed tomography scans obtained for other indications. Ann Intern Med. 2013;158(8):588–595. doi:10.7326/0003-4819-158-8-201304160-00003
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.