")
Back to Journals » Infection and Drug Resistance » Volume 16
Efficacy of Nirmatrelvir-Ritonavir versus Azvudine for COVID-19 Treatment in Tibet: A Retrospective Study
Authors Zhao X , Cheng Y , Zhang M, Qianda B, Zhouma B, Yangzhen B, Zheng Y, Zhang S, Zhao H
Received 31 May 2023
Accepted for publication 1 September 2023
Published 11 September 2023 Volume 2023:16 Pages 6053—6060
DOI https://doi.org/10.2147/IDR.S423725
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi Ruan
Xiang Zhao,1 Yuan Cheng,1 Meng Zhang,1 Bianba Qianda,2 Baima Zhouma,3 Bianba Yangzhen,3 Yao Zheng,4 Shuo Zhang,5 Huiying Zhao6
1Department of Respiratory and Critical Care Medicine, Peking University First Hospital, Beijing, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, People’s Hospital of Tibet Autonomous Region, Lhasa, People’s Republic of China; 3Department of Tuberculosis, Third People’s Hospital of Tibet Autonomous Region, Lhasa, People’s Republic of China; 4Departments of Internal Medicine, Affiliated Hospital of Xizang Minzu University, Lhasa, People’s Republic of China; 5Department of Emergency Medicine, Peking University First Hospital, Beijing, People’s Republic of China; 6Department of Intensive Care Unit, Peking University People’s Hospital, Beijing, People’s Republic of China
Correspondence: Yuan Cheng, Department of Respiratory and Critical Care Medicine, Peking University First Hospital, Beijing, 100034, People’s Republic of China, Tel +86-13811659696, Fax +86-01083575753, Email [email protected]
Background: Nirmatrelvir-ritonavir, also known as paxlovid, is a widely used antiviral drug against coronavirus disease 2019 (COVID-19). Azvudine, a drug previously used to treat human immunodeficiency virus-1, has also been used to treat COVID-19 in China. However, only a few clinical studies have evaluated the effects of azvudine. Additionally, studies comparing nirmatrelvir-ritonavir with azvudine have been limited in number.
Methods: We carried out a retrospective case‒control analysis at the Third People’s Hospital of the Tibet Autonomous Region. Eighty-two eligible patients with COVID-19 who received azvudine treatment were included. A total of 145 control patients who received nirmatrelvir-ritonavir treatment were selected by propensity score matching for age, sex, the severity of disease, and initial cycle threshold values. A comparison of the nucleic acid test negative conversion time, the length of hospitalization, and mortality rate was conducted.
Results: Overall, the mean nucleic acid test negative conversion time was comparable between the nirmatrelvir-ritonavir and azvudine groups (7.0 [11.0, 15.0] vs 9.0 [6.0, 12.0] days, P=0.064). However, for patients with mild COVID-19, the nucleic acid test negative conversion time was significantly shorter in the nirmatrelvir-ritonavir group than in the azvudine group (6.0 [5.0, 8.0] vs 8.0 [6.0, 11.0] days, P=0.029). The nirmatrelvir-ritonavir group and the azvudine group did not differ significantly in length of hospitalization (8.0 [5.5,10.5] vs 8.0 [5.0,10.0] days, P=0.378). Regarding the mortality rate, there were 4 (2.8%) deaths in the nirmatrelvir-ritonavir group and 3 (3.7%) in the azvudine group (P=0.706).
Conclusion: Azvudine is generally as effective as nirmatrelvir-ritonavir, but for patients with mild COVID-19, nirmatrelvir-ritonavir could suppress the virus more rapidly. For those who cannot be treated with nirmatrelvir-ritonavir, azvudine might be an effective therapy for COVID-19.
Keywords: nirmatrelvir-ritonavir, azvudine, COVID-19, clinical outcome, high altitude
Introduction
Globally, coronavirus disease 2019 (COVID-19) continues to cause public health concerns, resulting in millions of deaths.1 The spread of COVID-19 has not yet been completely controlled. From 5 June to 2 July 2023, over885000new cases and over 4900 deaths were still reported worldly.2 With the emergence of novel and evolving SARS-CoV-2 variants, new vaccines and drugs are needed.3 Nirmatrelvir-ritonavir was granted Emergency Use Authorization for COVID-19 patients in December 2021 to fight the disease.4 Currently, many studies have indicated nirmatrelvir-ritonavir could reduce the risk of disease progression to severe COVID-19, the viral clearance time, and the length of hospitalization.5,6 Nevertheless, a few practical points still need to be noted regarding real world application of this drug. Despite being given as a short treatment course, drug‒drug interactions cause the most concern.7 Moreover, $530 for a 5-day session may not be affordable for all patients.8 Consequently, the development of novel small molecule antiviral drugs is urgently required.9
China experienced a COVID-19 outbreak in 2022, and the Omicron variant strain BA 2.76 was first detected in Tibet in August. Azvudine, as a conditionally approved drug to treat adult human immunodeficiency virus-1 patients with high viral loads, was authorized for the treatment of patients with COVID-19 on July 25, 2022.10,11 Experiments with monkeys demonstrated that azvudine could inhibit SARS-CoV-2 replication and that it had notable therapeutic efficacy in treating COVID-19.12 However, limited clinical trials have evaluated the effectiveness of azvudine in patients with COVID-19, and studies comparing the efficacy of nirmatrelvir-ritonavir and azvudine are also rare.
The objective of this study was to compare the efficacy of azvudine and nirmatrelvir-ritonavir in treating COVID-19 using a retrospective, propensity-matched analysis.
Methods
Study Population
This was a retrospective case‒control study performed at the Third People’s Hospital of the Tibet Autonomous Region (Lhasa, Tibet). We identified 731 patients with COVID-19 at the hospital between August 1, 2022 and September 30, 2022. Nasopharyngeal specimens were analyzed using real-time polymerase chain reaction (RT‒PCR) to diagnose SARS-CoV-2 infection.
Patients treated with only nirmatrelvir-ritonavir or azvudine as an antiviral agent were included in this study. The following were the exclusion criteria: 1) receiving other antiviral drugs; 2) an asymptomatic infection without any antiviral treatment; 3) age under 18 years; 4) pregnancy or lactation; 5) receiving nirmatrelvir-ritonavir or azvudine with an initial cycle threshold (Ct) value >35; and 6) transfer to another hospital or lack of data.
Furthermore, we matched patients in the nirmatrelvir-ritonavir and azvudine groups by propensity score matching (PSM) based on age, sex, the severity of disease, and initial Ct values. For each azvudine user, we selected the control with the closest propensity score (within 0.2 SD), and we paired them at a ratio of 1:2. As a result, the number of matching pairs determined the sample size.
The study was conducted in compliance with the principles of the Declaration of Helsinki and was approved by the ethical committee of the Third People’s Hospital of the Tibet Autonomous Region (ME-TBHP-23-03). All patients in the retrospective cohort study were anonymous, and the individual informed consent was not required. The Third People’s Hospital of the Tibet Autonomous Region specifically waived the requirement for informed consent.
Data Collection
The following baseline characteristics were assessed: age, sex, mean arterial pressure, body mass index, oxygen saturation, leukocyte count, lymphocyte count, and Ct value. Information about the previous history of chronic disease, vaccination status, number of vaccine doses administered, and COVID-19 infection-related symptoms were also individually collected at baseline. “Baseline” was defined as the date of admission. COVID‐19 severity status was classified as mild, common, severe, and critical according to the Chinese Diagnosis and Treatment Protocol for COVID-19 (Version 9)13 and the National Institutes of Health and expert consensus on the diagnosis and treatment of critically ill patients with COVID-19 at high altitudes in China.14 Mild symptoms without pneumonia on imaging were considered mild COVID-19. Clinical symptoms, pneumonia on computed tomography, and peripheral capillary oxygen saturation (SpO2) of >85% when breathing at rest were defined as common COVID-19. Pneumonia, SpO2 <85% when breathing air at rest, or arterial blood partial pressure of oxygen/fraction of breathed oxygen <192 mmHg was characterized as severe COVID-19. Shock or the requirement for mechanical ventilation was considered critical COVID-19.13,14
All assays were performed at the Department of Clinical Laboratory of the Third People’s Hospital of the Tibet Autonomous Region using standard methods.
Treatment
In the nirmatrelvir-ritonavir group, 300 mg of nirmatrelvir and 100 mg of ritonavir were administered every 12 hours for 5 days. In the azvudine group, 5 mg whole azvudine tablets were swallowed once every 24 hours for 7 days.13,14 In addition to antiviral therapy, all patients received routine treatment according to the guidelines and expert consensus for COVID-19.13,14
Study Outcomes
The primary outcome was nucleic acid test negative conversion time, characterized as two consecutive days of negative RT‒PCR results (Ct value ≥35 for ORF1ab and N genes). The secondary outcomes included the length of hospitalization and death. Negative nucleic acid test conversion and disease improvement were the criteria for discharge from the hospital.
Statistical Analysis
Data are presented as numerical values, mean ± standard deviation, or median (interquartile range). The Mann–Whitney U-test or the t-test was used to analyze continuous variables. The chi-square test was applied to categorical variables to compare differences between the two categories. We treated all missing information as missing data without imputed values. IBM SPSS Statistics for Windows, version 27 (IBM Corp., Armonk, N.Y., USA) was used to perform all analyses. A two‐tailed P‐value of <0.05 between the two groups was considered statistically significant.
Results
Baseline Characteristics
A total of 82 eligible patients with COVID-19 who received azvudine treatment were included in this study. A total of 145 controls who received nirmatrelvir-ritonavir treatment were selected by PSM for age, sex, the severity of disease, and initial Ct values (Figure 1). The baseline characteristics of the two groups are shown in Table 1. No significant differences in age, sex, Ct values, vaccination status, or symptoms before treatment were observed. Leukocyte levels were not significantly different in the nirmatrelvir-ritonavir and azvudine groups (4.8 [4.0,6.3] × 109/L vs 5.0 [4.0,6.1] × 109/L, P=0.933), but lymphocyte levels were significantly lower in the nirmatrelvir-ritonavir group (1.3 [0.9,1.6] × 109/L vs 1.6 [1.2,2.1] × 109/L, P=0.001). Oxygen saturation was lower in both groups with 88.0 [85.0, 90.0] % in the nirmatrelvir-ritonavir group and 89.0 [86.0, 91.0] % in the azvudine group (P=0.029).
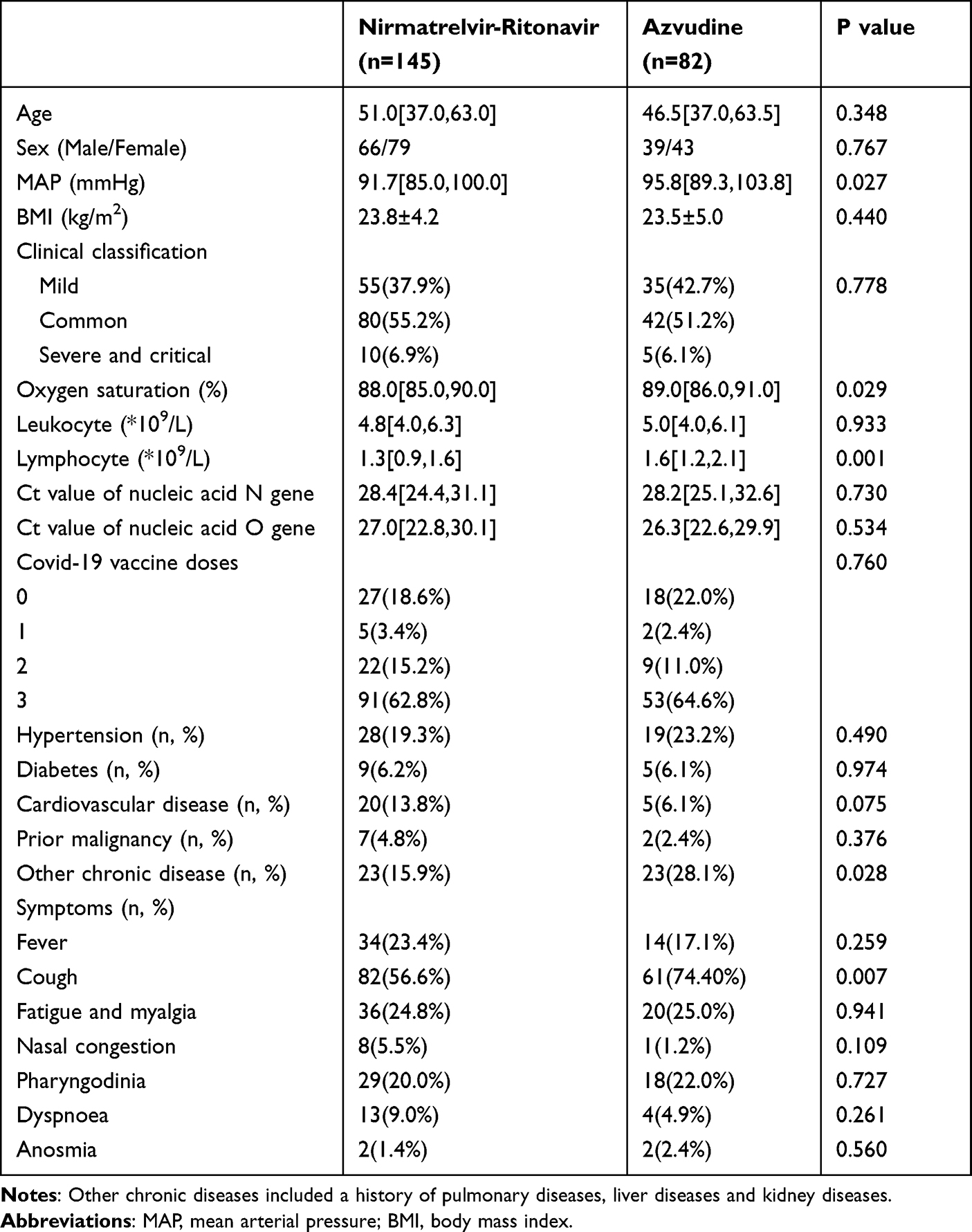 |
Table 1 Baseline Characteristics of Enrolled Patients After Propensity Score Matching |
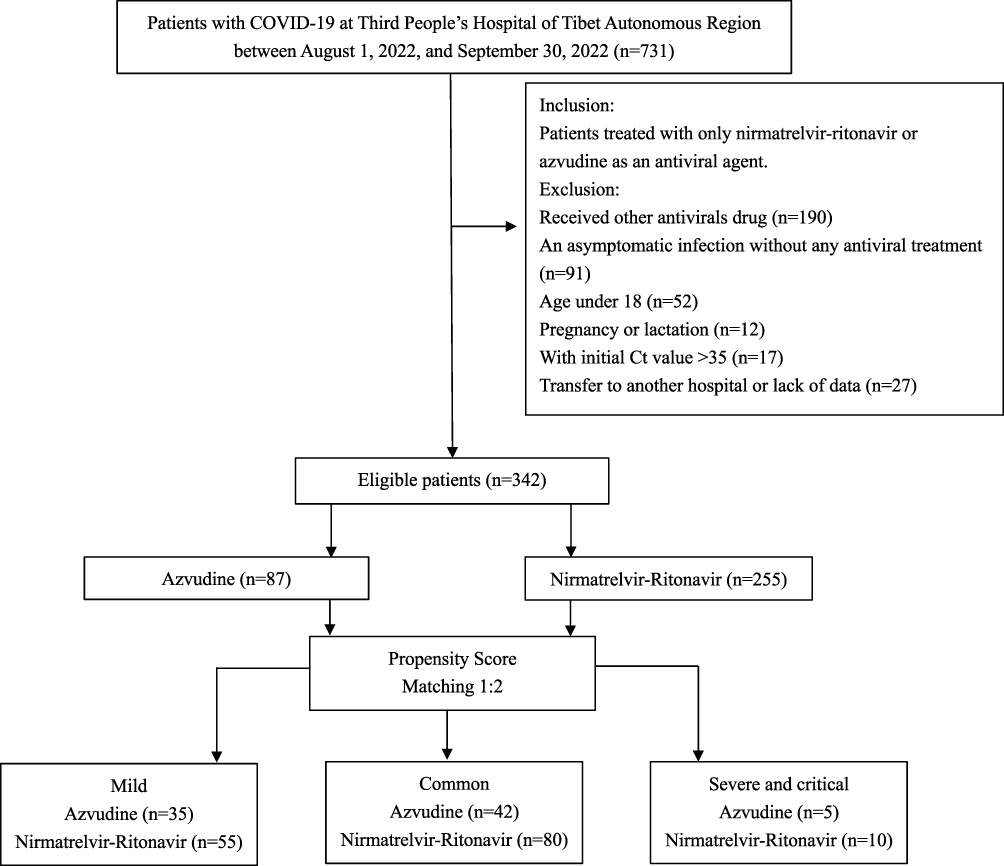 |
Figure 1 Study recruitment/inclusion flowchart. |
In addition, we divided the patients into three groups based on the severity of disease: mild, common, and severe/critical. The detailed characteristics of these groups are shown in Supplementary Tables 1-3. Statistically, there were no significant differences in age, sex, Ct value, or vaccination status between the groups; however, the nirmatrelvir-ritonavir group had lower lymphocyte counts than the azvudine group.
Outcomes
The primary and secondary outcomes are summarized in Table 2. In total, the mean SARS‐CoV‐2 negative conversion time was 7.0 [11.0, 15.0] days in the nirmatrelvir-ritonavir group and 9.0 [6.0, 12.0] days in the azvudine group. There was no significant difference between the two groups (P=0.064). However, compared with azvudine, the nirmatrelvir-ritonavir group had a significantly shorter SARS‐CoV‐2 negative conversion time for patients with mild COVID-19 (6.0 [5.0, 8.0] vs 8.0 [6.0, 11.0] days, P=0.029).
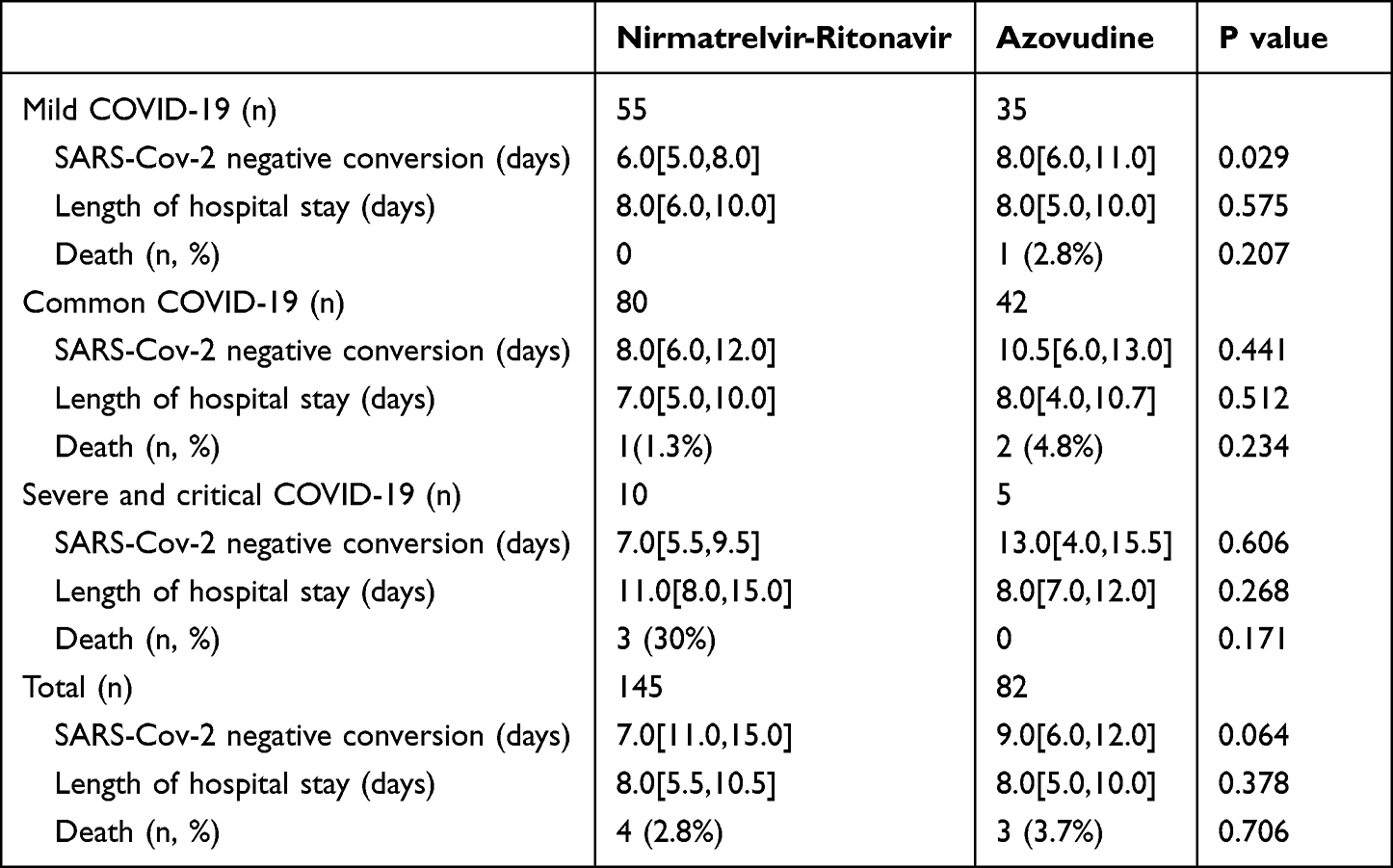 |
Table 2 Primary and Secondary Outcomes in the Nirmatrelvir-Ritonavir and Azvudine Groups |
The nirmatrelvir-ritonavir group and azvudine group exhibited no statistically significant difference in the length of hospitalization (8.0 [5.5,10.5] vs 8.0 [5.0,10.0] days, P=0.378). In addition, no significant difference was found in the length of hospitalization for patients with different disease severities.
Regarding the mortality rate, there were four (2.8%) deaths in the nirmatrelvir-ritonavir group, mainly in patients with severe and critical COVID-19, and three (3.7%) deaths in the azvudine group. This difference was not statistically significant (P=0.706).
Discussion
In the current study, we compared the antiviral effect of azvudine in patients with COVID-19 with matched historical controls who received nirmatrelvir-ritonavir. In general, the mean nucleic acid test negative conversion time was comparable between the nirmatrelvir-ritonavir and azvudine groups, but nirmatrelvir-ritonavir could suppress the virus more rapidly in patients with mild COVID-19. The length of hospitalization and mortality rate between the two groups were not significantly different. These findings suggest that azvudine might be an effective treatment for COVID-19 among patients who cannot receive nirmatrelvir-ritonavir.
RNA-dependent RNA polymerase (RdRp) and main protease (Mpro) are essential for viral replication by SARS CoV-2.15 Azvudine is a nucleoside analogue that inhibits human immunodeficiency virus-1 RdRp.11 It appears to be a relatively inexpensive (US $40 per course) and effective treatment.16 A small-sample randomized controlled clinical trial was conducted in China, and the results showed that azvudine could shorten the nucleic acid negative conversion time and help patients who have received other treatment regimens recover faster.17 Another study of 281 patients also confirmed that azvudine could shorten the time to nucleic acid conversion and the time to second negative nucleic acid conversion (6.7 days vs 9.40 days).18 Based on these results, azvudine is more effective than a placebo. However, few studies have compared the efficacy of nirmatrelvir-ritonavir to that of azvudine. The results from a single-center retrospective study in Beijing showed that nirmatrelvir-ritonavir could suppress the virus faster at the initial stage of hospitalization and had a shorter nucleic acid test negative conversion time than azvudine (days, 5.8 [95% CI, 4.7–7.4] vs 10.0 [95% CI, 8.2–11.7]).19 In our study, the mean SARS‐CoV‐2 negative conversion time was comparable between the nirmatrelvir-ritonavir and azvudine groups (7.0[11.0,15.0] vs 9.0[6.0,12.0] days). However, when we grouped the patients according to the severity of the disease the nirmatrelvir-ritonavir group had a shorter negative conversion time in patients with mild COVID-19 (6.0 [5.0, 8.0] vs 8.0 [6.0, 11.0] days, P=0.029). Unfortunately, we do not know the percentage of patients with mild infection in Gao et al’s study.
Another noteworthy point was that our research was carried out at an average altitude of 3500 m in Lhasa. Previous studies have shown that the infection and mortality rates in high-altitude areas were decreased when compared with low-altitude areas.20,21 This may be related to the lower expression level of angiotensin-converting enzyme 2 in high-altitude areas, which is a key entry receptor for SARS-CoV-2 in mediating acute lung injury and other organ injuries.22,23 In addition, our patients had a lower SPO2 at baseline than those in Gao et al’s study, which may be attributable to long-term high-altitude living and not to COVID-19.19 Consequently, the evaluation of patients with severe COVID-19 in our study may be affected. Therefore, we adopted the classification standards for plateaus based on Chinese guidelines and expert consensus, and SpO2 <85% was characterized as severe COVID-19.13,14 Ct values were also associated with disease severity and progression.24 Patients with severe and critical COVID-19 in our study had mean Ct values of approximately 25 (Supplementary Table 3), and the outcomes were similar for both groups. Overall, azvudine appears to play a role similar to that of nirmatrelvir-ritonavir among patients with severe infections. Interestingly, a recent study form Xiangya Hospital also suggested that azvudine might have a stronger protective effect on patients with severe COVID-19 who were not recommended to use nirmatrelvir-ritonavir and molnupiravir.25 More studies are needed to confirm these findings.
Compared to nirmatrelvir-ritonavir, azvudine has a different mechanism of antiviral action. The 4’-azide group of azvudine plays an important role in inhibiting SARS-CoV-2 RNA replication through intramolecular hydrogen bonds with the 3’-hydroxyl group, thereby reducing the nucleophilicity of the 3’-hydroxyl group.16 Further, after being phosphorylated in host cells, it is embedded into viral RNA during synthesis, thereby terminating RNA replication.11 Azvudine can also be concentrated largely in the thymus in its active form, inhibiting SARS-CoV-2 replication efficiently in vivo, preserving the immune function of the thymus, and rapidly curing patients with COVID-19.12 As the mechanism of action of azvudine is based on in vitro studies, further research is needed to elucidate its possible mechanisms against SARS-CoV-2 in patients.
There are several limitations to be considered in this study. First, although we matched the baseline data by PSM, this was a single-center retrospective study, making selection bias inevitable Moreover, owing to economic issues in Tibet, not all patients with a positive nucleic acid test were immediately admitted to the hospital, making it impossible to track and report changes in Ct values. In some patients, antiviral drugs were not taken at the onset of COVID-19, which may have affected the results. It is necessary to conduct randomized controlled trials in the future to verify these results.
Conclusions
The antiviral effect was comparable between the nirmatrelvir-ritonavir and azvudine groups, but nirmatrelvir-ritonavir could suppress the virus more rapidly in patients with mild COVID-19. These findings suggest that azvudine might be an effective treatment for COVID-19 in patients who cannot receive nirmatrelvir-ritonavir.
Data Sharing Statement
The data that support the findings of this study are available upon reasonable request from the corresponding author.
Patient Consent Statement
The research on patients was approved by the Third People’s Hospital of the Tibet Autonomous Region Clinical Research Ethics Committee, approval number ME-TBHP-23-03. All patients in the retrospective cohort study were anonymous, and the individual informed consent was not required. The Third People’s Hospital of the Tibet Autonomous Region specifically waived the requirement for informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all the following areas; took part in drafting, revised or critically reviewed the article; approved final version of the manuscript; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was supported by the Beijing Natural Science Foundation (L222151), Beijing CSCO Clinical Oncology Research Foundation (Y-HS202202-0073), and Beijing Health Science and Technology Achievements and Appropriate Technology Promotion Project (BHTPP2022085).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Steele MK, Couture A, Reed C, et al. Estimated Number of COVID-19 Infections, Hospitalizations, and Deaths Prevented Among Vaccinated Persons in the US, December 2020 to September 2021. JAMA Netw Open. 2022;5(7):e2220385. doi:10.1001/jamanetworkopen.2022.20385
2. Weekly epidemiological update on COVID-19 - 27 April 2023. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---27-april-2023.
3. Fernandes Q, Inchakalody VP, Merhi M, et al. Emerging COVID-19 variants and their impact on SARS-CoV-2 diagnosis, therapeutics and vaccines. Ann Med. 2022;54(1):524–540. doi:10.1080/07853890.2022.2031274
4. Najjar-Debbiny R, Gronich N, Weber G, et al. Effectiveness of Paxlovid in Reducing Severe Coronavirus Disease 2019 and Mortality in High-Risk Patients. Clin Infect Dis. 2023;76(3):e342–e349. doi:10.1093/cid/ciac443
5. Hammond J, Leister-Tebbe H, Gardner A, et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with Covid-19. N Engl J Med. 2022;386(15):1397–1408. doi:10.1056/NEJMoa2118542
6. Wang Y, Zhao D, Chen X, Liu X, Xiao W, Feng L. The effect of nirmatrelvir-ritonavir on viral clearance and length of hospital stay in patients infected with SARS-CoV-2 omicron variants. Influenza Other Respir Viruses. 2023;17(2):e13095. doi:10.1111/irv.13095
7. Marzolini C, Kuritzkes DR, Marra F, et al. Recommendations for the Management of Drug-Drug Interactions Between the COVID-19 Antiviral Nirmatrelvir/Ritonavir (Paxlovid) and Comedications. Clin Pharmacol Ther. 2022;112(6):1191–1200. doi:10.1002/cpt.2646
8. Beasley D. Price of COVID treatments from Pfizer, Merck, GSK align with patient benefits-report. Reuters Healthc Pharmaceuticals. 2022:56.
9. Lee CYS, Suzuki JB. COVID-19: variants, immunity, and therapeutics for non-hospitalized patients. Biomedicines. 2023;11(7):2055. doi:10.3390/biomedicines11072055
10. Yu B, Chang J. The first Chinese oral anti-COVID-19 drug Azvudine launched. Innovation. 2022;3(6):100321. doi:10.1016/j.xinn.2022.100321
11. Yu B, Chang J. Azvudine (FNC): a promising clinical candidate for COVID-19 treatment. Signal Transduct Target Ther. 2020;5(1):236. doi:10.1038/s41392-020-00351-z
12. Zhang JL, Li YH, Wang LL, et al. Azvudine is a thymus-homing anti-SARS-CoV-2 drug effective in treating COVID-19 patients. Signal Transduct Target Ther. 2021;6(1):414. doi:10.1038/s41392-021-00835-6
13. National Health Commission of the People’s Republic of China. Diagnosis and treatment plan for COVID-19 (trial version 9. Int J Epidemiol Infect Dis. 2022;49:73–80.
14. Shang Y, Pan C, Yang X. Expert Consensus on the Diagnosis and Treatment of Critically Ill Patients with COVID-19 at High Altitudes in China. Chin J Crit Care Intensive Care Med. 2020;1–7.
15. Lei S, Chen X, Wu J, Duan X, Men K. Small molecules in the treatment of COVID-19. Signal Transduct Target Ther. 2022;7(1):387. doi:10.1038/s41392-022-01249-8
16. Yang L, Wang Z. Bench-to-bedside: innovation of small molecule anti-SARS-CoV-2 drugs in China. Eur J Med Chem. 2023;257:115503. doi:10.1016/j.ejmech.2023.115503
17. Ren Z, Luo H, Yu Z, et al. A Randomized, Open-Label, Controlled Clinical Trial of Azvudine Tablets in the Treatment of Mild and Common COVID-19, a Pilot Study. Adv Sci. 2020;7(19):e2001435. doi:10.1002/advs.202001435
18. da Silva RM, Abreu Cabral P G, de Souza SB, et al. Serial viral load analysis by DDPCR to evaluate FNC efficacy and safety in the treatment of mild cases of COVID-19. Front Med. 2023;10:1143485. doi:10.3389/fmed.2023.1143485
19. Gao Y, Luo Z, Ren S, et al. Antiviral effect of azvudine and nirmatrelvir-ritonavir among hospitalized patients with COVID-19. J Infect. 2023;86(6):e158–e160. doi:10.1016/j.jinf.2023.03.023
20. Segovia-Juarez J, Castagnetto JM, Gonzales GF. High altitude reduces infection rate of COVID-19 but not case-fatality rate. Respir Physiol Neurobiol. 2020;281:103494. doi:10.1016/j.resp.2020.103494
21. Arias-Reyes C, Carvajal-Rodriguez F, Poma-Machicao L, et al. Decreased incidence, virus transmission capacity, and severity of COVID-19 at altitude on the American continent. PLoS One. 2021;16(3):e0237294. doi:10.1371/journal.pone.0237294
22. Liu M, Wang T, Zhou Y, Zhao Y, Zhang Y, Li J. Potential Role of ACE2 in Coronavirus Disease 2019 (COVID-19) Prevention and Management. J Transl Int Med. 2020;8(1):9–19. doi:10.2478/jtim-2020-0003
23. Stephens KE, Chernyavskiy P, Bruns DR. Impact of altitude on COVID-19 infection and death in the United States: a modeling and observational study. PLoS One. 2021;16(1):e0245055. doi:10.1371/journal.pone.0245055
24. Zheng S, Fan J, Yu F, et al. Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in Zhejiang province, China, January-March 2020: retrospective cohort study. BMJ. 2020;369:m1443. doi:10.1136/bmj.m1443
25. Sun Y, Jin L, Dian Y, et al. Oral Azvudine for hospitalised patients with COVID-19 and pre-existing conditions: a retrospective cohort study. EClinicalMedicine. 2023;59:101981. doi:10.1016/j.eclinm.2023.101981
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.