Back to Journals » International Journal of General Medicine » Volume 19
Efficacy of Intestinal Obstruction Catheter Combined with Modified Dachengqi Decoction in Elderly Patients with Early Postoperative Inflammatory Intestinal Obstruction: A Randomised Study
Authors Liu J, Zhong Y, Deng Q, Peng Y, Wang X, Long C, Ji Y, Duan C
Received 2 March 2026
Accepted for publication 27 May 2026
Published 3 June 2026 Volume 2026:19 604394
DOI https://doi.org/10.2147/IJGM.S604394
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Gopal Krishna Dhali
Jiusi Liu,1 Yuzhen Zhong,2 Qiliang Deng,3 Yanping Peng,4 Xiong Wang,1 Chaohui Long,5 Youjun Ji,2 Caihua Duan3
1Department of Gastrointestinal Surgery, Ji’an Central People’s Hospital, Ji’an, Jiangxi, 343000, People’s Republic of China; 2School of Clinical Medicine, Jinggangshan University, Ji’an, Jiangxi, 343009, People’s Republic of China; 3Department of Gastroenterology, Ji’an Central People’s Hospital, Ji’an, Jiangxi, 343000, People’s Republic of China; 4Department of Traditional Chinese Medicine, Ji’an Central People’s Hospital, Ji’an, Jiangxi, 343000, People’s Republic of China; 5Department of Proctology, Ji’an Central People’s Hospital, Ji’an, Jiangxi, 343000, People’s Republic of China
Correspondence: Caihua Duan, Department of Gastroenterology, Ji’an Central People’s Hospital, Ji’an, Jiangxi, 343000, People’s Republic of China, Email [email protected]
Objective: This study aimed to evaluate the efficacy of a combined therapy integrating a nasointestinal decompression catheter with a modified Dachengqi Decoction (mDQD) for elderly patients diagnosed with early postoperative inflammatory intestinal obstruction (EPIIO) following gastrointestinal emergency surgery.
Methods: We conducted a prospective, randomized controlled trial involving 62 elderly EPIIO patients. Participants were randomly assigned to an experimental group (n=31) or a conventional group (n=31). Both groups received standard nasointestinal catheter decompression and conventional Western medical therapy. The experimental group received additional treatment with mDQD administered through the catheter. Outcomes included recovery times (symptom resolution, first flatus, hospital stay), inflammatory markers (white blood cell count, C‑reactive protein, interleukin‑6), and intestinal barrier function (D‑lactate, diamine oxidase), measured before treatment and at 7 and 14 days post‑treatment.
Results: The experimental group showed statistically significant improvements in several recovery metrics, including shorter time to symptom resolution, first flatus, and hospital discharge, compared with the conventional group (all P < 0.05). In addition, the experimental group had greater reductions in systemic inflammatory markers and better restoration of intestinal barrier function at days 7 and 14 (P < 0.05). No major adverse events were reported in either group.
Conclusion: The combined therapy of an intestinal obstruction catheter and modified Dachengqi Decoction was associated with improved recovery outcomes in elderly patients with early postoperative inflammatory intestinal obstruction, including reduced inflammation and enhanced intestinal barrier function. However, these findings should be interpreted with caution owing to the small sample size and single‑center design. Larger, multicenter randomized trials are needed to confirm the efficacy of this integrated approach.
Keywords: inflammatory intestinal obstruction, elderly patients, Dachengqi Decoction, intestinal obstruction catheter, nutrition
A Letter to the Editor has been published for this article.
Introduction
Early postoperative inflammatory intestinal obstruction (EPIIO) is a common complication after gastrointestinal emergency surgery, particularly in elderly patients.1,2 In this population, the condition is associated with higher morbidity, prolonged hospitalization, and delayed functional recovery due to age‑related decline in physiological reserve and immune function.3–7 Current Western medical management primarily consists of gastrointestinal decompression, nil per os, parenteral nutrition, and supportive care.8–11 However, this approach often yields suboptimal outcomes: decompression may be incomplete, systemic inflammation persists, and the return of bowel function is frequently slow, leading to extended hospital stays and increased suffering.12–15
Endoscopic placement of a nasointestinal decompression tube has been proposed to achieve more effective decompression by aspirating fluid from the dilated small bowel.16–18 While this technique relieves mechanical distension, it does not directly address the underlying inflammatory response or promote restoration of intestinal motility and barrier function. Therefore, additional strategies that simultaneously reduce inflammation and protect the intestinal mucosa are needed.
Traditional Chinese Medicine (TCM) considers EPIIO as a syndrome of “internal excess‑heat accumulation” resulting from surgical trauma that depletes qi and blood, leading to dysfunction of the spleen and stomach.19,20 Dachengqi Decoction, a classical TCM formula, has been used for centuries to purge heat and accumulation. Importantly, modern pharmacological studies have provided clinical and translational evidence for its effects: it reduces pro‑inflammatory cytokines (eg, IL‑6, CRP), protects intestinal mucosal barrier integrity, improves gastrointestinal motility, and modulates gut microbiota.21–27 For instance, Chen et al demonstrated that Dachengqi Decoction ameliorated postoperative ileus in a mouse model by suppressing intestinal inflammation,21 and clinical studies have shown its beneficial effects in acute pancreatitis and sepsis‑associated intestinal injury.22–24 Nevertheless, in patients with EPIIO, oral administration of herbal decoction is often impractical due to vomiting or impaired intestinal transit.
To overcome this limitation, delivering Dachengqi Decoction directly through the intestinal obstruction tube – thereby placing the medication near the site of obstruction – offers a logical integrated approach combining mechanical decompression with pharmacotherapy. Despite the theoretical advantages, high‑quality randomized controlled trials evaluating this catheter‑based delivery of modified Dachengqi Decoction in elderly patients with EPIIO following gastrointestinal emergency surgery are lacking.
Therefore, the present study was designed to fill this gap. The objective was to evaluate the efficacy and safety of adding modified Dachengqi Decoction administered via the intestinal obstruction tube to standard decompression and conventional Western medical therapy. We hypothesized that, compared with conventional treatment alone, the combined regimen would lead to faster resolution of abdominal symptoms, shorter time to flatus and oral intake, greater reduction in systemic inflammatory markers (WBC, neutrophil count, CRP, IL‑6), improved intestinal barrier function (as reflected by D‑lactate and DAO), better correction of electrolyte imbalances, and enhanced nutritional status (albumin and prealbumin) in elderly patients with EPIIO after gastrointestinal emergency surgery.
Materials and Methods
General Information
Sample Size Estimation
Previous studies have suggested that the use of an intestinal obstruction tube combined with conventional Western medicine can significantly shorten the time to postoperative symptom improvement.28–30 This study aimed to compare the effects of adding Dachengqi Decoction versus not adding it to the treatment regimen of intestinal decompression tube plus conventional Western medicine. Therefore, the sample size was calculated based on the comparison of means between two independent samples. With a significance level (α) set at 0.05, a statistical power of 0.9, and an equal number of cases in both groups, the SPSS 25.0 statistical system estimated a requirement of 95 cases per group. However, due to limited recruitment time and practical constraints, a total of 62 patients (31 per group) were enrolled. Consequently, the study is underpowered to detect small effect sizes, and the results should be considered exploratory. This limitation is acknowledged in the Discussion. These patients were admitted to the Department of Gastrointestinal Surgery at Ji’an Central People’s Hospital between July 2024 and June 2025, based on clinical practicality.
Diagnostic Criteria
(1) Western Medicine Criteria: Recent history of gastrointestinal emergency surgery; initial recovery of bowel sounds or gradual initiation of oral intake after surgery, followed by the emergence of obstruction symptoms (cessation of flatus and defecation, predominantly abdominal distension with possibly insignificant abdominal pain); abdomen firm on palpation, with bowel sounds diminished, absent, or normal; abdominal X-ray revealing multiple air-fluid levels.31 (2) Traditional Chinese Medicine (TCM) Criteria: Meeting the TCM syndrome pattern of Internal Excess-Heat Accumulation: manifested as abdominal distension and pain with tenderness and guarding, constipation, dry mouth and tongue, halitosis, scanty dark urine, a red tongue with a yellow and thick coating, and a rapid, slippery pulse.
Inclusion Criteria
Patients meeting the above diagnostic criteria; aged between 60 and 75 years; having undergone laparoscopic surgery for conditions including acute appendicitis with perforation, gastroduodenal ulcer perforation, or intestinal obstruction, with successful procedures and no related complications; development of intestinal obstruction symptoms between postoperative days 4 and 14, without typical signs of peritonitis; patients in good general physical condition with normal cognitive function; ability to cooperate with transnasal intestinal obstruction tube placement; understanding and acceptance of the study protocol.
Exclusion Criteria
Presence of intestinal strangulation, vascular, paralytic, or mechanical intestinal obstruction; mesenteric vascular disease; concomitant malignancy; hematological or immune system diseases; severe hepatic or renal dysfunction; coagulation disorders.
Elimination Criteria
Patients assigned to the experimental group who were assessed by the TCM department as unsuitable for treatment with Dachengqi Decoction; patients whose condition deteriorated requiring emergency surgical intervention; patients requesting withdrawal from the study; patients with poor compliance.
Grouping
Patients were randomly assigned using a simple random number table into an experimental group (n=31) and a conventional treatment group (n=31). Comparison of baseline demographic and clinical characteristics showed no statistically significant differences between the two groups (P > 0.05), as detailed in Table 1. The study was approved by the Institutional Medical Ethics Committee, and all patients provided written informed consent. To ensure allocation concealment, the group assignments were placed in sequentially numbered, opaque, sealed envelopes by a researcher not involved in patient enrollment. After a patient provided written informed consent and met all eligibility criteria, the treating physician opened the next envelope to reveal the allocation.
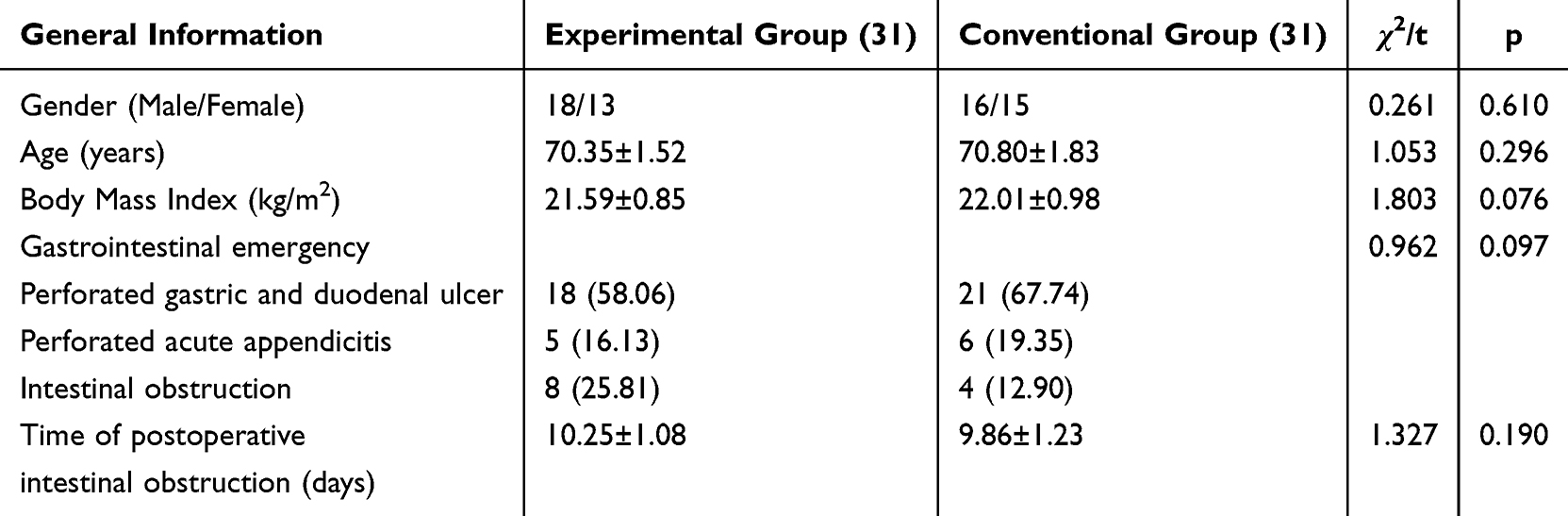 |
Table 1 Comparison of Baseline Characteristics Between the Two Groups [n (%), Mean ± SD] |
Methods
Both groups of patients underwent endoscopic-assisted placement of a transnasal intestinal obstruction decompression tube (Cure Medical International Trade [Dalian] Co., Ltd., model: MD-08A98H). The operation method was as follows: The endoscope was advanced to the horizontal part of the duodenum. Subsequently, a slippery guidewire was placed into the upper segment of the jejunum, after which the endoscope was withdrawn. A 5F angiography catheter was inserted over the guidewire to the upper jejunum. Under digital subtraction angiography (DSA) guidance, the intestinal obstruction tube was advanced transnasally to the distal small intestine. It was then carried further into the intestinal lumen by peristaltic movement for decompression. Diatrizoate meglumine contrast agent was injected to visualize intestinal dilatation and obstruction, and to confirm the obstruction site. Following this, 10–15 mL of sterile distilled water was injected into the anterior balloon to inflate it, and the guidewire was removed. The intestinal obstruction guidewire was further advanced into the stomach, leaving it in a relaxed loop within the gastric cavity, and connected to external negative pressure suction.
Conventional Treatment Group
Based on intestinal decompression via the obstruction tube, patients in this group received conventional Western medical interventions, including nil per os (NPO), correction of fluid-electrolyte and acid-base imbalances, intravenous nutritional support, and symptomatic treatment. Parenteral nutritional support was provided as follows: non-protein calories at 105–125 kcal/(kg·d), nitrogen supplementation at 0.15 g/(kg·d), with a calorie-to-nitrogen ratio of 150:1. Fat emulsion supplied 30–40% of non-protein calories, while glucose supplied 60%–70%. This was administered intravenously once daily (ivd, qd) for 7–14 days. Targeted pharmacological treatment included: Somatostatin (3 mg + 48 mL normal saline), administered via continuous pump infusion every 12 hours (q12h) for 5–10 days; and glucocorticoids (Dexamethasone, 5 mg, intravenous injection, q12h) for 3–5 days.
Experimental Group
In addition to intestinal decompression via the obstruction tube and the conventional Western medical regimen described above, patients in this group received treatment with modified Dachengqi Decoction administered through the intestinal obstruction tube. The base formula consisted of: Rhei Radix et Rhizoma (Dahuang) 15 g, Magnoliae Officinalis Cortex (Houpo) 15 g, Aurantii Fructus Immaturus (Zhishi) 12 g, and Natrii Sulfas (Mangxiao) 12 g.
To balance individual clinical needs with treatment reproducibility, modifications to the base formula were made according to a standardized decision algorithm based on specific symptoms and signs. This algorithm is presented in Supplementary Table 1. In brief:
For qi deficiency (fatigue, weak pulse), Astragali Radix (Huangqi) 20–30 g was added.
For blood stasis (dark tongue, fixed abdominal pain), Persicae Semen (Taoren) 12 g and Carthami Flos (Honghua) 9 g were added.
For severe abdominal distension due to qi stagnation, the dosage of Aurantii Fructus Immaturus (Zhishi) and Magnoliae Officinalis Cortex (Houpo) was increased by 3 g each, or stir‑fried Raphani Semen (Laifuzi) 15 g was added.
For persistent constipation with good tolerance, the dosage of Rhei Radix et Rhizoma (Dahuang) and Natrii Sulfas (Mangxiao) was increased by 3 g each.
If the patient developed diarrhea or excessively frequent bowel movements, the dosage of Rhei Radix et Rhizoma (Dahuang) and Natrii Sulfas (Mangxiao) was reduced (eg, to 9 g each), and their decoction method was changed from “added later” to “decocted together with other herbs”.
Once bowel movements became smooth, Natrii Sulfas (Mangxiao) was omitted from the formula.
All herbal medicines were sourced from the Chinese pharmacy department of Ji’an Central People’s Hospital. The pharmacy department dispensed and decocted the herbs. Each dose yielded 100 mL of decoction, which was packaged into 50 mL bags. The decoction was administered twice daily (morning and evening) via the intestinal obstruction tube by a specialized nurse. Following each infusion, the tube was clamped for 2 hours. One treatment course lasted for 7 days.
Observation Indicators
Blinding and Outcome Assessment: A blinded assessment method was employed. Personnel responsible for radiological evaluation, laboratory data analysis, and statistical analysis were unaware of the group assignments. Patients and treating clinicians were not blinded to group assignment because the experimental intervention (intracatheter administration of herbal decoction) could not be feasibly masked. However, outcome assessors (radiologists, laboratory technicians, and statisticians) were blinded to group allocation.
Recovery Parameters
The following recovery-related timepoints and parameters were recorded: time to disappearance of abdominal distension/pain, time to first anal (or stoma) flatus, time to initiation of liquid diet, time to resolution of air-fluid levels on imaging, total volume of gastrointestinal decompression drainage, time to removal of the decompression tube, and total hospital length of stay.
Inflammatory Markers
Fasting venous blood samples were collected from patients before treatment, and on days 7 and 14 after treatment. Approximately 6 mL of blood was drawn and distributed into three separate collection tubes. One tube containing anticoagulant was immediately analyzed using a multifunctional hematology analyzer (Dannan, USA, model EXCELL-22) to determine White Blood Cell count (WBC) and Absolute Neutrophil Count. The remaining two tubes without anticoagulant were centrifuged at high speed (radius: 5 cm, speed: 4000 r/min) for 10 minutes to obtain serum. The serum samples were aliquoted and stored at −80°C until batch analysis. Serum levels of C-reactive protein (CRP) were measured using immunonephelometry, and Interleukin-6 (IL-6) levels were determined using enzyme-linked immunosorbent assay (ELISA).
Intestinal Mucosal Barrier Function and Electrolyte Levels
The stored serum samples described above were used for analysis. D-lactate level was measured using an enzymatic colorimetric method. Diamine oxidase (DAO) activity was assessed using a double-antibody sandwich method. Serum levels of potassium (K⁺) and sodium (Na⁺) were determined using a fully automated biochemical analyzer (Mindray, China, model G92000).
Nutritional Status
The stored serum samples were also used to assess nutritional markers. Albumin (ALB) level was measured by immunoturbidimetry. Prealbumin (PA) level was determined using immunodiffusion assay.
Treatment Safety
All adverse events occurring during the treatment period were recorded and categorized, including tube-related complications (eg, displacement, blockage, nasal injury) and drug-related adverse reactions.
Statistical Methods
Data analysis was performed using SPSS statistical software (version 25.0). Measurement data conforming to a normal distribution are presented as the mean ± standard deviation (SD), and inter-group comparisons were conducted using the t-test. Data collected at multiple time points were analyzed using repeated measures analysis of variance (ANOVA). The interaction effect between time and treatment factors was first examined. If the interaction effect was statistically significant, a simple effects analysis was subsequently performed. If the interaction effect was not significant, the main effects were analyzed. Count data are described as rates (%) and were compared using the chi-square (χ2) test. A P-value of < 0.05 was considered indicative of a statistically significant difference.
Normality of continuous data was assessed using the Shapiro‑Wilk test. Data following a normal distribution are presented as mean ± SD and analyzed using parametric tests. No missing data occurred for any outcome measure during the 14‑day follow‑up; therefore, a complete case analysis was performed. All analyses were conducted on a per‑protocol basis, as no patient withdrew or was lost to follow‑up. No adjustment was made for multiple comparisons (eg, Bonferroni correction); thus, the reported P‑values should be interpreted as descriptive and hypothesis‑generating rather than confirmatory.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Ethical approval was obtained from the Scientific Research Ethics Committee of Ji’an Central People’s Hospital (Approval No. Lun Shen (2024) L00040). Written informed consent was obtained from all individual participants included in the study prior to their participation.
Results
A total of 78 elderly patients with EPIIO after gastrointestinal emergency surgery were assessed for eligibility. Of these, 16 were excluded (10 did not meet inclusion criteria, 4 declined to participate, and 2 had contraindications to catheter placement). The remaining 62 patients were randomized to the experimental group (n=31) or the conventional group (n=31). All 62 patients received the allocated intervention, completed the 14‑day follow‑up, and were included in the per‑protocol analysis (no withdrawals or losses to follow‑up). The participant flow is summarized in the CONSORT diagram (Figure 1). Patients were recruited between July 2024 and June 2025. The follow‑up period for each patient was 14 days post‑treatment, as specified in the protocol. Given the small sample size (31 per group) and the exploratory nature of the study, these findings should be interpreted cautiously. The study was underpowered to detect small effect sizes, as detailed in the Methods section and Discussion.
 |
Figure 1 The CONSORT flow diagram of our research. |
Comparison of Recovery Progress Between the Two Groups
The experimental group demonstrated significantly shorter time to the disappearance of abdominal distension/pain, time to first anal (or enterostomy) flatus, time to initiation of liquid diet, time to the resolution of air-fluid levels on imaging, time to catheter removal, and total hospital length of stay compared to the conventional group. Furthermore, the total volume of gastrointestinal decompression drainage in the experimental group was significantly greater than that in the conventional group (all P < 0.05). The primary recovery outcomes (time to symptom relief, time to first flatus, time to liquid diet, and hospital stay) are presented in Table 2. All recovery parameters favored the experimental group.
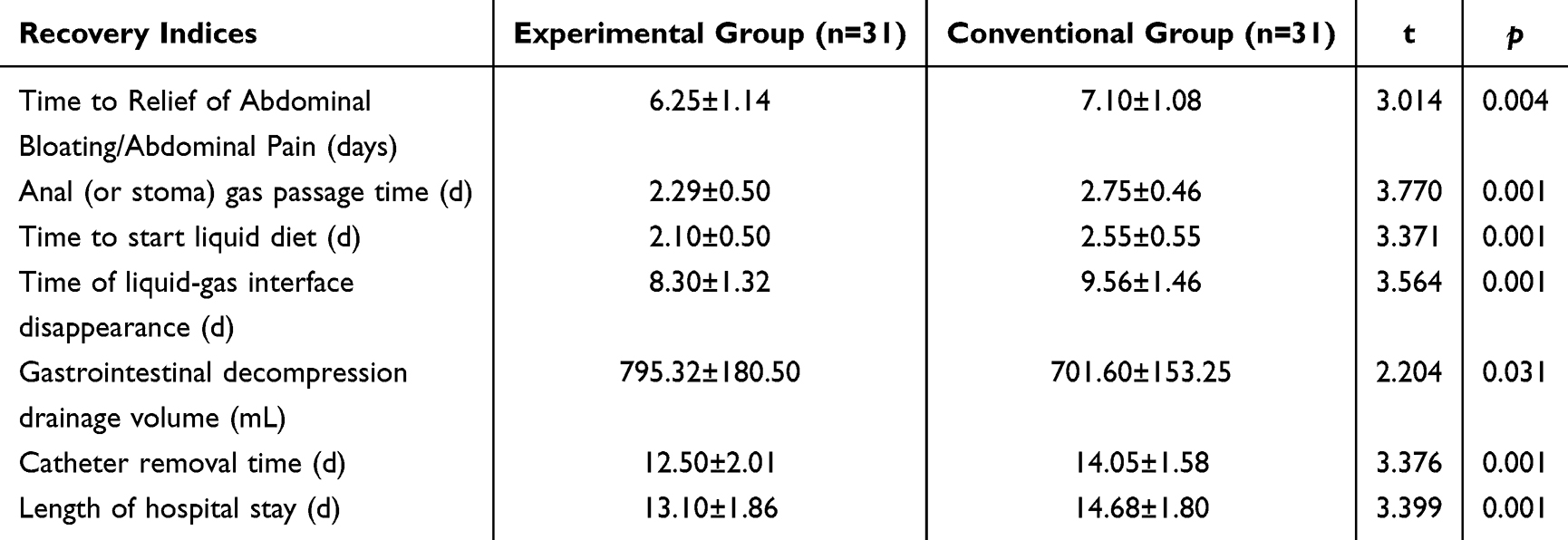 |
Table 2 Comparison of Postoperative Recovery Indices Between the Two Groups (Mean ± SD) |
Comparison of Inflammatory Markers Between the Two Groups
There was a significant interaction effect between group and time on serum levels of WBC, absolute neutrophil count, CRP, and IL-6 at different postoperative time points (P < 0.05). Simple effects analysis revealed that compared with pre-treatment levels, both groups showed significant decreases in WBC, absolute neutrophil count, CRP, and IL-6 at both 7 days and 14 days post-treatment (P < 0.05). Furthermore, at both the 7-day and 14-day post-treatment assessments, the experimental group demonstrated significantly lower levels of WBC, absolute neutrophil count, CRP, and IL-6 than the conventional group (P < 0.05). Table 3 summarizes the inflammatory markers. CRP and IL‑6 were considered the most clinically relevant indicators of systemic inflammation. WBC and absolute neutrophil count showed similar trends and are presented for completeness. The temporal trend for CRP is shown in Figure 2A, illustrating a greater decline in the experimental group over the 14‑day period.
 |
Table 3 Comparison of Inflammatory Markers Between the Two Groups (Mean ± SD) |
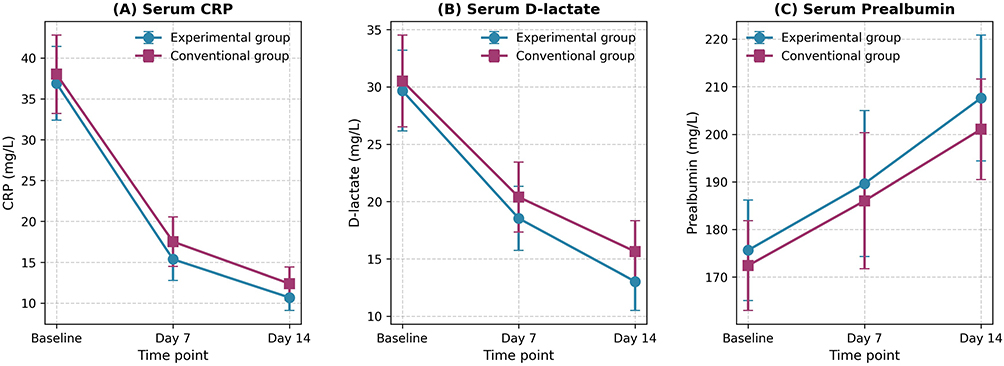 |
Figure 2 (A–C) Trends of selected outcomes over time. |
Comparison of Mucosal Barrier-Related Indicators and Electrolyte Levels Between the Two Groups
A significant interaction effect was observed between group and time for serum levels of D-lactate, DAO, K⁺, and Na⁺ at different postoperative time points (P < 0.05). Simple effects analysis indicated that compared to pre-treatment levels, both groups exhibited significant decreases in D-lactate and DAO, along with significant increases in K⁺ and Na⁺ at both 7 days and 14 days post-treatment (all P < 0.05). Furthermore, at both the 7-day and 14-day post-treatment assessments, the experimental group demonstrated significantly lower levels of D-lactate and DAO, and significantly higher levels of K⁺ and Na⁺ compared to the conventional group (all P < 0.05). Table 4 presents intestinal barrier function (D‑lactate, DAO) and electrolyte levels (K⁺, Na⁺). D‑lactate and DAO were the prespecified primary markers of mucosal barrier integrity; both improved significantly in the experimental group. Electrolyte changes followed a similar pattern and are shown for completeness. Figure 2B displays the trend for D‑lactate, showing a more pronounced reduction in the experimental group.
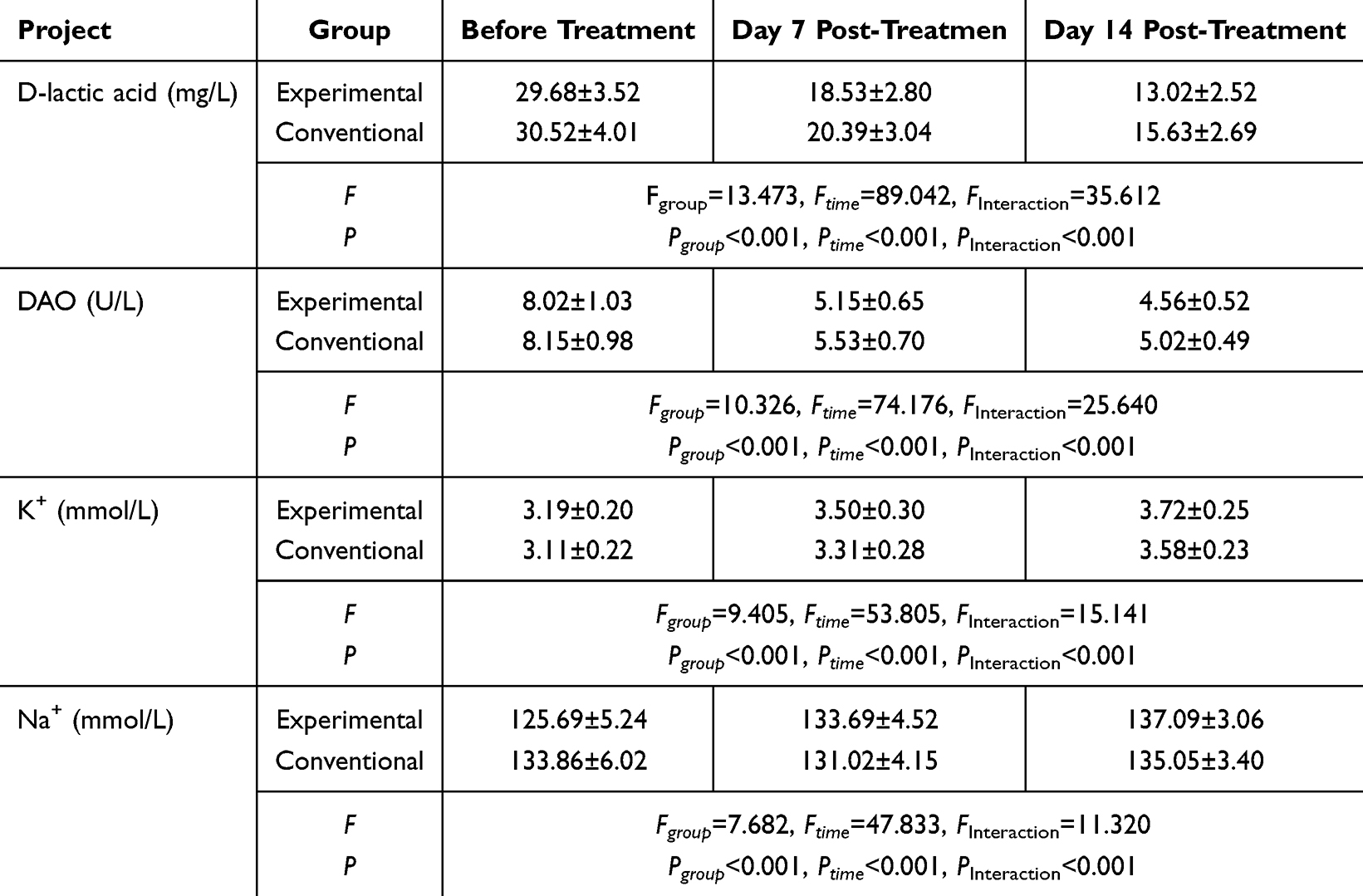 |
Table 4 Comparison of Intestinal Mucosal Barrier Function and Electrolyte Levels Between the Two Groups (Mean ± SD) |
Comparison of Nutritional Indicators Between the Two Groups
There was no statistically significant difference in the duration of parenteral nutrition use between the two groups (P > 0.05). A significant interaction effect was observed between group and time for serum levels of ALB and PA at different postoperative time points (P < 0.05). Simple effects analysis showed that compared to pre-treatment levels, both groups exhibited significant increases in ALB and PA at both 7 days and 14 days post-treatment (all P < 0.05). At 7 days post-treatment, there was no statistically significant difference in ALB and PA levels between the two groups (P > 0.05). However, at 14 days post-treatment, the experimental group demonstrated significantly higher levels of both ALB and PA compared to the conventional group (P < 0.05). Nutritional outcomes are shown in Table 5. Prealbumin (PA) is a more sensitive short‑term nutritional marker than albumin (ALB). Both increased in both groups, but the experimental group showed a significantly greater improvement at day 14. The duration of parenteral nutrition did not differ significantly between groups and is reported in the same table The trend for prealbumin (Figure 2C) indicates a faster and greater increase in the experimental group.
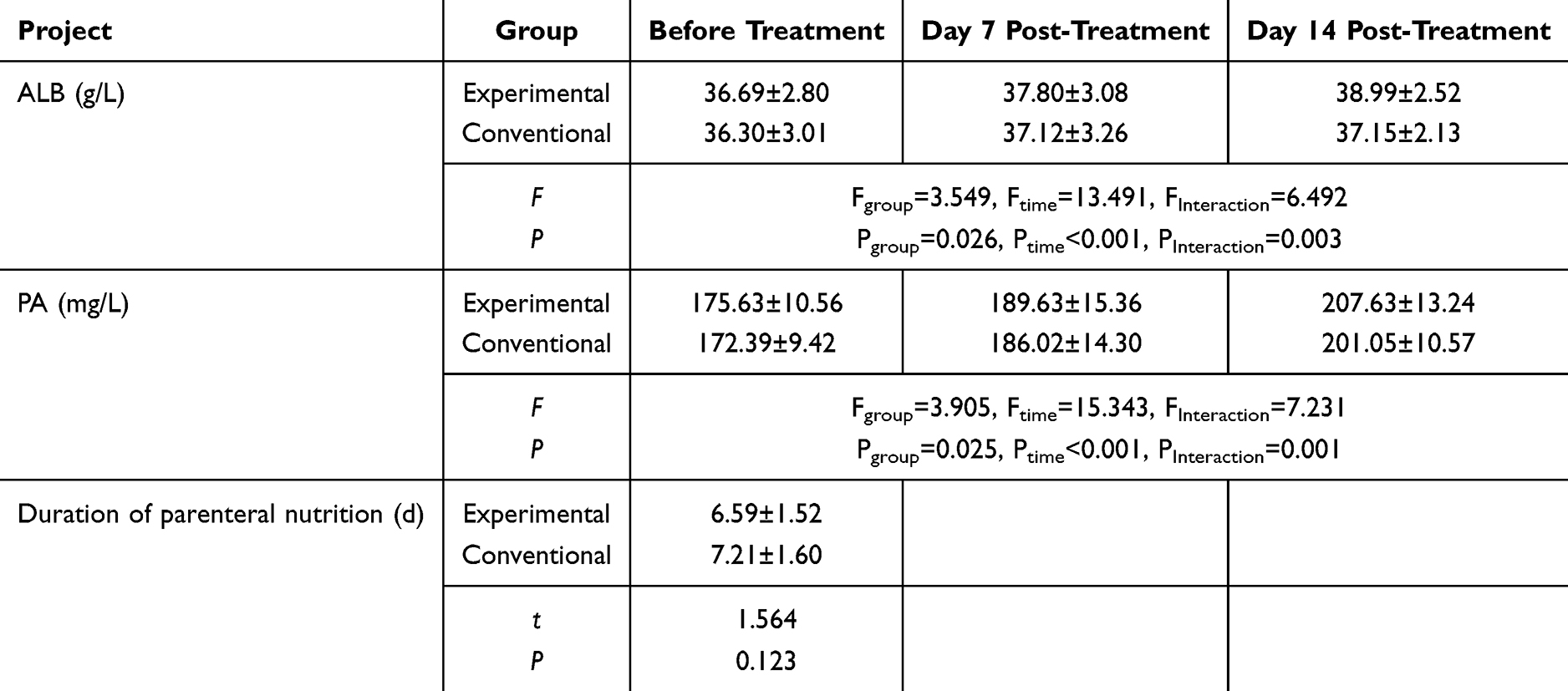 |
Table 5 Comparison of Nutritional Indices Between the Two Groups (Mean ± SD) |
Comparison of Treatment Safety Between the Two Groups
During the treatment period, no instances of abnormal liver or kidney function, allergic reactions, significant drug-related adverse reactions, or catheter-related complications were observed or recorded in either group.
Discussion
Postoperative early inflammatory intestinal obstruction (EPIIO) following gastrointestinal emergencies is characterized by a high incidence and prolonged course in elderly patients, often necessitating extended fasting periods and imposing significant physical and psychological distress.32–34 Conventional Western medical management primarily focuses on gastrointestinal decompression and symptom alleviation, often adopting a passive approach while awaiting spontaneous resolution of inflammation and functional recovery.8–11 However, this strategy may be associated with suboptimal decompression efficacy, poor tolerance to nutritional support in some elderly patients, consequently leading to prolonged hospitalization and extended patient suffering.12–15 Therefore, exploring more effective treatment strategies remains a clinical priority. Advances in medical technology have demonstrated that compared to standard nasogastric tubes, transnasal intestinal obstruction tubes provide more effective gastrointestinal decompression by aspirating deeper intestinal fluids, thereby reducing intraluminal pressure more rapidly and establishing a superior physical foundation for subsequent therapy.35–37 Nonetheless, the therapeutic action of the intestinal obstruction tube is largely confined to decompression, without directly addressing the underlying pathological mechanisms such as systemic inflammation and gastrointestinal paralysis.
In Traditional Chinese Medicine (TCM), EPIIO is categorized under syndromes such as “Yangming fu-organ excess” and “internal excess-heat accumulation”. Surgery is believed to cause visceral injury, depletion of qi and blood, and subsequent dysfunction of spleen and stomach in transportation and transformation. This leads to stagnation of clear nutrients and failure of turbid waste to descend, resulting in internal accumulation of damp-heat in the large intestine, manifesting as abdominal distension, pain, and difficulty with defecation and flatus.21 Dachengqi Decoction, a classic TCM formula, is highly effective in treating Yangming fu-organ excess and internal excess-heat accumulation syndromes, functioning to promote qi movement, resolve accumulations, remove blood stasis, and purge the bowels. However, the traditional oral administration of herbal decoctions is often impractical in patients with intestinal obstruction. Consequently, this study explored the administration of Dachengqi Decoction via the intestinal obstruction tube, forming an integrated Chinese-Western treatment combining physical decompression with pharmacotherapy, which theoretically offers synergistic therapeutic benefits. This study systematically evaluated the efficacy of this regimen across multiple dimensions, including recovery progression, inflammation, nutritional status, electrolytes, and intestinal barrier function.
The results of this study indicate that compared to conventional Western treatment, the administration of Dachengqi Decoction via the intestinal obstruction tube significantly shortened the time to resolution of abdominal distension/pain, time to initiation of liquid diet, time to first anal/enterostomy flatus, time to disappearance of air-fluid levels on imaging, time to catheter removal, and overall hospital stay, while increasing the total volume of gastrointestinal decompression drainage. These findings suggest that this integrated regimen facilitates rapid recovery. A recent clinical study from China (Li et al, 2023)38 also reported that treatment with a transnasal intestinal obstruction tube combined with Dachengqi Decoction significantly promoted symptom recovery and reduced systemic inflammation in postoperative patients with EPIIO of the qi deficiency and blood stasis pattern, which aligns with our core findings, albeit with differences in the specific treatment protocol. In the present study, the intestinal obstruction tube was advanced to the site of obstruction, providing direct and effective decompression of the dilated intestinal segment. Based on clinical experience, EPIIO after gastrointestinal emergency surgery predominantly presents as an internal excess-heat accumulation pattern, with qi deficiency and blood stasis as the key pathogenesis. Therefore, Dachengqi Decoction was administered via the tube and modified according to syndrome differentiation. The base formula (Rhei Radix et Rhizoma [Dahuang], Magnoliae Officinalis Cortex [Houpo], Aurantii Fructus Immaturus [Zhishi], Natrii Sulfas [Mangxiao]) was used to purge heat and accumulation vigorously. Modifications were made based on individual presentations: Astragali Radix (Huangqi) was added for concomitant qi deficiency; Persicae Semen (Taoren) and Carthami Flos (Honghua) for blood stasis; the dosage of Aurantii Fructus Immaturus (Zhishi) and Magnoliae Officinalis Cortex (Houpo) was increased, or stir-fried Raphani Semen (Laifuzi) was added for severe qi stagnation; the dosage of Rhei Radix et Rhizoma (Dahuang) and Natrii Sulfas (Mangxiao) was increased for severe constipation, and reduced if diarrhea occurred to moderate the purgative effect; Natrii Sulfas (Mangxiao) was omitted once bowel movements became normal to prevent excessive purgation damaging healthy qi. Furthermore, administering the herbal decoction directly near the lesion site via the tube maximizes the therapeutic effect of the TCM formula. After completing the Dachengqi Decoction course, the tube was retained for continued negative pressure suction decompression for 24–48 hours for observation and was removed only upon confirmation of no symptom recurrence. The primary recovery outcomes underscore the significant acceleration of clinical recovery facilitated by this integrated regimen.
Our results showed that serum levels of inflammatory markers, including WBC, absolute neutrophil count, CRP, and IL‑6, were significantly lower in the experimental group compared to the conventional group. This suggests that the combined therapy was associated with reduced systemic inflammatory responses. Although we did not directly measure molecular mechanisms in this study, previous pharmacological studies have reported that Dachengqi Decoction can reduce pro‑inflammatory cytokines (eg, IL‑6, CRP) and inhibit endotoxin proliferation.21–24 Therefore, it is plausible that the observed anti‑inflammatory effect may be related to these properties. However, this mechanistic interpretation remains speculative in the context of our study, as we did not perform cytokine profiling or pathway analysis. Similarly, our results demonstrated that the integrated treatment significantly reduced serum levels of D‑lactate and DAO while increasing K⁺ and Na⁺ levels, indicating improved intestinal barrier function and correction of electrolyte imbalances. Based on previous reports that Dachengqi Decoction can protect intestinal mucosa, promote gastrointestinal motility, and maintain gut microbiota homeostasis,25–27 it is possible that the observed improvements in barrier function are related to these effects. Nevertheless, direct evidence of barrier protection (eg, histology, tight junction protein expression) was not obtained in this study, and the electrolyte changes may simply reflect better overall clinical recovery rather than a specific effect of the herbal formula. These interpretations should therefore be considered hypothesis‑generating rather than conclusive.
Maintaining adequate nutritional status is crucial for promoting rapid recovery in patients with EPIIO following gastrointestinal emergencies.22,23,34 The lack of significant difference in the duration of parenteral nutrition use between the two groups in this study may be attributed to the rapid intestinal rehabilitation facilitated by the intestinal obstruction tube. Once effective decompression is achieved and edema subsides, a transition to enteral nutrition can occur earlier, aligning with modern minimally invasive surgical concepts and reducing reliance on intravenous nutrition. The results showed that serum levels of ALB and PA were significantly higher in the integrated treatment group than in the conventional group at 14 days post-treatment, indicating that this regimen helps improve nutritional status. This benefit is likely due to the rapid restoration of intestinal function, creating favorable conditions for nutritional improvement and enabling earlier initiation of oral intake. The lack of significant difference at 7 days may be related to the shorter treatment duration and the relatively long half-life of ALB, which may not yet reflect treatment-induced changes. Collectively, these results indicate that the integrated regimen not only alleviates symptoms but also fundamentally improves the patient’s nutritional and metabolic state, with this advantage becoming more pronounced over time.
Our findings are broadly consistent with a recent randomized study by Li et al (2023),38 which reported that a nasal‑intestinal obstruction tube combined with Dachengqi Decoction improved recovery and reduced inflammation in patients with EPIIO of the qi deficiency and blood stasis pattern. However, that study also had a small sample size and lacked multiple testing correction. Importantly, high‑quality, large‑scale, double‑blind, placebo‑controlled trials of TCM formulas in postoperative intestinal obstruction remain scarce. In contrast, non‑TCM interventions for postoperative ileus, such as prokinetic agents (eg, metoclopramide, erythromycin) and peripheral opioid antagonists (eg, alvimopan), have shown only modest or inconsistent benefits. The integrated approach evaluated in our study – combining mechanical decompression with catheter‑delivered herbal therapy – may offer a complementary strategy, but its comparative effectiveness against established non‑TCM treatments has not been tested. Future head‑to‑head trials are warranted.
Several limitations should be acknowledged. First, the sample size (31 per group) was substantially smaller than the initial calculation (95 per group), making the study underpowered and potentially leading to effect overestimation. Additionally, the study included only elderly patients aged 60–75 years; therefore, the findings may not directly apply to younger patients or the very old (>75 years). Second, multiple endpoints were tested without adjustment for multiple comparisons, raising the risk of false‑positive findings; thus, P‑values should be interpreted as descriptive and hypothesis‑generating. Third, individualized modification of Dachengqi Decoction according to TCM syndrome differentiation, while clinically realistic, limits reproducibility. A standardized algorithm (Supplementary Table 1) has been provided, but some subjectivity remains. Fourth, blinding was limited to outcome assessors and statisticians; patients and clinicians were not blinded due to the nature of the intervention, introducing possible performance bias. Fifth, the 14‑day follow‑up is insufficient to assess long‑term outcomes such as recurrence or rehospitalization. Sixth, this single‑center study may not be generalizable to non‑elderly patients, other hospitals with different TCM practices, or non‑integrated settings. Finally, the consistent statistical significance across nearly all endpoints despite the small sample size further suggests potential effect overestimation. Readers should interpret the findings with caution, and large‑scale, multicenter, double‑blind trials with longer follow‑up are needed to confirm these preliminary results.
Conclusions
In conclusion, the integrated treatment combining an intestinal obstruction tube with modified Dachengqi Decoction was associated with favorable outcomes in this cohort of elderly patients with EPIIO after gastrointestinal emergency surgery, including reduced systemic inflammation, improved intestinal mucosal barrier function, correction of electrolyte disturbances, enhanced nutritional status, and accelerated clinical recovery. No major adverse events were observed in this small cohort. However, given the substantial limitations – small sample size (underpowered), single‑center design, individualized (non‑standardized) herbal modifications, short follow‑up (14 days), and lack of multiple testing correction – these findings should be considered preliminary and hypothesis‑generating rather than definitive. This study provides initial insights for developing integrated Chinese‑Western medicine models, but large‑scale, multicenter, double‑blind randomized trials with longer follow‑up are needed to confirm efficacy and safety.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
The authors sincerely thank the Medical Ethics Committee of Ji’an Central People’s Hospital for reviewing and approving this study. We are also grateful to all the participating patients for their trust and cooperation. We extend our appreciation to the nurses and staff of the Department of Gastrointestinal Surgery for their invaluable assistance in patient care and the implementation of the nasal intestinal catheter procedure. We also acknowledge the colleagues who provided statistical analysis support. Finally, this work was supported by the Science and Technology Program of Jiangxi Provincial Administration of Traditional Chinese Medicine (Grant No. 2024B0788).
Funding
This work was supported by the Science and Technology Program of Jiangxi Provincial Administration of Traditional Chinese Medicine (Grant No. 2024B0788).
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this article.
References
1. Ro H, Tsuchiya Y, Tsukamoto R, et al. Experience with laparoscopic surgery for rectal obstruction caused by intestinal endometriosis with a frozen pelvis: a case report. Surg Case Rep. 2025;11(1):cr.24–0148. doi:10.70352/scrj.cr.24-0148
2. Zeineddin S, Hu A, Linton S, et al. Association between appendiceal stump closure method and post-operative bowel obstruction after laparoscopic appendectomy. J Pediatric Surg. 2023;58(4):643–13. doi:10.1016/j.jpedsurg.2022.12.015
3. Bond A, Soop M, Taylor M, et al. Home parenteral nutrition and the older adult: experience from a national intestinal failure unit. Clin Nutr. 2020;39(5):1418–1422. doi:10.1016/j.clnu.2019.06.019
4. Kang G, Cheah MCC, Yen PB, et al. Parenteral nutrition-related complications in older patients with acute intestinal failure: a descriptive cohort study. J Parenteral Enteral Nutr. 2024;48(2):174–183. doi:10.1002/jpen.2578
5. Peerani F. Update in inflammatory bowel disease management in the elderly. Current Gastroenterol Rep. 2025;27(1):56. doi:10.1007/s11894-025-01005-2
6. Granot M, Kopylov U, Talmor Y, et al. Elderly-onset inflammatory bowel disease has distinct disease characteristics and treatment patterns. United Eur Gastroenterol J. 2025;13(9):1754–1764. doi:10.1002/ueg2.70092
7. Shung DL, Abraham B, Sellin J, Hou JK. Medical and surgical complications of inflammatory bowel disease in the elderly: a systematic review. Dig Dis Sci. 2015;60(5):1132–1140. doi:10.1007/s10620-014-3462-2
8. Rami Reddy SR, Cappell MS. A systematic review of the clinical presentation, diagnosis, and treatment of small bowel obstruction. Current Gastroenterol Rep. 2017;19(6):28. doi:10.1007/s11894-017-0566-9
9. Zielinski MD, Bannon MP. Current management of small bowel obstruction. Adv Surg. 2011;45(1):1–29. doi:10.1016/j.yasu.2011.03.017
10. Maung AA, Johnson DC, Piper GL, et al. Evaluation and management of small-bowel obstruction: an Eastern association for the surgery of trauma practice management guideline. J Trauma Acute Care Surg. 2012;73(5):S362–S369. doi:10.1097/TA.0b013e31827019de
11. Banting SP, Waters PS, Peacock O, et al. Management of primary and metastatic malignant small bowel obstruction, operate or palliate. A systematic review. ANZ J Surg. 2021;91(3):282–290. doi:10.1111/ans.16188
12. Lin C-Q, Pan -L-L, Cheng Y, Wang S-J, Lin J-L. Operational key points of super-low placement of an intestinal decompression tube and its clinical efficacy in elderly patients with incomplete small bowel obstruction. Surg Endosc. 2025;40:1–7.
13. Chen W, Peng M, Ye Z, Ai Y, Liu Z. The mode and timing of administrating nutritional treatment of critically ill elderly patients in intensive care units: a multicenter prospective study. Front Med. 2024;11:1321599. doi:10.3389/fmed.2024.1321599
14. Li R, Tian Q, Tian Q. Efficacy of intestinal decompression with long nasointestinal tube and selective contrast radiography in the treatment of small bowel obstruction in elderly patients. Minerva Chirurgica. 2014;71(2):85–90.
15. Plotnikov G, Levy Y, Trotzky D, et al. Characteristics of older adults receiving enteral feeding at a geriatric medical center. BMC Geriatr. 2024;24(1):628. doi:10.1186/s12877-024-05202-y
16. Zuo L, Cao L, Ding C, et al. Strategy to small intestine obstruction caused by Crohn’s disease on the basis of transnasal ileus tube insertion. BMC Surg. 2022;22(1):183. doi:10.1186/s12893-022-01632-w
17. Komagamine J, Noritomi D. Jejunal intussusception caused by a nasointestinal ileus tube. Eur J Case Rep Internal Med. 2022;9(2):003161. doi:10.12890/2022_003161
18. Lin H, Luo Y, Fang H, et al. Decompression effects of nasointestinal tube versus nasogastric tube for adhesive intestinal obstruction: a Meta-analysis. Chin J Digestive Surg. 2022;2022:551–556.
19. Zhang X, Wang Q, Zhong Z, et al. Pathogenesis of spleen and stomach diseases and therapeutic effect of banxia xiexintang based on theory of” mutual interference of clear and Turbid Qi” in Huangdi Neijing. Chin J Exp Trad Med Formul. 2024;2024:225–231.
20. Greenwood MT. Dysbiosis, spleen Qi, phlegm, and complex difficulties. Med Acupuncture. 2017;29(3):128–137. doi:10.1089/acu.2017.1226
21. Chen C, Li M, Liu X, et al. Traditional Chinese Medicine Da-Cheng-Qi-Tang ameliorates impaired gastrointestinal motility and intestinal inflammatory response in a mouse model of postoperative ileus. Evidence-Based Complem Altern Med. 2020;2020(1):9074069. doi:10.1155/2020/9074069
22. Zhao J, Zhong C, He Z, Chen G, Tang W. Effect of da-cheng-qi decoction on pancreatitis-associated intestinal dysmotility in patients and in rat models. Evidence-Based Complem Altern Med. 2015;2015(1):895717. doi:10.1155/2015/895717
23. Zhao X, Zhang Y, Li J, et al. Tissue pharmacology of Da-Cheng-Qi decoction in experimental acute pancreatitis in rats. Evidence-Based Complem Altern Med. 2015;2015(1):283175. doi:10.1155/2015/283175
24. Liu Y, Lei Y, Shang L, et al. Protective effects of Dachengqi Decoction in sepsis-associated liver injury based on network pharmacology analysis and experimental validation. J Ethnopharmacol. 2025;353:120450. doi:10.1016/j.jep.2025.120450
25. Shuhan W, Jinxiao L, Luorui S, et al. Dachengqi decoction ameliorated liver injury in liver fibrosis mice by maintaining gut vascular barrier integrity. Phytomedicine. 2025;136:156272. doi:10.1016/j.phymed.2024.156272
26. Guo W, Zhang X, Zhou X, et al. Dachengqi decoction for the treatment of acute pancreatitis: a comprehensive analysis based on metabolites, pharmacokinetics, and metabolites efficacy mechanisms. Front Pharmacol. 2025;16:1549909. doi:10.3389/fphar.2025.1549909
27. Wan M, Liu W, Liu Y, et al. Multiomics-based investigation on the mechanism of Dachengqi decoction in improving constipation through the microbiota-gut-brain axis. Bioorg Chem. 2025;164:108895. doi:10.1016/j.bioorg.2025.108895
28. Yang W, Pu J. Efficacy of ileus tube combined with meglumine diatrizoate in treating postoperative inflammatory bowel obstruction after surgery. World J Gastrointest Surg. 2023;15(9):1950. doi:10.4240/wjgs.v15.i9.1950
29. Li W, Li Z, An D, Liu J, Zhang X. Role of the small intestinal decompression tube and Gastrografin in the treatment of early postoperative inflammatory small bowel obstruction. Zhonghua Wei Chang Wai Ke Za Zhi. 2014;17(3):275–278.
30. Truong S, Willis S, Riesener K, Seelig M, Bötjer A, Schumpelick V. Value of intraluminal intestinal decompression by endoscopic placement of a Dennis tube in therapy of ileus. Retrospective clinical study of 174 patients. Langenbecks Archiv fur Chirurgie. 1997;382(4):216–221. doi:10.1007/BF02391869
31. Chang KJ, Marin D, Kim DH, et al. ACR appropriateness criteria® suspected small-bowel obstruction. J Am College Radiol. 2020;17(5):S305–S314. doi:10.1016/j.jacr.2020.01.025
32. Yehaiya M, Yuan C, Aimaiti X, Li T. Investigating the factors influencing postoperative dynamic intestinal obstruction following laparoscopic colorectal radical surgery. Annali Italiani di Chirurgia. 2024;95(6):1178–1185. doi:10.62713/aic.3639
33. Takagi H, Wada N, Morishita S, et al. Postoperative small intestinal obstruction caused by barbed suture after robot-assisted laparoscopic sacrocolpopexy. IJU Case Rep. 2024;7(2):105–109. doi:10.1002/iju5.12677
34. Ni J, Liu J, Chen C. Role of early enteral nutrition on postoperative recovery of older patients undergoing intestinal obstruction surgery. Annali italiani di chirurgia. 2025;96(7):916–923. doi:10.62713/aic.4038
35. Chen S-Y, Huang R, Zhang Y, Xie Z-F, Huang H, Shi H. A retrospective single-center study of transnasal ileus tube insertion accompanied with cap-assisted endoscopic advancement for malignant adhesive bowel obstruction. Sci Rep. 2024;14(1):29227. doi:10.1038/s41598-024-80304-6
36. Shimizu S, Hara H, Muto Y, Kido T, Miyata R, Itabashi M. Laparoscopic management of small bowel obstruction secondary to a mesodiverticular band of a Meckel’s diverticulum in an adult: a case report and literature review. Medicine. 2024;103(30):e39164. doi:10.1097/MD.0000000000039164
37. Chusilp S, Yamoto M, Vejchapipat P, Ganji N, Pierro A. Nasogastric decompression after intestinal surgery in children: a systematic review and meta-analysis. Pediatric Surg Int. 2021;37(3):377–388. doi:10.1007/s00383-020-04818-6
38. L L, W YH, H XJ. Clinical study on nasal-intestinal obstruction tube combined with Da-Cheng-Qi decoction in the treatment of early postoperative inflammatory intestinal obstruction of Qi deficiency and blood stasis type. J Hunan Univ Chin Med. 2023;43(2):299–303.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Significance of Preoperative Albumin and Prealbumin in Predicting Adverse Events After Posterior Lumbar Interbody Fusion in Elderly Patients
Zhang S, Wang P, Wang S, Han D, Lu S
Clinical Interventions in Aging 2026, 21:605937
Published Date: 14 July 2026