")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
Efficacy of HP-3070, A Once-Daily Asenapine Transdermal System, in the Treatment of Adults with Schizophrenia: A PANSS Five-Factor Analysis
Authors Citrome L , Castelli M, Hasebe M, Terahara T, Faden J, Komaroff M
Received 13 December 2023
Accepted for publication 12 March 2024
Published 29 March 2024 Volume 2024:20 Pages 755—764
DOI https://doi.org/10.2147/NDT.S439712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Leslie Citrome,1 Mariacristina Castelli,2 Masami Hasebe,3 Takaaki Terahara,3 Justin Faden,4 Marina Komaroff2
1Department of Psychiatry and Behavioral Sciences, New York Medical College, Valhalla, NY, USA; 2Product Development, Noven Pharmaceuticals, Inc, Jersey City, NJ, USA; 3Hisamitsu Pharmaceutical Co., Inc, Tokyo, Japan; 4Department of Psychiatry, Lewis Katz School of Medicine at Temple University, Philadelphia, PA, USA
Correspondence: Leslie Citrome, Department of Psychiatry and Behavioral Sciences, New York Medical College, 40 Sunshine Cottage Road, Valhalla, NY, 10595, USA, Tel +1 845-362-2081, Email [email protected]
Introduction: HP-3070, a once-daily asenapine transdermal system, is the first antipsychotic “patch” formulation FDA approved for adults with schizophrenia. Positive and Negative Syndrome Scale (PANSS) score items can be grouped into a five-factor structure to describe specific schizophrenia symptom domains. This post hoc analysis of data from a pivotal study evaluated HP-3070’s efficacy by examining these factors.
Methods: In a phase 3 study, adults with an acute exacerbation of schizophrenia were randomized to six weeks of treatment with HP-3070 3.8mg/24h, 7.6mg/24h, or placebo. An analysis was performed using the five PANSS factor domains (negative symptoms, positive symptoms, disorganized thought, uncontrolled hostility/excitement, anxiety/depression). Mixed-model repeated-measures (MMRM) analysis included change from baseline (CFB) in PANSS factor score as the repeated dependent variable, with country, treatment, visit, treatment by visit interaction, and baseline PANSS score as covariates.
Results: The analysis included 607 patients. Treatment with HP-3070 3.8mg/24h resulted in a statistically significant LS mean CFB (improvement) vs placebo at Weeks 4– 6 for all domains except for anxiety/depression, where a numerical difference was observed in favor of active treatments. Among the domains, the positive symptom factor demonstrated the numerically greatest LS mean (SE) difference from placebo in CFB, which for HP-3070 7.6mg/24h was − 2.0 [0.57] and for HP-3070 3.8mg/24h was − 2.3 [0.57]; P< 0.001 for both. Treatment effect size for the positive symptom factor using Cohen’s d (95% confidence intervals) was 0.39 (0.17, 0.61) for HP-3070 7.6mg/24h and 0.45 (0.20, 0.64) for HP-3070 3.8mg/24h.
Discussion: Post hoc analysis using a PANSS five-factor model suggests that HP-3070 may address a broad range of symptoms in people with schizophrenia.
Keywords: asenapine, transdermal, patch, schizophrenia, positive and negative syndrome scale, five-factor
Introduction
Schizophrenia is a major cause of disability globally.1 The condition is associated with a number of treatment challenges, and the search for therapies that are effective, tolerable, and aligned with patient preferences can lead to multiple medication changes in individuals with schizophrenia.2,3
Asenapine, a second-generation antipsychotic, has been commercially available since 2009 as a sublingual tablet administered twice daily (BID).4,5 There are, however, known treatment challenges associated with administration of sublingual asenapine (SLA), such as frequency of administration (BID), food and drink restrictions, oral hypoesthesia, and dysgeusia;6,7 thus, alternative formulations would be welcome. HP-3070, a once-daily asenapine transdermal system, is the first antipsychotic “patch” approved by the US Food and Drug Administration (FDA) for adults with schizophrenia,8,9 providing a different means of delivering asenapine. Moreover, the option of transdermal administration provides another method to accommodate patient preferences and autonomy in medication selection for those who would prefer something other than a sublingual or oral tablet.7,10 Finally, in general, transdermal formulations allow caregivers to visually check for treatment adherence.7,10
In a phase 3 randomized controlled trial, once-daily applications of HP-3070 7.6 mg/24h or 3.8 mg/24h demonstrated significant improvement compared with placebo in Positive and Negative Syndrome Scale (PANSS) total scores.11 Differences in the least-squares mean (LSM) (95% confidence intervals [CIs]; adjusted P) change from baseline in PANSS total scores were −4.8 (−8.06, −1.64; adjusted P=0.003) and −6.6 (−9.81, −3.40; adjusted P<0.001) for 7.6 mg/24h and 3.8 mg/24h, respectively. Improvements were observed starting after 2–3 weeks of treatment and continued through Week 6 of treatment. HP-3070 was also generally well tolerated in patients, with a systemic safety profile consistent with what has been observed for SLA, although there were differences regarding potential effects at the site of administration inherent to the formulation (ie, dysgeusia with SLA and potential skin reactions with HP-3070).11 Discontinuations of HP-3070 in the pivotal trial due to application site reactions or skin disorders occurred in ≤0.5% of patients across all treatment groups.11
The PANSS includes 30 items divided across three subscales: Positive, Negative, and General Psychopathology.12 Further factor analytic studies suggest that there are five independent factors that can describe distinct symptom domains in schizophrenia: Positive, Negative, Cognitive/Disorganization, Depression/Anxiety, and Excitability/Hostility.13 This is an improvement over the original subdivision of the PANSS, as it lends further granularity for exploration of treatment effects on the symptoms of cognitive/disorganization, excitability/hostility, and depression/anxiety that often accompany psychosis. The objective of this post hoc analysis of the pivotal phase 3 study on HP-3070 was to evaluate its efficacy by examining effects on five different domains of the PANSS (negative symptoms, positive symptoms, disorganized thought, uncontrolled hostility, and anxiety/depression) using the factor structure originally published by Marder et al.14
Materials and Methods
This study is a post hoc analysis of data from the pivotal randomized, double-blind, placebo-controlled phase 3 trial of HP-3070 (ClinicalTrials.gov identifier: NCT02876900, registered August 3, 2016).
Patients and Study Design
Detailed methods for the pivotal phase 3 study have been reported.11,15 Briefly, the study, which was conducted between August 2016 and November 2017, enrolled adults experiencing acute exacerbations of schizophrenia (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition [DSM-5] criteria) at the time of screening.
Eligible patients had a Clinical Global Impression-Severity of Illness (CGI-S) scale score of ≥4 and PANSS total score of ≥80, with scores of ≥4 in ≥2 predefined PANSS positive subscale items (conceptual disorganization, delusions, hallucinatory behavior, unusual thought content) at screening and baseline, and were able to wear a patch for 24 hours. Patients were excluded if they were diagnosed with schizophrenia <6 months prior to enrollment, had a current DSM-5 diagnosis other than schizophrenia, were known non-responders to asenapine, or were resistant/refractory to antipsychotic treatment. Treatment resistance was defined as having little or no symptomatic response to ≥2 courses of antipsychotic treatment at a therapeutic dose for ≥6 weeks (as dosed according to the drug’s package insert).
No other antipsychotics, antidepressants, mood stabilizers, stimulants, or non-psychopharmacologic medications with psychotropic properties were permitted, except for selected psychotropic medications for specific conditions as described below. Lorazepam was allowed for insomnia, agitation, or anxiety only; if lorazepam was not available, another available benzodiazepine was permitted after Medical Advisor approval. Benztropine was allowed for treatment-emergent extrapyramidal symptoms such as drug-induced parkinsonism or dystonia, zolpidem was allowed for insomnia, and propranolol was allowed for akathisia. Medications for chronic non-psychiatric medical conditions were permitted, provided that the condition and treatment regimen were stable before screening.
After a 3–14-day screening/run-in period, eligible patients were randomized (1:1:1) to HP-3070 7.6 mg/24 h, HP-3070 3.8 mg/24 h, or placebo in the form of patches applied daily for 6 weeks. Study personnel applied patches, rotating daily across application sites (abdomen, hip, upper arm, upper back, upper chest).
Study Endpoints and Statistical Methods
All randomized and dosed patients with baseline and at least one post-baseline PANSS total score assessment (full analysis set) were evaluated weekly for change from baseline in PANSS score. Analysis of PANSS scores was performed according to the five factors as described by Marder et al.14 The analysis included the following five domains: 1) Negative symptoms (blunted affect [N1], emotional withdrawal [N2], poor rapport [N3], passive/apathetic social withdrawal [N4], lack of spontaneity and flow of conversation [N6], motor retardation [G7], active social avoidance [G16]); 2) Positive symptoms (delusions [P1], hallucinatory behavior [P3], grandiosity [P5], suspiciousness/persecution [P6], stereotyped thinking [N7], somatic concerns [G1], unusual thought content [G9], lack of judgment and insight [G12]); 3) Disorganized thought (conceptual disorganization [P2], difficulty in abstract thinking [N5], mannerisms and posturing [G5], poor attention [G11], disturbance of volition [G13], preoccupation [G15], disorientation [G10]); 4) Uncontrolled hostility/excitement (excitement [P4], hostility [P7], uncooperativeness [G8], poor impulse control [G14]); and 5) Anxiety/depression (anxiety [G2], guilt feelings [G3], tension [G4], depression [G6]).
Mixed-model repeated-measures (MMRM) analyses included change from baseline in PANSS factor score as the repeated dependent variable and country, treatment, visit, treatment by visit interaction, and baseline PANSS score as covariates. Effect size is described using Cohen’s d together with the respective 95% CI.
Results
Patient Disposition and Characteristics
In total, 616 eligible patients provided informed consent and were randomized into HP-3070 7.6 mg/24h, HP-3070 3.8 mg/24h, and placebo treatment groups, forming the intent-to-treat (ITT) analysis set.11 Of these patients, 614 received at least one dose of study medication and were included in the safety analysis set (SAS). The full analysis set (FAS), which included 607 patients who had at least one post-baseline PANSS assessment, was used for this post hoc analysis.
Baseline demographics and patient characteristics were balanced between the HP-3070 and placebo treatment groups, as previously reported (Table 1).11
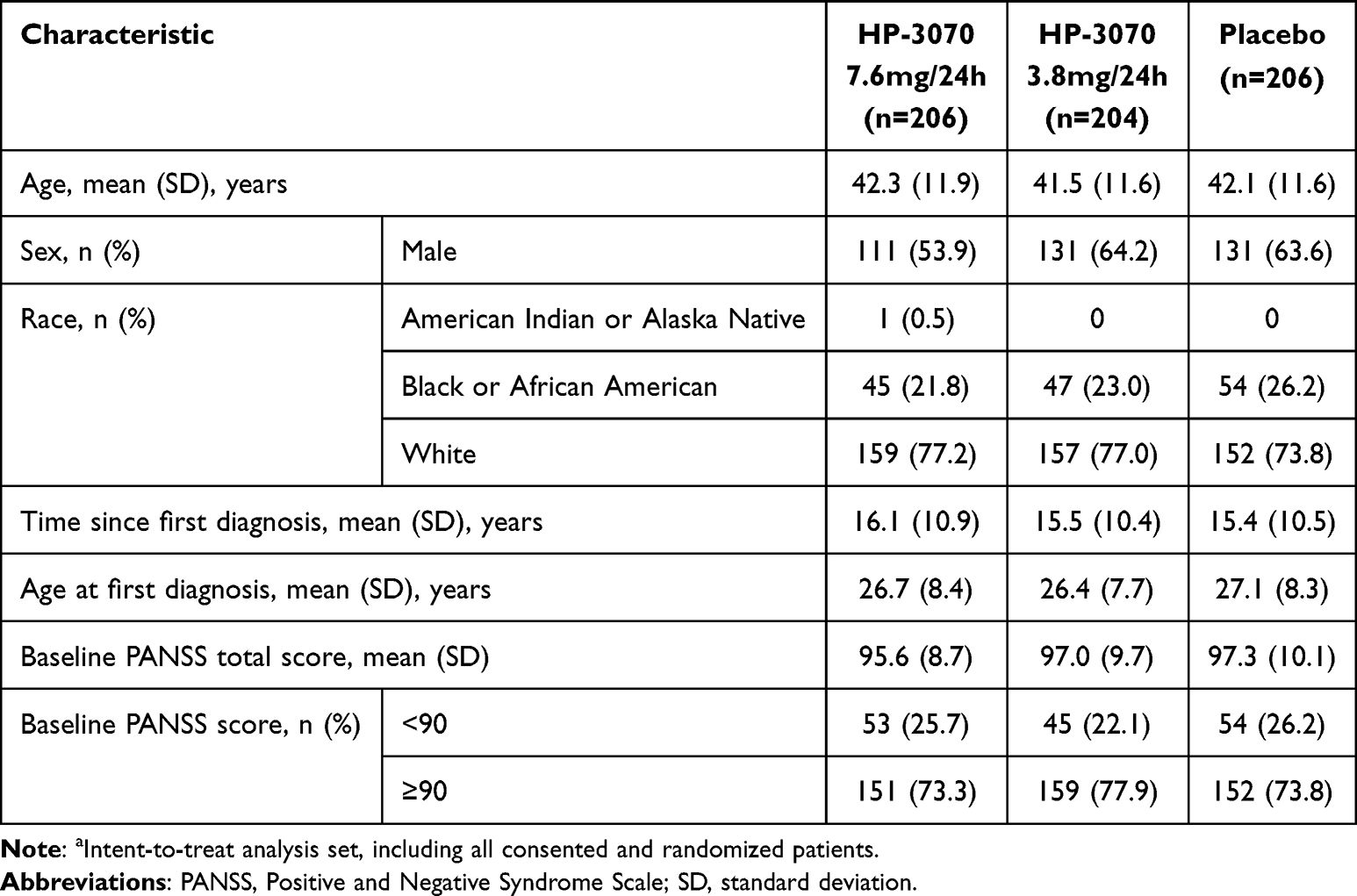 |
Table 1 Baseline Demographics and Clinical Characteristicsa |
Efficacy of HP-3070
Compared with patients receiving placebo, patients treated with either dose of HP-3070 showed treatment effects on all five PANSS Marder factor scores. The least-squares (LS) mean estimates of the difference from placebo in change from baseline for Weeks 1–6 are shown in Figure 1 (numerical data shown in Table 2).
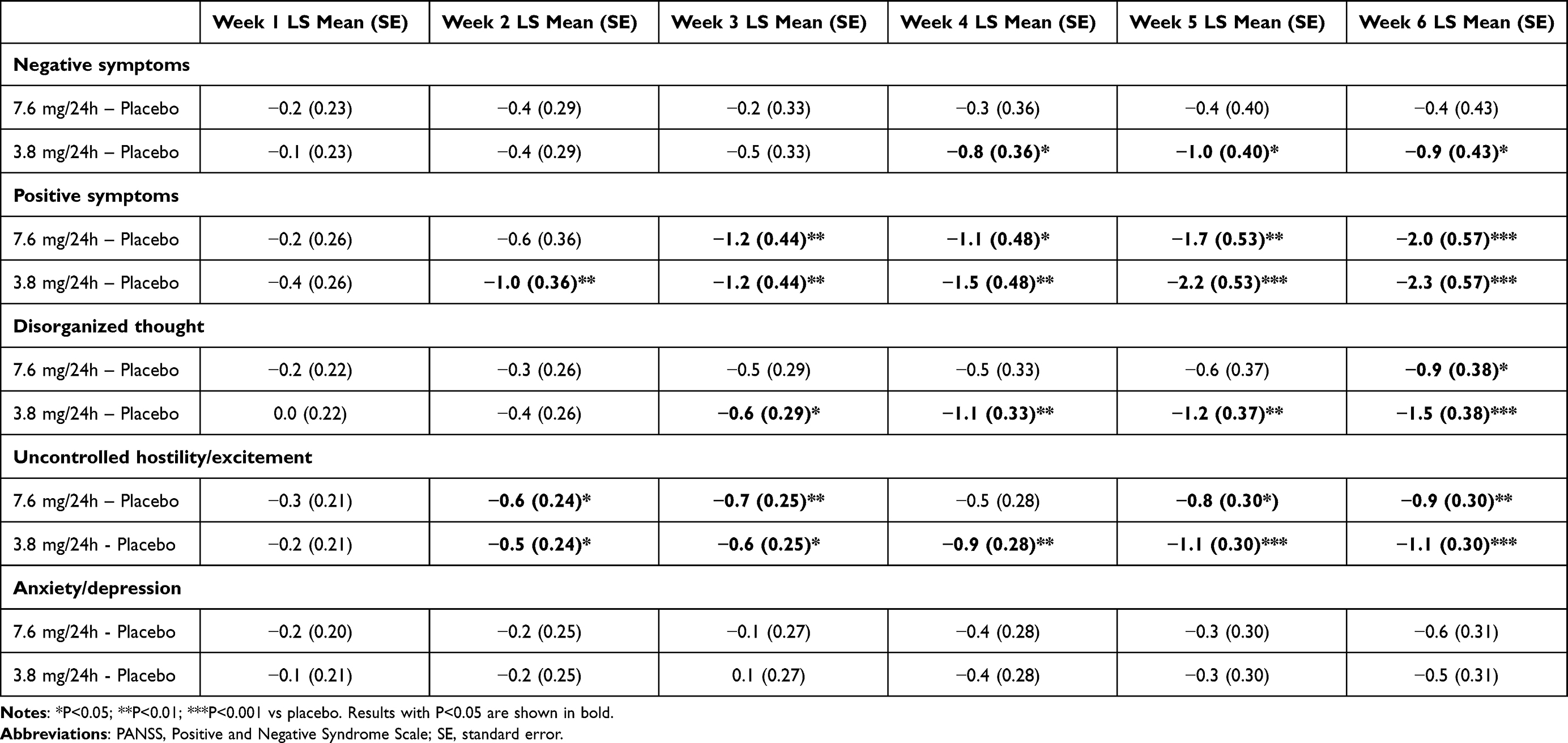 |
Table 2 LS Mean Changes from Baseline Vs Placebo in a 5-Factor PANSS Model for Weeks 1–6 |
 |
Figure 1 LS Mean Changes from Baseline to Week 6 in a 5-Factor PANSS Model. Abbreviations: LS, least-squares; PANSS, Positive and Negative Syndrome Scale; SE, standard error. Notes: *P<0.05; **P<0.01; ***P<0.001 vs placebo. |
For HP-3070 3.8 mg/24h, compared with placebo, significant improvements were observed during Weeks 2–6 for positive symptoms and uncontrolled hostility/excitement, during Weeks 3–6 for disorganized thought, and during Weeks 4–6 for negative symptoms. The anxiety/depression factor demonstrated numerical differences in favor of HP-3070 3.8 mg/24h compared with placebo, but these differences were not statistically significant.
For HP-3070 7.6 mg/24h, compared with placebo, numerical improvements were observed in all domains, with statistically significant improvements observed for positive symptoms (Weeks 3–6), disorganized thought (Week 6), and uncontrolled hostility/excitement (Weeks 2, 3, 5, and 6).
The LSM estimates of the difference from placebo in change from baseline to Week 6 for each factor are shown in Table 3. At Week 6, both doses demonstrated statistically significant improvement in positive symptoms, disorganized thought, and uncontrolled hostility/excitement, with the greatest LS mean (SE) differences from placebo in change from baseline seen for positive symptoms (−2.0 [0.57] for HP-3070 7.6 mg/24h vs placebo; −2.3 [0.57] for HP-3070 3.8 mg/24h vs placebo). Effect size differences at Week 6 ranged from 0.09 to 0.39 for HP-3070 7.6 mg/24h and 0.15 to 0.45 for HP-3070 3.8 mg/24h, with the largest numerical effect sizes seen for positive symptoms (Table 3).
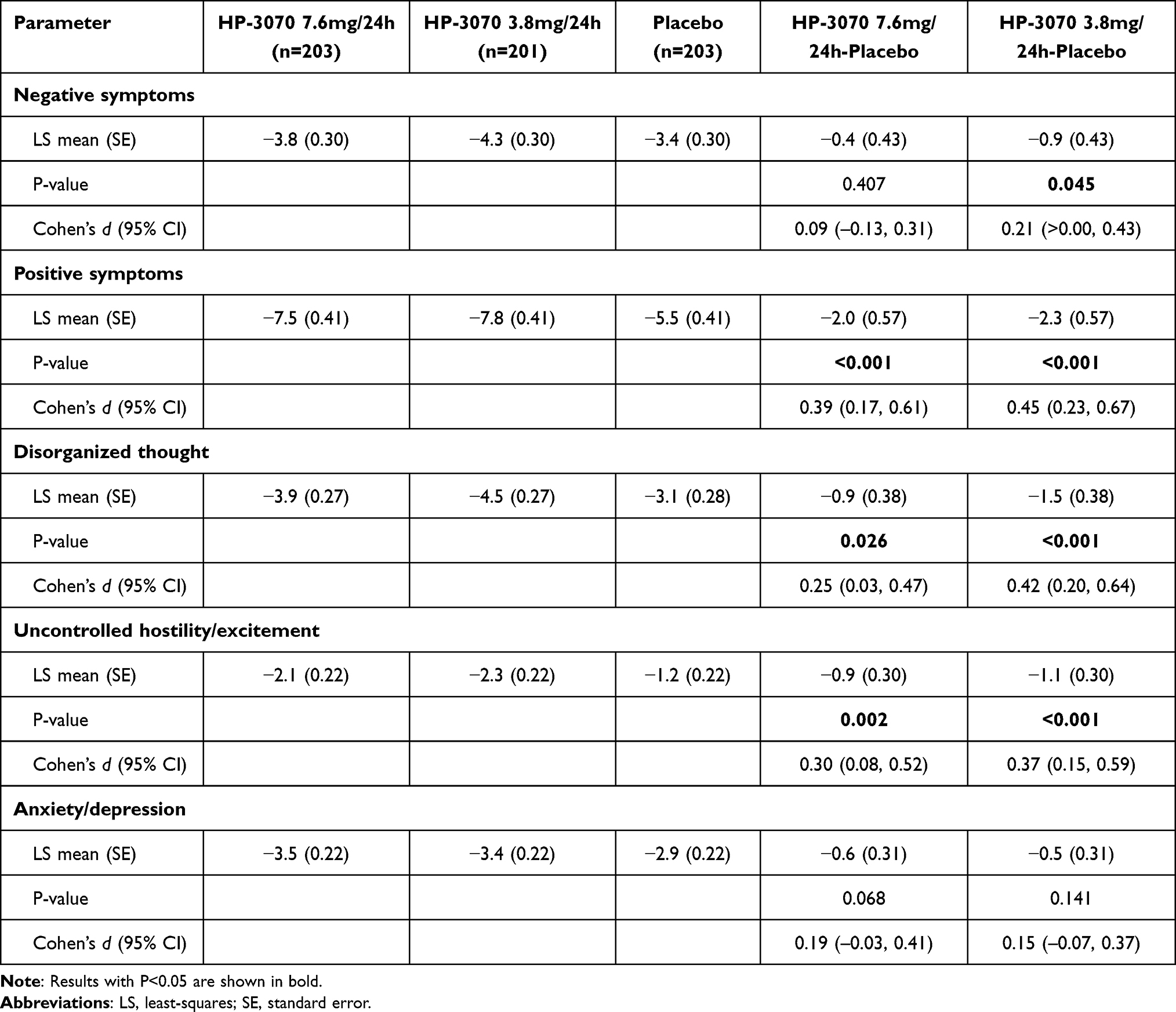 |
Table 3 LS Mean Changes from Baseline to Week 6 in a 5-Factor PANSS Model |
Discussion
HP-3070 has previously been shown to be both effective and well tolerated in the treatment of adults with schizophrenia. Significant improvements from baseline in PANSS total score were observed 2–3 weeks after initiating HP-3070 treatment compared with placebo and were generally maintained through Week 6 of the study.11 The observed efficacy and safety of HP-3070 were consistent with the known profile of SLA, other than tolerability characteristics of the formulation itself, with minimal dermal reactions.6,11,16,17 A prior post hoc analysis examining HP-3070’s specific effect on the PANSS hostility item demonstrated that HP-3070 was superior to placebo.15
This post hoc analysis of the phase 3 clinical study used a five-factor PANSS model as originally published by Marder et al14 to further investigate the efficacy of HP-3070 in adults with schizophrenia. Treatment effects on the abovementioned PANSS domains were observed, indicating an overall effect of HP-3070 on negative symptoms, positive symptoms, disorganized thought, uncontrolled hostility/excitement, and anxiety/depression. Among the five domains, positive symptoms exhibited the greatest Week 6 reductions from baseline in Marder five-factor PANSS analysis scores and the largest effect sizes vs placebo.
The PANSS five-factor model has previously been used to analyze the results of phase 3 studies comparing the efficacy of SLA 5 mg and 10 mg BID vs placebo in patients with acute schizophrenia.16,18 Dose equivalencies for SLA 5 mg and 10 mg BID are HP-3070 3.8mg/24h and 7.6mg/24h, respectively.19 Kane et al16 reported that after 6 weeks of treatment, both studied doses of SLA were superior to placebo on the PANSS positive symptoms domain and SLA 5 mg was superior to placebo on the anxiety/depression and disorganized thought factors, but SLA was not superior to placebo on negative symptom and hostility/excitement factors. In contrast, the present study found that treatment with HP-3070 3.8 mg/24h was superior to placebo at Week 6 on all factors except anxiety/depression and that HP-3070 7.6 mg/24h treatment was superior to placebo at Week 6 on all factors except anxiety/depression and negative symptoms. This PANSS factor analysis of SLA is limited by the inclusion of only one of the four original pivotal trials conducted on SLA.20,21
Takekita et al18 used a different approach toward analyzing SLA efficacy based on the five-factor model. Patients were separated into three groups according to severity based on PANSS factor scores (high positive symptoms [higher scores on positive symptoms, disorganized thoughts, and hostility/excitement]; high negative symptoms [higher scores on negative symptoms]; and overall lower PANSS scores at study baseline).18,22 The patient groups experiencing negative symptoms and overall lower PANSS scores showed significant improvement in total PANSS scores with both SLA doses vs placebo, while among patients experiencing positive symptoms, significant PANSS score improvement was observed only with the higher SLA dose (10 mg BID) vs placebo. The study was limited by the source of the data (a single study carried out in Japan, Republic of Korea, and Taiwan that was not one of the four pivotal trials that led to FDA approval in the US) and the exclusion of the PANSS anxiety/depression factor from consideration.
The PANSS five-factor model has also been utilized to compare the long-term efficacy of SLA to olanzapine using data from two 26-week studies conducted in patients with persistent negative symptoms of schizophrenia and their respective 26-week extensions.23,24 In the analysis by Buchanan et al23 in one of the core studies, changes favored olanzapine over asenapine for the PANSS hostility/excitement factor at weeks 20 and 26. In the other core study, changes favored olanzapine over asenapine for the PANSS positive symptom factor at week 26, disorganized thought factor at week 26, hostility/excitement factor at weeks 20 and 26, and anxiety/depression factor at weeks 20 and 26. In the report by Potkin et al,24 although SLA 5 and 10 mg BID did not show statistical superiority to olanzapine 5–20 mg once daily after 26 weeks of treatment, SLA was superior to olanzapine after 52 weeks of treatment on the negative symptom factor.
In general, a transdermal formulation may be preferred over oral formulations for some patients. A transdermal asenapine patch specifically addresses some of the challenges associated with SLA, such as frequency of administration (BID), food and drink restrictions, oral hypoesthesia, and dysgeusia.6,7
Limitations
A limitation of this study is that it was conducted post hoc rather than as a pre-specified analysis, which limits the strength of the conclusions. Because the data included in this analysis were taken from only one phase 3 study, the sample sizes were relatively small compared to other similar five-factor analyses of other agents that pool data from several studies.25 Although a treatment effect was observed for both doses of HP-3070 on all domains, for one factor, anxiety/depression, statistical significance between HP-3070 and placebo was not observed despite the numerical difference, potentially due to the relatively small sample size. Additionally, study participants were selected based on a requirement for high scores in certain PANSS positive subscale items, thereby increasing the likelihood of observing a larger effect size on positive symptoms. This may represent a limitation on translation of our findings to patients with a different symptom profile.
Conclusions
In this post hoc analysis exploring treatment effects across the five PANSS factors, HP-3070 demonstrated statistically significant treatment effects across multiple pathological dimensions that are typically associated with schizophrenia: negative symptoms, positive symptoms, disorganized thought, and uncontrolled hostility/excitement, with a numerical effect observed for anxiety/depression. These findings suggest that HP-3070 may address a broad range of symptoms in people with schizophrenia. Further studies investigating which symptoms within each of these dimensions respond best to HP-3070 treatment, and under which conditions these symptoms respond, are warranted.
As the first transdermal antipsychotic formulation approved in the United States for adults with schizophrenia, HP-3070 provides an additional and novel treatment option.
Data Sharing Statement
The data that support the findings of this study are available from Noven Pharmaceuticals. Restrictions apply to the availability of these data. Data can be requested by emailing Noven at [email protected].
Ethics Statement
The study protocol was approved by an independent ethics committee or review board at each study center (for list of ethics committees, see Supplemental Table 1). Written informed consent was obtained from all participants. The study was conducted in accordance with the ethical principles derived from the Declaration of Helsinki.
Acknowledgments
The authors thank Sandeep Byreddy, MS, for his contributions to data analysis and the development of this manuscript. The authors thank Michelle L. Jones, PhD, MWC, and Anthony DiLauro, PhD, of PharmaWrite, LLC, for medical writing and editorial assistance, which were funded by Hisamitsu Pharmaceutical Co, Inc. This manuscript was prepared according to the International Society for Medical Publication Professionals’ “Good Publication Practice for Communicating Company-Sponsored Medical Research: The GPP3 Guidelines”. Data from this paper were presented as a poster at Psych Congress 2022 (September 17–20, 2022, New Orleans, LA) and at NEI Congress 2022 (November 3–6, 2022, Colorado Springs, CO) and were published in abstract form as Citrome L et al. CNS Spectr. 2023;28(2):243–244 (https://doi.org/10.1017/S1092852923001773).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and have agreed to be accountable for all aspects of the work.
Funding
This study was funded by Hisamitsu Pharmaceutical Co, Inc. Although personnel at Hisamitsu Pharmaceutical Co, Inc. reviewed the manuscript, final approval for the decision to submit the manuscript was the sole decision of the authors.
Disclosure
Dr. Citrome served as a consultant to AbbVie/Allergan, Acadia, Adamas, Alkermes, Angelini, Astellas, Avanir, Axsome, Biogen, BioXcel, Boehringer Ingelheim, Cadent Therapeutics, Cerevel, Clinilabs, COMPASS, Delpor, Eisai, Enteris BioPharma, HLS Therapeutics, Idorsia, INmune Bio, Impel, Intra-Cellular Therapies, Janssen, Karuna, Lundbeck, Luye, Lyndra, MapLight, Marvin, MedAvante-ProPhase, Merck, Mitsubishi-Tanabe, Neumora, Neurocrine, Neurelis, Noema, Novartis, Noven, Otsuka, Ovid, Praxis, Recordati, Relmada, Reviva, Sage, Sumitomo/Sunovion, Supernus, Teva, University of Arizona, Vanda, and Wells Fargo, and one-off ad hoc consulting for individuals/entities conducting marketing, commercial, or scientific scoping research; served as a speaker for AbbVie/Allergan, Acadia, Alkermes, Angelini, Axsome, BioXcel, Eisai, Idorsia, Intra-Cellular Therapies, Janssen, Lundbeck, Neurocrine, Noven, Otsuka, Recordati, Sage, Sunovion, Takeda, and Teva; and performed CME activities organized by medical education companies such as Medscape, NACCME, NEI, and Vindico and universities and professional organizations/societies; owns stocks (small number of shares of common stock) in Bristol-Myers Squibb, Eli Lilly, Johnson & Johnson, Merck, and Pfizer purchased >10 years ago; has stock options in Reviva; and earns royalties/publishing income from Taylor & Francis (Editor-in-Chief, Current Medical Research and Opinion, 2022-present), Wiley (Editor-in-Chief, International Journal of Clinical Practice, through end 2019), UpToDate (reviewer), Springer Healthcare (book), and Elsevier (Topic Editor, Psychiatry, Clinical Therapeutics). Dr. Castelli and Dr. Komaroff received non-financial support from Hisamitsu Pharmaceutical Co, Inc., during the conduct of the study and received personal fees from Noven Pharmaceuticals, Inc. as employees, outside the submitted work. Mrs. Hasebe and Dr. Terahara received non-financial support from Hisamitsu Pharmaceutical Co, Inc. and received personal fees from Hisamitsu Pharmaceutical Co, Inc., outside the submitted work. Dr. Faden served in a consultancy/advisory role with and received grant support from BioXcel Therapeutics. The authors report no other conflicts of interest in this work.
References
1. GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry. 2022;9(2):137–150. doi:10.1016/S2215-0366(21)00395-3
2. Citrome L. A review of the pharmacology, efficacy and tolerability of recently approved and upcoming oral antipsychotics: an evidence-based medicine approach. CNS Drugs. 2013;27(11):879–911. doi:10.1007/s40263-013-0105-7
3. Faden J, Citrome L. Schizophrenia: one name, many different manifestations. Med Clin North Am. 2023;107(1):61–72. doi:10.1016/j.mcna.2022.05.005
4. Allergan USA, Inc. SAPHRIS® (asenapine) sublingual tablets [prescribing information]. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/022117s020s021lbl.pdf.
5. Musselman M, Faden J, Citrome L. Asenapine: an atypical antipsychotic with atypical formulations. Ther Adv Psychopharmacol. 2021;11:20451253211035269. doi:10.1177/20451253211035269
6. Citrome L. Asenapine for schizophrenia and bipolar disorder: a review of the efficacy and safety profile for this newly approved sublingually absorbed second-generation antipsychotic. Int J Clin Pract. 2009;63(12):1762–1784. doi:10.1111/j.1742-1241.2009.02228.x
7. Citrome L, Zeni CM, Correll CU. Patches: established and emerging transdermal treatments in psychiatry. J Clin Psychiatry. 2019;80(4):18. doi:10.4088/JCP.18nr12554
8. Hisamitsu Pharmaceutical Co., Inc. SECUADO® (asenapine) transdermal system [prescribing information]. Available from: https://dailymed.nlm.nih.gov/dailymed/getFile.cfm?setid=685eaf44-5944-4f38-afba-0a4fc0b3462b&type=pdf.
9. Noven Pharmaceuticals, Inc. SECUADO® (asenapine) transdermal system, the first-and-only transdermal patch for the treatment of adults with schizophrenia, is now available in the U.S. Available from: https://www.noven.com/wp-content/uploads/2020/04/PR041320.pdf.
10. Stevens JR, Justin Coffey M, Fojtik M, Kurtz K, Stern TA. The use of transdermal therapeutic systems in psychiatric care: a primer on patches. Psychosomatics. 2015;56(5):423–444. doi:10.1016/j.psym.2015.03.007
11. Citrome L, Walling DP, Zeni CM, et al. Efficacy and safety of HP-3070, an asenapine transdermal system, in patients with schizophrenia: a phase 3, randomized, placebo-controlled study. J Clin Psychiatry. 2021;82(1):20m13602 doi:10.4088/JCP.20m13602.
12. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–276. doi:10.1093/schbul/13.2.261
13. Lehoux C, Gobeil MH, Lefèbvre AA, Maziade M, Roy MA. The five-factor structure of the PANSS: a critical review of its consistency across studies. Clin Schizophr Relat Psychoses. 2009;3(3):103–110. https://www.clinicalschizophrenia.net/articles/the-fivefactor-structure-of-the-panss-a-critical-review-of-its-consistency-across-studies.pdf.
14. Marder SR, Davis JM, Chouinard G. The effects of risperidone on the five dimensions of schizophrenia derived by factor analysis: combined results of the North American trials. J Clin Psychiatry. 1997;58(12):538–546. doi:10.4088/JCP.v58n1205
15. Citrome L, Komaroff M, Starling B, Byreddy S, Terahara T, Hasebe M. Efficacy of HP-3070, an asenapine transdermal system, on symptoms of hostility in adults with schizophrenia: a post hoc analysis of a 6-week phase 3 study. J Clin Psychiatry. 2022;83(4):21m14355. doi:10.4088/JCP.21m14355
16. Kane JM, Cohen M, Zhao J, Alphs L, Panagides J. Efficacy and safety of asenapine in a placebo- and haloperidol-controlled trial in patients with acute exacerbation of schizophrenia. J Clin Psychopharmacol. 2010;30(2):106–115. doi:10.1097/JCP.0b013e3181d35d6b
17. Potkin SG, Cohen M, Panagides J. Efficacy and tolerability of asenapine in acute schizophrenia: a placebo- and risperidone-controlled trial. J Clin Psychiatry. 2007;68(10):1492–1500. doi:10.4088/JCP.v68n1004
18. Takekita Y, Hiraoka S, Iwama Y, et al. Divergence of dose-response with asenapine: a cluster analysis of randomized, double-blind, and placebo control study. CNS Spectr. 2022;27(3):369–377. doi:10.1017/S1092852921000043
19. Suzuki K, Castelli M, Komaroff M, Starling B, Terahara T, Citrome L. Pharmacokinetic profile of the asenapine transdermal system (HP-3070). J Clin Psychopharmacol. 2021;41(3):286–294. doi:10.1097/JCP.0000000000001383
20. Citrome L. Asenapine review, part II: clinical efficacy, safety and tolerability. Expert Opin Drug Saf. 2014;13(6):803–830. doi:10.1517/14740338.2014.908183
21. Szegedi A, Verweij P, van Duijnhoven W, Mackle M, Cazorla P, Fennema H. Meta-analyses of the efficacy of asenapine for acute schizophrenia: comparisons with placebo and other antipsychotics. J Clin Psychiatry. 2012;73(12):1533–1540. doi:10.4088/JCP.11r07596
22. Kinoshita T, Bai YM, Kim JH, Miyake M, Oshima N. Efficacy and safety of asenapine in Asian patients with an acute exacerbation of schizophrenia: a multicentre, randomized, double-blind, 6-week, placebo-controlled study. Psychopharmacology. 2016;233(14):2663–2674. doi:10.1007/s00213-016-4295-9
23. Buchanan RW, Panagides J, Zhao J, et al. Asenapine versus olanzapine in people with persistent negative symptoms of schizophrenia. J Clin Psychopharmacol. 2012;32(1):36–45. doi:10.1097/JCP.0b013e31823f880a
24. Potkin SG, Phiri P, Szegedi A, Zhao J, Alphs L, Cazorla P. Long-term effects of asenapine or olanzapine in patients with persistent negative symptoms of schizophrenia: a pooled analysis. Schizophr Res. 2013;150(2–3):442–449. doi:10.1016/j.schres.2013.08.024
25. Citrome L, Meng X, Hochfeld M. Efficacy of iloperidone in schizophrenia: a PANSS five-factor analysis. Schizophr Res. 2011;131(1–3):75–81. doi:10.1016/j.schres.2011.05.018
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.