Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Efficacy of Fire Needle Therapy Combined with Doxycycline Hydrochloride in the Management of Moderate-to-Severe Acne Vulgaris: A Randomized Controlled Trial
Authors Zhu T, Li JZ, Sun SY, Ji YF, Ji LX
Received 5 August 2025
Accepted for publication 7 November 2025
Published 13 November 2025 Volume 2025:18 Pages 7471—7484
DOI https://doi.org/10.2147/JMDH.S558510
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Veronica Swallow
Tao Zhu,1,* Jin-Zhen Li,2,* Shi-Yue Sun,3 Yu-Fang Ji,4 Lai-Xi Ji4
1School of Acu-Mox and Tuina, Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 2Department of Traditional Chinese Medicine, Fujian Maternity and Child Health Hospital, Fuzhou, People’s Republic of China; 3Institute of Acupuncture and Moxibustion, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China; 4School of Acu-Mox and Tuina, Shanxi University of Chinese Medicine, Jinzhong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lai-Xi Ji, School of Acu-Mox and Tuina, Shanxi University of Chinese Medicine, Jinzhong, People’s Republic of China, Email [email protected]
Objective: Fire needle therapy has shown promise in treating acne vulgaris (AV), improving facial lesions and patient quality of life. This study aims to investigate the effects of combining fire needle therapy with doxycycline hydrochloride tablets (DHT) on the Global Acne Grading System (GAGS), the échelle d’évaluation clinique des cicatrices d’acné (ECCA) grading scale, the Dermatology Life Quality Index (DLQI), and the serum levels of inflammatory factors interleukin-17 (IL-17), tumor necrosis factor-α (TNF-α), and interleukin-6 (IL-6) in patients with moderate-to-severe AV.
Methods: 70 patients with moderate-to-severe AV were randomly assigned to the control group (n=35) to receive oral DHT treatment once a day and the intervention group (n=35) to be treated with fire needle therapy on the basis of DHT once a week. The total treatment duration for both groups was 8 weeks. Therapeutic efficacy was evaluated at the 4-week and 8-week marks. The primary outcome measure evaluated was the GAGS score. The secondary outcome measures included the ECCA score, the DLQI score, and the serum levels of the inflammatory factors IL-17, TNF-α, and IL-6.
Results: Compared to baseline data, both groups exhibited marked improvements in skin lesions at both the 4-week and 8-week treatment marks. Significant reductions were observed in the GAGS, ECCA, and DLQI scores, as well as in the serum levels of the inflammatory factors IL-17, TNF-α, and IL-6. Notably, the intervention group demonstrated significantly greater improvements than the control group at both the 4-week and 8-week assessments.
Conclusion: An 8-week regimen of fire needle therapy combined with DHT improved lesion severity, scar symptoms, quality of life, and serum inflammatory cytokine levels in patients with moderate-to-severe AV compared to DHT monotherapy.
Keywords: needle therapy, doxycycline, acne vulgaris, clinical trail, skin lesions
Introduction
Acne Vulgaris (AV) is a chronic inflammatory disease of the pilosebaceous unit, characterized by androgen-induced increased sebum secretion, abnormal keratinization, inflammatory changes, and colonization of hair follicles on the face, neck, chest, and back by Cutibacterium acnes.1,2 Influenced by multiple genetic and environmental factors, AV is often locally accompanied by seborrhea. As the condition progresses, it can lead to scar formation and post-inflammatory hyperpigmentation (PIH), significantly impacting patients’ appearance and causing psychological distress.3–5 Statistical data indicate that the prevalence of AV among adolescents is as high as 93%, with a continuing upward trend, making it the most common dermatological condition globally.6 Notably, a substantial number of patients progress to moderate-to-severe AV, characterized by numerous inflammatory skin lesions.7 For the treatment of moderate-to-severe AV, oral isotretinoin or tetracycline antibiotics constitute the primary first-line therapies.8 Among these, tetracycline-class drugs (eg, doxycycline) exert their therapeutic effects by targeting the inhibition of Cutibacterium acnes. Importantly, doxycycline hydrochloride tablets (DHT) carries a lower risk of developing resistance compared to other antibiotics. However, due to the prolonged treatment duration required for moderate-to-severe AV, patients need long-term administration of DHT. This not only increases the risk of adverse effects such as nausea, vomiting, and dizziness but also predisposes them to relapse after discontinuation.9 Alternative therapies, such as retinoids combined with benzoyl peroxide, are used to enhance efficacy. Nevertheless, their application remains limited by factors including drug adverse effects and treatment costs.10,11 Based on current evidence-based medicine, clinical practice guidelines explicitly recommend against monotherapy with antibiotics and strongly emphasize the clinical necessity of combination therapy.12 Therefore, this study employed a combination therapy regimen as the treatment method for the intervention group.
Acupuncture, as a traditional Chinese medical (TCM) therapy, is widely used to treat various diseases, including acne, demonstrating favorable short-term and long-term efficacy.13 Fire needle therapy is a distinctive external treatment modality within acupuncture therapy, possessing unique advantages for treating AV through the principle of “internal disease treated by external application”. It achieves efficacy through meridian and collateral transmission and acupoints stimulation.14 Notably, our clinical team has observed that fire needle pretreatment can enhance the therapeutic efficacy of DHT for moderate-to-severe AV. Specifically, Fire needle therapy involves rapidly inserting a specially designed and heated-to-red needle into the specific acne papules and nodules on the face and swiftly withdrawing it. Its mechanism of action combines the stimulation of the needle with the thermal energy of moxibustion, aiming to induce inner heat toxin with the heated needle, expel pathogens and purge toxins, dredge meridians and activate collaterals, soften hard masses and dissipate nodules, achieving the effects of removing necrotic tissues and promoting tissue regeneration. It is widely used for the pretreatment of papules, scars, and pustules.15,16 According to the TCM treatment principle of “ using heat to induce heat”, fire needle can reduce the elevated osmotic pressure caused by tissue edema, thereby exerting anti-inflammatory effects.17 Clinical trials have shown that fire needle can reduce skin lesions and improve quality of life in AV patients.13,18 Collectively, fire needle therapy is effective for treating moderate-to-severe AV, exhibiting minimal systemic side effects and a lower recurrence rate. It can therefore serve as a complementary and alternative treatment approach. However, the current evidence supporting the efficacy of fire needle for moderate-to-severe AV is not yet sufficient to fully support its routine use in clinical practice.
The pathogenesis and progression of AV are frequently accompanied by a significant inflammatory response. As inflammation intensifies, the follicular wall may rupture, allowing sebum, microorganisms, and other contents to disseminate into the deeper dermis. This process can trigger folliculitis and perifolliculitis, clinically manifesting primarily as the formation of deep-seated cysts and nodules.19,20 Modern medical research indicates that the inflammatory response in AV is closely associated with Cutibacterium acnes.21 As a Gram-positive anaerobic bacterium, it activates keratinocytes primarily through Toll-like receptor 2 (TLR2) and, to a lesser extent, through Toll-like receptor 4 (TLR4), inducing the production of pro-inflammatory cytokines, thereby initiating the inflammatory cascade in acne.22 Studies demonstrate that the inflammatory cytokines TNF-α, IL-6, and IL-17 play pivotal roles in the pathogenesis of AV.23–28 Notably, an imbalance in the immune homeostasis between T helper 17 (Th17) cells and regulatory T (Treg) cells also plays a significant role in the pathological process of AV.29 Studies have confirmed that Th17/Treg imbalance can further activate inflammatory cells to secrete pro-inflammatory cytokines, driving the upregulation of key inflammatory factors, including TNF-α, IL-6, and IL-17, ultimately propelling AV towards progression as a chronic inflammatory disease.30
The objective of our randomized controlled trial (RCT) is to evaluate the effects of fire needle therapy combined with DHT on skin lesion severity, life quality, and serum inflammatory cytokine levels in patients with moderate-to-severe AV.
Materials and Methods
Study Design
From May 2022 to September 2024, recruitment of university students was conducted at the Dayitang Outpatient Department of Shanxi University of Chinese Medicine through posters and online announcements. The study protocol complied with the ethical principles of the 1975 Declaration of Helsinki and was approved by the Ethics Review Committee of Shanxi University of Chinese Medicine (Approval No.: 2019LL160). The trial was registered with the Chinese Clinical Trial Registry (Registration No.: ChiCTR2100045564). All participants provided written informed consent.
Participants
Diagnostic criteria for AV were established with reference to the relevant standards outlined in the Clinical Diagnosis and Treatment Guidelines: Dermatology and Venereology Volume.31 (1) The disease more common among adolescents and young adults, primarily involving seborrheic areas such as the face, forehead, chest, and back.
(2) Typical skin lesions include open comedones (blackheads), closed comedones (whiteheads), and various inflammatory lesions such as inflammatory papules, papulopustules, pustules, nodules, and cysts. (3) Patients may experience mild itching or pain. (4) The disease follows a chronic course, and PIH or scar formation after healing.
Diagnosis of Moderate-to-Severe AV employed the Pillsbury classification standard:32 Grade II (Moderate): Presence of comedones and a moderate number of papules and pustules, with a total skin lesion count between 31 and 50; Grade III (Severe): Presence of numerous papules and pustules, widely distributed, with a total skin lesion count between 51 and 100, and fewer than 3 nodules; Grade IV (Severe): Presence of nodular, cystic, or conglobate acne, with a total lesion count exceeding 100, and more than 3 nodules or cysts.
Inclusion criteria were as follows: (1) Met the above diagnostic criteria, presenting with clinical manifestations of moderate or severe AV, such as erythematous papules, pustules, nodules, or cysts; (2) Aged between 18 and 27 years, regardless of gender; (3) Agreed to participate in the study and provided written informed consent.
Exclusion criteria were as follows: (1) Pregnant or lactating women; (2) Individuals with coagulation disorders, hepatic or renal dysfunction, skin allergies, or a history of photosensitivity; (3) Individuals with concomitant internal, surgical, or gynecological diseases requiring chronic medication use. (4) Individuals with cognitive impairment. (5) Individuals with psychiatric disorders. (6) Individuals with a predisposition to hypertrophic scarring or keloid formation. (7) Individuals with needle phobia or a history of vasovagal syncope triggered by acupuncture. (8) Individuals with a history of autoimmune dysfunction.
Sample Size
Based on preliminary clinical observations (86% effective rate in the intervention group and 55% in the control group), sample size calculation was performed using PASS software version 11.0.4 (NCSS, USA). Setting a two-sided alpha level (α) of 0.05 and a statistical power of 80%, the analysis determined a requirement of 30 patients per group. Accounting for an anticipated 15% dropout rate, a final sample size of 70 patients was enrolled.
Randomization and Grouping
A total of 70 AV patients were enrolled in this study. Randomization was implemented using SPSS 26.0 to generate a random number table Participants were randomly allocated in a 1:1 ratio to respectively the intervention group (n=35) or the control group (n=35). All eligible patients who completed screening were assigned a unique randomization ID according to the generated sequence. Allocation concealment was ensured by having a research assistant independent of patient recruitment and outcome assessment encode the treatment assignments. The corresponding allocation information was sealed within sequentially numbered, opaque envelopes. The actual treatment procedures were administered by licensed physicians with extensive clinical experience, who opened the envelopes in sequential order and implemented the assigned intervention accordingly. To effectively control for measurement bias, all outcome assessors remained blinded to group assignment throughout the entire study duration.
Intervention Protocols
The control group only received DHT treatment, consisting of two components: (1) Facial cleansing: once-daily cleansing with an antimicrobial facial cleanser; (2) Medication: oral DHT (Active ingredient: doxycycline hydrochloride; Chemical name: 6-methyl-4- (dimethylamino) −3, 5, 10, 12, 12a, -pentahydroxy-1, 11-dioxo-1, 4, 4a, 5, 5a, 6, 11, 12a-octahydro-2-benzo [d] tetrabenzamide hydrochloride semi-ethanol hemihydrate; Hebei Dongfeng Pharmaceutical Co., Ltd)., 100 mg per dose, twice daily (administered after breakfast and dinner). Efficacy was assessed at the 4-week and 8-week treatment marks.
The intervention group received oral DHT plus fire needle therapy applied to lesion sites. Procedures are as follows: Participants assumed a suitable position, fully exposing facial or upper back lesion areas. The lesion sites underwent routine disinfection. A Panlong fine fire needle (0.5 mm diameter, 45 mm length; Beijing Luoyashanchuan Medical Devices Co., Ltd.) was selected. Heated the anterior two-thirds of the needle shaft until glowing red and then rapidly inserted it perpendicularly into the target lesion (pustule, nodule, or cyst) and immediately withdrawn. Insertion depth aimed to penetrate the lesional tissue and each lesion was treated with 2–3 punctures, carefully avoiding the danger triangle of the face. Following puncture, a sterile cotton swab was used to apply gentle pressure, expressing contents (pus, sebaceous plugs, bloody discharge) from comedones, papules, or pustules. Patients were instructed to avoid water contact at the puncture sites for 24 hours post-treatment. Fire needle therapy was administered once weekly and efficacy was assessed at the 4-week and 8-week treatment marks.
Throughout the treatment period, all participants were instructed to: (1) Maintain a light diet (avoiding spicy and greasy foods); (2) Refrain from using cosmetics; (3) Apply strict sun protection measures. (4) Strictly prohibit self-extraction of comedones by hand to avoid the risk of secondary infection.
Outcomes
Primary Outcomes
(1) Global Acne Grading System (GAGS)33
The GAGS was employed to assess acne severity. Patient facial photographs were captured using a digital camera (Canon X5, Tokyo, Japan) for counting papules and nodules. GAGS assessments were conducted at baseline, week 4, and week 8. The assessment area was divided into 6 regions with assigned base scores: the forehead, the left and right cheek areas (2 points each), the nasal area and the mandibular area (1 point each), and the chest and back (3 points). The scoring criteria for skin lesions are as follows: no skin lesions are scored as 0 points, and comedones, papules, pustules and nodules are scored as 1, 2, 3 and 4 points respectively. The final score of each partition is obtained by multiplying the score of the most severe skin lesion type in that area by the basic score of that area. The sum of the scores of all partitions is the total skin lesion score of the patient (ranging from 0 to 44 points). The classification criteria are as follows: 1 to 18 points are mild; 19 to 30 points are moderate; 31 to 38 points are severe; over 39 points are extremely severe. The higher the score, the more severe the skin lesion.
Secondary Outcomes
(1) échelle d’évaluation clinique des cicatrices d’acné (ECCA) grading scale34
The ECCA grading scale was employed to systematically evaluate scar characteristics at baseline, week 4, and week 8 post-treatment with a standardized questionnaire. The questionnaire comprised: (1) Scar Type Assessment (a-value): Icepick scars, Punched-out, V-shaped, diameter < 2 mm, Weight 15 points; Boxcar scars: Sharply demarcated, U-shaped, diameter 2–4 mm, Weight 20 points; Rolling scars: Superficial, undulating, W-shaped, diameter > 4 mm, Weight 25 points. (2) Scar Density Assessment (b-value): 3 points for more than 20 scars; 2 points for 5 to 20 scars; 1 point for less than 5 scars; 0 points for no scars. Total ECCA Score = a-value × b-value for each scar type present. The total score is the sum of all the weights. A higher total score indicates greater scar severity.
(2) Dermatology Life Quality Index (DLQI)35
The DLQI was administered via a structured questionnaire to systematically assess the impact on life quality across 10 domains: Symptoms and physical sensations; Psychological state (feelings); Daily activities; Social and leisure activities; Sports or physical activities; Work or study; Personal relationships (family/partner/friends); Sexual quality; Problems with treatment; Overall impact of skin condition. The assessment time points include the baseline period, 4 weeks of treatment and 8 weeks of treatment. The scoring criterion adopts a 4-level Likert scale (no effect =0 points, slight effect =1 point, moderate effect =2 points, severe effect =3 points). Each domain scored independently and then accumulated, with the total score range being 0 to 30 points. A higher total score indicates a greater negative impact on quality of life.
(3) Serum Cytokine Levels: IL-17, TNF-α, IL-6
Serum levels of IL-17, TNF-α, and IL-6 were quantitatively measured with Enzyme-Linked Immunosorbent Assay (ELISA): Fasting venous blood samples (5 mL) were collected from the antecubital vein of participants in both groups before treatment, at week 4, and at week 8. Blood samples were allowed to clot at room temperature for 30 minutes, then centrifuged at 4°C, 3000 rpm (with a centrifugation radius of 8 cm) for 10 minutes to separate serum. Assays were performed strictly according to the manufacturer’s instructions of the respective ELISA kits. Absorbance was measured at 450 nm using a microplate reader. And the serum concentrations of IL-17, TNF-α, and IL-6 were determined based on the standard curve.
Adverse Events
Adverse events occurring during the treatment period were recorded and monitored in both groups.
Statistical Analysis
Statistical analyses were performed using SPSS 26.0. The research data include two types, categorical data and quantitative data. The categorical data were analyzed using Pearson’s chi-square test. The quantitative data following a normal distribution were presented as mean ± standard deviation (SD) and homogeneity of variance was assessed. If variances were equal, independent samples t-test was used; If variances were unequal, non-parametric tests were used. Quantitative data following a non-normally distributed data were expressed as median and the upper and lower quartiles [M(P25, P75)], and a non-parametric test method was adopted. The threshold for statistical significance was set at P<0.05 for all tests.
Results
Baseline Characteristics
A total of 90 patients with moderate-to-severe AV were initially recruited. Of these, 9 did not meet the inclusion criteria, 5 declined participation, and 6 withdrew due to concomitant serious medical conditions. Consequently, 70 eligible patients were ultimately enrolled and randomly allocated into two groups (n=35 per group). A detailed flowchart of the study design is provided in Figure 1 and Table 1 presents the participants’ demographic characteristics, relevant AV history, and clinical classification. No statistically significant differences (all P>0.05) were observed between the two groups in baseline characteristics, including age, gender, BMI, preference for spicy or greasy foods, regularity of daily routine, disease duration, and AV severity. This indicates comparability between the groups.
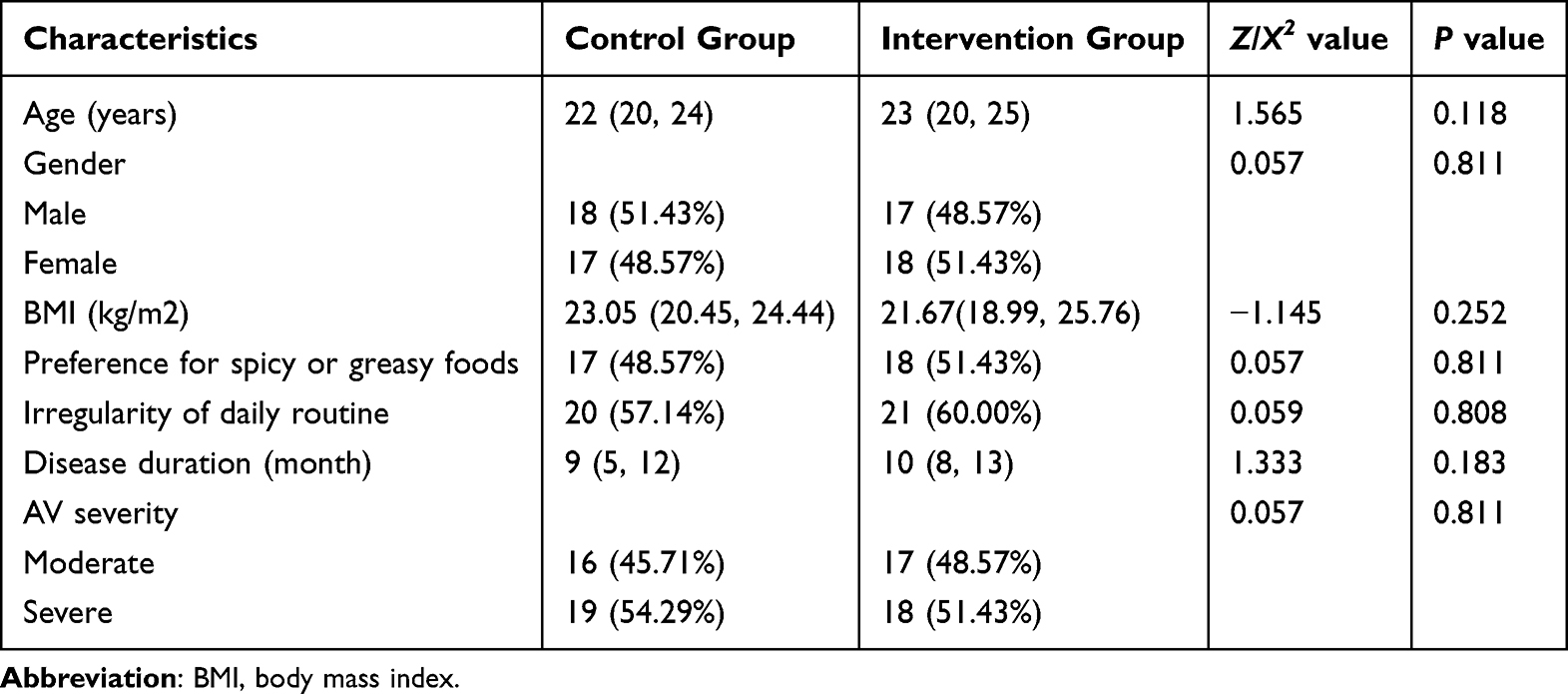 |
Table 1 Baseline Characteristics of Included Participants |
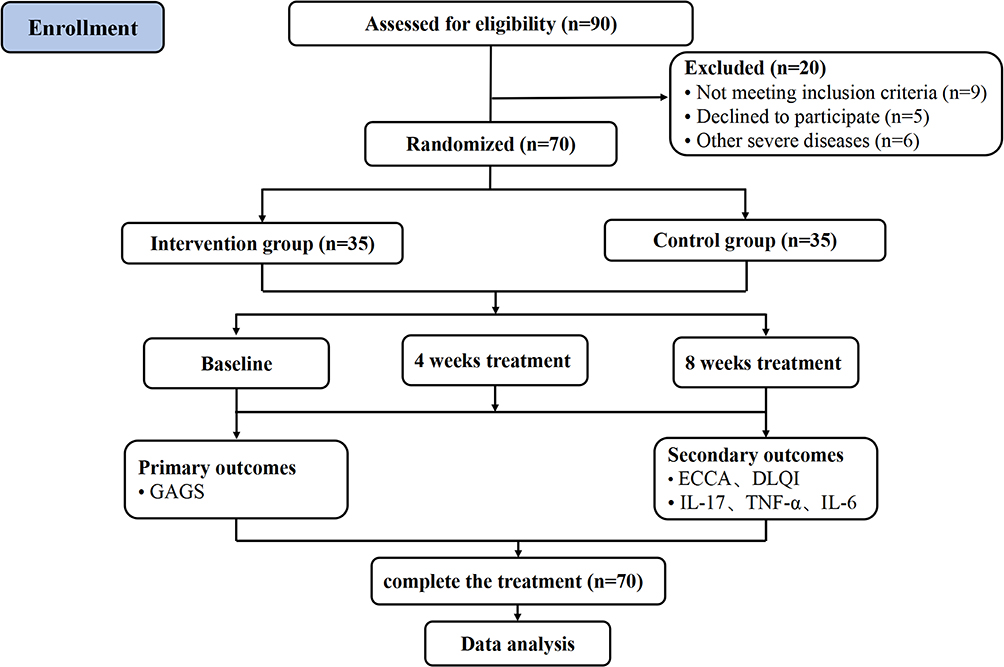 |
Figure 1 Flowchart of clinical trial design. Abbreviation: GAGS, global acne grading system; DLQI, dermatology life quality index; ECCA, échelle d’évaluation clinique des cicatrices d’acné; IL-17, interleukin-17; TNF-α, tumor necrosis factor-α; IL-6, interleukin-6. |
Primary Outcomes
GAGS scores were used to assess skin lesion improvement in patients with moderate-to-severe AV at 4 and 8 weeks post-treatment (Figure 2A and B), for which the patient provided written informed consent for publication. Baseline data indicated no statistically significant difference in GAGS scores between the two groups (P=0.306). Following treatment, both groups demonstrated statistically significant reductions in GAGS scores at both week 4 and week 8 compared to their respective baseline levels (Table 2). Notably, the intervention group exhibited significantly greater reductions in GAGS scores than the control group at both week 4 and week 8 (all P<0.001) (Figure 2B). This result indicates superior clinical efficacy of the fire needle therapy combined with DHT regimen in improving lesion symptoms. Furthermore, compared to the effects observed at week 4, both groups showed significantly more pronounced therapeutic effects at week 8, and this difference was statistically significant (all P<0.001).
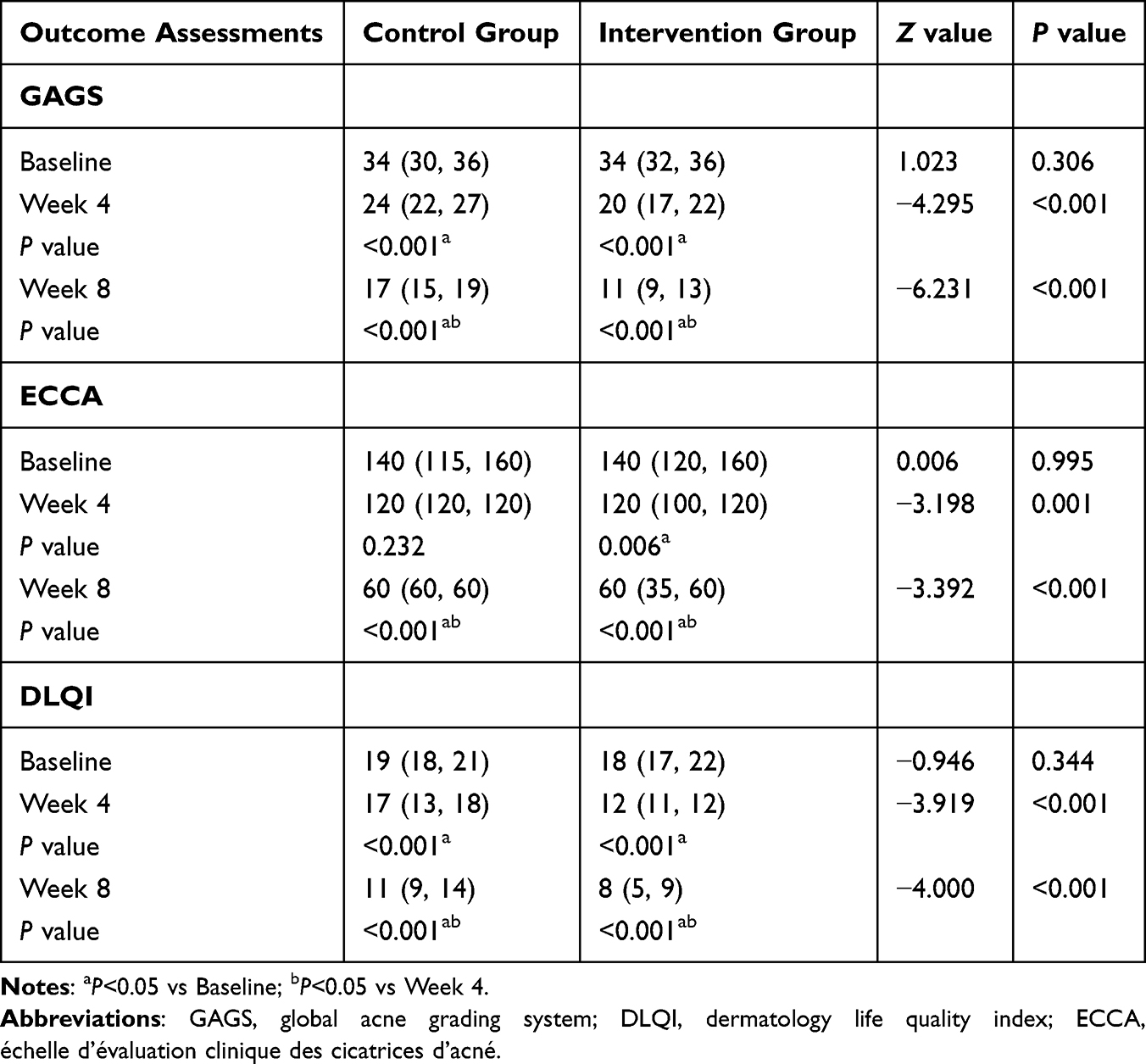 |
Table 2 Comparison of GAGS, ECCA, and DLQI Scores Before and After Treatment in Two Groups |
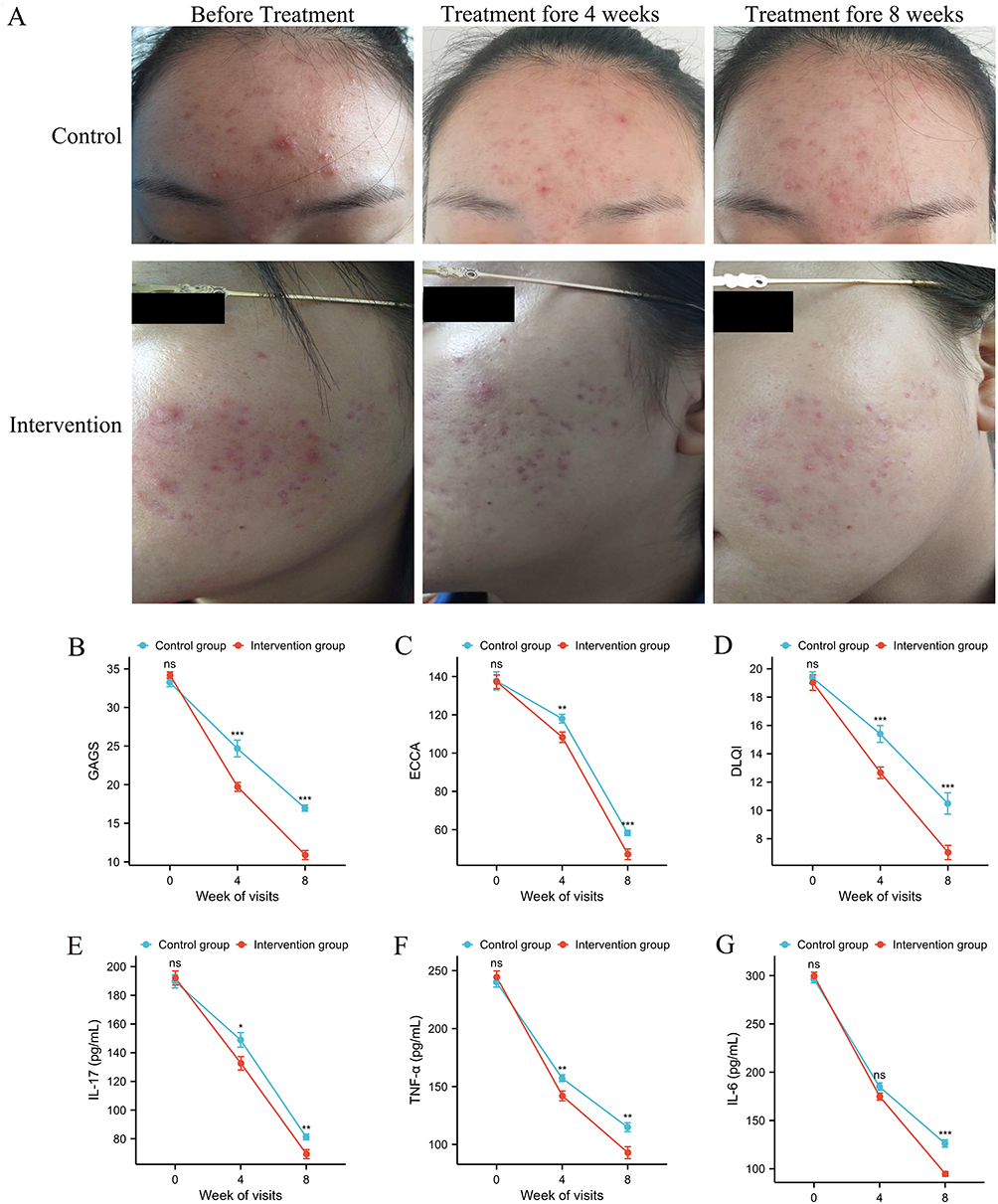 |
Figure 2 Comparison of facial images (A) GAGS (B) ECCA (C) DLQI (D) IL-17 (E) TNF-α (F) and IL-6 (G) before and after treatment in two groups. Written informed consent was obtained from the patient for publication of this figure. nsP>0.05, *P<0.05, **P<0.01, ***P<0.001 vs Control group. Abbreviation: GAGS, global acne grading system; DLQI, dermatology life quality index; ECCA, echelle d’evaluation clinique des cicatrices d’acne; IL-17, interleukin-17; TNF-α, tumor necrosis factor-α; IL-6, interleukin-6. |
Secondary Outcomes
Secondary outcomes in this study included the ECCA scar score, DLQI score, and levels of the inflammatory cytokines IL-17, TNF-α, and IL-6. As shown in Table 2, Figure 2C and D, both ECCA and DLQI scores demonstrated greater reductions in the intervention group compared to the control group. Scores decreased from baseline to week 4 and further to week 8. This indicates that the combination of fire needle therapy with DHTsignificantly reduced both ECCA and DLQI scores at weeks 4 and 8 (all P<0.001). Notably, the decline in DLQI scores was more rapid at week 4, followed by gradual attenuation by week 8. Significantly lower scores were observed in the intervention group for both ECCA and DLQI compared to the control group at both week 4 and week 8 (all P<0.01).
Table 3 and Figure 2E–G detailed the dynamic changes in serum inflammatory cytokine levels (IL-17, TNF-α, and IL-6) for both groups. Compared to baseline levels, significant decreases in IL-17, TNF-α, and IL-6 levels were observed in both groups at weeks 4 and 8 post-treatment. Further between-group analysis at week 8 revealed statistically significant differences: IL-17: P=0.008; TNF-α: P=0.006; IL-6: P<0.001.
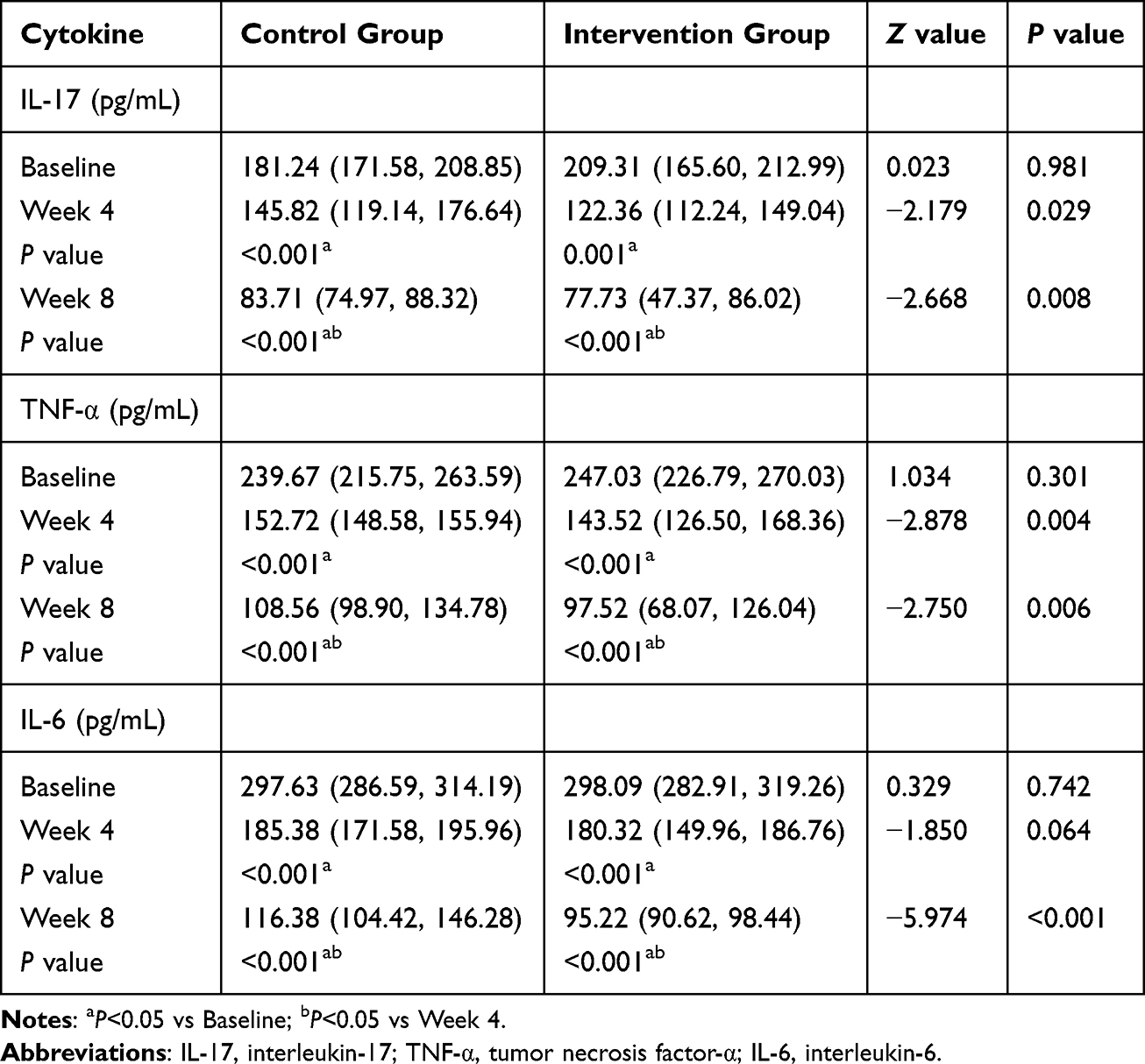 |
Table 3 Comparison of Serum Inflammatory Factors IL-17, TNF-Α and IL-6 Before and After Treatment in Both Groups |
Adverse Events
All patients in the intervention group experienced varying degrees of pain during fire needle therapy. Localized edema or minor bleeding was observed at the treatment site in 10 patients. Notably, edema following treatment of papules and pustules typically subsided within 0.5–1 hour while edema associated with nodules and cysts generally resolved within 12 hours. Two patients in the intervention group developed nausea and vomiting after taking DHT. These symptoms resolved within one week after discontinuation of the medication. In the control group, five patients reported nausea and vomiting associated with DHTadministration. Similarly, these symptoms resolved within one week after stopping the medication. Importantly, no serious adverse events occurred during or after the treatment period in either group.
Discussion
This study systematically evaluated the clinical efficacy of fire needle therapy combined with DHT for moderate-to-severe AV across four dimensions: skin lesion severity, acne scarring, life quality, and serum inflammatory cytokine levels (Figure 3). The GAGS served as the standard tool to assess lesion extent, the ECCA scale quantified changes in scar type and density, and the DLQI evaluated the impact of AV on patients’ life quality. The results indicate that fire needle therapy combined with DHT demonstrated superior efficacy compared to DHT monotherapy in patients with moderate-to-severe AV, as evidenced by significantly lower GAGS, ECCA, and DLQI scores at both the 4-week and 8-week marks. Notably, fire needle therapy exhibited a marked cumulative effect after 8 weeks, substantially diminishing the negative impacts of AV on quality of life and enhancing patient well-being. Crucially, the imbalance of pro-inflammatory cytokines (TNF-α, IL-6, IL-17) plays a pivotal role in local AV inflammation. Clinical research indicates that fire needle therapy effectively suppresses the chemotactic activity of inflammatory factors like IL-1, TNF-α, IL-17, and IL-6, thereby mitigating PIH and scar formation.36,37 Our clinical data further corroborate that serum levels of TNF-α, IL-6, and IL-17 were significantly reduced after 4 and 8 weeks of combined fire needle and DHT therapy. This reduction is likely mechanistically linked to the observed skin lesion improvement. This suggests that the combination therapy’s ability to decrease serum levels of these key inflammatory cytokines constitutes a vital mechanism underlying its efficacy in reducing local inflammation, promoting lesion repair, improving scar symptoms, and enhancing overall therapeutic outcomes.
 |
Figure 3 Fire needle therapy combined with DHT may enhance life quality of patients with moderate-to-severe AV by inhibiting the release of serum inflammatory factors (IL-17, TNF-α, IL-6), reducing local inflammation, promoting lesion repair, and improving scar symptoms. |
Both treatment groups received DHT, a broad-spectrum antibiotic known for its excellent lipophilicity, enabling penetration into the pilosebaceous unit and achieving high local skin concentrations. DHT effectively mitigates AV inflammation primarily by inhibiting the growth and proliferation of Cutibacterium acnes. Additionally, it reduces sebaceous gland size, suppresses sebaceous gland activity, decreases sebum production, and alleviates follicular hyperkeratosis.38,39 The key distinction between the regimens was the addition of fire needle therapy in the intervention group. Results revealed a significant advantage for the intervention group in both lesion improvement and inflammation control. Compared to the control group, the intervention group demonstrated superior efficacy in resolving papules, pustules, nodules, and cysts, highlighting the therapeutic superiority of the combination approach. When used together, fire needle therapy and DHT exhibit synergistic effects, collectively promoting acne resolution and skin repair while shortening the inflammation resolution time. While the control group demonstrated efficacy in reducing AV lesions, it was less effective than the intervention group in suppressing PIH and scar formation, which is the challenging aspects of acne management. Our findings revealed a significantly greater reduction in ECCA scores within the intervention group, indicating markedly less PIH and scar formation post-treatment. This enhanced benefit is related to the multiple effects of fire needle therapy combined with DHT treatment. Previous studies suggest fire needle therapy may inhibit scar formation by stimulating skin collagen fibers under high-temperature conditions, thereby activating tissue repair mechanisms.40 Related research also confirms that fire needle therapy can stimulate the immune system to release Vascular Endothelial Growth Factor (VEGF), promoting wound healing, improving facial microcirculation, accelerating inflammation resolution, and fostering collagen regeneration, ultimately reducing scar formation.41 Thus, the combination of fire needle therapy and DHT offers a comprehensive approach: DHT combats bacteria and inflammation internally, while fire needle therapy externally disrupts the bacterial microenvironment within acne lesions, promotes inflammation resolution and tissue regeneration. These modalities act synergistically, effectively reducing PIH and scar formation, demonstrating superior therapeutic outcomes and a distinct synergistic advantage.
The development and progression of AV are frequently accompanied by clinical manifestations such as scarring, pustules, and nodules, which persistently impair patients’ life quality. Severe acne can significantly affect appearance and even induce psychological distress.42 The results of this study demonstrate that compared to baseline levels, the intervention group exhibited the most significant therapeutic effects after both 4 and 8 weeks of treatment, effectively reducing inflammatory lesions like papules and pustules. Furthermore, at the 8-week mark, the intervention group showed significantly lower scores than the control group in specific DLQI dimensions: symptoms and physical sensations (itch/pain), feelings (embarrassment), daily activities, social and leisure activities, personal relationships, and treatment problems. This strongly suggests that the combination of fire needle therapy and DHT significantly improves patients’ life quality, likely attributable to the regimen’s superior efficacy in alleviating clinical symptoms. Importantly, no serious adverse events occurred in either group during treatment, indicating that the combination therapy did not increase the risk of adverse reactions. Evidence indicates that common adverse effects of DHT primarily include gastrointestinal reactions such as nausea and vomiting.43 These symptoms typically diminish with continued use and resolve spontaneously upon discontinuation, requiring no special intervention, thus highlighting the favorable safety profile of DHT. Concurrently, the addition of fire needle therapy facilitates rapid symptom relief, potentially reducing cumulative drug exposure and shortening the treatment duration. Consistent with prior research, our study confirms the synergistic effect of fire needle and doxycycline.44 Therefore, this combined regimen demonstrates a favorable safety profile.
The primary pathogenic mechanisms of acne are widely recognized as excessive sebum production, abnormal keratinization of the hair follicle and sebaceous duct, inflammation, bacterial overgrowth, and hormonal dysregulation.45 Current research confirms that Cutibacterium acnes play as the principal pathogenic bacterium in AV, which could activate monocytes via TLR2, triggering the release of pro-inflammatory cytokines such as IL-6, IL-17, TNF-α, and other inflammatory mediators, thereby initiating inflammatory acne lesions.45 Our results revealed significantly elevated serum levels of TNF-α, IL-6, and IL-17 in patients with moderate-to-severe AV at baseline. Following 4 and 8 weeks of intervention, the treatment group exhibited significant reductions in serum TNF-α and IL-17 levels compared to baseline, with the magnitude of improvement being significantly greater than that in the control group. Notably, though the reduction in IL-6 levels at week 4 showed no significant difference between groups, the intervention group demonstrated a significantly greater reduction in IL-6 compared to the control group at week 8. These findings suggest that fire needle therapy combined with DHT exerts its therapeutic effects, by suppressing the expression of serum TNF-α, IL-6, and IL-17, thereby effectively mitigating the inflammatory response in AV. Further mechanistic analysis indicates that the combination of fire needle therapy and DHT greatly suppresses excessive cellular immune activation. This leads to reduced recruitment and activation of inflammatory cells, decreased release of inflammatory mediators, and consequently, interruption of the excessive inflammatory response and immune-mediated tissue damage characteristic of AV progression, ultimately alleviating inflammatory lesions. For patients with moderate-to-severe AV, the combination regimen not only effectively reduces inflammatory cytokine levels but also modulates endocrine function, significantly improves clinical acne symptoms, and enhances overall therapeutic efficacy. Mechanistically, fire needle therapy utilizes its thermal effects to directly kill pathogenic microorganisms like Cutibacterium acnes and disrupt their microenvironment, inhibiting pathogen proliferation.46 The mechanical stimulus of the needle dilates the follicular opening, facilitating the expulsion of sebum and inflammatory debris, thereby accelerating local inflammation resolution.47 Additionally, fire needle directly damages the cyst wall and surrounding connective tissue in nodular-cystic acne, promoting tissue repair and achieving the effects of removing necrotic tissue and promoting granulation, ultimately improving the pathological skin condition.36
This study demonstrated that both fire needle therapy combined with DHT and DHT monotherapy effectively alleviated clinical symptoms and improved quality of life in patients with moderate-to-severe AV. However, several limitations warrant consideration: First, as a single-center study with a relatively small sample recruited solely from a university campus, the findings primarily reflect characteristics of this specific population. The generalizability to broader populations in other regions or countries requires further validation. Second, fire needle therapy, as a complex intervention, may involve placebo effects and patient expectancy. Employing a waitlist (no treatment) control group in future studies could serve as a more suitable reference standard, helping to mitigate bias from spontaneous AV resolution and allowing a more accurate assessment of fire needle efficacy. Third, due to the special procedures of fire needle administration, practitioners could not be blinded, introducing a potential source of bias. At last, the relatively high dropout rate caused by the impact of the COVID-19 pandemic may also cause certain deviations in the research results.
To address these limitations, future research should implement the following improvements: First, employ large-sample, multi-center randomized controlled trials to enhance generalizability and statistical power; Second, incorporate a sham fire needle (placebo) control group to control for placebo effects and spontaneous resolution bias; Third, strictly implement blinding of outcome assessors and actively explore patient blinding strategies (eg, using sham fire needle) to minimize bias arising from the lack of practitioner blinding; Fourth, optimize follow-up protocols (combining remote and on-site assessments) and utilize intention-to-treat (ITT) analysis principles coupled with advanced missing data handling techniques to manage high attrition rates; Last but not least, include long-term efficacy follow-up data and explore underlying mechanisms, such as relevant inflammatory biomarkers, to comprehensively and scientifically evaluate the clinical efficacy and mechanisms of fire needle therapy for AV.
Conclusion
This study demonstrated that an 8-week regimen of fire needle therapy combined with DHT improved lesion severity, scar symptoms, quality of life, and serum inflammatory cytokine levels in patients with moderate-to-severe AV compared to DHT monotherapy. The results indicate that the combination therapy is significantly efficacious in alleviating AV lesions, enhancing life quality, and reducing inflammatory cytokine levels. Given its favorable safety profile and synergistic effects with DHT, fire needle therapy offers a practical clinical advantage as an adjunct to conventional DHTtreatment for moderate-to-severe AV. Further studies are warranted to validate these benefits and provide a robust evidence base for clinical decision-making and broader implementation.
Abbreviations
AV, Acne vulgaris; DHT, Doxycycline hydrochloride tablets; GAGS, Global acne grading system; ECCA, échelle d’évaluation clinique des cicatrices d’acné; DLQI, Dermatology life quality index; IL-17, Interleukin-17; TNF-α, Tumor necrosis factor-α; IL-6, Interleukin-6.
Clinical Registration
The trial was registered with the Chinese Clinical Trial Registry (Registration No.: ChiCTR2100045564).
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study protocol complied with the ethical principles of the 1975 Declaration of Helsinki and was approved by the Ethics Review Committee of Shanxi University of Chinese Medicine (Approval No.: 2019LL160).
Acknowledgments
We sincerely thank all the participants for their efforts in this study.
Funding
This study was supported by funds from the Natural Science Foundation of China (82205280) and the Shanxi University of Traditional Chinese Medicine Science and Technology Innovation Ability Cultivation Plan Project (2019PY-078).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. What is acne? Pediatr Dermatol. 2025;42(2):389. doi:10.1111/pde.15934
2. Deng Y, Wang F, He L. Skin barrier dysfunction in acne vulgaris: pathogenesis and therapeutic approaches. Med Sci Monit. 2024;30(e945336). doi:10.12659/MSM.945336
3. Del Rosso JQ, Kircik L. The primary role of sebum in the pathophysiology of acne vulgaris and its therapeutic relevance in acne management. J DermatolTreat. 2024;35(1):2296855. doi:10.1080/09546634.2023.2296855
4. Zhang H, Zhang Z. Genetic variants associated with acne vulgaris. Int J Gen Med. 2023;16:3843–3856. doi:10.2147/IJGM.S421835
5. Morshed ASM, Noor T, Uddin Ahmed MA, et al. Understanding the impact of acne vulgaris and associated psychological distress on self-esteem and quality of life via regression modeling with CADI, DLQI, and WHOQoL. Sci Rep. 2023;13(1):21084. doi:10.1038/s41598-023-48182-6
6. Eichenfield DZ, Sprague J, Eichenfield LF. Management of acne vulgaris: a review. JAMA. 2021;326(20):2055–2067. doi:10.1001/jama.2021.17633
7. Van Steensel MAM. The genetics of acne. Ann Hum Genet. 2025;89(5):333–341. doi:10.1111/ahg.70014
8. Dessinioti C, Dreno B. Acne treatments: future trajectories. Clin Exp Dermatol. 2020;45(8):955–961. doi:10.1111/ced.14239
9. Auffret N, Leccia MT, Ballanger F, et al. Acne-induced post-inflammatory hyperpigmentation: from grading to treatment. Acta Derm Venereol. 2025;105(adv42925). doi:10.2340/actadv.v105.42925
10. Habeshian KA, Cohen BA. Current issues in the treatment of acne vulgaris. Pediatrics. 2020;145(Suppl 2):S225–S230. doi:10.1542/peds.2019-2056L
11. Al Muqarrab F, Almohssen A. Low-dose oral isotretinoin for the treatment of adult patients with mild-to-moderate acne vulgaris: systematic review and meta-analysis. Dermatol Ther. 2022;35(4):e15311. doi:10.1111/dth.15311
12. Geng R, Sibbald RG. Acne vulgaris: clinical aspects and treatments. Adv Skin Wound Care. 2024;37(2):67–75. doi:10.1097/ASW.0000000000000089
13. Chun-Yan C, Guang-Yao X, Yan-Yan S, et al. Acupuncture: a therapeutic approach against acne. J Cosmet Dermatol. 2021;20(12):3829–3838. doi:10.1111/jocd.14487
14. Guleria P, Joshi S, Parmar S, et al. Decoding acne vulgaris: insights into pathogenesis, treatment modalities, diagnosis and recent advancements. Recent Adv Inflamm Allergy Drug Discov. 2025;19(1):18–30. doi:10.2174/0127722708312980240718093537
15. Xu W, Xu J, Huang D, et al. Acne vulgaris: advances in pathogenesis and prevention strategies. Eur J Clin Microbiol Infect Dis. 2025;44(3):515–532. doi:10.1007/s10096-024-04984-8
16. Bhatt J, Kumar VJ, Chahat. “Acne vulgaris: key insights, treatment, and future prospects”. Mol Divers. 2025;2025. doi:10.1007/s11030-025-11209-3
17. Palmieri SA. Acne vulgaris in children and adolescents: what’s the cause and how to combat it. J Pediatr Pharmacol Ther. 2025;30(3):401–406. doi:10.5863/JPPT-25-01205
18. Jiao R, Zhai X, Zhang X, et al. Efficacy of acupuncture in improving symptoms and quality of life of patients with acne vulgaris: a randomized sham acupuncture-controlled trial. Acupunct Med. 2022;40(5):453–462. doi:10.1177/09645284221076506
19. Lu W, Zhu L, Tian Q, et al. Effect of acupoint catgut embedding, fire needle, auricular acupuncture on female post-adolescent acne and serum sex hormone. Zhongguo Zhen Jiu. 2018;38(8):833–838. doi:10.13703/j.0255-2930.2018.08.010
20. Tang L, Fu Q, Zhou ZW, et al. A systematic review and meta-analysis of randomized clinical trials of fire needle combined with ALA-PDT for the treatment of moderate-to- severe acne. Photodiagnosis Photodyn Ther. 2023;42:103200. doi:10.1016/j.pdpdt.2022.103200
21. Tang L, Zhou X, Su G. Successful treatment of a lactating women with severe acne through the combination of fire needle and photodynamic therapy: a case report. Photodiagnosis Photodyn Ther. 2024;48:104234. doi:10.1016/j.pdpdt.2024.104234
22. Hu HH, Li JH. Acne fulminans. N Engl J Med. 2024;391(15):1440. doi:10.1056/NEJMicm2406625
23. Heath CR, Usatine RP. Acne Vulgaris. Cutis. 2021;108(3):167. doi:10.12788/cutis.0339
24. Dréno B, Pécastaings S, Corvec S, et al. Cutibacterium acnes (Propionibacterium acnes) and acne vulgaris: a brief look at the latest updates. J Eur Acad Dermatol Venereol. 2018;32 Suppl 2:5–14. doi:10.1111/jdv.15043
25. Yuqiu L, Wenjia N, Guang L, et al. Research progress of acne-related receptors [J]. J Dermatol Venereol. 2025;32(06):449–454.
26. Piao X, Liu B, Guo L, et al. Picroside II shows protective functions for severe acute pancreatitis in rats by preventing NF-κB-dependent autophagy. Oxid Med Cell Longev. 2017;2017:7085709. doi:10.1155/2017/7085709
27. Hu L, Chen Y, Chen T, et al. A systematic study of mechanism of sargentodoxa cuneata and patrinia scabiosifolia against pelvic inflammatory disease with dampness-heat stasis syndrome via network pharmacology approach. Front Pharmacol. 2020;11:582520. doi:10.3389/fphar.2020.582520
28. Paulsson JM, Moshfegh A, Dadfar E, et al. In-vivo extravasation induces the expression of interleukin 1 receptor type 1 in human neutrophils. Clin Exp Immunol. 2012;168(1):105–112. doi:10.1111/j.1365-2249.2011.04548.x
29. Junyou L, Bai L, Jin W. Research progress in acne treatment [J]. Chinese J Leprosy Dermatol. 2025;41(07):533–537.
30. Sun JK, Zhang WH, Chen WX, et al. Effects of early enteral nutrition on Th17/Treg cells and IL-23/IL-17 in septic patients. World J Gastroenterol. 2019;25(22):2799–2808. doi:10.3748/wjg.v25.i22.2799
31. Bian Z. Chinese Clinical Dermatology [M]. Nanjing: Jiangsu Science and Technology Press; 2003:1165–1169.
32. Qiang J. Chinese acne treatment guidelines (2019 revised edition) [J]. J Clin Dermatol. 2019;48(09):583–588. doi:10.16761/j.cnki.1000-4963.2019.020
33. Doshi A, Zaheer A, Stiller MJ. A comparison of current acne grading systems and proposal of a novel system. Int J Dermatol. 1997;36(6):416–418. doi:10.1046/j.1365-4362.1997.00099.x
34. Dreno B, Khammari A, Orain N, et al. ECCA grading scale: an original validated acne scar grading scale for clinical practice in dermatology. Dermatology. 2007;214(1):46–51. doi:10.1159/000096912
35. Basra MK, Salek MS, Camilleri L, et al. Determining the minimal clinically important difference and responsiveness of the Dermatology Life Quality Index (DLQI): further data. Dermatology. 2015;230(1):27–33. doi:10.1159/000365390
36. Xing M, Yan X, Sun X, et al. Fire needle therapy for moderate-severe acne: a PRISMA systematic review and meta-analysis of randomized controlled trials. Complement Ther Med. 2019;44:253–260. doi:10.1016/j.ctim.2019.04.009
37. Qiaohui H, Junjie L, Meiying W. Observation on the clinical efficacy of fire needle combined with cyst acne prescription in the treatment of cystic acne. China Modern Drug Application. 2025;19(08):166–169. doi:10.14164/j.cnki.cn11-5581/r.2025.08.045
38. National Institute for Health and Care Excellence. Acne Vulgaris: Management (NICE Guideline NG198)[Z]. London: NICE; 2021:10.
39. Nottinghamshire Area Prescribing Committee. Acne Management Guideline. Nottingham: NAPC; 2023:2.
40. Zhang J, Lin P, Guo C, et al. Effects and safety of fire needle adjuvant chemical peels therapy in acne vulgaris: a systematic review and meta-analysis. J DermatolTreat. 2023;34(1):2240455. doi:10.1080/09546634.2023.2240455
41. Lirui Z, Cuilan Y, Yuxun W, et al. The expression and role of vascular endothelial growth factor in fire needle treatment of bedsore wound in mice. Shanghai J Acupuncture Moxibustion. 2012;2012:606–608.
42. Afsar FS, Seremet S, Demirlendi Duran H, et al. Sexual quality of life in female patients with acne. Psychol Health Med. 2020;25(2):171–178. doi:10.1080/13548506.2019.1679845
43. Zhao Z, Liu J, Huang J. Comparative study on the drug effects and adverse reactions of doxycycline and isotretinoin in the treatment of moderate to severe acne. Pak J Pharm Sci. 2025;38(1):71–75.
44. Dongmei Y, Juanjuan C. Clinical study on the treatment of moderate and severe acne by fire needle combined with doxycycline hydrochloride tablets. New Chin Med. 2025;57(12):120–125. doi:10.13457/j.cnki.jncm.2025.12.022
45. Li X, He C, Chen Z, Zhou C, Gan Y, Jia Y. A review of the role of sebum in the mechanism of acne pathogenesis. J Cosmet Dermatol. 2017;16(2):168–173. doi:10.1111/jocd.12345
46. Liu PF, Hsieh YD, Lin YC, et al. Propionibacterium acnes in the pathogenesis and immunotherapy of acne vulgaris. Curr Drug Metab. 2015;16(4):245–254. doi:10.2174/1389200216666150812124801
47. Du L, Cao Z, Wei J, et al. Fire needle pretreatment with 5-aminolevulinic acid photodynamic therapy combined with low-dose isotretinoin in the treatment of severe refractory nodulocystic acne. Photodiagnosis Photodyn Ther. 2024;47:104215. doi:10.1016/j.pdpdt.2024.104215
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.