")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Efficacy of Digitally Supported and Real-Time Self-Monitoring of Blood Glucose-Driven Counseling in Patients with Type 2 Diabetes Mellitus: A Real-World, Retrospective Study in North India
Authors Sabharwal M, Misra A, Ghosh A, Chopra G
Received 1 November 2021
Accepted for publication 16 December 2021
Published 5 January 2022 Volume 2022:15 Pages 23—33
DOI https://doi.org/10.2147/DMSO.S345785
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Mudit Sabharwal,1 Anoop Misra,2 Amerta Ghosh,2 Gautam Chopra1
1BeatO, Health Arx Technologies Pvt. Ltd., New Delhi, India; 2Fortis C-DOC Hospital, Center of Excellence for Diabetes, Metabolic Diseases, and Endocrinology, New Delhi, India
Correspondence: Mudit Sabharwal Email [email protected]
Purpose: Poor glycemic control is prevalent in patients with type 2 diabetes mellitus (T2DM) in India. This study aims to understand the effectiveness of a smartphone-connected glucometer, real-time feedback, and contextualized counseling on glycemic control and hypoglycemic episodes in T2DM patients.
Methods: This retrospective, multicenter study reviewed the medical records of T2DM patients belonging to several cities of north India, who were digitally engaged with a smartphone-connected glucometer and who had received at least one counseling session between September 2019 and July 2020. Intervention included self-monitoring of blood glucose (SMBG) using a smartphone-connected glucometer enabled with real-time transmission of information to certified diabetes educators (CDE) and their corresponding counseling based on SMBG findings.
Results: Of 7111 adult T2DM patients included in this study, majority (75%) of the patients received a single session of counseling, and the remaining patients received 2 (16.7%), 3 (5%), 4 (2%), or ≥ 5 (1.3%) sessions. The mean age of the patients was 51.6 years, and the majority (77.9%) were males. Digital monitoring of BG and counseling with CDE significantly reduced the mean fasting (by 9.6%), pre-prandial (by 9.9%), and post-prandial (by 9.2%) BG values in 53%, 52%, and 54% of patients, respectively. The majority (81.4%) of patients showed no hypoglycemic episode (≤ 70 mg/dL) post-counseling. The hypoglycemia episodes observed with FBG, pre-prandial, and post-prandial BG values were reduced significantly by 58.5%, 48.1%, and 61.8%, respectively, post-counseling.
Conclusion: Digitally supported and real-time SMBG-driven counselling was effective in glycemic control and reduction of hypoglycemic episodes in T2DM patients in India. Moreover, reduction in hypoglycemia may be due to back end real-time support of CDE intervention.
Keywords: type 2 diabetes mellitus, glucometer, glycemic control, self-monitoring of blood glucose, counseling
Introduction
The prevalence of diabetes remains high and continues to rise in India.1 According to the Global Burden Disease study,2 the prevalence of diabetes among adults (>20 years) has increased from 5.5% (1990) to 7.7% (2016) in India, and the number of people with diabetes is expected to double from 77 million in 2019 to 134.2 million in 2045.3 The crude death rate due to diabetes in India has increased by 131% between 1990 and 2016 from 10.0 to 23.1 per 100,000 population.2 However, given the sheer size of the diabetic population in India, combined with poor diabetes control (77% of patients have uncontrolled glycated hemoglobin [≥7%])4 without adequate primary care infrastructure,5 there is an unmet need to look at future models aided with technology for diabetes care. The fact that healthcare is primarily an out-of-pocket expense (71%)6 should also be taken into consideration in India, and relative to its per capita income, healthcare costs are very high, with ~25% of households having a catastrophic health expenditure equaling or exceeding 10% of their total household expenditure.1,7
Newer strategies must be devised to improve glycemic control in type 2 diabetes mellitus (T2DM) patients. Recently, technological developments such as artificial intelligence, machine learning, and digital interventions have emerged that can monitor patients’ blood glucose levels on a real-time basis.8 Artificial intelligence (AI) involves an automated process rather than manual monitoring and evaluations, which enable early detection and diagnosis of diabetes. AI-based techniques like case-based reasoning, machine learning, and artificial neural network facilitate self-management and improved decision-making.9 These AI technologies also embark on predicting diabetes, monitoring blood sugar, insulin injection and lifestyle guidance, and monitoring complications.10
It is essential to turn to digital tools and technologies that can enable remote monitoring and timely care at scale in a cost-effective manner, thereby reducing the burden both for the patients and the primary care infrastructure.11 This becomes even more pertinent in the present scenario with the prevailing COVID-19 pandemic, where people with underlying conditions such as diabetes are at a greater risk of adverse outcomes as they need to commute for most of their diabetes care and should avoid outdoor visits.12
Overall, the use of digital tools and technologies, including remote monitoring, tracking, real-time transmission of clinical information, and timely feedback, is suggested to have positive clinical outcomes and reduction in the overall management cost.13,14 Studies from the US, Europe, and China have demonstrated the effectiveness of digital health interventions (based on mobile/app usage and education/counseling) in improving glycemic control of diabetes patients.15–20 A US-based study assessed the effectiveness of digital diabetes program combining a Connected Glucose Meter and Certified Diabetes Educator Coaching and reported an average 18.4% reduction in the likelihood of having a day with hypoglycemia (blood glucose (BG) <70 mg/dL) and an average 16.4% reduction in hyperglycemia (BG >180 mg/dL) in between the 2nd and 12th month after engagement in comparison to the 1st month as the baseline.21
However, the use of digital technology in providing connected and timely care based on real-time transmission and receipt of patient BG data has not yet been scientifically studied in India. Hence, our study intended to evaluate the impact of connected diabetes care on glycemic control and hypoglycemia episodes of T2DM patients in north India. With increasing smartphone penetration, tech-savviness, added to the low cost of data in India, smartphone-enabled connected care could ensure a scalable and cost-effective method of diabetes care. The current study was planned to evaluate the effectiveness of connected diabetes care enabled by a smartphone-connected glucometer, real-time feedback, and contextualized counseling on glycemic control and hypoglycemia episodes in T2DM patients.
Materials and Methods
Connected Diabetes Care
Connected diabetes care entails the smartphone-connected glucometer wherein the patients monitor their BG levels, and there is a real-time transmission of information to certified diabetes educators (CDE). Based on the self-monitoring of blood glucose (SMBG) findings, patients are given corresponding telephonic counseling by CDEs. Patients are evaluated and, based on their profile, are advised to choose a healthy diet and encouraged to be physically active and to strictly follow the medication routine.
In addition, caregiver alerts, actionable nudging, feedbacks, and alerts are sent to the patient digitally to engage them, ensuring their BG levels are in appropriate control. Given the real-time information, physicians provide medical support to the patients and advise them regarding the required changes in their therapy.
BeatO Smartphone-Connected Glucometer
Custom smartphone-connected glucometer (BeatO developed by Health Arx Technologies Pvt. Ltd., India) provides a connected diabetes care program comprising (1) Smartphone-connected glucometer that interfaces with BeatO’s mobile app and saves readings on the cloud, (2) Real-time feedback and counseling support based on patient BG data by a team of CDE, and (3) Personalized nudging through in-app notifications and instant caregiver alerts (Figure 1). The patients can ask all kinds of questions related to diabetes education and management. The medium of conversation can be through a real-time call and counselling with CDEs or via a chatbot, where they can place their queries. A real-time feedback and prompt resolution is provided to the patients. BeatO is available in India and is offered directly to patients online on the BeatO app or as a part of a package through B2B (business to business) partners.
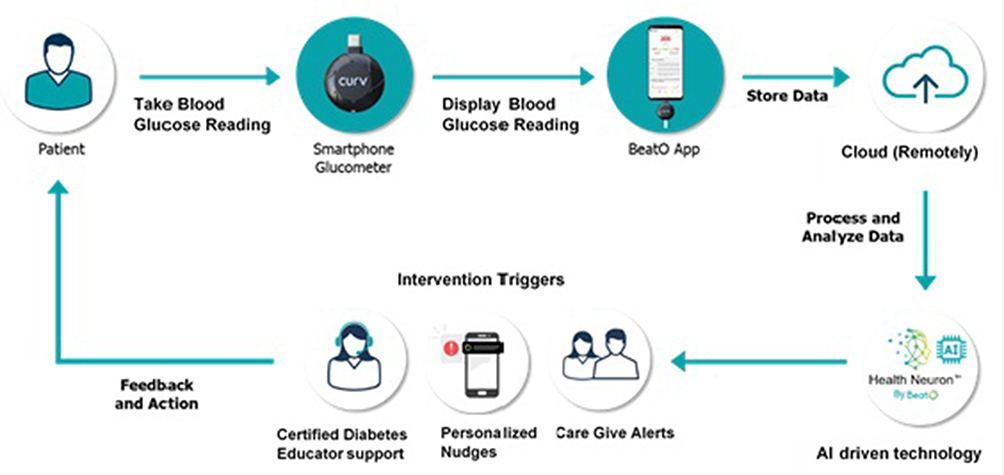 |
Figure 1 Connected diabetes care program for patients with type 2 diabetes. |
Once a patient takes a BG reading using the BeatO smartphone-connected glucometer, the readings and other contextual data are automatically saved on the app and stored centrally on the cloud. BeatO’s data-driven engine “Health NeuronTM” automatically triggers algorithmic actionable nudging, feedbacks, and alerts on the app. For example, if the blood glucose value is 59 mg/dL, the app may inform the patient, “Have 1 tbsp sugar or 30 mL of fruit juice immediately and recheck your levels after 15 mins”. In parallel, a caregiver alert to their saved contacts would be sent instantly as a short message service (SMS). If the fasting blood glucose (FBG) value is very high, for example, 303 mg/dL, the app may inform the patient, “Avoid high calorie and high carb meals. Check for infections, missed medication or stress”. A caregiver alert to their saved contacts would be instantly sent.
An interaction with BeatO’s CDE is triggered by Health NeuronTM either (1) automatically, when a BG value of fasting or pre-prandial BG value >140 mg/dL, post-prandial BG value >240 mg/dL, or any BG value <70 mg/dL, or (2) on-demand when a patient requests on the app. A typical CDE counseling session comprises contextual education about the patient’s blood glucose trends, nutrition recall, planning, physical activity planning, the importance of medication adherence, and the need to be in a safe BG range.
Study Design
This was a retrospective, multicenter, real-world study based on the SMBG data and medical records (reported history) of T2DM patients residing in multiple cities across north India. Out of 7111 T2DM patients, 2631 (37%) patients were from Tier 1 cities, while the majority of them, i.e., 4480 (63%) patients, were from Tier 2 and 3 cities. Patients aged >18 years who were engaged with BeatO’s connected diabetes care program between September 2019 and July 2020 (11 months) and received at least one CDE counseling session based on their SMBG values were included in this study. Pregnant women were excluded from the study.
Study Assessments
This study evaluated the SMBG-driven real-time contextualized feedback loop and counseling by CDE based on data-driven triggers and analyzed patients’ demographic, clinical, and medication-related information as a part of the digital diabetes engagement and care. Data was analyzed to understand the outcomes of glycemic control and the episodes of hypoglycemia and associated factors. The fasting, pre-prandial, and post-prandial BG values before and after counseling were compared to understand the effects of the overall intervention.
Pre-counseling BG values (BG values recorded in the 30 days period before the first counseling session) of patients were compared to post-counseling BG values (BG values recorded between the 15th and 45th day after the last counseling session). For individuals with more than one BG value available in the defined period, the average was taken for comparison, eg, if a patient had more than one FBG reading in the month before counseling, the average FBG value was considered for comparison. The effects of counseling on glycemic control and hypoglycemic episodes were assessed by comparing the predefined periods for pre-counseling and post-counseling BG values. At least a 5% improvement in pre-counseling versus post-counseling BG values was considered as improvement in glycemic control. A hypoglycemic episode was defined as a BG measurement below 70 mg/dL.
Statistical Methods
Data analysis was performed using Microsoft Excel (2016) and R Studio-3.6.3. Categorical variables were expressed as numbers (percentages) and compared using Chi-square test. Continuous variables were expressed as mean (standard deviation) and compared by using the paired-sample t-test. Statistical significance was considered at p <0.05.
Ethics Approval
This was a retrospective study, and the data from existing medical records were used for the study without any additional prospective components for research purposes. The patients’ confidentiality was maintained using anonymized and de-identified data at the source level. The user consent for conducting analyses for research purposes was taken electronically in a non-personally identifiable form when a patient registered on the app/website. Accordingly, permission for ICF waiver was obtained from the Ethics Committee for Research, Fortis C-DOC Hospital, Center of Excellence for Diabetes, Metabolic Diseases, and Endocrinology, New Delhi, India, dated 10th May 2021.
Results
A total of 7111 T2DM patients’ medical records were retrieved and reviewed. The mean age was 51.6 years, and the majority (77.9%) were males. The mean duration of diabetes was 9.2 years. Patterns of counseling session uptake showed that the majority received a single session of counseling (75%), and the remaining patients received 2 (16.7%), 3 (5%), 4 (2%), or ≥5 (1.3%) sessions (Table 1).
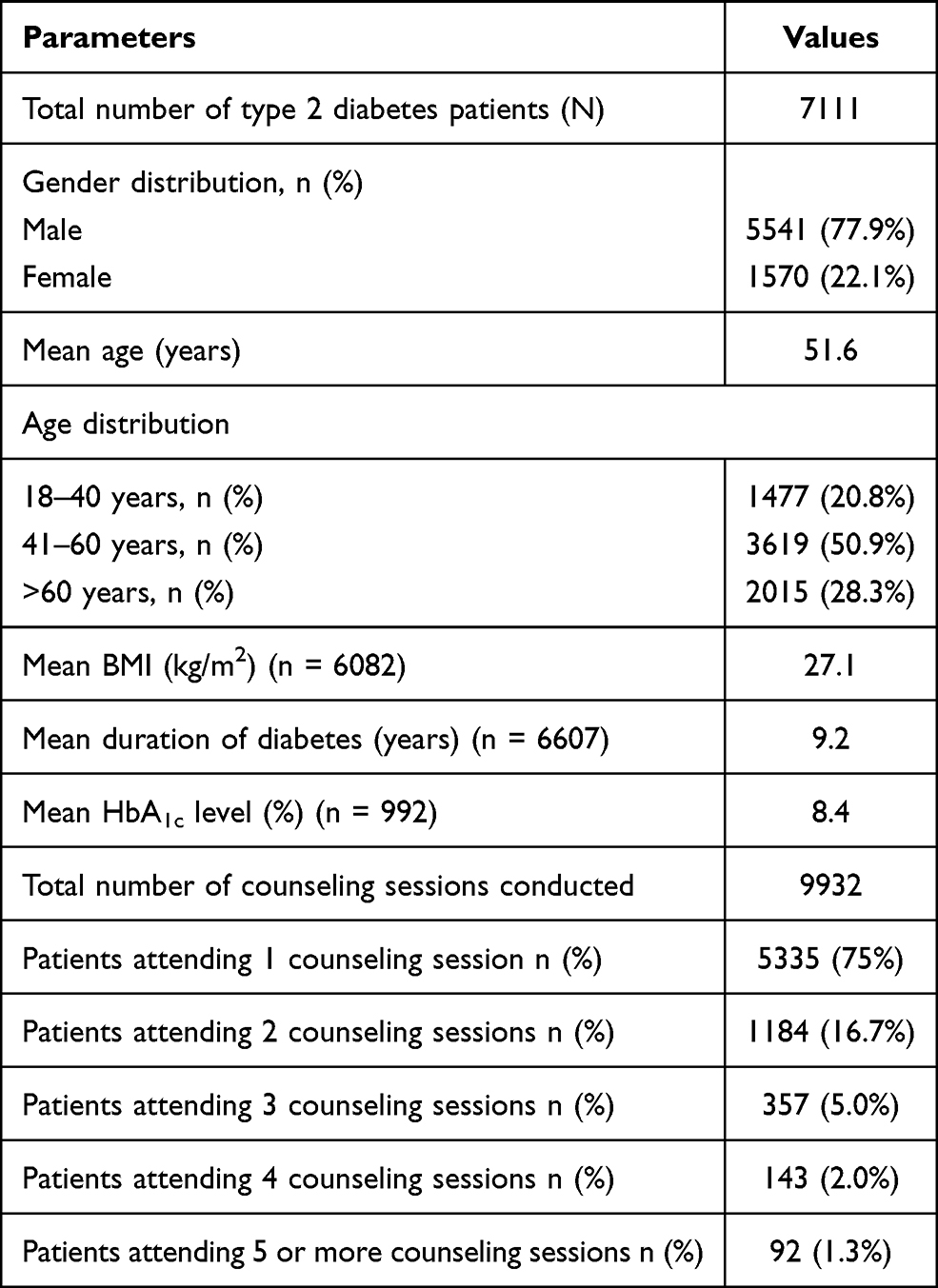 |
Table 1 Characteristics of Patients Engaged with Digital Diabetes Engagement Platform |
Effect of SMBG-Driven Counseling on Glycemic Control
Out of 7111 patients, 4458 patients had both pre-counseling and post-counseling mean BG value recordings, which met the baseline and comparator definition criteria for at least one or more types of readings (fasting, pre-prandial, and post-prandial). SMBG-driven real-time feedback and counseling led to a reduction (by at least 5%) in mean BG values across all types of readings. More than 5% reduction in mean fasting, pre-prandial, and post-prandial BG values was observed in 53%, 52%, and 54% of the patients, respectively (Figure 2).
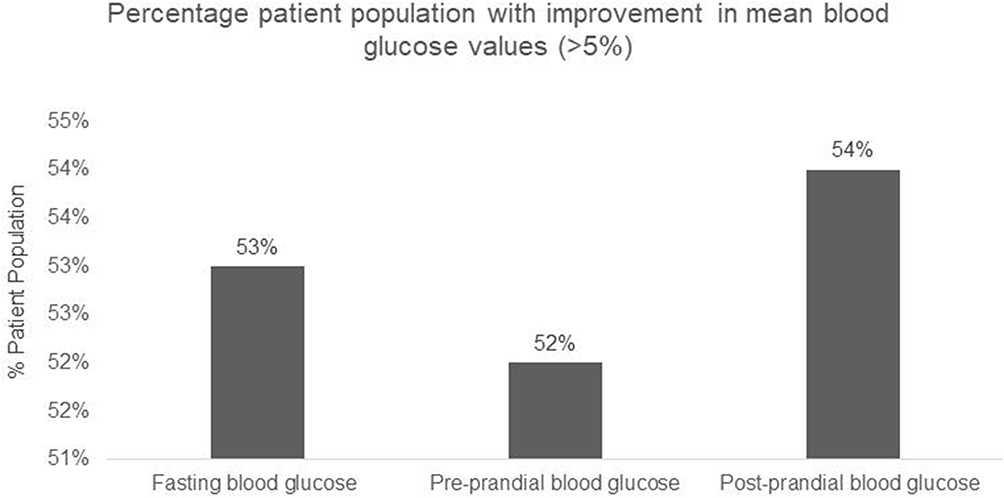 |
Figure 2 Improvement in mean BG values. |
Patients who had received one or more counseling sessions showed improvement in their mean BG levels (by ~10%; p <0.05) across all age groups. There was a statistically significant reduction in mean fasting (by 9.6%), pre-prandial (by 9.9%), and post-prandial BG values (by 9.2%) in adults and the elderly (Figure 3 and Table 2).
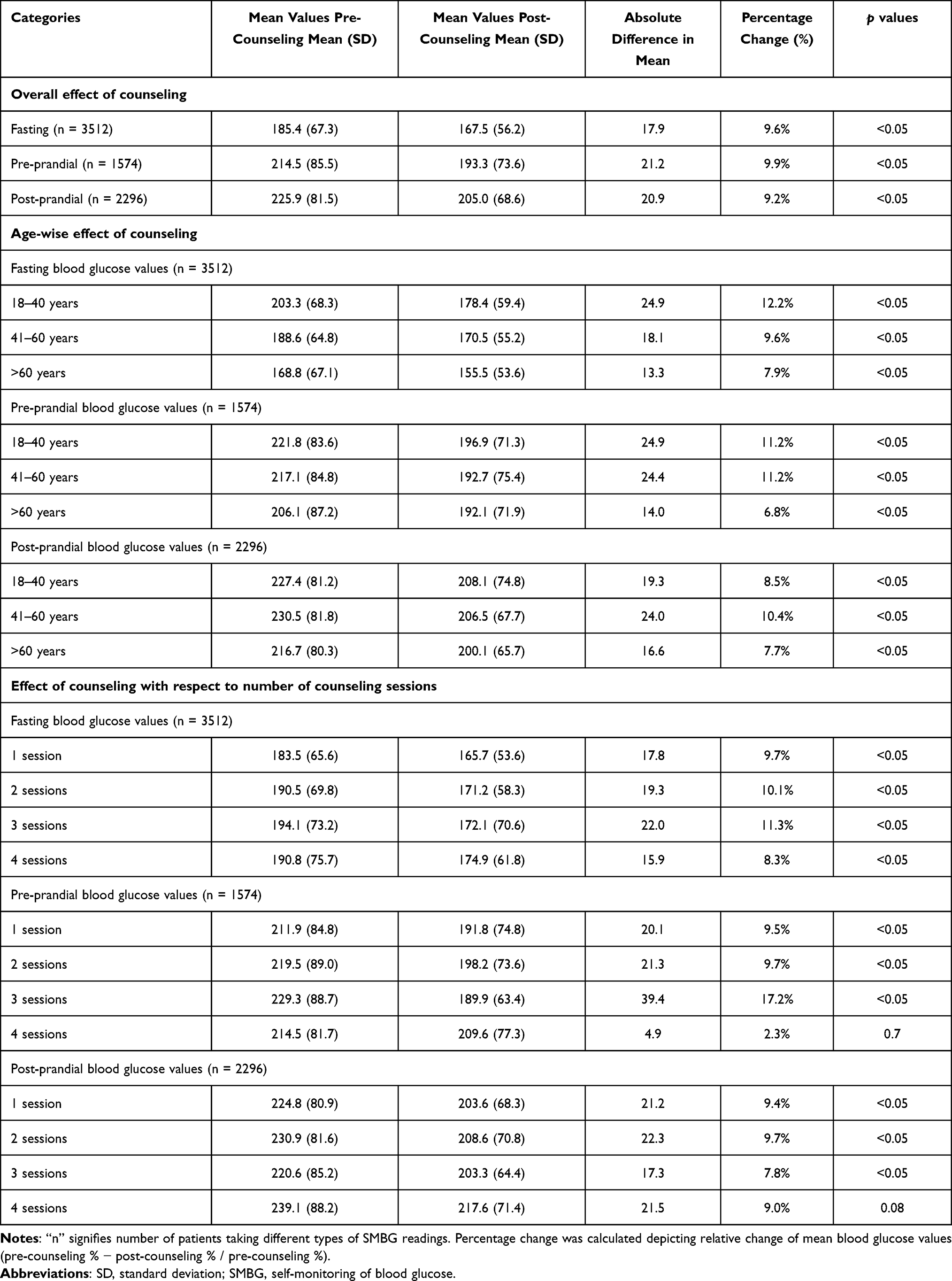 |
Table 2 Effect of SMBG-Driven Counseling on Mean Blood Glucose Levels |
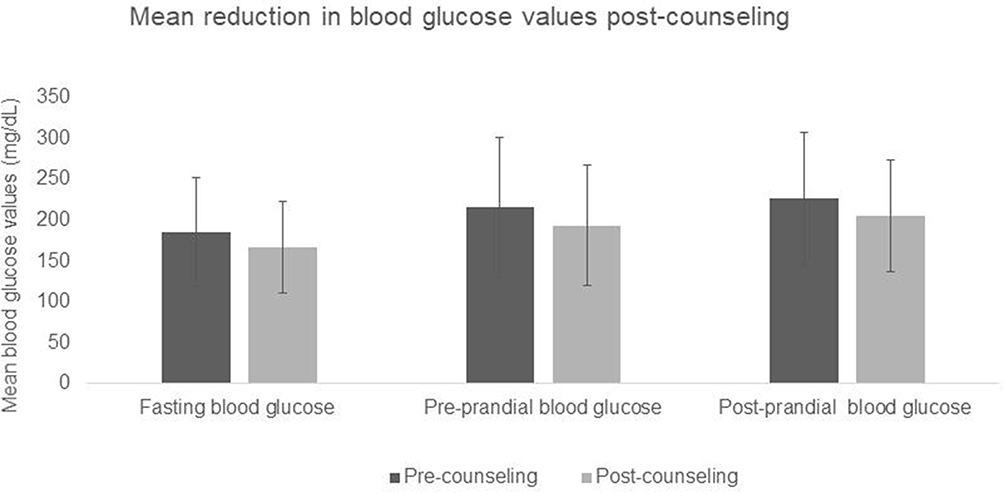 |
Figure 3 Effect of SMBG-driven counseling on mean BG values. |
Patients in the age group of 18–40 years showed up to a 12% reduction in their mean FBG values, while patients in the 40–60-year age group showed up to an 11% reduction in their pre-prandial mean BG values. Patients who had taken up to 3 counseling sessions showed statistically significant reductions in mean BG values across all types of readings (Table 2).
Effect of SMBG-Driven Counseling on the Hypoglycemia Episodes
The hypoglycemia episodes observed with FBG values reduced significantly from 734 to 316 episodes (58.5% reduction) post-counseling. Similarly, pre-prandial and post-prandial hypoglycemia episodes also showed a significant reduction by 48.1% (302 to 166 hypoglycemia episodes) and 61.8% (331 to 139 hypoglycemia episodes), respectively (Table 3 and Figure 4).
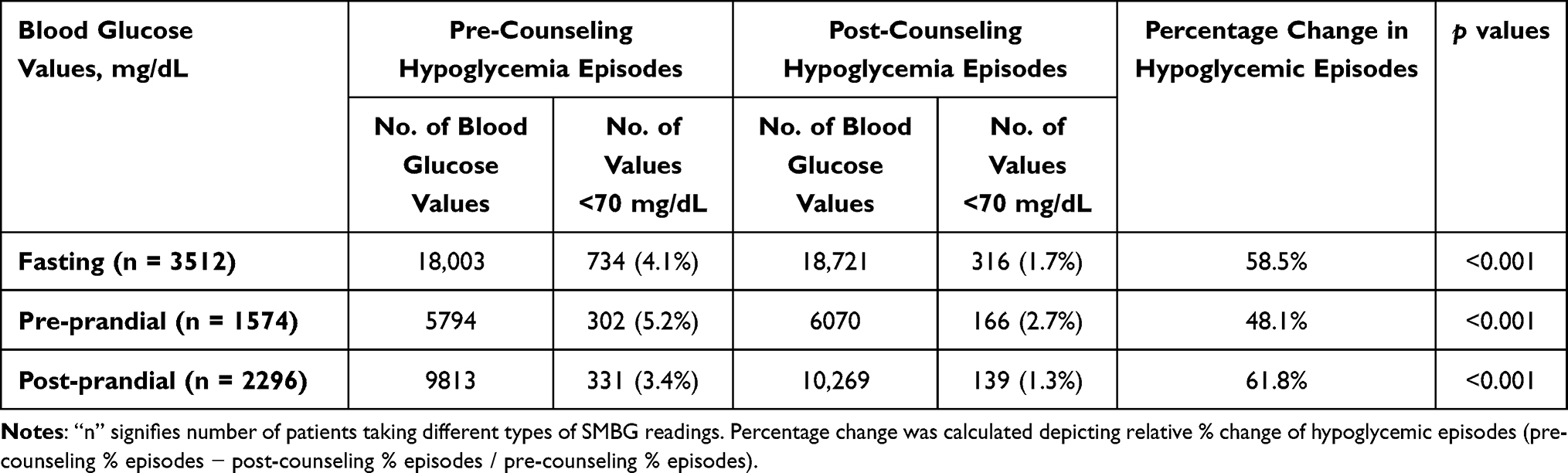 |
Table 3 Effect of SMBG-Driven Counseling on Hypoglycemia Episode |
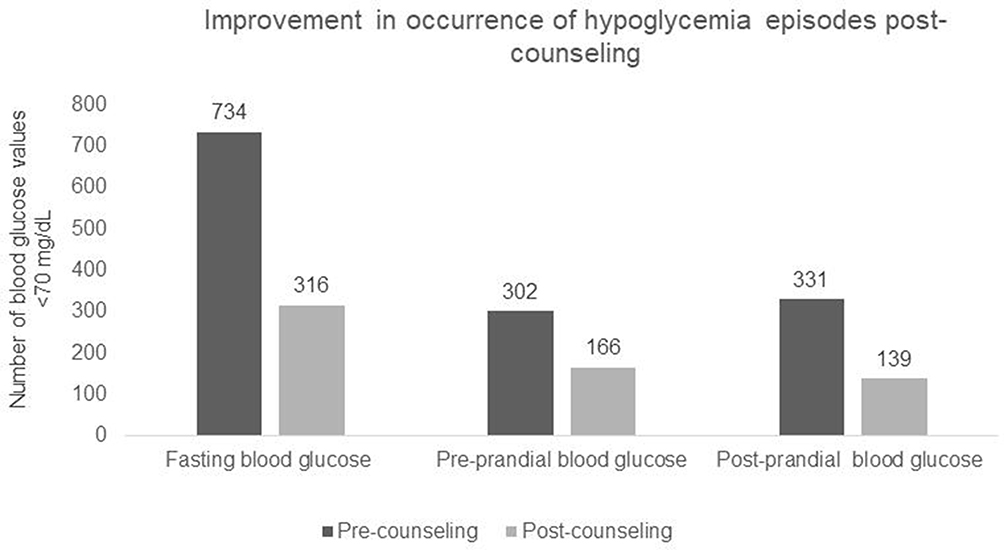 |
Figure 4 Impact of SMBG-driven counseling on occurrence of hypoglycemia episodes. |
Factors Associated with Hypoglycemia Episodes in Diabetes Patients
In total, 959 patients had hypoglycemia events before counseling, out of which 781 (81.4%) showed complete improvement without any BG reading ≤70 mg/dL post-counseling. Mean BMI of the patients who exhibited improvement in hypoglycemia episodes was 26.1 kg/m2. Among them, 29.8% of patients received insulin and 34.8% received sulfonylureas. The majority (77.3%) of the patients in the >60 years of age category showed improvement in hypoglycemia episodes post-counseling (Table 4). A total of 178 patients (18.6%) had at least one BG reading in the hypoglycemic range even after counseling. Similarly, 22.7% of elderly patients (>60 years) (Table 4) and 47.1% of patients who were using insulin had no improvements.
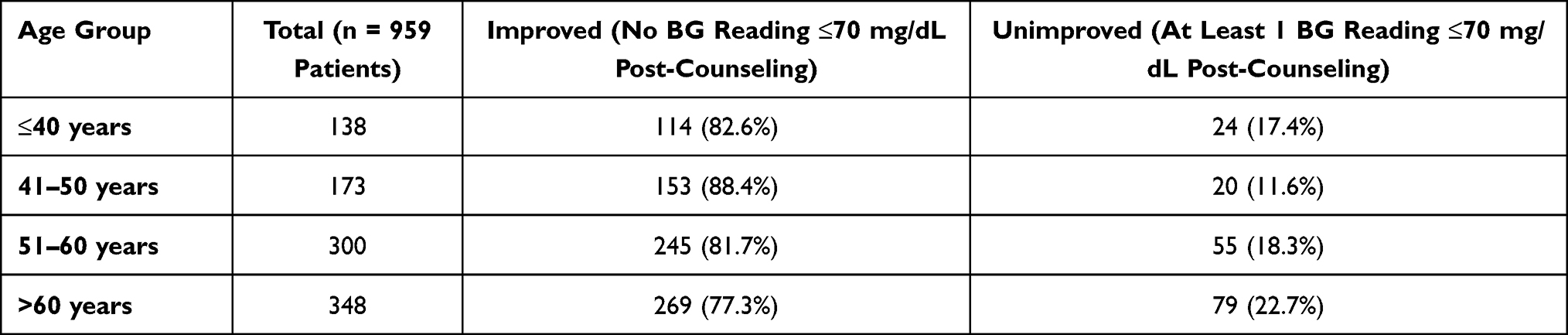 |
Table 4 Age Profiling of Patients Showing Hypoglycemia Episode Post-SMBG-Driven Counselling |
Discussion
Our study demonstrated a unique, real-world, evidence-based effect of connected SMBG-driven real-time feedback and counseling in T2DM management. The SMBG linked to real-time transmission of data, instant feedback, and counseling was an effective intervention in the reduction of mean BG values and hypoglycemia episodes. This is an important finding, especially in the Indian context, as hypoglycemia has a direct impact on the quality of life and healthcare costs for people with diabetes. Though cost-effectiveness was not in the scope of the study, the findings of the study were indicative that the digital intervention reduced time spent in travel, lab testing, and timely consultation. Eventually, it can have a significant effect on policy and program formulation for diabetes management in India and other developing countries with a high prevalence of diabetes, lacking primary care infrastructure, and largely out-of-pocket healthcare expenditure.
Our study examined the real-world population with diabetes using BeatO’s connected diabetes care program comprising BeatO’s smartphone-connected glucometer and real-time data-driven interventions through CDE, personalized nudging, and caregiver alerts. The study demonstrated that BeatO’s connected diabetes care program was effective in reducing the mean BG values nearly up to 10% across all age groups (>18 years) with an average of >50% study population achieving an effective and meaningful (>5%) mean BG reduction. In consonance, a study22 from south India assessing the effect of in-person counseling on 207 patients in the controlled hospital setting on BG levels found a higher reduction in the counseling group (from 237 to 203.4 mg/dL) than controls (229.7 to 211.4 mg/dL). A retrospective cohort study23 in the US assessing a mobile app displaying BG data and details about meals and medications to patients through customizable graphs found it to be effective in increasing the frequency of SMBG and dropping average BG levels (by 3.5%) in comparison to a control group (using no mobile app). Similarly, another retrospective study reported a significant improvement in the monthly average BG level in patients who were engaged with the digital self-management app, “Dario”, as compared to the non-users.24 The users of an SMBG app, “One Drop”, reported a significant reduction in HbA1c (1.36%) in a median of approximately 4 months.25
The present study also demonstrated a significant impact on the reduction of hypoglycemia episodes by 62% post-counseling. Moreover, not a single episode of hypoglycemia (<70 mg/dL) was observed post-counseling in majority (~81%; 781 of 959) of the patients. These findings are in corollary with the observations of a prospective pre-post study26 conducted in the US assessing the effect of a program of cellular-enabled glucose meter with real-time feedback by a CDE (“Livongo”) in outpatient clinical settings (86 patients). It was demonstrated that the intervention was effective in improving mean BG values as well as reducing the episodes of hypoglycemia (by 17%); however, the sample size was small to conclude on the respective clinical outcomes. However, our analysis was performed on large pragmatic, real-world evidence-based data that showed a clinically and statistically significant reduction in BG level (up to 10%) and hypoglycemic episodes (by 62%) in T2DM patients using the digitally driven remote monitoring and care.
Further, even among the elderly patients (aged >60 years), the present study showed a significant reduction (7.9%) in mean BG values. In addition, 77.3% of the elderly patients saw a reduction in hypoglycemia episodes. The proportion of patients not showing an improvement in the hypoglycemia episodes was higher (22.7%) in the elderly age group (>60 years) and in patients taking insulin (47.1% of unimproved patients were on insulin). Older adults with T2DM are at high risk of recurrent hypoglycemia, which might be due to their attenuated counter-regulatory mechanism to hypoglycemia or polypharmacy that can increase the risk of severe hypoglycemia.27 Hence, for the elderly (>60 years) and those on high doses of insulin, a more direct and intense intervention may be required to improve their hypoglycemia episodes.
Our study results also revealed that the average time taken for the reduction of mean BG values was only 34.8 days. This effect of contextual feedback and counseling through the real-time transmission of BG readings can also aid treating surgeons to keep a close watch on glucose values during or while preparing elderly patients, who are more vulnerable due to age and diabetes-related comorbidities, for elective surgeries.
Several mobile phone/text message-based intervention studies have demonstrated positive outcomes, including improved diabetes risk behaviors, specifically diet (fruits and vegetable consumption), a lower cumulative incidence of T2DM, and effectiveness and acceptability of m-health intervention in the Indian population for overall support in lifestyle modification and found these interventions scalable in resource-limited settings.28–31 However, our study is the first real-world study with a larger sample size estimating the impact of a comprehensive digital diabetes intervention on glycemic control in a wider representative Indian diabetes population. It provides the evidence for a wider extrapolation of the findings.
Strengths and Limitations
To our knowledge, this is the largest real-world study from India, assessing the effectiveness of SMBG-driven counseling coupled with a real-time feedback system for the management of T2DM in India. Our analysis has been performed on a large set of pragmatic data representing a wider population.
There were few study limitations, including the retrospective nature due to which there was a lack of assessment of other factors such as a change in medications, dose patterns, patient compliance to medications, and any external medical consultation done in the index time, which may have affected an individual’s glucose levels. Laboratory-based HbA1c values were not assessed, which would have been helpful to understand whether the reduced frequency of hyperglycemia and hypoglycemia events resulted in overall HbA1c improvement. The study had an over-representation of males (77.9%), given that BeatO is presently available for purchase online, and males are more likely to purchase online as compared to females at present in India.31
Conclusion
In Indian settings, this is one among few studies, which has evaluated the role of digital engagement in glycemic control and hypoglycemia prevention and establishes it as an evidence-based effective intervention. BeatO’s integrated and novel patient intervention through digital and connected diabetes care platform has shown a significant reduction in glycemic values and hypoglycemic events in a large patient population. These results demonstrate the real-world effectiveness of the BeatO’s program in improving significant clinical outcomes of type 2 diabetes mellitus patients in India.
Abbreviations
AI, artificial intelligence; BG, blood glucose; BMI, body mass index; CDE, certified diabetes educators; FBG, fasting blood glucose; HbA1c, glycated hemoglobin; SMBG, self-monitoring of blood glucose; T2DM, type 2 diabetes mellitus.
Data Sharing Statement
Data will be available from the corresponding author upon request.
Consent for Publication
All authors provided written consent to publish this study.
Acknowledgments
The authors would like to thank Rupali Jangid (Senior Medical Writer) for providing assistance in writing the original manuscript, Dr. Vamsi Krishna Kolukula (Medical Director, Medical Affairs), and Dr. Venugopal Madhusudhana (Vice President, Medical Affairs) for additional editorial assistance in the development of this manuscript. All the above belong to THB c/o Sekhmet Technologies Pvt Ltd., Gurugram, Haryana, India. The authors would also like to thank Ajrendra Gaurav (VP Products, Health Arx Technologies Pvt. Ltd., New Delhi, India) for assisting in data collation and data analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The study was funded by Health Arx Technologies Pvt. Ltd.
Disclosure
Gautam Chopra and Mudit Sabharwal declare that they serve as Chief Executive Officer and Head of Medical Affairs, respectively, at Health Arx Technologies Pvt. Ltd., New Delhi, India (manufacturer of BeatO smartphone-connected glucometer). The authors report no other conflicts of interest in this work.
References
1. Misra A, Tandon N, Ebrahim S, et al. Diabetes, cardiovascular disease, and chronic kidney disease in South Asia: current status and future directions. BMJ. 2017;357:j1420. doi:10.1136/bmj.j1420
2. Tandon N, Anjana RM, Mohan V, et al. The increasing burden of diabetes and variations among the states of India: the Global Burden of Disease study 1990–2016. Lancet Glob Health. 2018;6(12):e1352–1362. doi:10.1016/S2214-109X(18)30387-5
3. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas. Diabetes Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
4. Borgharkar SS, Das SS. Real-world evidence of glycemic control among patients with type 2 diabetes mellitus in India: the TIGHT study. BMJ Open Diabetes Res Care. 2019;7(1):e000654. doi:10.1136/bmjdrc-2019-000654
5. Faizi N, Najam Khalique AA, Shah MS. The dire need for primary care specialization in India: concerns and challenges. Family Med Prim Care. 2016;5(2):228–233. doi:10.4103/2249-4863.192382
6. Hooda SK. Out-of-pocket payments for healthcare in India: who have affected the most and why? J Health Manag. 2017;19(1):1–5. doi:10.1177/0972063416682535
7. Pandey A, Ploubidis GB, Clarke L, et al. Trends in catastrophic health expenditure in India: 1993 to 2014. Bull World Health Organ. 2018;96(1):18–28. doi:10.2471/BLT.17.191759
8. Rodríguez-Rodríguez I, Rodríguez J-V, Molina-García-Pardo J-M, Zamora-Izquierdo M-Á, Martínez-Inglés M-TM. A comparison of different models of glycemia dynamics for improved Type 1 diabetes mellitus management with advanced intelligent analysis in an internet of things context. Appl Sci. 2020;10(12):4381. doi:10.3390/app10124381
9. Ellahham S. Artificial intelligence: the future for diabetes care. Am J Med. 2020;133(8):895–900. doi:10.1016/j.amjmed.2020.03.033
10. Li J, Huang J, Zheng L, Li X. Application of artificial intelligence in diabetes education and management: present status and promising prospect. Front Public Health. 2020;8:173. doi:10.3389/fpubh.2020.00173
11. Fagherazzi G, Ravaud P. Digital diabetes: perspectives for diabetes prevention, management and research. Diabetes Metab. 2019;45(4):322–329. doi:10.1016/j.diabet.2018.08.012
12. Diabetes and coronavirus (COVID-19). Available from: https://www.diabetes.org/coronavirus-covid-19/how-coronavirus-impacts-people-with-diabetes.
13. Kaufman N. Digital therapeutics: leading the way to improved outcomes for people with diabetes. Diabetes Spectr. 2019;32(4):301–303. doi:10.2337/ds19-0012
14. Cafazzo JA. A digital-first model of diabetes care. Diabetes Technol Ther. 2019;21(S2):S252–S258. doi:10.1089/dia.2019.0058
15. Wu Y, Yao X, Vespasiani G, et al. Mobile app-based interventions to support diabetes self-management: a systematic review of randomized controlled trials to identify functions associated with glycemic efficacy. JMIR mHealth uHealth. 2017;5(3):e35. doi:10.2196/mhealth.6522
16. Kitsiou S, Pare´ G, Jaana M, Gerber B. Effectiveness of mHealth interventions for patients with diabetes: an overview of systematic reviews. PLoS One. 2017;12:e0173160. doi:10.1371/journal.pone.0173160
17. Greenwood DA, Gee PM, Fatkin KJ, et al. A systematic review of reviews evaluating technology-enabled diabetes self-management education and support. J Diabetes Sci Technol. 2017;11:1015–1027. doi:10.1177/1932296817713506
18. Bonoto BC, de Araújo VE, Godói IP, et al. Efficacy of mobile apps to support the care of patients with diabetes mellitus: a systematic review and meta-analysis of randomized controlled trials. JMIR mHealth uHealth. 2017;5(3):e4. doi:10.2196/mhealth.6309
19. Fu H, McMahon SK, Gross CR, et al. Usability and clinical efficacy of diabetes mobile applications for adults with type 2 diabetes: a systematic review. Diabetes Res Clin Pract. 2017;131:70–81. doi:10.1016/j.diabres.2017.06.016
20. Hou C, Carter B, Hewitt J, et al. Do mobile phone applications improve glycemic control (HbA1c) in the self-management of diabetes? A systematic review, meta-analysis, and GRADE of 14 randomized trials. Diabetes Care. 2016;39(11):2089–2095. doi:10.2337/dc16-0346
21. Downing J, Bollyky J, Schneider J. Use of a connected glucose meter and certified diabetes educator coaching to decrease the likelihood of abnormal blood glucose excursions: the Livongo for Diabetes Program. J Med Internet Res. 2017;19(7):e234. doi:10.2196/jmir.6659
22. Malathy R, Narmadha M, Ramesh S, et al. Effect of a diabetes counselling programme on knowledge, attitude and practice among diabetic patients in Erode district of south India. J Young Pharm. 2011;3(1):65–72.
23. Offringa R, Sheng T, Parks L, et al. Digital diabetes management application improves glycemic outcomes in people with type 1 and type 2 diabetes. J Diabetes Sci Technol. 2018;12(3):701–708. doi:10.1177/1932296817747291
24. Fundoiano-Hershcovitz Y, Hirsch A, Dar S, et al. Role of digital engagement in diabetes care beyond measurement: retrospective cohort study. JMIR Diabetes. 2021;6(1):e24030. doi:10.2196/24030
25. Osborn CY, van Ginkel JR, Marrero DG, et al. One Drop | Mobile on iPhone and Apple watch: an evaluation of HbA1c improvement associated with tracking self-care. JMIR mHealth uHealth. 2017;5(11):e179. doi:10.2196/mhealth.8781
26. Bollyky JB, Melton ST, Xu T, et al. The effect of a cellular-enabled glucose meter on glucose control for patients with diabetes: prospective pre-post study. JMIR Diabetes. 2019;4(4):e14799. doi:10.2196/14799
27. Muralidharan S, Ranjani H, Anjana RM, et al. Mobile health technology in the prevention and management of type 2 diabetes. Indian J Endocrinol Metab. 2017;21(2):334–340. doi:10.4103/ijem.IJEM_407_16
28. Pfammatter A, Spring B, Saligram N, et al. mHealth intervention to improve diabetes risk behaviors in India: a prospective, parallel group cohort study. J Med Internet Res. 2016;18(8):e207. doi:10.2196/jmir.5712
29. Ramachandran A, Snehalatha C, Ram J, et al. Effectiveness of mobile phone messaging in prevention of type 2 diabetes by lifestyle modification in men in India: a prospective, parallel-group, randomized controlled trial. Lancet Diabetes Endocrinol. 2013;1(3):191–198. doi:10.1016/S2213-8587(13)70067-6
30. Ajay VS, Jindal D, Roy A, et al. Development of a smartphone-enabled hypertension and diabetes mellitus management package to facilitate evidence-based care delivery in primary healthcare facilities in India: the mPower Heart Project. J Am Heart Assoc. 2016;5(12):e004343. doi:10.1161/JAHA.116.004343
31. Sethi RS, Sethi UJ. Does demography influence online purchase intention? Evidence from north-west India. Int J Adv Manag Econ. 2018;6(2):1–8.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.