Back to Journals » Journal of Pain Research » Volume 12
Efficacy of bilateral erector spinae plane block in the management of pain: current insights
Authors Tulgar S ![]() , Ahiskalioglu A
, Ahiskalioglu A ![]() , De Cassai A
, De Cassai A ![]() , Gurkan Y
, Gurkan Y
Received 15 February 2019
Accepted for publication 6 August 2019
Published 27 August 2019 Volume 2019:12 Pages 2597—2613
DOI https://doi.org/10.2147/JPR.S182128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Serkan Tulgar,1 Ali Ahiskalioglu,2 Alessandro De Cassai,3 Yavuz Gurkan4
1Department of Anesthesiology and Reanimation, Faculty of Medicine, Maltepe University, Istanbul, Turkey; 2Department of Anaesthesiology and Reanimation, School of Medicine, Ataturk University, Erzurum, Turkey; 3Section of Anaesthesiology and Intensive Care, Department of Medicine (DIMED), University of Padua, Padua, Italy; 4Department of Anesthesiology and Reanimation, Faculty of Medicine, Koç University, Istanbul, Turkey
Correspondence: Serkan Tulgar Fakültesi Maltepe, Üniversitesi Hastanesi, 39 Feyzullah Caddesi, Maltepe, Istanbul, Turkey
Tel +90 505 542 3985
Email [email protected]
Abstract: Erector spinae plane block (ESPB) is a newly described interfascial plane block, and the number of articles on the bilateral application of ESPB is increasing in the literature. In this paper, in addition to analyzing bilateral ESPB cases and studies published so far, we aimed to review the relevant anatomy, describe the mechanism of spread of the injectant, demonstrate varying approaches to ESPB, and summarize case reports and clinical trials, as well as provide current insight on this emerging and popular block. Randomized controlled studies, comparative studies of ESPB versus other methods, and pharmacokinetic studies of bilateral applications must be the next step in clearly understanding bilateral ESPB.
Keywords: bilateral erector spinae block, regional anesthesia, interfascial plane blocks
Introduction
Erector spinae plane block (ESPB) is an interfascial plane block first described in 2016 by Forero et al1 as an effective treatment method for the treatment of thoracic neuropathic pain. Studies published thereafter have however concentrated on the use of ESPB for perioperative or postoperative analgesia.2–4 The first bilateral ESPB, described for postoperative analgesia in laparoscopic ventral hernia surgery, was also reported from the same center where ESPB was originally described.5 The initial clinical findings suggested that ESPB injectant would spread to both the dorsal and ventral ramus of the spinal nerves, leading to blockage of both somatic and visceral pain, a effect similar to epidural analgesia.6,7 Time is required to determine the exact features and effectiveness of this block, as well as its safety and feasibility in various surgical procedures and pain syndromes, using anatomic studies, case reports, and clinical studies of bilateral ESPB. The objective of this narrative review article is to review the relevant anatomy, describe the mechanism of spread of the injectant, demonstrate varying approaches to ESPB, and summarize case reports and clinical trials, as well as provide current insight on this emerging and popular block.
Anatomic features of ESPB
Forero et al1 initially described two different approaches for application of local anesthetic. The first was application “into interfascial plane between rhomboid major and erector spinae muscles” and the second “into the interfascial plane deep to the erector spinae muscle”. The authors reported that the first approach could be insufficient and that better effectiveness could be achieved with application of the injectant deep into the erector spinae muscle in the interfascial plane. In one letter to the editor, a child undergoing surgery for funnel chest was reported to have undergone bilateral ESPB for postoperative analgesia using the “into interfascial plane between rhomboid major and erector spinae muscles” technique.8 In all other publications, bilateral ESPB has been performed using the “into the interfascial plane deep to the erector spinae muscle” technique.2,4
Spread of injectant: anatomic studies and radiological imaging
There have not been any studies evaluating the spread of injectant in bilateral ESPB. In order to predict the spread of bilateral ESPB and understand the differences in sensorial block between sides of application, anatomic cadaver studies and radiological imaging reports must be well understood. In many regional anesthesia techniques, injectant spread is determined through cadaveric or imaging studies, and the results of these studies usually correlate with clinical findings. However, each anatomic study of ESPB has reported differences in results, especially with regard to sensorial block. In a study of 20 ESPB applications on ten cadavers, Ivanusic et al9 reported that the injectant spread widely in the craniocaudal, posterior, and lateral planes, with spread of local anesthetic to the dorsal ramus posterior of the costotransverse ligament in all cases, and that injectant pass anteriorly to the transverse process or costotransverse process in only two cases. On the other hand, Adhikary et al10 reported that local anesthetic spread widely in the plane between the erector spinae muscle and the costotransverse process, with profound spread anterior to the transverse process encompassing the paravertebral space, neural foramina, ipsilateral epidural space, and ipsilateral sympathetic chain. In magnetic resonance imaging in Schwartzman et al11 local anesthetic was also shown to pass anteriorly. In contrast to this,10 no involvement of the sympathetic chain was observed, but circumferential spread of the epidural space was observed. Yang et al12 reported findings similar to Adhikary et al,10 with local anesthetic spread to the sympathetic chain.
Vidal et al13 reported that injectant spread was evident posterior to the transverse process deep to the erector spinae muscle, as well as the paravertebral and intercostal spaces. Spread to the neural foramina or epidural space was not evaluated. Craniocaudal spread was evaluated, with 20 mL injectant reported to spread a mean of 4.6 (3–7) intercostal spaces. Studies reporting spread of injectant in ESPB are demonstrated in Figure 1. It may be possible that lack of understanding of the fascia deep to the erector spinae muscle may be the cause of differing reports from anatomic studies. This fascia is multilayered, with at least three layers reported.14 In most studies, injectant has been applied at the fourth or fifth thoracic vertebral level, and it is very possible that injectant spread may be different for lower thoracic or lumbar ESPB applications.15,16 In bilateral ESPB, it is possible that spread may differ for each side, leading to the perception of block failure clinically. The spread of sensorial block may differ craniocaudally. Three different clinical presentations have been reported. While injectant may lead to complete block of the hemithorax or the hemiabdomen’s dermatome, in some cases the anterior cutaneous branch may be missed, while in others sensorial blockage of the dorsal ramus may lead to patchy block.17,18 The clinical features of ESPB will be better understood as further case reports and clinical studies are published.
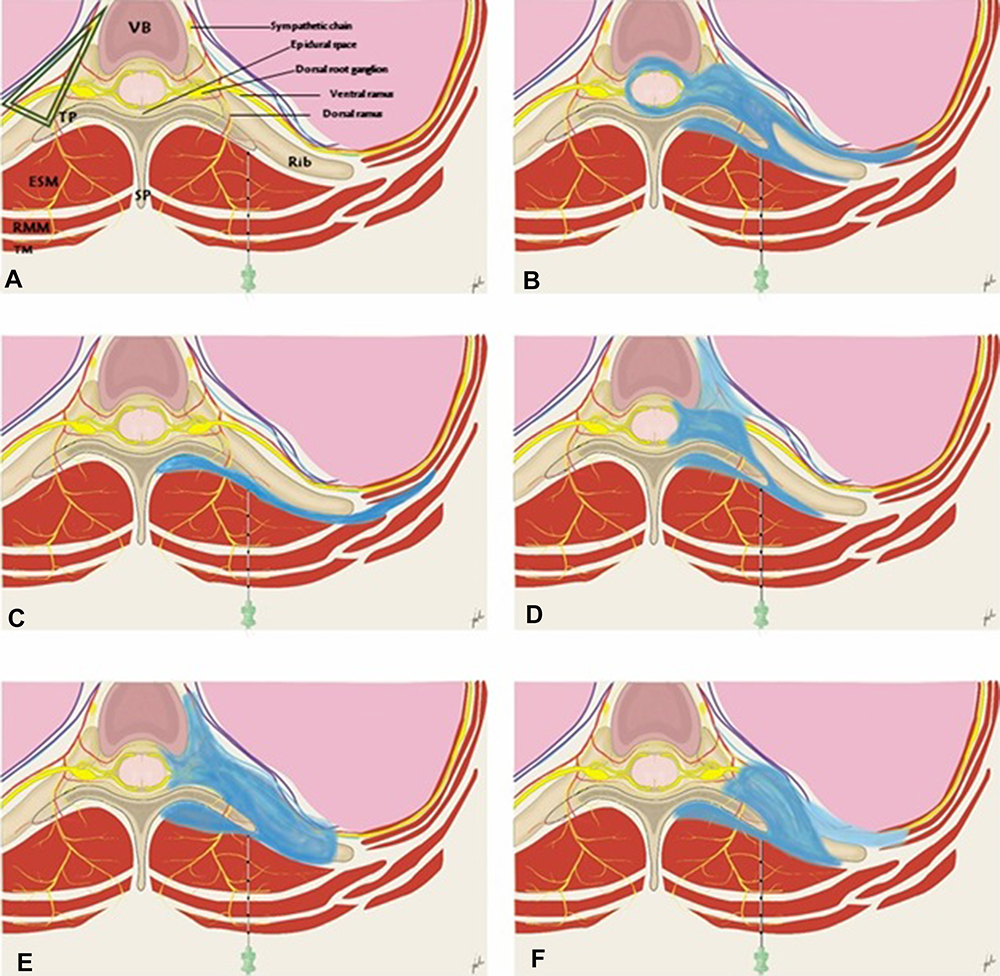 |
Figure 1 Illustration of results of anatomical and imaging studies related to erector spinae plane block. Notes: (A) Demonstration of anatomic structures. (B) Spread of injectant in Schwartzman et al.11 (C) Spread of injectant in Ivanusic et al.9 (D) Spread of injectant in Yang et al.12 (E) Spread of injectant in Adhikary et al.10 (F) Spread of injectant in Vital et al.13 Dark blue, obvious spread of injectant, Light blue (D, F), little spread of injectant. Green triangle, paravertebral space.Abbreviations: TM, trapezius muscle; RMM, rhomboid major muscle; ESM, erector spinae muscle; TP, transverse process; SP, spinous process; VB, thoracic vertebral body. |
Approaches, sonography, and technical features
The first description of ESPB was as the placement of an ultrasound probe 2.5–3 cm laterally to the spinous process at the fourth to fifth thoracic vertebral level on a parasagittal plane, directing the needle craniocaudally using the in-plane technique (Figures 2 [A and B] and 3).1 It should be kept in mind, however, that there are three layers of muscle above the transverse process between the Th2 and Th6 levels, whereas more inferiorly there are only two, due to the lack of the rhomboid muscle in this area (Figure 3.) Thereafter, the transverse-approach technique was described as placing the ultrasound probe on the transverse plane and inserting the needle from lateral to medial direction using the in-plane technique (Figure 1, C and D).19–21 Most recently, Yorukoglu et al22 described their technique in which bilateral ESPB was performed using one needle insertion over the spinous process that was advanced medially to laterally on both sides, described by the authors as a safe and easy technique for performing bilateral ESPB (Figure 4).
 |
Figure 2 (A) Position and orientation of the ultrasound transducer during a parasagittal scan of the upper thoracic region with the subject in the prone position. (B) Parasagittal ultrasound image of upper thoracic erector spinae plane block (ESPB). (C) Position and orientation of the ultrasound transducer during a transverse scan of the upper thoracic region with the subject in the prone position. (D) Transverse ultrasound image of upper thoracic ESPB. White arrow indicates needle.Abbreviations: T4, thoracic 4 vertebrae transverse process; TM, trapezius muscle; RMM, rhomboid major muscle; ESM, erector spinae muscle; ICM, intercostal muscle. |
 |
Figure 3 (A) Position and orientation of the ultrasound transducer during a parasagittal scan of the mid-thoracic region with the subject in the prone position. (B) Parasagittal ultrasound image of mid-thoracic erector spinae plane block. White arrow indicates needle. Abbreviations: T, transverse process; TM, trapezius muscle; ESM, erector spinae muscle; ICM, intercostal muscle. |
 |
Figure 4 (A) Position and orientation of the ultrasound transducer during a median transverse scan of the mid-thoracic region at the level of spinous process by Yorukoglu approach. (B) Transverse ultrasound image of the mid-thoracic bilateral erector spinae plane block. White arrow indicates needle. Abbreviations: TP, transverse process; SP, spinous process. |
For the lumbar region, ESPB was first described in hip surgery in the lateral position, advancing the needle craniocaudally using the in-plane technique.23 However, the out-plane technique in the parasagittal plane later became another popular technique for lumbar ESPB.24 Considering that lumbar ESPB requires deeper needle insertion when compared to thoracic ESPB, it is inevitable that different techniques are required. Recently, a modification of the shamrock technique for lumbar ESPB performed under ultrasound guidance in the lateral position (Aksu–De Cassai technique)25,26 was described as an easy-to-perform option in lumbar ESPB (Figure 5). Another modification/approach for lumbar ESPB is the Tulgar approach,27 in which local anesthetic is applied to both the posterior and anterior of the lumbar transverse process, which has a higher chance of guaranteeing block spread (Figure 6).
 |
Figure 5 (A) Position and orientation of the curvilinear ultrasound transducer during a transverse scan of the lumbar region above the iliac crest with the subject in the lateral decubitus position. (B) Ultrasound images of shamrock sign and Aksu/Cassai approaches for erector spinae plane block in the posterior axillary line above the iliac crest. White arrow indicates needle. Abbreviations: TP, transverse process; QLM, quadratus lumborum muscle; ESM, erector spinae muscle; PM, psoas muscle; VB, vertebral body. |
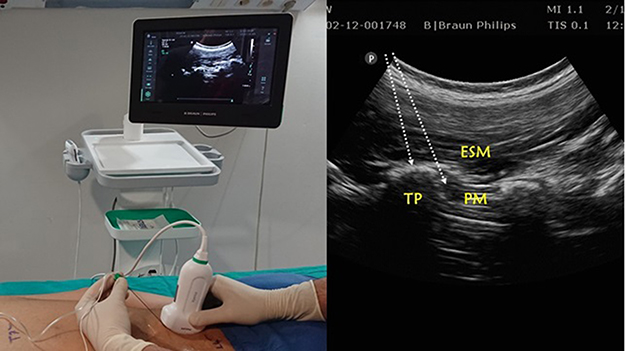 |
Figure 6 (A) Position and orientation of the ultrasound transducer during a parasagittal scan of the lumbar region with the subject in the prone position. (B) Ultrasound images of Tulgar approach for lumbar erector spinae plane block. White arrow indicates needle with in-plane approach.Abbreviations: TP, transverse process; ESM, erector spinae muscle; PM, psoas muscle. |
Positioning
Positioning for bilateral ESPB changes according to the place of application and the chosen technique, although the seated, side, or prone position is generally chosen for thoracic and lumbar ESPB. In the Aksu–Cassai and Tulgar approaches, the lateral decubitus position is used. It is possible that the position of the patient when performing ESPB may effect the spread of local anesthetic and thus the effect and quality of ESPB. No studies have examined this effect.
Operator and block technique
For bilateral ESPB, right-handed physicians must hold the transducer in their left hand, stand on the right side of the patient, and place the ultrasonography machine opposite themselves. For craniocaudal or caudocranial applications, the physician should choose a position suitable to their ergonomics. Although ESPB was first described with the in-plane technique, reports suggest that the out-of-plane technique is easier to apply.28 When the transverse process is chosen as the target, the out-of plane technique leads to safe application. The safety margin may also be increased by measuring the distance from the skin to the transverse process using ultrasonography.
Transducer selection and needle orientation
A high-frequency linear probe is usually chosen for the thoracic area, although a curvilinear (2–5 MHz) probe may be required for obese patients. When one of the Aksu–Cassai,25,26 Tulgar,27 or Yorukoglu approaches is used,22 a curvilinear (2–5 MHz) probe is suggested. The in-plane or out-of-plane technique should be used according to the physician's experience when inserting the needle for either thoracic or lumbar applications.
Needle length and gauge
While the needle length may change according to the location of the application and patient characteristics, generally a 22 G needle measuring 50, 80, or 100 mm is used for thoracic applications, while a 22 G needle measuring 80–100 mm should be used for lumbar or other applications.4,7,13,28
Catheterization
Catheter use in bilateral thoracic ESPB has been reported in the literature. Clinical trials using catheterization for bilateral ESPB in adults undergoing cardiac procedures have been reported.29,30 A case series of catheter use in bilateral ESPB in children with programmed intermittent bolus application, as well as continuous or intermittent bolus applications of local anesthesia via catheter for thoracotomy–esophagectomy, laparoscopic gastric surgeries, open abdominal surgeries, radical prostatectomy, and lumbosacral surgeries leading to effective postoperative analgesia, have been reported in the literature.6,31–37 While single-sided lumbar catheterization has been reported, to our knowledge there have been no reports of bilateral lumbar catheterization.38 Reports of catheterization and features associated with it, such as local anesthetic concentration, infusion speed, or time between boluses and initial dosage, are all based on the authors’ personal experience. There have not been any studies comparing of two differing modalities.
Local anesthetic volume and concentration
Local anesthetic volume and concentration is the most important factor for ESPB, as with all plane blocks. Plane blocks are volume-dependent, and thus dermatomal coverage increases with increased volume. ESPB applications have been performed using 10–40 mL volumes. When pediatric cases are evaluated, volume has been determined according to the child’s weight. This dosage is generally 0.5 mL/kg, without exceeding the maximum dosage of local anesthetic in children. The choice of local anesthetic agent has been reported to be ropivacaine, levobupivacaine, bupivacaine (at concentrations of 0.5%, 0.25%, or 0.375%), and lidocaine (1% or 2% concentration).2,4,28 When choosing a local anesthetic agent, an appropriate agent for single-shot use that would stay below the maximum and daily dosage should be chosen. Higher concentrations may be required for surgical anesthesia and lower concentrations for postoperative analgesia. There is evidence to suggest that dexamethasone being added to peripheral nerve blocks increases the block-effect time, including reports of dexamethasone increasing block time when used in ESPB for chronic pain, neuropathic pain, myofascial pain, and low-back pain. Some reports of ESPB with dexamethasone added to the injectant stand out, eg, dexamethasone was reported to increase analgesia time significantly with no requirement for analgesics in the first 12 hours, with a numeric rating scale (NRS) scores <3 in the first 24 hours.39,40
Literature review for bilateral ESPB
PubMed and Google Scholar were searched on February 10, 2019 using the terms “erector spinae block” and “erector spinae plane block”. Only English-language articles were reviewed. Irrelevant studies, single-sided ESPB, comments, replies, and reviews were excluded, leaving 42 case reports, letters, or case series and seven original research papers. Indications and clinical application sections were evaluated. Also, information was collected on anatomic bases, ESPB-application methods and approaches, and complications from 226 papers related to ESPB.
Reported indications
All indications, features of applied blocks, and authors’ comments are summarized in Table 1 (adult patients) and Table 2 (pediatric patients), with clinical studies summarized in Table 3. The local anesthetics used and their volume, concentration, and dosage, as well as additives, are the respective authors’ choices and do not indicate any suggestions by the authors of this review.
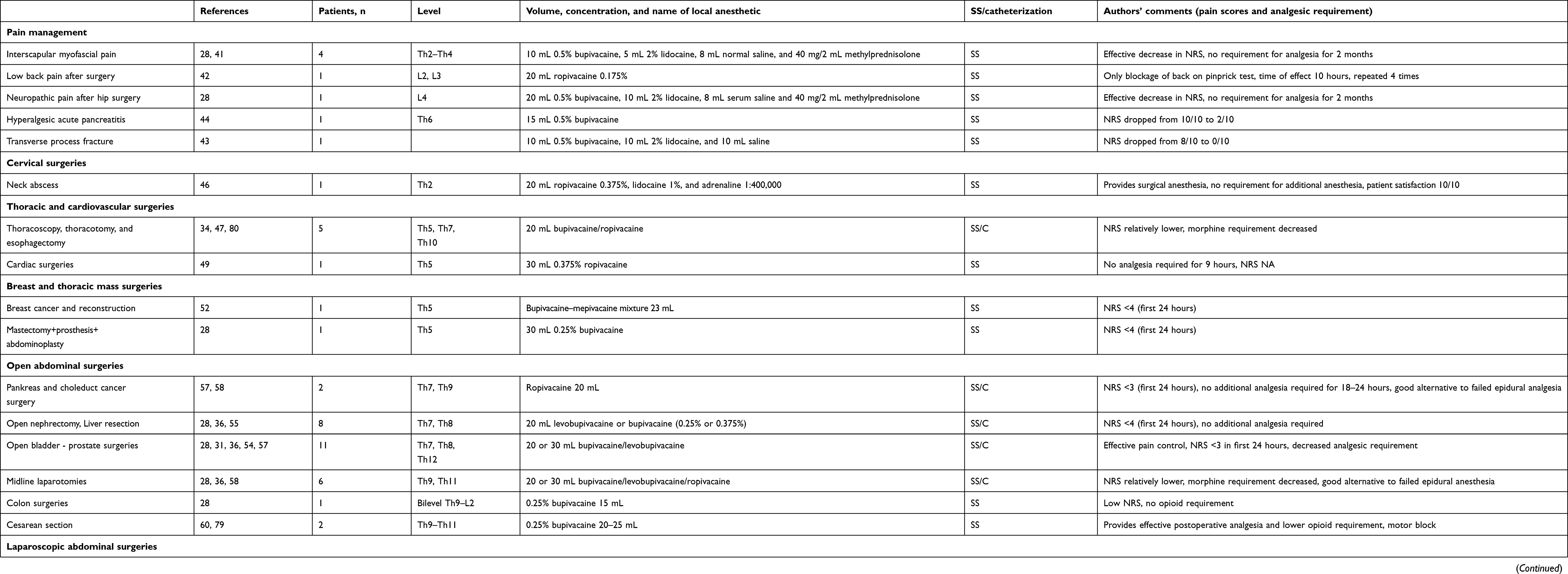 |
Table 1 Adult cases and case series of bilateral erector spinae plane block in the literature |
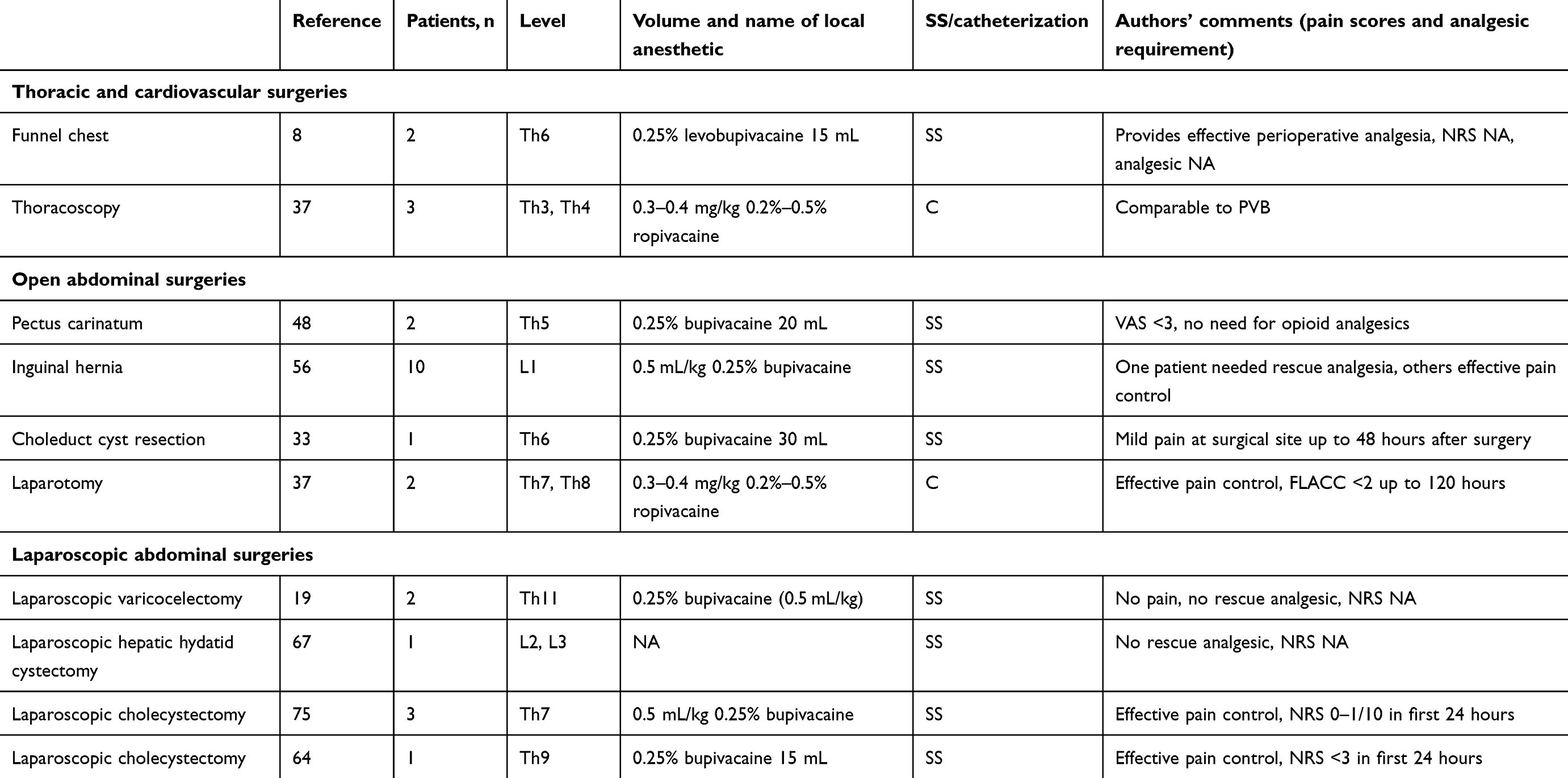 |
Table 2 Pediatric case reports and letters on bilateral erector spinae plane block |
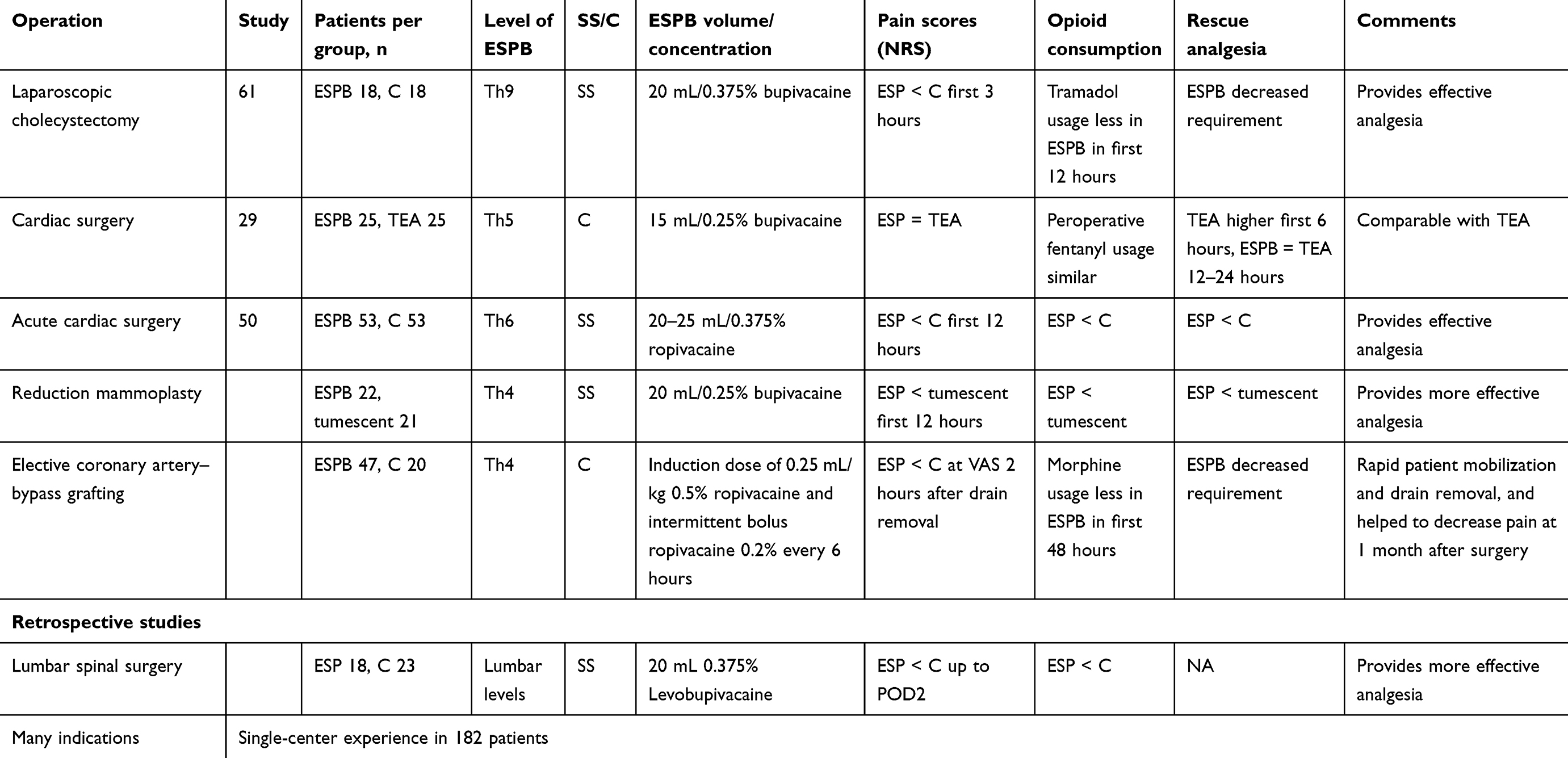 |
Table 3 Prospective randomized and retrospective studies of bilateral erector spinae plane block |
Pain management
As stated previously, ESPB was first described for the treatment of thoracic neuropathic pain.1 Although thereafter publications were nearly all regarding its use for perioperative pain management, there have been a few reports of indications for treatment of chronic pain. Of these, there have been relatively few reports of bilateral ESPB compared to unilateral. Bilateral ESPB has been used in lower cervical and interscapular myofascial pain, as well as chronic low-back pain.28,41,42 Also, bilateral ESPB was used for effective and long-term analgesic in a patient with fracture of the lumbar vertebra transverse process.43
Bilateral ESPB has been reported for effective analgesia in hyperalgesia caused by acute pancreatitis.44 Sensorial block between Th4 and Th10 dermatomes was achieved and NRS dropped from 10/10 to 2/10 when 15 mL 0.5% bupivacaine was applied bilaterally at Th6 level. Acute pancreatitis pain can only be managed through blockage of both visceral and sympathetic fibers of the celiac plexus, which is the continuation of the sympathetic chain branches from Th5 and Th9 nerve roots.45 This case report was in concordance with the findings of Adhikary et al,10 who also reported spread of injectant to the sympathetic chain.
Cervical surgeries
There has been only one case report of bilateral ESPB in the cervical region in a patient undergoing surgery for an abscess involving a large area of the posterior aspect of the neck, severely affecting neck extension and thus intubation, in which bilateral ESPB performed from Th2 was used as the main anesthetic method.46 Despite the requirement of partial local anesthetic infiltration perioperatively, the patient was reported to be highly satisfied with this method.
Thoracic and cardiovascular surgeries
Bilateral ESPB has been most commonly reported for use in thoracic and cardiovascular surgeries. It was first reported for postoperative analgesia requirements in chest-wall deformities, such as funnel chest and pectus carinatum, and thereafter in more complicated procedures, such as video-assisted thoracotomy surgery, thoracostomy, and thoracotomy with esophagectomy.8,34,35,37,47,48 There have been both case reports and clinical studies of bilateral ESPB used in cardiovascular surgeries. Bilateral ESPB led to requirement of no analgesia for the first 9 hours following aortic valve–replacement surgery.49 In a patient undergoing emergency heart surgeries, bilateral ESPB was evaluated in a randomized controlled trial and found to decrease the total rescue analgesia and opioid requirements, as well as NRS scores, in the first 12 hours and also decrease time spent intubated.50
A patient-matched controlled before-and-after study comparing the effects of bilateral ESPB (with catheter) with thoracic epidural analgesia on postoperative pain scores, opioid requirements, and time spent intubated found that extubation times were similar, NRS scores lower at some points but on average generally similar, and the first 48 hours' morphine consumption lower in the ESPB group (40 mg vs none).30 This study clearly demonstrated that bilateral ESPB can be used as an alternative to epidural analgesia in open cardiac surgeries.
Breast and thoracic mass surgeries
Several regional anesthesia techniques, such as pectoral nerve, serratus anterior, and paravertebral blocks, can be used in breast surgeries. ESPB is also now an available option. The majority of studies have been randomized controlled studies in single-sided breast surgery.51There is however a case report of bilateral ESPB being used in bilateral breast surgery for breast cancer and reconstructive surgery.52 Bilateral ESPB has been reported to lead to effective postoperative analgesia in a patient undergoing bilateral mastectomy and abdominoplasty.28 Also, a randomized controlled study compared tumescent anesthesia with bilateral ESPB in reduction mammoplasty, and found that NRS scores and tramadol consumption in the first 24 hours were significantly lower in the ESPB group. Aygun et al53 reported that bilateral ESPB led to effective postoperative analgesia in a subscapular placed bilateral elastofibroma patient.
Open abdominal surgeries
Open abdominal surgeries can lead to severe postoperative pain. While there have not been any clinical studies comparing the effect of bilateral ESPB with other modalities, case reports of bilateral ESPB used for successful postoperative analgesia are available for gastric surgeries, incisional and ventral hernias, living-donor liver transplantations, pancreas and gallbladder-choleduct surgeries, open colon surgeries, emergency ileus surgeries, radical prostatectomy and cystoprostatectomy, pyeloplasty, and many other upper or lower abdominal surgical procedures.33–37,54–58 Its effectiveness for postoperative analgesia has also been reported in cesarean sections.28,59,60
Laparoscopic abdominal surgeries
The source and characteristics of postoperative pain differ in laparoscopic surgery when compared to open procedures.7 One of the components of pain in upper abdominal laparoscopic procedures is the stretching of the peritoneum and peritoneal irritation caused by carbonic anhydrase response to the insufflations of parietal peritoneum with carbon dioxide. In lower abdominal procedures, pain differs according to whether the procedure is preperitoneal or retroperitoneal. While unilateral ESPB is generally sufficient in open surgeries, bilateral ESPB should be the choice in laparoscopic procedures, due to the characteristics and different components of pain. This is surely the reason that clinical trials and case reports on laparoscopic abdominal surgeries are more abundant compared to open procedures. Chin et al6 initially described the bilateral use of ESPB, and was the first to suggest that ESPB had an effect on visceral pain, also reporting that ESPB provided effective analgesia in laparoscopic gastric surgeries.
In the first study to evaluate the effectiveness of bilateral ESPB in laparoscopic abdominal surgeries, patients undergoing laparoscopic cholecystectomy underwent bilateral ESPB from Th9 with 0.375% 20 mL bupivacaine, which was reported to lead to decreased tramadol requirements in the first 12 postoperative hours, as well as decreased NRS scores in the first 3 hours.61 In another study of ESPB in laparoscopic cholecystectomy, unilateral ESPB using lower concentrations of local anesthesia led to statistically significantly less morphine consumption in the first 24 hours (7.5±5.8 mg vs 13.2±5.6 mg) when compared to a control group.62 There have not been any studies comparing differing concentrations of local anesthetic or unilateral ESPB with bilateral ESPB.
Bilateral ESPB has also been reported to be used in many upper and lower abdominal laparoscopic procedures, including laparoscopic sleeve gastrectomy, same-session laparoscopic cholecystectomy and inguinal hernia plus endoscopic retrograde cholangiopancreatography, laparoscopic varicocelectomy, laparoscopic hepatic cyst, laparoscopic nephrectomy, laparoscopic hysterectomy, laparoscopic Nissen fundoplication, laparoscopic hysterectomy, laparoscopic ovarian cystectomy, and laparoscopic hemicolectomy.7,19,22,28,63–67 However, in some cases bilateral ESPB has been reported to result in block failure or lack of efficiency.28
Spinal surgeries
Case reports and case series have reported the use of bilateral ESPB leading to effective perioperative and postoperative analgesia with decreased opioid requirements in cervical, thoracic, and lumbosacral spinal surgeries.32,39,68–73 Also, in a retrospective study, patients in a bilateral ESPB group (20 mL 0.375% bupivacaine) had lower average NRS scores and significantly less fentanyl requirement when compared to a control group (40 [40–60] μg vs 100 [80–100] μg, respectively).74
Pediatric surgeries
The management of postoperative pain in children is especially important. Good pain management leads to decreased postoperative morbidity, early mobilization, and decreased narcotic analgesic use (opioid-sparing effect). With the move from more conventional ultrasound-guided central blocks to peripheral blocks, regional anesthesia methods have become more popular in the pediatric patient group. Although there have been no randomized controlled studies of ESPB in pediatric patients, case series and technical notes have been published. Most cases have involved abdominal procedures, with some reports of ESPB in thoracic, cardiac, and urological procedures, reporting effective postoperative analgesia with a decrease in rescue-analgesia requirements.8,19,33,37,42,48,56,64,67,75 In all cases, ESPB was performed under general anesthesia and preoperatively. While single-shot doses were used in day-surgery cases, catheterization and intermittent boluses have been reported for thoracic and cardiac procedures for postoperative analgesia. There are some limitations to ESPB use in pediatric patients, due to its as yet incompletely understood mechanism of action. The spread of injectant in the paravertebral epidural space and the relationship of this spread and local anesthetic volume has not been studied in children. Pediatric cases of ESPB and their characteristics are shown in Table 2.
Dermatomal analysis
As well as different injectant spread among patients, the distribution of sensorial block may also vary in ESPB. ESPB performed with the same volume at the same level can lead to differing craniocaudal spread and thus sensorial block. Table 4 demonstrates block levels, volume, and content of injectant and the craniocaudal spread of sensorial block for bilateral ESPB applications reported in the literature. It is important to note that even when the same volume and content of injectant is applied at the same level, sensorial block is sometimes limited to the back, with no spread to the side or front of the thorax, and that some lower-volume applications lead to more sensorial block than higher-volume blocks. These are unexpected and unpredicted results of ESPB.
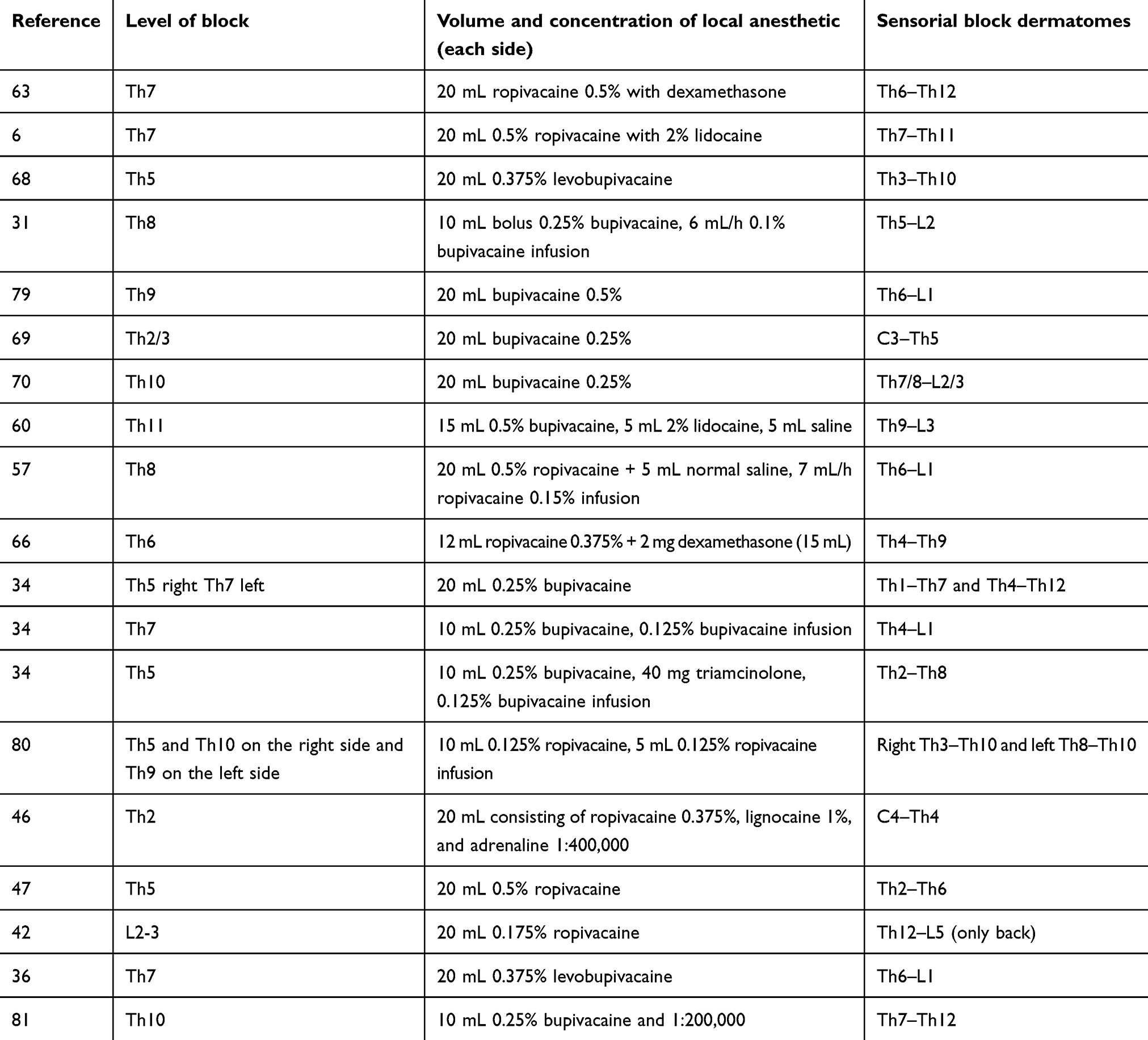 |
Table 4 Dermatomal analysis of bilateral erector spinae plane block from literature review |
Complications
There have been no specific reported complications of bilateral ESPB. The first reported complication of ESPB was pneumothorax.76 Bilateral lower-extremity motor weakness observed after bilateral ESPB in a patient that had undergone cesarean section has been reported, although whether this can be considered a complication of ESPB is a matter of debate.60 It has been reported that ESPB applied from the lumbar or lower thoracic levels may lead to effects similar to lumbar plexus block.23,77 Although motor weakness is not generally considered a complication, it is an unintended event. Therefore, care should be taken in patients undergoing lower thoracic or lumbar ESPB, and motor weakness should be evaluated. In a single-center study of 182 patients undergoing ESPB, one definite and two suspicious cases of minor symptoms of central nervous system local anesthesia toxicity were reported.28A case of priapism has been reported after a single-sided ESPB applied from the fourth lumbar level.78 The authors stated that this was probably due to spread of local anesthetic bilaterally to both sympathetic chains. Therefore, we have included this complication in this review.
Block failure/lack of efficiency
Block failure or lack of efficiency has been reported in two papers. The first was considered a failure of placement of the catheter, as the patient reported severe pain on the relevant side.57 In the second case, ESPB failure/lack of efficiency was reported in 12 patients of 182 (6.5%) that underwent ESPB. The authors reported no common denominator with regard to surgical procedures, application level, applied local anesthetic volume, or concentration in these patients.28 Further studies are required to determine if differences in fascia, incorrect dermatomal choice, or volume/concentration of local anesthetic, as well as the timing of bilateral ESPB, respiratory or abdominal dynamics, and patient position, effect the efficacy of bilateral ESPB.
Concerns and further debate
Bilateral ESPB has become an up-to-date and ambitious modality for the treatment of both chronic and acute or postoperative pain. It is a good alternative to paravertebral block and epidural analgesia in laparoscopic surgery, procedures that require incision in both hemithoraces or hemiabdomens, cardiac surgeries requiring parasternal incision, and gastrointestinal, gynecological, obstetric and urological cases requiring median approaches. Although there have been two clinical studies, most data on bilateral ESPB come from case reports. However, as a regional anesthesia technique, not all aspects of bilateral ESPB have yet become clear. There remain questions to be answered and mechanisms to be revealed.
It is not possible to demonstrate the posterolateral or craniocaudal spread of local anesthetic in this block. Sometimes, a wider range of dermatomal sensorial block can be observed with small volumes compared to larger volumes and sometimes differing sensorial blocks can be reported even when the same volume of injectant is used at the same level.6,35,47 Due to this discrepancy, it is difficult to accurately determine the required volume and level of ESPB block according to the size and incision site of the surgical procedure. These cases will appear in the literature as block failure of lack of efficiency. We believe the best approach is to choose the dermatome in the center of the surgical field and perform a bilateral ESPB.
Cadaveric studies and radiological imaging studies have revealed differing findings.4 In a cadaveric study, Uvanusic et al9 reported that no analgesia spread occurred anteriorly to the transverse process or paravertebral space. The effect of ESPB on blocking visceral pain in laparoscopic surgery and hyperalgesia in acute pancreatitis has however been demonstrated, and even a case of priapism secondary to sympathetic blockage by ESPB has been reported.6,7,44,78 There is no other regional anesthesia technique in which clinical results and anatomic studies differ so much. It is our belief that high-evidence-value clinical studies will bring answers to these questions soon.
In recently published findings of a case series supported by cadaveric data, the effectiveness of bilateral ESPB in open abdominal hysterectomy and spread of local anesthetic was demonstrated.82 In this study, 20 mL methylene blue was administered to each of four cadavers bilaterally from the Th9 level. Dye was then demonstrated to have spread to the the dorsal rami (100%), ventral rami (75%), and ganglion spinale and duramater (62.5%) of the Th9 level. However, as this study did not use fresh cadavers, we were not convinced that the findings have enough evidential quality to be included in our “Spread of injectant: anatomic studies and radiological imaging” section. Despite correlating with clinical findings, these cadaveric findings still require further confirmation. Although only 2.5 years have passed since the first ESPB block was reported, this block has been the subject of case reports and case series of clinical studies that have totaled more than 200 patients. This is due to its ease of application, safety due to the distance of the needle to nervous and vascular structures, presence of the transverse process between them, and the relatively small percentage of complications that have been observed. ESPB has been used in nearly all surgical procedures, other than head and neck, and genital and surgical procedures below the knee have had positive results reported. However, it must, not be forgotten that failed blocks and insufficient dermatomal blockage may also be reported.
There have been few randomized controlled clinical studies comparing bilateral ESPB and other regional anesthesia techniques. It is of course important that this technique provides superior analgesia or decreases opioid requirement when compared to a control group. However, discussions on its efficiency will continue until bilateral ESPB has been compared to paravertebral blocks or epidural analgesia. It is too early to draw clear conclusions on the true efficacy of bilateral ESPB before randomized controlled or comparative studies have been completed.
Another concern is the safety of bilateral ESPB. Literature report have used varying anesthetic agents at differing concentrations. Bilateral ESPB is not comparable to any other interfascial plane block with regard to the point of application. Although it is considered a fascial block, if there is paravertebral and intercostal spread, as is claimed, the amount of spread to this area cannot be predicted.11 If there is a risk of effects similar to paravertebral and intercostal nerve blocks, which have the highest risk of local anesthesia toxicity, unforeseen systemic toxicities may be observed. There is also the requirement for studies on the pharmacokinetics of local anesthetics in unilateral or bilateral ESPB.
Conclusion
When considering that the craniocaudal and vertical spread of local anesthetic and sensorial block is not clearly known or predictable, it seems that the mechanism of ESPB and spread of local anesthetics will be determined through clinical data, unlike other blocks. Despite the relatively small amount of data on bilateral ESPB, it appears to be a promising and effective method. However, randomized controlled studies, comparative studies of ESPB versus other methods, and pharmacokinetic studies of bilateral applications must be the next step in gaining clear understanding of this regional anesthesia technique.
Acknowledgment
The authors would like to thank Associate Professor David Terence Thomas, MD for his contributions to this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621–627. http://dx.doi.org/10.1097/AAP.0000000000000451
2. López MB, Cadórniga ÁG, González JML, Suárez ED, Carballo CL, Sobrino FP. Erector spinae block. A narrative review. Cent Eur J Clin Res. 2018;1(1):28–39. doi:10.2478/cejcr-2018-0005
3. Tsui BCH, Fonseca A, Munshey F, McFadyen G, Caruso TJ. The erector spinae plane (ESP) block: A pooled review of 242 cases. J Clin Anesth. 2018;53:29–34. doi:10.1016/j.jclinane.2018.09.036
4. De Cassai A, Bonvicini D, Correale C, Sandei L, Tulgar S, Tonetti T. Erector spinae plane block: a systematic qualitative review. Minerva Anestesiol. 2019. doi:10.23736/S0375-9393.18.13341-4
5. Chin KJ, Adhikary S, Sarwani N, Forero M. The analgesic efficacy of pre‐operative bilateral erector spinae plane (ESP) blocks in patients having ventral hernia repair. Anaesthesia. 2017. doi:10.1111/anae.13814/full
6. Chin KJ, Malhas L, Perlas A. The erector spinae plane block provides visceral abdominal analgesia in bariatric surgery: a report of 3 cases. Reg Anesth Pain Med. 2017;42(3):372–376. doi:10.1097/AAP.0000000000000615
7. Tulgar S, Selvi O, Kapakli MS. Erector spinae plane block for different laparoscopic abdominal surgeries: case series. Case Rep Anesthesiol. 2018. Available from: https://www.hindawi.com/journals/cria/2018/3947281/abs/.
8. Ueshima H, Otake H. Clinical experiences of erector spinae plane block for children. J Clin Anesth. 2017;44:41.
9. Ivanusic J, Konishi Y, Barrington MJ. A cadaveric study investigating the mechanism of action of erector spinae blockade. Reg Anesth Pain Med. 2018. doi:10.1097/AAP.0000000000000789
10. Adhikary SD, Bernard S, Lopez H, Chin KJ. Erector spinae plane block versus retrolaminar block: a magnetic resonance imaging and anatomical study. Reg Anesth Pain Med. 2018. doi:10.1097/AAP.0000000000000798
11. Schwartzmann A, Peng P, Maciel MA, Forero M. Mechanism of the erector spinae plane block: insights from a magnetic resonance imaging study. Can J Anaesth. 2018. doi:10.1007/s12630-018-1187-y
12. Yang HM, Choi YJ, Kwon HJ, O J, Cho TH, Kim SH. Comparison of injectate spread and nerve involvement between retrolaminar and erector spinae plane blocks in the thoracic region: a cadaveric study. Anaesthesia. 2018;73(10):1244–1250. doi:10.1111/anae.14408
13. Vidal E, Giménez H, Forero M, Fajardo M. Erector spinae plane block: a cadaver study to determine its mechanism of action. Rev Esp Anestesiol Reanim. 2018; Available from: doi:10.1016/j.redar.2018.07.004.
14. Elsharkawy H, Pawa A, Mariano ER. Interfascial plane blocks: back to basics. Reg Anesth Pain Med. 2018;43(4):341–346. doi:10.1097/AAP.0000000000000750
15. Kose HC, Kose SG, Thomas DT. Lumbar versus thoracic erector spinae plane block: similar nomenclature, different mechanism of action. J Clin Anesth. 2018;48:1. doi:10.1016/j.jclinane.2018.03.026
16. Tulgar S, Balaban O. Spread of local anesthetic in erector spine plane block at thoracic and lumbar levels. Reg Anesth Pain Med. 2019;44(1):134–135. doi:10.1136/rapm-2018-000027
17. Balaban O, Tulgar S, Ahiskalioğlu A, Thomas DT, Aydin T. Blockage of thoracoabdominal nerves through perichondrial approach (TAPA) for surgical anesthesia after failed erector spinae plane block in mini-laparatomy. J Clin Anesth. 2018;55:74–75. doi:10.1016/j.jclinane.2018.12.054
18. Ueshima H, Otake H. Limitations of the Erector Spinae Plane (ESP) block for radical mastectomy. J Clin Anesth. 2018;51:97. doi:10.1016/j.jclinane.2018.08.013
19. Aksu C, Gürkan Y. Erector spinae plane block: A new indication with a new approach and a recommendation to reduce the risk of pneumothorax. J Clin Anesth. 2018;54:130–131. doi:10.1016/j.jclinane.2018.11.007
20. Hruschka JA, Arndt CD. Transverse approach to the erector spinae block. Reg Anesth Pain Med. 2018;43(7):805. doi:10.1097/AAP.0000000000000836
21. Philip A, Kaushik V. Erector spinae block: transverse superior to paramedian sagittal? Reg Anesth Pain Med. 2019. doi:10.1136/rapm-2018-100141
22. Yörükoğlu HU, Aksu C, Tor Kılıç C, Gürkan Y. Bilateral erector spinae plane block with single injection. J Clin Monit Comput. 2019. doi:10.1007/s10877-018-00247-y
23. Tulgar S, Senturk O. Ultrasound guided erector spinae plane block at L-4 transverse process level provides effective postoperative analgesia for total hip arthroplasty. J Clin Anesth. 2018;44:68. doi:10.1016/j.jclinane.2017.11.006
24. Tulgar S, Selvi O, Senturk O, Ermis MN, Cubuk R, Ozer Z. Clinical experiences of ultrasound-guided lumbar erector spinae plane block for hip joint and proximal femur surgeries. J Clin Anesth. 2018;47:5–6. doi:10.1016/j.jclinane.2018.02.014
25. Aksu C, Gürkan Y. Aksu approach for lumbar erector spinae plane block for pediatric surgeries. J Clin Anesth. 2018;54:74–75. doi:10.1016/j.jclinane.2018.10.043
26. De Cassai A, Sgarabotto C, Dal Cin S. Old approach for a new indication: shamrock sign for ESP block. Reg Anesth Pain Med. 2019. doi:10.1136/rapm-2018-100170
27. Tulgar S, Unal OK, Thomas DT, Ozer Z. A novel modification to ultrasound guided lumbar erector spinae plane block: Tulgar approach. J Clin Anesth. 2019;56:30–31. doi:10.1016/j.jclinane.2019.01.016
28. Tulgar S, Selvi O, Senturk O, Serifsoy TE, Thomas DT. Ultrasound-guided erector spinae plane block: indications, complications, and effects on acute and chronic pain based on a single-center experience. Cureus. 2019;11(1). Available from: https://www.cureus.com/articles/16824-ultrasound-guided-erector-spinae-plane-block-indications-complications-and-effects-on-acute-and-chronic-pain-based-on-a-single-center-experience.
29. Nagaraja PS, Ragavendran S, Singh NG, et al. Comparison of continuous thoracic epidural analgesia with bilateral erector spinae plane block for perioperative pain management in cardiac surgery. Ann Card Anaesth. 2018;21(3):323–327. doi:10.4103/aca.ACA_174_17
30. Macaire P, Ho N, Nguyen T, et al. Ultrasound-guided continuous thoracic erector spinae plane block within an enhanced recovery program is associated with decreased opioid consumption and improved patient postoperative rehabilitation after open cardiac surgery-a patient-matched, controlled before-and-after study. J Cardiothorac Vasc Anesth. 2018. doi:10.1053/j.jvca.2018.11.021
31. Restrepo-Garces CE, Chin KJ, Suarez P, Diaz A. Bilateral continuous erector spinae plane block contributes to effective postoperative analgesia after major open abdominal surgery: a case report. A A Case Rep. 2017;9(11):319–321. doi:10.1213/XAA.0000000000000605
32. Melvin JP, Schrot RJ, Chu GM, Chin KJ. Low thoracic erector spinae plane block for perioperative analgesia in lumbosacral spine surgery: a case series. Can J Anaesth. 2018;65(9):1057–1065. doi:10.1007/s12630-018-1145-8
33. Singh S, Pandey R, Chowdhary NK. Bilateral ultrasound-guided erector spinae plane block for postoperative analgesia in choledochal cyst resection surgery. Saudi J Anaesth. 2018;12(3):499–500. doi:10.4103/sja.SJA_188_18
34. Jain K, Jaiswal V, Puri A. Erector spinae plane block: Relatively new block on horizon with a wide spectrum of application - A case series. Indian J Anaesth. 2018;62(10):809–813. doi:10.4103/ija.IJA_263_18
35. De Cassai A, Tonetti T, Galligioni H, Ori C. Erector spinae plane block as a multiple catheter technique for open esophagectomy: a case report. Braz J Anesthesiol. 2019;69(1):95–98. doi:10.1016/j.bjane.2018.06.001
36. Niraj G, Tariq Z. Continuous Erector Spinae Plane (ESP) analgesia in different open abdominal surgical procedures: a case series. J Oral Surg Anesth Hosp Dent Serv. 2018. Available from: https://www.ommegaonline.org/article-details/Continuous-Erector-Spinae-Plane-(ESP)-Analgesia-In-Different-Open-Abdominal-Surgical-Procedures:-A-Case-Series/1853.
37. Munshey F, Caruso TJ, Wang EY, Tsui BC. Programmed intermittent bolus regimen for erector spinae plane blocks in children: a retrospective review of a single-institution experience. Anesth Analg. 2018; doi:10.1213/ANE.0000000000003817.
38. Balaban O, Aydın T. Lumbar erector spinae plane catheterization for continuous postoperative analgesia in total knee arthroplasty: A case report. J Clin Anesth. 2019;55:138–139. doi:10.1016/j.jclinane.2018.12.017
39. Calandese F, Adduci A. Erector spinae plane block for acute postoperative pain management after anterior thoracolumbar spine surgery. J Clin Anesth. 2019;52:55–56. doi:10.1016/j.jclinane.2018.08.014
40. Pehora C, Pearson AM, Kaushal A, Crawford MW, Johnston B. Dexamethasone as an adjuvant to peripheral nerve block. Cochrane Database Syst Rev. 2017;11:CD011770.
41. Tulgar S, Thomas DT, Suslu H. Ultrasound guided erector spinae plane block relieves lower cervical and interscapular myofascial pain, a new indication. J Clin Anesth. 2019;53:74. doi:10.1016/j.jclinane.2018.10.008
42. Takahashi H, Suzuki T. Erector spinae plane block for low back pain in failed back surgery syndrome: a case report. JA Clin Rep. 2018;4(1):60. doi:10.1186/s40981-018-0198-6
43. Ahiskalioglu A, Kocak AO, Doymus O, Sengun E, Celik M, Alici HA. Erector spinae plane block for bilateral lumbar transverse process fracture in emergency department: A new indication. Am J Emerg Med. 2018;36(10):
44. Elkoundi A, Eloukkal Z, Bensghir M, Belyamani L, Lalaoui SJ. Erector spinae plane block for hyperalgesic acute pancreatitis. Pain Med. 2018; doi:10.1093/pm/pny232.
45. Vera-Portocarrero L, Westlund KN. Role of neurogenic inflammation in pancreatitis and pancreatic pain. Neurosignals. 2005;14(4):158–165. doi:10.1159/000087654
46. Evans HT, Leslie GJ, Rutka O, Keevil E, Burckett-St Laurent D. Bilateral erector spinae plane block for surgery on the posterior aspect of the neck: a case report. A A Pract. 2018. doi:10.1213/XAA.0000000000000926
47. Fiorelli S, Leopizzi G, Saltelli G, et al. Bilateral ultrasound-guided erector spinae plane block for postoperative pain management in surgical repair of pectus excavatum via Ravitch technique. J Clin Anesth. 2019;56:28–29. doi:10.1016/j.jclinane.2019.01.026
48. Nardiello MA, Herlitz M. Bilateral single shot erector spinae plane block for pectus excavatum and pectus carinatum surgery in 2 pediatric patients. Rev Esp Anestesiol Reanim. 2018;65(9):530–533. doi:10.1016/j.redar.2018.04.006
49. Nakamura RK, Machado FC, Novais LSR. Erector spinae plane block for perioperative analgesia in cardiac surgery. Case Rep Br JP. 2018;1(4):369–371.
50. Krishna SN, Chauhan S, Bhoi D, et al. Bilateral erector spinae plane block for acute post-surgical pain in adult cardiac surgical patients: a randomized controlled trial. J Cardiothorac Vasc Anesth. 2018. doi:10.1053/j.jvca.2018.05.050
51. Gürkan Y, Aksu C, Kuş A, Yörükoğlu UH, Kılıç CT. Ultrasound guided erector spinae plane block reduces postoperative opioid consumption following breast surgery: a randomized controlled study. J Clin Anesth. 2018;50:65–68. doi:10.1016/j.jclinane.2018.06.033
52. Bonvicini D, Tagliapietra L, Giacomazzi A, Pizzirani E. Bilateral ultrasound-guided erector spinae plane blocks in breast cancer and reconstruction surgery. J Clin Anesth. 2017;44:3–4. doi:10.1016/j.jclinane.2017.10.006
53. Aygun H, Akçay O, Thomas DT. Comment to Tulgar et al.“J Clin Anesth 2018; 52: 34–35”and report of bilateral erector spinae plane block usage in bilateral elastofibroma dorsi. J Clin Anesth. 2019;56:108. doi:10.1016/j.jclinane.2019.01.044
54. Tulgar S, Senturk O. Ultrasound guided low thoracic erector spinae plane block for postoperative analgesia in radical retropubic prostatectomy, a new indication. J Clin Anesth. 2018;47:4. doi:10.1016/j.jclinane.2018.02.013
55. Hacibeyoglu G, Topal A, Arican S, Kilicaslan A, Tekin A, Uzun ST. USG guided bilateral erector spinae plane block is an effective and safe postoperative analgesia method for living donor liver transplantation. J Clin Anesth. 2018;49:36–37. doi:10.1016/j.jclinane.2018.06.003
56. Aksu C, Gürkan Y. Opioid sparing effect of Erector Spinae Plane block for pediatric bilateral inguinal hernia surgeries. J Clin Anesth. 2018;50:62–63. doi:10.1016/j.jclinane.2018.06.048
57. Luis-Navarro JC, Seda-Guzmán M, Luis-Moreno C, Chin K-J. Erector spinae plane block in abdominal surgery: case series. Indian J Anaesth. 2018;62(7):549–554. doi:10.4103/ija.IJA_57_18
58. De Cassai A, Cin SD, Zarantonello F, Ban I. Erector spinae plane block as a rescue therapy for uncontrolled pain after laparotomic surgery: a report of two cases. Saudi J Anaesth. 2019;13(1):66–68.
59. Yamak EA, García DS, Fajardo-Pérez M. Erector spinae plane block for analgesia after lower segment caesarean section: case report. Rev Esp Anestesiol Reanim. 2018. Available from http://europepmc.org/abstract/med/29352577.
60. Selvi O, Tulgar S. Ultrasound guided erector spinae plane block as a cause of unintended motor block. Rev Esp Anestesiol Reanim. 2018. doi:10.1016/j.redar.2018.05.009
61. Tulgar S, Kapakli MS, Senturk O, Selvi O, Serifsoy TE, Ozer Z. Evaluation of ultrasound-guided erector spinae plane block for postoperative analgesia in laparoscopic cholecystectomy: A prospective, randomized, controlled clinical trial. J Clin Anesth. 2018;49:101–106. doi:10.1016/j.jclinane.2018.06.019
62. Aksu C, Kuş A, Yörükoğlu HU, Tor Kılıç C, Gürkan Y. The effect of erector spinae plane block on postoperative pain following laparoscopic cholecystectomy: a randomized controlled study. JARSS. 2019. Available from https://www.journalagent.com/anestezi/pdfs/JARSS_27_1_9_14.pdf.
63. Chin KJ, Adhikary S, Sarwani N, Forero M. The analgesic efficacy of pre-operative bilateral erector spinae plane (ESP) blocks in patients having ventral hernia repair. Anaesthesia. 2017;72(4):452–460. doi:10.1111/anae.13814
64. Thomas DT, Tulgar S. Ultrasound-guided erector spinae plane block in a child undergoing laparoscopic cholecystectomy. Cureus [Internet]. 2018; Available from. . https://www.cureus.com/articles/11183-ultrasound-guided-erector-spinae-plane-block-in-a-child-undergoing-laparoscopic-cholecystectomy.
65. Hannig KE, Jessen C, Soni UK, Børglum J, Bendtsen TF. Erector spinae plane block for elective laparoscopic cholecystectomy in the ambulatory surgical setting. Case Rep Anesthesiol [Internet]. 2018. Available from: https://www.hindawi.com/journals/cria/2018/5492527/abs/.
66. Petsas D, Pogiatzi V, Galatidis T, et al. Erector spinae plane block for postoperative analgesia in laparoscopic cholecystectomy: a case report. J Pain Res. 2018;11:1983–1990. doi:10.2147/JPR.S164489
67. Ince I, Aksoy M, Ozmen O. Ultrasound guided erector spinae plane block for postoperative analgesia in a 13 year-old child undergoing abdominal surgery: A new approach. J Clin Anesth. 2018;55:77–78. doi:10.1016/j.jclinane.2018.12.016
68. Ueshima H, Otake H. Clinical experiences of ultrasound-guided erector spinae plane block for thoracic vertebra surgery. J Clin Anesth. 2017;38:137. doi:10.1016/j.jclinane.2016.12.028
69. Ueshima H, Otake H. Blocking of multiple posterior branches of cervical nerves using an erector spinae plane block. J Clin Anesth. 2018;46:44. doi:10.1016/j.jclinane.2018.01.021
70. Singh S, Chaudhary NK. Bilateral ultasound guided erector spinae plane block for postoperative pain management in lumbar spine surgery: a case series. J Neurosurg Anesthesiol [Internet]. 2018. doi:10.1097/ANA.0000000000000518
71. Brandão J, Graça R, Sá M, Cardoso JM, Caramelo S, Correia C. Lumbar erector spinae plane block: successful control of acute pain after lumbar spine surgery - A clinical report. Rev Esp Anestesiol Reanim. 2018. doi:10.1016/j.redar.2018.10.005
72. Cesur S, Yayik AM, Ozturk F, Ahiskalioglu A. Ultrasound-guided low thoracic erector spinae plane block for effective postoperative analgesia after lumbar surgery: report of five cases. Cureus. 2018;10(11):e3603.
73. Chin KJ, Lewis S. Opioid-free analgesia for posterior spinal fusion surgery using erector spinae plane (Esp) blocks in a multimodal anesthetic regimen. Spine. 2018. doi:10.1097/BRS.0000000000002855
74. Ueshima H, Inagaki M, Toyone T, Otake H. Efficacy of the erector spinae plane block for lumbar spinal surgery: a retrospective study. Asian Spine J. 2018. doi:10.31616/asj.2018.0114
75. Aksu C, Gürkan Y. Ultrasound-guided bilateral erector spinae plane block could provide effective postoperative analgesia in laparoscopic cholecystectomy in paediatric patients. Anaesth Crit Care Pain Med. 2018. doi:10.1016/j.accpm.2018.03.008
76. Ueshima H. Pneumothorax after the erector spinae plane block. J Clin Anesth. 2018;48:12.
77. Darling CE, Pun SY, Caruso TJ, Tsui BCH. Successful directional thoracic erector spinae plane block after failed lumbar plexus block in hip joint and proximal femur surgery. J Clin Anesth. 2018;49:1–2.
78. Elkoundi A, Eloukkal Z, Bensghir M, Belyamani L. Priapism following erector spinae plane block for the treatment of a complex regional pain syndrome. Am J Emerg Med. 2019. doi:10.1016/j.ajem.2019.01.012
79. Yamak Altinpulluk E, García Simón D, Fajardo-Pérez M. Erector spinae plane block for analgesia after lower segment caesarean section: case report. Rev Esp Anestesiol Reanim. 2018. doi:10.1016/j.redar.2017.11.006
80. De Cassai A, Tonetti T, Galligioni H, Ori C. [Erector spinae plane block as a multiple catheter technique for open esophagectomy: a case report]. Rev Bras Anestesiol. 2019;69(1):95–98.
81. Wong YC, Shyr MH. Bilateral erector spinae plane blocks using a small volume of local anesthetic for acute pain control after single-port laparoscopic surgery. 2019.Available from: http://www.tcmjmed.com/preprintarticle.asp?id=245947.
82. Altinpulluk EY, Ozdilek A, Colakoglu N, et al. Bilateral postoperative ultrasound-guided erector spinae plane block in open abdominal hysterectomy: a case series and cadaveric investigation. Rom J Anaesth Intensive Care. 2019;26(1):83–88.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.