")
Back to Journals » International Journal of General Medicine » Volume 12
Efficacy of APD in perioperative period of non-abdominal operation for peritoneal dialysis patients
Authors Zhang Y, Feng S, Lu Y, Zhan Z, Shen H
Received 28 January 2019
Accepted for publication 11 April 2019
Published 24 May 2019 Volume 2019:12 Pages 207—212
DOI https://doi.org/10.2147/IJGM.S203158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yi Zhang,* Sheng Feng,* Ying Lu, Zhoubing Zhan, Huaying Shen
Department of Nephrology, The Second Affiliated Hospital of Soochow University, Suzhou, Jiangsu Province, People’s Republic of China
*These authors contributed equally to this work
Objectives: Whether automated peritoneal dialysis (APD) is a feasible strategy in perioperative period of uremic patients undergoing nonabdominal surgery remains unclear. This study was conducted to research the perioperative management and the best choice of dialysis modalities for peritoneal dialysis patients.
Materials and methods: A retrospective analysis was made on the clinical data of 58 ESRD patients who had received peritoneal dialysis for more than three months were treated with APD during perioperative period from July 2015 to March 2018 in the Second Affiliated Hospital of Soochow University. The differences of clinical parameters, such as urine volume, ultrafiltration volume, hemoglobin, renal function and electrolytes were collected and analyzed before and after APD.
Results: The vital signs of 58 patients were stable after APD treatment, and there were no significant differences in 24-hour urine volume, hemoglobin and electrolytes (calcium, phosphorus, potassium, sodium) before and after surgery (P>0.05). Compared with those before treatment, the amount of ultrafiltration increased significantly (P<0.05), creatinine, urea nitrogen and parathyroid hormone decreased significantly (P<0.05), while albumin decreased (P<0.05).
Conclusion: Application of APD for peritoneal dialysis patients undergoing nonabdominal surgery during the perioperative period is safe and effective.
Keywords: automated peritoneal dialysis, peritoneal dialysis, nonabdominal surgery, perioperative period
Introduction
Peritoneal dialysis (PD) has become a common renal replacement therapy for patients with end-stage renal disease (ESRD) because of its advantages in protecting the residual renal function, improving the quality of life, and maintaining the stability of the hemodynamics.1,2 Automated methods for delivering PD to persons with ESRD continue to gain popularity worldwide, particularly in developed countries.3 If one individualizes the therapy by adjusting diurnal dwell times, osmotic agents, and/or dextrose concentration, automated peritoneal dialysis (APD) seems to work for patients of all transport types.4 Its advantages lie not only in the increased ability of APD to achieve adequacy and ultrafiltration targets,5 but also APD can greatly reduce the time the patient dedicates daily to his/her treatment, providing more free time for leisure activities and for work.6 With the continuous improvement of peritoneal dialysis technology, the survival time of patients has improved significantly, and the number of patients who need surgery with complications is increasing.7 In patients with ESRD there are many complications, such as high toxin level, malnutrition, anemia, and abnormal coagulation function, so the risk of operation is significantly higher than that of the normal patients, and the mortality in the perioperative period is also significantly higher.8 In recent years, APD has been reported to be used for emergency dialysis after abdominal wall hernia repair,9 severe heart failure10 and new peritoneal dialysis catheter implantation in peritoneal dialysis patients.11 However, there are few reports on the perioperative application of peritoneal dialysis patients. Especially, for nonabdominal operations, it is still unclear whether the use of APD during the perioperative period can achieve significant clinical efficacy and help patients to pass the perioperative period successfully. Here, we will focus on the role of APD and its functions.
Materials and methods
Participants
Data of 90 ESRD patients with peritoneal dialysis undergoing surgery in the Second Affiliated Hospital of Soochow University from July 2015 to March 2018 were collected. Inclusion criteria included: age between 18 and 70 years, male or female; diagnosis of ESRD; peritoneal dialysis treatment ≥3 months; need APD treatment during perioperative period after nonabdominal due to various complications. The following criteria were used to exclude patients from this study: patients undergoing abdominal surgery; patients undergoing temporary hemodialysis or continuous renal replacement therapy (CRRT) treatment during the perioperative period. Finally, a total of 58 cases were included in the study. The relevant clinical data and laboratory indexes were recorded before and after APD treatment.
Dialysis mode
All patients were treated with Baxter’s dual system dialysis pipeline and lactate dialysate in the continuous ambulatory peritoneal dialysis(CAPD) or daytime ambulatory peritoneal dialysis(DAPD) before operation and the regimens were 3–5 cycles of 2,000 mL over 2 hours . The patients who have undergo surgical treatment were treated with the mode of continuous circulating peritoneal dialysis (CCPD) with FM-1 APD machine made by China Jilin Provincial Morestep Medical Equipment Co., Ltd. During the day, 2 L peritoneal dialysate was placed in the abdomen. At night, the dialysate was exchanged 3–4 times by computer operation, 1–3 L each time. Specific types of peritoneal dialysis fluid depend on the patient’s own situation.
Data collection
The general information for each research object(age,gender, start time of dialysis, primary diseases, complications), and surgical related data (operative name, surgical related diseases) were all enrolled. At the same time, the laboratory data, 24- hour urine volume, ultrafiltration, hemoglobin (Hb), serum creatinine (Scr), urea nitrogen (BUN), calcium, phosphorus, potassium, sodium, parathyroid hormone (PTH) and blood albumin (Alb), and other related indexes were observed before and after the treatment of APD.
Statistical methods
Statistical analyses were performed using SPSS for Windows version 22.0 (IBM Corporation, Armonk, NY, USA, ). Continuous data were expressed as mean ± SD, and categorical data were expressed as absolute value and percentage. Normal distribution data were analyzed by the paired t-test and nonparametric tests are used for data which do not conform to normal distribution. P<0.05 was considered statistically significant.
Ethical considerations
Ethical approval was obtained from the Ethics Committee of the Second Affiliated Hospital of Soochow University. The requirement to obtain written informed consent from each patient was waived because this was an observational retrospective study. All patient information was confidential, and data were analyzed anonymously. This study was conducted in accordance with the Declaration of Helsinki.
Results
Demographic and baseline characteristics of subjects
A total of 58 ESRD patients who were treated with APD during the perioperative period were enrolled, including 31 (53.4%) males and 27 (46.6%) females, with an average age of 55.41±13.94 (range: 22–69) years. The average age of dialysis in these 58 patients was 46.31±21.24 months. The other baseline conditions and surgical classification of 58 patients are detailed in Table 1.
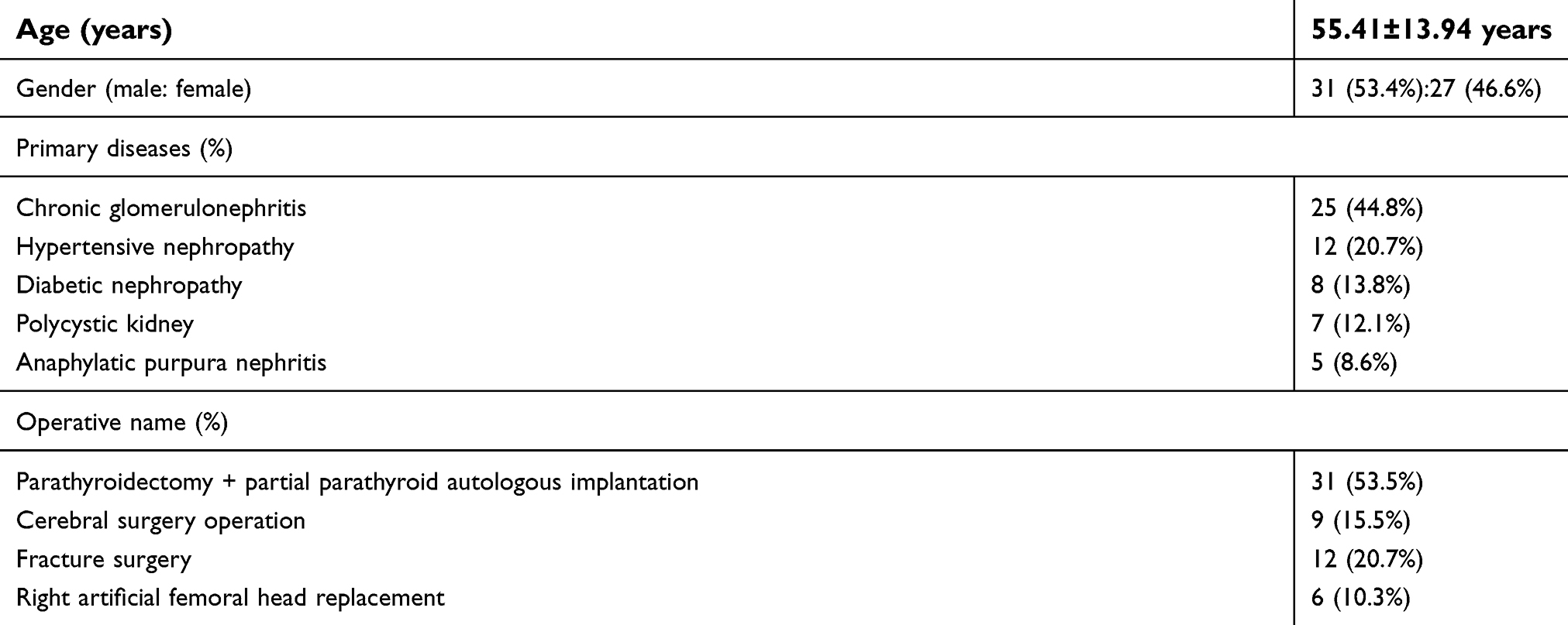 | Table 1 Baseline conditions and surgical classification |
Comparison of changes in parameters before and after APD treatment
All patients who met the criteria were treated with automated peritoneal dialysis on the first day postoperation. After one week of APD treatment, there was no significant difference in 24-hour urine volume, hemoglobin and electrolyte (calcium, phosphorus, potassium and sodium) in 58 patients (P>0.05). However, the amount of ultrafiltration increased significantly, creatinine, urea nitrogen, PTH and so on significantly decreased, albumin was lower than before treatment, the difference was statistically significant (all P<0.05, Table 2).
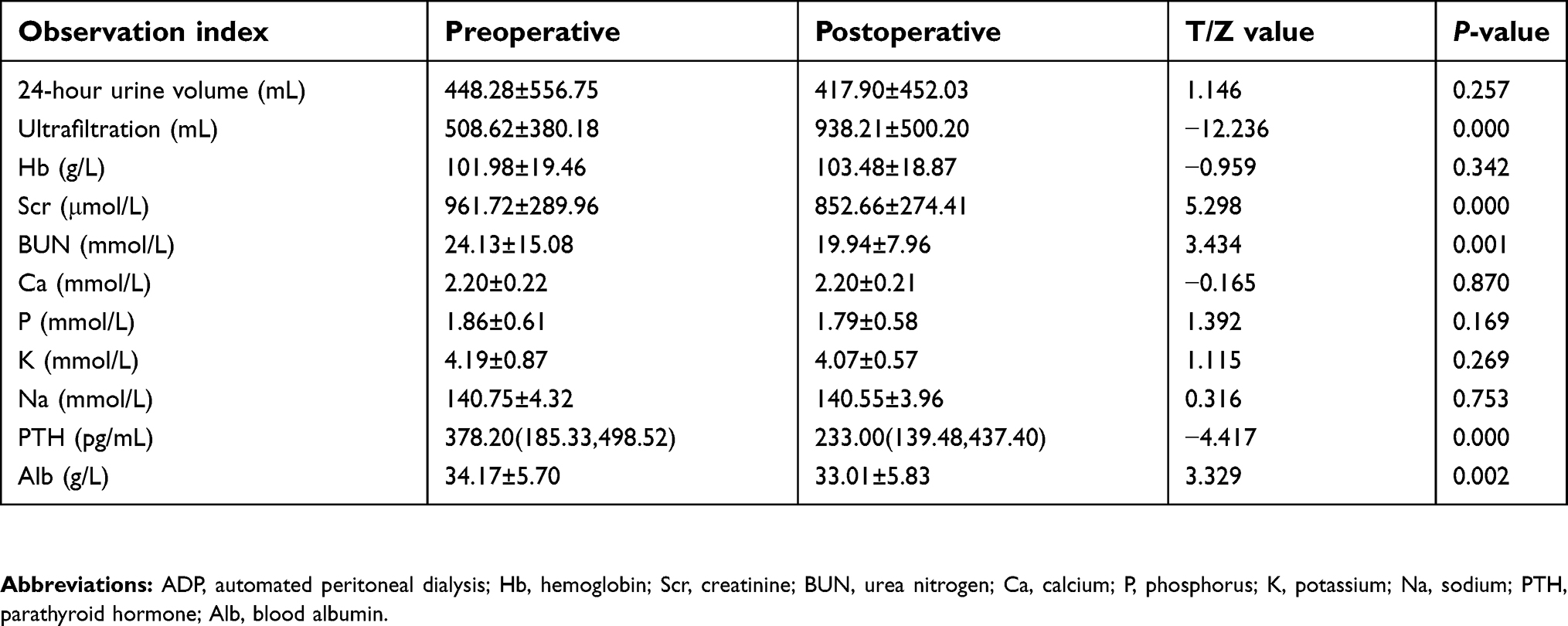 | Table 2 Comparison of changes in parameters before and after APD treatment |
There were 2 patients with complications after operation, one of which was local infection and bleeding and the other one was bleeding after parathyroidectomy. All patients improved after treatment with anti-infection and hemostasis.
Discussion
With the increasing number of patients with ESRD, the number of patients requiring surgical treatment due to uremia-related complications such as secondary hyperparathyroidism, fracture and a series of other factors is increasing. At present, no consensus has been reached on the selection of dialysis mode during perioperative period in China. The traditional view is peritoneal dialysis patients need to change into hemodialysis or CRRT during the perioperative period.12 Abroad, there are many studies on APD in peritonitis,13 residual renal function,14 quality of life15 and survival rate,16 but the application of APD in the perioperative period is very rare. Therefore, the study of APD in perioperative peritoneal dialysis patients with nonabdominal surgery has a certain clinical significance.
Notably, the utilization of APD is increasing worldwide. The latest research shows that the number of APD treatment models used in the long-term maintenance of peritoneal dialysis in Canada is more than 60%, and the proportion in the US has already increased from 54% to 70%.17,18 However, in China, APD treatment has not yet been included in the coverage of medical insurance, so the use of APD is far less frequent than in Western countries.
With the development of the world economy, the utilization and related studies of APD at home and abroad have been increasing year by year. APD has been reported to be used for urgent-start PD treatment,19–21 heart failure,10,22 and sleep monitoring.23 However, the application of APD in the perioperative period of nonabdominal operation in peritoneal dialysis patients still needs further study. The clinical effect of APD during nonabdominal operation is discussed in order to provide the basis for the selection of perioperative dialysis methods for peritoneal dialysis patients.
Our study found that 58 peritoneal dialysis patients using APD treatment can successfully pass the perioperative period, no serious complications. By comparing the 24-hour urine volume and ultrafiltration volume before and after APD treatment, we found that there was no significant difference in 24-hour urine volume before and after APD treatment, but the ultrafiltration volume after APD treatment was remarkably increased,24,25 which plays an important role in maintaining the postoperative volume balance of patients.26 The hemoglobin and electrolyte levels of the patients were basically stable before and after treatment, which was helpful to maintain the stability of the internal environment. Similar to the relevant findings, serum creatinine and urea nitrogen levels were significantly descendant after APD than before, suggesting that APD treatment can more thoroughly remove toxins and improve dialysis adequacy.27,28 These findings were similar to the previous results. The decrease of PTH after nonabdominal surgery in this study was probably attributed to the high proportion of parathyroidectomy, which was the side-effect of parathyroidectomy,29 but not to APD. In addition, APD treatment has a side effect, that is, the patient’s albumin decreased significantly, considered may be related to the surgical stress consumption and APD itself lead to protein loss. A recent study suggested that peritoneal albumin loss might even be somewhat higher in APD compared to CAPD patients.30 From this point of view, this result may be explained. To sum up, the utilization of APD during nonabdominal surgery perioperative period can improve ultrafiltration capacity, eliminate toxins, control volume, correct water, electrolyte and acid-base balance disorders. Therefore, APD treatment can be considered as an effective and enforceable strategy.
In clinical work, many doctors may prefer that CRRT has little effect on hemodynamics and can maintain the stability of arterial pressure and effective renal perfusion to a certain extent.31 However, CRRT requires temporary hemodialysis catheterization, which may increase the risk of infection and prolong hospitalization.32–37 APD treatment does not require additional blood purification pathways, and its clinical operation is simple and can reduce the workload of medical staff and patients. And compared with hemodialysis, the low cost of APD treatment can reduce the economic burden of patients to a large extent.38
This study was a single-center, retrospective cohort study with a relatively small sample size. Therefore, the clinical application of APD in the perioperative period of peritoneal dialysis still needs to be further confirmed by multicenter clinical research.
Conclusion
APD mode can effectively remove uremic toxins, correct electrolyte imbalance and reduce capacity load. The application of APD is safe and effective for peritoneal dialysis patients undergoing nonabdominal surgery during the perioperative period.
Acknowledgments
This work was supported by grants from the National Nature Science Foundation of China (81400762), and the Science and Technology Project of Suzhou, Jiangsu Province, China (SYS201469).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu FX, Gao X, Inglese G, Chuengsaman P, Pecoits-Filho R, Yu A. A global overview of the impact of peritoneal dialysis first or favored policies: an opinion. Perit Dial Int. 2015;35(4):406–420. doi:10.3747/pdi.2013.00204
2. Choy AS, Li PK. Sustainability of the peritoneal dialysis-first policy in Hong Kong. Blood Purif. 2015;40(4):320–325. doi:10.1159/000441580
3. Correa-Rotter R. APD in the developing world: is there a future? Semin Dial. 2002;15(6):385–387.
4. Bieber SD, Burkart J, Golper TA, Teitelbaum I, Mehrotra R. Comparative outcomes between continuous ambulatory and automated peritoneal dialysis: a narrative review. Am J Kidney Dis. 2014;63(6):1027–1037. doi:10.1053/j.ajkd.2013.11.025
5. Liakopoulos V, Dombros N. Patient selection for automated peritoneal dialysis: for whom, when? Perit Dial Int. 2009;29(Suppl 2):S102–S107.
6. Bro S, Bjorner JB, Tofte-Jensen P, et al. A prospective, randomized multicenter study comparing APD and CAPD treatment. Perit Dial Int. 1999;19(6):526–33.3.
7. Ladjevic N, Kalezic N, Ladjevic IL, Vuksanovic A, Durutovic O, Jovanovic D. Preoperative assessment of patients with end stage renal failure. Acta Chir Iugosl. 2011;58(2):131–136.
8. Thourani VH, Sarin EL, Keeling WB, et al. Long-term survival for patients with preoperative renal failure undergoing bioprosthetic or mechanical valve replacement. Ann Thorac Surg. 2011;91(4):1127–1134. doi:10.1016/j.athoracsur2010.12.056
9. Wakasugi M, Hirata T, Okamura Y, et al. Perioperative management of continuous ambulatory peritoneal dialysis patients undergoing inguinal hernia surgery. Surg Today. 2011;41(2):297–299. doi:10.1007/s00595-009-4237-9
10. Yang C, Liu J, Gong N, et al. Automated peritoneal dialysis could rapidly improve left heart failure by increasing peritoneal dialysis ultrafiltration: a single-center observational clinical study. Clin Nephrol. 2018;89(6):422–430. doi:10.5414/CN109303
11. Liu S, Zhuang X, Zhang M, et al. Application of automated peritoneal dialysis in urgent-start peritoneal dialysis patients during the break-in period. Int Urol Nephrol. 2018;50(3):541–549. doi:10.1007/s11255-018-1785-1
12. Morris-Stiff GJ, Bowrey DJ, Jurewicz WA, Lord RH. Management of inguinal herniae in patients on continuous ambulatory peritoneal dialysis: an audit of current UK practice. Postgrad Med J. 1998;74(877):669–670.
13. Sanchez AR, Madonia C, Rascon-Pacheco RA. Improved patient/technique survival and peritonitis rates in patients treated with automated peritoneal dialysis when compared to continuous ambulatory peritoneal dialysis in a Mexican PD center. Kidney Int Suppl. 2008;108:S76–S80. doi:10.1038/sj.ki.5002606
14. Michels WM, Verduijn M, Grootendorst DC, et al. Decline in residual renal function in automated compared with continuous ambulatory peritoneal dialysis. Clin J Am Soc Nephrol. 2011;6(3):537–542. doi:10.2215/CJN.00470110
15. Yang F, Luo N, Lau T, Yu ZL, Foo M, Griva K. Health-related quality of life in patients treated with continuous ambulatory peritoneal dialysis and automated peritoneal dialysis in Singapore. Pharmacoecon Open. 2018;2(2):203–208. doi:10.1007/s41669-017-0046-z
16. Michels WM, Verduijn M, Boeschoten EW, Dekker FW, Krediet RT. Similar survival on automated peritoneal dialysis and continuous ambulatory peritoneal dialysis in a large prospective cohort. Clin J Am Soc Nephrol. 2009;4(5):943–949. doi:10.2215/CJN.04440908
17. Van Biesen W, Veys N, Vanholder R, Lameire N. The role of APD in the improvement of outcomes in an ESRD program. Semin Dial. 2002;15(6):422–426.
18. Jain AK, Blake P, Cordy P, Garg AX. Global trends in rates of peritoneal dialysis. J Am Soc Nephrol. 2012;23(3):533–544. doi:10.1681/ASN.2011060607
19. Jo YI, Shin SK, Lee JH, Song JO, Park JH. Immediate initiation of CAPD following percutaneous catheter placement without break-in procedure. Perit Dial Int. 2007;27(2):179–183.
20. Stegmayr BG. Three purse-string sutures allow immediate start of peritoneal dialysis with a low incidence of leakage. Semin Dial. 2003;16(4):346–348.
21. Povlsen JV, Ivarsen P. How to start the late referred ESRD patient urgently on chronic APD. Nephrol Dial Transplant. 2006;21(Suppl 2):ii56–ii59. doi:10.1093/ndt/gfl192
22. Gotloib L, Fudin R. The impact of peritoneal dialysis upon quality of life and mortality of patients with end-stage congestive heart failure. Contrib Nephrol. 2006;150:247–253. doi:10.1159/000093602
23. Roumelioti ME, Argyropoulos C, Pankratz VS, et al. Objective and subjective sleep disorders in automated peritoneal dialysis. Can J Kidney Health Dis. 2016;3(6):93. doi:10.1186/s40697-016-0093-x.
24. Mujais S, Nolph K, Gokal R, et al. Evaluation and management of ultrafiltration problems in peritoneal dialysis. International society for peritoneal dialysis ad hoc committee on ultrafiltration management in peritoneal dialysis. Perit Dial Int. 2000;20(Suppl 4):S5–S21.
25. Eloot S, Vanholder R, Dequidt C, Van Biesen W. Removal of different classes of uremic toxins in APD vs CAPD: a randomized cross-over study. Perit Dial Int. 2015;35(4):436–442. doi:10.3747/pdi.2013.00202
26. Karkar A, Abdelrahman M. Outcome of patients treated with automated peritoneal dialysis: effects of selection of patients. Saudi J Kidney Dis Transpl. 2011;22(1):40–48.
27. Brown EA, Davies SJ, Rutherford P, et al. Survival of functionally anuric patients on automated peritoneal dialysis: the European APD outcome study. Clin J Am Soc Nephrol. 2003;14(11):2948–2957. doi:10.1097/01.ASN.0000092146.67909.E2
28. Vega ND, Gallego R, Oliva E, et al. Nocturnal ultrafiltration profiles in patients on APD: impact on fluid and solute transport. Kidney Int Suppl. 2008;73(108):S94–S101. doi:10.1038/sj.ki.5002609
29. Wan J, Li W, Zhong Y, et al. Parathyroidectomy decreases serum intact parathyroid hormone and calcium levels and prolongs overall survival in elderly hemodialysis patients with severe secondary hyperparathyroidism. J Clin Lab Anal. 2018;33(3):e22696.doi: 10.1002/jcla.22696.
30. Westra WM, Kopple JD, Krediet RT, Appell M, Mehrotra R. Dietary protein requirements and dialysate protein losses in chronic peritoneal dialysis patients. Perit Dial Int. 2007;27(2):192–195.
31. Cornejo R, Downey P, Castro R, et al. High-volume hemofiltration as salvage therapy in severe hyperdynamic septic shock. Intensive Care Med. 2006;32(5):713–722. doi:10.1007/s00134-006-0118-5
32. Aslam N, Bernardini J, Fried L, Burr R, Piraino B. Comparison of infectious complications between incident hemodialysis and peritoneal dialysis patients. Clin J Am Soc Nephrol. 2006;1(6):1226–1233. doi:10.2215/CJN.01230406
33. Brain M, Winson E, Roodenburg O, McNeil J. Non anti-coagulant factors associated with filter life in continuous renal replacement therapy (CRRT): a systematic review and meta-analysis. BMC Nephrol. 2017;18(1):69. doi:10.1186/s12882-017-0445-5
34. Kairaitis LK, Gottlieb T. Outcome and complications of temporary haemodialysis catheters. Nephrol Dial Transplant. 1999;14(7):1710–1714.
35. Oliver MJ, Callery SM, Thorpe KE, Schwab SJ, Churchill DN. Risk of bacteremia from temporary hemodialysis catheters by site of insertion and duration of use: a prospective study. Kidney Int. 2000;58(6):2543–2545. doi:10.1046/j.1523-1755.2000.00439.x
36. Parienti JJ, Dugue AE, Daurel C, et al. Continuous renal replacement therapy may increase the risk of catheter infection. Clin J Am Soc Nephrol. 2010;5(8):1489–1496. doi:10.2215/CJN.02130310
37. Lok CE, Foley R. Vascular access morbidity and mortality: trends of the last decade. Clin J Am Soc Nephrol. 2013;8(7):1213–1219. doi:10.2215/CJN.01690213
38. Gouveia D, Bignelli AT, Hokazono SR, et al. Analysis of economic impact between the modality of renal replacement therapy. J Bras Nefrol. 2017;39(2):162–171. doi:10.5935/0101-2800.20170019
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.