Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 17
Efficacy of Adding Intravenous Methylprednisolone to Nebulized Budesonide in RSV Pneumonia: Modification by Bacterial Co-Infection – A Retrospective Cohort Study
Authors Guo C ![]() , Guo T, Chen W, Guo G
, Guo T, Chen W, Guo G
Received 28 January 2026
Accepted for publication 7 May 2026
Published 17 May 2026 Volume 2026:17 599427
DOI https://doi.org/10.2147/PHMT.S599427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Can Guo, Tingyao Guo, Wenjuan Chen, Guojing Guo
Department of Pediatrics, Fuqing City Hospital of Fujian, Fuqing, Fujian, People’s Republic of China
Correspondence: Can Guo, Email [email protected]
Purpose: To evaluate the efficacy of intravenous methylprednisolone plus nebulized budesonide (IV+NEB CS) versus nebulized budesonide alone (NEB CS) in infants with RSV pneumonia, and to assess the influence of bacterial co-infection.
Methods: This retrospective study included 303 patients (≤ 36 months) with RSV pneumonia. Patients were divided into IV+NEB CS (n=140) and NEB CS (n=163) groups, then stratified by bacterial co-infection and antibiotic use. Primary outcomes were time to cough/fever/wheezing relief, disappearance of pulmonary signs, hospital stay, and glucocorticoid-related adverse events.
Results: (1) Wheezing relief was faster in the IV+NEB CS group [2.0 (1.5,4.0) vs 3.0 (2.0,4.0) days, P=0.010], but other outcomes did not differ. (2) Subgroup B (IV+NEB CS without bacterial infection) had the shortest median wheezing relief [2.0 (1.0,3.0) days], pulmonary sign resolution [4.0 (3.0,5.0) days], and hospital stay [4.0 (3.0,5.0) days]. (3) Antibiotic use was independently associated with shorter symptom relief and discharge (all P< 0.001); after adjusting for antibiotics, the main effect of IV+NEB CS was no longer significant for most outcomes. (4) Antibiotics also reduced CRP levels (P=0.002). (5) Adverse event rates did not differ between groups.
Conclusion: In non-severe RSV pneumonia, adding intravenous methylprednisolone to nebulized budesonide provides no consistent independent benefit after accounting for antibiotic use. The apparent faster recovery with combination therapy was largely explained by antibiotics. Routine intravenous corticosteroids are not recommended. When bacterial co-infection is suspected, antibiotics should be prioritized.
Keywords: respiratory syncytial virus, corticosteroids, lower respiratory tract infection, infants and toddlers, antibiotics
Introduction
Respiratory syncytial virus (RSV) is the primary cause of lower respiratory tract infections in infants and young children globally. In 2019, epidemiological data indicated that RSV-associated acute lower respiratory tract infections resulted in 3.6 million hospitalizations worldwide among this population. The mortality rate for children under 60 months was 1.6–2.4%, with more than 95% of these deaths occurring in low- and middle-income countries.1 Mortality statistics indicate that respiratory syncytial virus (RSV) is a leading cause of death from acute lower respiratory tract infections in children, surpassed only by pneumococcal pneumonia and Haemophilus influenzae type B.2
Current clinical management of RSV pneumonia is primarily supportive, as specific antiviral agents are unavailable.3,4 As potent anti-inflammatory agents, nebulized glucocorticoids can shorten the duration of clinical symptoms in children with mild to moderate disease, as demonstrated in some studies. This benefit arises from their strong local effects and reduced systemic adverse reactions.5,6 However, research indicates that RSV infection can inhibit glucocorticoid receptor regulatory gene expression in small airway epithelial cells,7 which may constrain the efficacy of locally administered glucocorticoids. Furthermore, respiratory viral infections can exacerbate host immunopathological damage and foster secondary bacterial infections through the excessive production of inflammatory cytokines.8,9 For children with rapidly progressing disease or severe symptoms, nebulized glucocorticoids alone may be insufficient to rapidly control systemic inflammation. Combining intravenous and nebulized administration offers a dual-route anti-inflammatory strategy. This approach may theoretically enhance efficacy through synergistic effects.
In clinical practice, intravenous methylprednisolone is occasionally administered to children with prominent wheezing or a suspected hyperinflammatory response, particularly when nebulized therapy alone fails to control symptoms.10 Methylprednisolone is selected for its potent systemic anti-inflammatory effect and rapid onset of action. Conversely, budesonide is preferred for nebulization owing to its high topical potency and favorable safety profile in infants.11
Currently, no consensus exists on employing combination therapy for RSV pneumonia. While intravenous glucocorticoids demonstrate clear benefits in conditions like acute pediatric asthma,12,13 their mechanism of action, appropriate patient populations, and optimal dosing for RSV pneumonia require further study. Specifically for non-severe infants and young children, high-quality clinical evidence supporting the efficacy and safety advantages of combination therapy remains lacking, which constrains clinical decision-making.
This retrospective cohort study evaluated the clinical efficacy of intravenous methylprednisolone combined with nebulized budesonide for treating RSV pneumonia in infants and young children. We specifically assessed its effects on the time to relief of key symptoms, the recovery of pulmonary signs, and the length of hospital stay. The findings provide evidence to help optimize anti-inflammatory treatment strategies for this population.
Subjects and Methods
Study Subjects
A retrospective analysis was conducted on pediatric patients hospitalized for RSV pneumonia at Fuqing City Hospital of Fujian between September 2021 and April 2025. Patients were categorized into two groups based on the treatment regimen actually received during hospitalization, as documented in electronic medical records: an exposed group receiving intravenous methylprednisolone combined with nebulized budesonide (IV+NEB CS) and an unexposed group receiving nebulized budesonide alone (NEB CS). Those diagnosed with bacterial co-infection via positive sputum culture received intravenous ceftriaxone or ceftazidime as anti-infective therapy. To evaluate the potential influence of antibiotic use, each treatment group was further stratified by antibiotic administration, yielding four subgroups: Group A (IV+NEB CS with bacterial infection), Group B (IV+NEB CS without bacterial infection), Group C (NEB CS with bacterial infection), and Group D (NEB CS without bacterial infection).
Inclusion Criteria
(1) Age ≤36 months; (2) Diagnosis of RSV pneumonia confirmed by etiological and radiological examinations; (3) Fulfilling the diagnostic criteria for community-acquired pneumonia.14
Exclusion Criteria
(1) Severe pneumonia;15 (2) Concomitant infection with other viruses or atypical pathogens; (3) Coexisting airway foreign body, asthma, pulmonary tuberculosis, bronchopulmonary dysplasia, or other respiratory diseases; (4) Dysfunction of other organs such as heart, liver, or kidney; (5) Presence of other systemic diseases; (6) Discharge before completion of treatment or inability to collect complete clinical data for other reasons.
Medication Administration
Both groups received nebulized budesonide at 1 mg twice daily. The exposed group also received a daily intravenous infusion of methylprednisolone at 1–2 mg/kg body weight, whereas the unexposed group did not.
Patients with suspected bacterial co-infection (based on positive sputum culture or clinical criteria) received intravenous ceftriaxone (50–80 mg/kg/day) or ceftazidime (30–50 mg/kg/day) as anti-infective therapy, administered for 5–7 days according to standard pediatric protocols. Details of antibiotic administration were extracted from medication records.
Data Collection
General information and clinical characteristics included gender, age in months, height in centimeters, weight in kilograms, body mass index (BMI, kg/m2), the interval from symptom onset to admission in days, and prior antibiotic use.
Clinical efficacy was assessed by recording the time in days to cough relief, fever resolution, wheezing relief, disappearance of pulmonary signs, and the total hospital stay.
Laboratory indicators comprised the pre- to post-treatment differences in serum white blood cell (WBC, ×109/L) count and serum C-reactive protein (CRP, g/L) levels.
Glucocorticoid-related adverse reactions, including hyperglycemia, gastrointestinal reactions, gastrointestinal bleeding, and neuropsychiatric behavioral abnormalities, were documented.
Statistical Methods
Statistical analyses were conducted with IBM SPSS Statistics 27. Normally distributed continuous variables are expressed as mean ± standard (mean ± SD) deviation and were compared across groups using one-way ANOVA; when ANOVA indicated significant differences, post hoc pairwise comparisons were performed with the least significant difference method. Non-normally distributed data are reported as median (interquartile range)[M (IQR)] and were compared using the Kruskal–Wallis H-test, followed by Mann–Whitney U-tests with adjusted significance levels for post hoc analysis. Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate. For time-to-event outcomes (eg, time to symptom relief), we assumed that all hospitalized patients achieved resolution before discharge, as severe pneumonia cases were excluded and no loss to follow-up occurred. A generalized linear model (GLM) with gamma distribution and log link function was employed to analyze the effects of treatment regimen (IV+NEB CS vs NEB CS), antibiotic use (yes vs no), and their interaction on clinical efficacy outcomes. This approach is appropriate for right-skewed continuous outcomes such as duration days. Main effects and interaction effects were estimated with adjustment for potential confounders (age, sex, BMI, time from onset to admission). Adjusted differences among the four subgroups (A/B/C/D) were evaluated. A P-value of less than 0.05 was considered statistically significant.
Ethics
This study received approval from the Ethics Committee of Fuqing City Hospital of Fujian (approval number: K(2025)15). The committee waived the requirement for informed consent because the research involved only the anonymized collection and retrospective analysis of existing data. All procedures strictly adhered to the principles of the Declaration of Helsinki and relevant ethical guidelines.
Results
From September 2021 to April 2025, 335 pediatric patients hospitalized with respiratory syncytial virus (RSV) pneumonia at Fuqing City Hospital of Fujian met the inclusion criteria. After excluding 32 cases based on the exclusion criteria, 303 patients were enrolled, comprising 140 in the exposed group and 163 in the unexposed group. Based on the presence of bacterial infection and antibiotic use, these patients were further categorized into four subgroups: Group A (n=40), Group B (n=100), Group C (n=37), and Group D (n=126).
Baseline Comparison
Status of Antibiotic Use
Antibiotics were administered for concomitant pulmonary bacterial infection to 40 children (28.6%) in the exposed group and 37 children (22.7%) in the unexposed group. The rate of antibiotic use did not differ significantly between the groups (P=0.242), which confirms a balanced distribution of this treatment (Table 1).
 |
Table 1 Comparison of Antibiotic Usage Between the Exposed and Unexposed Group |
General Demographic and Clinical Features
Gender: The male proportion was 65.0% in group A, 54.8% in group B, 43.2% in group C, and 55.6% in group D. Gender distribution did not differ significantly among the four subgroups (P=0.292) (Table 2).
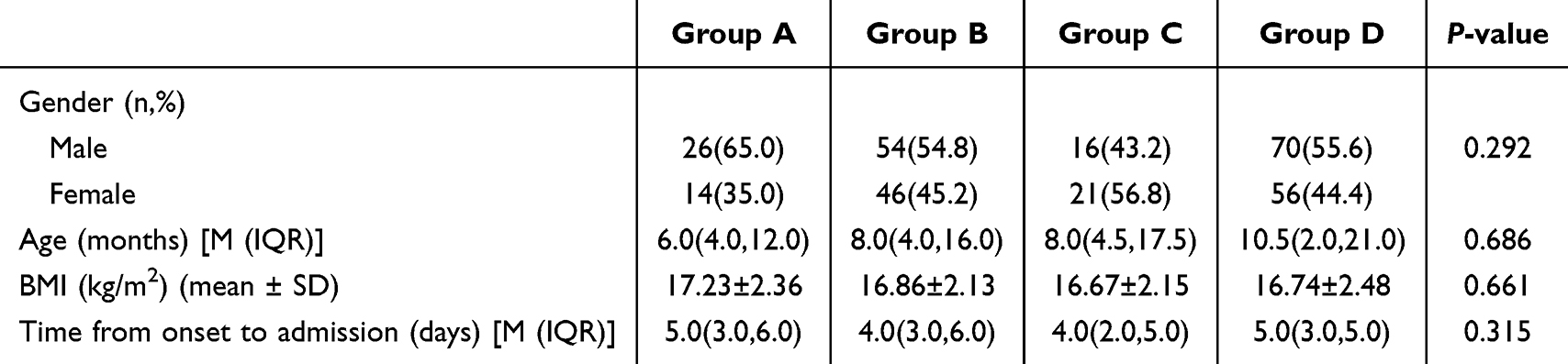 |
Table 2 Comparison of General Demographic and Clinical Features |
Age: The median age was 6.0 (4.0, 12.0) months in group A, 8.0 (4.0, 16.0) months in group B, 8.0 (4.5, 17.5) months in group C, and 10.5 (2.0, 21.0) months in group D. No statistically significant difference in age was observed among the four subgroups (P=0.686) (Table 2).
BMI: The mean BMI was 17.23 ± 2.36 kg/m2 in group A, 16.86 ± 2.13 kg/m2 in group B, 16.67 ± 2.15 kg/m2 in group C, and 16.74 ± 2.48 kg/m2 in group D. No statistically significant difference in BMI was observed among the four subgroups (P=0.661) (Table 2).
Time from onset to admission: The median time from onset to admission was 5.0 (3.0, 6.0) days in group A, 4.0 (3.0, 6.0) days in group B, 4.0 (2.0, 5.0) days in group C, and 5.0 (3.0, 5.0) days in group D. No statistically significant difference was observed among the four subgroups (P=0.315) (Table 2).
Clinical Efficacy
Exposed Group vs Unexposed Group
No significant differences were observed between the two groups in the time to cough relief, time to fever resolution, disappearance of pulmonary signs, or total hospitalization duration (P>0.05). The time to wheezing relief was significantly shorter in the exposed group than in the unexposed group [2.0 (1.5, 4.0) days vs 3.0 (2.0, 4.0) days, P=0.010] (Table 3).
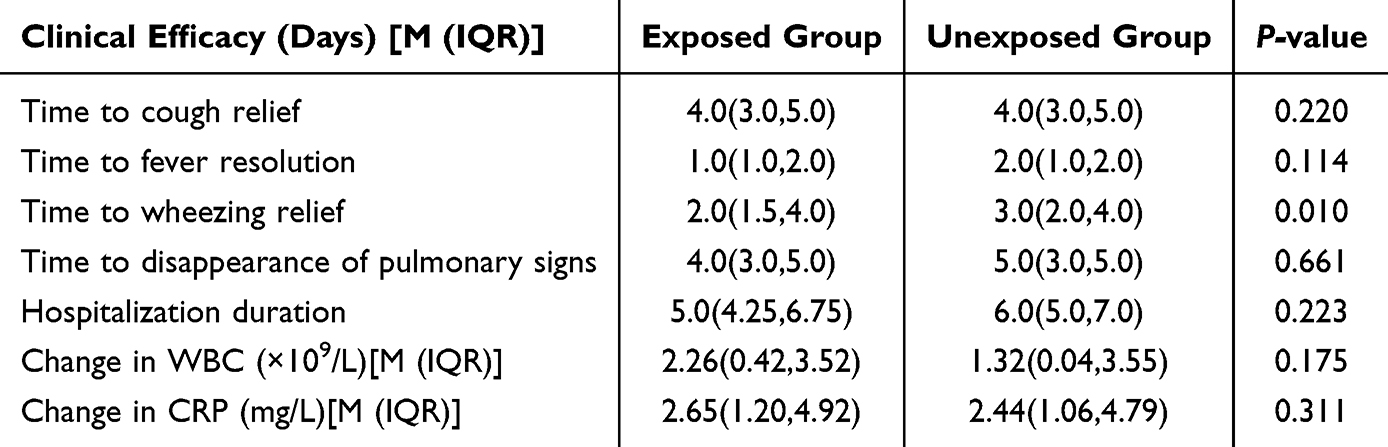 |
Table 3 Comparison of Clinical and Laboratory Indicators Efficacy Between Exposed and Unexposed Group |
Impact of Treatment Regimen and Antibiotic Use
Antibiotic treatment significantly reduced the time to cough relief (P<0.001), the time to resolution of pulmonary signs (P<0.001), the time to wheezing relief (P<0.001), and the duration of hospitalization (P<0.001) (Table 4).
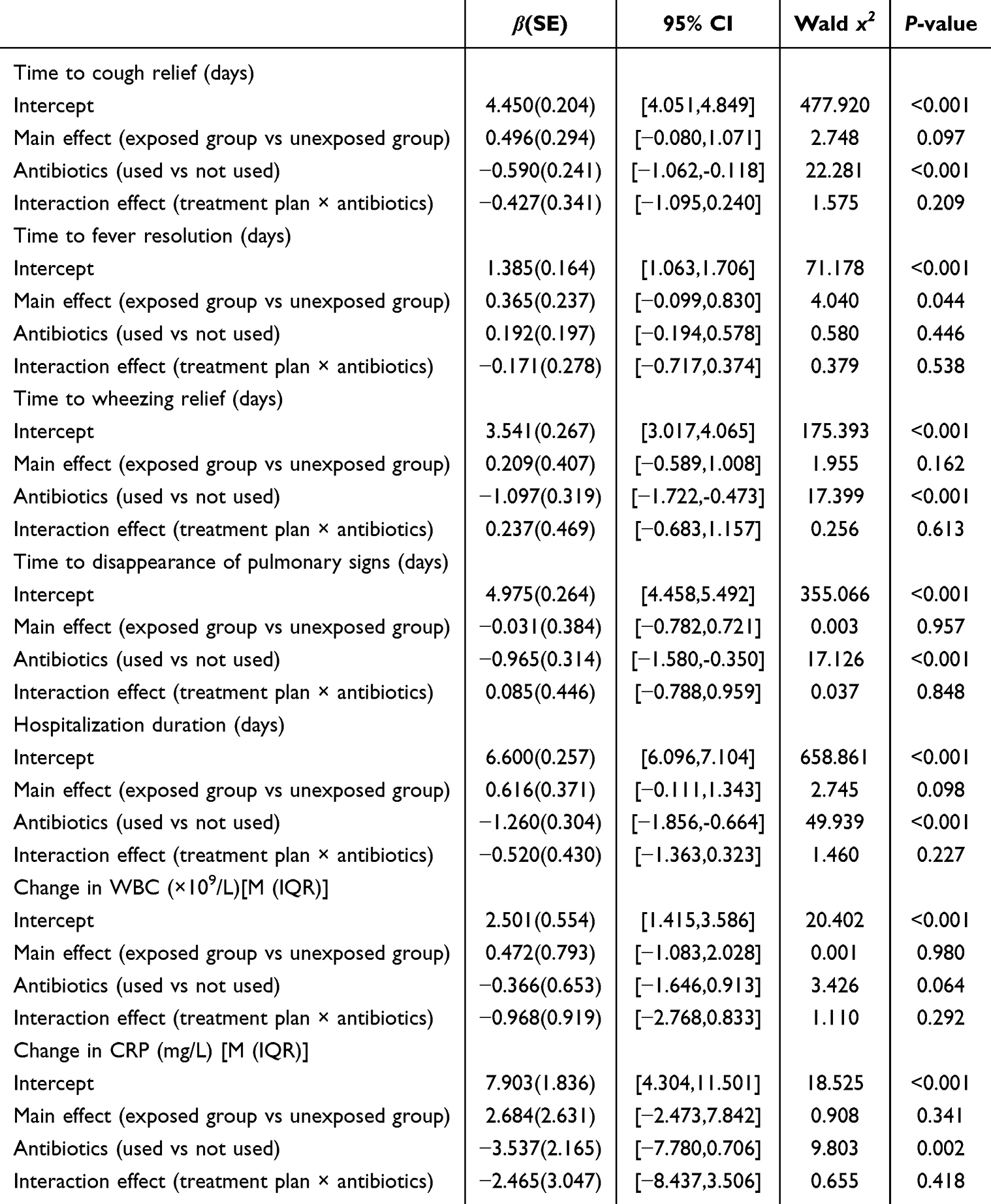 |
Table 4 Impact of Treatment Regimen and Antibiotics on Clinical Outcomes and Laboratory Indicators |
The main effect of the treatment regimen significantly reduced the time to fever resolution (P=0.044), though it did not significantly affect the other efficacy outcomes (Table 4). Notably, after adjusting for antibiotic use in the GLM, the main effect of IV+NEB CS on wheezing relief was no longer significant (P=0.162), indicating that the observed difference between exposed and unexposed groups in the unadjusted comparison (Table 3) was largely driven by antibiotic use rather than intravenous corticosteroids.
The interaction between treatment regimen and antibiotic use did not significantly affect any efficacy outcome (P>0.05) (Table 4).
Subgroup Comparison of Clinical Efficacy
Time to cough relief: The time to cough relief was significantly shorter in Group D [4.0 (3.0, 5.0) days] than in Group C [5.0 (4.0, 6.0) days] (P<0.001) (Table 5). Although the median and interquartile range (IQR) for Group A and Group B were identical [both 4.0 (3.0, 5.0) days], the difference between Group A and Group B was statistically significant (P = 0.014). As shown in Figure 1, the lower whisker of Group B extended to 1 day, whereas that of Group A extended only to 2 days, indicating a more favorable distribution of cough relief times in Group B despite identical median and IQR. This distributional difference explains the significant result from the Mann–Whitney U-test, which is based on rank sums rather than direct median comparison.
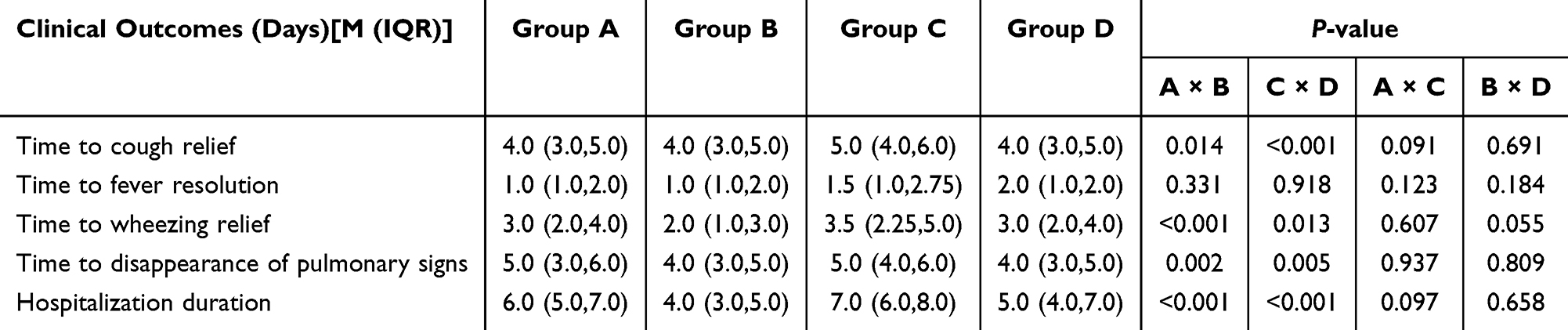 |
Table 5 Comparison of Clinical Outcomes Between Subgroups |
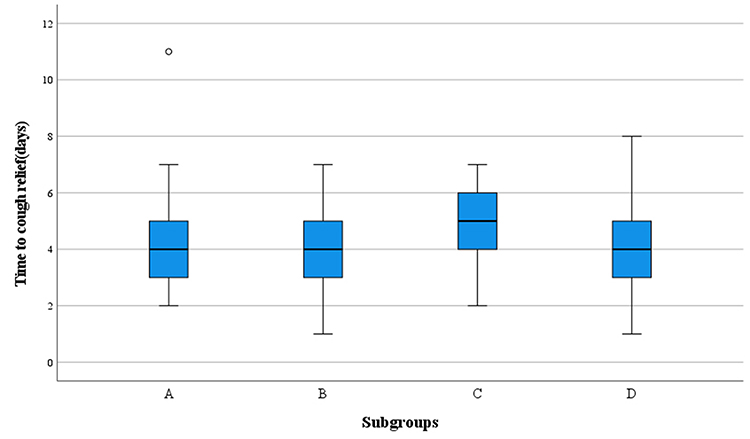 |
Figure 1 Boxplot of time to cough relief (days) among the four subgroups. |
Time to fever resolution: No statistically significant differences were observed among the subgroups regarding the time to fever resolution. (P>0.05) (Table 5).
Time to wheezing relief: The median time to wheezing relief in Group B [2.0 (1.0, 3.0) days] was significantly shorter than that in Group A [3.0 (2.0, 4.0) days] (P < 0.001). The median time in Group D [3.0 (2.0, 4.0) days] was slightly shorter than that in Group C [3.5 (2.25, 5.0) days] (P = 0.013) (Table 5).
Time to disappearance of pulmonary signs: The time to disappearance of pulmonary signs in Group B [4.0 (3.0, 5.0) days] was significantly shorter than that in Group A [5.0 (3.0, 6.0) days] (P=0.002). Similarly, the time in Group D [4.0 (3.0, 5.0) days] was significantly shorter than that in Group C [5.0 (4.0, 6.0) days] (P=0.005) (Table 5).
Hospitalization duration: Group B [4.0 (3.0, 5.0) days] was significantly shorter than Group A [6.0 (5.0, 7.0) days] (P<0.001), and Group D [5.0 (4.0, 7.0) days] was significantly shorter than Group C [7.0 (6.0, 8.0) days] (P<0.001) (Table 5).
Laboratory Indicators
Exposed Group vs Unexposed Group
The change in WBC [exposed group: 2.26 (0.42, 3.52) ×109/L vs unexposed group: 1.32 (0.04, 3.55) ×109/L] and CRP [exposed group: 2.65 (1.20, 4.92) mg/L vs unexposed group: 2.44 (1.06, 4.79) mg/L] from before to after treatment showed no statistically significant differences between the two groups (P>0.05) (Table 3).
Impact of Treatment Regimen and Antibiotic Use
Antibiotic administration significantly reduced CRP levels (P=0.002), though it did not significantly affect WBC levels (P=0.064) (Table 4).
Neither the main effect of treatment regimen nor its interaction with antibiotic use significantly influenced changes in WBC or CRP (P>0.05) (Table 4).
Comparison of Laboratory Indicators Among Subgroups
Change in WBC: The change in WBC was larger in Group C [3.05 (0.94, 4.56) ×109/L] than in Group D [1.01 (−0.13, 3.35) ×109/L, P=0.039] (Table 6).
 |
Table 6 Comparison of Laboratory Indicators Among Subgroups |
Change in CRP: The CRP difference was significantly higher in group C [2.90 (2.06, 13.75) mg/L] than in group D [2.23 (0.51, 3.89) mg/L, P=0.005] (Table 6).
Glucocorticoid-Related Adverse Reactions
No statistically significant difference was observed between the two groups in the incidence of hyperglycemia, gastrointestinal reactions, or neuropsychiatric behavioral abnormalities following glucocorticoid treatment (P>0.05). Gastrointestinal bleeding did not occur in either group (Table 7).
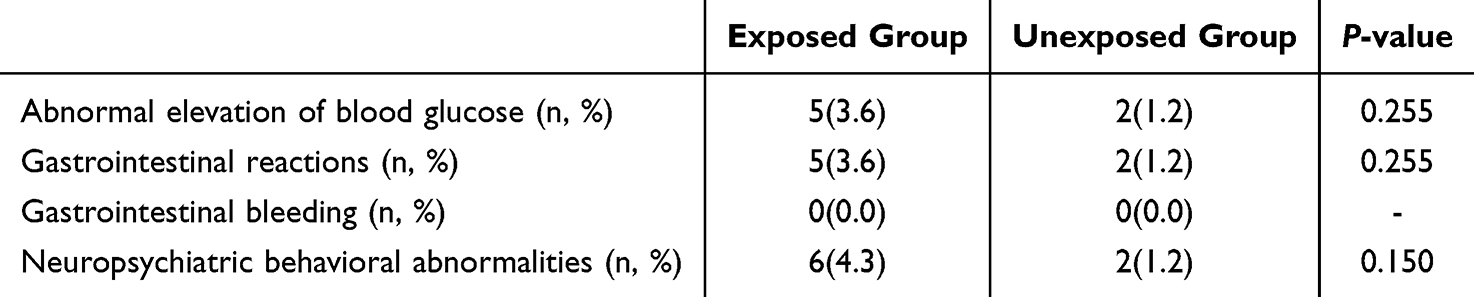 |
Table 7 Comparison of Glucocorticoid-Related Adverse Reactions Between the Exposed and Unexposed Group |
Discussion
This retrospective cohort study examines differences in efficacy between intravenous plus nebulized corticosteroids (IV+NEB CS) and nebulized corticosteroids alone (NEB CS) for treating respiratory syncytial virus (RSV) pneumonia in infants and young children, particularly regarding coexisting bacterial infection and antibiotic use. Our results indicate that children without bacterial infection who received IV+NEB corticosteroids (Group B) exhibited shorter wheezing duration, more rapid resolution of pulmonary signs, and a reduced hospital stay compared to those with bacterial infection receiving the same regimen (Group A). This comparison, however, does not isolate the effect of intravenous corticosteroids, as Groups A and B differed in both bacterial infection status and antibiotic use. Comparisons between groups with similar infection status (B versus D, and A versus C) revealed no statistically significant differences for any outcome (all P>0.05; Table 5). Consequently, we cannot attribute a “pronounced efficacy” to IV+NEB corticosteroids independent of bacterial infection control. The data instead imply that the presence of bacterial co-infection and concomitant antibiotic use are the predominant factors influencing recovery. The faster recovery observed in Group B relative to Group A is therefore likely attributable to the absence of bacterial infection—and thus no requirement for antibiotics—rather than to the intravenous corticosteroid component. This interpretation aligns with the non-significant interaction terms in the GLM (Table 4) and the absence of significant differences between B versus D and A versus C.
Although prior work has shown that RSV infection induces glucocorticoid receptor phosphorylation in airway epithelial cells, which diminishes corticosteroid sensitivity.16,17 Dual-route administration regimen, which suppresses systemic inflammation via the intravenous route while achieving high local drug concentrations in the airways via nebulization, may provide broader anti-inflammatory coverage.11,18 While Table 3 shows a significant difference in wheezing relief between the exposed and unexposed groups (P=0.010), the GLM adjusted for antibiotic use reveals that the main effect of IV+NEB CS is not significant (P=0.162, Table 4). This indicates that the apparent benefit of combination therapy in the crude comparison is confounded by antibiotic use. The only robust conclusion, therefore, is that antibiotic use—not intravenous corticosteroids—is consistently associated with improved outcomes across multiple domains. This finding suggests a shift in the underlying pathophysiology, indicating that the therapeutic focus should move from immunosuppression to anti-infective management.19,20 Importantly, the addition of intravenous methylprednisolone did not increase the incidence of glucocorticoid-related adverse events (Table 7), which supports its short-term safety profile in this population despite the absence of clinical benefit.
Previous studies confirm that bacterial co-infection exacerbates RSV pneumonia severity and prolongs hospitalization,21,22 a finding consistent with evidence that RSV impairs mucosal immunity and increases susceptibility to Streptococcus pneumoniae and Haemophilus influenzae.23 A large multicenter cohort study by Peña-López et al reported that although bacterial co-infection rates in RSV are low, they are associated with worse outcomes, and current evidence advises against indiscriminate antibiotic usage even in severe cases.24 Our subgroup analysis supports this: patients with bacterial co-infection (Groups A and C) had longer hospital stays and slower symptom resolution compared to those without co-infection (Groups B and D). Furthermore, among co-infected patients, the addition of IV+NEB CS (Group A) provided no additional benefit over NEB CS alone (Group C), suggesting that bacterial clearance outweighs supplementary anti-inflammatory effects. This suggests that in children with bacterial co-infection, recovery may be driven primarily by bacterial clearance, which outweighs the supplementary anti-inflammatory effects.19 This underscores the need to diagnose bacterial co-infection, through careful clinical evaluation or guided by biomarkers, prior to escalating immunosuppressive therapy.25,26
In our GLM analysis, antibiotic treatment significantly reduced time to symptom relief and hospital stay (all P<0.001). However, as the South African guidelines emphasize, antibiotics should not be used routinely in bronchiolitis but reserved for cases where bacterial co-infection is strongly suspected.27 This underscores the importance of accurate diagnosis of bacterial co-infection prior to escalating therapy.
This study has several limitations. First, the retrospective design may retain residual confounding despite statistical adjustments. Bacterial infection was defined clinically, and stratification could be refined by incorporating procalcitonin or culture data. Second, the analysis did not stratify patients by methylprednisolone dosage, leaving potential dose-dependent effects for future investigation. Finally, long-term outcomes such as recurrent wheezing were not systematically assessed.28 Future randomized controlled trials should address these limitations and include viral load monitoring, inflammatory biomarker measurement, and predefined subgroup analyses (eg, by bacterial co-infection status) to better define which children—if any—might benefit from systemic corticosteroids.
Conclusion
In infants and young children with non-severe RSV pneumonia, adding intravenous methylprednisolone to nebulized budesonide offers no consistent independent benefit after accounting for antibiotic use. The apparent faster recovery with combination therapy was largely explained by antibiotic treatment. Therefore, routine intravenous corticosteroids are not recommended. When bacterial co-infection is suspected, antibiotics should be prioritized, as they independently improve outcomes while corticosteroids provide no additional advantage. Future randomized trials are needed to identify potential subgroups that might benefit from systemic corticosteroids.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request. Due to patient privacy and institutional policies, de-identified data will be shared upon reasonable request to Can Guo, the corresponding author.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Fuqing City Hospital of Fujian (approval number: K(2025)15). The study strictly adhered to the Declaration of Helsinki and relevant ethical guidelines.
Consent for Publication
The requirement for informed consent was waived by the Ethics Committee, as the study involved only anonymized retrospective data collection and analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Li Y, Wang X, Blau DM, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet. 2022;399(10340): 2047–10. doi:10.1016/S0140-6736(22)00478-0
2. Nair H, Nokes DJ, Gessner BD, et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: a systematic review and meta-analysis. Lancet. 2010;375(9725): 1545–1555. doi:10.1016/S0140-6736(10)60206-1
3. Meissner HC. Viral bronchiolitis in children. N Engl J Med. 2016;374(1):62–72.
4. Brady MT, Byington CL, Davies HD, et al; Committee on Infectious Diseases and Bronchiolitis Guidelines Committee. Updated guidance for palivizumab prophylaxis among infants and young children at increased risk of hospitalization for respiratory syncytial virus infection. Pediatrics. 2014;134(2):e620–e638.
5. Kajosaari M, Syvänen P, Förars M, Juntunen-Backman K. Inhaled corticosteroids during and after respiratory syncytial virus-bronchiolitis may decrease subsequent asthma. Pediatr Allergy Immunol. 2000;11(3):198–202.
6. Hesselmar B, Adolfsson S. Inhalation of corticosteroids after hospital care for respiratory syncytial virus infection diminishes development of asthma in infants. Acta Paediatr. 2001;90(3):260–263.
7. Jeanette IWM, Jacqueline C, Michael NT. The respiratory syncytial virus (RSV) nonstructural proteins mediate RSV suppression of glucocorticoid receptor transactivation. Virology. 2014;449:62–69.
8. Beadling C, Slifka MK. How do viral infections predispose patients to bacterial infections? Curr Opin Infect Dis. 2004;17(3):185–191.
9. Rich HE, Bhutia S, Gonzales de Los Santos F, et al. RSV enhances Staphylococcus aureus bacterial growth in the lung. Infect Immun. 2024;92(10):e00304–e00324.
10. Yue L, Yan Y. Effects of methylprednisolone combined with advanced antibiotics and antiviral drugs on serum immunoglobulin and inflammatory factor levels in patients with viral pneumonia. Cell Mol Biol. 2023;69(15):154–159. doi:10.14715/cmb/2023.69.15.27
11. Rizz MC, Solé D. Inhaled corticosteroids in the treatment of respiratory allergy: safety vs efficacy. J Pediatr. 2006;82:S198–S205.
12. Roddy MR, Sellers AR, Darville KK, et al. Dexamethasone versus methylprednisolone for critical asthma: a single center, open-label, parallel-group clinical trial. Pediatr Pulmonol. 2023;58(6):1719–1727.
13. Gummalla P, Weaver D, Ahmed Y, Shah V, Keenaghan M, Doymaz S. Intravenous methylprednisolone versus intravenous methylprednisolone combined with inhaled budesonide in acute severe pediatric asthma. J Asthma. 2020;58(11):1512–1517.
14. Zar HJ, Jeena P, Argent A, Gie R, Madhi SA. Diagnosis and management of community-acquired pneumonia in childhood--South African Thoracic Society Guidelines. S Afr Med J. 2005;95(12 Pt 2):977–981, 984–990.
15. Dean P, Florin TA. Factors associated with pneumonia severity in children: a systematic review. J Pediatric Infect Dis Soc. 2018;7(4):323–334. doi:10.1093/jpids/piy046
16. Shi T, Denouel A, Tietjen AK, et al. Global disease burden estimates of respiratory syncytial virus-associated acute respiratory infection in older adults in 2015: a systematic review and meta-analysis. J Infect Dis. 2019;222(Supplement_7):S577–S783.
17. Agac A, Kolbe SM, Ludlow M, Osterhaus AD, Meineke R, Rimmelzwaan GF. Host responses to respiratory syncytial virus infection. Viruses. 2023;15(10):1999.
18. Rhen T, Cidlowski JA. Antiinflammatory action of glucocorticoids--new mechanisms for old drugs. N Engl J Med. 2005;353(16):1711–1723.
19. de Steenhuijsen Piters WA, Sanders EA, Bogaert D. The role of the local microbial ecosystem in respiratory health and disease. Philos Trans R Soc Lond B Biol Sci. 2015;370(1675):20140294.
20. Shah NS, Greenberg JA, McNulty MC, et al. Bacterial and viral co-infections complicating severe influenza: incidence and impact among 507 U.S. patients, 2013–14. J Clin Virol. 2016;80:12–19.
21. Cortazzo V, Agosta M, De Rose DU, et al. Clinical relevance of bacterial and/or viral coinfection in acute bronchiolitis in an Italian neonatal unit during the 2021–2023 seasons. Front Pediatr. 2025;13:1577913.
22. van Houten CB, Naaktgeboren C, Buiteman BJ, et al. Antibiotic overuse in children with respiratory syncytial virus lower respiratory tract infection. Pediatr Infect Dis J. 2018;37(11):1077–1081.
23. Smith CM, Sandrini S, Datta S, et al. Respiratory syncytial virus increases the virulence of Streptococcus pneumoniae by binding to penicillin binding protein 1a. A new paradigm in respiratory infection. Am J Respir Crit Care Med. 2014;190(2):196–207.
24. Peña-López Y, Sabater-Riera J, Raj P. Severe respiratory syncytial virus disease. J Intensive Med. 2024;4(4):405–416. doi:10.1016/j.jointm.2024.03.001
25. Giulia B, Luisa A, Concetta S, Bruna LS, Chiara B, Marcello C. Procalcitonin and community-acquired pneumonia (CAP) in children. Clin Chim Acta. 2015;451:215–218.
26. Waldron CA, Pallmann P, Schoenbuchner S, et al. Effectiveness of biomarker-guided duration of antibiotic treatment in children hospitalised with confirmed or suspected bacterial infection: the BATCH RCT. Health Technol Assess. 2025;29(16):1.
27. Green RJ, Zar HJ, Jeena PM, Madhi SA, Lewis H. South African guideline for the diagnosis, management and prevention of acute viral bronchiolitis in children. S Afr Med J. 2010;100(5):320–325. doi:10.7196/SAMJ.4016
28. Bont L, Van Aalderen WM, Kimpen JL. Long-term consequences of respiratory syncytial virus (RSV) bronchiolitis. Paediatr Respir Rev. 2003;1(3):221–227.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Long-Term Healthcare Utilization and Economic Burden of RSV Infection in Children ≤5 Years in Japan: Propensity Score Matched Cohort Study
Chirikov V, Botteman M, Simões EAF
ClinicoEconomics and Outcomes Research 2022, 14:699-714
Published Date: 9 November 2022