")
Back to Journals » International Journal of General Medicine » Volume 16
Efficacy and Safety of QiShen YiQi Dripping Pills in the Treatment of Coronary Heart Disease Complicating Chronic Heart Failure (Syndrome of Qi Deficiency with Blood Stasis): Study Protocol for a Randomized, Placebo-Controlled, Double-Blind and Multi-Centre Phase II Clinical Trial
Authors He X, Jiang Y, Li S, Liu D, Li Z, Han X, Zhang X, Dong X, Liu H, Huang J, Wang X, Long W, Ni S, Yang Z, Ye T
Received 24 August 2023
Accepted for publication 13 December 2023
Published 28 December 2023 Volume 2023:16 Pages 6177—6188
DOI https://doi.org/10.2147/IJGM.S436999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Xingling He,1– 4,* Yanhui Jiang,1,* Sijing Li,1– 4,* Donghua Liu,1– 4 Ziru Li,1– 4 Xiaowei Han,1– 4 Xiaojiao Zhang,1– 4 Xiaoming Dong,1 Haohui Liu,1 Jie Huang,1 Xiaojing Wang,5 Wenjie Long,1 Shihao Ni,1– 4 Zhongqi Yang,1 Taochun Ye1
1Department of Geriatrics, The First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 2Lingnan Medical Research Center, Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 3University Key Laboratory of Traditional Chinese Medicine Prevention and Treatment of Chronic Heart Failure, Guangzhou, Guangdong Province, People’s Republic of China; 4Guangzhou Key Laboratory for Chinese Medicine Prevention and Treatment of Chronic Heart Failure, Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 5Clinical Medical Center, Tasly Pharmaceutical Group Co. Ltd., Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Taochun Ye; Zhongqi Yang, Email [email protected]; [email protected]
Background: Heart failure (HF) is a serious and terminal stage of various cardiac diseases and the most common complication of coronary heart disease (CHD). Previous clinical studies have shown that Qishen Yiqi dropping pills (QSYQ) have the effect of treating chronic heart failure. This study aims to evaluate the clinical efficacy, safety and optimal effective dose of QSYQ in treating CHD complicating chronic HF with reduced ejection fraction (HFrEF).
Methods: We will conduct a randomized, double-blind, placebo controlled, multicenter clinical trial. A total of 228 individuals from 16 hospitals in China will be randomly assigned to the low-dose, high-dose, and placebo groups in a ratio of 1:1:1. The trial consists of a screening period (standard medical treatment for at least 2 weeks) and a 12-week treatment period. After randomization, follow-up will be conducted at the 4th, 8th and 12th week. The primary outcomes will be the 6-Minute Walk Test (6MWT) at Week 12. Secondary outcomes will include 6MWT distance at Week 4 and 8, New York Heart Association (NYHA) functional classification, Traditional Chinese Medicine (TCM) Syndrome score, echocardiography indices, N-terminal pro-B-type natriuretic peptide (NT-proBNP), oxyhemoglobin saturation, Minnesota living with heart failure questionnaire (MLHFQ) score, grasp strength body mass index test and cardiovascular adverse events (AE).
Ethics and Dissemination: This trial has been approved by the Research Ethics Committee of the First Affiliated Hospital of Guangzhou University of Chinese Medicine, China (approval number: ZYYEC [2021]005). Written informed consent will be obtained from all participants. The results of this trial will be publicly shared through academic conferences and peer-reviewed journals.
Study Registration: Clinical Trials Registry (NCT04983043, Date: 07/08/2021, https://clinicaltrials.gov/ct2/show/NCT04983043).
Keywords: heart failure, coronary heart disease, Chinese medicine, QiShen YiQi Dripping Pill, syndrome of Qi deficiency with blood stasis
Introduction
HF is a complex clinical syndrome of impaired ventricular filling or ejection capacity caused by structural or functional abnormality of the heart.1 It is a severe manifestation of various advanced cardiac diseases.2,3 According to a Chinese epidemiological study, the prevalence of HF has increased by 44% during the past 15 years.4 Over 60 million HF patients are reported worldwide, five times the number of cancer patients.5 According to a recent survey, mortality among hospitalized patients with HF reaching 50% in five years following the onset of symptoms.6 With the acceleration of population aging, the prevalence of chronic diseases such as coronary heart disease and hypertension is on the rise.7 CHD is considered to be the main risk factor for the development of HF, and more than 50% of patients with heart failure in North America and Europe are the main cause.8 With the continuous high prevalence, mortality and readmission rate, HF has become one of the most serious cardiovascular diseases and one of the most common complications of CHD.3,9
One of the main pathogenesis of HFrEF is myocardial pathological remodeling, which leads to two key processes of HF progression, myocardial death and systemic reaction caused by excessive activation of neuroendocrine system.10 Current treatment options for chronic HFrEF include pharmacological and non-pharmacological treatments, aiming to prevent or reverse cardiac remodeling, alleviate clinical symptoms, improve quality of life, and reduce readmission and mortality.11,12 With the increasing number of patients with HF, how to further reduce the risk of death and hospitalization and improve the quality of life has become the focus of chronic heart failure (CHF) research.13 In today’s society, the treatment concept with traditional Chinese medicine characteristics has played an important role in the treatment of HF.14 In TCM, CHF can be used to explain some syndromes, such as “dyspnea”, “edema”, “palpitation” and “severe palpitation”. The pathophysiology of CHF is usually understood from the perspective of traditional TCM to be a condition marked by deficit in origin and excess in superficiality. The deficiency of origin is mainly Qi deficiency and the most frequent symptom is blood stasis.
QSYQ was developed and manufactured by Tasly Pharmaceutical Group Co., Ltd., approved by National Medical Products Administration in 2003 (Approval No.: GYZZ Z20030139; GYZZ Z20113048). It is a dripping pill preparation refined from the active ingredients of Astragalus, salvia and Panax notoginseng, and the volatile oil of Dalbergia odorifera, with the efficacy of invigorating qi and promoting blood circulation and relieving pain. It is clinically used to treat chest stuffiness. Previous ACT-IHF studies have shown that QSYQ has therapeutic effects on CHF, as indicated by an enhancement in left ventricular ejection fraction (LVEF), a decrease in NYHA functional class and modulation of B-type natriuretic peptide (BNP) levels.15 Laboratory studies have also demonstrated that QSYQ contain a variety of main bioactive components such as Salvianic acid A, tanshinone IIA, astragaloside and ginsenoside Rg1, which can improve myocardial injury, LVEF, and mitochondrial dysfunction in rats with HF.16
As a marketed drug, QSYQ has passed clinical and non clinical safety monitoring. The State Drug Administration issued the clinical trial notice (CYZB 1906600), approving the new clinical research with QSYQ as its main function in the treatment of CHF (qi deficiency and blood stasis syndrome). Therefore, in order to further improve the efficacy and safety observation indicators, this study plans to carry out a multicenter, randomized, double-blind, placebo-controlled parallel, standard drug addition trial, aiming to evaluate the clinical efficacy, safety and optimal dose of QSYQ in the treatment of chronic HFrEF (qi deficiency and blood stasis syndrome) caused by CHD.
Methods
Study Design
The study is a multi-center, randomized, double-blind, placebo-controlled trial with standard medicine added-on. Participants will enter a 2-week run-in phase during the screening period if they have not taken the prescribed medication for HFrEF for at least 2 weeks. Then, those eligible participants will be randomly assigned to the low-dose, high-dose and placebo group in a 1:1:1 ratio. The entire study is expected to last 12 weeks, and visit points are set up at the screening period, baseline, week 4 (± 2 days), week 8 (± 2 days) and week 12 (± 2 days) after treatment. Each participant will undergo a face-to-face visit assessment at a designated clinic on a scheduled date. The flowchart and timetable for the trial are shown in Figure 1 and Table 1.
 |
Table 1 Schedule of Assessments |
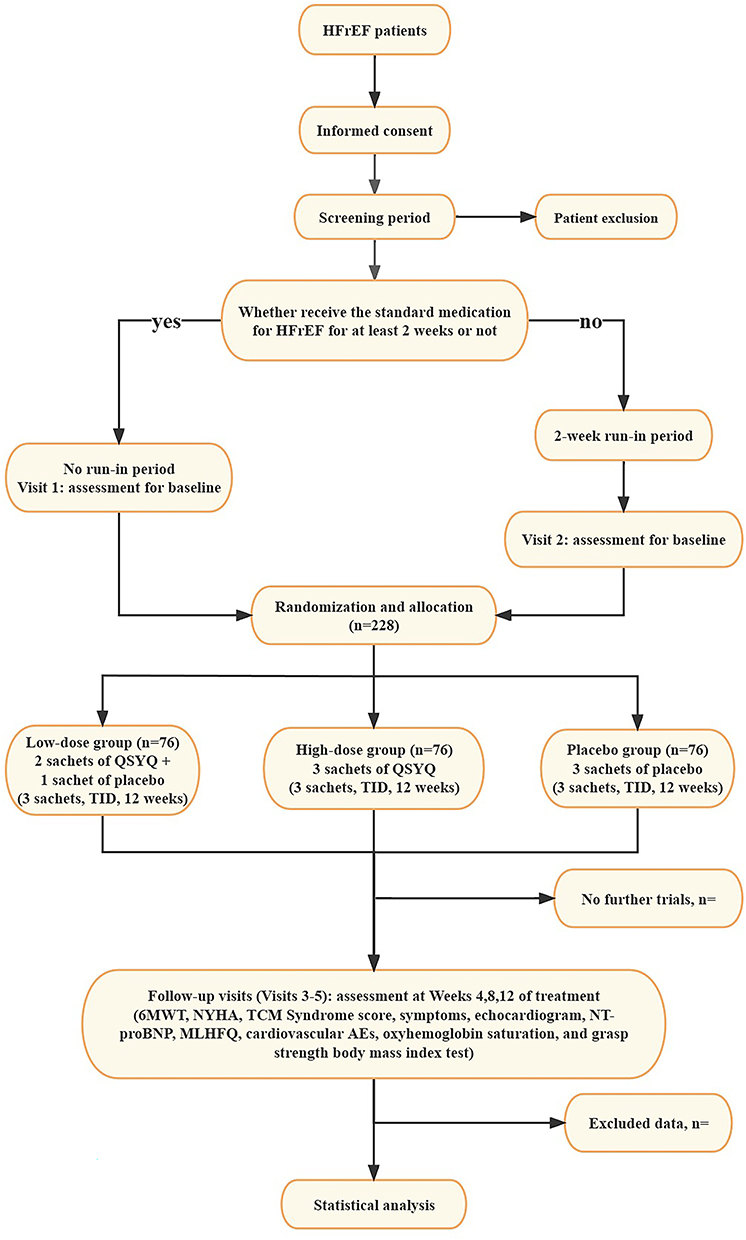 |
Figure 1 Flow chart of the study. The flow chart of enrolment, allocation, intervention and assessment. |
Study Setting
This trial is led by the First Affiliated Hospital of Guangzhou University of Chinese Medicine and will be simultaneously conducted in sixteen centers (Table 2). The subjects will be recruited through recruitment advertisements, which will be conducted in the outpatient department or independent reception room of each study location.
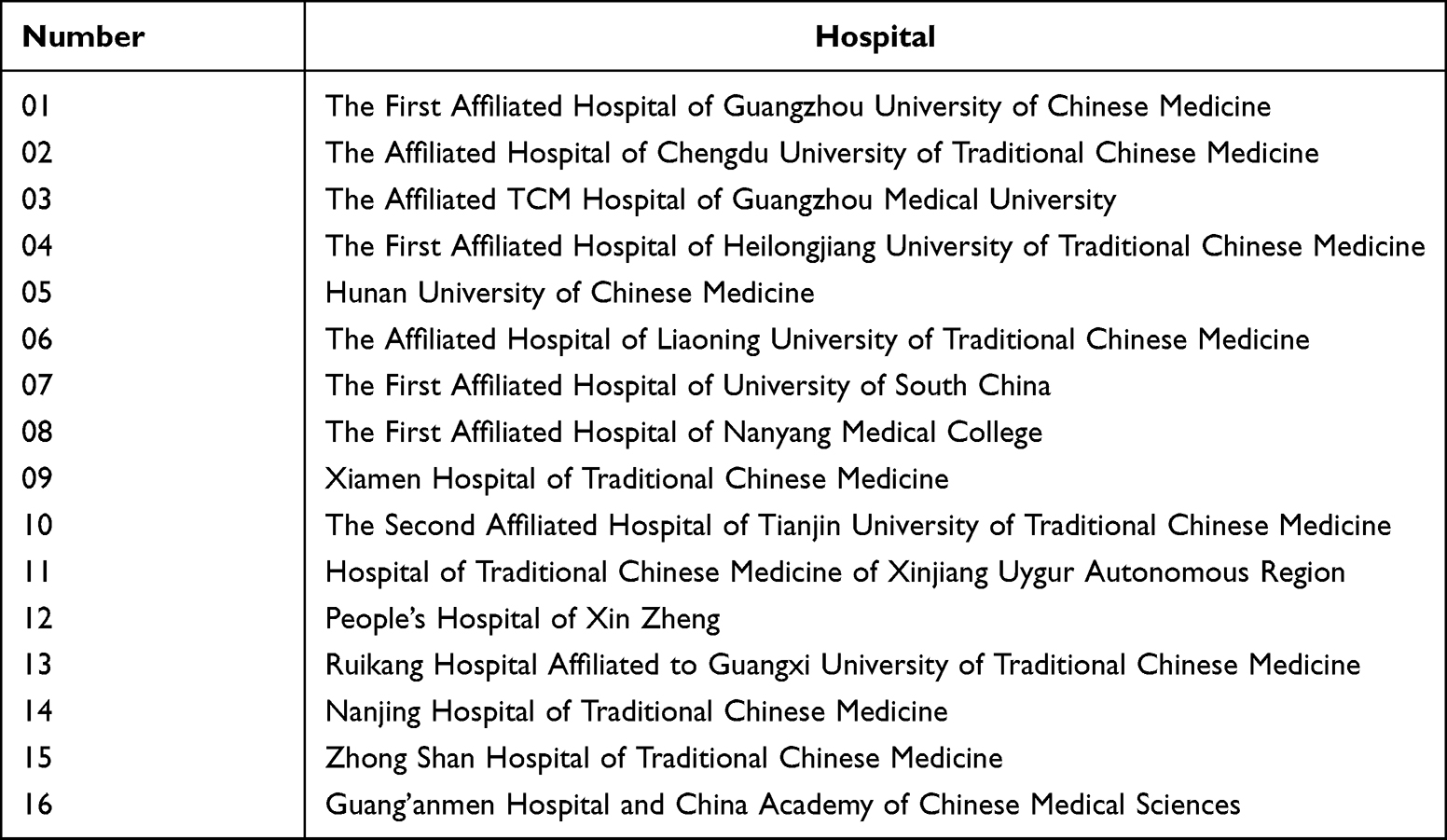 |
Table 2 Investigational Sites |
Participants
Inclusion Criteria
- Age 40–80 years, either sex;
- Meet the diagnostic criteria for CHD and CHF;
- Meet the TCM differentiation criteria of qi deficiency and blood stasis in CHF;
- LVEF < 45% (Modified Simpson’s Method);17
- Class II to IV for NYHA functional classification;
- Receive standard medication for CHF for at least 2 weeks, and do not receive intravenous administration of medication within 2 weeks;
- Understand the research requirements and are willing to provide written informed consent.
Exclusion Criteria
- HF caused by other heart diseases or systemic diseases, such as congenital heart disease, primary pulmonary hypertension, cardiomyopathy, heart valve disease, rheumatic disease, autoimmune disease, etc;
- Complicate with other severe medical conditions, such as pheochromocytoma, hematologic diseases, organ transplantation, and any cancer history;
- Severe or poorly controlled hypertension (systolic blood pressure ≥180mm Hg or diastolic blood pressure ≥110mm Hg); sitting blood pressure and systolic blood pressure ≤85mm Hg or symptomatic hypotension; severe primary diseases such as liver, kidney and haematopoietic system;
- Serum potassium ≥5.5 mmol/L;
- Patients with stable anticoagulant dose for less than 1 month, or INR > 3.0; Patients taking antiplatelet drugs for less than 1 month or with platelets below the lower limit of normal;
- Allergic to the investigational drug or its ingredients;
- Poorly controlled mental illness and drug addictions;
- Unable to complete 6MWT;
- Pregnant or lactating;
- Other situations judged by the researchers to be inappropriate for this study.
Withdrawal Criteria
- Refusal to continue the trial;
- Do not explicitly withdraw from the study but no longer receive treatment and follow-up;
- Poor compliance;
- Occurrence of some complications, serious adverse events (SAE) or special physiological changes that are not suitable for continued participation in the study;
- Unblinding.
If it is possible, investigators should take active steps to complete the last test for the analysis of efficacy and safety in case of any drop-out, withdrawal and loss to follow-up. Moreover, the study summary and reason for withdrawal should be filled in the case report form (CRF).
Randomization
The central block randomization method will be used for randomized allocation. The randomization sequence will be generated by a statistician of a third-party statistical unit (Department of Biostatistics, Southern Medical University) using SAS 9.4. The predetermined values of parameters such as block length and seed number will be recorded in a random number table to strengthen the interval validity of the design. Each sequential number will correspond to a sealed opaque envelope containing the information on the randomization group, according to a previously prepared randomized list of numbers, so as to guarantee concealment. The patients who meet the inclusion criteria will be assigned in a successive order according to the corresponding random numbers from small to large extracted in the order of their enrollment.
Blinding
The blinding of drugs shall be participated by the personnel of the statistical unit and those unrelated to the trial in the sponsor. The test drugs are packaged separately according to the visit time of the subjects, that is, an independent number of drugs will be issued during each visit during the treatment period. Neither the participants nor the medical team who treated them knew the grouping and could not determine the treatment method. The blind base is in duplicate, sealed and stored at the sponsor and the unblinded statistician respectively. In case of emergency, this test uses electronic emergency letters to unblind, and each random number corresponds to an emergency letter. Emergency unblinding will be carried out in Interactive Web Response System (IWRS), and the investigator will apply for authorization from the principal investigator, and all operation tracks will be retained.
Interventions
The trial consists of two parts: a screening period and a 12-week treatment period. After randomization, participants will receive 12 weeks of low-dose QSYQ, high-dose QSYQ, or placebo based on standard HFrEF medication (Figure 2).
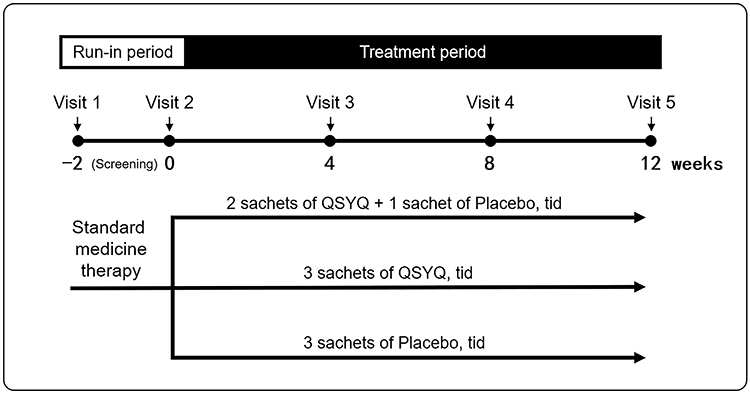 |
Figure 2 Study program for each subject. Abbreviation: QSYQ, QiShen YiQi Dripping Pill. |
Standard Medications
The standard medications for the HFrEF are detailed in Supplementary Material 1, as follows: (1) Improve cardiac remodeling: RAAS inhibitors, ACEIs/ ARBs/ ARNIs, or adding MRA (Supplementary Table 1); (2) Inhibit sympathetic nerve: Beta-blockers, or adding Ivabradine (Supplementary Table 2); (3) Reduce water-sodium retention: oral diuretics (Supplementary Table 3); (4) Cardiotonics: Digitalis. This treatment will remain unchanged during the trial unless patients experience clinically meaningful or SAEs.
Investigational Drug
Participants will receive a packed medicine kit every four weeks, for a total of three times. During the trial, different groups will receive the following treatments:
- Low-dose Group: Administered orally 2 sachets of QSYQ (0.52 g/sachet) and 1 sachet of QSYQ placebo (0.52 g/sachet) each time, 3 times a day for 12 weeks;
- High-dose Group: Administered orally 3 sachets of QSYQ (0.52 g/sachet) each time, 3 times a day for 12 weeks;
- Placebo Group: Administered orally 3 sachets of QSYQ placebo (0.52 g/sachet) each time, 3 times a day for 12 weeks.
In order to ensure good compliance, researchers will patiently explain to patients the significance of the trial and the importance of taking medicine on time. The amount of medication received, utilized, and returned by participants will be recorded in the CRFs to assess treatment adherence.
Prohibited Medications
During the study, other drugs for the treatment of CHF (such as Trimetazidine, Nicorandil, Dapagliflozin, Empagliflozin and Vericiguat) and any TCM should not be used. Relevant concomitant medications will be documented in the CRF as scheduled by the event.
Outcome Assessment
Primary Outcomes
6MWT distance: the change from baseline to Week 12. Determine the total mileage on the registration form and use the absolute change in 6MWT to assess the effectiveness of the treatment.
Secondary Outcomes
- 6MWT distance at Week 4 and 8;
- NYHA functional classification: In this study, we will measure the percentage of participants whose NYHA functional classification is improved/worsened/unchanged from baseline to Week 4, 8 and 12;
- TCM Syndrome score: change from baseline to Week 4, 8 and 12 in TCM Syndrome score. Three primary symptoms and 4 secondary symptoms are present. The state of the tongue and pulse is used to evaluate and score TCM symptoms. TCM basic symptoms are scored as follows: without = 0 points, light = 2 points, medium = 4 points, and heavy = 6 points. Secondary symptoms in TCM are graded as follows: absent = 0 points, present = 1 points.
 ;
; - Dyspnea, weakness and edema: From baseline to Week 4, 8, and 12, the rate of change and elimination of the symptoms (dyspnea, weakness, and edema) will be assessed;
- Echocardiogram: Measurements will be made of the left ventricle’s end diastolic diameter (LVEDD), end diastolic volume (LVEDV), end systolic volume (LVESV), LVEF, stroke volume (SV), and cardiac output (CO);
- NT-proBNP: NT-proBNP should be measured at baseline and at each subsequent visit, and the changes from baseline to Week 4, 8, and 12 should be evaluated. All the tests will be carried out by a central laboratory;
- MLHFQ Score: The MLHFQ consists of 21 elements representing varying degrees of impact of HF on health-related quality of life. Each item in this questionnaire is scored from 0 (none) to 5 (very much), and the total item score is from 0 (none) to 105 (very much);
- Cardiovascular AEs: To assess whether the incidence of cardiovascular AEs is higher than that in the placebo group during the study.
Exploratory Outcomes
- Peripheral blood oxygen saturation: An estimation of lung oxygenation and hemoglobin oxygen-carrying capacity is provided by monitoring peripheral oxygen saturation at baseline and each visit;
- Grip strength body mass index test: Every participant held the hand dynamometer firmly in one hand. The grip strength index was calculated by comparing the best performance with the body weight after holding the hand twice.
Safety Outcomes
As part of the safety evaluation process, vital signs, physical exams, lab testing, and AEs will be tracked throughout the study. Vital signs include body temperature, blood pressure, pulse and respiratory rate. Laboratory tests comprise complete blood count (white blood cell count, red blood cell count, hemoglobin, platelet, neutrophil count, eosinophil count, basophil count, and lymphocyte count), routine urine test (urine leukocytes, urine latent blood, urine protein, urine glucose, and ketonuria), serum electrolytes (serum potassium, serum natrium, and serum chlorine), liver function tests (alanine aminotransferase, aspartate transaminase, total bilirubin, γ-glutamyl transferase, and alkaline phosphatase), renal function tests (serum creatinine, and blood urea nitrogen), fasting blood-glucose, coagulation function (prothrombin time, activated partial thromboplastin time, thrombin time, fibrinogen, and international normalized ratio) and 12-lead electrocardiogram.
Investigators will frequently phone participants to check for any adverse events between the period they received the investigational medicine and their last follow-up visit. For all AEs, investigators will accurately fill in the “Adverse Event Record Form” in the study medical record and electronic Case Report Form (eCRF). If an AE or adverse reaction should occur in the trial, the researchers will take necessary measures to ensure the participant’s safety, record the event and determine whether the trial needs to be terminated at that time.
Sample Size Calculation
To the best of our knowledge, there are no previous studies on treating HFrEF due to CHD with QSYQ. An improvement of 6MWT distance was used as the main effect index according to the statistical requirements.18 We assumed the mean difference of 40, with a pooled SD of 45 for each group, α=0.05 (the significant level), and β=0.2 (power of 0.8). The sample size of each group will be estimated to be 63 (1:1:1 sample size ratio). To guarantee that the study has sufficient power to address the relevant research issue, a further 20% drop-out rate is assumed, and a total of 228 individuals (76 in each arm) will be enrolled.
Quality Control and Assurance
Data collection and management for this project will be done using an electronic Case Report Form (eCRF). According to the eCRF filling standards, the data administrator enters the original data into the eCRF in an accurate, timely, comprehensive and standardized manner. Investigators will carry out electronic signature verification after data submission and source data verification (SDV). Modifications to eCRF data must adhere to applicable standard operating procedures. If modified, the traces of changes must be retained, and re-signature verification is required. The monitor will examine the eCRF’s agreement with the source data. Researchers must strictly keep confidential the documents that display the identity of the subjects. In the case report form or other documents, only uppercase letters, numbers, and/or codes can be used to identify the subject, and the subject’s name cannot be used. Promptly, investigators must respond to any queries proposed by the electronic data capture (EDC) logic checker, monitor, or data administrator. The database locking record will be co-signed by the principal investigator, the sponsor, the statistician, and the data administrator after all the data are input. Then, the data administrator will lock the database. The database will be shut down by the data administrator after the statistical analysis is finished. In this study, special monitors will supervise the progress of the study, the source data verification, the administration of investigational drugs, and the compliance and ethics of clinical operations.
Statistical Analysis
SAS 9.4 will be used for analysis. All statistical tests will be conducted with a two-sided design, and difference will be considered significant if P < 0.05.
The randomized participants who have received therapy at least once and have any post-treatment data will be included in the full analysis set (FAS). Intention-to-treat (ITT) analysis will serve as the primary foundation for the effectiveness measurement analysis used to assess FAS data. According to the principle of the last observation carried forward (LOCF), we will take the data of the most recent follow-up visit as the final result of missing data. Participants who have consumed the experimental substance at least once will be the subject of a safety analysis.
Descriptive statistics will be used for drug exposure. The percentage of participants with medication compliance of 80–120% will be calculated. Medication compliance will be calculated using the medication counting method: Medication compliance = (Actual doses taken/Required doses) × 100%, where actual doses taken = the sum of actual dose taken; Required doses = the sum of protocol-specified doses required to be taken. The demographic characteristics and other baseline data will be described. Continuous variables will be expressed as several cases, mean, standard deviation, median, quartile, maximums, and minimums. Enumeration and rank data will be presented in terms of frequency and component proportions. Analysis of variance (ANCOVA) will be applied to the analysis of the changes in 6MWT distance, echocardiogram results, NT-proBNP, MLHFQ score, oxyhemoglobin saturation, and grasp strength body mass index test. Ranked data will be analyzed by Clopper-Pearson or Cochran-Mantel-Haensel χ2 test. Cardiovascular AE will be analyzed by Pearson χ2 and CMH χ2 tests. The primary outcome measurement will also be conducted by subgroup analysis based on LVEF (<40%, 40% to 45%) and NYHA functional classification (Class II, Class III).
Ethics Approval
Ethics approval was obtained from the Clinical Research Ethics Committee of the First Affiliated Hospital of Guangzhou University of Chinese Medicine (No. ZYYEC-2021-005) on 30 March 2021. The study has been registered in ClinicalTrials.gov with the ID NCT04983043 and updated on November 17, 2022 (Version 2.0). All items were drawn from the World Health Organization Trial Registration Dataset. The trial’s test medication, QiShen YiQi Dripping Pills, is a commercially available drug with the National Medical Products Administration approval (Approval Nos.: GYZZ Z20030139; GYZZ Z20113048). Tasly Pharmaceutical Group Co., LTD., the trial’s manufacturer, has been informed of the trial and has provided the test drug and placebo for this trial. Prior to enrollment, each participant will sign an informed consent form, and they will only be treated by a licensed clinician throughout the study. The study will adhere to the Helsinki Declaration, participants can decide to leave the trial at any moment, and any information that might reveal personal information will be kept secret.
Discussion
According to epidemiological data, the prevalence of HF in China is increasing.3,19 HFrEF is one of the common types of chronic heart failure. In the 2022 AHA/ACC/HFSA heart failure guidelines, the dynamic evolution of ejection fraction is underlined, and a sustained drop in ejection fraction is a sign of a poor prognosis.2 The main goal of clinical CHF treatment is to lower death and re-admission rates while enhancing the quality of life. At present, most patients with HF receive standard medical treatment based on guideline recommendations. Although it can improve some clinical symptoms of patients, the overall curative effect is not very satisfactory.13 How to further reduce the mortality and hospitalization rate of patients with CHF and improve the quality of life is still the difficulty and research focus of clinical treatment. TCM has shown certain advantages in the clinical treatment of HF by using the holistic concept and the method of syndrome differentiation and treatment.14 Qi deficiency and blood stasis syndrome is a common type in patients with HF and CHD. QSYQ is a Chinese patent medicine with the effect of activating blood circulation and removing blood stasis. Previous clinical studies manifested that QSYQ treatment added with standard medication is effective in improving the exercise tolerance of ischemic HF patients, which is reflected in extended 6MWT distance and significantly improved MLHFQ score.15 And a meta-analysis also showed that the addition of QSYQ extended the 6MWT distance, improved the left ventricular ejection fraction and reduced the level of NT-proBNP.20 Thus, QSYQ combined with Western therapy might be effective in treating HF patients.
The State Drug Administration approved the clinical study of QSYQ in the treatment of CHF (Qi deficiency and blood stasis syndrome), and stressed that attention should be paid to human experience and laboratory results to set the dose reasonably. As the main efficacy index of this trial, the 6MWT is a method to evaluate exercise capacity by measuring the distance walked in 6 minutes, which is widely used to evaluate the exercise tolerance of patients with HF, and can provide credible data about patients’ overall functional condition.21 Quality of life and symptoms were utilized in this study as observation indicators to assess from the viewpoints of doctors and patients, which helped to improve the objectivity of evaluation and reduce information bias. One of the therapeutic objectives for HF, according to several worldwide recommendations, is to improve quality of life.22 And the level of NT-proBNP is a significant biomarker for determining the prognosis of HF.23 Therefore, this phase II clinical study will explore the optimal dose of QSYQ in the treatment of patients with HFrEF due to CHD (Qi deficiency and blood stasis syndrome), confirm its safety and efficacy, and evaluate the improvement of exercise capacity and quality of life of patients with QSYQ.
To our knowledge, this is the first clinical study to explore the efficacy and safety of QSYQ in the treatment of CHD combined with HErEF (qi deficiency and blood stasis syndrome). At the same time, this study aims to explore the optimal therapeutic dose of QSYQ. If this study confirms the effectiveness, safety, and optimal dosage of QSYQ, the results will be used to develop reliable treatment plans for HF patients and provide new evidence-based medicine for the combination of traditional Chinese and Western medicine treatment of HF.
Abbreviations
6MWT, 6-Minute walk test; ANCOVA, Analysis of variance; ACEI, Angiotensin converting enzyme inhibitor; AE, Adverse event; ALT, Alanine aminotransferase; ARB, Angiotensin receptor blocker; ARNI, Angiotensin receptor-neprilysin inhibitor; BNP, Type B natriuretic peptide; CHD, Coronary heart disease; CHF, Chronic Heart failure; CO, Cardiac output; CRF, Case Report Form; CRT, Cardiac resynchronization therapy; EDC, Electronic data capture; eCRF, Electronic Case Report Form; eGFR, Estimated glomerular filtration rate; FAS, Full analysis set; HbA1c, Glycated haemoglobin; HF, Heart failure; HFrEF, Heart failure with reduced ejection fraction; ICD, Implantable cardioverter-defibrillator; IHF, Ischemic heart failure; INR, International normalized ratio; ITT, Intention-to-treat; IWRS, Interactive web response system; LOCF, Last observation carried forward; LVEDD, Left ventricle’s end diastolic diameter; LVEDV, Left ventricle’s end diastolic volume; LVEF, Left Ventricular Ejection Fraction; LVESV, Left ventricle’s end systolic volume; MLHFQ, Minnesota living with heart failure questionnaire; MRA, Mineralocorticoid receptor antagonist; NT-proBNP, N-terminal pro-B-type natriuretic peptide; NYHA, New York heart association; QSYQ, QiShen YiQi Dripping Pill; RAAS, Renin-angiotensin-aldosterone system; SDV, Source data verification; SV, Stroke volume; TCM, Traditional Chinese Medicine.
Trial Status
This study was registered with the Chinese Clinical Trial Register (NCT04983043) on July 8, 2021. The recruitment of participants has started in July 2021 and is going.
Data Sharing Statement
This is a research proposal so there are currently no available data. Further information not included in this article will be provided by the corresponding author upon completion of the trial.
Consent for Publication
The trial results will be published in a peer-reviewed journal or presented at academic conferences. All participants contributing substantively to the trial are recognized in the form of granting authorship.
Acknowledgments
We appreciate all of the participants who will cooperate with our research as well as the researchers and institutions who will work on this project together. In particular, we would like to thank the research centers that participated in this study, as well as the statistical and methodological experts from Southern Medical University.
Funding
This study is supported by the National Natural Science Foundation of China (Grant number: 82205236), Research Project of Traditional Chinese medicine Bureau of Guangdong Province (No. 2022ZYYJ01), Joint Funding Program between the City and the University/Institute (College) (No. 202201020474) and Guangzhou Science and Technology Plan Project (No. 202102080228). The funding sources have no role in the design of this study and will play no role in its execution, analyses, data interpretation, or decision to submit results.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Baman JR, Ahmad FS. Heart Failure. JAMA. 2020;324(10):1015. doi:10.1001/jama.2020.13310
2. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79(17):1757–1780. doi:10.1016/j.jacc.2021.12.011
3. Savarese G, Becher PM, Lund LH, Seferovic P, Rosano GMC, Coats AJS. Global burden of heart failure: a comprehensive and updated review of epidemiology. Cardiovasc Res. 2023;118(17):3272–3287. doi:10.1093/cvr/cvac013
4. Hao G, Wang X, Chen Z, et al. Prevalence of heart failure and left ventricular dysfunction in China: the China Hypertension Survey, 2012–2015. Eur J Heart Fail. 2019;21(11):1329–1337. doi:10.1002/ejhf.1629
5. Bragazzi NL, Zhong W, Shu J, et al. Burden of heart failure and underlying causes in 195 countries and territories from 1990 to 2017. Eur J Prevent Cardiol. 2021;28(15):1682–1690. doi:10.1093/eurjpc/zwaa147
6. Park LG, Dracup K, Whooley MA, et al. Sedentary lifestyle associated with mortality in rural patients with heart failure. Eur J Cardiovasc Nurs. 2019;18(4):318–324. doi:10.1177/1474515118822967
7. Groenewegen A, Rutten FH, Mosterd A, et al. Epidemiology of heart failure. Eur J Heart Fail. 2020;22(8):1342–1356. doi:10.1002/ejhf.1858
8. Pagliaro BR, Cannata F, Stefanini GG, et al. Myocardial ischemia and coronary disease in heart failure. Heart Fail Rev. 2020;25(1):53–65. doi:10.1007/s10741-019-09831-z
9. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Rev esp cardiologia. 2022;75(6):523. doi:10.1016/j.rec.2022.05.005
10. Murphy SP, Ibrahim NE, Januzzi JL. Heart failure with reduced ejection fraction: a review. JAMA. 2020;324(5):488–504. doi:10.1001/jama.2020.10262
11. Boorsma EM, Ter Maaten JM, Damman K, et al. Congestion in heart failure: a contemporary look at physiology, diagnosis and treatment. Nat Rev Cardiol. 2020;17(10):641–655. doi:10.1038/s41569-020-0379-7
12. Liang B, Zhao YX, Zhang XX, et al. Reappraisal on pharmacological and mechanical treatments of heart failure. Cardiovasc Diabetol. 2020;19(1):55. doi:10.1186/s12933-020-01024-5
13. Greene SJ, Fonarow GC, Butler J. Risk profiles in heart failure: baseline, residual, worsening, and advanced heart failure risk. Circulation. 2020;13(6):e007132. doi:10.1161/CIRCHEARTFAILURE.120.007132
14. Liang B, Gu N. Traditional Chinese Medicine for coronary artery disease treatment: clinical evidence from randomized controlled trials. Front Cardiovasc Med. 2021;8:702110. doi:10.3389/fcvm.2021.702110
15. Mao J, Zhang J, Lam CSP, et al. Qishen Yiqi dripping pills for chronic ischaemic heart failure: results of the CACT-IHF randomized clinical trial. ESC Heart Fail. 2020;7(6):3881–3890. doi:10.1002/ehf2.12980
16. Zhang Y, Yu J, Zhang W, et al. An integrated evidence-based targeting strategy for determining combinatorial bioactive ingredients of a compound herbal medicine Qishen Yiqi dripping pills. J Ethnopharmacol. 2018;219:288–298. doi:10.1016/j.jep.2018.02.041
17. Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiography. 2005;18(12):1440–1463. doi:10.1016/j.echo.2005.10.005
18. Liang B, Qu Y, Zhao QF, et al. Guanxin V for coronary artery disease: a retrospective study. Biomed Pharmacother. 2020;128:110280. doi:10.1016/j.biopha.2020.110280
19. Wang H, Chai K, Du M, et al. Prevalence and incidence of heart failure among urban patients in China: a national population-based analysis. Circulation. 2021;14(10):e008406. doi:10.1161/CIRCHEARTFAILURE.121.008406
20. Wang H, Li L, Qing X, et al. Efficacy of Qishen Yiqi Drop Pill for chronic heart failure: an updated meta-analysis of 85 studies. Cardiovasc Ther. 2020;2020:8138764. doi:10.1155/2020/8138764
21. Giannitsi S, Bougiakli M, Bechlioulis A, et al. 6-minute walking test: a useful tool in the management of heart failure patients. Therap Adv Cardiovasc Dis. 2019;13:1753944719870084. doi:10.1177/1753944719870084
22. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;18(8):891–975. doi:10.1002/ejhf.592
23. Salah K, Stienen S, Pinto YM, et al. Prognosis and NT-proBNP in heart failure patients with preserved versus reduced ejection fraction. Heart. 2019;105(15):1182–1189. doi:10.1136/heartjnl-2018-314173
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.